Embed Size (px)
Citation preview

Ovarian Cancer
Screening
DR SUJATA DHANUKA Associate Vice President- Medico-Marketing
METROPOLIS HEALTHCARE LTD

Ovarian cancer accounts for nearly 4% of all cancers among women
Fifth most common cause of cancer related death in women
Age adjusted incidence is 2 to 15 cases per 100,000 women
Ovarian cancer is commonly referred to as the ‘silent killer’ as it
causes vague symptoms and can be confused with other conditions
Most women present with advanced disease which are difficult to treat,
resulting in poor survival rate (5 year survival rate less than 35%)
Therefore diagnosing ovarian cancer in early stages becomes crucial
where tumor markers may play an important role. If ovarian cancer
is detected early, 5 year survival is dramatically improved (86%)
Facts form NICE Guidelines for Ovarian Cancer 2011
Introduction

Who should be screened?
• Women at average risk
(relative risk less than 3
times the relative risk of the
general population)
– A history of breast cancer
diagnosed at age 41 or older
and no family history of
breast or ovarian
– A history of infertility and/or
use of assisted reproductive
therapies, such as in vitro
fertilization (IVF).
– A history of endometriosis
– A history of hormone
replacement use for the
management of symptoms
related to menopause.
• Women at increased
risk (relative risk 3 to 6
times greater than that
of the general
population)
– A first degree relative
with ovarian cancer.
– A personal history of
breast cancer prior to
age 40 or A personal
history of breast cancer
in one or more close
relatives diagnosed
with breast or ovarian
cancer at any age.
• Women at inherited
increased risk
(relative risk > 6
times that of the
general population)
- Presence of a BRCA1 or
BRCA2 mutation.
- Presence of a mismatch
repair gene mutation
associated with a
hereditary cancer
syndrome known as
Hereditary Non-
Polyposis Colon
Cancer (HNPCC)
/Lynch syndrome.
3 types of patient groups:

Primary ovarian cancer markers Ovarian tumour Traditional markers
Epithelial tumours Ca-125, CEA, Ca 19.9
CA 72-4/TAG 72
Germ cell tumours
-fetoprotein,
- HCG,
Serum PLAP & LDH
Sex cord stromal tumours
Estradiol, testosterone &
inhibin

Tumour Markers Produced by Epithelial Ovarian Tumours
TUMOUR PERCENT OF TUMOURS
PRODUCING MARKERS
CA125 CA19-9 CEA PLAP
SEROUS: -
Benign
Borderline
Malignant
80
98
99
6
87
40
0
6
17
83
93
84
MUCINOUS: - Benign Borderline Malignant
0
12.5 16
73 87 86
45 87 97
0 0 0
ENDOMETROID CA 66 64 25 66
CLEAR CELL CA 75 70 15 0
UNDIFFERENTIATED 82 52 23 57
MIXED MULLERIAN tumour 80 80 40 33

CA-125 It is the most widely used tumor marker in diagnosis & prognosis of
Epithelial ovarian cancer
CA-125 as a screening test was initiated by the fact that about 83% of
patients with epithelial ovarian cancers have elevated levels
Also found in other tissues such as mesothelial cells of the pleura,
peritoneum, pericardium
However, it lacks sensitivity and specificity
In only 50% of symptomatic stage I cases are serum levels of CA 125
found to be elevated, as compared with the levels in 80% of
advanced-stage cases.

Lack of specificity Elevated in • Benign gynaecology – Endometriosis, Fibroids, Pelvic Inflammatory Disease • Other peritoneal inflammation • Cyclical variations in pre-menopausal age group • Benign conditions- Urinary retention, Chronic renal failure, Pancreatitis • Other malignant disease – gastric and lung
Lack of sensitivity
• Ca 125 not raised in 30% of women with ovarian cancer – early stage disease
Ca 125 levels U/mL Sensitivity % Specificity %
65 and greater 79 82
150 69 93
190 63 95

RMI (Risk of Malignancy Index)
It is a correlation of Clinical, USG findings and CA-125 levels
Feature RMI 1 Score RMI 2 Score
Ultrasound features:
•Multilocular cyst
•solid areas
•bilateral lesions
• Ascites
•intra-abdominal
metastases
0= none
1= one abnormality
3= two or more
abnormalities
0= none
1= one abnormality
4= two or more
abnormalities
Premenopausal 1 1
Postmenopausal 3 4
CA125 U/ml U/ml
RMI score = ultrasound score x menopausal score x CA125 level in U/ml.
The RMI 2 score was more sensitive than the RMI 1 system with results of 74 to 80% at a specificity of 89 to 92% and positive predictive values around 80%

RMI (Risk of Malignancy Index)
Jacobs I et al. Br J Obstet Gynecol.1990; 97:992-929.
RMI
Score
Sensitivity
(%)
Specificity
(%)
Likelihood ratio for
malignancy if
result is
Positive Negative
25 100 62.2 2.7 0.00
50 95.1 76.5 4.1 0.06
75 92.7 84.7 6.1 0.09
100 85.4 87.8 7.0 0.17
150 85.4 93.9 14.0 0.16
200 85.4 96.9 42.1 0.15
250 78.0 99.0 76.9 0.22
The RMI scoring system is the method of choice for predicting whether or not an
ovarian mass is likely to be malignant.
Women with an RMI score >200 should be referred to a center with experience in
ovarian cancer surgery.

HE4
Human Epididymis Protein 4 (HE4) is a relatively new marker for ovarian cancer
HE4 is over expressed in patients with ovarian cancers whereas normal ovarian
tissue has minimal production of HE4
Data suggests that HE4 and CA-125 have comparable sensitivities and
specificities; however HE4 is a better marker in the detection of early stages of
ovarian cancer
Also, HE4 has a better ability to discriminate cancer from benign disease based
on its sensitivity in this patient population

HE4 + CA-125
Recent investigations revealed that adding HE4 to CA-125 resulted in an
increased sensitivity and specificity than either marker alone
HE4 in combination with CA 125 is a more accurate tool for differential diagnosis
of ovarian cancer from a benign ovarian cyst or endometriosis (another benign
condition)

HE4 – Clinical Studies
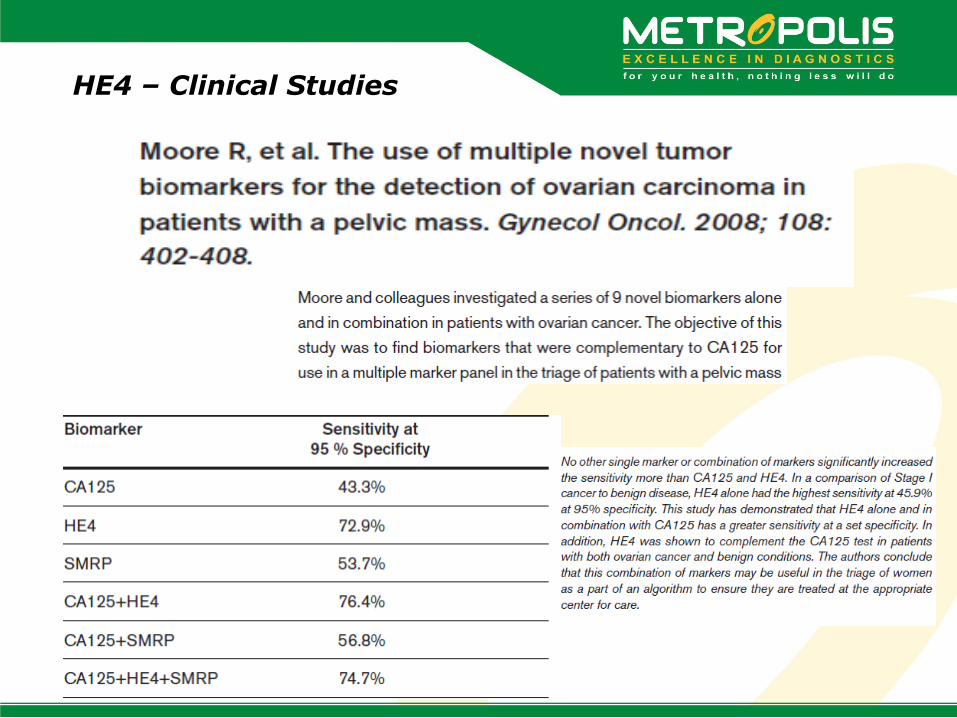
HE4 – Clinical Studies

HE4 – Clinical Studies

ROMA (Risk of Ovarian Malignancy Algorithm)
ROMA is a risk stratification tool that combines CA 125 and HE4 levels and uses
an algorithm to compute malignancy risk in a patient with pelvic mass
ROMA correctly classifies 89% of epithelial ovarian cancers (EOC) and low
malignant potential tumors as high risk and 75% of benign disease as low risk
The negative predictive value for the combined population was 93.9%, meaning
that there was a false negative rate of only 6%
The use of this combination assay will help to ensure that patients are given
optimal care by stratifying those at high risk to tertiary care centers that
specialize in ovarian cancer

ROMA vs RMI
ROMA has an increased sensitivity compared with RMI
At a specificity of 75%, the ROMA had a sensitivity of 94%, compared to the RMI, which
achieved a sensitivity of 85%.
This difference was found to be statistically significant.
Pre & Post Menopausal
Benign (n=315) vs EOC, All stages (n=124)
Sensitivity (95% CI) Specificity (95% CI)
RMI 85% (77% to 90%) 75% (70% to 80%)
ROMA™ 94% (89% to 98%) 75% (70% to 80%)
CI: Confidence Interval

ROMA vs RMI
When you look at early stage I & II invasive EOC patients, the ROMA achieved a
sensitivity of 86%, compared with a sensitivity of only 66% for the RMI.
This difference approached statistical significance with a p value of 0.05.
Pre & Post Menopausal
Benign (n=315) vs Stage I-II EOC (n=35)
Sensitivity (95% CI) Specificity (95% CI)
RMI 66% (48% to 81%) 75% (70% to 80%)
ROMA™ 86% (70% to 95%) 75% (70% to 80%)
CI: Confidence Interval
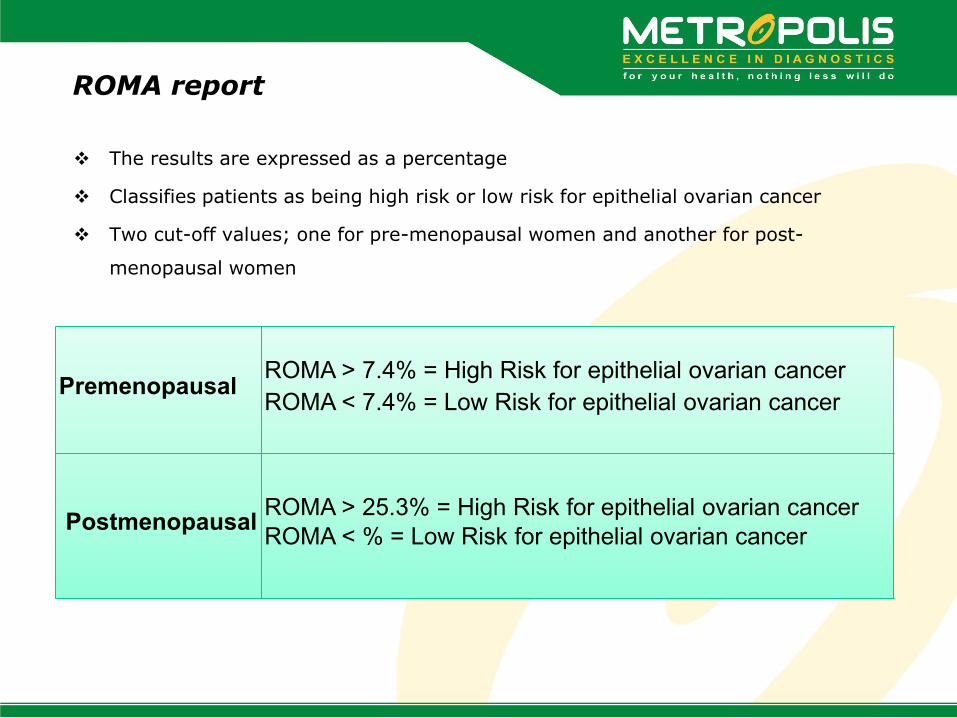
ROMA report
The results are expressed as a percentage
Classifies patients as being high risk or low risk for epithelial ovarian cancer
Two cut-off values; one for pre-menopausal women and another for post-
menopausal women
Premenopausal ROMA > 7.4% = High Risk for epithelial ovarian cancer ROMA < 7.4% = Low Risk for epithelial ovarian cancer
Postmenopausal ROMA > 25.3% = High Risk for epithelial ovarian cancer
ROMA < % = Low Risk for epithelial ovarian cancer

HE4 @ Metropolis

LIMITATIONS –
- HE4 serum concentrations in healthy individuals were related to
age with significantly higher concentrations in postmenopausal
women.
- Renal failure and effusions were the most important sources of
false positive HE4 serum concentrations. HE4 must be
interpreted carefully in patients with renal failure.
HE4- Limitations

Summary
HE4 levels are elevated in more than 50% of tumors that do not express
CA125
Combination assay results in a higher sensitivity and specificity than the
currently accepted Risk of Malignancy Index (RMI), with 87.4% sensitivity
and 56.8% specificity
CA125 + HE4 or HE4 alone have been shown to have greater sensitivity in
patients with early stage disease than CA125 alone
The combination of CA125 + HE4 is an accurate tool to stratify women
with a pelvic mass at risk for ovarian cancer.

Ovplex
The Ovplex is a diagnostic test for ovarian cancer, based on the presence of 5 biomarkers:
CA-125 C-Reactive Protein (CRP) Serum Amyloid A (SSA) Interleukin 6 (IL 6) Interleukin 8 (IL 8)
An algorithm is used to analyze the plasma concentrations of the above biomarkers and the results are expressed as the ‘Ovplex Index’ or the probability that the woman has ovarian cancer
Ovplex targets symptomatic women and is statistically significantly better than CA 125 alone in the detection of ovarian cancer
OvPlex™ outperforms CA125 for the detection of ovarian cancer in all stages of the disease - particularly, early stage
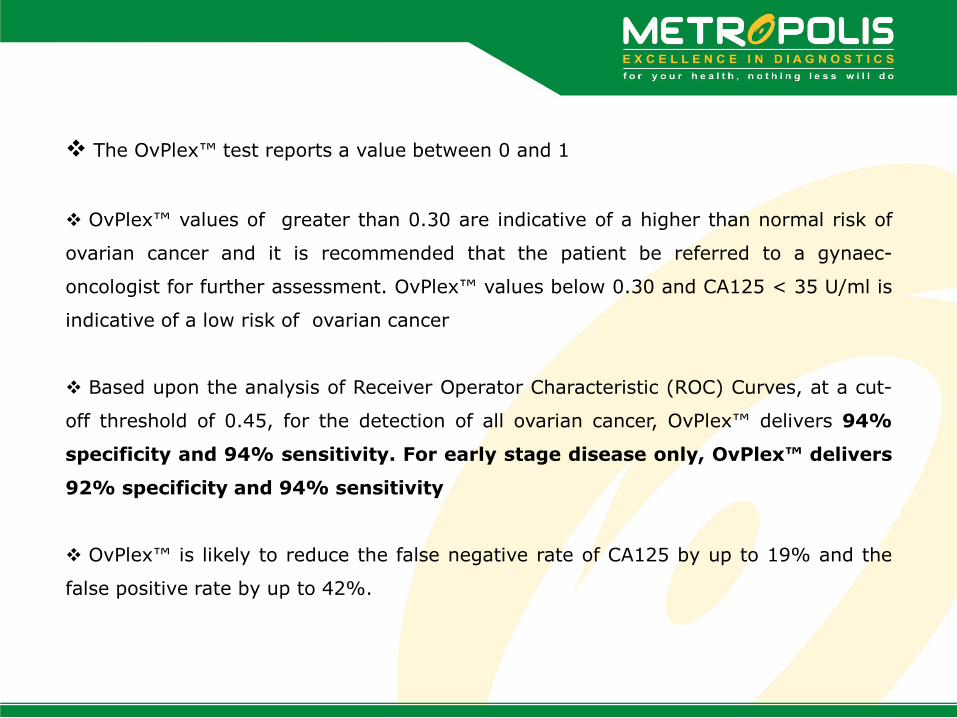
The OvPlex™ test reports a value between 0 and 1
OvPlex™ values of greater than 0.30 are indicative of a higher than normal risk of
ovarian cancer and it is recommended that the patient be referred to a gynaec-
oncologist for further assessment. OvPlex™ values below 0.30 and CA125 < 35 U/ml is
indicative of a low risk of ovarian cancer
Based upon the analysis of Receiver Operator Characteristic (ROC) Curves, at a cut-
off threshold of 0.45, for the detection of all ovarian cancer, OvPlex™ delivers 94%
specificity and 94% sensitivity. For early stage disease only, OvPlex™ delivers
92% specificity and 94% sensitivity
OvPlex™ is likely to reduce the false negative rate of CA125 by up to 19% and the
false positive rate by up to 42%.

Summary
Displays better diagnostic performance than CA125 alone, both for the detection of
early and late stage ovarian cancer. At a threshold of 0.45, OvPlex™ displays, 94%
sensitivity and 94% specificity
May improve the detection of ovarian cancer. At equivalent specificity with CA125,
OvPlex™ delivers 97% sensitivity
May reduce the false negative rate of CA125 by up to 19% and the false positive
rate by up to 42%
Traditional CA125 values are also provided for reference.

THANK YOU