Embed Size (px)
Citation preview

Overview of Adaptive Treatment Regimes
Sachiko MiyaharaDr. Abdus Wahed
Before starting the presentation…
≠Adaptive
Treatment Regimes
Adaptive Experimental
Design
Adaptive Treatment Regimes vs. Adaptive Experimental Design
• Adaptive Treatment Regimes“…adaptive as used here refers to a time- varying therapy for managing a chronic illness” (Murphy,2005)
• Adaptive Experimental Design“…such as designs in which treatment allocation probabilities for the present patients depend on the responses of past patients” (Murphy,2005)
Outline1. What is Adaptive Treatment Regime?
-Definition-Example-Objective
2. How to decide the best regime?- 3 different study designs- Comparison of 3 designs
3. Trial Example (STAR*D)
4. Inference on Adaptive Treatment Regimes
What is Adaptive Treatment Regime?
Definition:a set of rule which select the best
treatment option, which are made based on subjects’ condition up to
that point.
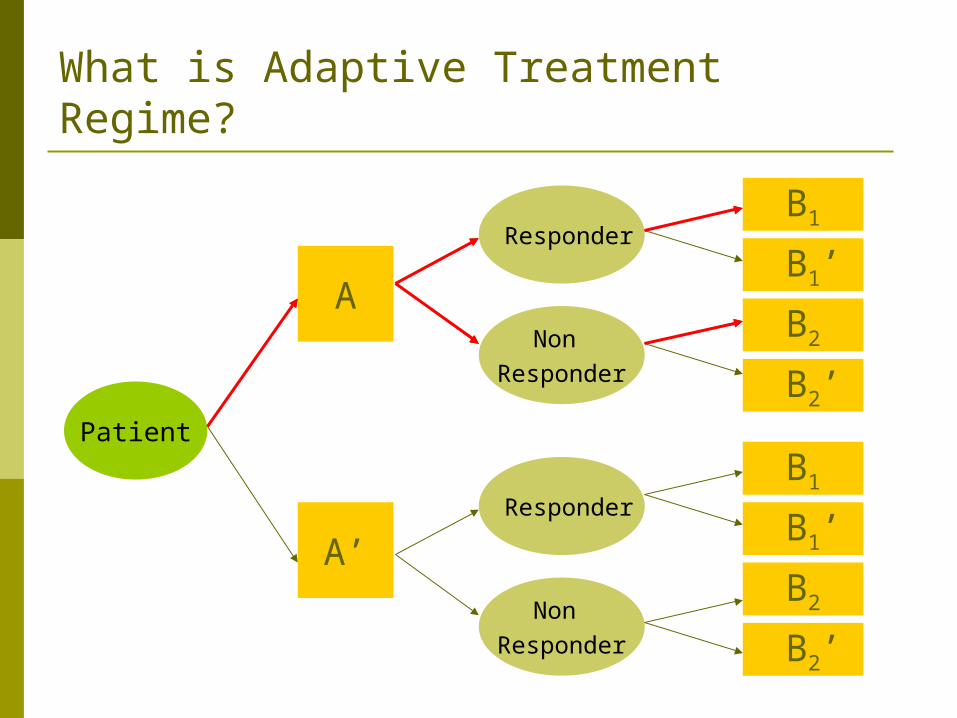
What is Adaptive Treatment Regime?
A
A’
B1
B1’
B2
B2’
B2’
B2
Non Responder
Responder
Responder
Non Responder
Patient
B1
B1’
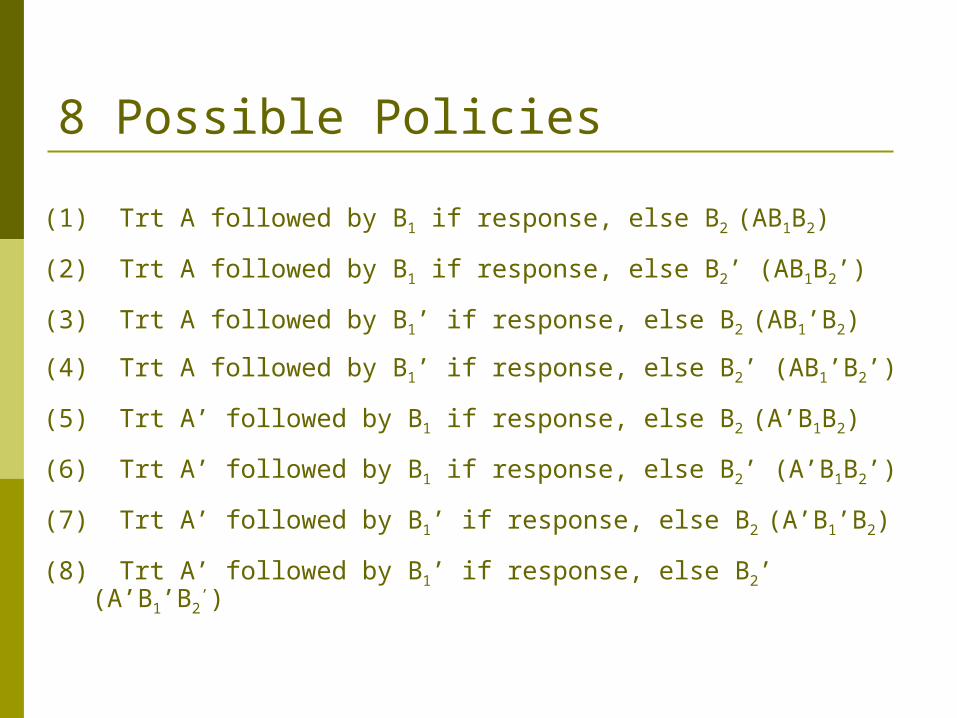
8 Possible Policies
(1) Trt A followed by B1 if response, else B2 (AB1B2)
(2) Trt A followed by B1 if response, else B2’ (AB1B2’)
(3) Trt A followed by B1’ if response, else B2 (AB1’B2)
(4) Trt A followed by B1’ if response, else B2’ (AB1’B2’)
(5) Trt A’ followed by B1 if response, else B2 (A’B1B2)
(6) Trt A’ followed by B1 if response, else B2’ (A’B1B2’)
(7) Trt A’ followed by B1’ if response, else B2 (A’B1’B2)
(8) Trt A’ followed by B1’ if response, else B2’ (A’B1’B2’)
What is the objective of the Adaptive Treatment Regimes?
• Objective:To know which treatment strategy works the best, given a patient’s history.
A treatment naïve patient comes to a physician’s office.
Questions:1. What treatment strategy should
the physician follow for that patient? 2. How should it be decided?
What is the objective of the Adaptive Treatment Regime?
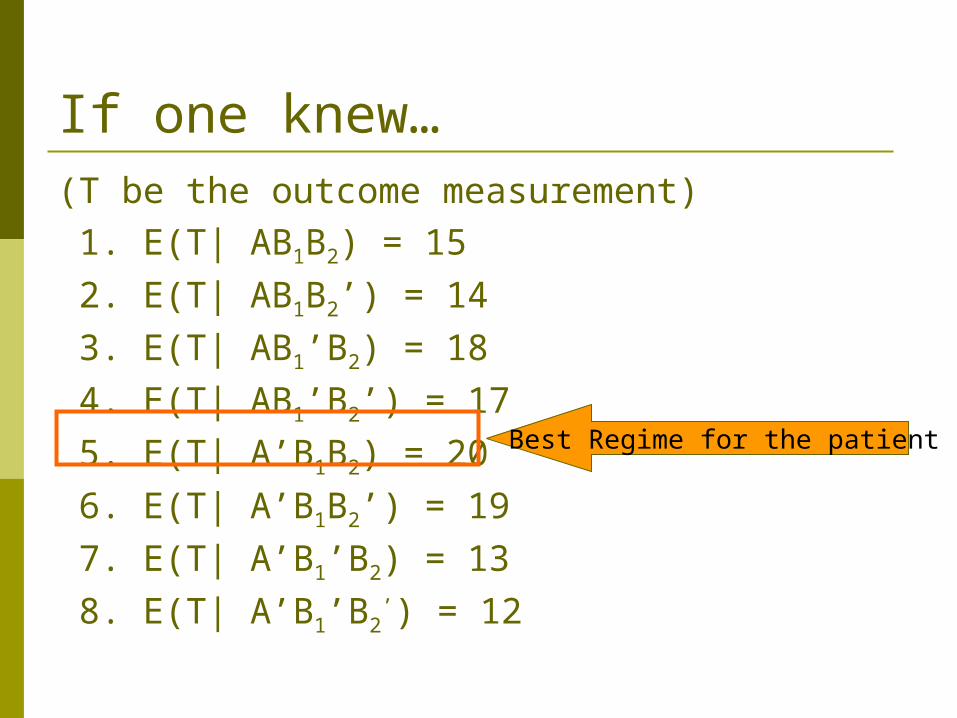
If one knew…(T be the outcome measurement) 1. E(T| AB1B2) = 15
2. E(T| AB1B2’) = 14
3. E(T| AB1’B2) = 18
4. E(T| AB1’B2’) = 17
5. E(T| A’B1B2) = 20
6. E(T| A’B1B2’) = 19
7. E(T| A’B1’B2) = 13
8. E(T| A’B1’B2’) = 12
Best Regime for the patient
In Reality…
Problems:
1. E(T| . ) are not known (need to estimate)2. How can one accurately and efficiently estimate E(T| . )?

How to estimate the expected outcome?
Three study designs:
1. A clinical trial with 8 treatments
2. Combine existing trials
3. SMART (Sequential Multiple Assignment Randomized Trials)
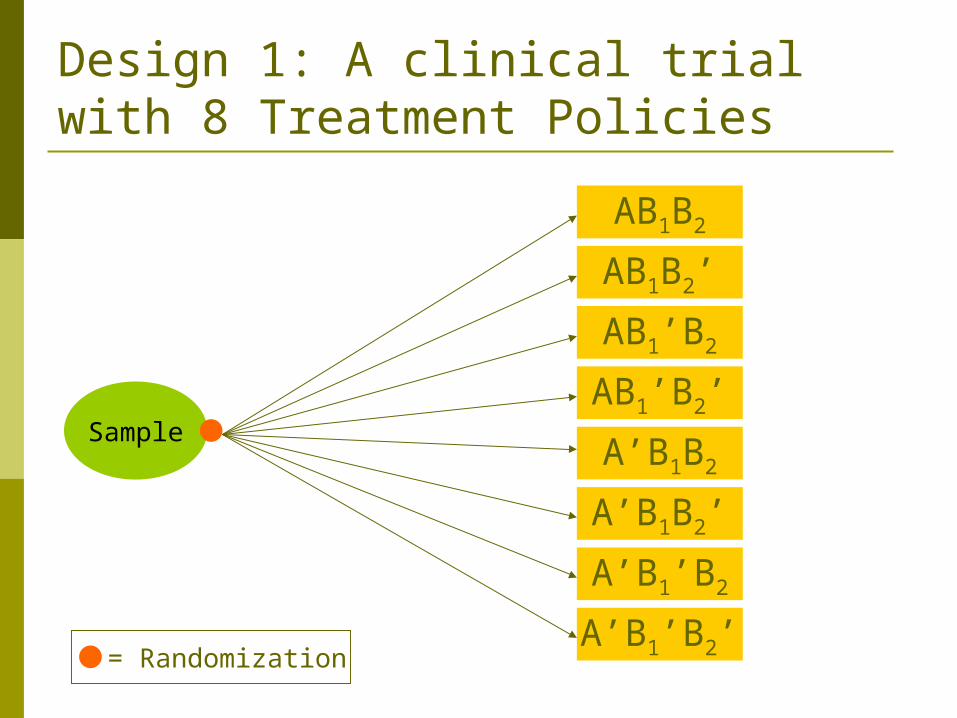
Design 1: A clinical trial with 8 Treatment Policies
AB1B2
AB1B2’
AB1’B2
AB1’B2’Sample
= Randomization
A’B1B2
A’B1B2’
A’B1’B2
A’B1’B2’
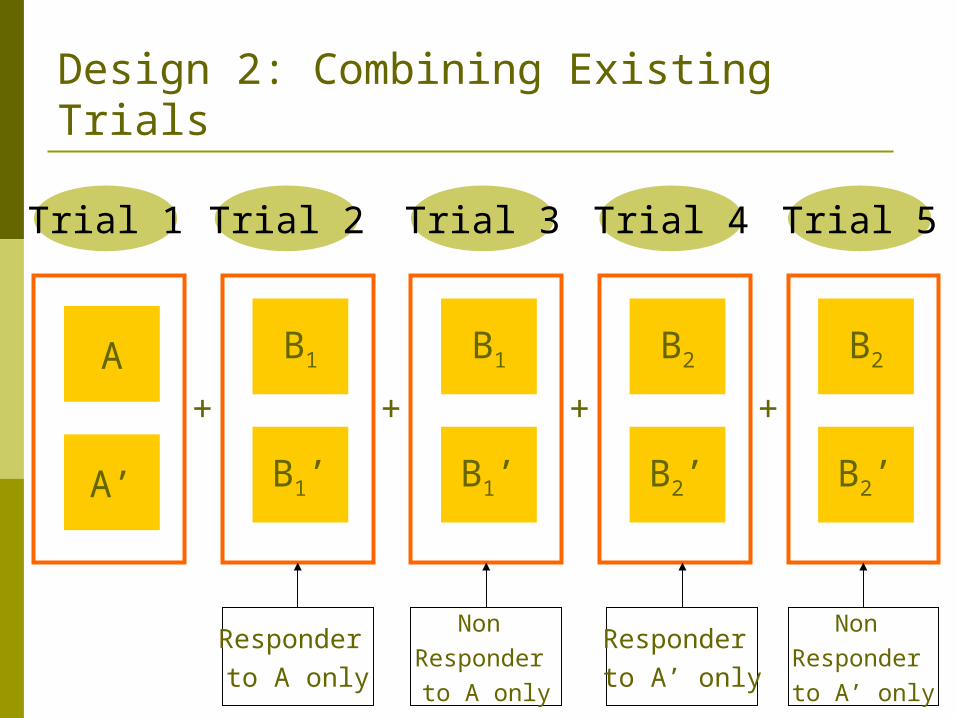
Design 2: Combining Existing Trials
A
A’
B1
B1’
+
Trial 1 Trial 5Trial 3Trial 2 Trial 4
+ + +
Responder to A only
Responder to A’ only
Non Responder to A only
Non Responder to A’ only
B1
B1’
B2
B2’
B2
B2’
Sequential Multiple Assignment Randomized Trials (SMART) proposed by Dr. Murphy
The SMART designs were adapted to:- Cancer (Thall 2000)- CATIE (Schneider 2001) – Alzheimer's Disease- STAR*D (Rush 2003) – Depression
Design 3: SMART
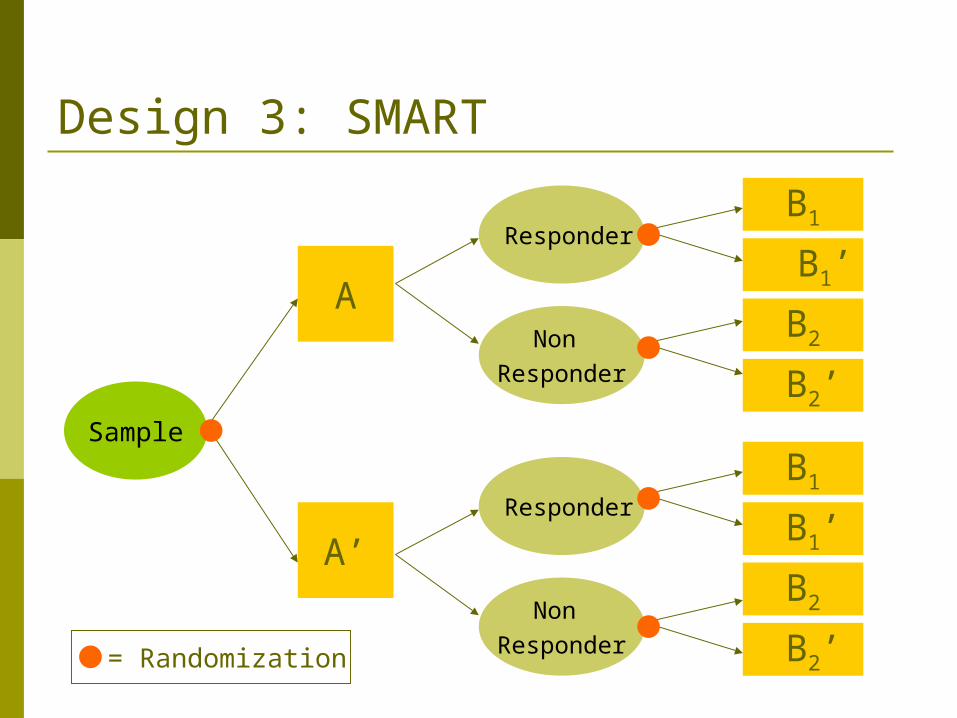
Design 3: SMART
A
A’
B1
B1’
B2
B2’
B2’
B2
B1’
B1
Non Responder
Responder
Responder
Non Responder
Sample
= Randomization
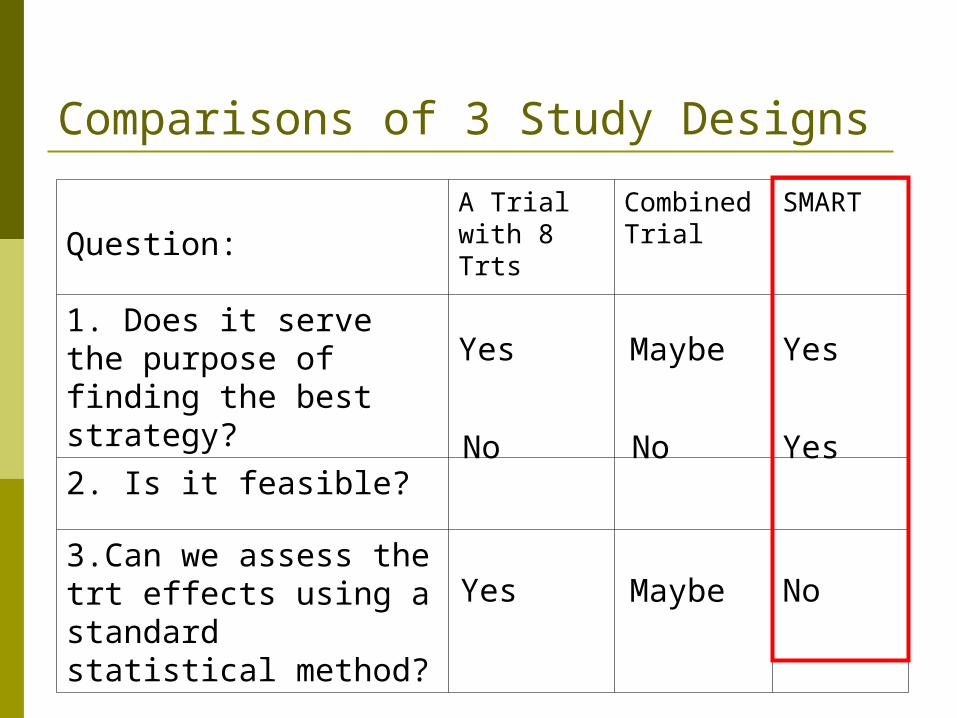
Comparisons of 3 Study Designs
Question:A Trial with 8 Trts
Combined Trial
SMART
1. Does it serve the purpose of finding the best strategy?
2. Is it feasible?
3.Can we assess the trt effects using a standard statistical method?
Yes Yes
Yes
Yes
Maybe
No
Maybe
No
No
Sequenced Treatment Alternatives To Relieve Depression (STAR*D)
1.What is STAR*D? 2.The Study Design
What is STAR*D?
• Multi-center clinical trial for depression
• Largest and longest study to evaluate depression
• N=4,041
• 7 years study period
• Age between 18-75
• Referred by their doctors
• 4 stages (3 randomizations)
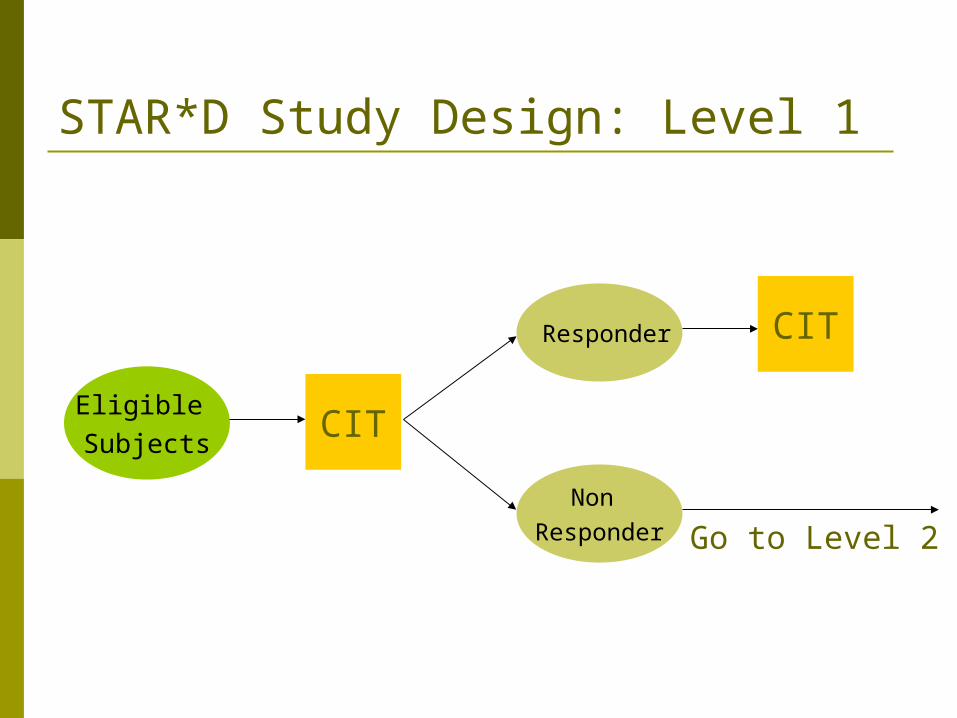
STAR*D Study Design: Level 1
Non Responder
Responder
Eligible Subjects
CIT
CIT
Go to Level 2
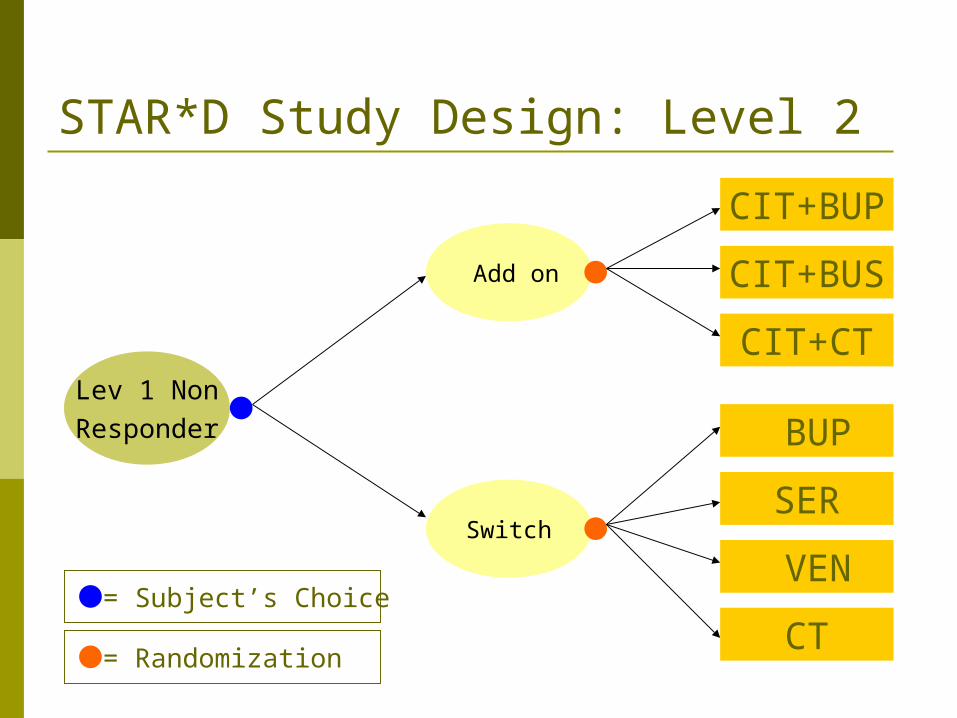
STAR*D Study Design: Level 2
CIT+CT
BUP
CT
VEN
SERSwitch
Add on
Lev 1 NonResponder
= Subject’s Choice
= Randomization
CIT+BUS
CIT+BUP
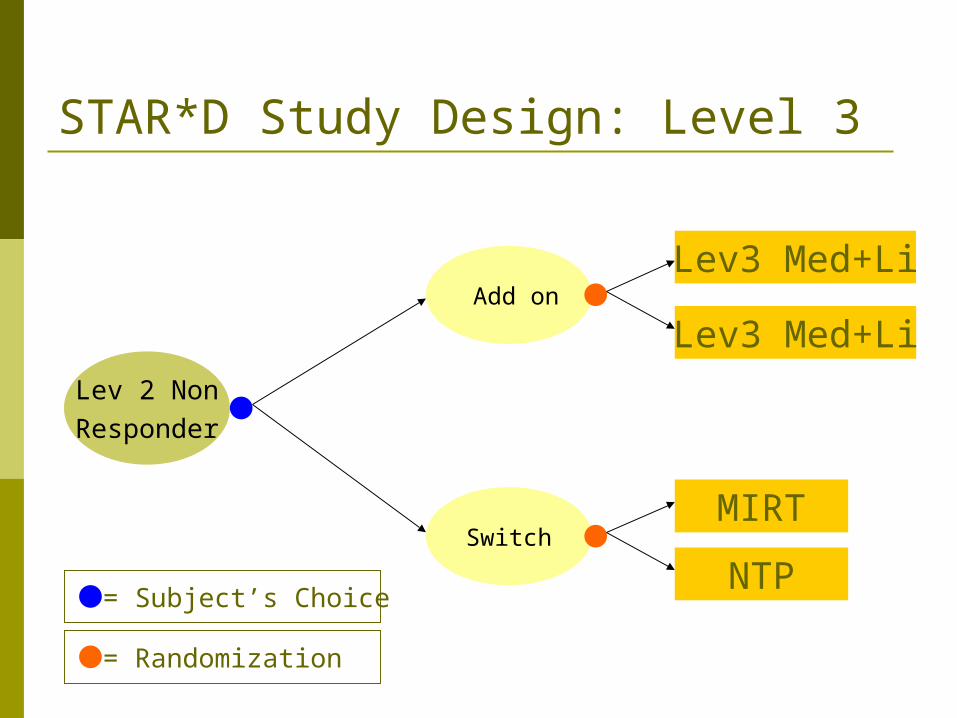
STAR*D Study Design: Level 3
Lev3 Med+Li
Lev3 Med+Li
NTP
MIRTSwitch
Add on
Lev 2 NonResponder
= Subject’s Choice
= Randomization
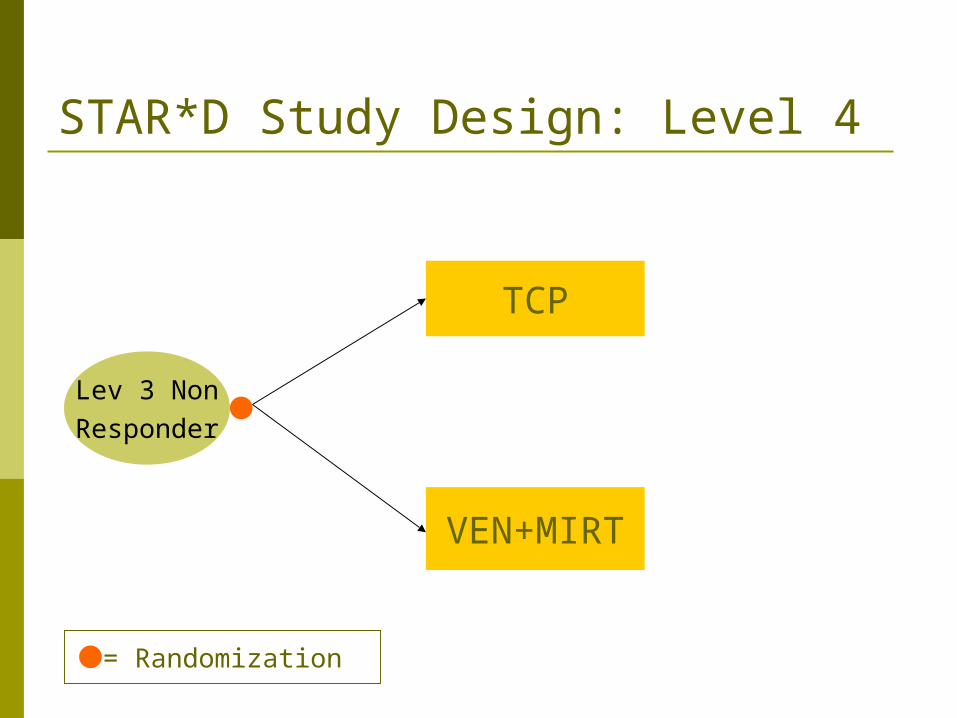
STAR*D Study Design: Level 4
VEN+MIRT
TCP
Lev 3 NonResponder
= Randomization
Details on Inference from SMART
• Remember the goal is to estimate E(T|AB1B2)
• First, how can we construct an unbiased estimator for
E(T|AB1B2)?
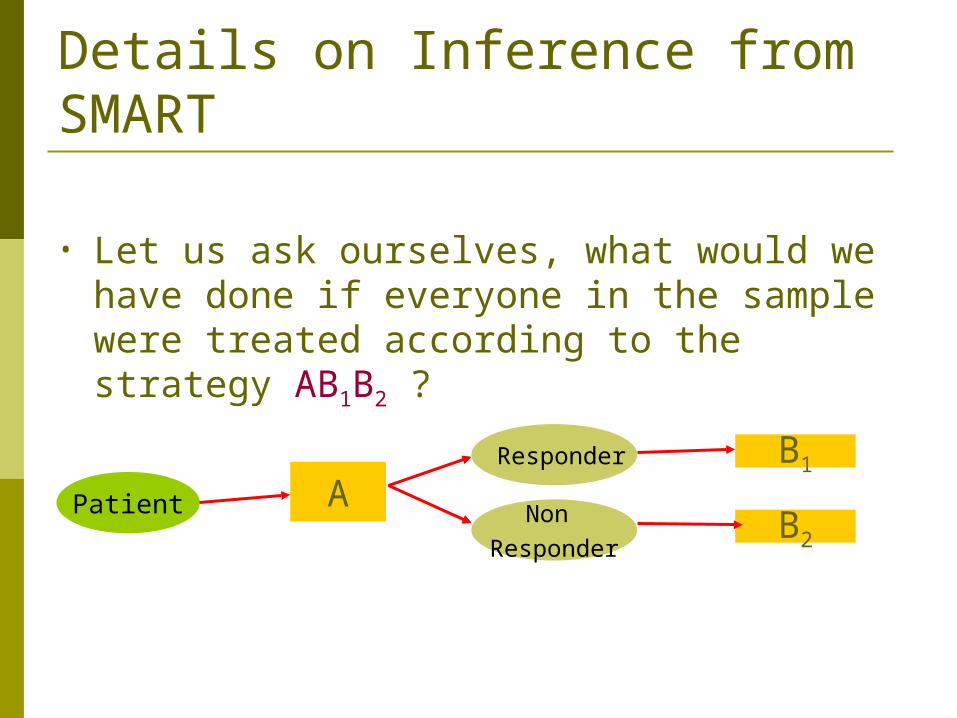
Details on Inference from SMART
• Let us ask ourselves, what would we have done if everyone in the sample were treated according to the strategy AB1B2 ?
AB1
B2Non
Responder
Responder
Patient
• What would we have done if everyone in the sample were treated according to the strategy AB1B2 ?
Answer: E(T|AB1B2) = ΣTi/n
Details on Inference from SMART
Applies to 8-arm randomization trial
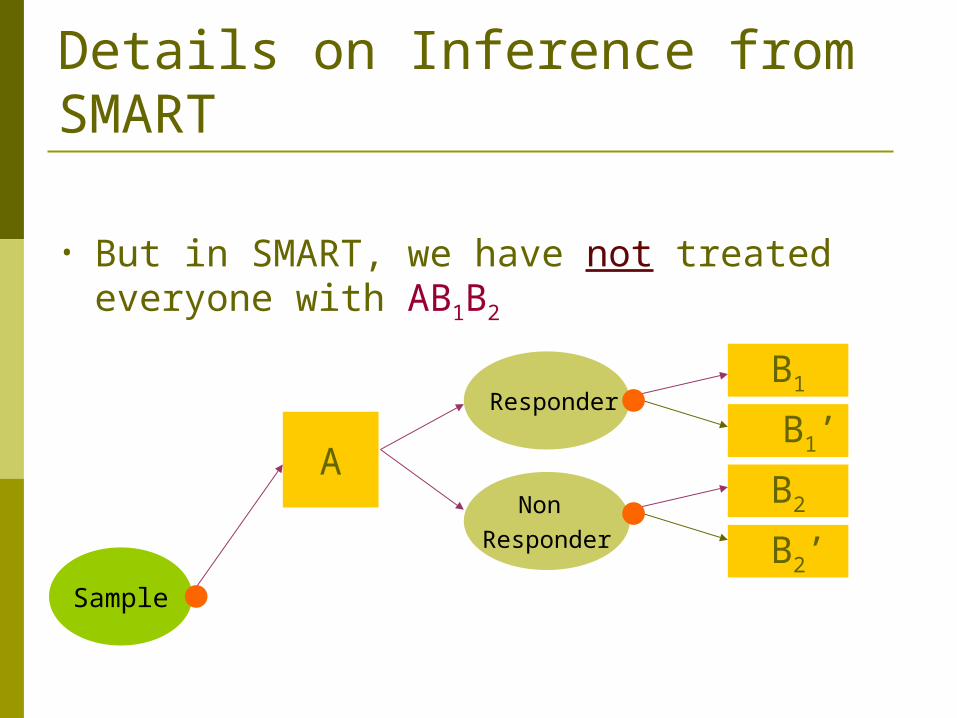
• But in SMART, we have not treated everyone with AB1B2
Details on Inference from SMART
A
B1
B1’
B2
B2’Non
Responder
Responder
Sample
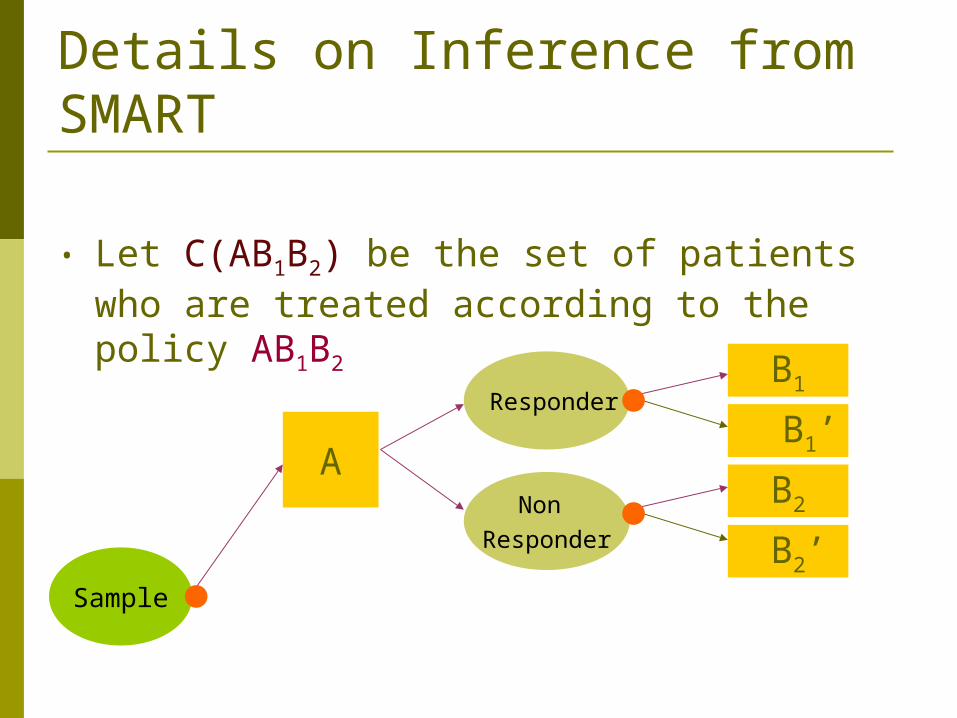
• Let C(AB1B2) be the set of patients who are treated according to the policy AB1B2
Details on Inference from SMART
A
B1
B1’
B2
B2’Non
Responder
Responder
Sample
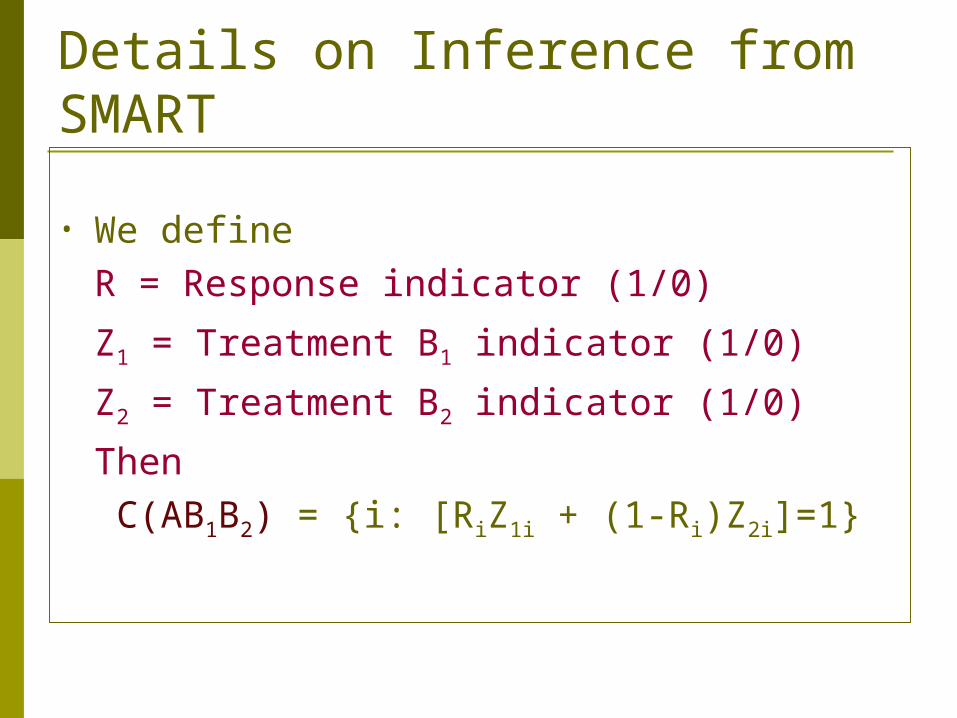
• We defineR = Response indicator (1/0)
Z1 = Treatment B1 indicator (1/0)
Z2 = Treatment B2 indicator (1/0)
Then C(AB1B2) = {i: [RiZ1i + (1-Ri)Z2i]=1}
Details on Inference from SMART
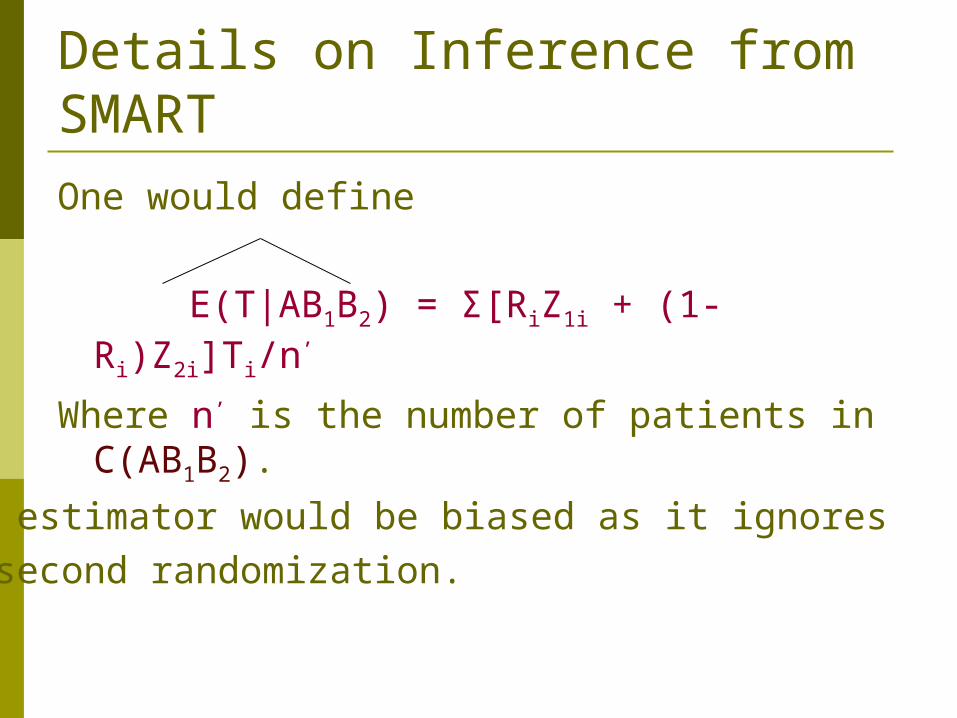
Details on Inference from SMARTOne would define
E(T|AB1B2) = Σ[RiZ1i + (1-Ri)Z2i]Ti/n’
Where n’ is the number of patients in C(AB1B2).
This estimator would be biased as it ignores the second randomization.
• There are two types of patients in the set C(AB1B2) who were treated according to the policy AB1B2
A responder who received B1
andA nonresponder who received B2
Details on Inference from SMART
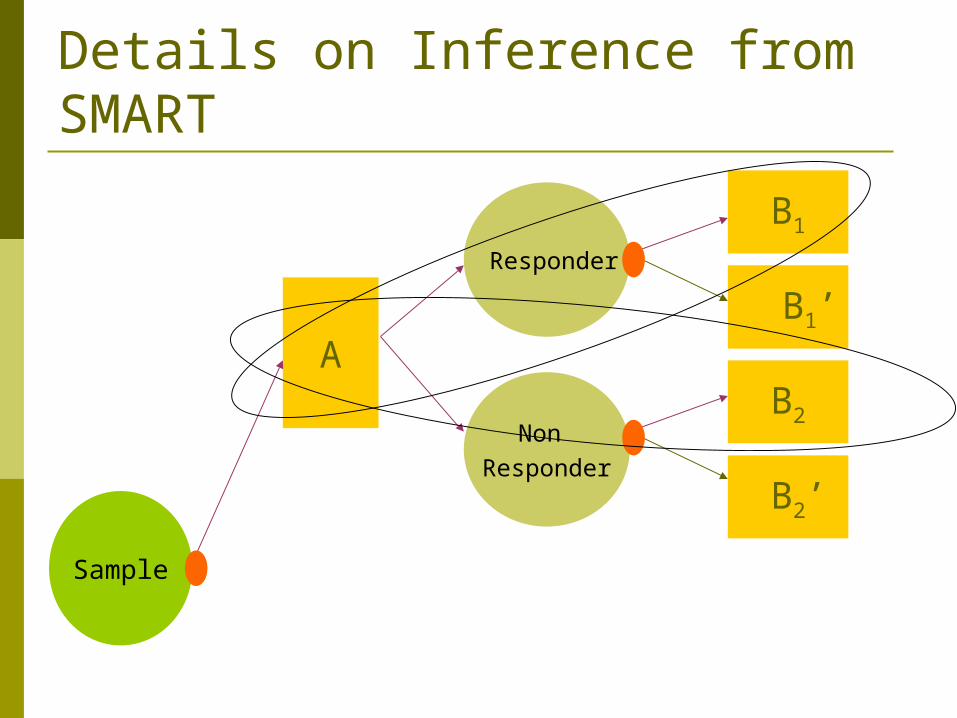
Details on Inference from SMART
A
B1
B1’
B2
B2’
Non Responder
Responder
Sample
• Assuming equal randomization,A responder who received B1 was equally eligible to receive B1
’
A responder who received B2 was equally eligible to receive B2
’
Details on Inference from SMART
• ThusA responder who received B1 in C(AB1B2) is representative of another patient who received B1
’
andA non-responder who received B2 in C(AB1B2) is representative of another patient who received B2
’
Details on Inference from SMART
• We define weights as follows A responder who received B1 in C(AB1B2) receives a weight of 2 [1/(1/2)], also
A non-responder who received B2 in C(AB1B2) receives a weight of 2 [1/(1/2)]
While everyone else receives a weight of zero.
Details on Inference from SMART
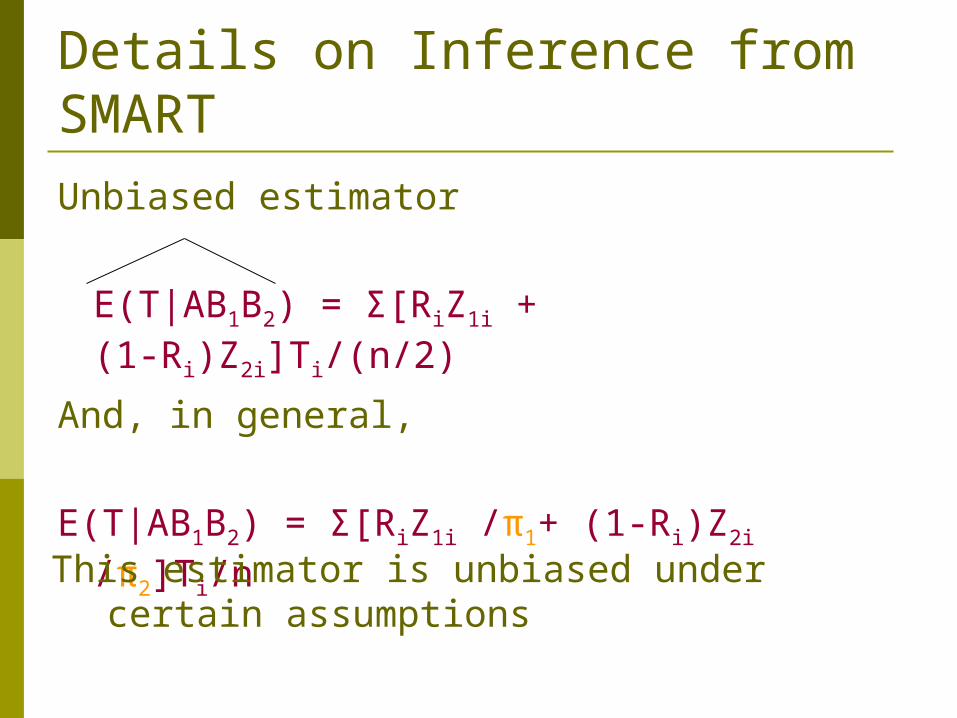
Details on Inference from SMARTUnbiased estimator
E(T|AB1B2) = Σ[RiZ1i + (1-Ri)Z2i]Ti/(n/2)
And, in general,
E(T|AB1B2) = Σ[RiZ1i /π1+ (1-Ri)Z2i /π2]Ti/n
This estimator is unbiased under certain assumptions
Issues
• Compare treatment strategies • Wald test possible but needs to derive
covariance between estimators (which may not be independent of each other)
• In survival analysis setting, how to derive formal tests to compare survival curves under different strategies
• Is log-rank test applicable?• Can the proportional hazard model be
applied here?
Issues
• Efficiency issues• How can one improve efficiency of the
proposed estimator• How to handle missing data (missing
response information, censoring, etc.)• How to adjust for covariates when
comparing treatment strategies• And most importantly,
Issues
• Is it possible to tailor the best treatment strategy decisions to individual characteristics?• For instance, could we one day hand
over an algorithm to a nurse (not physician) which would provide decisions like “If the patient is a caucacian female, age 50 or over, have normal HGB levels, bla bla bla…the best strategy for maintaining her chronic disease would be……..”
ATSRG link
http://www.pitt.edu/~wahed/ATSRG/main.htm





























