Embed Size (px)
Citation preview

19 November 1965, Volume 150, Number 3699
I
Pain Mechanisms: A New Theory
A gate control system modulates sensory input from theskin before it evokes pain perception and response.
Ronald Melzack and Patrick D. Wall
The nature of pain has been thesubject of bitter controversy since theturn of the century (1). There arecurrently two opposing theories ofpain: (i) specificity theory, whichholds that pain is a specific modalitylike vision or hearing, "with its owncentral and peripheral apparatus" (2),and (ii) pattern theory, which main-tains that the nerve impulse patternfor pain is produced by intense stimu-lation of nonspecific receptors since"there are no specific fibers and nospecific endings" (3). Both theories de-rive from earlier concepts proposed byvon Frey (4) and Goldscheider (5)in 1894, and historically they are heldto be mutually exclusive. Since it isour purpose here to propose a newtheory of pain mechanisms, we shallstate explicitly at the outset where weagree and disagree with specificity andpattern theories.
Specificity Theory
Specificity theory proposes that amosaic of specific pain receptors inbody tissue projects to a pain centerin the brain. It maintains that freenerve endings are pain receptors (4)and generate pain impulses that arecarried by A-delta and C fibers inperipheral nerves (6) and by the lat-eral spinothalamic tract in the spinalcord (2) to a pain center in thethalamus (7). Despite its apparentsimplicity, the theory contains an ex-plicit statement of physiological spe-
19 NOVEMBER 1965
cialization and an implicit psychologi-cal assumption (8, 9). Consider theproposition that the skin contains "painreceptors." To say that a receptor re-sponds only to intense, noxious stimu-lation of the skin is a physiologicalstatement of fact; it says that the re-ceptor is specialized to respond to aparticular kind of stimulus. To call areceptor a "pain receptor," however,is a psychological assumption: it im-plies a direct connection from the re-ceptor to a brain center where pain isfelt (Fig. 1), so that stimulation ofthe receptor must always elicit painand only the sensation of pain. Thisdistinction between physiological spe-cialization and psychological assump-tion also applies to peripheral fibersand central projection systems (9).
The facts of physiological speciali-zation provide the power of specificitytheory. Its psychological assumption isits weakness. As in all psychologicaltheories, there is implicit in specificitytheory the conception of a nervoussystem; and the model is that of afixed, direct-line communication sys-tem from the skin to the brain. Thisfacet of specificity theory, which im-putes a direct, invariant relationshipbetween stimulus and sensation, is ex-amined here in the light of the clini-cal, psychological, and physiologicalevidence concerning pain.
Clinical evidence. The pathologicalpain states of causalgia (a severe burn-ing pain that may result from a par-tial lesion of a peripheral nerve),phantom limb pain (which may occur
after amputation of a limb), and theperipheral neuralgias (which may oc-cur after peripheral nerve infections ordegenerative diseases) provide a dra-matic refutation of the concept of afixed, direct-line nervous system. Fourfeatures of these syndromes plague pa-tient, physician, and theorist (8, 10).
1) Surgical lesions of the peripheraland central nervous system have beensingularly unsuccessful in abolishingthese pains permanently, although thelesions have been made at almost everylevel (Fig. 2). Even after such opera-tions, pain can often still be elicitedby stimulation below the level of sec-tion and may be more severe thanbefore the operation (8, 10).
2) Gentle touch, vibration, andother nonnoxious stimuli (8, 10) cantrigger excruciating pain, and some-times pain occurs spontaneously forlong periods without any apparentstimulus. The fact that the thresholdsto these stimuli are raised rather thanlowered in causalgia and the neuralgias(10), together with the fact that re-ferred pain can often be triggered bymild stimulation of normal skin (8),makes it unlikely that the pains canbe explained by postulating pathologi-cally hypersensitive "pain receptors."
3) The pains and new "triggerzones" may spread unpredictably to un-related parts of the body where nopathology exists (8, 11).
4) Pain from hyperalgesic skinareas often occurs after long delays,and continues long after removal ofthe stimulus (10). Gentle rubbing, re-peated pin pricks, or the applicationof a warm test tube may produce sud-den, severe pain after delays as longas 35 seconds. Such delays cannot beattributed simply to conduction inslowly conducting fibers; rather, theyimply a remarkable temporal and spa-tial summation of inputs in the pro-duction of these pain states (5, 10).
Psychological evidence. The psycho-logical evidence fails to support theassumption of a one-to-one relation-
Dr. Melzack is associate professor in the de-partment of psychology at McGill University,Montreal, Canada. Dr. Wall is professor in thedepartment of biology at the Massachusetts In-stitute of Technology. Cambridge.
971

ship between pain perception and in-tensity of the stimulus. Instead, theevidence suggests that the amount andquality of perceived pain are deter-mined by many psychological varia-bles (12) in addition to the sensoryinput. For example, Beecher (13) hasobserved that most American soldierswounded at the Anzio beachhead "en-tirely denied pain from their extensivewounds or had so little that they didnot want any medication to relieve it"(13, p. 165), presumably becausethey were overjoyed at having escapedalive from the battlefield (25). If themen had felt pain, even pain sensa-tion devoid of negative affect, theywould, it is reasonable to assume, havereported it, just as lobotomized patients(14) report that they still have painbut it does not bother them. Instead,these men "entirely denied pain." Simi-larly, Pavlov's (15, 16) dogs thatreceived electric shocks, burns, or cuts,followed consistently by the presenta-tion of food, eventually responded tothese stimuli as signals for food andfailed to show "even the tiniest andmost subtle" (15, p. 30) signs ofpain. If these dogs felt pain sensation,then it must have been nonpainful pain(17), or the dogs were out to foolPavlov and simply refused to revealthat they were feeling pain. Both pos-sibilities, of course, are absurd. Theinescapable conclusion from these ob-servations is that intense noxious stim-ulation can be prevented from produc-ing pain, or may be modified to pro-vide the signal for eating behavior.
Psychophysical studies (18) thatfind a mathematical relationship be-tween stimulus intensity and pain in-tensity are often cited (2, 13, 18, 19)as supporting evidence for the assump-tion that pain is a primary sensationsubserved by a direct communicationsystem from skin receptor to pain cen-ter. A simple psychophysical func-tion, however, does not necessarily re-flect equally simple neural mechanisms.Beecher's (13) and Pavlov's (25) ob-servations show that activities in thecentral nervous system may intervenebetween stimulus and sensation whichmay invalidate any simple psycho-physical "law." The use of laboratoryconditions that prevent such activitiesfrom ever coming into play reducesthe functions of the nervous systemto those of a fixed-gain transmissionline. It is under these conditions thatpsychophysical functions prevail.
Physiological evidence. There is
Fig. 1. Descartes' (76) concept of the painpathway. He writes: "If for example fire(A) comes near the foot (B), the minuteparticles of this fire, which as you knowmove with great velocity, have the powerto set in motion the spot of the skin ofthe foot which they touch, and by thismeans pulling upon the delicate threadCC, which is attached to the spot of theskin, they open up at the same instant thepore, d.e., against which the delicatethread ends, just as by pulling at one endof a rope one makes to strike at the sameinstant a bell which hangs at the otherend."
convincing physiological evidence thatspecialization exists within the somes-thetic system (9), but none to showthat stimulation of one type of re-ceptor, fiber, or spinal pathway elicitssensations only in a single psychologi-cal modality. In the search for periph-eral fibers that respond exclusively tohigh-intensity stimulation, Hunt andMclntyre (20) found only seven outof 421 myelinated A fibers, and Ma-ruhashi et al. (21) found 13 out ofseveral hundred. Douglas and Ritchie(22) failed to find any high-thresholdC fibers, while Iggo (23) found afew. These data suggest that a smallnumber of specialized fibers may existthat respond only to intense stimula-tion, but this does not mean that theyare "pain fibers"—that they must al-ways produce pain, and only pain,when they are stimulated. It is morelikely that they represent the extremeof a continuous distribution of re-ceptor-fiber thresholds rather than aspecial category (24).
Similarly, there is evidence thatcentral-nervous-system pathways havespecialized functions that play a rolein pain mechanisms. Surgical lesionsof the lateral spinothalamic tract (2)or portions of the thalamus (25) may,
on occasion, abolish pain of pathologi-cal origin. But the fact that these areascarry signals related to pain does notmean that they comprise a specific painsystem. The lesions have multiple ef-fects. They reduce the total number ofresponding neurons; they change thetemporal and spatial relationshipsamong all ascending systems; and theyaffect the descending feedback thatcontrols transmission from peripheralfibers to dorsal horn cells.
The nature of the specialization ofcentral cells remains elusive despite thelarge number of single-cell studies.Cells in the dorsal horns (24, 26) andthe trigeminal nucleus (27) respondto a wide range of stimuli and re-spond to each with a characteristic fir-ing pattern. Central cells that respondexclusively to noxious stimuli have alsobeen reported (28, 29). Of particularinterest is Poggio and Mountcastle's(28) study of such cells in the pos-terior thalamus in anesthetized mon-keys. Yet Casey (30), who has re-cently confirmed that posteriorthalamic cells respond exclusively tonoxious stimuli in the drowsy orsleeping monkey, found that- the samecells also signaled information in re-sponse to gentle tactile stimulationwhen the animal was awake. Even ifsome central cells should be shownunequivocally to respond exclusivelyto noxious stimuli, their specializedproperties still do not make them "paincells." It is more likely that these cellsrepresent the extreme of a broad dis-tribution of cell thresholds to periph-eral nerve firing, and that they occupy 'only a small area within the total mul-tidimensional space that defines thespecialized physiological properties ofcells (9). There is no evidence to sug-gest that they are more important forpain perception and response than all >the remaining somesthetic cells that sig-nal characteristic firing patterns aboutmultiple properties of the stimulus, in-cluding noxious intensity. The view thatonly the cells that respond exclusivelyto noxious stimuli subserve pain andthat the outputs of all other cells areno more than background noise ispurely a psychological assumption andhas no factual basis. Physiological spe-cialization is a fact that can be re-tained without acceptance of the psy- ,chological assumption that pain is de- <termined entirely by impulses in astraight-through transmission systemfrom the skin to a pain center in thebrain.
SCIENCE, VOL. 150

'altern Theory
As a reaction against the psychologi-:al assumption in specificity theory,jew theories have been proposedvhich can be grouped under the gen-:ral heading of "pattern theory." Gold-icheider (5), initially one of the;hampions of von Frey's theory, was:he first to propose that stimulus in-ensity and central summation are thecritical determinants of pain. Twokinds of theories have emerged fromSoldscheider's concept; both recognizethe concept of patterning of the input,which we believe (9) to be essentialfor any adequate theory of pain, butone kind ignores the facts of physio-logical specialization, while the otherutilizes them in proposing mechanismsof central summation.
The pattern theory of Weddell (31)and Sinclair (3) is based on the earliersuggestion, by Nafe (17), that allcutaneous qualities are produced byspatiotemporal patterns of nerve im-pulses rather than by separate modal-ity-specific transmission routes. Thetheory proposes that all fiber endings(apart from those that innervate haircells) are alike, so that the pattern forpain is produced by intense stimulationof nonspecific receptors. The physio-logical evidence, however, reveals (9)a high degree of receptor-fiber spe-cialization. The pattern theory pro-posed by Weddell and Sinclair, then,fails as a satisfactory theory of painbecause it ignores the facts of physio-logical specialization. It is more rea-sonable to assume that the specializedphysiological properties of each re-ceptor-fiber unit—such as responseranges, adaptation rates, and thresholdsto different stimulus intensities—playan important role in determining thecharacteristics of the temporal patternsthat are generated when a stimulus isapplied to the skin (9).
Other theories have been proposed,within the framework of Goldschei-der's concept, which stress central sum-mation mechanisms rather than ex-cessive peripheral stimulation. Living-ston (8) was perhaps the first to sug-gest specific neural mechanisms to ac-count for the remarkable summationphenomena in clinical pain syndromes.He proposed that intense, patho-logical stimulation of the body sets upreverberating circuits in spinal inter-nuncial pools, or evokes spinal cordactivities such as those reflected by the"dorsal root reflex" (32), that can
19 NOVEMBER 1965
then be triggered by normally non-noxious inputs and generate abnormalvolleys that are interpreted centrally aspain. Conceptually similar mechanismswere proposed by Hebb (33) and Ge-rard (34), who suggested that hyper-synchronized firing in central cellsprovides the signal for pain.
Related to theories of central sum-mation is the theory that a specializedinput-controlling system normally pre-vents summation from occurring, andthat destruction of this system leads topathological pain states. Basically, thistheory proposes the existence of arapidly conducting fiber system which
" • *
\
i
: o
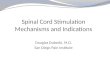
Fig. 2. MacCarty and Drake's (77) schematic diagram illustrating various surgicalprocedures designed to alleviate pain: 1, gyrectomy; 2, prefrontal lobotomy; 3, thaia-motomy; 4, mesencephalic tractotomy; 5, hypophysectomy; 6, fifth-nerve rhizotomy; 7,ninth-nerve neurectomy; 8, medullary tractotomy; 9, trigeminal tractotomy; 10, cervicalchordotomy; 11, thoracic chordotomy; 12, sympathectomy; 13, myelotomy; 14, Lissauertractotomy; 15, posterior rhizotomy; 16, neurectomy.
973

inhibits synaptic transmission in amore slowly conducting system thatcarries the signal for pain. These twosystems are identified as the epicriticand protopathic (7), fast and slow(35), phylogenetically new and old
(36), and myelinated and unmyeli-nated (10) fiber systems. Under patho-logical conditions, the slow system es-tablishes dominance over the fast, andthe result is protopathic sensation(7), slow pain (55), diffuse burning
pain (36), of hyperalgesia (10). It isimportant to note the transition fromspecificity theory (7, 35, 36) to thepattern concept: Noordenbos (10)does not associate psychological qual-ity with each system but attributes tothe rapidly conducting system the abil-ity to modify the input pattern trans-mitted in the slowly conducting, mul-tisynaptic system.
The concepts of central summationand input control have shown remark-able power in their ability to explainmany of the clinical phenomena ofpain. The various specific theoreticalmechanisms that have 'been proposed,however, fail to comprise a satisfac-tory general theory of pain. They lackunity, and no single theory so far pro-posed is capable of integrating the di-verse theoretical mechanisms. Moreimportant, these mechanisms have notreceived any substantial experimentalverification. We believe that recentphysiological evidence on spinal mech-anisms, together with the evidencedemonstrating central control over af-ferent input, provides the basis for anew theory of pain mechanisms thatis consistent with the concepts ofphysiological specialization as well aswith those of central summation andinput control.
Fig. 3. (Top) A histological section of the cat spinal cord (lumbar region). (Middle")Cross section of the dorsal quadrant. The stippled region is the substantia gelatinosa.(Bottom) Main components of the cutaneous afferent system in the upper dorsal horn.The large-diameter cutaneous peripheral fibers are represented by thick lines runningfrom the dorsal root and terminating in the region of the substantia gelatinosa; one ofthese, as shown, sends a branch toward the brain in the dorsal column. The finerperipheral fibers are represented by dashed lines running directly into the substantiagelatinosa. The large cells, on which cutaneous afferent nerves terminate, are shown aslarge black spheres with their dendrites extending into the substantia gelatinosa and theiraxons projecting deeper into the dorsal horn. The open circles represent the cells of thesubstantia gelatinosa. The axons (not shown) of these cells connect them to one anotherand also run in the Lissauer tract (LT) to distant parts of the substantia gelatinosa.[From Wall (37)]
Gate Control Theory of Pain
Stimulation of the skin evokes nerveimpulses that are transmitted to threespinal cord systems (Fig. 3): the cellsof the substantia gelatinosa in the dor-sal horn, the dorsal-column fibers thatproject toward the brain, and the firstcentral transmission (T) cells in thedorsal horn. We propose that (i) thesubstantia gelatinosa functions as agate control system that modulates theafferent patterns before they influencethe T cells; (ii) the afferent patternsin the dorsal column system act, inpart at least, as a central control trig-ger which activates selective brainprocesses that influence the modulat-ing properties of the gate control sys-tem; and (iii) the T cells activateneural mechanisms which comprise theaction system responsible for responseand perception. Our theory proposesthat pain phenomena are determinedby interactions among these threesystems.
Gate control system. The substantiagelatinosa consists of small, denselypacked cells that form a functionalunit extending the length of the spinal
974 SCIENCE, VOL. 150

;ord. The cells connect with one an-other by short fibers and by the longerSbers of Lissauer's tract (37, 38), butdo not project outside the substantiaEjelatinosa. Recent evidence (39) sug-gests that the substantia gelatinosa actsas a gate control system that modu-lates the synaptic transmission of nerveimpulses from peripheral fibers to cen-tral cells.
Figure 4 shows the factors involvedin the transmission of impulses fromperipheral nerve to T cells in the cord.Recent studies (39-41) have shownthat volleys of nerve impulses in largefibers are extremely effective initiallyin activating the T cells but that theirlater effect is reduced by a negativefeedback mechanism. In contrast, vol-leys in small fibers activate a positivefeedback mechanism which exaggeratesthe effect of arriving impulses. Experi-ments (37, 39, 41) have shown thatthese feedback effects are mediated bycells in the substantia gelatinosa. Ac-tivity in these cells modulates themembrane potential of the afferentfiber terminals and thereby determinesthe excitatory effect of arriving im-pulses. Although there is evidence, sofar, for only presynaptic control, theremay also be undetected postsynapticcontrol mechanisms that contribute tothe observed input-output functions.
We propose that three features ofthe afferent input are significant forpain: (i) the ongoing activity whichprecedes the stimulus, (ii) the stimu-lus-evoked activity, and (iii) the rela-tive balance of activity in large versussmall fibers. The spinal cord is con-tinually bombarded by incoming nerveimpulses even in the absence of ob-vious stimulation. This ongoing activ-ity is carried predominantly by smallmyelinated and unmyelinated fibers,which tend to be tonically active andto adapt slowly, and it holds the gatein a relatively open position. When astimulus is applied to the skin, it pro-duces an increase in the number of ac-tive receptor-fiber units as informationabout the stimulus is transmitted to-ward the brain. Since many of thelarger fibers are inactive in the ab-sence of stimulus change, stimulationwill produce a disproportionate rela-tive increase in large-fiber over small-fiber activity. Thus, if a gentle pres-sure stimulus is applied suddenly tothe skin, the afferent volley containslarge-fiber impulses which not only firethe T cells but also partially close thepresynaptic gate, thereby shorteningthe barrage generated by the T cells.
19 NOVEMBER 1965
L
INPUT
S
CENTRALCONTROL
GATE CONTROL SYSTEM
>+ / S
®\\ T
y)
ACTIONSYSTEM
Fig. 4. Schematic diagram of the gate control theory of pain mechanisms: L, thelarge-diameter fibers; S, the small-diameter fibers. The fibers project to the substantiagelatinosa (SG) and first central transmission (T) cells. The inhibitory effect exerted bySG on the afferent fiber terminals is increased by activity in L fibers and decreased byactivity in S fibers. The central control trigger is represented by a line running fromthe large-fiber system to the central control mechanisms; these mechanisms, in turn,project back to the gate control system. The T cells project to the entry cells of theaction system. +, Excitation; —, inhibition (see text).
If the stimulus intensity is increased,more receptor-fiber units are recruitedand the firing frequency of active unitsis increased (9, 24). The resultant pos-itive and negative effects of the large-fiber and small-fiber inputs tend tocounteract each other, and thereforethe output of the T cells rises slowly.If stimulation is prolonged, the largefibers begin to adapt, producing a rela-tive increase in small-fiber activity. Asa result, the gate is opened further,and the output of the T cells risesmore steeply. If the large-fiber steadybackground activity is artificially raisedat this time by vibration or scratch-ing (a maneuver that overcomes thetendency of the large fibers to adapt),the output of the cells decreases.
Thus, the effects of the stimulus-evoked barrage are determined by (i)the total number of active fibers andthe frequencies of nerve impulses thatthey transmit, and (ii) the balance ofactivity in large and small fibers.Consequently, the output of the T cellsmay differ from the total input thatconverges on them from the peripheralfibers. Although the total number ofafferent impulses is a relevant stimulusparameter, the impulses have differenteffects depending on the specializedfunctions of the fibers that carry them.Furthermore, anatomical specializationalso determines the location and theextent of the central terminations ofthe fibers (24, 41, 42).
There are two reasons for believing
that pain results after prolonged moni-toring of the afferent input by centralcells. First, threshold for shock on onearm is raised by a shock delivered aslong as 100 milliseconds later to theother arm (43). Second, in pathologi-cal pain states, delays of pain sensa-tion as long as 35 seconds after stimu-lation cannot be attributed to slow con-duction in afferent pathways (10). Wesuggest, then, that there is temporaland spatial summation or integrationof the arriving barrage by the T cells.The signal which triggers the actionsystem responsible for pain experienceand response occurs when the outputof the T cells reaches or exceeds acritical level. This critical level of fir-ing, as we have seen, is determined bythe afferent barrage that actually im-pinges on the T cells and has alreadyundergone modulation by substantiagelatinosa activity. We presume thatthe action system requires a definitetime period for integrating the totalinput from the T cells. Small, fastvariations of the temporal patternproduced by the T cells might be in-effective, and the smoothed envelopeof the frequency of impulses—whichcontains information on the rate ofrise and fall, the duration, and theamplitude of firing—would be the ef-fective stimulus that initiates the ap-propriate sequence of activities in thecells that comprise the action system.
Central control trigger. It is nowfirmly established {44) that stimula-
975

tion of the brain activates descendingefferent fibers (45) which can influ-ence afferent conduction at the earliestsynaptic levels of the somesthetic sys-tem. Thus it is possible for centralnervous system activities subserving at-tention, emotion, and memories ofprior experience to exert control overthe sensory input. There is evidence(44) to suggest that these central in-fluences are mediated through the gatecontrol system.
The manner in which the appropri-ate central activities are triggered intoaction presents a problem. While somecentral activities, such as anxiety orexcitement, may open or close the gatefor all inputs at any site on the body,others obviously involve selective, lo-calized gate activity. Men wounded inbattle may feel little pain from thewound but may complain bitterlyabout an inept vein puncture (13).Dogs that repeatedly receive food im-mediately after the skin is shocked,burned, or cut soon respond to thesestimuli as signals for food and salivate,without showing any signs of pain, yethowl as normal dogs would when thestimuli are applied to other sites onthe body (16). The signals, then, mustbe identified, evaluated in terms ofprior conditioning, localized, and in-hibited before the action system is ac-tivated. We propose, therefore, thatthere exists in the nervous system amechanism, which we shall call thecentral control trigger, that activatesthe particular, selective brain processesthat exert control over the sensory in-put (Fig. 4). There are two knownsystems that could fulfill such a func-tion, and one or both may play a role.
The first is the dorsal column-medial lemniscus system. The largestand most rapidly conducting A fiberswhich enter the spinal cord send shortbranches to the substantia gelatinosa,and long central branches directly tothe dorsal column nuclei. Fibers fromthese nuclei form the medial lemniscus,which provides a direct route to thethalamus and thence to the somato-sensory cortex. The striking character-istics of this system are that informa-tion is transmitted rapidly from theskin to the cortex, that separation ofsignals evoked by different stimulusproperties and precise somatotopic lo-calization are both maintained through-out the system (46), and that conduc-tion is relatively unaffected by anes-thetic drugs (47). Traditionally, thedorsal column system is supposed to
976
carry two-point discrimination, rough-ness discrimination, spatial localiza-tion, tactile threshold, and vibration(48). Complex discrimination and lo-calization, however, are not a modal-ity; they represent decisions based onan analysis of the input. Indeed, thetraditional view is questionable in thelight of Cook and Browder's (49) ob-servation that surgical section of thedorsal columns produced no perma-nent change in two-point discrimina-tion in seven patients.
The second candidate for the roleof central control trigger is the dorso-Iateral path (50), which originates inthe dorsal horn and projects, after re-lay in the lateral cervical nucleus, tothe brain stem and thalamus. This sys-tem has small, well-defined receptivefields (51) and is extremely fast; inspite of having one additional relay,it precedes the dorsal column-mediallemniscus volley in the race to thecortex (52).
Both these systems, then, could ful-fill the functions of the central controltrigger. They carry precise informa-tion about the nature and location ofthe stimulus, and they conduct sorapidly that they may not only set thereceptivity of cortical neurons for sub-sequent afferent volleys but may, byway of central-control efferent fibers,also act on the gate control system.Part, at least, of their function, then,could be to activate selective brainprocesses that influence informationwhich is still arriving over slowly con-ducting fibers or is being transmittedup more slowly conducting pathways.
Action system. Pain is generallyconsidered to be the sensory adjunctof an imperative protective reflex(55). Pain, however, does not consistof a single ring of the appropriatecentral bell, but is an ongoing process.We propose, then, that once the inte-grated firing-level of T cells exceeds acritical preset level, the firing triggersa sequence of responses by the actionsystem.
Sudden, unexpected damage to theskin is followed by (i) a startle re-sponse; (ii) a flexion reflex; (iii)postural readjustment; (iv) vocaliza-tion; (v) orientation of the head andeyes to examine the damaged area;(vi) autonomic responses; (vii) evo-cation of past experience in similarsituations and prediction of the conse-quences of the stimulation; (viii) manyother patterns of behavior aimed atdiminishing the sensory and affective
components of the whole experience,such as rubbing the damaged area,avoidance behavior, and so forth.
The perceptual awareness that accom-panies these events changes in qualityand intensity during all this activity.This total complex sequence is hiddenin the simple phrases "pain response"and "pain sensation." The multiplicityof reactions demands some concept ofcentral mechanisms which is at leastcapable of accounting for sequentialpatterns of activity that would allowthe complex behavior and experiencecharacteristic of pain.
The concept of a "pain center" inthe brain is totally inadequate to ac-count for the sequences of behaviorand experience. Indeed, the concept ispure fiction, unless virtually the wholebrain is considered to be the "paincenter," because the thalamus (7, 25),the limbic system (54), the hypothala-mus (55), the brain-stem reticular for-mation (56), the parietal cortex (57),and the frontal cortex (14) are allimplicated in pain perception. Otherbrain areas are obviously involved inthe emotional and motor features ofthe behavior sequence. The idea of a"terminal center" in the brain whichis exclusively responsible for pain sen-sation and response therefore becomesmeaningless.
We propose, instead, that the trig-gering of the action system by the Tcells marks the beginning of the se-quence of activities that occur whenthe body sustains damage. The diver-gence of afferent fibers going to thedorsal horns and the dorsal columnnuclei marks only the first stage of theprocess of selection and abstraction ofinformation. The stimulation of a sin-gle tooth results in the eventual acti-vation of no less than five distinctbrain-stem pathways (58). Two ofthese pathways project to corticalsomatosensory areas I and II (59),while the remainder activate the thal-amic reticular formation and the lim-bic system (60), so that the input hasaccess to neural systems involved inaffective (54) as well as sensory ac-tivities. It is presumed that interac-tions occur among all these systemsas the organism interacts with the en-vironment.
We believe that the interactions be-tween the gate control system and theaction system described above may oc-cur at successive synapses at any levelof the central nervous system in thecourse of filtering of the sensory input.
SCIENCE, VOL. 150

Similarly, the influence of central ac-tivities on the sensory input may takeplace at a series of levels. The gatecontrol system may be set and reset anumber of times as the temporal andspatial patterning of the input is ana-lyzed and acted on by the brain.
Adequacy of the Theory
The concept of interacting gate con-trol and action systems can accountfor the hyperalgesia, spontaneouspain, and long delays after stimulationcharacteristic of pathological painsyndromes. The state of hyperalgesiawould require two conditions: (i)enough conducting peripheral axonsto generate an input that can activatethe action system (if, as in the caseof leprosy, all components of theperipheral nerve are equally affected,there is a gradual onset of anesthesia),and (ii) a marked loss of the largeperipheral nerve fibers, which may oc-cur after traumatic peripheral-nervelesions or in some of the neuropathies(61), such as post-herpetic neuralgia(10). Since most of the larger fibersare destroyed, the normal presynapticinhibition of the input by the gatecontrol system does not occur. Thus,the input arriving over the remainingmyelinated and unmyelinated fibers istransmitted through the unchecked,open gate produced by the C-fiber in-put.
Spatial summation would easily oc-cur under such conditions. Any nerveimpulses, no matter how they weregenerated, which converge on the cen-tral cells would contribute to the out-put of these cells. These mechanismsmay account for the fact that non-noxious stimuli, such as gentle pres-sure, can trigger severe pain in patientssuffering causalgia, phantom limb pain,and the neuralgias. The well-known en-hancement of pain in these patientsduring emotional disturbance and sex-ual excitement (62) might be due toincreased sensory firing [as a result ofan increased sympathetic outflow (63,64)] which is unchecked by presynapticinhibition. Conversely, the absence ofsmall fibers in the dorsal roots in apatient with congenital insensitivity topain (65) suggests that the mecha-nisms for facilitation and summationnecessary for pain may be absent.
Spontaneous pain can also be ex-plained by these mechanisms. Thesmaller fibers show considerable spon-
19 NOVEMBER 1965
taneous activity, which would have theeffect of keeping the gate open. Low-level, random, ongoing activity wouldthen be transmitted relatively un-checked (because of the predominantloss of A fibers), and summation couldoccur, producing spontaneous pain inthe absence of stimulation. This is a pos-sible mechanism for the pains of anes-thesia dolorosa and the "spontaneous"pains which develop after peripheral-nerve and dorsal-root lesions. Becausethe total number of peripheral fibersis reduced, it may take considerabletime for the T cells to reach the firinglevel necessary to trigger pain re-sponses, so perception and response aredelayed. This same mechanism can alsoaccount for post-ischemic pressure-block hyperesthesia and for the delaysin sensation of as much as 10 secondswhich occur when the large peripheralfibers fail to conduct (66).
We propose that the A-fiber inputnormally acts to prevent summationfrom occurring. This would accountfor Adrian's (67) failure to obtainpain responses in the frog from high-frequency air blasts which fired periph-eral nerves close to their maximum fir-ing rate, in an experiment meant torefute the view that summation of theeffects of noxious stimuli is importantfor pain. It is now clear that the airblasts would tend to fire a high pro-portion of the low-threshold A fibers,which would exert presynaptic inhibi-tion on the input by way of the gatecontrol system; thus the impulseswould be prevented from reaching theT cells where summation might occur.The double effect of an arriving vol-ley is well illustrated by the effects ofvibration on pain and itch. Vibrationactivates fibers of all diameters, butactivates a larger proportion of A fi-bers, since they tend to adapt duringconstant stimulation, whereas C-fiberfiring is maintained. Vibration there-fore sets the gate in a more closed po-sition. However, the same impulseswhich set the gate also bombard theT cell and therefore summate with theinputs from noxious stimulation. It isobserved behaviorally (26, 68) that vi-bration reduces low-intensity, but en-hances high-intensity, pain and itch.Similar mechanisms may account forthe fact that amputees sometimes ob-tain relief from phantom limb pain bytapping the stump gently with a rub-ber mallet (69), whereas heavier pres-sure aggravates the pain (8).
The phenomena of referred pain,
spread of pain, and trigger points atsome distance from the original siteof body damage also point toward sum-mation mechanisms, which can be un-derstood in terms of the model. TheT cell has a restricted receptive fieldwhich dominates its "normal activi-ties." In addition, there is a wide-spread, diffuse, monosynaptic input tothe cell, which is revealed by electricalstimulation of distant afferents (41).We suggest that this diffuse input isnormally inhibited by presynaptic gatemechanisms, but may trigger firing inthe cell if the input is sufficiently in-tense or if there is a change in gateactivity. Because the cell remains dom-inated by its receptive field, anesthesiaof the area to which the pain is re-ferred, from which only spontaneousimpulses are originating, is sufficient toreduce the bombardment of the cell be-low the threshold level for pain. Thegate can also be opened by activities indistant body areas, since the substantiagelatinosa at any level receives inputsfrom both sides of the body and (byway of Lissauer's tract) from the sub-stantia gelatinosa in neighboring bodysegments. Mechanisms such as thesemay explain the observations that stim-ulation of trigger points on the chestand arms may trigger anginal pain(70), or that pressing other bodyareas, such as the back of the head,may trigger pain in the phantom limb(11).
The sensory mechanisms alone failto account for the fact that nerve le-sions do not always produce pain andthat, when they do, the pain is usuallynot continuous. We propose that thepresence or absence of pain is deter-mined by the balance between the sen-sory and the central inputs to the gatecontrol system. In addition to the sen-sory influences on the gate control sys-tem, there is a tonic input to the sys-tem from higher levels of the centralnervous system which exerts an inhibi-tory effect on the sensory input (44,71). Thus, any lesion that impairs thenormal downflow of impulses to thegate control system would open thegate. Central nervous system lesionsassociated with hyperalgesia and spon-taneous pain (7) could have this effect.On the other hand, any central nerv-ous system condition that increases theflow of descending impulses would tendto close the gate. Increased central fir-ing due to denervation supersensitivity(72) might be one of these condi-tions. A peripheral nerve lesion, then,
977

would have the direct effect of open-ing the gate, and the indirect effect, byincreasing central firing and thereby in-creasing the tonic descending influenceson the gate control system, of closingthe gate. The balance between sen-sory facilitation and central inhibitionof the input after peripheral-nerve le-sion would account for the variabilityof pain even in cases of severe lesion.
The model suggests that psychologi-cal factors such as past experience, at-tention, and emotion influence pain re-sponse and perception by acting on thegate control system. The degree of cen-tral control, however, would be deter-mined, in part at least, by the tem-poral-spatial properties of the inputpatterns. Some of the most unbearablepains, such as cardiac pain, rise so rap-idly in intensity that the patient is un-able to achieve any control over them.On the other hand, more slowly risingtemporal patterns are susceptible tocentral control and may allow the pa-tient to "think about something else"or use other stratagems to keep thepain under control (73).
The therapeutic implications of themodel are twofold. First, it suggeststhat control of pain may be achievedby selectively influencing the large, rap-idly conducting fibers. The gate maybe closed by decreasing the small-fiberinput and also by enhancing the large-fiber input. Thus, Livingston (74)found that causalgia could be effective-ly cured by therapy such as bathingthe limb in gently moving water, fol-lowed by massage, which would in-crease the input in the large-fiber sys-tem. Similarly, Trent (75) reports acase of pain of central nervous systemorigin which could be brought undercontrol when the patient tapped hisfingers on a hard surface. Conversely,any manipulation that cuts down thesensory input lessens the opportunityfor summation and pain, within thefunctional limits set by the opposingroles of the large- and small-fiber sys-tems. Second, the model suggests thata better understanding of the pharma-cology and physiology of the substan-tia gelatinosa may lead to new waysof controlling pain. The resistance ofthe substantia gelatinosa to nerve-cellstains suggests that its chemistry differsfrom that of other neural tissue. Drugsaffecting excitation or inhibition of sub-stantia gelatinosa activity may be ofparticular importance in future at-tempts to control pain.
The model suggests that the action
978
system responsible for pain perceptionand response is triggered after the cu-taneous sensory input has been modu-lated by both sensory feedback mech-anisms and the influences of the cen-tral nervous system. We propose thatthe abstraction of information at thefirst synapse may mark only the be-ginning of a continuing selection andfiltering of the input. Perception andresponse involve classification of themultitude of patterns of nerve im-pulses arriving from the skin and arefunctions of the capacity of the brainto select and to abstract from all the in-formation it receives from the somes-thetic system as a whole (7-9). A"modality" class such as "pain," whichis a linguistic label for a rich varietyof experiences and responses, repre-sents just such an abstraction from theinformation that is sequentially re-examined over long periods by theentire somesthetic system.
References and Notes
1. K. M. Dailenbach, Amer. J. Psychol. 52, 331(1939); K. D. Keele, Anatomies of Pain(Blackwell, Oxford, 1957).
2. W. H. Sweet, Handbook Physiol. 1, 459(1959).
3. D. C. Sinclair, Brain 78, 584 (1955).4. M. von Frey, Ber. Kgl. Sachs. Ges. Wiss. 46,
185 (1894); ibid., p. 283.5. A. Goldscheider, Ueber den Schmerz in
physiologischer und klinischer Hinsicht(Hirschwald, Berlin, 1894).
6. G. H. Bishop, Physiol. Rev. 26, 77 (1946);A-delta fibers are the smallest myelinatedfibers, C fibers are the unmyelinated fibers,in peripheral nerve.
7. H. Head, Studies in Neurology (Keegan Paul,London, 1920).
8. W. K. Livingston, Pain Mechanisms (Mac-milJan, New York, 1943).
9. R. Melzack and P. D. Wall, Brain 85 331(1962).
10. W. Noordenbos, Pain (Elsevier, Amsterdam1959).
11. B. Cronholm, Acta Psychiat. Neurol. Scand.Suppl. 72, 1 (1951).
12. W. K. Livingston, Sci. Amer. 88, 59 (1953);R. Melzack, ibid. 204, 41 (1961); T. X.Barber, Psychol. Bull. 56, 430 (1959).
13. H. K. Beecher, Measurement of SubjectiveResponses (Oxford Univ. Press, New York,1959).
14. W. Freeman and J. W. Watts, Psycho-surgery in the Treatment of Mental Disordersand Intractable Pain (Thomas, Springfield,III., 1950).
15. I. P. Pavlov, Conditioned Reflexes (Milford,Oxford, 1927).
16. , Lectures on Conditioned Reflexes(International Publishers, New York, 1928).
17. J. P. Nafe, in Handbook of General Experi-mental Psychology, C. Murchison, Ed. (ClarkUniv. Press, Worcester, Mass., 1934).
18. J. D. Hardy, H. G. Wolff, H. Goodell, PainSensations and Reactions (Williams andWilkins, Baltimore, 1952).
19. C. T. Morgan, Introduction to Psychology(McGraw-Hill, New York, 1961).
20. C. C. Hunt and A. K. Mclntyre, J. Physiol.London 153, 88, 99 (1960).
21. J. Maruhashi, K. Mizaguchi, I. Tasaki, ibid.117, 129 (1952).
22. W. W. Douglas and J. M. Ritchie, ibid.139, 385 (1957).
23. A. Iggo, ibid. 143, 47 (1958).24. P. D. Wall, / . Neurophysiol. 23, 197 (1960).25. V. H. Mark, F. R. Ervin, P. I. Yakovlev,
Arch. Neurol. 8, 528 (1963).26. P. D. Wall and J. R. Cronly-Dillon, ibid.
2, 365 (1960).
27. P. D. Wall and A. Taub, J. Neurophysiol25, 110 (1962); L. Kruger and F. MichelExp. Neurol. S, 157 (1962).
28. G. F. Poggio and V. B. Mountcastle, BullJohns Hopkins Hasp. 106, 226 (1960).
29. G. M. Kolmodin and C. R. Skoglund, ActcPhysiol. Scand. SO, 337 (1960); G. Gordon.S. Landgren, W. A. Seed, / . Physiol. London158, 544 (1960); J. S. Eisenman, S. Land-gren, D. Novin, Acta Physiol. Scand. Suppl214, 1 (1963).
30. K. L. Casey, "A search for nociceptive ele-ments in the thalamus of the awake squirrejmonkey," paper read at the 16th Autumnmeeting of the American Physiological So-ciety, Providence, R.I., 1964.
31. G. Weddell, Annu. Rev. Psychol. 6, 119(1955).
32. D. H. Barron and B. H. C. Matthews, J,Physiol. London 92, 276 (1938).
33. D. O. Hebb, The Organization of Behavior(Wiley, New York, 1949).
34. R. W. Gerard, Anesthesiology 12, 1 (1951).35. T. Lewis, Pain (Macmillan, New York,
1942).36. G. H. Bishop, / . Nervous Mental Disease
128, 89 (1959).37. P. D. Wall, Progr. Brain Res. 12, 92 (1964).38. J. Szentagothai, J. Comp. Neurol. 122, 219
(1964).39. P. D. Wall, / . Physiol. London 164, 508
(1963); L. M. Mendell and P. D. Wall, ibid.172, 274 (1964).
40. P. D. Wall, / . Neurophysiol. 22, 205 (1959);J. Physiol. London 142, 1 (1958).
41. L. M. Mendell and P. D. Wall, Nature 20697 (1965).
42. D. G. Whitlock and E. R. Perl, Exp. Neurol3, 240 (1961).
43. A. M. Halliday and R. Mingay, Quart. J.Exp. Psychol. 13, 1 (1961).
44. K. E. Hagbarth and D. I. B. Kerr, J.Neurophysiol. 17, 295 (1954).
45. H. G. J. M. Kuypers, W. R. Fleming, J. W.Farinholt, Science 132, 38 (1960); A. Lund-berg, Progr. Brain Res. 12, 197 (1964).
46. V. B. Mountcastle, in Sensory Communica-tion, W. A. Rosenblith, Ed. (MassachusettsInstitute of Technology, Cambridge, 1961).
47. J. D. French, M. Verzeano, W. H. Magoun,AM.A. Arch. Neurol. Psychiat. 69, 519(1953): F. P. Haugen and R. Melzack,Anesthesiology 18, 183 (1957).
48. T. C. Ruch and J. F. Fulton, MedicalPhysiology and Biophysics (Saunders, Phila-delphia, 1960).
49. A. W. Cook and E. J. Browder Arch.Neurol. 12, 72 (1965).
50. F. Morin, Amer. J. Physiol. 183, 245 (1955).51. E. Oswaldo-Cruz and C. Kidd, J. Neuro-
physiol. 27, 1 (1964).52. U. Norrsell and P. Voerhoeve, Acta Physiol.
Scand. 54, 9 (1962).53. C. S. Sherrington, in Textbook of Physiology,
E. A. Schafer, Ed. (Pentland, Edinburgh,1900).
54. J. V. Brady, Handbook Physiol. 3 1529(1960).
55. W. R. Hess, Diencephalon: Autonomic andExtrapyramidal Functions (Grune, New York,1954).
56. J. M. R. Delgado, / . Neurophysiol. 18, 261(1955); R. Melzack, W. A. Stotler, W. K.Livingston, ibid. 21, 353 (1958).
57. P. Schilder and E. Stengel, AM.A. Arch.Neurol. Psychiat. 25, 598 (1931).
58. D. I. B. Kerr, F. P. Haugen, R. Melzack,Amer. J. Physiol. 183, 253 (1955).
59. R. Melzack and F. P. Haugen, ibid. 190,570 (1957).
60. W. J. H. Nauta and H. G. J. M. Kuypers,in Reticular Formation of the Brain, H. H.Jasper et al., Eds. (Little, Brown, Boston,1958).
61. W. Blackwood, W. H. McMenemey, A.Meyer, R. M. Norman, D. S. Russell, Green-field's Neuropathology (Arnold, London,1963).
62. W. R. Henderson and G. E. Smyth, / .Neurol. Neurosurg. Psychiat. 11, 88 (1948).
63. K. E. Chernetski, J. Neurophysiol. 27, 493(1964).
64. J. Doupe. C. H. Cullen, G. Q. Chance, / .Neurol. Neurosurg. Psychiat. 7, 33 (1944).
65. A. G. Swanson, G. C. Buchan, E. C. Alvord,Arch. Neurol. 12, 12 (1965).
66. D. C. Sinclair and J. R. Hinshaw, Brain 74,318 (1951)
67. E. D. Adrian, The Basis of Sensation: TheAction of Sense Organs (Christophers, Lon-don, 1928).
SCIENCE, VOL. 150

6 8 R Melzack, P . D . WaU, A. Z. Weisz, Exp.Neurol. 8. 35 (1963); R. Melzack and B.Schecter, Science 147, 1047 (1965).
69 W R. Russell and J. M. K. Spalding, Brit.' Med. J. 2, 68 (1950).
70 H. Cohen, Trans. Med. Soc. London 64, 65' (1944).
71. A. Taub, Exp. Neurol. 10, 357 (1964).7? G. W. Stavraky, Supersensitivity following
Lesions of the Nervous System (Univ. ofToronto Press, Toronto, 1961); S. K. Sharp-less, Annu. Rev. Physiol. 26, 357 (1964).
73. R. Melzack, A. Z. Weisz, L. T. Sprague,Exp. Neurol. 8, 239 (1963).
74. W. K. Livingston, Ann. N.Y. Acad. Sci. 50,247 (1948).
75. S. E. Trent, / . Nervous Mental Disease 123,356 (1956).
76. R. Descartes, "L'Homme" (Paris, 1644),M. Foster, transl., in Lectures on the Historyof Physiology during the 16th, 17th and 18thCenturies (Cambridge Univ. Press, Cam-bridge, England, 1901).
77. C. S. MacCarty and R. L. Drake, Proc. StaffMeetings Mayo Clinic 31, 208 (1956).
78. This study was supported in part by contractSD-193 from the Advanced Research ProjectsAgency, U.S. Department of Defense (toR.M.); and in part by the Joint Services Elec-tronics Program under contract DA36-039-AMC-0320O(E), the Bell Telephone Labora-tories, Inc., the Teagle Foundation, Inc., theNational Science Foundation (grant GP-2495),the National Institutes of Health (grantsMH-04737-05 and NB-04897-02), the NationalAeronautics and Space Administration (grantNsG-496), and the U.S. Air Force (ASDcontract AF33 (615J-1747).
The X-ray Analysis ofComplicated Molecules
Dorothy Crowfoot Hodgkin
I first met the subject of x-ray diffrac-tion of crystals in the pages of the bookW. H. Bragg wrote for school childrenin 1925, Concerning the Nature ofThings. In this he wrote: "Broadlyspeaking, the discovery of x-rays hasincreased the keenness of our visionover ten thousand times and we cannow 'see' the individual atoms andmolecules." I also first learnt at thesame time about biochemistry whichprovided me with the molecules itseemed most desirable to "see." AtOxford, seriously studying chemistry,with Robinson and Hinshelwood amongmy professors, I became captivated bythe edifices chemists had raised throughexperiment and imagination—but stillI had a lurking question. Would it notbe better if one could really "see"whether molecules as complicated asthe sterols, or strychnine, were just asexperiment suggested? The process of"seeing" with x-rays was clearly moredifficult to apply to such systems thanmy early reading of Bragg had sug-gested; it was with some hesitation thatI began my first piece of research workwith H. M. Powell on thallium dialkylhalides, substances remote from, yetcuriously connected with, my later sub-jects for research.
A series of lucky accidents (a chancemeeting in a train between an old friendof mine, A. F. Joseph, and ProfessorLowry was one) took me to Cambridge19 NOVEMBER 1965
to work with J. D. Bernal in 1932.There our scientific world ceased toknow any boundaries. In a subdepart-ment of mineralogy, changed duringmy stay into one of physics, we ex-plored the crystallography of a widevariety of natural products, the struc-ture of liquids and particularly water,Rochelle salt, isomorphous replacementand phase determination, metal crystalsand pepsin crystals, and speculatedabout muscular contraction. Our closestfriends were biologists and biochemists.I left Cambridge with great reluctanceto try to settle down academically andtry to solve at least one or two of themany problems we had raised.
I do not need here to give a detailedaccount of the theoretical backgroundof structure analysis by the x-ray dif-fraction of crystals since this was donelong ago by W. L. Bragg (1) andagain 2 years ago, very beautifully, byPerutz and Kendrew (2). The experi-mental data we have to employ are thex-ray diffraction spectra from the crys-tal to be studied, usually recorded pho-tographically, and their intensities esti-mated by eye. These spectra correspondwith a series of harmonic terms whichcan be recombined to give us a repre-sentation of the x-ray scattering ma-terial in the crystal, the electron density.The calculation involves the summationof a Fourier series in which the termshave the amplitudes and phases of the
observed spectra; both depend on thepositions of the atoms in the crystal,but only the amplitudes are easily mea-surable. As Perutz and Kendrew ex-plained, the introduction of additionalheavy atoms into a crystal under in-vestigation at sites which can be foundmay make it possible to calculate phaseangles directly from the observed am-plitudes of the spectra given by theisomorphous crystals. One is then inthe position that, from a sufficient num-ber of measurements, one can calculatedirectly the electron density and seethe whole structure spread out beforeone's eyes. However, the feat involvedin the calculations described 2 yearsago was prodigious—tens of thousandsof reflections for five or six crystalswere measured to provide the electrondensity distribution in myoglobin andhemoglobin. More often, and with mostcrystals, the conditions for direct elec-tron density calculation are not initiallymet and one's progress towards the finalanswer is stepwise; if some of the atomscan be placed, particularly the heavieratoms in the crystal, calculations, neces-sarily imperfect, of the electron densitycan be started from which new regionsin the crystal may be identified; thecalculation is then repeated until thewhole atomic distribution is clear. Atthe outset of my research career, twoessential tools became available, thePatterson synthesis and Beevers andLipson strips. Patterson showed that afirst Fourier synthesis calculated direct-ly from the raw data without phase in-formation, represented the inter-atomicvector distribution in the crystal struc-ture (3). This was capable, in simple
Copyright © 1965 by the Nobel Foundation.The author is Wolfson Research Professor of
the Royal Society in the Chemical Crystal-lography Laboratory, Oxford University, Oxford,England. This article is the lecture she deliveredin Stockholm. Sweden. 11 December 1964, whenshe received the Nobel Prize in chemistry. It ispublished here with the permission of the NobelFoundation and will be included in the completevolumes of Nobel lectures in English, publishedby the Elsevier Publishing Company, Amsterdamand New York.
979