Embed Size (px)
Citation preview

Page 1 of 38
ADDENDUM NO. 2 September 1, 2015 CountyCare Third Party Administration and Benefits Management RFP # H15-0046
1. General
This addendum revises RFP documents. This addendum is issued to proposers of record prior to execution of contract, and forms a part of contract documents and modifies previously issued documents. Insofar as previously issued contract documents are inconsistent with modifications indicated by this addendum, modifications indicated by this addendum shall govern. Where any part of the contract documents are modified by this addendum, all unaltered provisions shall remain in effect.
2. Addendum Acknowledgement Form
Acknowledge receipt of this addendum in the space provided on the Addendum Acknowledgement Form. Proposers must include the signed form with their response. Failure to do so will subject Proposers to disqualification.
3. Changes and Clarifications
a. Scope of Work No. 2 (Case Management) and all of its subsections (2.1 and 2.2) is
officially removed from the scope for this RFP.
b. Section 7.1.4.6 a (Quality Assurance Plan) is officially removed from the scope of this
RFP.
4. Attachments
All documents listed below are attached to the Addendum No. 2 PDF file unless otherwise noted.

Page 2 of 38
a. Answer to Vendor Questions (below).
b. CountyCare Organizational Chart.
c. Claim Volumes by Primary Diagnoses.
d. CountyCare Pharmacy Claims May to July 2015.
e. CountyCare Risk Stratification Data August 2015.
f. Dental Data.
NEXT PAGE

Page 3 of 38
4.1 Response to Vendor Questions
ID Question CCHHS Response
Q-001 Can you please explain how Optical Services (eye exams and eyewear) are currently being delivered to CountyCare members? Specifically, is CountyCare currently at risk for Optical Services? If so, can you please describe CountyCare's delivery system for Optical Services?
CountyCare is at risk for optical services, sub-capping an at-risk OBM for these services. The delivery system is managed by this vendor. Benefits match those of the IL Medicaid program.
Q-002 On Page 9, Section 3.1.1. Network, the CountyCare Contracted Network by Provider Type data included does not specify optometrists, ophthalmologists or optical suppliers by provider type, however, we note a number of Federally-Qualified Health Centers (FQHC) as well as some providers listed as "Multi-Specialty." Can you please clarify if any of the currently-contracted FQHCs and/or Multi-Specialty Clinics have eye care professionals and/or optical dispensing on site? If so, are these eye care professionals /optical dispensaries currently on CountyCare's provider panel and is there an expectation that the selected Optical Benefits Manager will contract with these locations? If so, will the selected Optical Benefits Manager be expected to honor an existing reimbursement schedule in place between CountyCare and the applicable provider(s)? If so, please provide all applicable reimbursement schedule(s).
There are FQHCs and multispecialty providers who offer eye care currently contracted by CountyCare which the OBM will need to include in their network, honoring existing reimbursement schedules. (See Q-017)
Q-003 Based upon our review of the Illinois Department of Healthcare and Family Services' Handbook for Providers of Optometric Services, Chapter O-200, Policy and Procedures for Optometric Services (Issued May 2009), it is our understanding that the Illinois Medicaid program uses the Illinois Department of Corrections (DOC) for fabrication of eyeglasses, with optometrists reimbursed for professional services and, if appropriate, a dispensing fee for eyeglasses. Is a Medicaid Managed Care Plan such as CountyCare and its contracted Optical Benefits Manager required to use the Department of Corrections for eyeglass fabrication or will the selected Optical Benefits Manager be permitted to utilize its standard sources for eyeglass fabrication?
The contracted OBM may use its standard sources for eyeglass fabrication. While contracting with the IL DOC is not required, it is highly recommended. Fees for fabrication that are not at-risk, require approval by CountyCare. (See Q-006)
Q-004 Within the Scope of Work #5, are we correct in interpreting that the selected Optical Benefits Manager will be responsible for all services rendered by optometrists, including wellness vision exams, eyewear dispensing and medical eye care services that are within an optometrist's scope of license?
Yes, this interpretation is accurate.

Page 4 of 38
ID Question CCHHS Response
Q-005 Within the Scope of Work #5, with regard to the "Note" on page 74 that reads, "Ophthalmological services are excluded from this SOW and provided for under medical serices managed by CountyCare's back office Proposer," is it correct to assume that this is only referring to medical services provided by ophthalmologists and that the Optical Benefits Manager may include ophthalmologists on its provider panel for purposes of rendering wellness vision services (wellness eye exams and eyewear dispensing)?
Yes, this assumption is correct.
Q-006 Within the Scope of Work #5, on page 76, Section 7.5.4.6.a), please confirm our understanding that the Optical Benefits Manager will be required to reimburse its contracted providers at 100% of the Illinois Department of Healthcare and Family Services Medicaid fee schedule (or the provider's usual and customary fee schedule, whichever is lower). If reimbursement is required to be at 100% of the HFS Medicaid reimbursement schedule and the Optical Benefits Manager is not required to use the Department of Corrections for eyeglass fabrication, is there a fee schedule the OBM must utilize for eyewear reimbursement or may the OBM use its own standard reimbursement schedule?
The contracted OBM may use its standard sources for eyeglass fabrication. While contracting with the IL DOC is not required, it is highly recommended. (See Q-003)
Q-007 In Section 8.4., on page 84, "Response Section 3: Scopes of Work Requirements," do the suggested number of pages listed in this section include supporting documentation respondents may supply to help supplement responses, or are these suggested page counts for bidder's narrative response only, with supporting documentation not included in the suggested page counts?
The 'suggested' number of pages is for the narrative response only. Supporting documents should be placed in the appendix section, or the proposer may provide a link to an online website if available. (See Q-013)
Q-008 In Section 8.14, page 88, "Pricing Proposal," and Section 11.2, page 90, "Number of Copies," please confirm our understanding is accurate that proposers are to submit (a) 1 original paper copy, 1 electronic copy via USB thumb drive, and 10 paper copies of the Full response except for the Pricing Proposal Spreadsheet and the Economic Disclosure Statement; AND (b) in a separate envelope, 1 original paper copy, 1 electronic copy via USB thumb drive, and 10 paper copies of the Pricing Proposal Spreadsheet and the Economic Disclosure Statement.
Yes, this interpretation is accurate.
Page 5 of 38
ID Question CCHHS Response
Q-009 In Section 8.14, page 88, "Pricing Proposal" and Pricing Proposal Spreadsheet, please confirm if CountyCare wishes to receive only a non-risk administrative services (ASO) bid, only a risk-based capitated bid, or both. Based upon the statement in Section 8.14, page 88, "Pricing Proposal" that reads, "Cost of claims should not be included in this pricing proposal," we interpreted this to mean that only an ASO bid is desired. However, when reviewing the Pricing Proposal Spreadsheet, we noted that it contained columns asking if the bid is "at risk" and the example given states, "At-Risk PMPM for Optical Services."
CCHHS will accept either risk-based or ASO-only pricing. Risk-based pricing should be an all-inclusive rate, while ASO-only pricing should exclude claims costs. (See Q-010)
Q-010 In Section 8.14, page 88, "Pricing Proposal" and Pricing Proposal Spreadsheet, for a non-risk bid, should the bidder indicate both its administrative fee and the projected cost of claims as separate line items OR does CountyCare prefer to receive only the administrative fee, with no cost of claims projection?
ASO-only pricing should exclude claims costs. (See Q-009)
Q-011 In Section 8.14, page 88, "Pricing Proposal" and Pricing Proposal Spreadsheet, are bidders required to propose on the basis of tiered pricing or may a bidder elect to provide its proposal on a Per Member Per Month (PMPM) basis? If a tiered structure is required, please provide the desired tier parameters.
Proposers may submit either tiered or PMPM pricing. Additionally, proposers may choose to tier PMPM pricing based on membership levels. (See Q-098, Q-102, Q-103, Q-105)
Q-012 Within Section 7.5.4, Scope of Work #5 Requirements, pages 77-78, Subsection 7.5.4.10.) "Prior Approval," please provide a copy of the applicable prior authorization procedures.
Prior authorization is required for all services performed by a non-participating facility or by a non-participating physician. All procedure codes that are not listed in the AMA CPT manual (e.g. CPT codes 6xx99) also require prior authorization.
Q-013 In Section 8.1, page 84, "Executive Summary", does the 2 page limit include the Company Organization chart or can bidders submit as a separate attachment along with the 2 pages for the Executive Summary?
The Company Organization Chart should be included in the 'Executive Summary' regardless of whether it exceeds the suggested 2-page limit or not. (See Q-007)
Q-014 Our firm makes every effort to work with and incorporate MBE/WBE firms into our business model when bidding on opportunities throughout the country. Please validate that the MBE 35% requirement is applicable to each SOW individually or if the 35% requirement is meant towards the proposal as a whole.
The 35% is in reference to an overall contract goal as directed by the Cook County Office of Contract Compliance.
Q-015 What is the scope of the claims related exclusion for the MBE/WBE goal?
All claims paid to providers of care are excluded from the MBW/WBE goal as they are not expenses borne by the TPA/benefits administrators.

Page 6 of 38
ID Question CCHHS Response
Q-016 Can CountyCare please provide 12 months of claims experience history as it relates to Statement of Work #5, including service type (e.g. exam, eyewear, etc.), provider location and claims costs?
Because this is currently an at-risk contract, detailed claims history is not available. (See Q-165)
Q-017 Can CountyCare please provide the existing provider network that services the work outlined in Statement of Work #5?
There are FQHCs and multispecialty providers who offer eye care currently contracted by CountyCare which the OBM will need to include in their network, honoring existing reimbursement schedules. (See Q-002)
Q-018 Please clarify correct RFP No. - RFP No. H15-0044 OR RFP No. H15-0046 - Both numbers are noted in RFP.
The correct RFP number is the one listed on the cover page: H15-0046
Q-019 What is the volume of members for High-Risk Care Coordination (SOW 2.2)?
This Addendum No. 2 officially removes Scope of Work #2, Case Management, and all of its subsections from the scope of this RFP.
Q-020 What qualifies as “3 years of experience providing delegated care coordination support to a large managed care population”? Is it 3 years of contracts with managed care or experience with the population? If contracting with managed care then how can community based organizations qualify to apply
N/A (see Q-019)
Q-021 Does one have to be a certified Medicaid provider to apply if the service is non-medical?
Assuming this question is related to providers in the network, yes, they must be Medicaid certified. There are, however, a few exceptions (e.g. residential drug treatment for ACA adults) as allowed by the State.
Q-022 How does the 35% MWBE goal apply to non-profits?
The 35% MBE/WBE requirement applies the same to all business types, including non-profits.
Q-023 Would it be possible to release 12 months of RX claims data?
Three months of Rx data are being provided as CountyCare believes this is most relevant to future activity. (See Q-178)
Q-024 It is not clear what functions CCHHS is retaining vs functions it is delegating to the TPA and/or co-sharing with the TPA. Does CCHHS have a functional chart or table it can share that illustrates the responsibilities that CCHHS retains vs those of the TPA?
All functions in SOW #1 are for delegation to the TPA. SOW subsection #1.6 defines the areas where CCHHS seeks support from the TPA to achieve goals in the MCCN as cited.
Q-025 Please clarify whether CCHHS will be performing compliance-related activities or the TPA will be performing.
Proposer will be performing compliance-related functions with oversight by CCHHS' Corporate Compliance Committee and Corporate Compliance Officer.
Page 7 of 38
ID Question CCHHS Response
Q-026 Please clarify whether CCHHS will be performing Fraud, Waste and Abuse activities or the TPA will be performing. Does CCHHS envision utilizing a FWA vendor?
CCHHS Corporate Compliance is ultimately responsible for overseeing the Fraud, Waste and Abuse process but will not be performing the day-to-day functions. Rather, proposer will be responsible for preventing, detecting and reporting day-to-day health care Fraud, Waste, Abuse and financial misconduct, as required by federal and state statutory, regulatory and contractual obligations pursuant to Section 6.3.3. of the RFP.
Q-027 Please provide some information about your current credentialing process. Are all providers credentialled through CCHHS or through a CVO or TPA? Are all providers up-to-date in credentialling? Are most providers due for recredentialing at the same time or staggered throughout the year?
CountyCare providers are credentialed by the TPA either directly, or through a delegated agreement overseen by the TPA. All credentialing is monitored by CountyCare's Credentialing Committee. All providers are up to date. Renewals are rolling, every two years.
Q-028 We understand the TPA will be performing Member and Provider complaints. Please clarify if TPA or CCHHS will be peforming Member and Provider appeals and grievances (2nd level reviews).
Proposer will be responsible for managing all levels of the Member and Provider appeals and grievances process, with oversight and final authority resting with CCHHS.
Q-029 Throughout the TPA SOW, CCHHS has listed a number of member related functions that it expects the Proposer to perform, such as creation of member handbooks, ID cards, eduational materials etc. Please confirm the cost of producing/printing/mailing these materials is incurred by CCHS.
These costs are incurred by the TPA, not CCHHS, and should be included in the Proposer's pricing proposal.
Q-030 Please confirm whether the cost of the 24 hr Nurse hotline as well as the cost of interpreter/translation services is incurred by CCHHS.
These costs are incurred by the TPA, not CCHHS, and should be included in the Proposer's pricing proposal.
Q-031 We understand that the Proposer will be performing certain UM functions. Please confirm TPA will be performing 1st level appeals. Will CCHHS be performing 2nd level appeals?
Proposer will be managing the Member Appeal process. Proposer will manage the entire 1st Level Appeal at the Plan level. Proposer will participate in the 2nd Level Appeal, also referred to as the State Fair Hearing, including submission of documentary evidence, providing oral testimony and issuing correspondence to members. CCHHS will oversee the Member Appeal process. (See Q-032)
Q-032 We understand that the Proposer will be performing certain BH functions. Will CCHS have its own BH committee? BH Peer Review Committee? Please confirm TPA will be performing 1st level BH appeals. Will CCHHS be performing 2nd level BH appeals?
CCHHS has an interdisciplinary, cross-departmental BH Committee. BH Peer review will be the responsibility of the TPA, with oversight by CountyCare's Peer Review Committee. BH appeals mirror those for physical health as outlined in Q-031. TPA is also expected to process BH claims and provide related UM services. (See Q-031)
Q-033 Please provide additional information regarding behavioral health expectations for care management and co-location at provider sites
The expectation is for the vendor to process BH claims and provide related UM services. The TPA

Page 8 of 38
ID Question CCHHS Response
will not perform BH care management nor co-locate its services at provider sites.
Q-034 Please confirm that CCHHS intends (or does not intend) to delegate the Quality function to Proposer. Will CCHHS have its own Quality Committee? Are there functions that CCHHS will retain related to Quality?
CCHHS will perform the Quality of Care reviews and maintain its own Quality Committee but the proposer should be prepared to perform HEDIS quality measurement, other performance measurement as required by CMS, HFS or EQRO, and assist CCHHS with other quality measurement using administrative data.
Q-035 The RFP (page 47) includes a section titled Excluded Scope of Work Requiring Proposer Interface. Under the column titled "Anticipated Touch Points" it is mentioned Establish Data Links" Can CCHHS elaborate as to what these data links will entail? How many data links are expected?
Proposer will be required to receive files from the state through its MMIS system or other state connections (e.g. 834, 834 monthly, 835, 837 series). Additionally, proposer must be able to process these files into their system and subsequently provide them to CCHHS and each 'excluded vendor' who requires the files to determine eligibility or process claims. Another touch point for the TPA is accepting encounters from each benefits manager, serving as the conduit for submission to the State. Proposers should expect and should estimate sufficient time during initial planning/transition to identify and establish all necessary connections, as well as plan the resources necessary for ongoing support of this effort. (See Q-239)
Q-036 Confirm whether TPA will need to provide TPA personnel within CCHHS designated physical office location/space. If yes, confirm whether such space will be provided by CCHHS.
No, TPA will not need to provide TPA personnel within CCHHS designated physical office location/space.
Q-037 Confirm whether TPA will need to have a dedicated Provider hotline.
Yes.
Q-038 Confirm that CCHHS is responsible for Provider Education and Provider contract management.
Proposer will provide the contract management solution/tool and manage contracts on CCHHS' behalf. Proposer and CCHHS will collaborate jointly on Provider Education however Corporate Compliance training requirements identified within RFP section 6.3 will be the primary responsibility of the Proposer. CCHHS reserves the right to request the Proposer to customize the education materials.
Q-039 Confirm that CCHHS will perform provider contract negotiations for Out-of-Network and on as needed basis.
Yes. All provider contracting will be the responsibility of CCHHS.
Q-040 Confirm whether health screenings/risk assessments must be performed on all new members.
Yes. See MCCN Section 5.14.1.1 for details.
Page 9 of 38
ID Question CCHHS Response
Q-041 7.1.4.o Have the health risk assessments already been developed?
Yes, current care coordination providers/teams have already developed health risk screenings.
Q-042 7.1.4.4.r Have the education materials already been developed?
No.
Q-043 7.1.4.5.d Nurse Triage Line. Can you provide any information on current usage and staffing levels for this 24/7 service?
In 2015 total inbound call volume has ranged between 3,100-4,000 calls/month; the range of calls requiring a nurse has been 200-500/month. No data about staffing is available.
Q-044 Confirm that TPA will not be performing Third party recovery, COB or subrogation.
The TPA will perform third-party recovery, COB and subrogation for CountyCare. Additionally, the TPA is expected to provide pre and post claims review. The processes and mechanisms for these functions require CountyCare approval.
Q-045 The RFP requires 3 references from each of the subcontracted vendors, in addition a response to the SOW questions. Are there any other documents needed from the subcontractors besides the SOW responses and the 3 references?
As stated in Section 8.7 of the RFP, it is important for the Evaluation Committee to understand the partner or subcontractor's company background, level of participation, and alignment with the project scope. The Executive Summary and the SOW should incorporate appropriate references to the type of work and level of effort by partners. The Evaluation Committee will be looking for cohesive teams that can deliver the proposed services.
Q-046 In the Company Profile table, it asked for Registration Number issued by Illinois Secretary of State - is that our registrations number to do business in Illinois or is that something we should have been assigned when we registered to be a CCHHS vendor?
It refers to the registration number to do business in Illinois
Q-047 Confirm that PBM, vision, dental & transportation are the only carved out services.
Each SOW stands alone and may be contracted separately. Please note that the TPA scope includes utilization management for all members, as well as claims processing for BH services.
Q-048 In Universal Eligibility #2, it asks for list of clients for each SOW we are responding to, does that mean if we are subcontracting any of the SOWs that the subcontractor needs to provide list of their clients?
Yes, subcontractors providing a significant part of the SOW need to provide clients list and the three (3) required references.
Q-049 In Universal Eligibility #2, its asks for office locations, does that mean we need to list the subcontractor office locations?
Yes. The Evaluation Committee will carefully evaluate the capacity and experience of proposed subcontractors and partners, and through the System Director of Supply Chain Management, reserves the right to reject any proposed personnel/team if it is determined not to be in CCHHS’ best interest. All selected teams including partners and subcontractors are subject to State-level Readiness Review.
Q-050 Do you prefer the Attachments come at the very end or after each section?
Attachments are preferred at the end of the overall response. (See Q-007)
Page 10 of 38
ID Question CCHHS Response
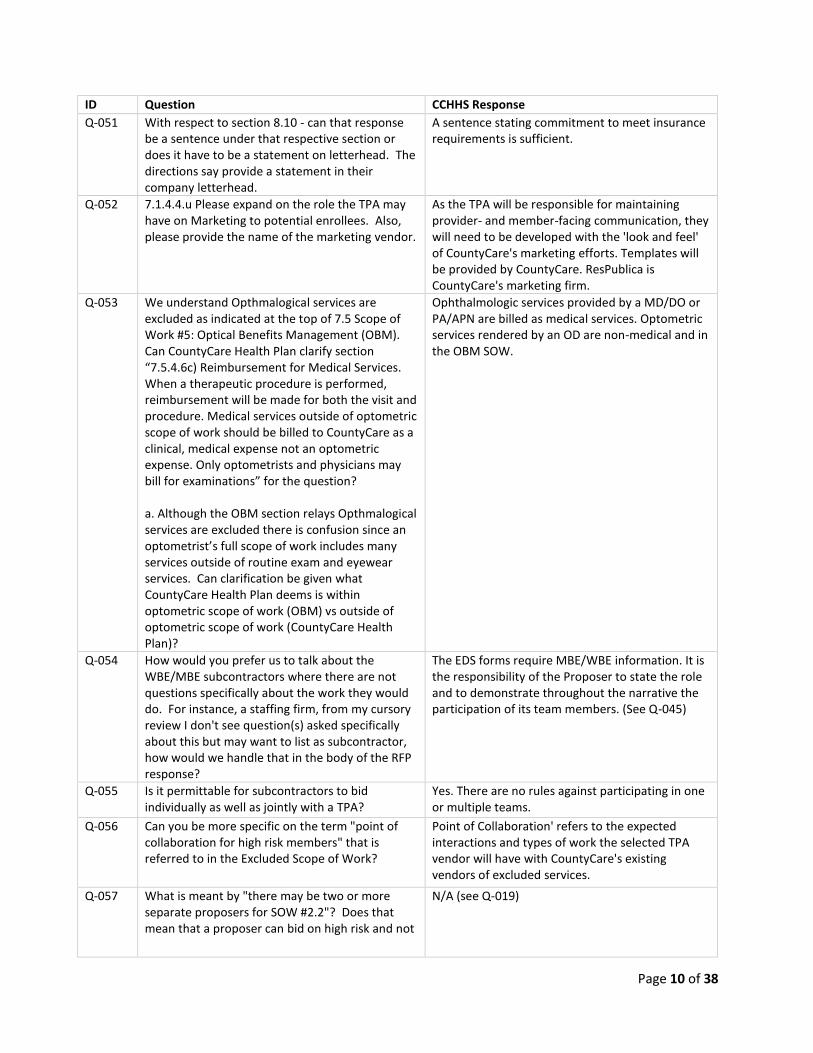
Q-051 With respect to section 8.10 - can that response be a sentence under that respective section or does it have to be a statement on letterhead. The directions say provide a statement in their company letterhead.
A sentence stating commitment to meet insurance requirements is sufficient.
Q-052 7.1.4.4.u Please expand on the role the TPA may have on Marketing to potential enrollees. Also, please provide the name of the marketing vendor.
As the TPA will be responsible for maintaining provider- and member-facing communication, they will need to be developed with the 'look and feel' of CountyCare's marketing efforts. Templates will be provided by CountyCare. ResPublica is CountyCare's marketing firm.
Q-053 We understand Opthmalogical services are excluded as indicated at the top of 7.5 Scope of Work #5: Optical Benefits Management (OBM). Can CountyCare Health Plan clarify section “7.5.4.6c) Reimbursement for Medical Services. When a therapeutic procedure is performed, reimbursement will be made for both the visit and procedure. Medical services outside of optometric scope of work should be billed to CountyCare as a clinical, medical expense not an optometric expense. Only optometrists and physicians may bill for examinations” for the question? a. Although the OBM section relays Opthmalogical services are excluded there is confusion since an optometrist’s full scope of work includes many services outside of routine exam and eyewear services. Can clarification be given what CountyCare Health Plan deems is within optometric scope of work (OBM) vs outside of optometric scope of work (CountyCare Health Plan)?
Ophthalmologic services provided by a MD/DO or PA/APN are billed as medical services. Optometric services rendered by an OD are non-medical and in the OBM SOW.
Q-054 How would you prefer us to talk about the WBE/MBE subcontractors where there are not questions specifically about the work they would do. For instance, a staffing firm, from my cursory review I don't see question(s) asked specifically about this but may want to list as subcontractor, how would we handle that in the body of the RFP response?
The EDS forms require MBE/WBE information. It is the responsibility of the Proposer to state the role and to demonstrate throughout the narrative the participation of its team members. (See Q-045)
Q-055 Is it permittable for subcontractors to bid individually as well as jointly with a TPA?
Yes. There are no rules against participating in one or multiple teams.
Q-056 Can you be more specific on the term "point of collaboration for high risk members" that is referred to in the Excluded Scope of Work?
Point of Collaboration' refers to the expected interactions and types of work the selected TPA vendor will have with CountyCare's existing vendors of excluded services.
Q-057 What is meant by "there may be two or more separate proposers for SOW #2.2"? Does that mean that a proposer can bid on high risk and not
N/A (see Q-019)

Page 11 of 38
ID Question CCHHS Response
on long term care? What is meant by "customizable methodology"?
Q-058 If the Proposer has worked for CCHHS previously, would CCHHS be willing to provide a letter of reference or a letter of good standing?
Letters of reference must be requested directly from the appropriate CCHHS User Department, which may at its own discretion provide, or not provide a letter of recommendation. The User Department leading this RFP cannot commit to provide a letter of recommendation on behalf of another User Department, but may be requested to provide a letter itself.
Q-059 Are high risk populations who are managed by entities that have successfully completed readiness review assessments and are delegated for care coordination excluded from the SOW #2.2 for the High Risk Care Coordination?
N/A (see Q-019)
Q-060 Will a census be provided prior to quoting? Please refer to the supplemental "Dental-Data" attached.
Q-061 Will a detailed copy of the current dental plans that are being offered be provided?
CountyCare follows the State Medicaid dental benefit, adding 2x annual cleanings and home dental visits as additional benefits. Deep cleanings and home visits, when deemed medically appropriate, are also covered benefits. See link below to State Medicaid benefits. http://www2.illinois.gov/hfs/SiteCollectionDocuments/DORM.PDF
Q-062 Will monthly detailed dental claims experience be provided prior to quoting?
Please refer to the supplemental "Dental-Data" attached.
Q-063 Will monthly dental enrollment by plan, split according to adults and children be provided?
Please refer to the supplemental "Dental-Data" attached.
Q-064 Will monthly dental paid claims by plan split according to adults and children be provided?
Please refer to the supplemental "Dental-Data" attached.
Q-065 Will the monthly number of dental claims by plan split according to adults and children be provided?
Please refer to the supplemental "Dental-Data" attached.
Q-066 In the meeting, reference was made that the awarded TPA will be required to adhere to the Cook County billing requirements. Can you provide the billing format for section 7.3.4.2c and 7.3.4.2d?
There is no specific billing format, but there is a billing procedure. CountyCare will work with the selected Proposer to define the appropriate level of invoice information, but summary level information on invoices is typically required, along with a detailed claims file through SFTP that matches the invoice amount. Cook County's "29A Voucher" is required with each invoice. (See Q-136) Sample 29A can be found online at: http://blog.cookcountyil.gov/economicdevelopment/wp-content/uploads/2013/03/BLANK-29A-FORM-final.pdf

Page 12 of 38
ID Question CCHHS Response
Q-067 Will the list of Cook County Safety net providers as referenced to on page 66, Section 7.3.4.1b of the RFP be provided?
The safety-net provides referenced here include those currently in the CountyCare contracted provider network. This includes all FQHCs and many safety-net hospitals, including CCHHS, which have existing dental programs. (See Q-135)
Q-068 In reference to page 20, question 6, can you please expand on the types of programs that you are referring to? Are you referring to services that we offer our clients in order to communicate their benefits in different languages to meet the needs and diversity of our clients? Or are you referring to specific programs that we offer the public to promote overall health & wellness?
CCHHS is interested in knowing what programs your organization has implemented to support a culturally diverse population. This would include, for example, services that you offer your clients in order to communicate their benefits in different languages to meet the needs and diversity of our clients. See also, program elements issued by NCQA to Implement Multicultural Health Standards including, but not limited to the following: (1) Race/Ethnicity and Language Data, (2) Access and Availability of Language Services, (3) Practitioner Network Cultural Responsiveness, (4) Culturally and Linguistically Appropriate Services Program, (5) Reducing Health Care Disparities. These standards can be accessed online at: http://www.ncqa.org/Portals/0/Publications/Implementing%20MHC%20Standards%20Ideas%20and%20Examples%2004%2029%2010.pdf
Q-069 In reference to page 20, question 7, would you please expand on the types of access and specific systems that are desired?
CountyCare is requiring direct access into the IS systems of its contracted providers. This includes a 'direct line of sight' to the algorithms and assumptions behind the systems operating CountyCare's business. (See Q-155, Q-237, Q-240)
Q-070 If we are responding to the Dental Benefits Management only, are we required to respond to 7.1 which appears to only apply to medical?
No. Proposers may respond to each SOW independently. SOW #7.3 contains the DBM requirements (page 66 of the RFP).
Q-071 In reference to page 67, section 7.3.4.2a, the request appears to not apply to dental benefit management. If this does apply to the dental benefit management would you please expand upon the requirement and provide examples, if available?
This question applies to the extent the proposer will have required prior authorizations in place for dental services. Pharmacy PA will be under the PBM scope of work.
Q-072 In reference to page 68, section 7.3.4.5a, are you requesting reporting features in addition to the reports specifically listed in section 7.3.4.4c? If there is data beyond what is requested in 7.3.4.4c would you please elaborate?
7.4.3.5a refers specifically to submission of encounter data to CountyCare's TPA in the state approved format. Additional data needs are found in 7.3.4.4c, Quality Improvement Plan (QIP), which includes, but is not limited to, gathering and analyzing noted data elements.
Q-073 It is our intention to provide responses, within the recommended page limits. In the event that our answers require a longer response in certain
No, Proposers will not be penalized for adding information.

Page 13 of 38
ID Question CCHHS Response
areas, will we be penalized or have points deducted for doing so?
Q-074 Will CCHHS provide two (2) years of claims data to support data analysis of population? Or provide additional data by population segment (product and condition): • Chronic condition prevalence rates (Asthma, Diabetes, CAD, COPD, HF) • Cost comparisons • ED Utilization per 1000 • IP Utilization per 1000 • PCP visits per 1000 • Preventable re-admission rates • Frequent and Non-Emergent ED utilization by facility and diagnosis
Diagnoses data by primary diagnoses at specialty level and major diagnoses groups is provided for January to March, 2015. See "Claims-volumes-by-Primary D-Dx" attached.
Q-075 7.2.2.3(f)(3) Proposer has an evaluation plan for care management effectiveness which includes quantitative targets and outcomes, qualitative/strategic indicators, member feedback and can generate specific opportunities for improvement - Can you provide current vendor's key performance indicators including trend and baseline?
N/A (see Q-019)
Q-076 7.2.2.3(h) Caseload Standards: Can you provide a count of members under management by each program/waiver in last year?
N/A (see Q-019)
Q-077 7.2.2.3(l) Education Through Care Coordinators: Can you provide the number of targeted and engaged in past year for ED reduction?
N/A (see Q-019)
Q-078 7.2.2.3(j) Transition of Care & 7.2.2.3(k) Coordination of Care: Is this requirement meant to be in the Case Management SOW? If yes, how is current vendor of high-risk care coordination fulfilling this requirement?
N/A (see Q-019)
Q-079 A 24 Hour Nurse Line is presently required under SOW 7.1.2.5d. Vendors who propose to only provide services under SOW 7.2 will, most likely have a 24 Hour Nurse Line that is fully integrated in their delivery model. The Care Coordination effectiveness is likely to be considerably degraded with a non workflow-integrated NAL. There is the potential, then for two separate Nurse Lines. So as to not degrade the effectiveness of the Care Coordination Tools and Services under SOW 7.2 and eliminate potential confusion for Members and Providers, will CCHHS consider moving the 24 Hour Nurse Line requirement to SOW 7.2 while requiring the successful vendor to support all of
N/A (see Q-019)

Page 14 of 38
ID Question CCHHS Response
the outlined 24 Hour Nurse Line requirements under SOW 7.1.2.5d?
Q-080 How will success of your High-Risk Care Coordination program be defined and measured?
N/A (see Q-019)
Q-081 Please confirm we will receive raw data for the entire population to perform 7.2.2.3(b) Risk Stratification.
CountyCare will provide aggregate data. See "CountyCare-RiskStratification-Aug2015" attached.
Q-082 Under Section 3.1.6, in your Call Center Volume Table found on page 17: Can you please more broadly define what sort of calls are included in the Medical Management line item?
This pertains mostly to Prior Authorizations.
Q-083 How will current provider of high-risk care coordination complete transition of active cases.
CountyCare will work with its current TPA to ensure all necessary information is provided to ensure continuity and transition of care.
Q-084 7.2.2.3(b) Risk Stratification Type of data: • EMR • ADT • Historical claims (medical, pharmacy, behavioral) • Labs/results • Utilization management How much history for each (6 mos, 1 year, 2 years)
N/A (see Q-019)
Q-085 7.2.2.3(b) Risk Stratification: Can you provide clarification on "purchasers", who and how is data obtained?
N/A (see Q-019)
Q-086 7.2.2.3(b) Risk Stratification: Can you clarify where data from "members or caregivers and practitioners" is coming from? Is this self-reported data from an HRA and/or provider EMR?
N/A (see Q-019)
Q-087 Attachment A: 2.4 List of individuals in an Administrative Capacity. Please clarify required positions for a vendor responding to only 7.2 Care Coordination.
N/A (see Q-019)

Page 15 of 38
ID Question CCHHS Response
Q-088 Attachment A: 2.4 List of individuals in an Administrative Capacity. Please clarify how the role of Care Coordination and Disease Management Program Manager will have oversight if any of the vendor providing 7.2 Care Coordination requirements.
N/A (see Q-019)
Q-089 Attachment A: 2.8.1 Cultural Competence Plan: Please clarify the requirements in the event there are multiple vendors fufilling this SOW. Which Vendor is utimately responsible versus participation?
Each vendor is required to implement a Cultural Competency Plan under which the Covered Services shall be provided in a culturally competent manner by ensuring the cultural competence of all staff, from clerical to executive management. A tracking mechanism is required with the data channeling into a central repository managed by the TPA. Each Vendor is also required to provide training to all staff upon hire and annually. CCHHS reserves the right to require the selected Proposer to customize its Cultural Competence Plan and related training.
Q-090 8.9 - Please clarify and define CCHHS's "conflict of interest".
“Conflict of Interest” is defined in the MCCN Contract in Section 9.2.30 as an interest of Contractor, and Contractor’s officers, directors, employees and subcontractors, which may be direct or indirect, professional, personal, financial, or beneficial in nature that, in the sole discretion of CCHHS, compromises, appears to compromise, or gives the appearance of impropriety with regard to Contractor’s duties and responsibilities under this Contract. This term shall include potential Conflicts of Interest. A Conflict of Interest may exist even if no unethical or improper act results from it or may arise where Contractor becomes a party to any litigation, investigation, or transaction that materially impacts Contractor's ability to perform under this Contract. Any situation where Contractor’s role under the Contract competes with Contractor’s professional or personal role may give rise to an appearance of impropriety. Any conduct that would lead a reasonable individual, knowing all the circumstances, to a conclusion that bias may exist or that improper conduct may occur, or that gives the appearance of the existence of bias or improper conduct, is a Conflict of Interest.

Page 16 of 38
ID Question CCHHS Response
Q-091 8.10 Insurance Requirements - Please provide the Insurance Standard and definitions for coverage amounts.
CCHHS will work with the selected proposer to identify the appropriate insurance requirements per scope. (See Q-182)
Q-092 8.12 Legal Actions. Please clarify and define "significant financial settlement".
Significant financial settlements are those which the proposer considers significant relevant to their organization.
Q-093 Are you interested in a vision value add (retail allowance to allow members to purchase upgraded frames and lenses) or any upgraded benefits?
Yes
Q-094 Is the ACA vision benefit only for Children or are adults covered as well?
Adults also have specific coverage. Refer to IL Medicaid Optic services for adults. T-100 and T-200 http://www2.illinois.gov/hfs/MedicalProvider/Handbooks/Pages/Chapter100.aspx
Page 17 of 38
ID Question CCHHS Response
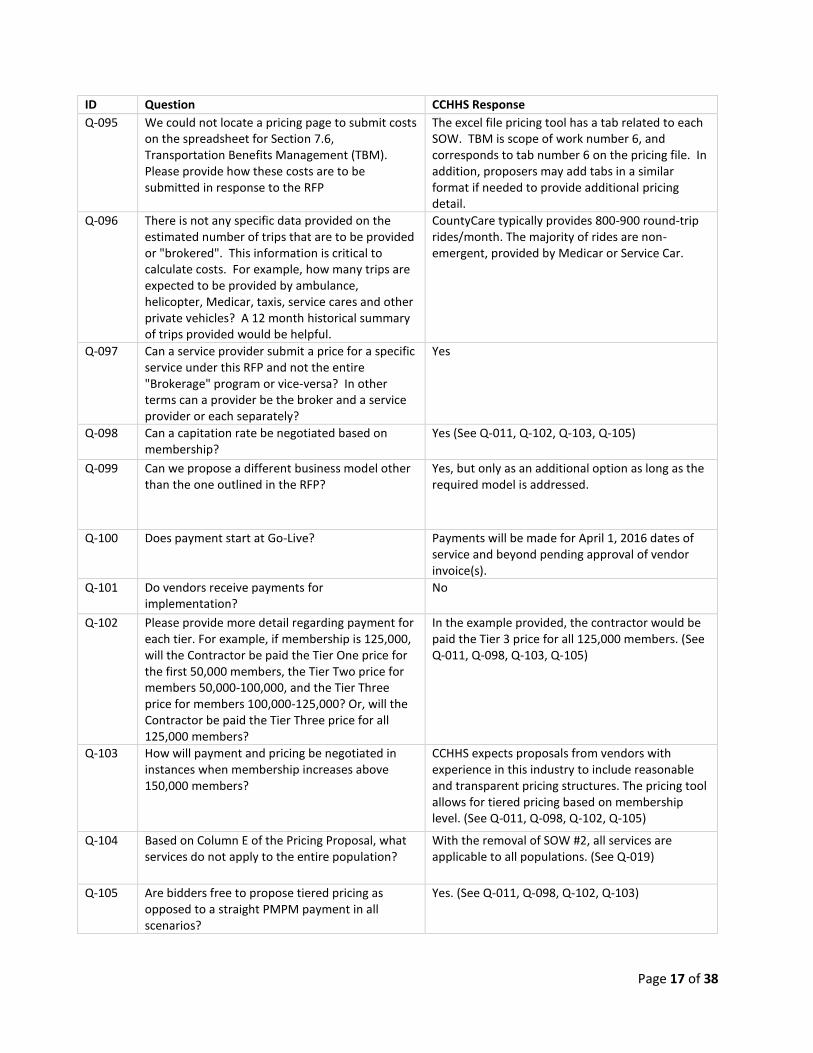
Q-095 We could not locate a pricing page to submit costs on the spreadsheet for Section 7.6, Transportation Benefits Management (TBM). Please provide how these costs are to be submitted in response to the RFP
The excel file pricing tool has a tab related to each SOW. TBM is scope of work number 6, and corresponds to tab number 6 on the pricing file. In addition, proposers may add tabs in a similar format if needed to provide additional pricing detail.
Q-096 There is not any specific data provided on the estimated number of trips that are to be provided or "brokered". This information is critical to calculate costs. For example, how many trips are expected to be provided by ambulance, helicopter, Medicar, taxis, service cares and other private vehicles? A 12 month historical summary of trips provided would be helpful.
CountyCare typically provides 800-900 round-trip rides/month. The majority of rides are non-emergent, provided by Medicar or Service Car.
Q-097 Can a service provider submit a price for a specific service under this RFP and not the entire "Brokerage" program or vice-versa? In other terms can a provider be the broker and a service provider or each separately?
Yes
Q-098 Can a capitation rate be negotiated based on membership?
Yes (See Q-011, Q-102, Q-103, Q-105)
Q-099 Can we propose a different business model other than the one outlined in the RFP?
Yes, but only as an additional option as long as the required model is addressed.
Q-100 Does payment start at Go-Live? Payments will be made for April 1, 2016 dates of service and beyond pending approval of vendor invoice(s).
Q-101 Do vendors receive payments for implementation?
No
Q-102 Please provide more detail regarding payment for each tier. For example, if membership is 125,000, will the Contractor be paid the Tier One price for the first 50,000 members, the Tier Two price for members 50,000-100,000, and the Tier Three price for members 100,000-125,000? Or, will the Contractor be paid the Tier Three price for all 125,000 members?
In the example provided, the contractor would be paid the Tier 3 price for all 125,000 members. (See Q-011, Q-098, Q-103, Q-105)
Q-103 How will payment and pricing be negotiated in instances when membership increases above 150,000 members?
CCHHS expects proposals from vendors with experience in this industry to include reasonable and transparent pricing structures. The pricing tool allows for tiered pricing based on membership level. (See Q-011, Q-098, Q-102, Q-105)
Q-104 Based on Column E of the Pricing Proposal, what services do not apply to the entire population?
With the removal of SOW #2, all services are applicable to all populations. (See Q-019)
Q-105 Are bidders free to propose tiered pricing as opposed to a straight PMPM payment in all scenarios?
Yes. (See Q-011, Q-098, Q-102, Q-103)

Page 18 of 38
ID Question CCHHS Response
Q-106 Would the County consider changing the experience requirements for Section 7.1.2. to a minimum of two years' experience as a TPA and removing the requirement for NCQA accreditation?
No.
Q-107 Please provide a list of the lab processing systems are currently in use by all locations.
LabCorp and Quest are the only two contracted reference labs, outside of hospital-based reference labs, currently in the CountyCare network.
Q-108 What are the current risk stratification percentages?
N/A (see Q-019)
Q-109 Is there call volume historical data outlining the frequent/highest call times?
By comparison, Monday's across the board have the highest call volume. Early mornings (7-8 AM), mid-day (11 AM) and late afternoons (3-4 PM) also tend to have an increase in call volume.
Q-110 What are the current assessments being used by other vendors in which the RFP excludes SOW (ex: CSN and Mental Health Pop)? This is important information to know to ensure that a universal screening process is being used for membership.
Current care management vendors, La Rabida Care Coordination and MHN ACO, each use health risk screens and assessments that they developed for their own populations.
Q-111 Please clarify the meaning of the following statement: "Contractors shall support providers in achieving linguistic and physical accessibility."
Contractor shall perform Quality Assurance evaluations of Provider practices, which shall include monitoring of Enrollee accessibility to ensure linguistic and physical accessibility. Contractor shall support Providers in achieving accessibility. See MCCN ref: 2.7.5, Provider Monitoring.
Q-112 Please provide criteria used to determine adequate capacity.
Without a reference, we can only assume adequate capacity is related to a proposer's ability to provide adequate capacity to scale its services to new and future populations.
Q-113 How does a vendor hold a PCP accountable for appointment criteria?
If this is in reference to Section 5.7.3 of the MCCN, Proposers are expected to monitor accessibility standards as defined in this section and obtain, monitor and follow-up on any necessary corrective action plans (CAPs) for PCPs failing to meet the minimum requirements.
Q-114 Who are the identified CountyCare vendors that were excluded from the program and how does the vendor interact with them?
The excluded vendors are listed in the "Brief Description" section of the table found on pages 47-49. Interactions between them and the vendor is also noted in this table in the "Anticipated Touch Points with Proposers to RFP SOW" column.
Q-115 How will the calls be routed to the Contractor? Can COUNTYCARE describe the expected handoff to be provided by the Contractor? Is COUNTYCARE okay with the Contractor providing a US# number where the calls can be forwarded to by COUNTYCARE customer?
CountyCare's main phone number (312-864-8200) will not change. The selected vendor will work with CCHHS' communications department to appropriately route calls.

Page 19 of 38
ID Question CCHHS Response
Q-116 Will the calls need to be recorded? If yes please provide the percentage of calls and days of storage?
Yes. See MCCN Section 5.18.6.6 for details.
Q-117 Can COUNTYCARE confirm if email and chat support is also in scope? If yes will Contractor be provided customer email & chat application to be used? If yes please provide the Service levels and historical handle time for the non-voice queues.
Email and chat support are not specified as requirements within the MCCN contract. However, CountyCare encourages vendors to provide as many member engagement options as possible and would welcome these options as part of a Proposer's response.
Q-118 How does COUNTYCARE expect to connect to customer data center for application/CRM data connectivity?
It is CountyCare's expectation that the vendor will provide the access and connectivity to CRM, to any other care management tools, and to claims systems for the purposes of verifying provider and rate loads, as well as viewing claims status.
Q-119 Does COUNTYCARE support IPSEC VPN tunnel over internet?
Yes. This is done through a site-to-site connection via our Cisco ASA firewall. For State requirements refer to MCCN Attachment XIV.
Q-120 Does COUNTYCARE require a dedicated space with partition for the call center?
CountyCare requires a dedicated call center staff. A separated physical space for this team is not required.
Q-121 Are there any BCP/DR requirements for the solution?
Yes. Refer to MCCN Attachment XIV.
Q-122 Are there any specific monitor screen size/ agent desktop hardware/software requirements?
CountyCare will work with selected Proposer on this as there is variability.
Q-123 What is COUNTYCARE’s expectations with respect to the LAN setup at the delivery location?
All IS networks are expected to be compliant with industry- standard HIPAA security functions.
Q-124 Intentionally left blank
Q-125 · Call routing: How does COUNTYCARE plan to route these calls to Contractor? Would COUNTYCARE collect these calls and deliver them on a Contractor provided Access Number?
CountyCare will provide the member and provider call center telephone number (312-864-8200). Vendor will work with CountyCare to establish a phone tree that will direct members to specific locations beyond the call center itself. CountyCare will expect the call center vendor will provide necessary State required reports as well as reports requested by CountyCare in order to conduct business.
Q-126 · IVR: Would these calls be provided post IVR treatment or Contractor needs to provide the IVR functionality. In case of the later, what is the IVR requirement? Request to provide as much detail as possible to ascertain the commercials
Contractor needs to provide IVR functionality.
Q-127 · Call Recording: What percentage of calls need to be recorded and the retention period? What is the expected SLA for care retrieval.
See Section 5.18.6.6 of the MCCN for details.
Q-128 · CTI: Is there any requirement for CTI integration for screen pop up?
Yes
Q-129 · Phone: Hard phone /Soft phone Hard

Page 20 of 38
ID Question CCHHS Response
Q-130 Circuit for Data connectivity : Typically for data connectivity Contractor suggests site to site VPN tunnel over the internet however depending on the user base and the response time to access applications hosted in the client network we go for MPLS based dedicated circuits. In case of MPLS connectivity, would COUNTYCARE be able to provide the circuits?
If data circuits are required we can work with the vender on circuit orders and sizing.
Q-131 What will be COUNTYCARE’s data center location/termination address for establishing the MPLS connectivity?
The data center at CCHHS' Stroger Hospital is the primary location, with the data center at CCHHS' Oak Forest Health Center serving as the backup location. The Stroger Hospital address is 1901 W Harrison Street, Chicago. The Oak Forest address is 15900 Cicero Ave, Oak Forest, IL. All circuits headed for Stroger have the dmark in the data center. At Oak Forest dmarks need to be extended to the data center.
Q-132 Tools & applications access: How does COUNTYCARE provide access to its hosted tools and business specific applications to its vendors? Would it be through a portal/Citrix or VDI farm?
We support site-to-site tunnels via Cisco ASA firewalls for vender access. We have AT&T OptEman metro fiber Internet service that support ASA firewalls .
Q-133 What is the total number of interfaces/integrations?
Six
Q-134 What is your anticipated number of members/enrollees by end of 2016?
CCHHS is budgeting an average of 180,000 members/month for its 2016 Fiscal Year (Dec 1-Nov 30).
Q-135 Section 3.1.1 Network - Does Cook County have any dental providers in the network?
Yes. This includes all FQHCs and many safety-net hospitals, including CCHHS, which have existing dental programs. (See Q-067)
Q-136 Section 7.3.4.2c) - Can we get the details for the "Cook County Format"
There is no specific billing format, but there is a billing procedure. CountyCare will work with the selected Proposer to define the appropriate level of invoice information, but summary level information on invoices is typically required, along with a detailed claims file through SFTP that matches the invoice amount. Cook County's "29A Voucher" is required with each invoice. (See Q-066) Sample 29A can be found online at: http://blog.cookcountyil.gov/economicdevelopment/wp-content/uploads/2013/03/BLANK-29A-FORM-final.pdf
Q-137 Section 8.5b requires 3 letters of recommendation and 8.5c requires 3 references. Can there be any crossover between these two requests, or does it have to be 6 different organizations.
The references and letters of recommendation can be from the same organization/person.

Page 21 of 38
ID Question CCHHS Response
Q-138 Section 5 UR 2, requires disclosure of any CAPS over the last 7 years. Are these only CAPS that resulted in a penalty? Are they only CAPS that are from a governmental entity? CAP's from private companies are not public information that can be disclosed.
CountyCare requests all CAPs be provided for review. As noted in the RFP (Sect 8, pg. 84), any page of a Proposal that Proposer asserts to contain confidential, proprietary information such as trade secrets shall be clearly marked “CONFIDENTIAL PROPRIETARY INFORMATION” at the top of the page in at least one-half inch (1/2”) size letters. The specific portions of the page are asserted to contain a trade secret shall be noted as such. However, the proposer is hereby warned that any part of its Proposal or any other material marked as confidential, proprietary, or trade secret, can only be protected to the extent permitted by Illinois Statutes.
Q-139 Section 8.14 requires the submission of TPA pricing and specifically states “cost of claims should not be included”. For Dental Benefits Management, in addition to TPA pricing, is it acceptable to also provide a full risk proposal that would achieve more effective cost control over total claims costs?
Yes
Q-140 We registered for RFP H15-0046 on August 7, 2015. However, we listed RFP No. H15-0044. That is the number that is listed on the header of the TPA_Services_RFP document. Can you please confirm that our firm was able to register on time under RFP No. H15-0046?
Yes. Note that registration is not required to submit a response. In addition, SCM is implementing website enhancements and effective 8/19/2015, the website prompts users to register in order to download the RFP. This will in turn, allow vendors that download the RFP to receive future addenda. Please visit the website on a regular basis to make sure your firm is seeing all addenda (as the enhancements are being tested). (see Q-249)
Q-141 Do all of the SOWs and the services listed under each SOW apply to the MBE/WBE requirement?
Yes. (See Q-015)
Q-142 Can the clients for the three relevant references (8.5b) to be provided, be the same clients providing the three letters of recommendation (8.5b)?
Yes. (See Q-137)
Q-143 Is Centene currently providing the Care Management program (tools and high risk)? If not who is the provider?
MHN ACO serves all of the FHP and ACA members empaneled to its participating providers. La Rabida Care Coordination serves all Children with Special Needs (CSNs). The TPA serves all other members, including all waiver and SPD members assigned to MHN ACO participating providers.
Q-144 Are all CCHHS contracted providers reimbursed on a Capitation basis or a combination of Capitation and Discount FFS? If the latter, what is the percent of Capitation vs. FFS?
CountyCare network providers are reimbursed on a FFS basis with one exception, Community Counseling Centers of Chicago (C4), which is reimbursed on a PMPM capitation for behavioral health services to FHP and ICP members. CountyCare anticipates extending more capitation agreements in the near future.

Page 22 of 38
ID Question CCHHS Response
Q-145 Is it possible to obtain a list by specialty of providers that are reimbursed on a Fee for Service or Discount FFS basis?
As all providers are paid FFS, this list would be too extensive to provide in detail. Aggregate, summary data are included in the RFP, Section 3.1, CountyCare Statistics (pgs. 8-17).
Q-146 Will the vendor(s) selected for scope of work 2.1 and 2.2 (Care Coordination) be notified as soon as the Third Party Administrator vendor has an IT system ready, so that technology changes and/or issues are addressed with the Care Coordination vendor(s) before contract services start in April 2016?
N/A (see Q-019)
Q-147 Can a vendor under Scope 2.2 apply to serve a defined segment of the high-risk population only?
N/A (see Q-019)
Q-148 Since funding sources can dictate the type of services that can be provided, our question is: Is all of the funding for this RFP solely from Medicaid or are there other funding sources?
Medicaid funding will be used to pay for all Medicaid-allowed benefits. CountyCare may, at its discretion and expense, implement special services outside the Medicaid benefits package. Selected vendors will be expected to support CountyCare in these 'non-traditional' payment and coverage models.
Q-149 Section 5, UR2 Question 1, pg 20 Universal Eligibility - UR2 requirement –“Provide names of at least 3 current working interfaces- regarding bi-directional health information exchange” Is CountyCare looking for names of these interfaces, or the names of the transactions (e.g. 834 eligibility, 820 payment, 837 claims, 835 remittance), or of clients using this functionality?
The names of transactions and clients, not the names of the interfaces themselves.
Q-150 Is there currently any issues or concerns or shortcomings with your current providers contracted for services? If so, can you comment on what those are to help vendors understand areas of dissatisfaction or concern? Can the selected vendor modify the contracts with existing providers in the network? Can new or different providers be contracted?
To the extent 'current providers contracted for services' refers to CountyCare's network of clinical providers, the general concern is quality of care and patient access to services. Selected Proposers cannot modify contracts with network providers. All network contracts are maintained by CountyCare. New or different providers can be recommended to CountyCare for contracting at its sole discretion. Subcontractors to a selected vendor, likewise, require CountyCare's approval, at its sole discretion.
Q-151 Will any of the vendors that have been historically providing the services identified in the RFP to CountyCare be precluded from responding to this RFP?
Any organization that meets the stated requirements may submit a proposal.
Q-152 In Section 8.7, the RFP states… “CCHHS has established a goal that MBE/WBE firms retained as subcontractors receive a minimum 35% of this procurement.” If vendors respond to only one SOW, is it expected that the vendor still provide 35% participation to a MBE/WBE?
Yes, each proposal received should include its MBE/WBE participation plan in accordance with the stated MBE/WBE goals.

Page 23 of 38
ID Question CCHHS Response
Q-153 Will CountyCare consider extending the due date of proposals by 2 additional weeks, till October 14th?
No
Q-154 Will CountyCare allow for a second round of questions, based on the insights gained by the responses from the first submission? This would allow all responders an opportunity to gain greater insight to improve their proposal response.
No (See Q-236, Q-270)
Q-155 Can CountyCare elaborate on this request, “Proposer agree to provide access to systems housing CountyCare activity”? What type of access are you wanting /requiring, for what efforts or duration? Can you provide greater context and purpose of this requirement?
CountyCare is requiring direct access into the IS systems of its contracted providers. This includes a 'direct line of sight' to the algorithms and assumptions behind the systems operating CountyCare's business. (See Q-069, Q-237, Q-240)
Q-156 Section 8.3 states… “This section must address the requirements of Section 6.” However, Section 6.3 states… “NOTE: A Proposer submitting a response only on SOW 2.1, may respond to this…” Does this mean vendors only responding to SOW 2.1- Case Management Tools, need to respond to Section 6.3 in its entirety or is it expected that all vendors to respond to Section 6.3 regardless if they respond to Section 2.1?
N/A (see Q-019)
Q-157 Section 7.2.2.3(h) Is there any existing staff already in place we are supplementing? If so, can you describe? Or will we need to build this staff from the ground up in order to ensure we achieve the appropriate Caseload Standards?
The selected Proposer will be required to produce a staffing model prior to go-live. Staff currently performing this work are employed by CountyCare's current TPA vendor. It is anticipated that the newly selected vendor will work in cooperation with the existing TPA to assess staffing capacity in the transition.
Q-158 For the services under SOW 2.2 would CountyCare award contracts to different vendors for SOW 2.2? Could CountyCare envision a scenario where they would choose one partner for a CM Platform/Technology and another for the operational layer of staff and infrastructure? Will the technology platform selected in RFP H15-0044 be used to operate the Care Coordination SOW as described in this RFP?
N/A (see Q-019)

Page 24 of 38
ID Question CCHHS Response
Q-159 Who takes the Vision & Dental risk? Is this a sub-cap arrangement? Full-risk; shared-risk or other?
CountyCare holds ultimate risk for all claims. Vision is currently a full-risk sub-capitated arrangement, while dental is an ASO arrangement with the cost of claims passed through to CCHHS.
Q-160 How does CountyCare provide real-time alerts to their PCMHs? What system is CountyCare using? Is there an HIE?
Real-time alerts on ED and inpatient discharges are provided through a contract with the Medical Home Network. This scope is excluded from the TPA SOW. No other real-time alerts are provided at this time.
Q-161 Is it expected that vendors provide PPO wrap network for members seeking care outside of Cook County?
No. CountyCare retains all provider contracting and will fulfill this function as needed.
Q-162 Should vendors assume that the compliance officer should be 100% dedicated to the project?
Proposer shall have a designated individual who is responsible for overseeing the corporate compliance and fraud waste and abuse plan and who will serve as the liaison to the CountyCare Compliance Officer. Pursuant to the Federal Sentencing Guidelines, this individual shall be given adequate resources, have appropriate authority and direct access to the governing authority, and shall serve as the focal point for compliance activities. Therefore, Proposer shall have a designated individual and a dedicated team sufficient to meet federal and state statutory, regulatory and contractual compliance obligations.
Q-163 Does the ability exist to modify terms and conditions of the contract (Attachment A)?
To the extent CCHHS and the State agree, any amendment is possible. See RFP Section 8.11.
Q-164 Are comparable systems/services acceptable versus what may be detailed in the RFP and/or Attachment A? (i.e. Alternative/comparable means other than FTP)?
Yes as long as the systems/services are compliant with HIPAA, NIST, and CCHHS policies. Secure file-sharing is a mandatory requirement.
Q-165 Please provide transportation data for the past 12 months that details: --Total claims by month --Claims by month broken out by level of service: ----public transit (bus), ----Taxicab/Service Car (ambulatory) ----Medicar (wheelchair) ----Stretcher/gurney vehicle (non-ambulance) ----non-emergency BLS ambulance, ----non-emergency ALS ambulance, ----emergency BLS ambulance, ----emergency ALS ambulance ---- emergency helicopter ----unique or exceptional modes of transportation
Because this is currently an at-risk contract, detailed claims history is not available. (See Q-016)
Q-166 Intentionally left blank

Page 25 of 38
ID Question CCHHS Response
Q-167 Please provide any information regarding overnight travel in the last 12 months: --Number of events --Total cost of overnight travel
CountyCare has not incurred any overnight travel.
Q-168 How is distribution of passes for public transportation handled currently?
Passes are distributed by our transportation TPA as well as our medical home providers. Please note this process could change at CountyCare's discretion.
Q-169 Is mileage reimbursement an acceptable mode of transport?
While CountyCare endorses this type of innovation, such services are allowed only to the extent it is consistent with the current Medicaid standards as detailed in the RFP or the current IL Medicaid Handbook for Transportation Benefits. (See Q-279)
Q-170 When referring to “Private Automobile are you referring to mileage reimbursement?
No. The reference to 'private automobile' in section 7.6.4.1 is not for mileage reimbursement, but for an eligible provider type that a proposer can contract with.
Q-171 How are emergency ambulance and emergency ambulance levels of service handled currently
Emergency ambulance and levels of service are not included in the RFP SOW.
Q-172 Is there an existing protocol for the provision of NEMT services or any other document that describes service requirements and expectations that are different than those established by the State? If so, please provide.
No
Q-173 Are you able to provide separate call center data directly related to the transportation benefit? --Number of calls per month --Average length of call
No. Unfortunately, these data are not currently tracked by CountyCare.
Q-174 How many days notice are required for a member to schedule their transportation?
CountyCare does not have a requirement for scheduling transportation in advance. Rather, it expects its vendor to have minimal barriers to accessing services, including near real-time availability 24/7/365 when needed.

Page 26 of 38
ID Question CCHHS Response
Q-175 Are there any Service Level Agreements (Performance Standards) in place currently?
Yes. These include: Customer Satisfaction surveys to 5% of riders, Rate of On-time Pick-ups and Monthly Missed Trips, and Call Center Performance. Proposers are required to provide recommended SLAs in their response. CountyCare reserves the right to negotiate and establish additional performance standards.
Q-176 Is there any information regarding the number and types of complaints received over the past year related to transportation services?
Complaints regarding transportation services have included, but are not limited to, long wait times and unavailability of enough drivers. Transportation complaints totaled over half of all complaints in recent months.
Q-177 It appears sections 7.6.2 and 7.6.3 feature identical requirements (RFP page 79). Is this correct or is a change to the RFP requirements forthcoming?
Section 7.6.2 should read: 1. Demonstrate that vendor has a transpiration network in Cook County or the ability to produce a network within 90 days that will meet network adequacy requirements. 2. Demonstrated ability to process Medicaid claims with accuracy, timeliness and submit encounter to the state on the states required timeline. 3. Proven ability to operate a transportation program under a State Medicaid guidelines.

Page 27 of 38
ID Question CCHHS Response
Q-178 Will CCHHS provide 12-months of pharmacy claims data history?
Three months of Rx data are being provided as CountyCare believes this is most relevant to future activity. (See Q-023)
Q-179 Please provide the name and email address of CCHHS’s CFO or CEO so we may forward our financial statements directly to them.
Please forward financial information to the identified POC - [email protected]
Q-180 Please confirm who the incumbent PBM is and contract termination date.
US Script. Contract co-terminates with the current TPA contract on March 31, 2016.
Q-181 Please clarify if section 6.3.4. applies to Medicare, MMP (the Part D portion), and/or Medicaid.
CountyCare does not offer Medicare or MMP products, only Illinois Medicaid.
Q-182 To fully comply with CCHHS insurance requirements request, please provide required policies and limits required for PBM services.
CCHHS will work with the selected proposer to identify the appropriate insurance requirements per scope. (See Q-091)
Q-183 Will there be in-person finalist presentations? If yes, are there target dates?
Site visits and/or demonstrations are tentatively scheduled the last week of October, 2015.
Q-184 What criteria will CCHHS use to make a PBM vendor selection?
See RFP Sections 7.4.2 and 10.2 - detailed evaluation criteria and tactics are currently under development.
Q-185 Please clarify what is meant by “ability to tailor point-of-sale edits in full” referenced in requirements 7.4.4.3 f and h.
PBM's routinely have multiple edits in place that control access to medications. CCHHS seeks to have access to all edits in place with an understanding of the hierarchy or logic of the edits. Moreover, CCHHS seeks to have the full ability to work with the PBM to remove/change/add edits as desired by the plan. To the extent that unique programming is required to implement a requested change, it is expected that such costs will be borne by the PBM.
Q-186 Please clarify what is meant by “suspected use” in FWA requirement 7.4.4.8.
Proposer shall clearly explain the process for preventing, detecting and eliminating fraud, waste, abuse, and financial misconduct.
Q-187 How does CCHHS delegate appeals and grievances today?
CCHHS' current TPA performs all Member and Provider Appeals and Grievance functions, with oversight by CCHHS.
Q-188 Please provide some examples of “other clients” referenced in requirement 7.4.4.9.
Other clients' may be Plan Members, Plan Members' authorized representatives, and/or Providers.
Q-189 How many CCHHS users currently need access to incumbent PBM’s online tools?
We anticipate a minimum of three CCHHS users would require access.

Page 28 of 38
ID Question CCHHS Response
Q-190 How do you currently develop and maintain your formulary?
All changes are reviewed by our internal Pharmaceutical & Therapeutics Committee. CountyCare expects to maintain its current formulary with some minor modifications. Regular guidance from the PBM on additions, deletions, or changes to the formulary or prior authorization requirements based on the emergence of new drugs or medical evidence or significant changes in cost or utilization is expected.
Q-191 What questions do you have about prospective bidders’ formulary service model?
None (see Q-192, 199)
Q-192 How many full-time employees comprise the CCHHS pharmacy staff?
CountyCare's pharmacy services are under the direction of its Medical Director, in conjunction with CCHHS' Director of Pharmacy. As a provider of pharmacy services, CCHHS operates seven pharmacy locations and one mail order pharmacy and employs 303 staff, including 129 full-time pharmacists.
Q-193 Please provide the number of Administrative Pharmacy Prior Authorizations in the past 12 months.
Six months of prior authorization data is provided. See "CountyCare-PAdata-JanToJune2015" attached.
Q-194 Please provide the number of Clinical pharmacy Prior Authorizations in the past 12 months.
Six months of prior authorization data is provided. See "CountyCare-PAdata-JanToJune2015" attached.
Q-195 Please provide the number of Direct Member Reimbursements (paper claims) processed in the past 12 months.
To our knowledge, CountyCare has not processed any Direct Member Reimbursements.
Q-196 Does CCHHS use e-prescribing? Yes
Q-197 Is your current pharmacy benefit integrated with medical under one contract?
Yes
Q-198 What percentage of pharmacy claims are filled in-house?
Approximately 12% of all claims, and 15% of specialty claims are filled within CCHHS pharmacies (see Q-192). CountyCare intends to implement strategies that would increase the percentage of drugs provided through CCHHS pharmacies over time.
Q-199 Does CCHHS require a wrap pharmacy network? Yes, the CountyCare pharmacy network extends well beyond that of CCHHS (see Q-198) and includes both national and local providers.

Page 29 of 38
ID Question CCHHS Response
Q-200 Are all specialty medications filled by in-house pharmacies?
No. Only 15% of specialty drugs are filled at CCHHS pharmacies. CountyCare does expect this to increase dramatically over time as it obtains Specialty Pharmacy approvals.
Q-201 Does CCHHS require a specialty network from the bidding PBM?
Yes.
Q-202 On Page 10, graphic 3.1.2 what does ICP stand for, is this the Senior and Special needs population?
ICP = Integrated Care Program. This is the name of Illinois Medicaid program for Seniors and Persons with Disabilities (SPDs). SPD and ICP are used interchangeably.
Q-203 What clinical programs are in place today to address specialty drug costs? Specifically around behavior health, Hep C, HIV and anti-psychotics?
Care Management is a general program to address all areas of care and utilization; there are no additional, dedicated programs for the areas named in this questions.
Q-204 What pharmacy programs are in place today to help case managers manage pharmacy spend?
Pharmacy programs are overseen by CountyCare's leadership, not case managers, and implemented in partnership with the PBM. CountyCare encourages PBMs to provide functionality that could be extended to case managers located at the Plan or within provider practices. Please note that if this is in reference to Case Management (SOW No. 2), this is no longer in-scope. (See Q-019)
Q-205 Do you have advanced analytics in place to for pharmacy data? Do you merge medical and pharmacy data?
We monitor pharmacy spending on a monthly basis for a variety of key operational metrics. Merging medical and pharmaceutical spending in routine metrics is a goal for our future operations and any future PBM should be prepared to assist us in reaching this level of data integration and analysis.

Page 30 of 38
ID Question CCHHS Response
Q-206 Do you have dashboarding capabilities to assist case managers with pharmacy data? Do you have dashboarding capabilities on physicians?
No. This capacity has not yet been developed, yet our long-term goal would certainly envision such functionality and any future PBM should be prepared to assist us in achieving this. Please note that if this is in reference to Case Management (SOW No. 2), this is no longer in-scope (See Q-019).
Q-207 Our firm does not price services as a TPA. SOW 4 does not accommodate PBM pricing with network discounts, rebates and performance guarantees. Can we use an alternate pricing table?
As stated in the pre-proposal conference, Proposer may add supplemental tabs to the pricing proposal, as long as the new tabs follow a similar format and provide sufficient information for the EC to understand the components.
Q-208 Do you currently have a traditional PBM pricing model with AWP guarantees and no administrative fee?
No. Current pricing has AWP guarantees plus administrative fees.
Q-209 Do you intend to award the whole population to one PBM?
CCHHS reserves the right to contract with more than one vendor for any of the SOWs. However, we anticipate contracting with only one PBM.
Q-210 Is there a consultant assisting you on this bid process?
Yes.
Q-211 What is the pricing metric that is guaranteed? Can we request a conference call to explain your pricing document?
No, questions should have been asked via this document or at the pre-proposal conference.
Q-212 What are the key challenges/pain points that CCHHS expects to solve through this RFP? Please describe any key business objectives/goals that CCHHS desires to achieve from vendor partners.
CountyCare has become the largest Medicaid managed care plan serving Cook County residents. As such, we believe that we would be best served by a TPA that does not operate a competing plan in our market.
Q-213 Can CCHHS share any projected growth in membership expected over the term of the contract?
CCHHS is budgeting an average of 180,000 members/month in its FY'16 (Dec 1-Nov 30).
Q-214 Is CCHS open for the vendor partner to propose a Global Delivery model (i.e a mix of Offshore/Near-Shore/Onshore options) for providing the services? Can CCHHS highlight any specific functional areas where there might be a restriction on using offshore/near-shore delivery?
Offshore vendors may not be used.
Q-215 Is there an expectation that CCHHS will be able to download data and generate a custom/ad hoc report or generate from pre designated template with specified qualifiers?
Both are expectations of CountyCare.
Q-216 Intentionally left blank
Q-217 Intentionally left blank
Q-218 Intentionally left blank
Q-219 Intentionally left blank
Q-220 Intentionally left blank
Q-221 Intentionally left blank
Q-222 Intentionally left blank

Page 31 of 38
ID Question CCHHS Response
Q-223 Intentionally left blank
Q-224 Intentionally left blank
Q-225 Intentionally left blank
Q-226 Intentionally left blank
Q-227 Intentionally left blank
Q-228 Intentionally left blank
Q-229 Intentionally left blank
Q-230 Intentionally left blank
Q-231 Intentionally left blank
Q-232 Intentionally left blank
Q-233 Intentionally left blank
Q-234 Intentionally left blank
Q-235 Will CCHHS provide branding guidelines for public websites?
Yes
Q-236 2. Schedule. Would CCHHS entertain the possibilty of going through a second round of questions and answers, to allow potential proposers the opportunity to ask clarifying questions about the responses to the first round of questions and to ask additional questions based on further review of the RFP? Reference: p. 8
No (see Q-154, Q-270)
Q-237 Please clarify information needed for question 7 of the Universal Eligibility Requirements - Proposers agree to provide access to systems housing CountyCare activity. Reference: Universal Eligibility Requirements & information al Requests, UR2, p 20
CountyCare is requiring direct access into the IS systems of its contracted providers. This includes a 'direct line of sight' to the algorithms and assumptions behind the systems operating CountyCare's business. (See Q-069, Q-155, Q-240)
Q-238 Intentionally left blank
Q-239 Requirement 7.1.4.1c states that a single integrated data base must be provided. Please provide additional detail relative to the requirements/specifications. Reference: p. 30
CountyCare is looking for its TPA to aggregate claim-level data into a single data system for comprehensive analytics purposes. Technical specifications of the claims data are consistent with ANSI-standards (e.g. 834, 820, 837, adjudicated claims data etc.). The TPA will also be required to transfer files on a regular basis to other entities including the CCHHS data warehouse. (See Q-035)
Q-240 Requirement asks for the "Ability for end user to download data required". Please clarify who the "end user" refers to. Reference: TPA Services SOW, 7.1.4.1h) p. 31
End users would be CCHHS/CountyCare leadership. We require the ability to export detailed data into an Excel file for further analysis. (See Q-069, Q-155, Q-237).

Page 32 of 38
ID Question CCHHS Response
Q-241 Please provide a summary of the employees and their respective responsibilities of .those individuals that will be employed by the CountyCare program, as it relates to 7.1.4.2a. Is there an organizational chart for CountyCare leadership staff? Reference: p. 32
The CountyCare organizational chart is attached (see "CountyCare Org Chart 2015-08"). Roles and responsibilities are consistent with those defined in the MCCN, Section 2.3
Q-242 7.1.4.2e addresses claims systems requirements and requires proposers to provide detail regarding a workflow diagram, a claims inventory monitoring process, lists of edits, a hierarchy of how claim may be deleted or altered, and several other pieces. While this particular requirement is more detailed than most, it is nonetheless only one of well over 100 requirements for which proposers are to provide brief detailed responses within a 75 page suggested limit. Could you please provide guidance as to the extent to which portions of responses might be included as attachments, so that we can provide sufficient narrative responses within the page limits? For example, we presume the sample reports can be attached? What about diagrams, workflows, lists of edits, process descriptions, and the like? Reference: p. 34
Detailed requests such as these should be included in a separate 'Attachments' binder which does not have page restrictions.
Q-243 is the Proposer required to pay any fees related to processing claims, i.e. clearing house fees, fees related to recoveries, etc. , as it relates to 7.1.4.2e? Reference: p. 34
These costs are borne by the TPA/Benefits Managers and should be included in the Proposer's pricing proposal.
Q-244 7.1.4.4e) and 7.1.4.4.m(2) appear to be duplicate questions - please confirm. Reference: TPA Services SOW, 7.1.4.4e) p. 38, 7.1.4.4m) p. 42
Correct. Proposers may ignore 7.1.4.4e) and answer 7.1.4.4m(2) only. Please note this as "Intentionally Left Blank" in your response.
Q-245 7.2.2.1 High-Risk Care Coordination. Can you please describe high-risk members are identified and stratified? Reference: p. 58
N/A (see Q-019)
Q-246 Criteria 2. states "demonstrate existing contracted network of dental providers (inclusive of Cook County's safety net provider) with capacity to serve CountyCare's members". Will we need to demonstrate the network at time of RFP submission or prior to Go-Live?
A network of providers will be required for the selected Proposer(s) to pass State Readiness Review prior to the April 1 go-live. Proposers who do not have this in place when the RFP response is due are encouraged to provide a detailed, time-sensitive work plan to achieve this objective.

Page 33 of 38
ID Question CCHHS Response
Reference: DBM SOW, 7.3.2 Scope of Work Evaluation Criteria, p.66
Q-247 Please advise on the numbering in SOW #5 Optical Benefits Management, section 7.5.4.9. Should the sub sections under the description be 7.5.4.9a, 7.5.4.9b, etc. instead of 5.9a, 5.9b? Reference: OBM SOW, 7.5.4.9, p.77
Yes, the numbering in this section should be 7.5.4.9a), 7.5.4.9b), etc. Please make this change in your response.
Q-248 The suggested number of pages for 1 SOW is 75 pages. If responding to SOW #1 only, is SOW #1 referring to the first SOW which is 7.1 TPA Services? Or does is mean that if a proposer responds to only 1 SOW, regardless of which one it is, that the suggested page limit is 75 pages? Reference: 8.4 Scope of Work Requirements, p. 84
If a proposer responds to only one SOW, regardless of which one it is, the suggested page limit is 75 pages
Q-249 We submitted our firm's information per the instructions in order to receive notifications of any Addenda that are issued. However, when we reviewed the list on the CCHHS website of registered entities, we did not see our company listed. How do we make sure that we are on this list? Reference: 11.1 Registration, p. 89
Registration is not required to submit a response. In addition, SCM is implementing website enhancements and effective 8/19/2015, the website prompts users to register in order to download the RFP. This will in turn, allow vendors that download the RFP to receive future addenda. Please visit the website on a regular basis to make sure your firm is seeing all addenda (as the enhancements are being tested). (See Q-140)
Q-250 11.2 Number of Copies. Should each SOW be submitted separately in its own binder or can all SOW responses be submitted together in one binder? Reference: p. 90
Proposers should submit one binder for all SOWs, and one binder or a web link for all attachments.
Q-251 How often do you fund for payment of dental benefits - daily? Multiple days per week?
Once or twice weekly.
Q-252 Do you currently mandate that all providers receive benefit payment electronically?
No. Electronic Fund Transfer (EFT) from the TPA/Benefits Managers to the provider is preferred and all selected proposers will be expected to encourage this form of payment when possible.

Page 34 of 38
ID Question CCHHS Response
Q-253 Do you already have an 837 claims file format in use today? Are you open to discussions about an alternative claims file format?
Yes, we have 837 claims file format in use today as required for claim submission to the State of IL. Alternative data extracts consisting of adjudicated claims will be considered for analytics purposes if -- and only if -- they include all detailed data at the claim line level, and can be provided regularly to multiple parties including the CCHHS data warehouse, TPA, and analytics teams.
Q-254 Please clarify what is meant by "Disease burden" N/A (see Q-019)
Q-255 Can you clarify and give an example of a "care gap alert" as referenced
A care gap alert flags a type of care for which the member would be eligible or expected to get but for which there is no claim. For example, a woman over 50 would be expected to get a yearly mammogram, and if there have been no claims for mammograms the IT system identifies this as a member’s potential care gap. This alert would activate the member, providers, care coordinators and any other staff so that action can be taken.
Q-256 Please provide an example of a "blended caseload" using the limits identified
N/A (see Q-019)
Q-257 In this section you reference providing "access needed services" to members prior to enrollment with CountyCare. Would you be more specific about what type of services and for what time frame.
N/A (see Q-019)
Q-258 Is the Proposer to create and/or publish all Member Welcome Material?
Yes, although CountyCare may provide certain published literature, such as the member handbook. All member materials will be approved by CountyCare. All non-health tip related materials will be approved by CountyCare and the State.
Q-259 Is the 24 hour telephone number on the ID card that of CountyCare or the Proposer
Access through the 24/7 line is through the central number and members may choose this option from the phone tree. This is a means for tracking why members call and so that the performance can be reported to the State.
Q-260 Are the Member Handbook and Enrollee Handbook the same?
Yes.

Page 35 of 38
ID Question CCHHS Response
Q-261 Would you provide examples of "member interactions" tracked by this system
Member interactions are required to be tracked and is reportable to the state on a monthly basis. System refers to care management systems that track members' interactions with care coordinators and others who impact their care. In these cases the care coordinator, as an example, may send specific health literature to members which can be tracked in the system and reported. In addition, the call center may be requested to send a new member kit or new ID card as well as other requested material. This is to be tracked and reported as well.
Q-262 Please clarify what is meant by "regardless of organizational affiliation" in the CCHHS requirment column.
N/A (see Q-019)
Q-263 3.1.15 shows the pharmacy benefit went from 97,246 members in January 2015 to 176,710 members in June 2015. Is this correct? If yes, what was the cause of the increase and is the growth expected to continue? If no, can you please provide a corrected version of 3.1.5?
The growth in membership was caused by growth in CountyCare's FHP population resulting from the State's implementation of mandatory managed care in Cook County. The growth rate is expected to be stable for 2016 at 180,000 members/month.
Q-264 Please provide detailed claims data. Requested data fields for a claims file include: - Fill date - NDC - Pharmacy NABP - Mail/retail indicator - Brand/Generic indicator - Paid/reversed/rejected indicator o Can omit as long as we know Rejected claims are excluded from the claims file - Quantity - Days supply
A summary of three months of pharmacy claims is provided. See "CountyCarePharmacyClaims-MaytoJuly2015" attached.
Q-265 Contract Term - Will extensions to the contract be at CCHHS’s sole option or require mutual agreement?
CCHHS will, at its sole option, initiate the negotiations for any available extension options to the contract.
Q-266 Contract Term - Will renegotiation of rates be considered as part of extension discussions?
CountyCare fosters strong business relationships with its vendors and as such, makes business decisions as appropriate and as necessary. Most decisions are driven by the ability to fulfil the CountyCare mission and protect the interest of its funders (taxpayers).
Q-267 Will Transportation Benefits Management include transportation to or from the Cook County Department of Corrections or Juvenile Temporary Detention Center?
Transportation from the Cook County Department of Corrections (i.e. Cook County Jail) and the Cook County Juvenile Temporary Detention Center will be needed only for CountyCare members upon their release from either of these settings. This occurs 24/7/365 at varying rates throughout the

Page 36 of 38
ID Question CCHHS Response
day, with most releases from the Cook County Jail occurring between 9 PM and 2 AM.
Q-268 Is secured transportation required? No
Q-269 CountyCare’s MCCN Contract -- Will you supply a sample contract prior to the proposal submission deadline?
Attachment A is embedded in the RFP's PDF document and contains all relevant sections of the MCCN Contract to the RFP SOWs. To access this attachment, you must open the PDF in Adobe Acrobat, not the web browser. (See Q-270)
Q-270 The RFP refers to an attachment A, but did not include this attachment. Will you allow a questions period specific to the contract prior to the RFP submission deadline?
Attachment A is embedded in the RFP's PDF document. To access this attachment, you must open the PDF in Adobe Acrobat, not the web browser. No, we will not allow another round of questions. (See Q-154, Q-236, Q-269)
Q-271 Corporate Compliance – Are there any compliance trainings CCHHS will require outside of the following: HIPAA, FWA, DRA, Code of Ethics, Cultural Competency and Mandatory Abuse reporting?
CCHHS does not currently anticipate requiring additional trainings but reserves the right to add trainings as required by statute, regulation or contract.
Q-272 Grievance and Appeals – Will the Proposer use CCHHS’ systems and/or resources for the appeals process or does CCHHS anticipate that the Transportation Benefits Management Provider handle appeals from beginning to end?
For transportation services, CCHHS anticipates that the TPA will manage the appeal process using its systems and resources. The Transportation Benefits Manager will be required to cooperate and provide information, upon request, for the administration of the appeals process.
Q-273 The RFP states that “the ideal proposer will serve as a ‘broker’ or transportation services…” Does CCHHS anticipate that transportation services will include emergency and non-emergency transportation?
The scope of work for 7.6 is non-emergency transportation only. (See Q-274, Q-278)
Q-274 Would CCHHS consider a proposal that only provides the Non-Emergency Medical Transportation brokerage operation?
Yes. This is the scope of work that is desired. (See Q-273, Q-278)
Q-275 Scope of Work #6 - Will you please define UM as used in the first paragraph of section 7.6.1?
Utilization Management refers to the establishment of controls and monitoring processes related to the usage of transportation services by CountyCare members.
Q-276 Will you please expand on what is meant by “multiple product lines within one contracted service” in 7.6.2 #7?
CountyCare expects to expand beyond Medicaid-only members in the upcoming year. The successful proposer will be evaluated on their ability to service multiple products managed by one payor.

Page 37 of 38
ID Question CCHHS Response
Q-277 Does this refer to capacity and/or experience serving as a transportation broker that subcontracts with a network of providers to arrange different types of transportation such as bus passes, or trips via sedan, wheelchair, or ambulance, and so forth?
See Q-276
Q-278 Participation Requirements – Is the provider to manage both emergency and nonemergency transportation?
Non-emergency only. (See Q-273, Q-274)
Q-279 May the proposer also utilize a volunteer driver program, where friends/family of the participant received mileage reimbursement for providing transportation?
While CountyCare endorses this type of innovation, such services are allowed only to the extent it is consistent with the current Medicaid standards as detailed in the RFP or the current IL Medicaid Handbook for Transportation Benefits. (See Q-169)

Page 38 of 38
ADDENDUM ACKNOWLEDGEMENT FORM As required by the RFP, Proposers must submit this acknowledgement form with their response. One acknowledgement form per response, listing all addenda, is appropriate.
Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____ Addendum No.: _____
Company Name: _____________________________________________________________
Representative’s Name: ____________________________________________________________
Signature: ______________________________________________________________
Date: ______________________________________________________________ END OF ADDENDUM

CountyCare Claims: Volume By Primary Diagnoses
January to March, 2015
Primary Dx by Specialty by ED Visits
Primary Dx by Dx Category Groups by ED Visits*
* ≥50 ED & ≥50 Inpatient encounters

Primary Dx by Specialty by Inpatient Encounters
Primary Dx by Dx Category Groups by Inpatient Encounters*
* ≥50 ED & ≥50 Inpatient encounters

Primary Dx by Specialty by Claims Amount
Primary Dx by Dx Category Groups by Claims Amount*
* ≥50 ED & ≥50 Inpatient encounters

Primary Dx by Specialty by Distinct Members
Primary Dx by Dx Category Groups by Distinct Members*
* ≥50 ED & ≥50 Inpatient encounters

Apr 2015 May 2015 Jun 2015 Apr 2015 May 2015 Jun 2015 Apr 2015 May 2015 Jun 2015
$520,902 $508,143 $493,074 $872,014 $843,497 $835,318 $19,685 $13,157 $17,203
4,371 3,989 4,003 7,714 7,194 6,824 145 107 119
4,303 3,898 3,968 7,572 7,016 6,652 154 108 120
3,519 3,214 3,198 6,760 6,353 5,841 110 86 95
14,778 13,504 13,125 31,361 29,059 27,059 559 377 396
456 474 468 885 875 856 88 79 76
83,850 79,499 72,793 97,591 105,234 102,555 2,740 2,810 2,830
4.20% 4.04% 4.39% 12.87% 11.47% 10.90% 6.77% 6.58% 7.52%
$119.17 $127.39 $123.18 $113.04 $117.25 $122.41 $135.76 $122.97 $144.56
$121.06 $130.36 $124.26 $115.16 $120.22 $125.57 $127.83 $121.83 $143.35
$148.03 $158.10 $154.18 $251.33 $258.11 $280.09 $280.85 $311.18 $339.18
$35.25 $37.63 $37.57 $55.59 $57.68 $61.09 $53.36 $83.16 $84.80
$1,142 $1,072 $1,054 $1,786 $1,795 $1,855 $328 $325 $365
3.50 3.49 3.38 4.29 4.30 4.13 3.93 3.64 3.37
3.55 3.58 3.41 4.37 4.41 4.24 3.70 3.60 3.34
4.20 4.20 4.10 9.04 8.95 9.16 10.73 7.69 7.99
7.73 6.80 6.85 7.65 7.28 6.83 1.25 1.09 1.25
$168 $275$8,086 $6,634
Claim Dollars Per Service by
Category
Adjunctive General
$7,734
Average Paid Per Provider
Unique Patients Per Provider
Average Services Per Claim
Average Services Per Visit
$12,068 $13,248
Average Services Per Patient
Access Rate
Claim Metrics
Average Paid Per Claim
Average Paid Per Visit
Average Paid Per Patient
Average Paid Per Service
Visits
Patients
Services
Billing Providers
Membership by Subgroup
Membership Count
$13,656
ICP
$347
Total Paid
FHPACA
Metrics
Claims

$199,335 $167,456 $172,975 $270,068 $240,986 $236,341 $5,094 $4,089 $4,121
$6,138 $5,592 $5,059 $9,900 $9,674 $11,772 $682 $136 $273
$0 $0 $0 $0 $0 $0 $0 $0 $0
$0 $0 $0 $0 $0 $504 $0 $0 $0
$113,939 $109,699 $97,975 $43,624 $48,030 $50,749 $6,055 $2,817 $2,013
$0 $0 $0 $52,570 $79,442 $106,377 $0 $0 $150
$0 $0 $1,496 $1,300 $1,765 $3,153 $0 $488 $0
$5,461 $9,033 $9,825 $329,495 $299,254 $231,586 $233 $294 $224
$0 $0 $33 $0 $0 $499 $0 $0 $0
$71,520 $79,150 $84,654 $9,184 $8,717 $9,155 $3,237 $2,705 $6,774
$116,423 $130,579 $113,324 $143,804 $142,380 $171,526 $4,037 $2,459 $3,373
$520,902 $508,143 $493,074 $872,014 $843,497 $835,318 $19,685 $13,157 $17,203
199 155 187 368 408 419 7 4 5
8,412 7,393 7,355 16,177 14,837 13,818 312 233 242
47 41 38 127 133 159 5 1 2
0 0 0 0 0 0 0 0 0
0 0 0 0 0 1 0 0 0
2,753 2,549 2,287 1,001 1,091 1,120 131 65 56
0 0 0 220 264 331 0 0 1
1 3 17 28 37 62 0 4 0
351 474 550 10,220 9,194 7,414 10 14 9
0 0 1 0 0 3 0 0 0
213 223 234 28 24 32 13 10 18
2,802 2,666 2,456 3,192 3,071 3,700 81 46 63Restorative
Oral Maxillofacial Surgery
Orthodontics
Periodontics
Preventive
Prosthodontics - Fixed
Prosthodontics - Removable
Approved Services by
Category
Adjunctive General
Diagnostic
Endodontics
Implant Services
Maxillofacial Prosthetics
Periodontics
Preventive
Prosthodontics - Fixed
Prosthodontics - Removable
Restorative
Total Claim Dollars
Diagnostic
Endodontics
Implant Services
Maxillofacial Prosthetics
Oral Maxillofacial Surgery
Orthodontics
$168 $275$8,086 $6,634
Adjunctive General
$7,734 $12,068 $13,248 $13,656 $347

14,778 13,504 13,125 31,361 29,059 27,059 559 377 396
2.37 1.95 2.57 3.77 3.88 4.09 2.55 1.42 1.77
100.32 92.99 101.04 165.76 140.99 134.74 113.87 82.92 85.51
0.56 0.52 0.52 1.30 1.26 1.55 1.82 0.36 0.71
0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0.00 0.00 0.00 0.00 0.00 0.01 0.00 0.00 0.00
32.83 32.06 31.42 10.26 10.37 10.92 47.81 23.13 19.79
0.00 0.00 0.00 2.25 2.51 3.23 0.00 0.00 0.35
0.01 0.04 0.23 0.29 0.35 0.60 0.00 1.42 0.00
4.19 5.96 7.56 104.72 87.37 72.29 3.65 4.98 3.18
0.00 0.00 0.01 0.00 0.00 0.03 0.00 0.00 0.00
2.54 2.81 3.21 0.29 0.23 0.31 4.74 3.56 6.36
33.42 33.54 33.74 32.71 29.18 36.08 29.56 16.37 22.26
176.24 169.86 180.31 321.35 276.14 263.85 204.01 134.16 139.93
$40.63 $42.80 $41.36 $32.79 $32.47 $32.59 $49.59 $42.02 $55.00
$23.70 $22.65 $23.52 $16.69 $16.24 $17.10 $16.33 $17.55 $17.03
$130.60 $136.40 $133.14 $77.95 $72.74 $74.04 $136.40 $136.40 $136.40
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $503.50 $0.00 $0.00 $0.00
$41.39 $43.04 $42.84 $43.58 $44.02 $45.31 $46.22 $43.34 $35.95
$0.00 $0.00 $0.00 $238.96 $300.92 $321.38 $0.00 $0.00 $150.00
$0.00 $0.00 $88.00 $46.44 $47.71 $50.86 $0.00 $122.00 $0.00
$15.56 $19.06 $17.86 $32.24 $32.55 $31.24 $23.29 $21.02 $24.93
$0.00 $0.00 $32.90 $0.00 $0.00 $166.23 $0.00 $0.00 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$41.55 $48.98 $46.14 $45.05 $46.36 $46.36 $49.84 $53.47 $53.53
$35.25 $37.63 $37.57 $27.81 $29.03 $30.87 $35.21 $34.90 $43.44
$2.30 $2.06 $2.42 $1.79 $2.09 $2.34 $3.16 $1.95 $2.89
$56.65 $52.10 $54.09 $39.95 $37.93 $40.46 $46.31 $47.54 $43.37
$1.74 $1.74 $1.58 $1.46 $1.52 $2.02 $6.20 $1.59 $2.87
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $0.09 $0.00 $0.00 $0.00
Paid Per Patient
Adjunctive General
Diagnostic
Endodontics
Implant Services
Maxillofacial Prosthetics
Periodontics
Preventive
Prosthodontics - Fixed
Prosthodontics - Removable
Restorative
Average Paid Per Service
Diagnostic
Endodontics
Implant Services
Maxillofacial Prosthetics
Oral Maxillofacial Surgery
Orthodontics
Prosthodontics - Fixed
Prosthodontics - Removable
Restorative
Services Per 1000 Members
Average Paid Per Service
Adjunctive General
Implant Services
Maxillofacial Prosthetics
Oral Maxillofacial Surgery
Orthodontics
Periodontics
Preventive
Total Services
Services Per 1000 Members
Adjunctive General
Diagnostic
Endodontics

$32.38 $34.13 $30.64 $6.45 $7.56 $8.69 $55.04 $32.76 $21.19
$0.00 $0.00 $0.00 $7.78 $12.50 $18.21 $0.00 $0.00 $1.58
$0.00 $0.00 $0.47 $0.19 $0.28 $0.54 $0.00 $5.67 $0.00
$1.55 $2.81 $3.07 $48.74 $47.10 $39.65 $2.12 $3.42 $2.36
$0.00 $0.00 $0.01 $0.00 $0.00 $0.09 $0.00 $0.00 $0.00
$20.32 $24.63 $26.47 $1.36 $1.37 $1.57 $29.42 $31.45 $71.31
$33.08 $40.63 $35.44 $21.27 $22.41 $29.37 $36.70 $28.60 $35.50
$148.03 $158.10 $154.18 $129.00 $132.77 $143.01 $178.96 $152.99 $181.08
$0.10 $0.08 $0.11 $0.12 $0.13 $0.13 $0.13 $0.06 $0.10
$2.38 $2.11 $2.38 $2.77 $2.29 $2.30 $1.86 $1.46 $1.46
$0.07 $0.07 $0.07 $0.10 $0.09 $0.11 $0.25 $0.05 $0.10
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$1.36 $1.38 $1.35 $0.45 $0.46 $0.49 $2.21 $1.00 $0.71
$0.00 $0.00 $0.00 $0.54 $0.75 $1.04 $0.00 $0.00 $0.05
$0.00 $0.00 $0.02 $0.01 $0.02 $0.03 $0.00 $0.17 $0.00
$0.07 $0.11 $0.13 $3.38 $2.84 $2.26 $0.09 $0.10 $0.08
$0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
$0.85 $1.00 $1.16 $0.09 $0.08 $0.09 $1.18 $0.96 $2.39
$1.39 $1.64 $1.56 $1.47 $1.35 $1.67 $1.47 $0.88 $1.19
$6.21 $6.39 $6.77 $8.94 $8.02 $8.15 $7.18 $4.68 $6.08
Prosthodontics - Fixed
Prosthodontics - Removable
Restorative
Total Cost PMPM
Implant Services
Maxillofacial Prosthetics
Oral Maxillofacial Surgery
Orthodontics
Periodontics
Preventive
Restorative
Average Paid Per Patient
Cost PMPM
Adjunctive General
Diagnostic
Endodontics
Oral Maxillofacial Surgery
Orthodontics
Periodontics
Preventive
Prosthodontics - Fixed
Prosthodontics - Removable

Risk Stratification
August, 2015
ACHN: Ambulatory Care Health Network (Primary care clinic system of the Cook County Health & Hospital System)
MHN ACO: Medical Home Network Accountable Care Organization
Access: Access Community Health Network (FQHC)
Members
% Risk Stratified
TARGET = 60%
% High Risk of all mbrs*
% Risk Stratified
TARGET = 60%
% High Risk of all mbrs*
% Pop HRS/HRA TARGET = 80% % High Risk
% Pop HRS/HRA
TARGET = 80%% High Risk
ACHN 32,903 35% 1.8% 62% 0.5% 77% 30.0% 50% 92%MHN ACO 79,204 71% 5.0% n/a n/a n/a n/a 28% 32%Access 26,929 28% 1.3% 60% 0.3% 85% 33.3% 56% 94%All other 31,893 31% 1.3% 55% 0.3% 79% 26.8% 46.2% 92%Total 170,929 51% 3.2% 59% 0.4% 79% 29.7% 44% 77.8%* includes high, mod, low and unknown
Members
Actual Target Actual Target Actual TargetSPD-All Members 3,047 37% 2.3% 5%ACA-All Members 79,402 51% 4.2% 2% 70% 8.5% 15%* 42% 2.1% 2%FHP-All Members 88,236 51% 2.3% 2% 72% 3.4% 15%* 13% 0.4% 2%ACA & FHP 167,638 51% 3.2% 2% 71% 5.0% 15%* 31% 1.5% 2%Total 170,685 51% 3.2%
MHN Providers
Transplant Caseload: All Products
New Members: All Products, in May
High Utilizers (Top 1%): All Products
Full Population: All Products, All members
% Pop HRS/HRA
% Pop HRS/HRA
% High Risk
All Network PC Providers
% High Risk % High Risk
Non-MHN Providers
% Pop HRS/HRA

CountyCare Pharmacy ClaimsMay to July, 2015
Total Claims ACA FHP ICP Unknown Total
May-15 131,178 42,149 6,754 279 180,360
Jun-15 118,641 41,640 6,631 187 167,099
Jul-15 118,435 39,904 6,904 60 165,303
Total 368,254 123,693 20,289 526 512,762
Total Paid (Ingredient & Dispensing) ACA FHP ICP Unknown Total
May-15 $11,940,141 $2,378,516 $974,646 $13,523 $15,306,825
Jun-15 $11,632,168 $2,524,467 $1,185,248 $11,714 $15,353,597
Jul-15 $11,453,248 $2,406,133 $1,230,339 $611 $15,090,331
Total $35,025,557 $7,309,115 $3,390,233 $25,848 $45,750,753
Drug Category (GPI-2) Total Paid
Ave Per
Claim Claims
Distinct
Members
ANTIVIRALS 14,926,712$ 1,370$ 10,899 3,108
ANTIDIABETICS 5,155,846$ 174$ 29,697 11,322
ANTIASTHMATIC AND BRONCHODILATOR AGENTS 4,493,102$ 127$ 35,510 12,578
HEMATOLOGICAL AGENTS - MISC. 2,845,410$ 2,187$ 1,301 822
ANALGESICS - ANTI-INFLAMMATORY 1,897,437$ 70$ 27,100 19,591
ANTINEOPLASTICS 1,664,379$ 1,131$ 1,472 632
PSYCHOTHERAPEUTIC AND NEUROLOGICAL AGENTS - MISC. 1,013,711$ 292$ 3,473 1,898
ANTICONVULSANTS 1,004,604$ 67$ 15,009 6,977
ANTIPSYCHOTICS/ANTIMANIC AGENTS 967,266$ 124$ 7,783 3,136
DIAGNOSTIC PRODUCTS 941,336$ 120$ 7,845 5,423
DERMATOLOGICALS 931,458$ 40$ 23,098 12,353
GASTROINTESTINAL AGENTS - MISC. 820,053$ 402$ 2,041 1,164
ANTIHYPERTENSIVES 574,448$ 22$ 26,362 17,094
CONTRACEPTIVES 547,066$ 42$ 12,948 6,322
HEMATOPOIETIC AGENTS 455,341$ 59$ 7,708 4,609
ASSORTED CLASSES 410,352$ 520$ 789 277
ANTIDEPRESSANTS 398,037$ 17$ 23,328 10,237
ANTIHYPERLIPIDEMICS 389,054$ 21$ 18,119 12,285
ANTICOAGULANTS 379,760$ 151$ 2,514 991
OPHTHALMIC AGENTS 362,674$ 43$ 8,343 4,186
ENDOCRINE AND METABOLIC AGENTS - MISC. 362,142$ 398$ 909 514
ANALGESICS - OPIOID 357,275$ 16$ 22,020 12,359
CALCIUM CHANNEL BLOCKERS 317,420$ 23$ 13,584 9,289
MEDICAL DEVICES 289,541$ 15$ 19,013 7,204
ULCER DRUGS 262,368$ 17$ 15,690 9,679
PROGESTINS 232,623$ 362$ 643 410
CARDIOVASCULAR AGENTS - MISC. 232,257$ 4,075$ 57 24
VASOPRESSORS 229,673$ 351$ 655 499
ANTI-INFECTIVE AGENTS - MISC. 220,510$ 25$ 8,663 6,650
BETA BLOCKERS 212,749$ 20$ 10,529 7,163
NASAL AGENTS - SYSTEMIC AND TOPICAL 184,652$ 20$ 9,382 5,833
ADHD/ANTI-NARCOLEPSY/ANTI-OBESITY/ANOREXIANTS 181,205$ 103$ 1,754 770
DIURETICS 138,175$ 9$ 16,254 11,007
MUSCULOSKELETAL THERAPY AGENTS 129,876$ 22$ 5,861 4,370
VAGINAL PRODUCTS 126,242$ 63$ 2,011 1,475
ANTIFUNGALS 122,129$ 26$ 4,616 3,270
THYROID AGENTS 119,153$ 24$ 4,979 3,110
PENICILLINS 118,568$ 11$ 10,746 8,875
ANTIMALARIALS 106,212$ 180$ 590 388
URINARY ANTISPASMODICS 98,330$ 89$ 1,111 535
TETRACYCLINES 94,407$ 58$ 1,638 1,210
VACCINES 90,236$ 127$ 710 498
GENITOURINARY AGENTS - MISCELLANEOUS 87,455$ 33$ 2,643 1,543
MACROLIDES 84,963$ 24$ 3,550 3,091
DIGESTIVE AIDS 80,577$ 370$ 218 86
CORTICOSTEROIDS 68,537$ 10$ 6,720 4,392
MULTIVITAMINS 65,523$ 11$ 6,140 3,404
MINERALS & ELECTROLYTES 63,360$ 12$ 5,361 3,302
LAXATIVES 63,156$ 7$ 8,536 5,389
OTIC AGENTS 59,489$ 46$ 1,290 1,073
ANTIANXIETY AGENTS 57,475$ 7$ 8,841 4,517
ESTROGENS 51,517$ 85$ 605 272
ANTIHISTAMINES 47,340$ 5$ 9,670 6,645
MIGRAINE PRODUCTS 46,524$ 49$ 941 523
ANTIEMETICS 43,892$ 16$ 2,793 2,041
URINARY ANTI-INFECTIVES 42,196$ 39$ 1,092 940
GOUT AGENTS 36,329$ 32$ 1,125 680
ANTIANGINAL AGENTS 34,502$ 38$ 910 538
ANALGESICS - NonNarcotic 33,494$ 3$ 13,344 9,931
CEPHALOSPORINS 31,949$ 14$ 2,321 2,044
TOXOIDS 31,751$ 54$ 585 528
ANDROGENS-ANABOLIC 27,500$ 141$ 195 82
FLUOROQUINOLONES 24,226$ 10$ 2,444 2,094
VITAMINS 24,151$ 3$ 7,165 4,764
ANTIPARKINSON AGENTS 22,578$ 29$ 783 370
ANTIDOTES 22,185$ 152$ 146 79
CARDIOTONICS 20,623$ 65$ 316 219
HYPNOTICS 19,276$ 10$ 1,868 925
COUGH/COLD/ALLERGY 18,815$ 8$ 2,244 1,624
RESPIRATORY AGENTS - MISC. 17,289$ 2,881$ 6 2
MOUTH/THROAT/DENTAL AGENTS 17,020$ 10$ 1,638 1,240
ANTIMYCOBACTERIAL AGENTS 15,156$ 54$ 283 146
ANORECTAL AGENTS 14,834$ 35$ 422 317
ANTIARRHYTHMICS 14,282$ 89$ 161 100
PASSIVE IMMUNIZING AGENTS 12,274$ 682$ 18 11
CHEMICALS 10,006$ 417$ 24 14
PHARMACEUTICAL ADJUVANTS 6,789$ 323$ 21 14
ANTIDIARRHEALS 6,298$ 15$ 426 311
OXYTOCICS 4,906$ 149$ 33 32
!Unknown! 4,075$ 11$ 380 278
HEMOSTATICS 3,933$ 131$ 30 15
NUTRIENTS 3,435$ 18$ 195 103
ANTIMYASTHENIC AGENTS 3,085$ 106$ 29 10
ANTHELMINTICS 1,042$ 74$ 14 11
ANTISEPTICS & DISINFECTANTS 984$ 7$ 134 94
ANTACIDS 683$ 3$ 203 134
NEUROMUSCULAR AGENTS 486$ 243$ 2 1
DIETARY PRODUCTS/DIETARY MANAGEMENT PRODUCTS 337$ 337$ 1 1
ALTERNATIVE MEDICINES 268$ 3$ 103 62
SULFONAMIDES 207$ 52$ 4 1
AMINOGLYCOSIDES 185$ 5$ 34 26
LOCAL ANESTHETICS-Parenteral 6$ 6$ 1 1

Direct Report Indirect Report
Jay Shannon, MDCEO
Doug ElwellDeputy CEO, Finance & Strategy
Steven GlassExecutive Director
Andrea McGlynn, RNDir, Clinical Services
Case/Disease Mgt Program Mgr
Justine Morton, RNMgr, Quality & Credentiling
Mgr, Social Programs
Michelle Brown-Graham, RNClinical Case Manager
Silvia WiseAA IV
Elmer Abbo, MDMedical Director
Dir. Enrollment & Outreach
Gretchen GrieserInterim Mgr, Enrollment &
Retention
Heather HolbergMgr, Enrollment & Retention
Jerry KiplingerDir, Operations
Mgr, Operations
Reports Manager
Ryan Tyrell LipinskiCorporate Compliance Ofcr
Aaron GaleenerDir, Finance
Sr. Financial Analyst
Yvette Blakely-Alexander
AA V
Position Filled
Hiring in Process
Key:
Organizational Chart
Updated: Aug’15
Dajuana ParmoreBusiness Manager III
Jeanne KleinMgr, Provider
Relations
Danielle DeanAA IV
Analyst V
Financial Analyst
Tina BarksdaleDir, Business Development
Accreditation Project Manager
Compliance Manager
AA III