Embed Size (px)
Citation preview

1
The Musgrove Park Pacing Document January 2015, Dr Mark J Dayer Version 23.

2
Index
INDEX 2
THE MUSGROVE PARK PACING DOCUMENT 4
LATEST CHANGES 5
IMPLANTATION STANDARDS 7
OUR RATES 9
BOOKING 11
PATIENTS PRESENTING WITH COMPLETE HEART BLOCK 12
TREATMENT INDICATIONS 13
INDICATIONS IN GREATER DETAIL 14
IMPLANTABLE LOOP RECORDERS 36
PRE-‐OPERATIVE ASSESSMENT 38
DAY CASE PACING 39
CONSENT FORMS 40
ANTIPLATELETS AND ANTICOAGULANTS 41
DEVICE SELECTION 43
ADMISSION CHECKLIST 44
DEVICE RELATED INFECTIONS – PREVENTION 45
THE WHO SURGICAL SAFETY CHECKLIST 49
MONITORING OF THE PATIENT DURING THE PROCEDURE 50
TEMPORARY PACING 51
CONTRAST MEDIA USE 52
ANALGESIA AND SEDATION 53
SURGICAL TECHNIQUE 54
LEAD SELECTION 55
SCREENING 56
POST IMPLANT CARE 57
PACING CHECK AND CHEST X-‐RAY POST PROCEDURE 58

3
POST-‐OPERATIVE WOUND CARE 59
ICD TESTING AND VT STIMULATION 60
COMPLICATIONS AND AUDIT 61
DEVICE RELATED INFECTIONS – MANAGEMENT 62
LEAD EXTRACTION 63
PNEUMOTHORAX AND HAEMOTHORAX 64
FOLLOW-‐UP STANDARDS 65
VITATRON AND BIATRIAL GENERATOR REPLACEMENT ADVICE 66
ATRIAL FIBRILLATION 67
VENTRICULAR TACHYCARDIA 68
ELECTROMAGNETIC INTERFERENCE AND OTHER ENVIRONMENTAL ISSUES 69
DEVICE DEACTIVATION 70
MEDTRONIC DEVICES THAT ARE MRI COMPATIBLE 71
PACEMAKERS AND RADIOTHERAPY 72
PACEMAKERS AND DIATHERMY 74
OPTIVOL ALERTS 77
DRIVING 78
MDA/MHRA ALERTS 79
REFERENCES 83

4
The Musgrove Park Pacing Document The purpose of this document is to:
1. Provide standards, policies and protocols that we should adhere to in the department. 2. Act as a point of reference when questions arise
I would like to thank all of those who have provided suggestions and articles for this document. Dr Mark Dayer, November 2014

5
Latest Changes June 2012
1. Please note that all patients are now screened for MSSA and MRSA. Pacing procedures should not normally be undertaken without such screens being available, unless it is clinically urgent. In this situation decolonisation should start immediately and continue until the swab results are available.
2. Antibiotics should be given within half an hour of the start of the procedure.
3. Liquiband flex is now the preferred tissue adhesive. Liquiband should not be used.
4. The recommendation that all trainees who have done <100 implants, or trainees who are
felt to require closer monitoring, should be directly supervised by a senior operator.
5. The consent forms have been updated.
6. Please note the latest advisory on St Jude Riata leads.
7. Treatment indications. There is updated guidance on the management of patients with inherited cardiac conditions.
June 2013
1. Antibiotic prophylaxis and prevention of device-‐related infection. All patients from July 1st 2013 will be advised to use a chlorhexidine wash +/-‐ Mupirocin (if MRSA/MSSA positive).
2. Device selection.
3. Hypertrophic cardiomyopathy.
4. The management of Riata leads.
5. Pacemakers and diathermy.
6. The management of Sorin Isoline leads.
7. The acute management of complete heart block.
8. The programming of pacemakers and ICDs.
9. MRI-‐safe Medtronic devices.
10. Pacemakers and radiotherapy.

6
June 2014
1. NICE Guidelines 2014 for ICDs and CRT-‐Ds. These new guidelines radically expand the number of patients in whom a device is recommended.
2. DFT Testing. This should no longer be undertaken in the majority of cases.
3. Implant side. Most implants should be on the left unless there are particular indications.
4. AF letter. The AF letter has been updated.
5. Consent forms. All consent forms have been updated.
6. The device deactivation protocols have been updated.
7. The temporary pacing guidelines have been updated.
8. The protocols for perioperative management have been updated.

7
Implantation Standards The HR-‐UK competency standards 2010 lay down some minimum stipulations. They have been largely adopted by specialist commissioners for ICDs and CRTs, although some of the criteria are more demanding. I have reproduced the key recommendations here.
For Doctors
1. There should be at least 2 active implanting consultants per centre. If ICDs/CRTs are implanted then there will a minimum of 2 implanting ICD/CRT consultants per centre.
2. At least 1 implanter should have accreditation in device therapy (HRUK or IBHRE).
3. Each implanter should perform 35 primary pacemaker implants / year.
4. Each implanter performing ICD and/or CRT procedures should perform a minimum of 30 new complex device implants per year, with a minimum total new device implant rate (including pacemakers) of 60 per year. At least 20 should be CRT-‐D/P and at least 10 should be ICDs.
5. Each implanter will undertake appropriate CPD, including implications for driving.
For Physiologists
1. At least 1 physiologist should have accreditation in device therapy (HRUK or IBHRE).
2. All physiologists must undertake appropriate CPD in device therapy and associated patient advice including implications for driving according to DVLA guidelines.
3. Each physiologist should be actively involved in 35 primary pacemaker implants / year
4. Each physiologist undertaking ICD and or CRT procedures should have documented
experience of at least 25 CRT and 25 ICD implantation and follow-‐up procedures. There will be a minimum of 2 cardiac physiologists actively involved.
For Nurses
1. Arrangements should be made that at least 2 nurses are denoted as specialist arrhythmia nurses/centre.
2. All specialist nurses must undertake appropriate CPD in device therapy and associated patient advice including implications for driving according to DVLA guidelines (see DVLA guidelines).

8
3. All implanting centres must collect data on their patients, devices and follow-‐up, which is immediately available. They must contribute data to the National Cardiac Rhythm Management Audit. They must be aware of MHRA notices.
For Services
1. Anaesthetic support will be available for ICD implantation.
2. There must be a 24-‐hour service to deal with patients admitted with multiple shock delivery or other device related issues. This will consist of an appropriately trained cardiac physiologist and cardiologist, either on site or with clearly defined and agreed protocols with other implanting centres.
The full HR-‐UK document can be found here. A more comprehensive document from the Pan-‐London Arrhythmia project group is can be found here. The specialist commissioning document can be found here.

9
Our Rates We appear to implant devices at below the national average rates. The reasons for this are likely to be multifactorial. Firstly we have a mature pacing service. Many newer services still have a large pool of eligible patients. Secondly, there is a lack of capacity, which tends to inhibit referrals. Thirdly we have not had a functioning heart failure service for some time; a well-‐functioning heart failure service tends to identify more patients. The data below are from 2011 – the latest data currently available as of 26th May 2014; the local area team reports for 2012 are not yet available. They will be found here.
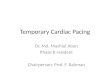
1. New Pacemaker Rates
Somerset implanted new pacemakers at a rate of 500.3 / million (red bar). The median implant rate across the UK was 524 / million in 2011 (black bar).
500.3 524.0
0 100 200 300 400 500 600 700 800 900
1 8 15
22
29
36
43
50
57
64
71
Somerset
85
92
99
106
113
120
127
134
141
148
155
162
169
176
183
190
Implant Rate / Million
PCT
New Pacemaker Implant Rate -‐ 2011

10
2. New ICD Rates
Somerset implanted new ICDs at a rate of 47.6 / million (red bar). The median implant rate across the UK was 73.1 / million in 2011 (black bar).
3. Total CRT Rates (CRT-‐P and CRT-‐D)
Somerset implanted CRTs (CRT-‐P and -‐D) at a rate of 57.3 / million (red bar). The median implant rate across the UK was 106 / million in 2011 (black bar).
47.6
73.1
0
20
40
60
80
100
120
140
160
180
2 Somerset 48 71 94 117 140 163 186
Implant Rate / Million
PCT
New ICD Implant Rate -‐ 2011
57.3
106.0
0
50
100
150
200
250
300
350
2 Somerset 55 82 109 136 163
Implant Rate / Million
PCT
Total CRT Implant Rate -‐ 2011

11
Booking We have lists on:
1. Monday pm -‐ MD/OG 2. Tuesday am -‐ MD/OG 3. Wednesday am/pm -‐ MD 4. Thursday am -‐ OG 5. Friday am -‐ SKW
There has to be some priority given to emergency cases, and therefore elective work may have to be cancelled. The highest priority needs to go to:
1. Those with a temporary wire in situ -‐ they should be done on the next pacing list if appropriate.
2. Those with an infected system -‐ similarly they should be done on the next pacing list if appropriate.
3. Those patients without a temporary wire, yet who are unstable, should be done on the next pacing list if appropriate, or a temporary wire should be sited.
There are "stable" in patients who should wait to be swabbed for MRSA/MSSA and listed according to list availability and whether decolonisation is required. Generally speaking decolonisation should have taken place for 48h prior to device implantation. We should set a target that no patient should wait as an in-‐patient for longer than one week, unless there are clinical reasons for delaying the procedure. Outpatients who have been cancelled need to be rebooked within 1 month. To facilitate the management of inpatients and patients who have had to be cancelled we have devised a points system to guide the booking of lists. Lists can be booked to 5 points but no more without discussion with the operator. There should be no more than 3 elective points per list, generally speaking, to leave time for in-‐patient cases. ILR, 1 point Box Change (no TPW) or VVI, 1.5 points DDD or B/C with TPW, 2 points ICD Box Change, 2 points ICD, 2.5 points System Upgrade (excluding new LV lead), 3 points CRT-‐P/D or upgrade including new LV lead, 5 points It is important that we keep track of waiting times. As is always the case, allowing space to deal with emergency cases results in less efficient use of lab time.

12
Patients Presenting with Complete Heart Block There has been some debate on the appropriateness of admitting patients who are found to have complete heart block. Clearly, each decision needs to be tailored to the particular patient, but we have had a number of near misses where patients have been offered an outpatient appointment or an outpatient pacemaker. My personal view is that if it is appropriate to pace the patient they should be admitted as soon as the condition is noted. It is hard to be sure of the prognosis of CHB. The median survival after diagnosis in an early publication was 25.3 months1, with many deaths occurring early. There are no modern long-‐term data on survival as pacing is so common. Our current practice in “high-‐risk” patients with CAD is to admit them and undertake angiography if indicated. This is a condition that is half as mortal as CHB. The RITA 3 trial2 compared medical treatment to angiography/angioplasty in patients with unstable angina / NSTEMIs. Mortality at 1 year was 4.6% in the invasive arm vs. 3.9% in the conservative arm. The intervention group, however, were readmitted less and did have less angina. Going back to the very early days3, patients with “preinfarctional (unstable) angina” had a survival of 75% at 24 months. It is only logical therefore to admit patients with CHB. They have a far higher mortality untreated than other conditions that we routinely admit. This appears to have the support of the majority of my colleagues.

13
Treatment Indications There are no guidelines that adequately cover all situations for devices. From the HR-‐UK document (HR-‐UK competency standards 2010) “It is recognised that published guidance does not cover all patient groups and may not be appropriate in certain situations. Furthermore, clinical judgement based on published evidence must be used for indications not yet considered by NICE. However, it is important to demonstrate compliance with best practice and regular audit of device indications and outcomes is strongly recommended”.
1. It is important to comply with NICE technology appraisal TA88 on pacing mode for symptomatic bradycardia due to sick sinus syndrome and/or AV block. That is that dual chamber pacing should be used, unless there is chronic atrial fibrillation or “when patient-‐specific factors, such as frailty or the presence of comorbidities, influence the balance of risks and benefits in favour of single-‐chamber ventricular pacing”. This is a standard to which we are audited. “Centres implanting >10% of patients in sinus rhythm with VVI(R) devices should review their practice in accordance with NICE guidance.”
2. In patients with type 1 second degree AV block on a resting ECG aged > 45 years, a
permanent pacemaker is associated with longer survival4. This has yet to appear in the guidelines.
On 25th June 2014 NICE released TA314. These are the latest indications for ICDs and CRT-‐P/Ds. They can be found here. These guidelines considerably broaden the indications for devices in patients with left ventricular systolic dysfunction. They are summarised below. The other technology appraisals/guidelines that we should be referred to are:
1. ACC/AHA/HRS 2008 Guidelines for Device-‐Based Therapy of Cardiac Rhythm Abnormalities
2. Heart Rhythm UK Position Statement on Clinical Indications for Implantable Cardioverter
Defibrillators in Adult Patients with Familial Sudden Cardiac Death Syndromes
3. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy

14
Indications in Greater Detail
Implantable Cardioverter Defibrillators The NICE 2014 guidance is detailed first, followed by recommendations from HR-‐UK and finally a review of the latest 2011 guidance for HCM. ICDs are recommended for patients for both primary and secondary prevention.
Secondary Prevention That is, for patients who present, in the absence of a treatable cause, with one of the following:
1. Having survived a cardiac arrest due to either ventricular tachycardia (VT) or ventricular fibrillation (VF).
2. Spontaneous sustained VT causing syncope or significant haemodynamic compromise.
3. Sustained VT without syncope or cardiac arrest, and who have an associated reduction in
ejection fraction (LVEF of less than 35%) (No worse than class III of the New York Heart Association functional classification of heart failure).
Primary Prevention 1. A familial cardiac condition with a high risk of sudden death, including:
a. Long QT syndrome b. Hypertrophic cardiomyopathy c. Brugada syndrome d. Arrhythmogenic right ventricular dysplasia
2. Patients who have undergone surgical repair of congenital heart disease
3. Implantable cardioverter defibrillators (ICDs), cardiac resynchronisation therapy (CRT) with
defibrillator (CRT-‐D) or CRT with pacing (CRT-‐P) are recommended as treatment options for people with heart failure who have left ventricular dysfunction with a left ventricular ejection fraction (LVEF) of 35% or less as specified in the table below:
There are a number of comments about this list:

15
1. List 1a to 1d is not exhaustive, and also there are further nuances for each of these
conditions and risk stratification is important on a case-‐by-‐case basis. HR-‐UK has issued further guidance for patients with inherited cardiac conditions5 and this is reviewed below and there is also detail in the ACC/AHA 2008 guidelines6 and the latest HCM guidance7.
2. “Patients who have undergone surgical repair of congenital heart disease” is considered too broad a brush, and the GUCH consultants will guide us.
3. It is helpful to discuss absolute risks and benefits with patients. For patients with heart
failure, the online Seattle Heart Failure Model is a helpful calculator. It is available as a smartphone app. For example, A 65 year man in NYHA class III, an ejection fraction of 25% secondary to ischaemic heart disease, a systolic BP of 110mmHg, with a mild anaemia (12.5) and who is on 80mg furosemide, an ACE-‐inhibitor, beta-‐blocker, statin and spironolactone, with a QRS duration of >120ms has an estimated 5-‐year survival of 67%. The mean life expectancy is 8.1 years. A biventricular pacemaker will increase the 5-‐year survival to 75% (9.6 years) and a biventricular ICD to 78% (10.1 years). This is very useful and can really show people what difference (or lack of) intervention makes.
4. We have debated at times “time dependency” – that is, is the time after a myocardial infarction when the indication for an ICD is discovered, relevant. It had been suggested by some that those with a very remote myocardial infarction do not benefit. However, this is not evidence based, and a recent re-‐analysis of data suggested that there is no “time dependence”. Even those with very remote myocardial infarction, who now fulfil the criteria for device implantation, benefit8.

16
Long QT Syndrome A QTc of >450ms in men and 460ms in women is abnormal. The longest QT interval in individual leads should be used, unless it is >40ms longer than other leads. The precise methods for measuring the QT interval are described in the 2009 AHA/ACCF/HRS guidelines9. The overall risk of SCD in patients with LQTS on beta-‐blockers is estimated to be around 0.1% per annum. Indicators of high risk include:
1. Personal history of aborted SCD.
2. Syncope and QT prolongation >500ms.
3. There is little evidence to support that the sudden death of a sibling is a risk factor. Note beta-‐blockers such as nadolol (40mg-‐320mg/day) or propranolol (80mg-‐640mg/day) which block β1 and β2 receptors are preferred to more cardioselective beta-‐blockers such as bisoprolol.
Current ACC/AHA/ESC Guidance Class I. Implantation of an ICD along with the use of beta-‐blockers is recommended for
LQTS patients with previous cardiac arrest (level of evidence: A). Class IIa. Implantation of an ICD with continued use of beta-‐blockers can be effective to
reduce SCD in LQTS patients experiencing syncope and/or VT while receiving beta-‐blockers (level of evidence: B).
Class IIb. Implantation of an ICD with the use of beta-‐blockers may be considered for
prophylaxis of SCD for patients in categories possibly associated with higher risk of cardiac arrest such as LQT2 and LQT3 (level of evidence: B).
HR-‐UK Recommendations
1. Long QT syndrome patients presenting with ventricular fibrillation/cardiac arrest without reversible precipitant should undergo ICD implantation in addition to oral beta-‐blockade (Estimated risk 3.37% per annum).
2. Long QT syndrome patients experiencing continuing syncope despite beta-‐blockade or left
cardiac sympathetic denervation (LCSD) (when VT/VF has not been excluded as the cause of syncope) should undergo ICD implantation (Estimated risk 2.18% per annum).
3. The identification of an LQT2 or LQT3 genotype should not by itself constitute an indication
for ICD implantation (Estimated risk 0.6% per annum (LQT2), 0.56% per annum (LQT3)).

17
Brugada Syndrome The diagnosis of Brugada syndrome requires the presence of the type I Brugada ECG pattern (Coved ST elevation, J point elevation ≥ 2mm), the absence of cardiac structural disease and at least one of 10:
1. Syncope 2. Prior cardiac arrest 3. Documented / inducible polymorphic VT 4. Ventricular fibrillation 5. Family history of SCD < 45 years 6. Nocturnal agonal respiration
Indicators of a high risk of SCD are:
1. A personal history of aborted SCD or syncope 2. A spontaneous type I ECG 3. Male gender 4. South East Asian Origin
A family history of SCD or a SCN5A mutation does not carry an increased risk of SCD.
Current ACC/AHA/ESC Guidance Class I. An ICD is indicated for Brugada syndrome patients with previous cardiac arrest. Class IIa. An ICD is reasonable for Brugada syndrome patients with spontaneous ST segment
elevation in V1, V2, or V3 who have had syncope; an ICD is reasonable for Brugada syndrome patients with documented VT that has not resulted in cardiac arrest.
Class IIb. EP testing may be considered for risk stratification in asymptomatic Brugada
syndrome patients with spontaneous ST elevation.
HR-‐UK Recommendations Brugada syndrome patients presenting with ventricular fibrillation/cardiac arrest without reversible precipitant should undergo ICD implantation (Estimated risk 7.7%-‐13.8% per annum). Brugada syndrome patients with syncope (when VT/VF has not been excluded as the cause of syncope) should undergo ICD implantation (Estimated risk 1.9%-‐8.8% per annum). A firm recommendation regarding ICD implantation in patients with a spontaneous type 1 ECG without symptoms cannot be made at this time; either a conservative strategy or ICD implantation based on results of EP testing can be supported by different series. An EP study is not unreasonable. A negative EP study has a high negative predictive value in asymptomatic patients. Asymptomatic individuals who require a drug to induce the type 1 ECG pattern are at low risk of sudden death and the risks of ICD therapy are likely to outweigh the benefits in this group.

18
Catecholaminergic Polymorphic VT Patients are usually children, adolescents or young adults who present with syncope occurring during exercise or emotion and:
1. Bidirectional VT or 2. Polymorphic VT or 3. Idiopathic VF
There may be a family history. There is no evidence of structural heart disease. There is a tendency to sinus bradycardia. I suspect that older patients will begin to be diagnosed with this condition as awareness increases.
Current ACC/AHA/ESC Guidance Class I. Implantation of an ICD along with the use of beta-‐blockers is recommended for
patients with CPVT who are survivors of cardiac arrest (level of evidence C). Class IIa. Implantation of an ICD along with the use of beta-‐blockers can be effective for
affected patients with CPVT with syncope and/or documented sustained VT while receiving beta-‐blockers (level of evidence C).
HR-‐UK Recommendations Catecholaminergic polymorphic ventricular tachycardia patients presenting with ventricular fibrillation/cardiac arrest without reversible precipitant should undergo ICD implantation in addition to oral beta-‐blockade or LCSD (Estimated risk 1.2% per annum). Catecholaminergic polymorphic ventricular tachycardia patients experiencing sustained VT or syncope (when VT/VF has not been excluded as the cause) despite beta-‐blockade or LCSD should be considered for ICD implantation. Recommendation: Catecholaminergic polymorphic ventricular tachycardia patients experiencing exercise-‐induced sustained VT despite beta-‐blockade or LCSD should be considered for ICD implantation.

19
Arrhythmogenic Right Ventricular Cardiomyopathy Patients usually present in their late teens or twenties with palpitations, syncope or SCD. The ECG shows T wave inversion in V1-‐V3 ± RBBB. Epsilon waves are occasionally present. The ECG during VT is characteristically LBBB. There are particular echocardiographic / MRI features that are beyond the scope of this guideline11.
Current ACC/AHA/ESC Guidance Class I. Implantable cardioverter defibrillator implantation is recommended for the
prevention of SCD in patients with ARVC with documented sustained VT or VF (level of evidence: B).
Class IIa. Implantable cardioverter defibrillator implantation can be effective for the
prevention of SCD in patients with ARVC with extensive disease, including those with LV involvement, one or more affected family members with SCD, or undiagnosed syncope when VT or VF has not been excluded as the cause of syncope (level of evidence: C).
Class IIb. EP testing might be useful for the risk assessment of SCD in patients with ARVC
(level of evidence: C).
HR-‐UK Recommendations Arrhythmogenic right ventricular cardiomyopathic patients presenting with ventricular fibrillation/cardiac arrest (Estimated risk 21% per annum) or poorly tolerated VT (Estimated risk 9% per annum) should undergo ICD implantation. Arrhythmogenic right ventricular cardiomyopathic patients presenting with syncope (when VT/VF has not been excluded as the cause of syncope) should undergo ICD implantation (Estimated risk 8% per annum). Arrhythmogenic right ventricular cardiomyopathic patients presenting with ventricular arrhythmias and severe structural disease should be considered for ICD implantation. Arrhythmogenic right ventricular cardiomyopathic patients who are asymptomatic with mild disease are at low risk of sudden death (Estimated risk 0.1% per annum), and the risks of ICD therapy may outweigh the benefits in this group.

20
Sarcoidosis Sarcoidosis is a relatively common granulomatous disorder can cause sudden cardiac death. There is a clear indication for an ICD in those with ventricular arrhythmias. The decision whether to offer a patient a primary prevention device is more difficult. It should be remembered, however, that ventricular dysfunction is a strong predictor of ventricular arrhythmias, as is heart block6,12.

21
Hypertrophic Cardiomyopathy The latest guidelines for the diagnosis and treatment of HCM were released at the end of 20117. Maron and Maron have produced a recent clinical update13. There is a need to risk-‐assess patients and the latest guidance is reproduced below (figure 1). When discussing risks with patients, it is useful to estimate the absolute risk of SCD. O’Mahoney et al.14 have estimated the risk of SCD according to the number of common risk factors (table 1) from a cohort of 1606 patients. The prescriptions of ICDs to patients with HCM remain controversial.
Table 1
Number of Risk Factors*
Annual rate Of shocks CI Relative Risk CI Significance
0 0.45% 0.29-‐0.70 1 N/A N/A 1 0.65% 0.45-‐0.92 1.43 0.82-‐2.51 0.21 2 1.3% 0.89-‐1.90 2.87 1.61-‐5.14 <0.001 3 1.9% 0.92-‐4.10 4.32 1.82-‐10.21 <0.001 ≥4 5.0% 1.88-‐13.4 11.37 3.85-‐33.62 <0.0001
*Risk factors:
• Family history of SCD • Non-‐sustained VT • Unexplained syncope • Abnormal blood pressure response to exercise • LVH > 30mm
There remains debate over the importance of particular risk factors. The guidelines below suggest that a single risk factor is an adequate reason for device implantation. This is not a universally held view, and given the minimal additional risks that one risk factor conveys, some may choose not to offer therapy to this group. Probably the most sensible approach is to discuss the absolute risks with the patient and let them decide.
Risk Stratification
Class I
1. All patients with HCM should undergo comprehensive SCD risk stratification at initial evaluation to determine the presence of the following (Level of Evidence: B):
a. A personal history for ventricular fibrillation, sustained VT, or SCD events, including appropriate ICD therapy for ventricular tachyarrhythmias.
b. A family history for SCD events, including appropriate ICD therapy for ventricular tachyarrhythmias.
c. Unexplained syncope. d. Documented NSVT defined as 3 or more beats at greater than or equal to 120 bpm
on ambulatory (Holter) ECG. e. Maximal LV wall thickness greater than or equal to 30 mm.

22
Class IIa
1. It is reasonable to assess blood pressure response during exercise as part of SCD risk stratification in patients with HCM (Level of Evidence: B).
2. SCD risk stratification is reasonable on a periodic basis (every 12 to 24 months) for patients
with HCM who have not undergone ICD implantation but would otherwise be eligible in the event that risk factors are identified (12 to 24 months) (Level of Evidence: C).
Class IIb
1. The usefulness of the following potential SCD risk modifiers is unclear but might be considered in selected patients with HCM for whom risk remains borderline after documentation of conventional risk factors:
a. CMR imaging with LGE (Level of Evidence: C). b. Double and compound mutations (i.e., >1) (Level of Evidence: C). c. Marked LVOT obstruction (Level of Evidence: B).
Class III: Harm
1. Invasive electrophysiologic testing as routine SCD risk stratification for patients with HCM should not be performed (Level of Evidence: C).
ICD Recommendations The decision to place an ICD in patients with HCM should include application of individual clinical judgment, as well as a thorough discussion of the strength of evidence, benefits, and risks to allow the informed patient's active participation in decision-‐making (Level of Evidence: C).
Class I
1. ICD placement is recommended for patients with HCM with prior documented cardiac arrest, ventricular fibrillation, or haemodynamically significant VT (Level of Evidence: B).
Class IIa
1. It is reasonable to recommend an ICD for patients with HCM with: a. Sudden death presumably caused by HCM in 1 or more first-‐degree relatives (Level
of Evidence: C). b. A maximum LV wall thickness greater than or equal to 30 mm (Level of Evidence: C). c. One or more recent, unexplained syncopal episodes (Level of Evidence: C).
2. An ICD can be useful in select patients with NSVT (particularly those <30 years of age) in
the presence of other SCD risk factors or modifiers (Level of Evidence: C).
3. An ICD can be useful in select patients with HCM with an abnormal blood pressure response with exercise in the presence of other SCD risk factors or modifiers (Level of Evidence: C).

23
4. It is reasonable to recommend an ICD for high-‐risk children with HCM, based on unexplained syncope, massive LV hypertrophy, or family history of SCD, after taking into account the relatively high complication rate of long-‐term ICD implantation (Level of Evidence: C).
Class IIb
1. The usefulness of an ICD is uncertain in patients with HCM with isolated bursts of NSVT when in the absence of any other SCD risk factors or modifiers (Level of Evidence: C).
2. The usefulness of an ICD is uncertain in patients with HCM with an abnormal blood
pressure response with exercise when in the absence of any other SCD risk factors or modifiers, particularly in the presence of significant outflow obstruction (Level of Evidence: C).
Class III: Harm
1. ICD placement as a routine strategy in patients with HCM without an indication of increased risk is potentially harmful (Level of Evidence: C).
2. ICD placement as a strategy to permit patients with HCM to participate in competitive athletics is potentially harmful (Level of Evidence: C).
3. ICD placement in patients who have an identified HCM genotype in the absence of clinical
manifestations of HCM is potentially harmful (Level of Evidence: C).

24
Figure 1 – Recommendations for ICDs in HCM. Modified from the 2011 ACCF/AHA Guidelines7

25
Cardiac Resynchronisation Therapy See the section above on ICDs and NICE TA314. We do implant patients who have atrial fibrillation. It is imperative that heart rate control is adequate and strong consideration should be given to AV node ablation. There is now clear evidence that it can be of benefit15 and it is in line with guidance from the ESC16. Biventricular pacing / CRT has an inconsistent impact on ventricular arrhythmias and should not be “sold” to patients as a method for reducing arrhythmias, however placement of an LV lead in a posterior or lateral (but not anterior) lead position may reduce ventricular arrhythmia burden. This should only be undertaken in patients with an indication for CRT however17. In terms of lead positioning, it seems important to avoid the apex18,19. The lateral position is still preferred, but if it is not possible, an anterior position is acceptable. Noheria et al. have summarised the variations in coronary sinus anatomy that commonly exist20. Patients who have a routine indication for pacing, and who are likely to pace for large percentages of the time (e.g. patients with complete heart block) should undergo echocardiography. Those patients with a reduced ejection fraction should be considered for biventricular pacing21,22. Generally patients who are implanted should be fit enough to be discharged, but patients who are in hospital will sometimes be considered. Cardiac resynchronisation therapy in patients with severe heart failure mandating in-‐patient treatment has been shown to have a good survival post device implantation23.

26
Conventional Pacing Indications This guidance has been derived from the ACC/AHA/HRS 2008 and HRS/ACCF 2012 guidelines for device-‐based therapy6.
Recommendations for Permanent Pacing in Sinus Node Dysfunction (SND) Note: dual chamber or AAI pacing is recommended in this situation to reduce the risk of AF. Rate adaptive pacing can be useful in patients with chronotropic incompetence. Strategies to minimise ventricular pacing should be used. A VVI system should only be used if pacing is likely to be infrequent and/or there are significant co-‐morbidities. As the risk of developing AV block is high, in our department AAI pacing is not recommended.
Class I
1. Permanent pacemaker implantation is indicated for SND with documented symptomatic bradycardia, including frequent sinus pauses that produce symptoms. (Level of Evidence: C)
2. Permanent pacemaker implantation is indicated for symptomatic chronotropic
incompetence. (Level of Evidence: C)
3. Permanent pacemaker implantation is indicated for symptomatic sinus bradycardia that results from required drug therapy for medical conditions. (Level of Evidence: C)
Class IIa
1. Permanent pacemaker implantation is reasonable for SND with heart rate less than 40 bpm when a clear association between significant symptoms consistent with bradycardia and the actual presence of bradycardia has not been documented. (Level of Evidence: C)
2. Permanent pacemaker implantation is reasonable for syncope of unexplained origin when
clinically significant abnormalities of sinus node function are discovered or provoked in electrophysiological studies. (Level of Evidence: C)
Class IIb
1. Permanent pacemaker implantation may be considered in minimally symptomatic patients with chronic heart rate less than 40 bpm while awake. (Level of Evidence: C)
Class III
1. Permanent pacemaker implantation is not indicated for SND in asymptomatic patients. (Level of Evidence: C)

27
2. Permanent pacemaker implantation is not indicated for SND in patients for whom the symptoms suggestive of bradycardia have been clearly documented to occur in the absence of bradycardia. (Level of Evidence: C)
3. Permanent pacemaker implantation is not indicated for SND with symptomatic bradycardia
due to nonessential drug therapy. (Level of Evidence: C)
Recommendations for Acquired Atrioventricular Block in Adults AV block is common in elderly patients and in patients with coronary artery and aortic valve disease. Significant AV block is rare in younger individuals, and a cause should be sought24. Note that high degrees of AV block in younger patients can be vagally mediated and this is not an indication for pacing25. Conversely, Mobitz type I AV block in more elderly patients (>70 years approximately) is not necessarily a benign condition and strong consideration should be given to pacing26. Dual chamber pacing should be the default position unless there is a particular clinical situation (e.g. significant comorbidity or difficult vascular access) that makes single chamber pacing more desirable.
Class I
1. Permanent pacemaker implantation is indicated for third degree and advanced second-‐degree AV block at any anatomic level associated with bradycardia with symptoms (including heart failure) or ventricular arrhythmias presumed to be due to AV block. (Level of Evidence: C)
2. Permanent pacemaker implantation is indicated for third degree and advanced second-‐
degree AV block at any anatomic level associated with arrhythmias and other medical conditions that require drug therapy that results in symptomatic bradycardia. (Level of Evidence: C)
3. Permanent pacemaker implantation is indicated for third degree and advanced second-‐
degree AV block at any anatomic level in awake, symptom-‐free patients in sinus rhythm, with documented periods of asystole greater than or equal to 3.0 seconds or any escape rate less than 40 bpm, or with an escape rhythm that is below the AV node. (Level of Evidence: C)
4. Permanent pacemaker implantation is indicated for third-‐degree and advanced second-‐
degree AV block at any anatomic level in awake, symptom-‐free patients with AF and bradycardia with 1 or more pauses of at least 5 seconds or longer. (Level of Evidence: C)
5. Permanent pacemaker implantation is indicated for third degree and advanced second-‐
degree AV block at any anatomic level after catheter ablation of the AV junction. (Level of Evidence: C)

28
6. Permanent pacemaker implantation is indicated for third degree and advanced second-‐degree AV block at any anatomic level associated with postoperative AV block that is not expected to resolve after cardiac surgery. (Level of Evidence: C)
7. Permanent pacemaker implantation is indicated for third-‐degree and advanced second-‐
degree AV block at any anatomic level associated with neuromuscular diseases with AV block, such as myotonic muscular dystrophy, Kearns-‐Sayre syndrome, Erb dystrophy (limb-‐girdle muscular dystrophy), and peroneal muscular atrophy, with or without symptoms. (Level of Evidence: B)
8. Permanent pacemaker implantation is indicated for second-‐degree AV block with
associated symptomatic bradycardia regardless of type or site of block. (Level of Evidence: B)
9. Permanent pacemaker implantation is indicated for asymptomatic persistent third-‐degree
AV block at any anatomic site with average awake ventricular rates of 40 bpm or faster if cardiomegaly or LV dysfunction is present or if the site of block is below the AV node. (Level of Evidence: B)
10. Permanent pacemaker implantation is indicated for second-‐ or third-‐degree AV block
during exercise in the absence of myocardial ischemia. (Level of Evidence: C)
Class IIa
1. Permanent pacemaker implantation is reasonable for persistent third-‐degree AV block with an escape rate greater than 40 bpm in asymptomatic adult patients without cardiomegaly. (Level of Evidence: C)
2. Permanent pacemaker implantation is reasonable for asymptomatic second-‐degree AV
block at intra-‐ or infra-‐His levels found at electrophysiological study. (Level of Evidence: B)
3. Permanent pacemaker implantation is reasonable for first-‐ or second-‐degree AV block with symptoms similar to those of pacemaker syndrome or hemodynamic compromise. (Level of Evidence: B)
4. Permanent pacemaker implantation is reasonable for asymptomatic type II second-‐degree
AV block with a narrow QRS. When type II second-‐degree AV block occurs with a wide QRS, including isolated right bundle-‐branch block, pacing becomes a Class I recommendation. (See "Chronic Bifascicular Block.") (Level of Evidence: B)
Class IIb
1. Permanent pacemaker implantation may be considered for neuromuscular diseases such as myotonic muscular dystrophy, Erb dystrophy (limb-‐girdle muscular dystrophy), and peroneal muscular atrophy with any degree of AV block (including first-‐degree AV block), with or without symptoms, because there may be unpredictable progression of AV conduction disease. (Level of Evidence: B)

29
a. Myotonic dystrophy is the most common form of muscular dystrophy in adults. Cardiac involvement is characterised by myocardial fibrosis leading to degeneration of the conducting system and ventricular dysfunction. It is not unreasonable to implant a pacemaker (if not an ICD) in patients with atrial arrhythmias, a PR interval longer than 240ms or a QRS duration of > 120ms, or an ICD in patients with significant left ventricular dysfunction. See Groh et al27. NOTE: In patients with syncope an ICD is reasonable (discuss individual cases with Bristol), particularly if there are other risk factors.
2. Permanent pacemaker implantation may be considered for AV block in the setting of drug
use and/or drug toxicity when the block is expected to recur even after the drug is withdrawn. (Level of Evidence: B)
Class III
1. Permanent pacemaker implantation is not indicated for asymptomatic first-‐degree AV block. (Level of Evidence: B) (See "Chronic Bifascicular Block.")
2. Permanent pacemaker implantation is not indicated for asymptomatic type I second-‐
degree AV block at the supra-‐His (AV node) level or that which is not known to be intra-‐ or infra-‐Hisian. (Level of Evidence: C)
3. Permanent pacemaker implantation is not indicated for AV block that is expected to
resolve and is unlikely to recur (e.g., drug toxicity, Lyme disease, or transient increases in vagal tone or during hypoxia in sleep apnoea syndrome in the absence of symptoms). (Level of Evidence: B)
Recommendations for Permanent Pacing in Chronic Bifascicular Block
Class I
1. Permanent pacemaker implantation is indicated for advanced second-‐degree AV block or intermittent third-‐degree AV block. (Level of Evidence: B)
2. Permanent pacemaker implantation is indicated for type II second-‐degree AV block. (Level
of Evidence: B)
3. Permanent pacemaker implantation is indicated for alternating bundle-‐branch block. (Level of Evidence: C)
Class IIa
1. Permanent pacemaker implantation is reasonable for syncope not demonstrated to be due to AV block when other likely causes have been excluded, specifically ventricular tachycardia (VT). (Level of Evidence: B)

30
2. Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of a markedly prolonged HV interval (greater than or equal to 100 milliseconds) in asymptomatic patients. (Level of Evidence: B)
3. Permanent pacemaker implantation is reasonable for an incidental finding at
electrophysiological study of pacing-‐induced infra-‐His block that is not physiological. (Level of Evidence: B)
Class IIb
1. Permanent pacemaker implantation may be considered in the setting of neuromuscular diseases such as myotonic muscular dystrophy, Erb dystrophy (limb-‐girdle muscular dystrophy), and peroneal muscular atrophy with bifascicular block or any fascicular block, with or without symptoms. (Level of Evidence: C)
Class III
2. Permanent pacemaker implantation is not indicated for fascicular block without AV block or symptoms. (Level of Evidence: B)
3. Permanent pacemaker implantation is not indicated for fascicular block with first-‐degree
AV block without symptoms. (Level of Evidence: B)
Recommendations for Permanent Pacing After the Acute Phase of Myocardial Infarction
Class I
1. Permanent ventricular pacing is indicated for persistent second-‐degree AV block in the His-‐Purkinje system with alternating bundle-‐branch block or third-‐degree AV block within or below the His-‐Purkinje system after ST-‐segment elevation MI. (Level of Evidence: B)
2. Permanent ventricular pacing is indicated for transient advanced second-‐ or third-‐degree
infranodal AV block and associated bundle-‐branch block. If the site of block is uncertain, an electrophysiological study may be necessary. (Level of Evidence: B)
3. Permanent ventricular pacing is indicated for persistent and symptomatic second-‐ or third-‐
degree AV block. (Level of Evidence: C)
Class IIb
1. Permanent ventricular pacing may be considered for persistent second-‐ or third-‐degree AV block at the AV node level, even in the absence of symptoms. (Level of Evidence: B)
Class III
1. Permanent ventricular pacing is not indicated for transient AV block in the absence of intraventricular conduction defects. (Level of Evidence: B)

31
2. Permanent ventricular pacing is not indicated for transient AV block in the presence of isolated left anterior fascicular block. (Level of Evidence: B)
3. Permanent ventricular pacing is not indicated for new bundle-‐branch block or fascicular
block in the absence of AV block. (Level of Evidence: B)
4. Permanent ventricular pacing is not indicated for persistent asymptomatic first-‐degree AV block in the presence of bundle-‐branch or fascicular block. (Level of Evidence: B)
Recommendations for Permanent Pacing in Hypersensitive Carotid Sinus Syndrome and Neurocardiogenic Syncope
Class I
1. Permanent pacing is indicated for recurrent syncope caused by spontaneously occurring carotid sinus stimulation and carotid sinus pressure that induces ventricular asystole of more than 3 seconds. (Level of Evidence: C)
Class IIa
1. Permanent pacing is reasonable for syncope without clear, provocative events and with a hypersensitive cardioinhibitory response of 3 seconds or longer. (Level of Evidence: C)
Class IIb
1. Permanent pacing may be considered for significantly symptomatic neurocardiogenic syncope associated with bradycardia documented spontaneously or at the time of tilt-‐table testing. (Level of Evidence: B)
Class III
1. Permanent pacing is not indicated for a hypersensitive cardioinhibitory response to carotid sinus stimulation without symptoms or with vague symptoms. (Level of Evidence: C)
2. Permanent pacing is not indicated for situational vasovagal syncope in which avoidance
behaviour is effective and preferred. (Level of Evidence: C)
Recommendations for Pacing After Cardiac Transplantation
Class I
1. Permanent pacing is indicated for persistent inappropriate or symptomatic bradycardia not expected to resolve and for other Class I indications for permanent pacing. (Level of Evidence: C)

32
Class IIb
1. Permanent pacing may be considered when relative bradycardia is prolonged or recurrent, which limits rehabilitation or discharge after postoperative recovery from cardiac transplantation. (Level of Evidence: C)
2. Permanent pacing may be considered for syncope after cardiac transplantation even when
bradyarrhythmia has not been documented. (Level of Evidence: C)
Recommendations for Permanent Pacemakers That Automatically Detect and Pace to Terminate Tachycardias
Class IIa
1. 1 Permanent pacing is reasonable for symptomatic recurrent SVT that is reproducibly terminated by pacing when catheter ablation and/or drugs fail to control the arrhythmia or produce intolerable side effects. (Level of Evidence: C)
Class III
1. Permanent pacing is not indicated in the presence of an accessory pathway that has the capacity for rapid anterograde conduction. (Level of Evidence: C)
Recommendations for Pacing to Prevent Tachycardia
Class I
1. Permanent pacing is indicated for sustained pause-‐dependent VT, with or without QT prolongation. (Level of Evidence: C)
Class IIa
1. Permanent pacing is reasonable for high-‐risk patients with congenital long-‐QT syndrome. (Level of Evidence: C)
Class IIb
1. Permanent pacing may be considered for prevention of symptomatic, drug-‐refractory, recurrent AF in patients with coexisting SND. (Level of Evidence: B)
Class III
1. Permanent pacing is not indicated for frequent or complex ventricular ectopic activity without sustained VT in the absence of the long-‐QT syndrome. (Level of Evidence: C)
2. Permanent pacing is not indicated for torsade de pointes VT due to reversible causes.
(Level of Evidence: A)

33
Recommendation for Pacing to Prevent Atrial Fibrillation
Class III
1. Permanent pacing is not indicated for the prevention of AF in patients without any other indication for pacemaker implantation. (Level of Evidence: B)
Recommendations for Pacing in Patients With Hypertrophic Cardiomyopathy
Class I
1. Permanent pacing is indicated for SND or AV block in patients with HCM as described previously (see "Sinus Node Dysfunction," and "Acquired Atrioventricular Block in Adults"). (Level of Evidence: C) When risk factors for SCD are present, consider a DDD ICD.
Class IIb
1. Permanent (dual chamber) pacing may be considered in medically refractory symptomatic patients with HCM and significant resting or provoked LV outflow tract obstruction. (Level of Evidence: A) When risk factors for SCD are present, consider a DDD ICD.
Class III
1. Permanent pacemaker implantation is not indicated for patients who are asymptomatic or whose symptoms are medically controlled. (Level of Evidence: C)
2. Permanent pacemaker implantation is not indicated for symptomatic patients without
evidence of LV outflow tract obstruction. (Level of Evidence: C)
Recommendations for Permanent Pacing in Children, Adolescents, and Patients With Congenital Heart Disease
Class I
1. Permanent pacemaker implantation is indicated for advanced second-‐ or third-‐degree AV block associated with symptomatic bradycardia, ventricular dysfunction, or low cardiac output. (Level of Evidence: C)
2. Permanent pacemaker implantation is indicated for SND with correlation of symptoms
during age-‐inappropriate bradycardia. The definition of bradycardia varies with the patient's age and expected heart rate. (Level of Evidence: B)
3. Permanent pacemaker implantation is indicated for postoperative advanced second-‐ or
third-‐degree AV block that is not expected to resolve or that persists at least 7 days after cardiac surgery. (Level of Evidence: B)

34
4. Permanent pacemaker implantation is indicated for congenital third-‐degree AV block with a wide QRS escape rhythm, complex ventricular ectopy, or ventricular dysfunction. (Level of Evidence: B). A recent review by Bordachar et al28 recommended pacing for:
a. Symptomatic patients and for b. Asymptomatic patients presenting with
i. Profound bradycardia, or ii. Left ventricular dysfunction, or iii. A wide QRS interval, or iv. A prolonged QT interval.
It is now recognized that a subset of paced patients develop dilated cardiomyopathy and heart failure, and therefore regular follow-‐up is important.
5. Permanent pacemaker implantation is indicated for congenital third-‐degree AV block in the
infant with a ventricular rate less than 55 bpm or with congenital heart disease and a ventricular rate less than 70 bpm. (Level of Evidence: C)
Class IIa
1. Permanent pacemaker implantation is reasonable for patients with congenital heart disease and sinus bradycardia for the prevention of recurrent episodes of intra-‐atrial re-‐entrant tachycardia; SND may be intrinsic or secondary to antiarrhythmic treatment. (Level of Evidence: C)
2. Permanent pacemaker implantation is reasonable for congenital third-‐degree AV block
beyond the first year of life with an average heart rate less than 50 bpm, abrupt pauses in ventricular rate that are 2 or 3 times the basic cycle length, or associated with symptoms due to chronotropic incompetence. (Level of Evidence: B)
3. Permanent pacemaker implantation is reasonable for sinus bradycardia with complex
congenital heart disease with a resting heart rate less than 40 bpm or pauses in ventricular rate longer than 3 seconds. (Level of Evidence: C)
4. Permanent pacemaker implantation is reasonable for patients with congenital heart
disease and impaired haemodynamics due to sinus bradycardia or loss of AV synchrony. (Level of Evidence: C)
5. Permanent pacemaker implantation is reasonable for unexplained syncope in the patient
with prior congenital heart surgery complicated by transient complete heart block with residual fascicular block after a careful evaluation to exclude other causes of syncope. (Level of Evidence: B)
Class IIb
1. Permanent pacemaker implantation may be considered for transient postoperative third-‐degree AV block that reverts to sinus rhythm with residual bifascicular block. (Level of Evidence: C)

35
2. Permanent pacemaker implantation may be considered for congenital third-‐degree AV block in asymptomatic children or adolescents with an acceptable rate, a narrow QRS complex, and normal ventricular function. (Level of Evidence: B)
3. Permanent pacemaker implantation may be considered for asymptomatic sinus
bradycardia after biventricular repair of congenital heart disease with a resting heart rate less than 40 bpm or pauses in ventricular rate longer than 3 seconds. (Level of Evidence: C)
Class III
1. Permanent pacemaker implantation is not indicated for transient postoperative AV block with return of normal AV conduction in the otherwise asymptomatic patient. (Level of Evidence: B)
2. Permanent pacemaker implantation is not indicated for asymptomatic bifascicular block
with or without first-‐degree AV block after surgery for congenital heart disease in the absence of prior transient complete AV block. (Level of Evidence: C)
3. Permanent pacemaker implantation is not indicated for asymptomatic type I second-‐
degree AV block. (Level of Evidence: C)
4. Permanent pacemaker implantation is not indicated for asymptomatic sinus bradycardia with the longest relative risk interval less than 3 seconds and a minimum heart rate more than 40 bpm. (Level of Evidence: C)

36
Implantable Loop Recorders Implantable loop recorders (ILRs) are being implanted increasingly frequently, particularly with the release of the new NICE guidelines (Transient loss of consciousness in adults and young people, CG109). All loop recorders should be approved by the clinical lead for cardiology prior to implantation. In terms of preparation for the procedure, the same guidelines that are used for permanent pacing are relevant. All patients should be seen by the arrhythmia nurses prior to implantation. All patients should be monitored remotely. We have a separate ILR proforma. We have trained a specialist nurse to implant loop recorders and the documents relevant to this process can be found here.

37
The Programming of ICDs The goal of ICD programming is to keep the patient safe and reduce the risk of inappropriate shocks. Inappropriate shocks are more than just painful – they can be life threatening. The MADIT-‐RIT trial29 (sponsored by Boston) was published in 2012 and directly examined the impact of different programming strategies in patients with dual chamber ICDs (or CRT-‐Ds). This trial randomised 1500 patients with ICDs to one of three strategies:
1. Conventional therapy a. 170-‐199 bpm, 2.5s delay (i.e. 7-‐8 beats), onset/stability on, ATP then shock b. ≥200 bpm, 1s delay (i.e. >3 beats), quick convert ATP then shock
2. High-‐rate
a. 170-‐199 bpm, monitor-‐only zone b. ≥200 bpm, 2.5s delay (i.e. 8 beats), quick convert ATP then shock
3. Delayed-‐therapy
a. 170-‐199 bpm, 60s delay (i.e. 170-‐199 beats), Rhythm ID Detection Enhancements on, ATP then shock
b. 200-‐249 bpm, 12s delay (i.e. 40-‐50 beats), Rhythm ID Detection Enhancements on, ATP then shock
c. ≥250 bpm, 2.5s delay (i.e. >10 beats), quick convert ATP then shock Patients with high-‐rate or delayed therapy had a significantly better outcome than patients with “conventional therapy”. They had fewer shocks and a reduced mortality. There was little to choose between the high-‐rate and delayed therapy groups. This study strongly suggests that it is safe to use higher thresholds than have been used in the past and delay therapy. Therefore, for patients with primary prevention devices, or patients who have had a VF arrest, it is appropriate to set their VF zone to > 200 bpm and delay therapy (e.g. for Medtronic/Biotronik devices 30/40 with ATP during charging). A VT zone should only be set where VT has been documented, and it is appropriate to delay therapies when the VT is less than 200 bpm. Further support in setting longer detection intervals comes from ADVANCE III30 (sponsored by Medtronic). This showed that patients set to 30/40 intervals had significantly fewer therapies than those set to 18/24. The time to the first inappropriate shock was far longer. There was no difference in mortality.

38
Pre-‐operative Assessment All patients should undergo some form of pre-‐operative assessment prior to pacemaker implantation. Patients should be assessed at the earliest opportunity. The purpose is to:
1. Prepare the patient psychologically for the procedure, including explaining what the procedure entails and possible complications. A consent form should be given to the patient, as should appropriate literature.
2. Ensure the procedure is appropriate. 3. Ensure the procedure is safe. 4. Identify any potential problems, including procedure related problems and problems with
aftercare. The pacing proforma should start to be completed. All patients who are having an ICD or reveal device inserted should see the arrhythmia nurses pre-‐operatively in addition to attending POAC. The arrhythmia nurses have defined their role in pacing. They have also produced specific guidance for their pre and post follow-‐up ICD clinics. All patients should be given a copy of their consent form prior to the procedure and a copy of the pacemaker leaflet or ICD leaflet. For patients receiving a new implant/upgrade the appropriate Arrhythmia Alliance leaflet and/or Cameron Health documentation should be included. These can be found here.
Useful links:
British Heart Foundation Pacemakers ICDs
Arrhythmia Alliance Booklets

39
Day case pacing
Day case pacing was reported as being safe and acceptable in 198931. The study was extended and the conclusions did not change32. It is now routine practice in many trusts. A number of years ago, the audit commission identified our trust as an outlier and suggested we could reduce the number of bed days occupied by pacemaker patients by 373 per annum (Report, see page 11). We have moved towards day case pacing and recent data suggest our average length of stay for routine pacing procedures has declined significantly.
A number of criteria need to be met for a patient to be suitable for same-‐day discharge, as not all patients will be.
1. The patient should be operated on in the morning.
2. The patient should have someone at home who is able to look after them.
3. The chest X-‐ray should be done at least 4 hours after the procedure.
4. The pacing check should be done at least 4 hours after the procedure.
5. The procedure should have proceeded without complications and the operator should be
happy for the patient to go home.
6. It should be remembered that there is a small, but recognised, risk of pro-‐arrhythmia shortly after implant of CRT devices33, although most patients who undergo CRT implantation on a morning list will be expected to be discharged the same day.

40
Consent Forms The consent forms have been reviewed and revised to reflect the real-‐world complication rates that occur in this centre. There are different consent forms for different procedures. They can be found here. The amount of information which can be included on the trust consent forms is limited and it is important to have a thorough discussion with the patient. Generally speaking a person capable of performing that procedure should obtain consent. Preferably the person performing the procedure should obtain consent. Foundation year doctors should not obtain consent. They were updated in 2014 to take into account an editorial by Daniel Sokol34, and a complaint about a frozen shoulder.

41
Antiplatelets and anticoagulants Haematomas post device insertion are painful, concerning for patients, may prolong hospital stay, and increase the risk of device related infection35. There seems little doubt that heparin bridging in patients taking warfarin is not cost-‐effective, lengthens hospital stays and may be less safe36. It should be remembered that aspirin and clopidogrel also raise the risk of bleeding and dual antiplatelet therapy appears to raise the risk of bleeding to an even greater extent. Pocket haematoma is a recognised risk factor for infection. Tompkins and Henrikson37,38 provide the most comprehensive approach, however, their advice is perhaps a little complex to follow in practice. The advice by Baron et al.39,40 is a little more practical.
1. Aspirin or clopidogrel may be withheld for 5 days prior to the procedure when it has been prescribed for primary (not secondary) prevention of cardiovascular events.
2. There is generally a very good reason why patients are taking dual antiplatelet therapy. It is appropriate to review the indication, as occasionally it will have been continued inadvertently, however the default position should be that it should continue.
3. In patients with non-‐valvular AF, warfarin should be continued if the patient has had a
previous embolic event, has known atrial thrombus or has a CHADS2 score of < 4 (annual stroke risk 5.9%). Otherwise warfarin should be withheld.
4. Warfarin should be continued in patients:
a) With prosthetic valves, b) On current treatment for:
i. DVT ii. PE iii. Left atrial or ventricular thrombus. iv. Certain thrombophilias – e.g. Protein C deficiency (Discuss)
If warfarin is continued, the procedure can proceed if the INR is less than or equal to 3.0 (3.5 if the patient has a prosthetic valve). The haematologists have supported this policy. If severe bleeding occurs then octaplex or beriplex should be administered as per protocol. If this is required the event should be reported to the clinical lead and the haematologists. Operations should generally not be performed on patients taking Dabigatran, Rivaroxaban or Apixaban (New Oral Anticoagulants, NOACS). These agents are not clearly reversible. In these situations the effects of the anticoagulant wear off (and restart) more rapidly and an individual decision should be made. If it is not safe to stop anticoagulation they should be transferred onto warfarin. If the agents can be stopped then the following guidance should be followed. A pacing procedure should be regarded as high risk of bleeding. For Rivaroxaban and Apixaban it is recommended that the NOAC is stopped 48h prior to the procedure. For Dabigatran the recommended duration depends upon renal function (see below)41. Generally the NOAC can be restarted 6h after the procedure if there are no signs of bleeding, although it may be appropriate to wait until the following day.

42
For Dabigatran (Pradaxa)
Renal function (CrCl in ml/min)
Estimated half life (hours)
High risk of bleeding or major surgery
(hours) ≥80 ≈13 48
≥50-‐<80 ≈15 72 ≥30-‐<50 ≈18 96
More information can be found for Dabigatran here, Rivaroxaban here and Apixaban here
Other haematological abnormalities A contemporaneous INR and platelet count should be reviewed prior to device implantation. A platelet count of less than 100 or an INR of > 1.3 in a patient not on anticoagulant should trigger a haematological opinion. Similarly, if there are known bleeding tendencies these should be noted and discussed with the haematologists prior to the procedure. There is no indication for taking a routine group and save sample.

43
Device Selection We have a limited number of devices on the shelf. Selection should be as follows:
1. VVI PPM – Biotronik Effecta. The Medtronic Sensia is available for particularly small/thin patients.
2. DDD PPM a. Ventricular pacing all the time (CHB) – Biotronik Effecta b. SSS or need to avoid ventricular pacing – Medtronic Sensia c. Vasovagal syncope – Biotronik Evia d. Need for MRI scan in the future – Medtronic Ensura/Advisa (see here)
For ICDs we currently use Biotronik and Medtronic. Single chamber ICDs should be used preferentially due to the lower complication rates and increased device longevity42,43, unless there are documented ventricular or atrial arrhythmias or a conventional pacing indication, where an atrial lead may be beneficial for diagnostic/therapeutic purposes. Please note that when consenting patients, manufacturers estimates of longevity may not match real world experience43. For CRT-‐Ds and CRT-‐Ps we use Medtronic and occasionally St Jude devices. External subcutaneous ICDs (Cameron Health, now purchased by Boston Scientific) may be considered for younger patients (<60) with no pacing indication (ARVC, CPVT, Brugada, Idiopathic VF, LQTS). The manual for programmer use is embedded here, as are the documents relating to its approval as a new procedure and a specific leaflet for patients. We are trying to move towards a situation where all devices can be remotely monitored (there are now data to suggest mortality is reduced) and are MRI safe. This will take many years due to financial constraints. We are currently in the midst of a new tender process, and this section may need rewriting imminently.

44
Admission Checklist
• The admission to hospital must be used not only to ensure the patient is prepared for the device implant from a physical but also a psychological viewpoint.
• The operator or someone capable of performing the procedure should obtain consent
prior to arrival in the lab.
• The indications for insertion of the implantable device should be reviewed.
• Any history of recent or current infection must be noted.
• Any significant co-‐morbidity must be recorded, in particular LV impairment, respiratory disease, renal dysfunction and diabetes. Any previous anaesthetic problems should be documented.
• The MRSA/MSSA status and decolonisation regime should be reviewed and documented.
• The drug history is vital especially in relation to warfarin or NOAC, clopidogrel and aspirin
use.
• Allergies must be noted.
• Whether the patient is right or left handed must also be documented, although device implantation will generally be on the left hand side.
• Examination: the physical examination should record any signs of infection as well as the
ability to lay flat – particular attention should be paid to pain and breathing issues.
• The chest X-‐ray should be reviewed.
• Pacemaker implants will generally be performed under local anaesthesia with or without sedation. ICD implants may be performed under local anaesthesia with sedation. For elective procedures the patient should be starved of solids for 6 hours and clear fluid for 2 hours prior to receiving intravenous sedation.
• An intravenous cannula should be inserted on the ipsilateral side to the intended
pacemaker site.
• All women of childbearing age must have a pregnancy test and/or sign an LMP form.
• The chest should be clippered using an electric razor near the site of pacemaker insertion if required. The groin should also be clippered if a temporary pacing wire is required.
• The trust antimicrobial policy on prophylactic antibiotics should be followed.

45
Device Related Infections – Prevention
Introduction Device related infection is a common and difficult problem. Between 0.5-‐2%44,45 of patients experience this (higher rates with complex devices) and it is associated with higher healthcare costs and around a 5% mortality, rising if there is endocarditis46. Risk factors for infection, aside from operator experience include46-‐50:
1. Early reintervention (OR 15.04) 2. Corticosteroid use (OR 13.90) 3. Renal failure (OR 11.97) 4. CRT-‐D implantation (OR 7.57) 5. Fever < 24 hrs. prior to implant (5.83) 6. Renal insufficiency (OR 5.46) 7. Box change (OR 3.67) 8. Oral anticoagulant (OR 2.82) 9. Heart failure (OR 2.57) 10. Presence of TPW (OR 2.46) 11. Male gender (2.23)
Later this year, a comprehensive review of infection prevention and treatment will be published.
Recommendations There are a number of recommendations and guidelines as to how to reduce device related infection. There is some evidence from units that have had a spike in device-‐related infections, that a comprehensive infection control program can reduce device-‐related infections51. Our recommendations are based upon the measures outlined in that document. A good general overview of strategies to prevent surgical site infection has been written by Anderson et al. 200852. A new document has been produced by BSAC in 201453.
Pre-‐operative care
1. All patients should wash with Skinsan or Octenisan for five days prior to the procedure. The reason for such a prolonged period is to keep things simple, if additional Bactroban is required. According to NICE, patients should shower or bath (or have a bed bath) on the day of surgery where possible (NICE CG74), possibly with an antibacterial agent such as triclosan51. A Cochrane review has emphasised that there is no clear evidence for the use of antiseptics however. The IHI recommend that patients bathe/shower with chlorhexidine gluconate soap for at least three days prior to hip surgery.
2. All patients should be screened for MRSA and MSSA and should not normally undergo pacemaker implantation if positive. If positive these patients should be decolonized before the procedure. This may not be possible for emergency cases. Decolonisation for both MRSA and MSSA should take place five days before the procedure date. In addition to the Skinsan/Octenisan wash, patients are recommended to use Bactroban (Mupirocin) nasally three times per day. Note that there is clear evidence for the use of Mupirocin according to

46
a recent Cochrane review. There are standard letter for patients and GPs. More detailed management of patients with MRSA can be found here.
3. In emergency situations, decolonisation will not be possible, but in semi-‐elective situations the procedure should be delayed. It is recommended that patients who are admitted and are likely to require pacing should commence decolonisation straight away. They should be swabbed at the same time and decolonisation can stop if the swabs are negative. Ideally they should have at least 48h of decolonisation. A protocol for the screening of inpatients can be found here.
4. Screening of operators/staff may be required if:
a) Infections persist despite the measures in this document being undertaken b) If the same organisms are isolated in many different patients
We will be guided by microbiology if this is necessary.
5. Patients with open wounds which are known to be colonized, or have active infection
should not normally undergo pacemaker implantation until these issues have been resolved, unless clinically imperative.
6. Patients who have had antibiotics should not undergo implantation of a pacemaker within
30 days unless there is a pressing clinical indication51.
7. Electrical clippers with a single use head on the day of surgery should be used if hair removal is required. Razors should not be used (NICE CG74). If razors are used inadvertently the patient should be cancelled unless it is an emergency.
8. In patients with poor blood glucose control it may be reasonable to use a sliding scale perioperatively, although further research is required54. There is a good summary in Anesthesia and Analgesia55. Implantation should not normally take place if the blood sugar is >11mmol/l. Where possible the HbA1c levels should be <7% before surgery56.
9. Patients who smoke should be encouraged to stop perioperatively, preferably for at least 30 days prior to the procedure57.
10. Antibiotic prophylaxis should be used as per protocol (Teicoplanin 6mg/Kg rounded to the
nearest 100mg iv and Gentamycin 3mg/Kg iv) and within 30 minutes of the procedure. There is surprisingly little evidence for this, although what is there is clear that antibiotics are better than no antibiotics35,58 and the use is supported by a now withdrawn Cochrane review. A recently performed survey by Jonathan Sandoe showed that the practice across the UK is highly variable59.
11. There is also no clear evidence on whether antibiotics should be given into the pocket.
Povidone-‐iodine irrigation of the pocket does not appear to help60. An antibacterial envelope may do24,61, but we do not routinely use these.

47
Intra-‐operative care
1. There is little evidence to suggest that putting devices in in operating theatres is safer than putting devices in in catheter laboratories62. There are standards for ventilation for health care facilities63. These specify minimum recommended standards for air changes, humidity and temperature. We have had recommendations from the health protection agency that there should be a minimum of 10 air changes per hour in each lab, preferably 18-‐20. We appear to have a greater number of air changes in our labs (see link). There is also general information for the specification of labs for diagnostic imaging (HBN 6) and more general guidance on ventilation (HTM 03-‐01).
2. There should be minimal movement of staff into and out of the theatre (NICE CG74).
3. Scrubbing with chlorhexidine, rather than povidone-‐iodine is recommended for 5 minutes prior to the procedure. There is some evidence that new alcohol-‐based scrubs may be more effective. The no-‐touch technique should be used when gowning and gloving. The guidance can be found in a Cochrane review. If the operator is allergic to chlorhexidine, then until the alcohol-‐based scrubs are available, then povidone-‐iodine with alcohol should be used.
4. Staff should wear hats and masks. It is accepted that there is little evidence for this practice. Hats and masks should not be re-‐used.
5. The surgical safety checklist should be performed. See below.
6. Oxygen saturations should be maintained above 95% (NICE CG74).
7. Maintaining patient normothermia is important; hypothermia appears to be an important
risk factor for surgical site infection (NICE CG74).
8. A venogram should only be used where access problems are felt likely to be an issue. A venogram should be performed where new leads are to be inserted and there is a pre-‐existing device. Of note the cephalic vein should be used where possible to minimise the risk of pneumothorax. An ultrasound probe should be available to facilitate axillary vein access.
9. The instruments should be inspected prior to use. Any which appear to have rust on them
should be discarded as per advice from infection control. They should be sent back to CSSD for de-‐rusting and re-‐sterilisation.
10. The skin should be prepared using chlorhexidine rather than povidone-‐iodine, unless there
is a documented allergy64 (Also NICE CG74). We use Chloroprep. The applicator should be applied over the area to be incised in a gentle back and forth manner for 30 seconds, before wider painting of the surgical field is undertaken. There is some evidence that this is better than a circular method of applying the antiseptic. The skin should be allowed to dry naturally and completely before applying the drape. If the operator is allergic to chlorhexidine, then until alcohol-‐based scrubs are available, povidone-‐iodine should be used. The povidone-‐iodine preparation should contain alcohol (See IHI how-‐to guide:

48
prevent surgical site infection for hip and knee arthroplasty). Some advocate combining iodine and chlorhexidine65,66.
11. There are also some limited data that Integuseal reduces contamination of wounds67 but
we do not routinely use this.
12. Drapes, which adhere to the wound itself, should generally not be used68, although an Ioban drape may be considered.
13. Operators who have performed less than 50 procedures should not perform box changes. 14. Diathermy use should be minimised (NICE CG74).
15. There are some data to suggest that monofilaments are superior to braided sutures69 and
if braided sutures are to be used then antimicrobial coated sutures are beneficial70. After a trial of ethibond (a braided synthetic suture) due to the difficulty of adequately securing leads, we now use Vicryl Plus (2-‐0, 31mm 1/2c round bodied needle, 70cm), an antiseptic coated version of Vicryl.
16. Anecdotally we have noticed that using Surgicel has been associated with infection. This may simply be an association rather than a causal link, but for the time being use of this should be avoided if at all possible, although it may still have a role if there is excess bleeding.
17. It is unclear whether gentamicin given into the pocket reduces infection and this is not
recommended.
18. There is no evidence that tissue adhesives are superior to sutures for closing the skin layer71, but they may be used for convenience. Liquiband should not be used, as it does not have the tensile strength, rather Liquiband flex is most appropriate.
Post-‐operative care
1. Lead coats should be washed between procedures. Shoes should be washed daily.
2. It is unclear whether post-‐operative antibiotics need to be given. It is common practice in many units and we have made it standard practice. Many studies, which have examined the role of antibiotic use in preventing pacemaker-‐related infection, have used post-‐operative antibiotics72-‐74. There is some logic to giving antibiotics for 48 hours to allow the skin to heal, but longer courses do not appear beneficial75. We no longer routinely give post-‐operative antibiotics.
3. There is very little evidence-‐based advice for washing after pacemaker insertion.
Dermabond can be wetted on the evening after surgery, but should not be soaked or scrubbed. For skin wounds closed with nylon the wound can be washed the following day76, and this is in line with other studies77. We have advised, after consultation with infection control, that wounds not covered with tissue adhesive should be covered for two days and can be washed on the third day.

49
The WHO Surgical Safety Checklist A modified surgical safety checklist has been devised. This should be performed for every procedure and the document placed in the patients’ notes. This is a must do. There are good reasons why we should do this which are beyond the scope of this guideline. Further information on the rationale behind this and videos of how to perform (and not perform) the surgical safety checklist can be found here and here.

50
Monitoring of the Patient During the Procedure The patient should be monitored during the procedure:
1. The welfare of the patient should be checked on a regular basis
2. Oxygen saturations and respiratory rate should be monitored continuously
3. Blood pressure should be measured every 10 minutes, unless directed to repeat more often
4. If sedation is given, then oxygen is likely to be necessary and a mask should be applied
prior to draping the patient.
5. Blood glucose levels should be monitored as appropriate.

51
Temporary Pacing Temporary pacing is to be avoided. Generally speaking a femoral approach to temporary pacing should be recommended. An internal jugular approach may be used, but an ultrasound probe should be used to help locate the vein (NICE -‐ TA49). A 5F lead is to be preferred and the sheath should be withdrawn at the end of the procedure unless there is concern over bleeding or unless an oversized sheath has been inserted to permit central access. Please note that following a death due to MRSA septicaemia, antibiotics should be commenced at the time of implantation (Teicoplanin + Gentamycin) as per microbiological protocols until the time of pacing wire removal or implantation of a new system; the presence of a temporary pacing wire is a recognised risk factor for infection of the new system. Because of the risk of infection, the general aim should be to insert a permanent system on the next available list, unless it is thought that the wire will only be required briefly. A temporary pacing wire is not recommended where a box change is to be performed and there is no evidence of an underlying rhythm. Sedation should be given and external pacing pads applied. There is evidence that the insertion of a temporary wire increases the risk of device-‐related infection and the procedure itself is not without complication. Updated guidelines are available here.

52
Contrast Media Use The trust-‐wide policy should be adhered to. Careful use of fluids is required in many patients however, and therefore a case-‐by-‐case assessment will be required.

53
Analgesia and Sedation Sedation should be offered to patients if required. Currently we tend to use morphine and midazolam, however, outside of cardiology there is an increasing tendency to use of fentanyl (25mcg of fentanyl is equivalent to 2.5mg morphine). Fentanyl tends to induce less nausea and itching compared with morphine but may not be as good at controlling pain, and therefore it may not be sensible to change practice78. The safe sedation policy should be adhered to. There are a number of important points:
• In accordance with the guidelines for general anaesthesia, for elective procedures, patients should be starved of solids for six hours and clear fluid (this includes coffee or tea with skimmed milk) for two hours prior to receiving intravenous sedation.
• No more than 10mg of midazolam should be given – if more is required the assistance of an anaesthetist should be sought.
• If as a consequence of sedation it proves difficult to rouse the patient the assistance of an anaesthetist should be sought.

54
Surgical Technique Be aware of the correct scrubbing technique and use a closed glove technique. It is recommended that the previous operation note is read prior to any revision. In the NICE clinical guideline on the prevention of surgical site infection, incise drapes are not routinely recommended. Non-‐iodophor drapes have been associated with increased rates of infection. Iodophor impregnated drapes should not be used with chlorhexidine – and chlorhexidine has been shown to reduce the rates of infection. With regards to local anaesthetic, bupivacaine lasts for considerably longer than lignocaine, but less can be given: Bupivacaine: 2mg/kg 1%, 10mg/ml, 14mls for 70Kg man typically Lignocaine: 3mg/kg 1%, 10mg/ml, 21mls for 70Kg man typically Lignocaine with adrenaline: 7mg/kg 1%, 10mg/ml 49mls for 70Kg man typically We have an intralipid policy in the case of overdose. If possible the old scar should be excised, but this may not be possible if there has been considerable migration of the device, and may be more challenging if diathermy/plasmablade is not available. A marker pen can help to ensure a good cosmetic result. Toothed forceps are less damaging to the skin than non-‐toothed forceps. We are continuing to use silk to secure the leads, having trialled ethibond. The device should not be under the suture line and the pocket should be enlarged if this is the case. Currently I use a combination of subcutaneous antibiotic coated Vicryl and Liquiband flex to close the wound. The topical cyanoacrylate material does not conclusively reduce wound infection, but is convenient for patients. There are a number of different closure techniques, and there is a good argument for using monofilament sutures. Interrupted sutures requiring removal are not recommended except in the case of wound infection.

55
Lead Selection Lead selection is at the discretion of the operator. Active fix atrial leads should generally be used in patients who have undergone cardiac surgery. There is evidence that straight screw-‐in atrial leads offer better stability79,80. J-‐shaped atrial leads with an active fix mechanism should not usually be implanted as they have an unacceptably high rate of perforation81. Active fix ventricular leads of 7F or less should generally not be implanted at the right ventricular apex. They should not be advanced with the stylet fully in. At present there is no conclusive evidence that septal pacing is superior to right ventricular apical pacing, and therefore this should be left to the discretion of the operator. Harry Mond has produced a cogent argument as to why we should pace separately and guides on how to do it correctly82. St Jude produces the ‘Mond’ stylet for pacing in the RVOT. Generally speaking, single coil ICD leads should be selected ahead of dual coil leads. In practice there is minimal difference in the defibrillation threshold when formally tested83, and anecdotally device extraction is more straightforward with a single coil, minimising adhesions in the SVC where tears can often occur.

56
Screening
HCAs and Screening We have successfully trained a number of HCAs to undertake screening for any procedures performed in the pacing lab. The documentation can be found here.
Screening at the End of the Procedure It is unacceptable to leave any equipment in a patient and such an event can result in significant penalties for the trust. It is imperative to account for all equipment at the end of the procedure and screening should be performed to ensure that no equipment has been left in the patient including wires, needles or swabs. Only radio-‐opaque swabs should be used.
Skin dose During occasional procedures there will be concern over the total radiation dose to the patient. The policy can be found here.

57
Post Implant Care
Patient problem/need
Aims of Care Actions
Potential risk of bleeding from wound site Risk of vasovagal event
To prevent bleeding Early identification of problems
1. May sit up immediately with assistance. 2. May mobilise when effects of sedation have worn off and patient able. 3. Observe and record BP, heart rate, O2 saturations, PAR score, sedation score every 15mins for 1hr then every 30min for 1hr then hourly for 4hrs then every 4 hrs. 4. Observe wound site for bleeding/discharge swelling as above. 5. If bleeding or severe swelling occurs inform a doctor and apply direct manual pressure for at least 10 minutes or until bleeding ceases. It is then appropriate to apply a pressure dressing for 4 hours.
Risk of pneumothorax
Observe for signs -‐ Shortness of breath -‐ Difficulty in breathing -‐ Reduced oxygen saturations -‐ Chest pain
1. Monitor O2 saturations as above. 2. CXR 4 hrs. Post implant for all new systems or sooner if operator directs.
For box change with TPW
To prevent bleeding from leg Early identification of problems
1. Haemostasis should be achieved in the pacing room by manual pressure. 2. Patient should lie flat for 1hr, then sit for 1hr then mobilise. 3. Observe puncture site for bleeding/swelling when recording observations. 4. If bleeding or swelling occurs apply direct pressure for 10 minutes, or until bleeding ceases.
Hydration and nutritional needs To maintain needs
1. May eat or drink on return to ward depending on sedation levels. 2. Encourage oral fluids.
Potential risk of lead displacement.
To reduce the risk of lead displacement To identify lead displacement
1. Patient must not elevate the arm on implant side above shoulder level for 1 month (N/A for box change). 2. Observe for signs of displacement -‐ change in BP, heart rate. Obtain 12 lead ECG. 3. Contact pacing technicians on ext. 2360 for device check. 4. Arrange chest X-‐ray. 5. Contact implanting Dr if lead displacement has occurred.
Pain from wound site To alleviate/reduce to an acceptable level for the patient
1.Assess pain level frequently. Use verbal/non-‐verbal /vital signs. Commence pain chart where appropriate. 2. Offer regular analgesia, monitor and record effect. 3. Assist to comfortable position. 4. Encourage diversional activities where applicable.
Healing of wound To promote healing without complications
1. Manage the wound aseptically. 2. Remove dressing after 2 days unless directed otherwise. 3. Explain to the patient that they can wash it after 3 days. 3. Arrange appointment in Day Case for suture removal if required.
Educational, Psychological, Social and Spiritual needs
To reduce anxiety, promote return to normal activities.
1. Allow patient time to discuss anxieties and fears. 2. Ensure patient has appropriate literature and post care advice 3. Contact BHF Arrhythmia nurses if patient requires further support.

58
Pacing Check and Chest X-‐ray Post Procedure These should be done 4 hours after the procedure and should be documented in the notes. The operator should generally review the chest X-‐ray. The patient should also be reviewed by the operator at this stage and may then be discharged if appropriate. The chest X-‐ray should be checked for:
1. The presence of a pneumothorax or haemothorax or other complication.
2. The position of the leads.
3. That the leads have been fully inserted into the box.
4. That there are no retained items.

59
Post-‐operative Wound Care We have reviewed the advice we give to patients about their wounds and it is now in the pacing leaflet. It bears repeating here: Advise the patient that if they develop a temperature, or the wound becomes red or inflamed, they should contact the pacemaker clinic promptly or the cardiac day unit or coronary care. If glue has been used to close the wound please ensure that it is left uncovered. Advise the patient that the glue will start to flake off after 7 days. They can shower on the same evening of the procedure but should not soak the area; the area should be patted dry with a clean towel. If there is a dressing covering the wound site it should be removed after 2 days and the wound left uncovered. The wound should be kept clean and dry for 3 days after the procedure. The patient can then shower normally and pat the area dry with a clean towel. If there are dissolvable sutures closing the wound the sutures will dissolve and no further action is needed. If there are non-‐dissolvable sutures then the patient should be given an appointment to come back to the Cardiac Day Unit to have them removed, usually 7 days after the procedure.

60
ICD Testing and VT Stimulation
ICD Testing Routine DFT testing should not be undertaken. Nonetheless, the risk of complications appears low84,85, and even relatively recent reviews have recommended the practice continue86. More recent data have called into question its value87-‐92 and there are increasing calls to stop this practice. The SIMPLE trial has now been presented (at HRS 2014) and reported online, but the full paper has not yet been published. This trial randomised 2500 patients to DFT testing or not. There was a signal of harm from DFT testing, although mortality was not affected. It remains reasonable to test patients with:
1. A right sided implant 2. Where there are potential issues with the functioning of the device (e.g. a low R wave) 3. After device revision for failure to defibrillate 4. Very dilated left ventricles (>7.0cm) – this is a local recommendation and reflects the fact
that we have had a number of DFT failures in patients with such large ventricles. This policy may require revision once the SIMPLE trial has been published. We have a separate proforma for DFT testing. If patients have atrial fibrillation they should have an INR of > 2.0 for 3 weeks prior to DFT testing. They may be DFT tested on Dabigatran or Apixaban. DFT testing should not take place if the patient is on Rivaroxaban, at present. If patients have left ventricular thrombus they should have an echo to demonstrate that it has resolved prior to DFT testing. Other reasons for not testing include: known untreated severe coronary artery disease and patient preference. We have a document that is sent out to patients prior to their admission.
VT Stimulation There are very few indications for a VT stimulation study. The protocol is as follows:
1. Drive train 600ms, 1 extrastimulus from 400ms down in 20ms intervals to refractory, then a second extrastimulus down to refractory.
2. Drive train 500ms, as above. 3. One site only – RV apex or RVOT.

61
Complications and Audit Complications are an important issue relating to permanent pacemaker implantation. Surprisingly there are no generally accepted norms of complication rates in pacemaker surgery93. We are a centre that offers experience to first and second year registrars, and it can be expected that we will have a higher rate of complications and procedures will take longer94. Out long-‐term complication rate has been published95. More recently our complication rate has been falling. This is probably because we now have fewer operators and we are supervising each registrar-‐led implant. This practice should continue. All complications should be reviewed, and any serious complications should be the subject of a root cause analysis. Complications will be reported to HR-‐UK from April 2014. There are a number of standards laid down by HR-‐UK, although whether these are representative of real-‐world complications is debatable.
1. Each centre must maintain a database of implants and complications within 12 months for pneumothorax and requiring re-‐intervention. This is currently maintained on CVIS. Monthly uploads to CCAD should be undertaken no more than 3 months in arrears.
2. Standards for complications have been defined by HR-‐UK. Kirkfeldt et al. have recently published overall complication rates in Denmark. Complication risk depends on case mix and more complex procedures carry a higher complication rate.
HR-‐UK Kirkfeldt 201496
a. Ventricular lead displacement 1.0% 2.4% (All leads) b. Atrial lead displacement 2.0% c. Pneumothorax 1.3% 0.9% (Requiring drainage) d. Perforation 0.4% 0.6% e. Infection 0.6% 0.8%
3. Immediate anaesthetic support should be available for ICD implantation. We can say that
we have this, in that we can fast-‐bleep the on-‐call anaesthetic team. It is explicitly stated that if an implanters complications exceed these limits then practice should be reviewed and advice sought from within the centre or elsewhere. All complications must be reported to the device lead. The national audits can be found here.

62
Device Related Infections – Management Any patient with a suspected device related infection should be admitted immediately. The infection should be reported to the clinical lead. Blood cultures should be taken and echocardiography arranged. Antibiotics should be commenced after discussion with the microbiologists, but should include both gram positive and negative cover. Vancomycin and Gentamycin are appropriate until organisms and sensitivities are known. Please see the pie chart below for details on the typical microbiology with device related infections47. In the vast majority of cases device extraction should be considered. This should be performed as soon as is practicable – typically on the next list.
The AHA have released guidelines for the management of device related infection97. I have included specific references on outcomes98 and Staphylococcus aureus99. These guidelines say:
• CIED removal is not required for superficial or incisional infection at the pocket site if there is no involvement of the device. Seven to 10 days of antibiotic therapy with an oral agent with activity against staphylococci is reasonable.
• Complete removal of all hardware, regardless of location (subcutaneous, transvenous, or epicardial), is the recommended treatment for patients with established CIED infection.
The guidelines include a number of pathways to guide management, which should be followed. UK guidelines will be released later this year.
Coagulase negative
staphylococci42%
MSSA25%
MRSA4%
Other G+ve cocci
4%
G-ve bacilli9%
Polymicrobial7%
Fungal2%
Culture negative
7%
Microbiology of Device InfectionsSohail et al. 200720

63
Lead Extraction Leads and systems should only be extracted if they are less than 1 year old. All other patients should be referred to Bristol or Harefield for device extraction. I have included references to articles for patients100 and the formal guidelines101.

64
Pneumothorax and Haemothorax
The pneumothorax rate in our centre is too high. The cephalic route should be used preferentially. The axillary vein is an alternative. All pneumothoraxes should be reported to the clinical lead. The management of pneumothoraxes are detailed in the trust guidelines for the management of pneumothorax and chest drain insertion; these should be referred to. Essentially if a small pneumothorax (<2cm) is noted and the patient is asymptomatic then the patient should have a chest X-‐ray the following day. Assuming the pneumothorax is no larger the patient should be brought back to the day unit in 1 week for a repeat film. If the pneumothorax is >2cm then it may be aspirated once in patients without underlying chest disease. If the pneumothorax remains then a chest drain should be inserted. Of note, it is clinically more appropriate to follow the non-‐trauma pathway despite the aetiology. The respiratory team are very helpful.

65
Follow-‐up Standards The Heart Rhythm Society and European heart rhythm association have suggested follow-‐up standards102, as have Heart Rhythm UK. Arrangements for 24-‐hour cover should be in place for all device patients. This is particularly important for ICD patients where device-‐related and arrhythmic complications occur frequently and can be life-‐threatening. Follow-‐up should be performed at nationally accepted intervals:
1. Within 2 months of implantation.
2. 6-‐12 monthly for bradycardia pacing.
3. 3-‐6 monthly for CRT and ICD therapy.
4. Patients should have urgent follow up if they report symptoms that may be associated with device malfunction, or if a shock has been delivered.
Remote monitoring of devices should be encouraged and should now be the standard of care. Currently HR-‐UK feels that yearly face-‐to-‐face follow-‐up is required even if remote monitoring is in place. This is currently being reviewed by HR-‐UK. Clinic follow-‐up should include:
1. Wound review.
2. Device checks – battery, lead impedance, pacing thresholds, sensitivity. Any important changes or findings should be discussed with a consultant. The rate response behaviour should be assessed by examining the heart rate histograms, and if necessary by simple exercise testing, and adjusted appropriately
3. Recorded patient rhythm data a. Episodes of possible atrial fibrillation should be recorded and the GP notified (see
below). b. Episodes of ventricular arrhythmias should be recorded and the appropriate
consultant should be notified.
4. For CRT patients record should be made of % ventricular pacing. If the value falls below 95% the appropriate consultant should be notified.

66
Vitatron and Biatrial Generator Replacement Advice
Vitatron Pacemakers We have a specific document detailing when to replace Vitatron pacemakers.
Biatrial Pacemakers We have a small number of patients with biatrial devices in situ. Biatrial devices are no longer manufactured and therefore a like-‐for-‐like box change cannot take place. Some patients may not need a pacemaker. The first question is whether the patient remains in sinus rhythm or not. If they are in sinus rhythm the next question is whether atrial pacing alone can continue to suppress atrial fibrillation. Therefore it is reasonable to try for one month with no atrial pacing (DDI 40), left atrial pacing and right atrial pacing in turn. If there is clear benefit for one of the pacing modes then it is reasonable to change the device. Although it is thought that atrial pacing is ineffective in preventing atrial fibrillation, this is clearly not the case for some individuals. If the patient is in chronic atrial fibrillation then the device should be turned down to VVI 40 if not already done so to determine the need for backup ventricular pacing. If there is a need then it is reasonable to change the device for a Talos SR.
Atrial Defibrillators We have a very small number of patients with atrial defibrillators. Decisions should be made on an individual patient basis when device change is required.

67
Atrial Fibrillation Atrial high rates are frequently detected at follow-‐up. Episodes may be brief or prolonged, and may or may not be associated with symptoms. Atrial fibrillation is recognised as increasing the risk of stroke and it important to ensure that patients take antiplatelets or anticoagulants depending on underlying risk factors. There is no consensus, however, as to how much atrial fibrillation, as detected by device diagnostics, is significant. The literature103,104 suggests that device detected atrial fibrillation is a significant risk factor for stroke. We have constructed a sample letter to send to GPs.

68
Ventricular Tachycardia Ventricular tachycardia (VT) is frequently detected by CIEDs. In a recent study 1 in 4 patients with at least one follow-‐up had non-‐sustained VT (NSVT) documented105. The prognostic significance is uncertain, but an abstract at HRS in 2012 by Seth et al. suggested that it is a benign finding and that beta-‐blockers have no impact on survival. It is difficult to know what to do with such findings and management depends on patient characteristics and symptoms. The finding of NSVT should prompt a clinical review of the case. Most patients do not have a history of ischaemic heart disease or impaired left ventricular function and are asymptomatic. A beta-‐blocker may be considered if there are associated symptoms of concern to the patient. An ICD may be considered in those patients with significant left ventricular impairment or syncope. In patients with a CRT-‐pacemaker, VT lasting for >64 beats with a ventricular rate of >150bpm, was associated with a poor outcome106, although the incidence of such arrhythmias was low. Revascularisation may be considered in those with significant angina.

69
Electromagnetic Interference and Other Environmental Issues Pacemakers are affected by electromagnetic fields, although they are increasingly shielded from their effects. A number of companies have produced specific documentation, which I have collected, but for copyright reasons cannot include in this document. The companies are usually happy to provide specific advice and guidance, and some companies, such as Medtronic, will perform site visits. St Jude provides specific information on pressure testing and their devices may be more appropriate for those who wish to continue diving. We have had some specific guidance from Medtronic on the use of cochlear implants and CRT-‐D devices. A distance of 6” (15cm) should be maintained between the cochlear implant and CRT-‐D. The implant will not damage the device; if the device detects the magnet in the implant it will alarm. In this situation the person with the implant should move away from the person with the device.

70
Device Deactivation Device deactivation is often performed too late. The final decision should always rest with the patient as long as they remain competent to make the decision, however illogical their views may appear to be. The subject should be raised prior to implantation, as this issue is likely to arise at some stage. A surprising number of patients do not believe that they can die with an ICD in situ. There has been a useful discussion article in BMJ palliative care107 and also by Grubb and Karabin108. The Heart Rhythm Society and European Heart Rhythm Association have released a consensus statement109. We have produced our own guidance. The Arrhythmia Alliance has produced a useful booklet. I have included a link to Bristol’s guidance.

71
MRI compatible devices A wide variety of devices are now MRI compatible. Some ICDs are now MRI compatible. If a patient requires an MRI advice should be sought from the cardiac physiologists. The restrictions vary between companies and devices, and therefore no specific guidance can be given. Although not used in the UK widely, protocols exist for the safe MRI scanning of non-‐MRI compatible devices. At present we do not undertake such scans at Musgrove.

72
Pacemakers and Radiotherapy There is a theoretical risk that radiotherapy can damage permanent pacemakers if the pacemaker is in the line of the beam. Occasionally the presence of a pacemaker will shield the area that is targeted. In such situations it may be reasonable to move the pacemaker and close collaboration with the radiotherapists is required. A number of companies have produced guidelines around how much radiation their pacemakers can receive before they are likely to malfunction and these should be referred to. I have copies of these documents. Makkar et al have proposed a protocol for the management of CIEDs in this context.110 The following figures are based upon their recommendations.
Figure 2 – The management of CIEDs prior to radiotherapy
Before Radiotherapy
Course
Oncology
Proximity of device to radiation target,
in cm
Estimate of radiation dose
Cardiology
Device details
Device implant indication
Complete device interrogation
Pacing dependent?
Review of manufacturers guidance

73
Figure 3 – the management of CIEDs during and after radiotherapy
During radiotherapy (RT)
Surgical relocation of device if beam < 2.5cm from the implant unless clinical situation precludes
Oncology
Ensure device is not within beam
Avoid high energy (>10MV) beams
Avoid beam modiUiers
Cardiology
Turn on audible alerts for device malfunction
Pacemaker
Patients receiving less than device speciUic limit (if available) or 2Gy (if not available): Device
evaluation at end of RT
Patients receiving more than limit require baseline and weekly evaluation
ICD
Baseline and weekly evaluation
If unable to relocate device then pre and post device interrogation should be performed with each RT
session

74
Pacemakers and Diathermy The following algorithm is based upon the PACED-‐OP protocol111. The guideline is evidence based and reduces the need for device reprogramming with no evidence of harm. Diathermy, particularly monopolar diathermy, has the capacity to interfere with pacemaker function, potentially leading to failure to pace, or an inappropriate shock from an ICD, or inadvertent device reprogramming. However, many of these reports are based upon the observation of older devices that were more prone to electromagnetic interference. The two following figures detail the management of devices. The first figure details the management of the “pacing” function of pacemakers AND ICDs. The second figure details the management of the “shock” function of ICDs. The old protocol for managing pacemakers and ICDs in the context of diathermy can be found here. A slide set is available on request. MHRA guidance is also relevant.

75
Figure 4 – The management of the “pacing” function of pacemakers AND ICDs.
Electromagnetic interference (EMI)
expected?
No
No intervention
Yes
Pacing dependent? (deUined as paced rhythm on pre-‐op
ECG)
No
No intervention. If bradycardic post surgery interrogate
device
Yes
EMI between mandible and xiphoid?
No
No reprogramming pre-‐op ECG post-‐op
If bradycardic then interrogate device
Yes
Program VOO pre-‐op and then re-‐program post-‐op (prior to leaving recovery)

76
Figure 5 – The management of the “shock” function of ICDs
Electromagnetic interference (EMI)
expected?
No
No intervention
Yes
EMI between mandible and xiphoid?
No
Magnet over device during procedure*
*Unless particular Boston/Guidant model [H170, H173, H175, H177, H179, H230, H235, H239] – in which case program therapy off pre-‐op and on post-‐op. DO NOT USE
MAGNET
Yes
Program therapy off pre-‐op and on post-‐op

77
Optivol alerts Currently as we receive the data we cannot ignore it. Optivol rises can signify impending heart failure decompensation or an increased likelihood of shocks and therefore someone needs to check on the patient. At present the cardiac physiologist should phone the patient or contact the heart failure specialist nurses. If they are feeling more unwell they should be advised to visit their GP. We have prepared a standard letter. Further details can be found here.

78
Driving The DVLA at a glance guide should be used to determine eligibility for driving. This document as it is subject to frequent review and the online site should always be checked. Of note, this guide should be referred to after ATP or an ICD shock, irrespective of whether it is symptomatic or not, or appropriate or inappropriate. Of note, after pacemaker implant the legal advice is not to drive for 1 week, unless there is an underlying condition which requires control for longer – for example sick sinus syndrome with syncope requires “control” for 4 weeks before driving can resume. Please note that the guidelines relating to HGVs are different.

79
MDA/MHRA Alerts The MHRA website should be checked on a monthly basis for relevant alerts. Particular alerts of current relevance include:
1. Cameron Health subcutaneous ICD. There is a current medical device alert for the Cameron Health subcutaneous ICD These models are no longer in circulation and the advisory does not apply to the current model. We have three patients Cameron health devices in; none are affected by this alert.
2. Sprint Fidelis Leads. Please note that the recommendation from Medtronic is that leads
with problems should be replaced with an ICD lead rather than a new pace-‐sense lead if possible. It is imperative that certain programming changes are applied. It is recommended that lead replacement is undertaken when a box change is performed.
3. St Jude ICD leads. See below. I suspect this guidance will change over time.
4. Inappropriate ERI in certain Medtronic pacemakers.
5. Magnet instability and inappropriate battery readings in certain Sorin pacemakers.
6. Header issues on certain Boston ICDs implanted subpectorally.
7. PhD feature when applied in certain Sorin ICDs may inhibit pacing.
8. Sorin Isoline ICD leads. In 0.222% of leads an internal insulation breach was found under the shock coils. There have been no deaths reported. The leads should not be implanted (not an issue at Musgrove). There is no indication to replace the lead prophylactically. All patients should be monitored 3 monthly (which is our standard practice). There are particular programming issues that should be addressed.

80
St Jude Riata Leads – Further Details A total of 16 of the Silicone Riata models have been implanted in Musgrove Park between 2004 & 2008; the Riata / Durata Optim models (50% silicone & 50% Polyurethane) were mainly used 2008 onwards and are not affected.
Introduction In certain St Jude leads there is a risk of premature erosion of the insulation around the conductors. The precise clinical significance of this problem has yet to be defined. The two leads affected are the Riata 8F leads (1500 series) and the Riata ST 7F leads (7000 series). The rates of externalised conductors seen on fluoroscopy are around 17.9% at 4.9 years in the 8F leads and 9.4% at 4.8 years in the 7F leads. There is little correlation between the presence of externalised conductors and electrical faults. The rate of electrical faults appears to be around 1-‐2%. High energy shorting leading to an ineffective shock has occurred as a result of erosions in the pocket or around the SVC coil. It has been hypothesised that the presence of externalised conductors may predispose to thrombus formation or electrical irritation of the heart but there are no data to support this. It is important to remember that looking back at the history of device implants there has been a tendency to over-‐react to problems that have been identified and intervention on patients carries definite risk. Please see the following websites for more detailed information: MHRA FDA St Jude Riata Lead Communication
Notes 1. All patients should be informed that they have a lead under advisory. There is no need for
immediate action but increased vigilance is necessary.
2. All patients should have their device settings changed as per St Jude recommendations. 3. There are a number of points relating to this:
I. It is important to determine high voltage lead impedance (HVLI) on a six-‐monthly basis. This requires a small shock (10V) to be delivered down the leads in patients who have Atlas or older devices, and therefore can only be done at a clinic visit. Patients should be warned about this, as it will surprise them the first time it is done.
II. It is particularly important to look for far-‐field HV noise coil using an unused EGM channel.
III. It is sensible to narrow the alarm windows for lead impedances to tighter tolerances than recommended on riatacommunication.com -‐ the HVLI upper and lower limits

81
should be set between 10-‐15 Ohms above and below the settled impedance rate. This may increase the number of false alarms but detection of early problems may be enhanced.
IV. The SVC coil should be programmed off to minimise the risk of a short circuit at the time of defibrillation, although there are only a few cases of this fault reported. It is reasonable to offer a DFT subsequently, although the real world impact is likely to be minimal, and it some patients it may be felt that the risks outweigh the benefits.
V. Detection times in the VT/VF zones should be extended to minimise the risk of inappropriate shocks.
4. All patients should be offered remote monitoring with monthly checks.
5. Patients should be seen in person every 6 months, or 3 monthly if remote monitoring is not available. Of note, when seen in person provocative testing (such as shoulder/arm movements) should be undertaken.
6. Patients with electrical issues should be offered lead replacement +/-‐ lead extraction. 7. In keeping with American guidelines all patients should be offered fluoroscopic imaging of
their leads. This should focus on the RV lead in the right atrium. Views should be obtained in RAO (45O), AP and LAO (45O) views. Criteria for determining if there are externalised conductors can be found here. Chest X-‐rays are not an appropriate imaging modality.
8. It may be reasonable to offer yearly fluoroscopic screening if patients wish. This may permit us
to understand better the evolution of externalised conductors but clearly has ethical and financial issues and requires careful discussion with the patient.
9. The clinical significance of externalised conductors visualised on fluoroscopy or at box change
is not clear. The presence of externalised conductors does not mandate lead change, but some patients may opt for this after discussion of the risks and benefits. Electrical abnormalities are not more common in these leads and electrical abnormalities may occur with no obvious lead disruption.
10. Prior to box change fluoroscopic screening of the leads should take place. The identification of
externalised conductors should prompt a discussion of the risks and benefits of lead insertion +/-‐ extraction prior to any procedure.
11. Prior to box change it is sensible to perform a DFT test. Patients do not need to be put into VF
but can have a QRS-‐synchronised shock. The shock should be at least 20J. This can sometimes reveal electrical problems with the lead.
12. Prior to box change a venogram should be performed as lead issues may be revealed in the
pocket and it may be appropriate to reschedule the procedure if the operator is not skilled in extraction / venoplasty and it has been agreed with the patient that a lead change will take place if externalised conductors are found.
13. All lead issues must be reported to both the MHRA and St Jude.

82
Accufix leads The Telectronics Accufix and Encor leads have a retained stylet – in some situations that has eroded through the lead and perforated the atrium. We should maintain a list of such patients and it is important that they attend for regular screening of their leads. Generally 6 monthly screening is recommended. Further details can be found at here.

83
References 1. Levine SA, Miller H, Penton GB. Some clinical features of complete heart block. Circulation 1956;13:801-‐24. 2. Fox KA, Poole-‐Wilson PA, Henderson RA, et al. Interventional versus conservative treatment for patients with unstable angina or non-‐ST-‐elevation myocardial infarction: the British Heart Foundation RITA 3 randomised trial. Randomized Intervention Trial of unstable Angina. Lancet 2002;360:743-‐51. 3. Gazes PC, Mobley EM, Jr., Faris HM, Jr., Duncan RC, Humphries GB. Preinfarctional (unstable) angina-‐-‐a prospective study-‐-‐ten year follow-‐up. Prognostic significance of electrocardiographic changes. Circulation 1973;48:331-‐7. 4. Coumbe AG, Naksuk N, Newell MC, Somasundaram PE, Benditt DG, Adabag S. Long-‐term follow-‐up of older patients with Mobitz type I second degree atrioventricular block. Heart 2013;99:334-‐8. 5. Garratt CJ, Elliott P, Behr E, et al. Heart Rhythm UK position statement on clinical indications for implantable cardioverter defibrillators in adult patients with familial sudden cardiac death syndromes. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2010;12:1156-‐75. 6. Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-‐Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation 2008;117:e350-‐408. 7. Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Journal of the American College of Cardiology 2011;58:e212-‐60. 8. Hess PL, Laird A, Edwards R, et al. Survival benefit of primary prevention implantable cardioverter-‐defibrillator therapy after myocardial infarction: Does time to implant matter? A meta-‐analysis using patient-‐level data from 4 clinical trials. Heart Rhythm 2013;10:828-‐35. 9. Rautaharju PM, Surawicz B, Gettes LS, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. Journal of the American College of Cardiology 2009;53:982-‐91. 10. Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 2005;111:659-‐70. 11. Marcus FI, McKenna WJ, Sherrill D, et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation 2010;121:1533-‐41. 12. Schuller JL, Zipse M, Crawford T, et al. Implantable cardioverter defibrillator therapy in patients with cardiac sarcoidosis. Journal of cardiovascular electrophysiology 2012;23:925-‐9.

84
13. Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet 2013;381:242-‐55. 14. O'Mahony C, Tome-‐Esteban M, Lambiase PD, et al. A validation study of the 2003 American College of Cardiology/European Society of Cardiology and 2011 American College of Cardiology Foundation/American Heart Association risk stratification and treatment algorithms for sudden cardiac death in patients with hypertrophic cardiomyopathy. Heart 2013. 15. Hyde JA, Darouiche RO, Costerton JW. Strategies for prophylaxis against prosthetic valve endocarditis: a review article. J Heart Valve Dis 1998;7:316-‐26. 16. Dickstein K, Vardas PE, Auricchio A, et al. 2010 Focused Update of ESC Guidelines on device therapy in heart failure: an update of the 2008 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure and the 2007 ESC guidelines for cardiac and resynchronization therapy. Developed with the special contribution of the Heart Failure Association and the European Heart Rhythm Association. European heart journal 2010;31:2677-‐87. 17. Kutyifa V, Zareba W, McNitt S, et al. Left ventricular lead location and the risk of ventricular arrhythmias in the MADIT-‐CRT trial. European heart journal 2013;34:184-‐90. 18. Thebault C, Donal E, Meunier C, et al. Sites of left and right ventricular lead implantation and response to cardiac resynchronization therapy observations from the REVERSE trial. European heart journal 2012;33:2662-‐71. 19. Singh JP, Klein HU, Huang DT, et al. Left ventricular lead position and clinical outcome in the multicenter automatic defibrillator implantation trial-‐cardiac resynchronization therapy (MADIT-‐CRT) trial. Circulation 2011;123:1159-‐66. 20. Noheria A, Desimone CV, Lachman N, et al. Anatomy of the Coronary Sinus and Epicardial Coronary Venous System in 620 Hearts: An Electrophysiology Perspective. Journal of cardiovascular electrophysiology 2013;24:1-‐6. 21. Chan JY, Fang F, Zhang Q, et al. Biventricular pacing is superior to right ventricular pacing in bradycardia patients with preserved systolic function: 2-‐year results of the PACE trial. European heart journal 2011;32:2533-‐40. 22. Curtis AB, Worley SJ, Adamson PB, et al. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med 2013;368:1585-‐93. 23. Zaeem F, Giedriemiene D, Coleman C, et al. CRT-‐D Therapy in Patients with Decompensated NYHA Class-‐Four CHF. Cardiology research and practice 2012;2012:319205. 24. Kolek MJ, Dresen WF, Wells QS, Ellis CR. Use of an Antibacterial Envelope is Associated with Reduced Cardiac Implantable Electronic Device Infections in High-‐Risk Patients. Pacing and clinical electrophysiology : PACE 2012. 25. Alboni P, Holz A, Brignole M. Vagally mediated atrioventricular block: pathophysiology and diagnosis. Heart 2013. 26. Sutton R. Mobitz type 1 second degree atrioventricular block: the value of permanent pacing in the older patient. Heart 2012. 27. Groh WJ, Groh MR, Saha C, et al. Electrocardiographic abnormalities and sudden death in myotonic dystrophy type 1. N Engl J Med 2008;358:2688-‐97. 28. Bordachar P, Zachary W, Ploux S, Labrousse L, Haissaguerre M, Thambo JB. Pathophysiology, clinical course, and management of congenital complete atrioventricular block. Heart Rhythm 2013;10:760-‐6. 29. Moss AJ, Schuger C, Beck CA, et al. Reduction in inappropriate therapy and mortality through ICD programming. N Engl J Med 2012;367:2275-‐83. 30. Gasparini M, Proclemer A, Klersy C, et al. Effect of long-‐detection interval vs standard-‐detection interval for implantable cardioverter-‐defibrillators on antitachycardia pacing and shock delivery: the ADVANCE III randomized clinical trial. Jama 2013;309:1903-‐11. 31. Haywood GA, Camm AJ, Ward DE. Insertion of permanent pacemakers as a day case procedure. BMJ 1989;299:1139.

85
32. Haywood GA, Jones SM, Camm AJ, Ward DE. Day case permanent pacing. Pacing and clinical electrophysiology : PACE 1991;14:773-‐7. 33. Kantharia BK, Patel JA, Nagra BS, Ledley GS. Electrical storm of monomorphic ventricular tachycardia after a cardiac-‐resynchronization-‐therapy-‐defibrillator upgrade. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2006;8:625-‐8. 34. Sokol DK. Let's stop consenting patients. BMJ 2014;348:g2192. 35. de Oliveira JC, Martinelli M, Nishioka SA, et al. Efficacy of antibiotic prophylaxis before the implantation of pacemakers and cardioverter-‐defibrillators: results of a large, prospective, randomized, double-‐blinded, placebo-‐controlled trial. Circ Arrhythm Electrophysiol 2009;2:29-‐34. 36. Ahmed I, Gertner E, Nelson WB, et al. Continuing warfarin therapy is superior to interrupting warfarin with or without bridging anticoagulation therapy in patients undergoing pacemaker and defibrillator implantation. Heart Rhythm 2010;7:745-‐9. 37. Tompkins C, Henrikson CA. Optimal strategies for the management of antiplatelet and anticoagulation medications prior to cardiac device implantation. Cardiol J 2011;18:103-‐9. 38. Tompkins C, Henrikson CA. Our approach to anticoagulation in patients undergoing device implants or replacement. Journal of cardiovascular electrophysiology 2013;24:110-‐2. 39. Baron TH, Kamath PS, McBane RD. Antithrombotic therapy and invasive procedures. N Engl J Med 2013;369:1079-‐80. 40. Baron TH, Kamath PS, McBane RD. Management of antithrombotic therapy in patients undergoing invasive procedures. N Engl J Med 2013;368:2113-‐24. 41. Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-‐valvular atrial fibrillation. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2013;15:625-‐51. 42. Peterson PN, Varosy PD, Heidenreich PA, et al. Association of single-‐ vs dual-‐chamber ICDs with mortality, readmissions, and complications among patients receiving an ICD for primary prevention. Jama 2013;309:2025-‐34. 43. Horlbeck FW, Mellert F, Kreuz J, Nickenig G, Schwab JO. Real-‐world data on the lifespan of implantable cardioverter-‐defibrillators depending on manufacturers and the amount of ventricular pacing. Journal of cardiovascular electrophysiology 2012;23:1336-‐42. 44. Johansen JB, Jorgensen OD, Moller M, Arnsbo P, Mortensen PT, Nielsen JC. Infection after pacemaker implantation: infection rates and risk factors associated with infection in a population-‐based cohort study of 46299 consecutive patients. European heart journal 2011;32:991-‐8. 45. Darouiche R, Mosier M, Voigt J. Antibiotics and antiseptics to prevent infection in cardiac rhythm management device implantation surgery. Pacing and clinical electrophysiology : PACE 2012;35:1348-‐60. 46. Sohail MR, Sultan OW, Raza SS. Contemporary management of cardiovascular implantable electronic device infections. Expert Rev Anti Infect Ther 2010;8:831-‐9. 47. Sohail MR, Uslan DZ, Khan AH, et al. Risk factor analysis of permanent pacemaker infection. Clin Infect Dis 2007;45:166-‐73. 48. Bloom H, Heeke B, Leon A, et al. Renal insufficiency and the risk of infection from pacemaker or defibrillator surgery. Pacing and clinical electrophysiology : PACE 2006;29:142-‐5. 49. Klug D, Balde M, Pavin D, et al. Risk factors related to infections of implanted pacemakers and cardioverter-‐defibrillators: results of a large prospective study. Circulation 2007;116:1349-‐55.

86
50. Margey R. Cardiac implantable electronic device infections: the enemy that lurks beneath the skin. J Long Term Eff Med Implants 2010;20:203-‐17. 51. Borer A, Gilad J, Hyam E, et al. Prevention of infections associated with permanent cardiac antiarrhythmic devices by implementation of a comprehensive infection control program. Infect Control Hosp Epidemiol 2004;25:492-‐7. 52. Anderson DJ, Kaye KS, Classen D, et al. Strategies to prevent surgical site infections in acute care hospitals. Infect Control Hosp Epidemiol 2008;29 Suppl 1:S51-‐61. 53. Sandoe JA, Barlow G, Chambers JB, et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). The Journal of antimicrobial chemotherapy 2014. 54. Ata A, Lee J, Bestle SL, Desemone J, Stain SC. Postoperative hyperglycemia and surgical site infection in general surgery patients. Arch Surg 2010;145:858-‐64. 55. Joshi GP, Chung F, Vann MA, et al. Society for Ambulatory Anesthesia consensus statement on perioperative blood glucose management in diabetic patients undergoing ambulatory surgery. Anesthesia and analgesia 2010;111:1378-‐87. 56. Dronge AS, Perkal MF, Kancir S, Concato J, Aslan M, Rosenthal RA. Long-‐term glycemic control and postoperative infectious complications. Arch Surg 2006;141:375-‐80; discussion 80. 57. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 1999;20:250-‐78; quiz 79-‐80. 58. Da Costa A, Kirkorian G, Cucherat M, et al. Antibiotic prophylaxis for permanent pacemaker implantation: a meta-‐analysis. Circulation 1998;97:1796-‐801. 59. Lowe E, Tayebjee MH, Pratty J, Sandoe JA. Survey of antibiotic prophylaxis for implantable cardiac electronic device (ICED) insertion in England. International journal of cardiology 2012;157:286-‐7. 60. Lakkireddy D, Valasareddi S, Ryschon K, et al. The impact of povidone-‐iodine pocket irrigation use on pacemaker and defibrillator infections. Pacing and clinical electrophysiology : PACE 2005;28:789-‐94. 61. Bloom HL, Constantin L, Dan D, et al. Implantation success and infection in cardiovascular implantable electronic device procedures utilizing an antibacterial envelope. Pacing and clinical electrophysiology : PACE 2011;34:133-‐42. 62. Remmelts HH, Meine M, Loh P, et al. Infection after ICD implantation: operating room versus cardiac catheterisation laboratory. Neth Heart J 2009;17:95-‐100. 63. Ninomura P, Hermans R. Ventilation standard for health care facilities. American Society of Heating, Refrigerating and Air-‐Conditioning Engineers Journal 2008:52-‐8. 64. Darouiche RO, Wall MJ, Jr., Itani KM, et al. Chlorhexidine-‐Alcohol versus Povidone-‐Iodine for Surgical-‐Site Antisepsis. N Engl J Med 2010;362:18-‐26. 65. Langgartner J, Linde HJ, Lehn N, Reng M, Scholmerich J, Gluck T. Combined skin disinfection with chlorhexidine/propanol and aqueous povidone-‐iodine reduces bacterial colonisation of central venous catheters. Intensive care medicine 2004;30:1081-‐8. 66. Guzel A, Ozekinci T, Ozkan U, Celik Y, Ceviz A, Belen D. Evaluation of the skin flora after chlorhexidine and povidone-‐iodine preparation in neurosurgical practice. Surgical neurology 2009;71:207-‐10; discussion 10. 67. Towfigh S, Cheadle WG, Lowry SF, Malangoni MA, Wilson SE. Significant reduction in incidence of wound contamination by skin flora through use of microbial sealant. Arch Surg 2008;143:885-‐91; discussion 91.

87
68. Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev 2007:CD006353. 69. Katz S, Izhar M, Mirelman D. Bacterial adherence to surgical sutures. A possible factor in suture induced infection. Ann Surg 1981;194:35-‐41. 70. Leaper D, McBain AJ, Kramer A, et al. Healthcare associated infection: novel strategies and antimicrobial implants to prevent surgical site infection. Ann R Coll Surg Engl 2010;92:453-‐8. 71. Coulthard P, Esposito M, Worthington HV, van der Elst M, van Waes OJ, Darcey J. Tissue adhesives for closure of surgical incisions. Cochrane Database Syst Rev 2010:CD004287. 72. Richardson RL, Jr., Pate JW. Prevention of infection of pacemaker pocket. Jama 1973;225:1388. 73. Bluhm G, Jacobson B, Julander I, Levander-‐Lindgren M, Olin C. Antibiotic prophylaxis in pacemaker surgery-‐-‐a prospective study. Scand J Thorac Cardiovasc Surg 1984;18:227-‐34. 74. Muers MF, Arnold AG, Sleight P. Prophylactic antibiotics for cardiac pacemaker implantation. A prospective trail. British heart journal 1981;46:539-‐44. 75. Dwivedi SK, Saran RK, Khera P, et al. Short-‐term (48 hours) versus long-‐term (7 days) antibiotic prophylaxis for permanent pacemaker implantation. Indian Heart J 2001;53:740-‐2. 76. Noe JM, Keller M. Can stitches get wet. Plastic and reconstructive surgery 1988;81:82-‐4. 77. Heal C, Buettner P, Raasch B, et al. Can sutures get wet? Prospective randomised controlled trial of wound management in general practice. BMJ 2006;332:1053-‐6. 78. Claxton AR, McGuire G, Chung F, Cruise C. Evaluation of morphine versus fentanyl for postoperative analgesia after ambulatory surgical procedures. Anesthesia and analgesia 1997;84:509-‐14. 79. Zoppo F, Zerbo F, Brandolino G, Bacchiega E, Lupo A, Bertaglia E. Straight screw-‐in atrial leads "J-‐post shaped" in right appendage versus J-‐shaped systems for permanent atrial pacing: a safety comparison. Pacing and clinical electrophysiology : PACE 2011;34:325-‐30. 80. Kirkfeldt RE, Johansen JB, Nohr EA, Moller M, Arnsbo P, Nielsen JC. Risk factors for lead complications in cardiac pacing: a population-‐based cohort study of 28,860 Danish patients. Heart Rhythm 2011;8:1622-‐8. 81. Luria DM, Feinberg MS, Gurevitz OT, et al. Randomized comparison of J-‐shaped atrial leads with and without active fixation mechanism. Pacing and clinical electrophysiology : PACE 2007;30:412-‐7. 82. Mond HG. The road to right ventricular septal pacing: techniques and tools. Pacing and clinical electrophysiology : PACE 2010;33:888-‐98. 83. Aoukar PS, Poole JE, Johnson GW, et al. No benefit of a dual coil over a single coil ICD lead: Evidence from the Sudden Cardiac Death in Heart Failure Trial. Heart Rhythm 2013;10:970-‐6. 84. Garcia-‐Garcia M, Palacios-‐Martinez M, Ponce-‐de-‐Leon A, et al. The role of core groups in transmitting Mycobacterium tuberculosis in a high prevalence community in Southern Mexico. Int J Tuberc Lung Dis 2000;4:12-‐7. 85. Birnie D, Tung S, Simpson C, et al. Complications associated with defibrillation threshold testing: the Canadian experience. Heart Rhythm 2008;5:387-‐90. 86. Vischer AS, Sticherling C, Kuhne MS, Osswald S, Schaer BA. Role of defibrillation threshold testing in the contemporary defibrillator patient population. Journal of cardiovascular electrophysiology 2013;24:437-‐41. 87. Michowitz Y, Lellouche N, Contractor T, et al. Defibrillation threshold testing fails to show clinical benefit during long-‐term follow-‐up of patients undergoing cardiac resynchronization therapy defibrillator implantation. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing,

88
arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2011;13:683-‐8. 88. Brignole M, Occhetta E, Bongiorni MG, et al. Clinical evaluation of defibrillation testing in an unselected population of 2,120 consecutive patients undergoing first implantable cardioverter-‐defibrillator implant. Journal of the American College of Cardiology 2012;60:981-‐7. 89. Estes NA, 3rd. Defibrillation testing: should the paradigm shift? Journal of the American College of Cardiology 2012;60:988-‐9. 90. Arnson Y, Suleiman M, Glikson M, et al. Role of defibrillation threshold testing during implantable cardioverter-‐defibrillator placement: data from the Israeli ICD Registry. Heart Rhythm 2014;11:814-‐21. 91. Stavrakis S, Patel NH, Reynolds DW. Defibrillation threshold testing does not predict clinical outcomes during long-‐term follow-‐up: a meta-‐analysis. Pacing and clinical electrophysiology : PACE 2013;36:1402-‐8. 92. Codner P, Nevzorov R, Kusniec J, Haim M, Zabarski R, Strasberg B. Implantable cardioverter defibrillator with and without defibrillation threshold testing. The Israel Medical Association journal : IMAJ 2012;14:343-‐6. 93. Haug B, Kjelsberg K, Lappegard KT. Pacemaker implantation in small hospitals: complication rates comparable to larger centres. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2011;13:1580-‐6. 94. Eberhardt F, Bode F, Bonnemeier H, et al. Long term complications in single and dual chamber pacing are influenced by surgical experience and patient morbidity. Heart 2005;91:500-‐6. 95. Bond R, Augustine D, Dayer M. Pacemaker complications in a district general hospital. British Journal of Cardiology 2012;19:90-‐4. 96. Kirkfeldt RE, Johansen JB, Nohr EA, Jorgensen OD, Nielsen JC. Complications after cardiac implantable electronic device implantations: an analysis of a complete, nationwide cohort in Denmark. European heart journal 2014;35:1186-‐94. 97. Baddour LM, Epstein AE, Erickson CC, et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation 2010;121:458-‐77. 98. Madhavan M, Sohail MR, Friedman PA, et al. Outcomes in patients with cardiovascular implantable electronic devices and bacteremia caused by Gram-‐positive cocci other than Staphylococcus aureus. Circ Arrhythm Electrophysiol 2010;3:639-‐45. 99. Uslan DZ, Dowsley TF, Sohail MR, et al. Cardiovascular implantable electronic device infection in patients with Staphylococcus aureus bacteremia. Pacing and clinical electrophysiology : PACE 2010;33:407-‐13. 100. Buch E, Boyle NG, Belott PH. Pacemaker and defibrillator lead extraction. Circulation 2011;123:e378-‐80. 101. Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm 2009;6:1085-‐104. 102. Wilkoff BL, Auricchio A, Brugada J, et al. HRS/EHRA expert consensus on the monitoring of cardiovascular implantable electronic devices (CIEDs): description of techniques, indications, personnel, frequency and ethical considerations. Heart Rhythm 2008;5:907-‐25. 103. Glotzer TV, Hellkamp AS, Zimmerman J, et al. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke: report of the Atrial Diagnostics Ancillary Study of the MOde Selection Trial (MOST). Circulation 2003;107:1614-‐9.

89
104. Glotzer TV, Daoud EG, Wyse DG, et al. The relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: the TRENDS study. Circ Arrhythm Electrophysiol 2009;2:474-‐80. 105. Faber TS, Gradinger R, Treusch S, et al. Incidence of ventricular tachyarrhythmias during permanent pacemaker therapy in low-‐risk patients results from the German multicentre EVENTS study. European heart journal 2007;28:2238-‐42. 106. Boveda S, Marijon E, Jacob S, et al. Incidence and prognostic significance of sustained ventricular tachycardias in heart failure patients implanted with biventricular pacemakers without a back-‐up defibrillator: results from the prospective, multicentre, Mona Lisa cohort study. European heart journal 2009;30:1237-‐44. 107. Pettit SJ, Browne S, Hogg KJ, et al. ICDs in end-‐stage heart failure. BMJ Supportive and Palliative Care 2012;2:94-‐7. 108. Grubb BP, Karabin B. Ethical Dilemmas and End-‐of-‐Life Choices for Patients with Implantable Cardiac Devices: Decisions Regarding Discontinuation of Therapy. Current treatment options in cardiovascular medicine 2011;13:385-‐92. 109. Lampert R, Hayes DL, Annas GJ, et al. HRS Expert Consensus Statement on the Management of Cardiovascular Implantable Electronic Devices (CIEDs) in patients nearing end of life or requesting withdrawal of therapy. Heart Rhythm 2010;7:1008-‐26. 110. Makkar A, Prisciandaro J, Agarwal S, et al. Effect of radiation therapy on permanent pacemaker and implantable cardioverter-‐defibrillator function. Heart Rhythm 2012;9:1964-‐8. 111. Mahlow WJ, Craft RM, Misulia NL, et al. A Perioperative Management Algorithm for Cardiac Rhythm Management Devices: The PACED-‐OP Protocol. Pacing and clinical electrophysiology : PACE 2013;36:238-‐48.