Embed Size (px)
Citation preview

REVIEW ARTICLE
Oxygen transport in blood at high altitude: role of the hemoglobin–oxygenaffinity and impact of the phenomena related to hemoglobinallosterism and red cell function
Accepted: 10 April 2003 / Published online: 18 September 2003� Springer-Verlag 2003
Abstract Altitude hypoxia is a major challenge to theblood O2 transport system, and adjustments of theblood–O2 affinity might contribute significantly to hy-poxia adaptation. In principle, lowering the blood–O2
affinity is advantageous because it lowers the circulatoryload required to assure adequate tissue oxygenation upto a threshold corresponding to about 5,000 m altitude,whereas at higher altitudes an increased blood–O2
affinity appears more advantageous. However, the ra-ther contradictory experimental evidence raises thequestion whether other factors superimpose on theapparent changes of the blood–O2 affinity. The mostimportant of these are as follows: (1) absolute temper-ature and temperature gradients within the body; (2) theintracapillary Bohr effect; (3) the red cell populationheterogeneity in terms of O2 affinity; (4) control ofaltitude alkalosis; (5) the possible role of hemoglobin asa carrier of the vasodilator nitric oxide; (6) the effect ofvaried red cell transit times through the capillaries.
Keywords Altitude hypoxia Æ Oxygen equilibriumcurve Æ Hemoglobin allosterism Æ Red cell function
Introduction
The blood–O2 equilibrium curve (OEC), i.e., the partialpressure of O2 (PO2) versus hemoglobin (Hb) O2 satu-
ration (SO2) plot, and the P50, i.e., the PO2 at whichSO2=50%, are useful indexes of the blood–O2 affinity.A variety of factors, the most important of which arepH, partial pressure of CO2 (PCO2), the red blood cell(RBC) concentration of 2,3-diphosphoglyceric acid(DPG), temperature and the amount of Hb bound tocarbon monoxide, influence OEC and hence the P50
(Severinghaus 1966; Siggaard-Andersen 1971; Thomas1972; Severinghaus 1979; Winslow et al. 1983; Rovidaet al. 1984; Siggaard-Andersen et al. 1984). Exposure toaltitude is well known to decrease the blood–O2 affinity(P50 rises by 2–5 mmHg, depending on altitude andexposure duration) by increasing the blood DPG con-tent (Lenfant et al. 1971), but Mg2+, ATP and Cl) alsoplay important roles (Mairbaurl et al. 1993).
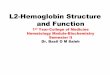
Under normal conditions, the sigmoidicity of theOEC facilitates the blood O2 transport as virtually allHb is loaded with O2 in the lungs at a relatively lowarterial PO2 (PaO2), while O2 is unloaded in the tissuesat a relatively high venous PO2 (PvO2). Thus, the re-quired amount of O2 is carried at a relatively low flow,thereby optimizing the cardiac output and the circula-tory load. In theory, changes in the blood–O2 affinityshould have important effects on the blood O2 transport.In the lungs, where PaO2 is set by the ventilation rate,the changes in P50 have little effect on arterial O2 satu-ration (SaO2) due to the flatness of the OEC in its upperportion. In contrast, PvO2 and venous O2 saturation(SvO2) are significantly affected (Fig. 1). In healthy hu-mans at sea level, the increased blood–O2 affinity wouldadversely influence the circulation, whereas the reverse isexpected in the case of decreased blood–O2 affinity.Table 1 reports an attempt to quantify the circulatory‘‘advantage’’ of increased P50 under normal conditionsat sea level.
The above considerations were made considering thewhole body as a lumped compartment, with the sub-script ‘‘v’’ denoting the mixed venous return. However,the same change in the blood–O2 affinity is expected tohave different effects in various organs, depending ontheir O2 requirement and the blood flow through them
Eur J Appl Physiol (2003) 90: 351–359DOI 10.1007/s00421-003-0954-8
Michele Samaja Æ Tiziano Crespi Æ Marco Guazzi
Kim D. Vandegriff
M. Samaja (&) Æ T. Crespi Æ M. GuazziDipartimento di Medicina,Chirurgia e Odontoiatria, Ospedale San Paolo,Universita’ Di Milano, via di Rudini’ 8,20142 Milan, ItalyE-mail: [email protected].: +39-028-9179250Fax: +39-028-9179251
K. D. VandegriffSangart, Inc., San Diego,California, USA

(Samaja 1988). In organs with high O2 requirement, suchas the heart and the working muscles, the high O2
extraction diminishes the dependence of that organ on
the changes in the blood–O2 affinity. In an extreme case,should an organ be able to extract all O2 from blood, thechanges in the blood–O2 affinity should have no effect atall on that organ. In contrast, in organs with low O2
extraction, such as the kidney, the changes in the blood–O2 affinity should have important effects. However, forthe sake of clarity, this manuscript concerns the wholebody as a single compartment.
Physiological effects of changes in the blood–O2 affinity
Theory
Exposure to altitude and arterial hypoxemia is a majorchallenge to the blood O2 transport system, and changesin blood–O2 affinity might contribute significantly tohypoxia adaptation. As yet there is no agreement on thequestion of whether a decreased or an increased blood–O2 affinity is preferable. Results from animals adaptedto live at altitude, the great majority of which haveblood P50 values lower than their sea level counterparts,suggest that an increased blood O2 affinity is advanta-geous (Monge and Leon-Velarde 1991). However, withthe exception of early reports, probably compromised bylack of knowledge of thermolabile DPG as an importantcofactor of the Hb–O2 affinity, all subsequent studies inhumans invariably report decreased blood–O2 affinitydue to increased DPG. Thus the question arises ofwhether this represents an adaptive or a maladaptivepattern. A theoretical study (Samaja et al. 1986) sug-gested that decreased blood–O2 affinity is preferable upto 5,500 m altitude, because decreased SvO2 tends to
Table 1 Advantage led by aP50 [i.e., the oxygen pressure (PO2) atwhich oxygen saturation (SO2)=50%] increase of 1 mmHg. Twoblood–O2 equilibrium curves (OEC) are calculated (Winslow et al.1983) varying the pH to simulate the unit change in the P50. In theiso-SO2 model [i.e. decreasing venous oxygen pressure (PvO2) atconstant venous oxygen saturation (SvO2)] (see Fig. 1), thePO2 iscalculated at the indicated arterial oxygen saturation (SaO2) andSvO2 values that were chosen arbitrarily, and the change in arterialto venous oxygen pressure (Da–vPO2) is then calculated. Loweringthe blood–O2 affinity by 1 mmHg P50 increases Da–vPO2 by3.2 mmHg, thereby representing an advantage for the perfusedtissue. In the (iso-PO2) model (i.e. increasingSvO2 at constantPvO2), SO2 is calculated at the indicatedPaO2 and PvO2 values that
were chosen arbitrarily, and the change in arterial to venous oxygensaturation (Da–vSO2) is then calculated. In this case, the unit changein the P50 increases Da-vSO2 by 1.4%. To estimate the physiologicaladvantage of this change, the Fick’s equation is used in the formQ= _VV O2/{[Hb](SaO2)SvO2)+a(PaO2)PvO2)}, where Q is the car-diac output (liters per minute), _VV O2 is the O2consumption(0.25 l min)1 at rest), [Hb] is the Hb concentration (160 g l)1), a isthe O2 solubility in plasma (1.4·10)6 mol l)1 at 37�C; Roughtonand Severinghaus 1973), and the other values are from the table.The cardiac output needed to sustain the assumed _VV O2 decreasesby 5.8% for unitP50 decrease. DPG 2,3-Diphosphoglyceric acid;Hbhemoglobin
OEC ‘‘left’’ OEC ‘‘right’’
High O2 affinity Low O2 affinity
Constant parameters pH 7.445 7.400PCO2, mmHg 40 40DPG Hb)1, mol mol)1 0.8 0.8P50, mmHg 27.8 28.8
Iso-SO2 model PO2 at SaO2=95%, mmHg (PaO2) 94.8 99.5PO2 at SvO2=70%, mmHg (PvO2) 39.2 40.7Da–vPO2, mmHg 55.6 58.8
Iso-PO2 model SO2 at PaO2=95 mmHg, %(SaO2) 95.0 94.5SO2 at PvO2=40 mmHg, %(SvO2) 71.0 69.1Da–vSO2, % 24.0 25.4Cardiac output, l min)1 6.51 6.15
Fig. 1 Increasing the blood–O2 affinity [i.e., shifting from thecontinuous curve on the right to the dashed curve on the left withdecreased P50, i.e., the oxygen pressure (PO2) at which oxygensaturation (SO2)=50%] has little effect on arterial oxygensaturation (SaO2) [not shown in the figure, arterial oxygen pressure(PaO2) is assumed constant because it is primarily controlled by theventilatory rate rather than by the blood–O2 affinity]. In the venouscompartment, the same increase in the blood–O2 affinity shouldhave one of the following effects: (1) decreasing venous oxygenpressure (PvO2) at constant venous oxygen saturation (SvO2) (iso-SO2 model); (2) increasing SvO2 at constant PvO2 (iso-PO2 model);(3) a combination of both. Thus, increasing the blood–O2 affinityadversely influences the circulation, because: (1) in the iso-SO2
model, tissues are forced to operate at a lower PO2; (2) in the iso-PO2 model, a higher cardiac output is required to compensate forthe decreased the change in arterial to venous oxygen saturation;(3) a combination of both. Table 1 reports a quantification of theseeffects
352

maximize the change in arterial to venous oxygen satu-ration (Da–vSO2), thereby lowering the circulatory load.In contrast, above this altitude, increased blood–O2
affinity is preferable because the preservation of SaO2
becomes a priority.
Experimental studies
Table 2 summarizes the essential results from some ofthe studies aimed at demonstrating the physiologicaladvantage of changes in the blood–O2 affinity in vivo orex vivo. Despite the majority of them being fundamen-tally in agreement with the theoretical predictions, con-siderable controversy remains. It is therefore legitimateto address the question whether such conflicting exper-imental evidence can be at least in part explained byovercoming the phenomena that tend to mask the effectof the measured changes in the blood–O2 affinity. Ouraim here is to assess some of these phenomena, namelythose that are linked to the blood–O2 affinity, but whichhave not yet been adequately measured or assessedunder hypoxic conditions.
Phenomena linked to Hb allosterism and RBC functionthat might mask the measured changes in theblood–O2 affinity
Temperature
Most often, the blood–O2 affinity is measured at thestandard 37�C temperature, but temperature has beenlong known to be an important allosteric factor of Hbfunction (Barcroft and King 1909). From the averageslope of the log10P50 versus temperature relationship(0.023 mmHg �C)1) (Samaja et al. 1983), P50 is expectedto decrease by 1.5 mmHg �C)1 temperature decrease.There are two aspects of this issue. First, central tem-perature should be taken into account when character-izing the blood–O2 affinity at altitude, but few studies, ifany, report this parameter. Temperature control at alti-tude is subject to many variables, but it is likely thathypothermia is more frequent at altitude than at sea leveland may therefore be one of the factors that mask themeasured changes in the blood–O2 affinity. Second, it islikely that considerable temperature gradients occur inthe body, especially at altitude with high blood hemat-ocrit and impaired circulation through some peripheralareas. Thus, the blood–O2 affinity characteristics may bequite different in the lungs and in some peripheral areasof the body. For example, for a ‘‘central’’ P50 value of28 mmHg at 37�C, the local P50 values in activelyworking muscles and upper joints may be 36.5 mmHgand 8.7 mmHg if temperature in these areas shifts to42�C and 15�C, respectively. Such changes are muchwider than those usually measured in humans at altitude,but we are not aware of studies reporting the existence ofsuch temperature gradients at altitude.
Hydrostatic pressure
Hydrostatic pressure decreases the P50 by 0.033 mmHgatm)1 without either altering the RBC DPG content oraffecting the Donnan equilibrium (Reeves and Morin1986). These changes, however, appear too modest tocompete with those attributed to altitude exposure.
Bohr effect
The equilibrium of the reaction HHb+O2��H-bO2+H+ shifts toward the formation of deoxygenatedHb on increasing acidity of the medium, the well knownBohr effect. Whereas arterial pH (pHa) normally fluc-tuates in a narrow range, the end-capillary pH is sub-jected to wide changes as a function of the metabolicstate and changing release of lactic acid. Thus, theblood–O2 affinity is expected to decrease progressivelyalong the capillary, thereby increasing the O2 delivery totissue in proportion to the tissue metabolic needs. Thismechanism may thus act as a signal originated from thetissue and targeted to the RBC to modulate O2 delivery(Wasserman et al. 1991). At sea level, the acidification ofmuscle capillary blood due to lactic acidosis was shownto facilitate the O2 transport during exercise (Stringeret al. 1994). We are not aware of similar studies per-formed at altitude, but class C heart failure patients mayrepresent a reliable model for hypoxia (Perego et al.1996). It was shown that, of the three mechanisms thatcan enhance the O2 delivery to working muscles, i.e.,increasing PaO2, increasing [Hb] and increasing P50 dueto the intracapillary Bohr effect, the last is a majorcontributor in class C patients (Agostoni et al. 1996).Thus, enhanced HbO2 dissociation, secondary to lactateproduction and acidification of capillary blood, helps tooxygenate the tissue above the anaerobic threshold. Ataltitude, however, this model is more complicated be-cause natives and lowlanders generate lower-than-ex-pected amounts of lactate on exercise, the so-called‘‘lactate paradox’’ (Grassi et al. 1996). In principle, thisshould diminish the relevance of the Bohr effect at alti-tude, but we are not aware of capillary blood pH mea-surements in hypobaric hypoxia, either direct orindirect, i.e., femoral vein pH, which is often used as anindex of end-capillary pH in working muscles duringexercise (Stringer et al. 1994). Thus the doubt remainswhether the expected decreased blood buffer power ataltitude, because of lower bicarbonate levels, may partlycompensate for the lower lactate output in maintainingthe physiological significance of lactic acid as a majorcontributory factor for O2 delivery to tissues.
Blood as a non-homogeneous population of RBCs
Lack of nuclei and mitochondria in the mature RBCrenders this cell unable to perform certain functions thatnormally occur in most aerobic cells, including protein
353

Table
2Summary
ofstudiesreportingthephysiologicaladvantageordisadvantageofchanges
intheblood–O
2affinity()
negative;
+positive;
=none).RBC
Red
bloodcell;Cr
creatine;
PCrphosphocreatine;
IHPinositolhexaphosphate;NaOCN
sodium
cyanate
Reference
P50change(m
mHg),methodused
Main
measurement
Main
conclusion,andeff
ectofincreasedHb–O
2affinity
Woodsonet
al.1973
36to
23,Exchangetransfusionwith
DPG-depletedblood
Work
perform
ance
inrats
Perform
ance
decreases,
)
Wranneet
al.1974
26to
24,AcidosisandDPG
depletion
Work
capacity
inman
Noeff
ect,=
Yhapet
al.1975
26to
20,DPG
depletion
_ VVO
2in
isolatedhindlimb
_ VVO
2decreasesdueto
lowered
O2extraction,)
Bakker
etal.1976
25to
18,DPG
depletion
_ VVO
2andbileflow
inratliver
atvaryingperfusionrates
Bileflow
rate
decreasesin
norm
oxia
andhypoxia._ VVO
2
decreasesin
hypoxia,butnotin
norm
oxia,)/=
Bakker
etal.1976,1977
25to
18,DPG
depletion
_ VVO
2andbileflow
inratliver
atvaryinghem
atocrits
Nochange,
butPVO
2islower
at2%
hem
atocrit,+
Tureket
al.1978a
33to
22,NaOCN
treatm
ent
PVO
2and
D a–vSO
2O
2transport
impaired
innorm
oxia,more
efficientin
hypoxia,+
Tureket
al.1978b
36to
22,NaOCN
treatm
ent
BloodO
2content,cardiacoutputand
flow
toorgansin
hypoxia
Noeff
ectin
hearts,highO
2affinitydisadvantageousfor
other
organsin
mildhypoxia,butadvantageous
inseverehypoxia,+
/=Martin
etal.1979
32to
14,Carbonmonoxide
_ VVO
2in
workingrathearts
Nochangedueto
increasedcoronary
flow
andcapillary
density,=
Malm
berget
al.1979
42to
21,StorageandNaOCN
Compensationto
hem
orrhagic
shock
inrats
Lim
ited
O2deliveryduringhypotension,)
Ross
andHlastala
1981
30to
14,StorageandNaOCN
O2extractionin
isolatedskeletalmuscle
_ VVO
2decreasesdueto
factors
unrelatedto
RBC–O
2
affinity,=
WoodsonandAuerbach
1982
38to
17,Exchangetransfusionwith
DPG-depletedblood
Cardiacoutputandflow
distributionin
sedatedrats
Nochangein
cardiacoutput,increasedcoronary
and
cerebralbloodflow,)
Lister1984
23to
31,Exchangetransfusion
_ VVO
2andO
2transport
inthehypoxic
lamb
Improved
cardiacfunction,)
Apsteinet
al.1985
33to
17,Storage
Cardiacfunctionin
isolatedrabbithearts
Decreasedperform
ance
and
_ VVO
2,)
Stucker
etal.1985
19to
47,IH
Ploading
_ VVO
2in
isolatedrathearts
Increased
_ VVO
2,)
Teisserie
etal.1985
31to
41,IH
Ploading
Bloodgasses
inexchange–tranfusedpiglets
IncreasedPaO
2and
D a–vSO
2,decreasedcardiacoutput,
)Koehleret
al.1986
26to
37,Exchangetransfusionwith
heterologouslow-O
2affinityblood
Cerebralbloodflow
response
tohypoxia
inlambsin
vivo
Reducedcerebralbloodflow
andO
2transport
tobrain,+
Rosenberget
al.1986
17to
32,Exchangetransfusionwith
heterologouslow-O
2affinityblood
Cerebralbloodflow
andbloodgasses
inlambsin
vivo
Noeff
ectontheabilityto
maintain
theO
2transport
duringhypoxia,=
Allanet
al.1986
16to
8,Treatm
entwithBW12C
Functionofisolatedrabbithearts
Decreasedfunction,PvO
2andincreasedlactate
output,
)Baronet
al.1987
21to
43,IH
Ploading
CardiacfunctionandO
2extraction
inperfusedrabbithearts
Increased
_ VVO
2,withincreasedvascularresistance
dueto
IHP,)
Woodsonet
al.1987
32to
22,Bloodmanipulation
Isolatedperfusedrathearts
DecreasedO
2extraction,increasedcoronary
bloodflow,)
Teisserie
etal.1987
26to
80,IH
Ploading
Long-term
effects
oncardiacoutputin
pigs
Increased
D a–vSO
2,)
GutierrezandAndry
1989
31to
21,NaOCN
O2extractionandPCr/Crratioin
hypoxic
hindlimbs
Noeff
ectontissueoxygenationdueto
peripheral
limitationto
O2diffusion,=
Samaja
etal.1991
30to
15,Storage
Cardiacfunctionin
isolatedrathearts
exposedto
low-flow
ischem
iaPerform
ance
insensitiveto
P50changes,=
Khandelwalet
al.1993
Allosteric
modificationofHb
TissueP
O2
IncreasedtissuePO
2,)
Liard
andKunert1993
31to
39,IH
Ploading
Hem
odynamicsin
dogs
DecreasedcardiacoutputandincreasedO
2delivery,)
Kunertet
al.1996
36to
52,allosteric
modification
ofHb
TissueP
O2andflow
inratcrem
aster
muscle
IncreasedO
2deliveryandresistance,=
Curtiset
al.1997
30to
42,allosteric
modification
ofHb
TissueP
O2andO
2extractionin
canineskeletalmuscle
Noeff
ectonO
2extraction,increasedtissueP
O2,=
Weiss
etal.1999
Allosteric
modificationofHb
Myocardialhigh-energyphosphatesduring
low-flow
ischem
iain
dogs
Ameliorationofmetabolicandfunctionalconsequences
ofischem
ia,)
Berlinet
al.2002
17to
33,IH
Ploading
Cardiacfunctionin
heartsduringlow-flow
ischem
iaDecreasedfunction,)
354

synthesis and energy generation from processes requir-ing O2. The inability to repair damage leads to unbal-anced metabolism, altered ion homeostasis and a limited120-day life span. In humans, the RBC removal from thecirculation by the reticuloendothelial system is selectivefor the aging RBC (Clark 1988) and is characterized byreduced deformability (Linderkamp and Meiselman1982) and DPG content (Seaman et al. 1980). Inactiva-tion of membrane Na+–K+-ATPase leads to shrinkingand >20% increase in RBC [Hb]. The combined effectof increased [Hb] and decreased [DPG] reduces the[DPG]/[Hb] ratio from 1.0 mol mol)1 in the ‘‘young’’RBC to 0.5 mol mol)1 in the ‘‘old’’ RBC, which corre-sponds to a decrease in P50 from 29 mmHg to 23 mmHg(Samaja and Rovida 1987). The various types of RBCcoexist in blood, and despite differences in rheologicalproperties (Linderkamp and Meiselman 1982), there isno evidence that capillaries select the RBC passagebased on their age. Therefore, capillaries are perfusedsequentially with RBCs that vary widely in their O2
affinity properties. One may wonder whether the chan-ges in whole blood P50 by 2–5 mmHg, as those observedin humans at altitude, still retain biological significancewhen wider changes are already routinely present at themicrocirculatory level.
The majority of the techniques used for determiningthe blood–O2 affinity make use of blood or RBC sampleswith volumes in the microliter-to-milliliter range.Therefore, the measured values represent the average ofthe various RBC types in that sample. It is likely that theinter-individual P50 or OEC variability stems from al-tered distribution in ‘‘young’’ and ‘‘old’’ RBCs ratherthan from intrinsic changes in the Hb–O2 affinity. TheRBC distribution is profoundly altered in several blooddisorders (Nakashima et al. 1973). At altitude, the wholeRBC population undergoes rejuvenation, because in-creased erythropoiesis inputs more ‘‘young’’ RBCs intothe blood (Samaja et al. 1993), but we are not aware ofstudies reporting modifications of the RBC life span ataltitude, making it difficult to assess whether the RBCheterogeneity increases or decreases at altitude.
High-altitude alkalosis
At altitude, hypoxic stimulation of chemoreceptors in-creases alveolar ventilation, thereby increasing CO2
washout, reducing PaCO2 and increasing pHa. Althoughat sea level pHa is allowed to fluctuate within a rathernarrow 7.37–7.43 range, at altitude the mechanisms thattitrate pHa to the normal value are less efficient.Therefore, the blood remains alkaline, perhaps becauseof the slow renal compensation that cannot cope withcontinuous CO2 washout from the lungs. After 7–10 days at 6,450 m, pHa remains at 7.496 (0.006) andbase excess (BE) is )6 mEq l)1, whereas a BE of )10 to)9 mEq l)1 is necessary for complete compensation(Winslow et al. 1984; Samaja et al. 1997). Alkalosis in-creases the blood–O2 affinity, an effect contrasted by
increased DPG. As a result, in Caucasians at 6,300 m,and despite an increased [DPG]/[Hb] ratio from 0.80 to1.36 (Samaja et al. 1997), P50 increased from 28 mmHgto only 30 mmHg. At this altitude, this might be con-sidered as a protective mechanism. At 6,450 m, hyper-ventilatory alkalosis increases SaO2 to an extent thatcorresponds to a descent by 1,300 m (Samaja et al.1997), and at 8,848 m, the extreme alkalosis in a personon the summit of Mount Everest should have allowedthis subject to maintain essentially the same SaO2 as thatmeasured at 6,300 m (Winslow et al. 1984). Therefore, atextreme altitudes alkalosis helps maintaining Da–vSO2
despite low PaO2.Prolonged alkalosis, however, is not compatible with
normal body function and one of the effects of accli-matization is to reduce alkalosis, with subjects withacute mountain sickness (AMS) being more alkaloticthan non-AMS subjects (Samaja et al. 1997). As amatter of fact, acetazolamide, a drug used to fight AMS,tends to lower pHa by inhibiting carbonic anhydrase(Bradwell et al. 1987). Comparative analysis of the pH–arterial pressure of CO2 (PaCO2) relationships in othergroups of subjects helps to address this issue. In Sherpas,PaCO2 is higher, and their pHa is lower than in Cauca-sians (Samaja et al. 1997). As BE is comparable, it ispossible that less hypoxic ventilatory drive in Sherpas(Lahiri et al. 1969) prevents excessive PaCO2 fall and riseof alkalosis. Probably, low DPG in Sherpas’ bloodcontributes to a larger extent to keep high SaO2 thanhyperventilation does in Caucasians.
Nitric oxide
Nitric oxide (NO) is an endothelium-derived relaxingfactor with a number of effects in somatic cells as astimulator of soluble guanylate cyclase. The local con-centration of NO produced by endothelial cells(�400 nM) is in excess of that required to activate sol-uble guanylate cyclase (20 nM), but the reaction of NOwith HbO2 is so fast (k=107 M)1 s)1) that virtually allNO should be inactivated by HbO2 (Hobbs et al. 2002).Yet, it is unquestionable that NO mediates a largenumber of effects in the circulation. The apparent par-adox that endothelial cells release NO in a medium, theblood, which is particularly rich in HbO2, a NO inacti-vator, led to the conjecture that NO has a role in thehuman respiratory cycle (McMahon et al. 2002).
The hypothesis that Hb is a transporter of NO arosefrom the observation that NO does not only bind to theheme to form nitrosyl-Hb (HbNO), but also to the thiolgroup at the highly conserved b-cysteine 93 (b-Cys93)residue to form the S-nitrosothiol derivative (HbSNO)(Jia et al. 1996). Total bound NO is essentially constantin oxygenated and deoxygenated blood, but when bloodis in the oxygenated state, HbSNO is predominant,whereas HbNO is higher in the deoxygenated state(McMahon et al. 2000). Thus, Hb binds both O2 andNO in the lungs at two different sites, and in the low PO2
355

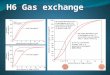
environment in the capillaries, some NO bound tob-Cys93 is made free (McMahon et al. 2000) (Fig. 2).The presence of thiol acceptors, one of which is theanion-exchanger-1 ( or band-3 protein) in the RBCmembrane (Pawloski et al. 2001), may mediate NOexport out of the RBC, thereby promoting localvasorelaxation and improving O2 delivery upon Hbdeoxygenation (McMahon et al. 2002). Althoughfavored by low tissue PO2, it is difficult to assess whetherthe Hb-mediated trans-nitrosylation may overcome theblood–O2 affinity changes at altitude. But the depen-dence of this phenomenon on the allosteric state of Hbsuggests that the NO-donor activity of HbSNO mayenhance the O2 delivery properties of blood in a fashiondependent on local hypoxia (Pawloski et al. 2001).
Although suggestive, this hypothesis requires confir-mation. First, a recent study was unable to confirm theallosteric effect underlying NO release by HbSNO, andshowed dominance of the Hb scavenging over the NO-donor properties due to the high NO–heme affinity thatprecludes reaction of NO with b-cys93 (Deem et al.2001). Second, the low P50 of purified HbSNO(<10 mmHg) should require very severe hypoxia toaccomplish NO release (McMahon et al. 2000). Third,the decrease in P50 upon in vitro incubation with NOand NO donors correlates with methemoglobin forma-tion, suggesting that this species, and not HbSNO, is thefinal product of the NO reaction with Hb (Hrinczenkoet al. 2000). Finally, it is likely that the Hb function as aNO transporter is linked to the effects of hypoxia on NOproduction, but it is not yet clear whether NO produc-tion increases or decreases at altitude. Whereas somedata show that hypoxia increases NO production
(Nathan 1992; Agvald et al. 2002), others suggest thatthe reverse is true (Nelin et al. 1996; Fike et al. 1998;Guzel et al. 2000). Also, although NO production rate iselevated during exercise, exhaled NO is not related todecreased SaO2 during heavy exercise (Sheel et al. 2000).
RBC transit time
The RBC might not have enough time in the capillary torelease all O2. To evaluate this possibility, the Fick dif-fusion equation has been used in a simple boundaryanalysis to estimate the external resistance to O2 diffu-sion for RBCs (Vandegriff and Olson 1984a, b,c). TheO2 flux at the RBC interface can be calculated using asimple diffusion equation for PO2 values across a dif-fusion barrier (P1–P2):
d O2½ �=dt � D P1 � P2ð Þ=Dr ð1Þ
where D is the O2 diffusion constant between phases P1
and P2, and Dr is the diffusion distance between P1 andP2.
Using this analysis, we can evaluate the effects on O2
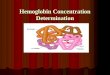
transport in the capillaries of the lung, assuming con-stant Dr. The rate of O2 uptake by the RBCs at sea levelis determined by the PO2 in alveolar gas spaces (i.e.,alveolar PO2�100 mmHg = P1 in Eq. 1), which makesthe O2 concentration gradient very steep. The time toreach equilibrium between the gas space and PaO2 isvery fast (Fig. 3), and the O2 binding affinity of RBCshemoglobin (i.e., P2 in Eq. 1) is not a critical parameter.This does not hold true at high altitude, where alveolarO2 is much lower. As alveolar PO2 decreases, the dif-fusion gradient becomes narrower as a function of thepulmonary O2 concentration (i.e., decreasing P1 inEq. 1) (Fig. 3). In addition, if the RBC has a high P50
(P2 in Eq. 1), the gradient will be narrowed even further(flP1)›P2). Thus, the hemoglobin O2 binding charac-teristics will be a critical factor at high altitude (Van-degriff and Winslow 1995).
Conclusion
At altitude, the modulation of the O2 delivery to tissuesby fine tuning of the blood–O2 affinity is of greatimportance, because relatively small changes in the
Fig. 2 Putative molecular mechanism by which nitric oxide (NO) iscarried by oxyhemoglobin and exported out of the red blood cell(RBC) upon hemoglobin (Hb) deoxygenation. In the lung, Hbbinds O2 at the heme and NO at the b-Cys93 residue, which lies in apocket of the Hb b chain (left panel). Thus, in the oxygenated state,the NO groups are hidden from the environment. In thecorrespondence of the oxy-to-deoxy transition, the a-threonine41residue interacts with b-Cys93, thereby exposing the NO groups(right panel). Some NO groups are autocaptured by the heme, butothers are transferred to thiol acceptors such as the anionexchanger on the surface of the RBC membrane that pumps NOout of the RBC. As a result, the low PO2 in peripheral tissues forcesthe allosteric changes that destabilize the b-Cys93–NO bond. TheNO released upon deoxygenation promotes vasodilatation andenhances the O2 delivery
356

blood–O2 affinity are capable to maximize Da–vSO2 andoptimize the O2 transport to tissue keeping the circula-tory load to a minimum. However, other factors inde-pendent of the measured P50, and linked to Hballosterism and RBC function, may have effects thatpotentially mask those related to the changes in blood–O2 affinity.
Acknowledgement We gratefully acknowledge the helpful advice byProfessor Robert M. Winslow, Sangart, Inc., for the discussion ofthe RBC transit time.
References
Agostoni PG, Wasserman K, Perego GB, Marenzi GC, Guazzi M,Assanelli E, Lauri G, Guazzi MD (1996) Oxygen transport tomuscle during exercise in chonic congestive heart failure sec-ondary to idiopathic dilated cardiomyopathy. Am J Cardiol79:1120–1124
Agvald P, Adding LC, Artlich A, Persson MG, Gustafsson LE(2002) Mechanism of nitric oxide generation from nitroglycerinand endogenous sources during hypoxia in vivo. Br J Phar-macol 135:373–382
Allan G, Chapple DJ, Hughes B (1986) Effects of an increase inhemoglobin O2 affinity produced by BW12C on myocardialfunction in the erythrocyte-perfused rabbit heart in vitroand myocardial infarct size in the dog. Br J Pharmacol89:183–190
Apstein CS, Dennis RC, Briggs LL, Vogel WM, Frazer J, ValeriCR (1985) Effect of erythrocyte storage and oxyhemoglobinaffinity changes on cardiac function. Am J Physiol 248:H508–H515
Bakker JC, Gortmaker GC, Offerjins FGJ (1976) The influence ofthe position of the oxygen dissociation on oxygen-dependentfunctions of the isolated perfused rat liver. Pflugers Arch366:45–52
Bakker JC, Gortmaker GC, Devries Van Rossen A, Offerijns FGJ(1977) The influence of the position of the oxygen dissociationon oxygen-dependent functions of the isolated perfused rat li-ver. Pflugers Arch 368:63–70
Barcroft J, King WOR (1909) The effect of temperature on thedissociation curve of blood . J Physiol (Lond) 39:374–384
Baron JF, Vicaut E, Stucker O, Villereal MC, Ropars C, TeisserieB, Duvelleroy M (1987) Isolated heart as a model to study theeffects of the in oxygen hemoglobin affinity. Adv Biosci 67:73–78
Berlin G, Challoner KE, Woodson RD (2002) Low-O2 affinityerythrocytes improve performance of ischemic myocardium.J Appl Physiol 92:1267–1276
Bradwell AR, Dykes PW, Coote JH (1987) Effect of acetazolamideon exercise at altitude. Sports Med 4:157–163
Clark MR (1988) Senescence of red blood cells: progress andproblems. Physiol Rev 68:503–554
Curtis SE, Walker TA, Bradley WE, Cain SM (1997) Raising P50increases tissue PO2 in canine skeletal muscle but does not affectcritical O2 extraction ratio. J Appl Physiol 83:1681–1689
Deem S, Gladwin MT, Berg JT, Kerr ME, Swenson ER (2001)Effects of S-nitrosation of hemoglobin on hypoxic pulmonaryvasoconstriction and nitric oxide flux. Am J Resp Crit CareMed 163:1164–1170
Fike CD, Kaplowitw MR, Thomas CJ, Nelin LD (1998) Chronichypoxia decreases nitric oxide production and endothelial nitricoxide synthase in newborn pig lungs. Am J Physiol 274:L517–L526
Grassi B, Marzorati M, Kayser B, Bordini M, Colombini A, ContiM, Marconi C, Cerretelli P (1996) Peak blood lactate and bloodlactate vs workload during acclimatization to 5,050 m and indeacclimatization. J Appl Physiol 80:685–692
Gutierrez G, Andry JM (1989) Increased hemoglobin oxygenaffinity does not improve oxygen consumption in hypoxemia.J Appl Physiol 66:837–843
Guzel NA, Sayan H, Erbas D (2000) Effects of moderate altitudeon exhaled nitric oxide, erythrocytes lipid peroxidation andsuperoxide dismutase levels. Jpn J Physiol 50:187–190
Hobbs AJ, Gladwin MT, Patel RP, Williams DLH, Butler AR(2002) Hemoglobin: NO transporter, NO inactivator, or NOneof the above? Trends Pharmacol Sci 23:406–411
Hrinczenko BW, Alayash AI, Wink DA, Gladwin MT, RodgersGP, Schechter AN (2000) Effect of nitric oxide and nitric oxidedonors on red blood cell oxygen transport. Br J Haematol110:412–419
Jia L, Bonaventura C, Bonaventura J, Stamler JS (1996) S-nitro-sohemoglobin: a dynamic activity of blood involved in vascularcontrol. Nature 380:221–226
Khandelwal SR, Randad RS, Lin PS, Meng H, Pittman RN,Kontos HA, Choi SC, Abraham DJ, Schmidt-Ullrich R (1993)Enhanced oxygenation in vivo by allosteric inhibitors ofhemoglobin saturation. Am J Physiol 265:H1450–H1453
Koehler RC, Traystman RJ, Jones JR (1986) Influence of reducedoxyhemoglobin affinity on response to hypoxic hypoxia. Am JPhysiol 251:H756–H763
Kunert MP, Liard JF, Abraham DJ, Lombard JH (1996) Low-affinity hemoglobin increases tissue PO2 and decreases arteri-olar diameter and flow in the rat cremaster muscle. MicrovascRes 52:58–68
Lahiri S, Edelman NH, Cherniack NS, Fishman AP (1969) Bluntedhypoxic drive to ventilation in subjects with life-long hypox-emia. Fed Proc 28:1289–1295
Lenfant C, Torrance JD, Reynafarje C (1971) Shift of the O2–Hbdissociation curve at altitude: mechanism and effect. J ApplPhysiol 30:625–631
Liard JF, Kunert MP (1993) Hemodynamic changes induced bylow blood oxygen affinity in dogs. Am J Physiol 264:R396–R401
Linderkamp O, Meiselman HJ (1982) Geometric-osmotic andmembrane mechanical properties of density-separated humanred cells. Blood 59:1121–1127
Lister G (1984) Oxygen transport in the intact hypoxic newbornlamb: acute effects of increasing P50. Pediatr Res 18:172–177
Mairbaurl H, Oelz O, Bartsch P (1993) Intercations between Hb,Mg, DPG, ATP and Cl determine the change in Hb–O2 affinityat high altitude. J Appl Physiol 74:40–48
Fig. 3 Diffusion limitation of O2 uptake by RBCs. Calculations arefor a 70-kg person with 5 ml kg min)1 O2 uptake and normalpulmonary function. The three curves correspond to three levels ofalveolar O2 tension: 100, 75, and 50 mmHg. The figure is redrawnfrom (Vandegriff and Winslow 1995) with the help of ProfessorRobert M. Winslow
357

Malmberg PO, Hlastala MP, Woodson RD (1979) Effect of in-creased blood-oxygen affinity on oxygen transport in hemor-rhagic shock. J Appl Physiol 47:889–895
Martin JL, Duvelleroy M, Teisserie B, Duruble M (1979) Effect ofan increase in HbO2 affinity on the calculated capillaryrecruitment of an isolated rat heart. Pflugers Arch 382:57–61
McMahon T, Moon RE, Luschinger BP, Carraway MS, Stone AE,Stolp BW, Gow AJ, Pawloski JR, Watke P, Singel DJ, Pian-tadosi CA, Stamler JS (2002) Nitric oxide in the human respi-ratory cycle. Nat Med 8:711–717
McMahon TJ, Stone AE, Bonaventura J, Singel DJ, Stamler JS(2000) Functional coupling of oxygen binding and vasoactivityin S-nitrosohemoglobin. J Biol Chem 275:16738–16745
Monge CC, Leon-Velarde F (1991) Physiological adaptation tohigh altitude: oxygen transport in mammals and birds. PhysiolRev 71:1135–1172
Nakashima K, Susuma O, Miwa S (1973) Red cell density in var-ious blood disorders. J Lab Clin Med 82:297–302
Nathan C (1992) Nitric oxide as a secretory product of mammaliancells. FASEB J 6:3051–3064
Nelin LD, Thomas CJ, Dawson CA (1996) Effect of hypoxia onnitric oxide production in neonatal pig lung. Am J Physiol271:H8–H14
Pawloski JR, Hess DT, Stamler JS (2001) Export by red cells ofnitric oxide bioactivity. Nature 409:622–626
Perego GB, Marenzi GC, Guazzi M, Sganzerla P, Assanelli E,Palermo P, Conconi B, Lauri G, Agostoni PG (1996) Contri-bution of PO2, P50, and Hb to changes in arteriovenous oxygencontent during exercise in heart failure. J Appl Physiol 80:623–631
Reeves RB, Morin RA (1986) Pressure increases oxygen affinity ofwhole blood and erythrocyte suspensions. J Appl Physiol61:486–494
Rosenberg AA, Harris AP, Koehler RC, Hudak ML, TraystmanRJ, Jones JR (1986) Role of O2–hemoglobin affinity in theregulation of cerebral blood flow in fetal sheep. Am J Physiol251:H56–H62
Ross BK, Hlastala MP (1981) Increased hemoglobin–oxygenaffinity does not decrease muscle oxygen consumption. J ApplPhysiol 51:864–870
Roughton FJW, Severinghaus JW (1973) Accurate determinationof O2 dissociation curve of human above 98.7% saturation withdata on O2 solubility in unmodified human blood from 0� to37�C. J Appl Physiol 35:861–869
Rovida E, Niggeler M, Carlone S, Samaja M (1984) Carboxyhe-moglobin and oxygen affinity of human blood. Clin Chem30:1250–1251
Samaja M (1988) Prediction of the oxygenation of human organs atvarying blood oxygen carrying properties. Respir Physiol72:211–218
Samaja M, Rovida E (1987) The oxygen affinity properties of oldand young human erythrocytes (abstract). Ann Clin Biochem24:126
Samaja M, Melotti D, Rovida E, Rossi Bernardi L (1983) Effect oftemperature on the p50 value for human blood. Clin Chem29:110–114
Samaja M, di Prampero PE, Cerretelli P (1986) The role of 2,3-DPG in the oxygen transport at altitude. Respir Physiol 64:191–202
Samaja M, Motterlini R, Tarantola M, Beretta M, Rossi F, Sab-bioneda L, Porcellati M, Zanella A (1991) Viability of the IHP-loaded red cell in the hypoperfused isolated rat heart. AdvBiosci 81:181–188
Samaja M, Brenna L, Allibardi S, Cerretelli P (1993) Human redcell aging at 5050 m altitude: a role during adaptation to hy-poxia. J Appl Physiol 75:1696–1701
Samaja M, Mariani C, Prestini A, Cerretelli P (1997) Acid–basebalance and O2 transport at high altitude. Acta Physiol Scand159:249–256
Seaman C, Wyss S, Piomelli S (1980) The decline in energeticmetabolism with aging of the erythrocyte and its relationship tocell death. Am J Hematol 8:31–42
Severinghaus JW (1966) Blood gas calculator. J Appl Physiol21:1108–1116
Severinghaus JW (1979) Simple, accurate equations from humanblood O2 dissociation computations. J Appl Physiol 46:599–602
Sheel AW, Edwards MR, McKenzie DC (2000) Relationship be-tween decreased oxyhemoglobin saturation and exhaled nitricoxide during exercise. Acta Physiol Scand 169:149–156
Siggaard-Andersen O (1971) An acid–base chart for arterial bloodwith normal and pathophysiological reference areas. Scand JClin Lab Invest 27:239–245
Siggaard-Andersen O, Wimberley PD, Gothgen I, Siggaard-Andersen M (1984) A mathematical model of the hemoglobin-oxygen dissociation curve of human blood and of the oxygenpartial pressure as a function of temperature. Clin Chem30:1646–1651
Stringer W, Wasserman K, Casaburi R, Porszasz J, Maehara K,French W (1994) Lactic acidosis as a facilitator of oxyhemo-globin dissociation during exercise. J Appl Physiol 76:1462–1467
Stucker O, Vicaut E, Villereal MC, Ropars C, Teisserie BP, Duv-elleroy MA (1985) Coronary response to large decrease ofhemoglobin O2 affinity in isolated rat heart. Am J Physiol249:H1224–H1227
Teisserie B, Ropars C, Vallez MO, Herigault RA, Nicolau C (1985)Physiological effects of high-P50 erythrocyte transfusion onpiglets. J Appl Physiol 58:1810–1817
Teisserie B, Ropars C, Villereal M C, Nicolau C (1987) In vivoconsequences of rightward shift of the hemoglobin dissociationcurve. Adv Biosci 67:89–94
Thomas LJ (1972) Algorithms for selected blood acid-base andblood gas calculations. J Appl Physiol 33:154–158
Turek Z, Kreuzer F, Ringnalda BEM (1978a) Blood gases at sev-eral levels of oxygenation in rats with a left-shifted bloodoxygen dissociation curve. Pflugers Arch 376:7–13
Turek Z, Kreuzer F, Turek Maischeider M, Ringnalda BEM(1978b) Blood O2 content, cardiac output, and flow to organs atseveral levels of oxygenation in rats with a left-shifted bloodoxygen dissociation curve. Pflugers Arch 376:201–207
Vandegriff KD, Olson JS (1984a) The kinetics of O2 release byhuman red blood cells in the presence of external sodiumdithionite. J Biol Chem 259:12609–12618
Vandegriff KD, Olson JS (1984b) Morphological and physiologicalfactors affecting oxygen and release by red blood cells. J BiolChem 259:12619–12627
Vandegriff KD, Olson JS (1984c) A quantitative description inthree dimensions of oxygen uptake by human red blood cells.Biochem J 45:825–835
Vandegriff KD, Winslow RM (1995) A theoretical analysis ofoxygen transport: A new strategy for the design of hemoglobin-based red cell substitutes. In: Winslow RM, Vandegriff KD,Intaglietta M (eds) Blood substitutes: physiological basis ofefficacy. Birkhauser, Boston, pp 143–154
Wasserman K, Hansen JE, Sue DY (1991) Facilitation of oxygenconsumption by lactic acidosis during exercise. News PhysiolSci 6:29–34
Weiss RG, Mejia MA, Kass DA, DiPaula AF, Becker LC, Ger-stenblith G, Chacko VP (1999) Preservation of canine myo-cardial high-energy phosphates during low-flow ischemia withmodification of hemoglobin-oxygen affinity. J Clin Invest103:739–746
Winslow RM, Samaja M, Winslow NJ, Rossi Bernardi L, ShragerRI (1983) Simulation of continuous blood O2 equilibrium curveover the physiologic pH, DPG and pCO2 range. J Appl Physiol54:524–529
Winslow RM, Samaja M, West JB (1984) Red cell function atextreme altitudes on Mount Everest. J Appl Physiol 56:109–116
Woodson RD, Wranne B, Detter JC (1973) Effect of increasedblood oxygen affinity on work performance of rats. J Clin In-vest 52:2717–2724
Woodson RD, Auerbach S (1982) Effect of increased oxygenaffinity and anemia on cardiac output and its distribution. JAppl Physiol 53:1299–1306
358

Woodson RD, Hoerl C, Borchardt M (1987) P50 shifts and tissueoxygen pressure. Adv Biosci 67:79–80
Wranne B, Nordgren L, Woodson RD (1974) Increased bloodoxygen affinity and physical work capacity in man. Scand J ClinLab Invest 33:347–352
Yhap EO, Wright CB, Popovic NA, Alix EC (1975) Decreasedoxygen uptake with stored blood in the isolated hindlimb.J Appl Physiol 38:882–885
359