-
Predicting non-diabetic renal disease in typvalue of glycated
hemoglobin
ld
UKacktal, B
a r t i c l e i n f o
Article history:Received 30 October 2014Received in revised form
28 November 2014
rch Group, 1993; UK98).biochemical analysespersistent
microalbu-
minuria. Estimated glomerular ltration rate (eGFR) declines
prior tomore severe macroalbuminuria in type 2 diabetes (T2D);
hence acombination of eGFR and albuminuria can be used to stage
andmonitor patients (American Diabetes Association, 2013;
Kidney
Journal of Diabetes and Its Complications xxx (2015) xxxxxx
5SS Birmingham, UK. Tel.: +44 1214242158; fax: +44
1214241159.E-mail addresses: [email protected] (M.
Pallayova),
Contents lists available at ScienceDirect
Journal of Diabetes an
j ourna l homepage: [email protected] (A. Mohammed),
[email protected](G. Langman), [email protected]
(S. Taheri), [email protected]
Control & Complications Trial ReseaProspective Diabetes Study
(UKPDS) Group, 19
The diagnosis of DN is usually made throughof urine and blood.
An early manifestation is
Conict of Interest: MP has received grant/research support from
Slovakian DiabetesAssociation/Lilly Diabetes Clinical Research
Initiative. AM, GL, ST and ID declare that theyhave no competing
interests. Corresponding author at: Renal Unit Heartlands Hospital
Bordesley Green East B91. Introduction
Diabetic nephropathy (DN) is a major microvascular
complicationof diabetes mellitus associated with end-stage renal
disease requiringrenal replacement therapy. A major contributor to
development andprogression of DN is glycemic control as shown by
major diabetes
studies (Stratton, Adler, Neil, et al., 2000; The
MicroalbuminuriaCollaborative Study Group, 1999). Other modiable
factors for DNinclude hypertension, obesity, smoking, and
dyslipidemia (Gross etal., 2005). There is encouraging evidence
suggesting that timely andlong-term tight glycemic control
effectively delays the onset andslows the progression of DN in both
type 1 and type 2 diabetes (The(I. Dasgupta).1 The permanent
address of Maria Pallayova: Depar
Faculty of Medicine, Pavol Jozef Safarik University, Kosic2 The
present address of Azharuddin Mohammed: Ren
Uttoxeter Road, Derby, DE22 3NE, UK.3 The present address of
Shahrad Taheri: Departme
Medical College in Qatar, PO Box 24144, Doha, Qatar.
http://dx.doi.org/10.1016/j.jdiacomp.2014.12.0051056-8727/ 2014
Elsevier Inc. All rights reserved.
Please cite this article as: Pallayova, M.,hemoglobin, Journal
of Diabetes and Its Comdeterioration inHbA1cprior
tobiopsypredictedNDRD inT2D. Further studies are needed tovalidate
thendings. 2014 Elsevier Inc. All rights reserved.Accepted 8
December 2014Available online xxxx
Keywords:Glycated hemoglobinRenal biopsyRenal diseaseType 2
diabetes mellitusNon-diabetic renal disease
51) over 10 years for nephrotic-range proteinuria, microscopic
hematuria, or rapidly declining renal function.Results: Thirty-ve
(68.6%) biopsies were diagnostic of NDRD, and 16 (31.4%) revealed
isolated diabeticnephropathy. The most common NDRDs were
interstitial nephritis (20%), progressive crescentic
glomerulo-nephritis (14%), membranous nephropathy (11%), and focal
segmental glomerulosclerosis (11%). The odds forNDRDdeclined by 97%
in the presence of diabetic retinopathy (P b 0.001). The
deterioration of HbA1c during theyear before biopsy predicted NDRD
even after adjusting for diabetic retinopathy (OR, 7.65; 95% CI,
1.36123.04;P = 0.003). A model based on the interaction between the
HbA1c values 12 months before biopsy and theabsolute change in
these values during the preceding year predicted NDRD with 73.7%
sensitivity and 75%specicity (AUC, 0.77; 95% CI,
0.590.94).Conclusions: This study demonstrated a considerably high
prevalence of NDRD in T2D adults undergoing renalbiopsy. The
absence of diabetic retinopathy, lower HbA1c values 12 months
before biopsy and greatera b s t r a c t
Aims: The indications for renal biopsy in type 2
diabetesmellitus (T2D) are notwell established.We investigatedthe
prevalence, spectrum, and predictors of biopsy-proven non-diabetic
renal disease (NDRD) in T2D.Methods:An observational,
single-center, retrospective study of T2D adults who underwent
renal biopsies (N =Maria Pallayova a,1, Azharuddin Mohammed a,2,
GeraShahrad Taheri c,d, Indranil Dasgupta a,a Renal Unit,
Heartlands Hospital, Bordesley Green East, Birmingham, UKb
Department of Histopathology, Heartlands Hospital, Bordesley Green
East, Birmingham,c Collaborations for Leadership in Applied Health
Research and Care for Birmingham and Bld Diabetes Centre, Heart of
England NHS Foundation Trust, Birmingham Heartlands Hospitment of
Human Physiology,e, Slovak Republic.al Unit, Royal Derby
Hospital,
nt of Medicine, Weill Cornell
et al., Predicting non-diabetplications (2015), http://dx.e 2
diabetic adults: The
Langman b,3,
Country/National Institute for Health Research, University of
Birmingham, Birmingham, UKirmingham, UK
d Its Complications
.JDCJOURNAL.COMDisease: Improving Global Outcomes (KDIGO) CKD
Work Group,2013). While diabetes is the major cause of renal
disease in patientswith diabetes, in about a third of patients,
renal dysfunction is due toother causes (non-diabetic renal
disease; NDRD) (Chong, Keng, Tan,et al., 2012; Das, Dakshinamurty,
Prayaga, & Uppin, 2012; Harada,Akai, Sumida, et al., 2013;
Kleinknecht, Bennis, & Altman, 1992; Lee,
ic renal disease in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
-
2 M. Pallayova et al. / Journal of Diabetes and Its
Complications xxx (2015) xxxxxxChung, & Choi, 1999; Mazzucco,
Bertani, Fortunato, et al., 2002; Olsen& Mogensen, 1996;
Richards et al., 1992; Soni, Gowrishankar, Kishan,& Raman,
2006; Yaqub, Kashif, & Hussain, 2012). In the NDRD group,the
treatment of renal disease may require a different strategy. A
renalbiopsy is helpful indetermining theunderlyingpathophysiology
inNDRD.
The selection criteria for renal biopsy in diabetic patients are
notwell established. In type 1 diabetes, the presence of
proteinuria withshort diabetes duration and/or rapidly declining
renal function,especially in the absence of diabetic retinopathy,
has been suggestedas a signal for the need for renal biopsy (Mauer,
Fioretto,Woredekal, et al.,2001). In T2D, the criteria are less
clear since dysglycemia is present formany years prior to
diagnosis. Commonly, proteinuria N1 g/24 hours,renal involvement
without diabetic retinopathy, or unexplainedhematuria has been used
as indicators for renal biopsy (Wong, Choi,Szeto, et al., 2002).
Identication of novel predictors of renal diseasewillimprove the
current selection criteria for renal biopsy and facilitate
earlydetection of NDRD in T2D. Early diagnosis and appropriate
treatmentmay help slow progression to end stage renal disease. In
this study, wesought to investigate the prevalence, spectrum, and
predictors ofbiopsy-proven NDRD in adults with T2D.
2. Subjects, material and methods
This was a retrospective observational study of T2D patients
whounderwent renal biopsies over 10 years in our center. As this
was anaudit of retrospective data, the local research ethics
committee feltthat no formal ethics approval was required.
Fifty-one native renal biopsies obtained from 51 adults with
adocumented diagnosis of T2D, referred to our center between
2002and 2012, were analysed. In our center, as a policy, DN is
diagnosed onclinical grounds and kidney biopsies are only carried
out if there areatypical clinical features. Indications for biopsy,
in this cohort,included nephrotic range proteinuria (N3 g/24
hours), signicantmicroscopic hematuria ( ++), or rapidly declining
renal function.Renal biopsy specimens were examined by light
microscopy, directimmunouorescence, and electron microscopy, where
indicated.
The biopsy report, biochemical results, and clinical information
atthe time of renal biopsy and follow-up were studied.
Glomerularltration rate estimates were calculated using the
4-variableModication of Diet in Renal Disease Study equation (Levey
et al.,1999). Glycemic control was assessed by glycated
hemoglobin(HbA1c) levels, measured using National Glycohemoglobin
Standar-dization Program (NGSP) certied method, standardized to
theDiabetes Control and Complications Trial assay. HbA1c values
arereported in both NGSP percentage units with International
Federationof Clinical Chemistry (IFCC) units (mmol/mol) in
parentheses.
The primary outcome measure was the prevalence and nature
ofhistologically-proven NDRD. The secondary outcome
measuresincluded predictors of NDRD vs. DN and the risk factors for
adverserenal outcome. Adverse renal outcomes included reaching end
stagerenal disease requiring renal replacement therapy or chronic
kidneydisease (CKD) leading to death, or a composite of the
two.
2.1. Statistical analyses
The ShapiroWilk test was applied to assess normality of
datadistribution. Continuous variables with normal distribution
arepresented as means standard deviation (SD) and compared usingthe
Student's t test. Continuous variables with non-normal
distribu-tion are presented as medians and interquartile ranges
(IQR) andcompared using the Wilcoxon rank-sum test or the
Wilcoxon--matched pairs signed-ranks test. The chi-square test was
applied toexamine patterns between categorical variables.
Univariate andmultivariate standard and exact logistic regression
modeling wereemployed to identify the association between
biopsy-proven NDRDand potential predictors. The logistic regression
models were ttedPlease cite this article as: Pallayova, M., et al.,
Predicting non-diabethemoglobin, Journal of Diabetes and Its
Complications (2015), http://dx.using a stepwise bidirectional
elimination algorithm, with inclusionand exclusion criteria of P
0.15 and P 0.2 respectively.
The number in whom complete data were available is mentioned
inthe text. Absolute changes () in eGFR and in HbA1c were
calculated bysubtracting values 12 months before biopsy from those
at the time ofbiopsy. The follow-up eGFR were calculated by
subtracting the eGFRvalues at the time of biopsy from the values 12
months after.
Findings were considered to be statistically signicant at the
5%level. Statistical calculations were performed using Stata 11.2
SpecialEdition (StataCorp LP, College Station, TX).
3. Results
3.1. Sample characteristics and renal biopsy ndings
Theentire cohortof renal biopsypatients (N =
51)waspredominantlymale (64.7%), of mixed ethnicity (28White
Europeans, 18 South-Asians, 3African Caribbean, 2 with not stated
ethnicity), aged 61 12 years(mean SD). The median (IQR) duration of
T2D was 9 years (215 years) (n = 45). At the time of renal biopsy,
the NGSP HbA1c was7.2% (6.47.8%), the IFCC HbA1c 55 (4662) mmol/mol
(n = 42).Twenty-two of 39 (56.4%) patients had diabetic
retinopathy. The median(IQR) eGFR was 23.5 ml/min/1.73 m2 (1139.5
ml/min/1.73 m2), and60.4% of patients had stage 45 CKD. Twenty-one
of 36 (58.3%) proteinuricpatients had nephrotic range proteinuria
(albumin/creatinine ratioN250 mg/mmol or protein/creatinine ratio
N300 mg/mmol), and 16 of35 (45.7%) had microscopic hematuria.
Thirty-four of 46 (73.9%) patientswere on
reninangiotensinaldosterone system (RAAS) blockade therapy.
Thirty-ve (68.6%) biopsies were diagnostic of NDRD, 16
(31.4%)revealed isolated DN, and 4 (7.8%) showed NDRD superimposed
onDN. The spectrum of NDRD was as follows: interstitial nephritis
7(20%), progressive crescentic glomerulonephritis 5 (14.3%),
membra-nous nephropathy 4 (11.4%), focal segmental
glomerulosclerosis 4(11.4%), acute tubular necrosis 3 (8.6%),
immunoglobulin A nephrop-athy 2 (5.7%), ischemic nephropathy 2
(5.7%), minimal changenephropathy 1 (2.9%), minimal change
nephropathy + interstitialnephritis 1 (2.9%), mesangiocapillary
glomerulonephritis 1 (2.9%),amyloidosis 1 (2.9%), oxalate
nephropathy 1 (2.9%), myeloma castnephropathy 1 (2.9%), brillary
glomerulonephritis 1 (2.9%), andcollagenobrotic glomerulopathy 1
(2.9%). In more than 50% of NDRD,histology prompted alteration in
therapeutic management.
Table 1 shows characteristics of the two subgroups based on
renalbiopsy ndings. The patients with NDRD had better glycemic
control12 months before biopsy (n = 32), a smaller decrease in
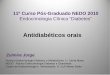
HbA1c duringthe year before biopsy (n = 31; Fig. 1a, b), and a
lower rate of diabeticretinopathy than thosewith isolated DN.
Therewas a trend towardsmoreSouth-Asians in the DN subgroup. We did
not nd any difference in eGFRprior to biopsy, at the time of
biopsy, and 12 months after biopsy betweenthe two subgroups.
Following the therapeutic adjustments based on renalbiopsy ndings,
the patients with NDRD had signicantly greaterimprovement in eGFR
12 months after biopsy (n = 38) than patientswith isolated DN
(Table 1). Similar numbers received RAAS blockadetherapy in the
twosubgroups. Therewerenodifferences indurationofT2D(n = 45) and in
pharmacological treatment of diabetes (n = 47; Table 1).
By the end of 2012, overall mortality was 29.4% with no
differencebetween the subgroups. There was no difference in number
ofpatients requiring renal replacement therapy. However, a
compositeadverse renal outcome (reaching end stage renal disease
requiringrenal replacement therapy + CKD leading to death; n = 48)
washigher in isolated DN subgroup (Table 1).
3.2. Predictors of renal disease and risk factors for
adverserenal outcomes
Table 2 presents the results of a univariate exact logistic
regressionanalysis for unadjusted (crude) associations between NDRD
andic renal disease in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
-
ND
; +0; +3
)
.8
15)
3M. Pallayova et al. / Journal of Diabetes and Its Complications
xxx (2015) xxxxxxTable 1Characteristics of patients (N = 51)
according to renal biopsy ndings.
Variable Patients with
Age (years) 63 11Sexfemale (%) 40South-Asian ethnicity (%)
30.3Duration of diabetes (years) 7.5 (113)Diabetes treatmentdiet
only (%) 9.4Diabetes treatmentOHA/GLP-1 agonists (%) 53.1Diabetes
treatmentinsulin/insulin + OHA (%) 37.5HbA1c at the time of biopsy-
NGSP HbA1c (%) 7.2 0.88- IFCC HbA1c (mmol/mol) 55 9.6
HbA1c 6 months before biopsy- NGSP HbA1c (%) 7.4 (6.3-8.0)- IFCC
HbA1c (mmol/mol) 57 (4564)
HbA1c 12 months before biopsy- NGSP HbA1c (%) 6.9 (6.5-8.0)-
IFCC HbA1c (mmol/mol) 52 (4864)
HbA1c during the year before biopsy- NGSP HbA1c (%) 0.1 (0.5-
IFCC HbA1c (mmol/mol) 1.1 (5.5
Diabetic retinopathy (%) 34.6eGFR 12 months before biopsy
(ml/min/1.73 m2) 58 (4077)eGFR 6 months before biopsy (ml/min/1.73
m2) 45 (3981)eGFR at the time of biopsy (ml/min/1.73 m2) 16
(1036)eGFR 6 months after biopsy (ml/min/1.73 m2) 33 (1747.5eGFR 12
months after biopsy (ml/min/1.73 m2) 37.8 22eGFR during the year
before biopsy (ml/min/1.73 m2) 31.3 25eGFR 12 months after biopsy
(ml/min/1.73 m2) 6.8 17.4Urine PCR at the time of biopsy (mg/mmol)
367 (26510RAAS blockade therapy at the time of biopsy (%)
74.2Adverse renal outcome (%) 34.4
18.2independent variables with odds ratios (OR), 95% condence
intervals(95% CI), and P-values. For subjects with diabetic
retinopathy, theexpected log odds of having NDRD decreased by 3.39,
and the odds forNDRD declined by 97% (P b 0.001). The unadjusted OR
of theassociation between NDRD and HbA1c 12 months before biopsy
was0.60; for every 1% (10.9 mmol/mol) increase in the HbA1c 12
monthsbefore biopsy, the odds for NDRD declined by 40% (P = 0.018).
Therewas a trend towards higher odds for NDRD with deterioration
ofHbA1c during the year before biopsy (P = 0.054). We also observed
atrend towards higher odds for NDRDwith the increasing INTHbA1c
(avariable consistent with the interaction between HbA1c 12
monthsbefore biopsy and HbA1c during the year before biopsy); P =
0.069.
The association between NDRD and deterioration of HbA1c
duringthe year before biopsy remained signicant even after
adjusting fordiabetic retinopathy in the nal multivariate
regression model (OR7.65; 95% CI, 1.36 to 123.04; P = 0.003). Our
results further showed astatistically signicant joint distribution
of diabetic retinopathy andINTHbA1c. After adjusting for the
diabetic retinopathy, the expectedodds for NDRD increased by 1.28
for every one unit (1%) increase inINTHbA1c (OR 1.28; 95% CI, 1.03
to 1.82; P = 0.013).
Fig. 2 shows estimated predicted probabilities of having NDRD,by
the HbA1c 12 months before biopsy, ranging from an appro-ximately
85% probability of having NDRD in patients with arelatively low
preceding HbA1c to a b50% probability in patientswith HbA1c of
N8.5% (69 mmol/mol). Of importance, the patientswho experienced
deterioration in HbA1c during the year prior tobiopsy had at least
63% probability of having NDRD (Fig. 2, plussymbols). The HbA1c 12
months before biopsy in these patientswas b8% (64 mmol/mol).
- Renal replacement therapy after biopsy (%)- Mortality (%)
22.9- the time until death (months) 29 22.9
Continuous variables with normal distribution are presented as
means SD. Continuousnephropathy; eGFR, glomerular ltration rate
estimates; eGFR, an absolute change in eGFchange in HbA1c; IFCC,
International Federation of Clinical Chemistry; NDRD,
non-diabetichypoglycemic agents; PCR, protein to creatinine ratio;
RAAS, reninangiotensinaldosterone
Please cite this article as: Pallayova, M., et al., Predicting
non-diabethemoglobin, Journal of Diabetes and Its Complications
(2015), http://dx.RD (n = 35) Patients with isolated DN (n = 16)
P
58 14 0.16725 0.29861.5 0.0519 (419) 0.4336.7 0.75766.7
0.38226.7 0.465
7.7 1.7661 19.2 0.188
8.9 (6.6-12.2)74 (48110) 0.288
9 (7.2-10.6)75 (5592) 0.047
.3) 0.9 (1.75; 0.3)
.3) 9.8 (19.1; 3.3) 0.023100 b0.00155 (4663) 0.64841 (2856)
0.24429 (1749) 0.15828.5 (1836) 0.55032.1 24.4 0.31821.1 16
0.2337.1 16.4 0.015441 (130.5-871) 0.68573.3 0.95068.8 0.02425
0.579To further dene the importance of HbA1c in predicting the
NDRD,we performed receiver operating characteristic (ROC) curve
analysisof three HbA1c-based predictive models for NDRD (Fig. 3).
In the rstmodel, the HbA1c 12 months before biopsy was used. The
cut point ofthe HbA1c 12 months before biopsy of6.2% (44 mmol/mol)
was thebest predictor of NDRD with 100% sensitivity. However, the
17%specicity reected high rate (83%) of false positives (area under
thecurve AUC, 0.29; 95% CI, 0.07 to 0.51). In the second model,
wemeasured predictive accuracy of the HbA1c during the year priorto
biopsy. The HbA1c during the year prior to biopsy of 0.4%(4.4
mmol/mol) was the best predictor of NDRD (73.7% sensitivity,66.7%
specicity; AUC, 0.75; 95% CI, 0.56 to 0.93). Since the
precedingHbA1c and the HbA1c during the year before biopsy are
closelyinterrelated, the third predictive ROC curve model included
aninteraction term between the two aforementioned
predictors(INTHbA1c; INTHbA1c = HbA1c 12 months before biopsy *
HbA1cduring the year before biopsy). The ROC curve analysis showed
that theINTHbA1c cut-off of 2.48% (27.1 mmol/mol) was the
bestpredictor of NDRD with 73.7% sensitivity and 75% specicity
(AUC,0.77; 95% CI, 0.59 to 0.94; Fig. 3).
4. Discussion
There were three major ndings in the present study. First,
renalbiopsies with histological conrmation of renal involvement
revealeda considerably high prevalence of NDRD in a cohort of T2D
patientswith signicant dipstick hematuria, nephrotic range
proteinuria, and/or rapidly declining renal function. Second, this
study conrmed thepreviously recognized associations between poor
long-term glucose
43.8 0.129
24 27.4 0.738
variables with non-normal distributions are presented as medians
(IQR). DN, diabeticR; GLP-1, glucagon-like peptide-1; HbA1c,
glycated hemoglobin; HbA1c, an absoluterenal disease; NGSP,
National Glycohemoglobin Standardization Program; OHA,
oralsystem.
ic renal disease in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
-
Table 2Unadjusted (crude) associations between non-diabetic
renal disease and inde-pendent variables.
Variable P-value OR 95% CI
Age 0.171 1.04 0.99 to 1.09Sex female 1.00 (reference) male
0.474 0.51 0.10 to 2.14
Ethnicity White European 1.00 (reference) South-Asian 0.107 0.28
0.06 to 1.25
Duration of diabetes 0.493 0.97 0.89 to 1.06Diabetes treatment
Diet only 1.00 (reference) OHA/GLP-1 agonists 0.607 0.53 0.05 to
5.86 insulin/insulin + OHA 0.950 1.08 0.09 to 13.54
HbA1c 12 months before biopsy 0.018 0.60 0.35 to 0.93HbA1c at
the time of biopsy 0.200 0.71 0.41 to 1.19HbA1c during the year
before biopsy 0.054 1.89 0.99 to 4.46INTHbA1c 0.069 1.06 1.00 to
1.14Diabetic retinopathy b0.001 0.03 0.00 to 0.24eGFR 12 months
before biopsy 0.401 1.02 0.98 to 1.06eGFR at the time of biopsy
0.374 0.99 0.96 to 1.02eGFR during the year before biopsy 0.211
0.98 0.94 to 1.01Microscopic hematuria 0.116 4.86 0.75 to
56.13Nephrotic proteinuria 1.000 1.02 0.19 to 5.17
4 M. Pallayova et al. / Journal of Diabetes and Its
Complications xxx (2015) xxxxxx
N
GSP
HbA
1c [%
]
P=0.047
N=12 N=8 N=15
P=0.02
N=20 N=19 N=2756
78
910
1112
1314
15Isolated diabetic nephropathy Non-diabetic renal disease
HbA1c 12 months before renal biopsyHbA1c 6 months before renal
biopsyHbA1c at the time of renal biopsy
P=0.023
-2
02
Isolated diabetic nephropathy Non-diabetic renal disease
HbA
1c [%
]
a
bcontrol and presence of diabetic retinopathy and DN in T2D
(Strattonet al., 2000). Third, besides the previously identied
predictors of NDRDthat include new onset nephrotic range
proteinuria, shorter duration ofdiabetes, and the absence of
diabetic retinopathy (Chang, Park, Kim,et al., 2011; Pham, Sim,
Kujubu, Liu, & Kumar, 2007; Sharma, Bomback,Radhakrishnan, et
al., 2013), this is the rst study to demonstrate that inT2D, the
HbA1c 12 months before biopsy and the absolute change inHbA1c
during the year before biopsy predict the type of renal
disease.This study also shows that those with biopsy-proven NDRD
have abetter composite outcome of end stage renal disease and
death.
Our nding of high prevalence of NDRD in T2D is consistent
withobservations made by others (Chong et al., 2012; Das et al.,
2012;Harada et al., 2013; Kleinknecht et al., 1992; Lee et al.,
1999;Mazzuccoet al., 2002; Olsen & Mogensen, 1996; Richards et
al., 1992; Soni et al.,2006; Yaqub et al., 2012). These studies
showed a variable prevalenceof NDRD of 1878%. This is attributed to
selection criteria for renalbiopsy and to the geographical and
ethnic differences in the incidenceof various NDRD. The nding of
high prevalence of NDRD in thiscohort of T2D patients with renal
impairment and atypical featureshas important clinical
implications; at least 50% of patients had NDRDthat was treatable
with steroids and immunosuppressive agents. Thetherapeutic
adjustments based on histology and resultant modica-tion of course
of NDRDmay explain the improvement in eGFR and thebetter composite
adverse renal outcome in the NDRD subgroup. Bycontrast, there is no
specic treatment for isolated DN (AmericanDiabetes Association,
2013; Gross et al., 2005; Kidney Disease:
N=31
-6
-4
Two-sample Wilcoxon rank-sum (Mann-Whitney) test
N
GSP
Fig. 1. a: Long-term glucose control in type 2 diabetic patients
with isolated diabeticnephropathy vs. non-diabetic renal disease.
HbA1c, glycated hemoglobin; NGSP,National Glycohemoglobin
Standardization Program. b: Changes in HbA1c during theyear before
renal biopsy in patients with isolated diabetic nephropathy vs.
non-diabeticrenal disease. HbA1c, glycated hemoglobin; HbA1c, an
absolute change in HbA1c;NGSP, National Glycohemoglobin
Standardization Program.
Please cite this article as: Pallayova, M., et al., Predicting
non-diabethemoglobin, Journal of Diabetes and Its Complications
(2015), http://dx.Improving Global Outcomes (KDIGO) CKD Work Group,
2013). Earlyand accurate diagnosis of NDRD is important for
diabetic patients since
Urine PCR at the time of biopsy 0.384 1.00 1.0 to 1.0RAAS
blockade therapy at thetime of biopsy
1.000 1.04 0.19 to 5.03
CI, condence interval; eGFR, glomerular ltration rate estimates;
eGFR, an absolutechange in eGFR; GLP-1, glucagon-like peptide-1;
HbA1c, glycated hemoglobin; HbA1c,an absolute change in HbA1c;
INTHbA1c, a variable consistent with the interactionbetween HbA1c
12 months before biopsy and HbA1c during the year before
biopsy;OHA, oral hypoglycemic agents; OR, odds ratio; PCR, protein
to creatinine ratio; RAAS,reninangiotensinaldosterone
system.treatment and prognosis may vary according to the underlying
cause.Several recent cross-sectional and longitudinal studies
have
reported associations between HbA1c and kidney function in
T2Dwith mixed results (Hsu, Chang, Huang, et al., 2012; Lee, Li,
Lin, et al.,2013; Lin, Chen, Chen, et al., 2013; Luk, Ma, Lau, et
al., 2013;Rodrguez-Segade, Rodrguez, Garca Lpez, Casanueva, &
Camia,2012; Sugawara, Kawai, Motohashi, et al., 2012). Lee and
colleagues(Lee et al., 2013) demonstrated a negative effect of
preceding HbA1c(recorded 1 year before) on eGFR in T2D patients
with CKD stages 3
unknown HbA1c during the year before biopsy
decrease in HbA1c during the year before biopsyincrease in HbA1c
during the year before biopsy
.1
.2
.3
.4
.5
.6
.7
.8
.9
5 6 7 8 9 10 11 12 13NGSP HbA1c 12 months before biopsy [%]
pro
babi
lity o
f NDR
D
Fig. 2. Predicted probabilities of having non-diabetic renal
disease in type 2 diabetes, bythe HbA1c 12 months before biopsy.
HbA1c, glycated hemoglobin; HbA1c, an absolutechange in HbA1c;
NDRD, non-diabetic renal disease; NGSP, National
GlycohemoglobinStandardization Program.
ic renal disease in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
-
5M. Pallayova et al. / Journal of Diabetes and Its Complications
xxx (2015) xxxxxxand 4. In our study, a trend towards the positive
association betweenthe HbA1c 12 months before biopsy and eGFR was
observed in thesubgroup with isolated DN (r = 0.56; P = 0.058; n =
12). There wasno association between the preceding HbA1c and eGFR
even after thepatients were grouped according to CKD stages. Of
importance, ourresults show that both the HbA1c 12 months before
biopsy and theabsolute change in HbA1c during the year before
biopsy differbetween patients with isolated DN and NDRD with
similarlydecreased eGFR at the time of renal biopsy. Our study is
consistentwith previous observations that annual variation in HbA1c
couldpredict DN in patients with T2D and that long-term variability
ofHbA1c predicts microalbuminuria (Hsu et al., 2012; Sugawara et
al.,2012) and development/progression of renal and
cardiovascularcomplications of T2D (Luk et al., 2013;
Rodrguez-Segade et al., 2012).
The ROC curve analysis of the three proposed
HbA1c-basedpredictive models showed that although both the HbA1c 12
monthsbefore biopsy and its change during the year before biopsy
predictedtype of renal disease, the model based on the interaction
between thetwo variables (INTHbA1c) had the best predictive
accuracy for NDRD.Since different predictors may be sensitive to
different aspects of renaldiseases, this new predictor may improve
the overall predictivecapability of the HbA1c-based models.
Fig. 3. ROC curve of the three HbA1c-based predictive models for
non-diabetic renaldisease. HbA1c, glycated hemoglobin; HbA1c, an
absolute change in HbA1c during theyear prior to biopsy; INTHbA1c,
an interaction term between the HbA1c 12 monthsbefore biopsy
predictor and theHbA1c during the year before biopsy predictor;
NDRD,non-diabetic renal disease; ROC, receiver operating
characteristic.In the present study, the patients histologically
diagnosed withNDRD had fairly good long-term diabetes control 12
months prior tobiopsy. Our ndings indicate that the HbA1c either
remains stable orgradually deteriorates in patients with NDRD
despite the decline inrenal function during the year prior to renal
biopsy. This observationmay be explained by the adverse impact of
inammatory and immuneresponses to progressive NDRD on glucose
control. Both acute andchronic inammation leads to stress
hyperglycemia, consistent with amaladaptive and detrimental
response to stress and inammation(Collier, Dossett, May, &
Diaz, 2008). Furthermore, in patients withisolated DN, the elevated
preceding HbA1c levels improved signi-cantly during the year before
renal biopsy. Decreased renal degrada-tion of insulin typically
ensues later in the course of CKD (Rabkin,Ryan, & Duckworth,
1984), which could account for the improvedglucose control prior to
biopsy in patients with isolated DN.
There are several limitations to our study that should
beconsidered in relation to the ndings. The relatively small
samplesize and retrospective nature precluded examination of
inuence ofethnicity, arterial hypertension, anemia, smoking, and
others. Data onsome clinical variables and characteristics were not
available for somepatients and thus could not be included in our
analyses. The exactstages of diabetic retinopathy could not be
established in each case to
Please cite this article as: Pallayova, M., et al., Predicting
non-diabethemoglobin, Journal of Diabetes and Its Complications
(2015), http://dx.further correlate with the type of renal disease.
A nal limitationconcerns the applicability of the results to
practical decisionmaking inthe general diabetic population, as only
T2D adults with suspicion ofunderlying NDRD were enrolled.
Despite these limitations, our study demonstrates a
considerablyhigh prevalence of histologically-proven NDRD in T2D
adults under-going renal biopsy. It also shows theHbA1c levels
during the year beforerenal biopsy differ between NDRD and isolated
DN. Besides thepredictive value of diabetic retinopathy, we have
identied the HbA1c12 months before biopsy and HbA1c as important
novel candidatepredictors of NDRD and DN in T2D. While HbA1c
remains the bestlong-termmarker of glycemic control in patients
with T2D, our ndingssuggest that annual evaluation of HbA1c and its
dynamic changes alongwith the assessment of diabetic retinopathy
could facilitate earlydetection of NDRD in T2D. Clinical signicance
of this nding isemphasized by the fact that the selection criteria
for renal biopsy inT2D adults are still not well established and
novel predictors of renaldisease are critically needed. Prospective
studies are needed to validatethe proposed HbA1c-based predictive
models for NDRD with a view torening the current selection criteria
for renal biopsy in T2D patients,and identify patients that will
benet from specic therapeuticinterventions that will reduce adverse
renal outcomes.
References
American Diabetes Association (2013). Standards of medical care
in diabetes2013.Diabetes Care, 36(Suppl. 1), S11S66.
Chang, T. I., Park, J. T., Kim, J. K., et al. (2011). Renal
outcomes in patients with type 2diabetes with or without coexisting
non-diabetic renal disease. Diabetes Researchand Clinical Practice,
92, 198204.
Chong, Y. B., Keng, T. C., Tan, L. P., et al. (2012). Clinical
predictors of non-diabetic renaldisease and role of renal biopsy in
diabetic patients with renal involvement: Asingle centre review.
Renal Failure, 34, 323328.
Collier, B., Dossett, L. A., May, A. K., & Diaz, J. J.
(2008). Glucose control and theinammatory response. Nutrition in
Clinical Practice, 23, 315.
Das, U., Dakshinamurty, K. V., Prayaga, A., & Uppin, M. S.
(2012). Nondiabetic kidneydisease in type 2 diabetic patients: A
single center experience. Indian Journal ofNephrology, 22,
358362.
Gross, J. L., de Azevedo, M. J., Silveiro, S. P., Canani, L. H.,
Caramori, M. L., & Zelmanovitz, T.(2005). Diabetic nephropathy:
Diagnosis, prevention, and treatment. Diabetes Care,28, 164176.
Harada, K., Akai, Y., Sumida, K., et al. (2013). Signicance of
renal biopsy in patients withpresumed diabetic nephropathy. Journal
of Diabetes Investigation, 4, 8893.
Hsu, C. C., Chang, H. Y., Huang, M. C., et al. (2012). HbA1c
variability is associated withmicroalbuminuria development in type
2 diabetes: A 7-year prospective cohortstudy. Diabetologia, 55,
31633172.
Kidney Disease: Improving Global Outcomes (KDIGO) CKDWork Group
(2013). KDIGO2012 Clinical Practice Guideline for the Evaluation
and Management of ChronicKidney Disease. Kidney International.
Supplement, 3, 1150.
Kleinknecht, D., Bennis, D., & Altman, J. J. (1992).
Increased prevalence of nondiabeticrenal pathology in type 2
diabetes mellitus. Nephrology, Dialysis, Transplantation,
7,12581259.
Lee, E. Y., Chung, C. H., & Choi, S. O. (1999). Non-diabetic
renal disease in patients withnon-insulin dependent diabetes
mellitus. Yonsei Medical Journal, 40, 321326.
Lee, C. L., Li, T. C., Lin, S. Y., et al. (2013). Dynamic and
dual effects of glycatedhemoglobin on estimated glomerular ltration
rate in type 2 diabetic outpatients.American Journal of Nephrology,
38, 1926.
Levey, A. S., Bosch, J. P., Lewis, J. B., Greene, T., Rogers,
N., & Roth, D. (1999). A moreaccurate method to estimate
glomerular ltration rate from serum creatinine: anew prediction
equation. Modication of Diet in Renal Disease Study Group. Annalsof
Internal Medicine, 130, 461470.
Lin, C. C., Chen, C. C., Chen, F. N., et al. (2013). Risks of
diabetic nephropathy withvariation in hemoglobin A1c and fasting
plasma glucose. The American Journal ofMedicine, 126,
1017.e11017.e10.
Luk, A. O., Ma, R. C., Lau, E. S., et al. (2013). Risk
association of HbA1c variability withchronic kidney disease and
cardiovascular disease in type 2 diabetes: Prospectiveanalysis of
the Hong Kong Diabetes Registry. Diabetes/Metabolism Research
andReviews, 29, 384390.
Mauer, M., Fioretto, P., Woredekal, Y., et al. (2001). Diabetic
nephropathy. In R. W.Schrier (Ed.), Diseases of the kidney and
urinary tract (pp. 20832116) (7th ed.).Philadelphia, PA: Lippincott
Williams & Wilkins.
Mazzucco, G., Bertani, T., Fortunato, M., et al. (2002).
Different patterns of renal damagein type 2 diabetes mellitus: A
multicentric study on 393 biopsies. American Journalof Kidney
Diseases, 39, 713720.
Olsen, S., &Mogensen, C. E. (1996).Howoften
isNIDDMcomplicatedwith non-diabetic renaldisease? An analysis of
renal biopsies and the literature. Diabetologia, 39, 16381645.
Pham, T. T., Sim, J. J., Kujubu, D. A., Liu, I. L., & Kumar,
V. A. (2007). Prevalence ofnondiabetic renal disease in diabetic
patients. American Journal of Nephrology, 27,322328.ic renal
disease in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
-
Rabkin, R., Ryan, M. P., & Duckworth, W. C. (1984). The
renal metabolism of insulin.Diabetologia, 27, 351357.
Richards, N. T., Greaves, I., Lee, S. J., Howie, A. J., Adu, D.,
& Michael, J. (1992). Increasedprevalence of renal biopsy
ndings other than diabetic glomerulopathy in type 2diabetes
mellitus. Nephrology, Dialysis, Transplantation, 7, 397399.
Rodrguez-Segade, S., Rodrguez, J., Garca Lpez, J. M., Casanueva,
F. F., & Camia, F.(2012). Intrapersonal HbA(1c) variability and
the risk of progression ofnephropathy in patients with type 2
diabetes. Diabetic Medicine, 29, 15621566.
Sharma, S. G., Bomback, A. S., Radhakrishnan, J., et al. (2013).
The modern spectrum ofrenal biopsy ndings in patients with
diabetes. Clinical Journal of the AmericanSociety of Nephrology, 8,
17181724.
Soni, S. S., Gowrishankar, S., Kishan, A. G., & Raman, A.
(2006). Non diabetic renaldisease in type 2 diabetes mellitus.
Nephrology (Carlton, Vic.), 11, 533537.
Stratton, I. M., Adler, A. I., Neil, H. A., et al. (2000).
Association of glycaemia withmacrovascular and microvascular
complications of type 2 diabetes (UKPDS 35):Prospective
observational study. BMJ, 321, 405412.
Sugawara, A., Kawai, K., Motohashi, S., et al. (2012). HbA1c
variability and thedevelopment of microalbuminuria in type 2
diabetes: Tsukuba Kawai DiabetesRegistry 2. Diabetologia, 55,
21282131.
The Diabetes Control and Complications Trial Research Group
(1993). The effect of intensivetreatmentof diabeteson
thedevelopment andprogressionof long-termcomplications
ininsulin-dependent diabetesmellitus. The New England Journal of
Medicine, 329, 977986.
The Microalbuminuria Collaborative Study Group (1999).
Predictors of the develop-ment of microalbuminuria in patients with
type 1 diabetes mellitus: A seven-yearprospective study. Diabetic
Medicine, 16, 918925.
UK Prospective Diabetes Study (UKPDS) Group (1998). Intensive
blood-glucose controlwith sulphonylureas or insulin compared with
conventional treatment and risk ofcomplications in patients with
type 2 diabetes (UKPDS 33). Lancet, 352, 837853.
Wong, T. Y., Choi, P. C., Szeto, C. C., et al. (2002). Renal
outcome in type 2 diabetic patientswith or without coexisting
nondiabetic nephropathies. Diabetes Care, 25, 900905.
Yaqub, S., Kashif,W., &Hussain, S. A. (2012). Non-diabetic
renal disease in patientswith type-2 diabetes mellitus. Saudi
Journal of Kidney Diseases and Transplantation, 23, 10001007.
6 M. Pallayova et al. / Journal of Diabetes and Its
Complications xxx (2015) xxxxxxPlease cite this article as:
Pallayova, M., et al., Predicting non-diabethemoglobin, Journal of
Diabetes and Its Complications (2015), http://dx.ic renal disease
in type 2 diabetic adults: The value of
glycateddoi.org/10.1016/j.jdiacomp.2014.12.005
Predicting non-diabetic renal disease in type 2 diabetic adults:
The value of glycated hemoglobin1. Introduction2. Subjects,
material and methods2.1. Statistical analyses
3. Results3.1. Sample characteristics and renal biopsy
findings3.2. Predictors of renal disease and risk factors for
adverse renal outcomes
4. DiscussionReferences