Embed Size (px)
Citation preview

www.elsevier.com/locate/humpath
Human Pathology (2013) 44, 320–328
Original contribution
Papillary thyroid carcinoma with hobnail features:histopathologic criteria to predict aggressive behavior☆,☆☆
Sofia Asioli MDa,⁎, Lori A. Erickson MDb, Alberto Righi MDa,Ricardo V. Lloyd MD, PhD c
aDepartment of Biomedical Sciences and Human Oncology, University of Turin, 10126 ItalybDepartment of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN 55905, USAcUniversity of Wisconsin School of Medicine and Public Health, Madison, WI 53703, USA
Received 8 May 2012; revised 6 June 2012; accepted 10 June 2012
pTP
0h
Keywords:Hobnail;Papillary carcinoma;Thyroid
Summary Recent reports indicate that papillary thyroid carcinoma with hobnail features, also designatedas micropapillary variant of papillary thyroid carcinoma, is a rare but very aggressive variant ofpapillary thyroid carcinoma. We examined the histopathologic and immunohistochemical features of 24cases of papillary thyroid carcinoma with hobnail/micropapillary component to determine the prognosticsignificance of the amount of hobnail/micropapillary features in these tumors. The patients included 18women and 6 men. Ages ranged from 28 to 78 years (mean, 57 years). Tumor size ranged from 1 to 5.8cm (mean, 3 cm). The average follow-up time was 106 months (range, 4-274 months). Twelve cases(50%) of papillary thyroid carcinoma showed more than 30% hobnail/micropapillary features, and allbut 3 cases were associated with an aggressive behavior. During the follow-up, 6 of these patients diedof disease after a mean of 44.8 months, and 3 patients remained alive with extensive disease after amean follow-up of 32.3 months. Metastases to lymph nodes or distant organs showed a hobnail patternof growth similar to the primary tumor. The remaining 3 patients with prominent hobnail/micropapillaryfeatures were alive with no evidence of disease after a mean follow-up of 125.3 months. The other 12papillary thyroid carcinoma cases (50%) showed less than 30% hobnail/micropapillary features. Nine ofthese patients were alive without disease after a mean of 162 months, and 1 patient died of sepsis, whichwas not related to thyroid tumor after 155 months. Two patients in this group died of disease after 21and 163 months, respectively. These findings confirm earlier observations that papillary thyroidcarcinoma with hobnail/micropapillary features is an aggressive variant of papillary thyroid carcinoma.Tumors with more than 30% hobnail/micropapillary features were often very aggressive, although 2patients with tumors with 10% hobnail/micropapillary features also had poor outcomes.© 2013 Elsevier Inc. All rights reserved.
☆ Disclosure Summary: All authors declare the absence of any conflict of interest.☆☆ This work was supported by grants of the Italian Ministry of University (ex-60%) and Ricerca Sanitaria Finalizzata Piedmont Region (to S. A.). A.R. is
art of and funded by the PhD programme “Scienze Biomediche ed Oncologia Umana: Tecniche avanzate di localizzazione dei tumori umani,” University ofurin. Preliminary results from this article were published as a platform presentation at the 101th Annual Meeting of the United States and Canadian Academy ofathology (Vancouver, British Columbia, Canada, March 2012).⁎ Corresponding author.E-mail address: [email protected] (S. Asioli).
046-8177/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2012.06.003

321Hobnail features predict aggressive behavior
1. Introduction
The “hobnail” variant of papillary thyroid carcinoma(PTC) is a newly described entity most striking for itshobnail and micropapillary patterns and a high nuclear/cytoplasmic (N/C) ratio, with apically placed and occasion-ally grooved bulging nuclei that form characteristic hobnailcells in at least 30% of the neoplastic cells [1].
Recent reports indicate that the hobnail variant ofpapillary carcinoma is a rare, moderately differentiatedvariant of PTC with aggressive behavior, most likely due to ahigh stage at presentation and a high propensity for lymphnode metastases, and significant mortality [1-6].
The general concept of loss of cellular polarity has beenused to describe similar thyroid type tumors (called micro-papillary PTC), which may be related to micropapillarycarcinomas in other sites such as the breast, pancreas, lung,and urinary bladder [7-9]. Although micropapillary carcino-ma can be diagnosed as a pure histologic type, they are moreoften found admixed with other types of cancers [10].
Studies from other organs such as the breast thatcategorized the tumors intogroups according to thepercentageof micropapillary component have found no correlationbetween the proportion of micropapillary carcinoma and thepercentage of lymph node metastasis or lymphovascularinvasion; tumors with any amount of micropapillary patternshowed a higher propensity for lymphovascular invasion andlymph node metastasis compared with other types ofcarcinoma [8,10].
Although micropapillary component may not be anindependent predictor of an aggressive clinical behavior,the characteristic hobnail pattern with variable degrees ofmicropapillary features appears to be associated with a pooroutcome [10].
Some other variants of PTC such as classical and diffusesclerosing in rare cases could show a micropapillary patternof growth (personal observation).
The aim of the present study was to define the prevalenceof this PTC tumor type and to evaluate the prognosticsignificance of the amount of hobnail/micropapillary featuresin these tumors.
2. Materials and methods
2.1. Patient selection
We reviewed 3551 primary PTCs from patients whounderwent primary surgical treatment for thyroid carcinomabetween 1955 and 2004 at the Mayo Clinic, Rochester, MN(2534 cases) and at the Molinette Hospital & University ofTurin, Italy (1017 cases), during the period 1992 to 2011. Atotal of 22 cases of PTC with hobnail/micropapillary featureswere identified from the Mayo Clinic of Rochester, MN (16cases), and the University of Turin, Italy (6 cases). Thefollowing selection criteria were used: correlation to
previously reported diagnostic criteria for hobnail PTC [1]including loss of polarity/cohesiveness with hobnail/micro-papillary features in 10% or more of the tumor cells andavailability of clinical and follow-up data and of pathologicmaterial (slides and paraffin blocks). The hobnail cellsshowed increased N/C ratios, moderately to highly pleo-morphic nuclei located in the middle or apex of thecytoplasm, and abundant cytoplasm with eosinophilia. Twoadditional cases, meeting the above diagnostic criteria, wereincluded from the consultation files of the authors. Eight ofthese cases had been included in a previous study [1].
Institutional review board permission was obtained forthe study.
Data regarding age, sex, presentation, gross pathology, andpostsurgery radiotherapy (iodine radiotherapy and externalbean radiotherapy) were obtained by review of clinical filesand contacting the referring pathologist or clinician.
The pathologic staging was assigned according to theSeventh Edition Cancer Staging Manual of the AmericanJoint Committee on Cancer [11].
Disease persistence, recurrence, and metastases wereevaluated by medical record review, imaging studies, orhistopathologic examination of resected or recurrent tumorsand/or metastases.
2.2. Immunohistochemistry
We examined a mean of 6 (range, 3-10) hematoxylin andeosin–stained microscopic slides. In all cases, we examinedat least 1 section for each centimeter of the tumor for thepresence of cellular polarity/cohesiveness with hobnail/micropapillary features according to above selection criteria.Additional sections were cut and stained with antibodiesagainst thyroid transcription factor 1 (TTF-1) (8G7G3/1,1:700; Dako, Carpinteria, CA), thyroglobulin (2H11/6E1cocktail, 1/50BRD; Zymed, San Francisco, CA), p53 (DO7,1:2000; Dako), mitochondria (JJ3-J, 1:100; Bio Genex, SanRamon, CA), Mucin 1 (MUC 1) (Ma695, 1:100; Novocastra,Newcastle upon Tyne, UK), cytokeratin 7 (OB-TL12/30,1:200; Dako), cytokeratin 19 (RCK 108, 1:20; Dako), E-cadherin (4A2C7, 1:100; Zymed), β-catenin (E-5, 1:200;Santa Cruz, Santa Cruz, CA), epithelial membrane antigen(E29, 1:50; Dako), HBME1 (HBME1, 1:40; Dako), and Ki-67 (MIB-1, 1:300; Dako). Immunoreactions were performedaccording to the standard automated immunohistochemicalprocedure (Ventana XT autostainer; Ventana MedicalSystems, Tucson, AZ). Immunoreactions were developedusing biotin-free dextran-chain detection system (EnVision;Dako), and immunoreactions were developed using diami-nobenzidine as the chromogen.
2.3. Statistical analysis
All data were analyzed using Stata\SE statistical software(version 10.0; StataCorp LT, College Station, TX). A level ofP b .05 was considered to be statistically significant.

Table 1 The clinical and pathologic features of 24 cases of PTC with hobnail/micropapillary features
Case Age/sex Size (cm) Vascularinvasion
Nuclearatypia
Mitoses(atypicalmitoses)
Percentage ofhobnail/MPfeatures
PostsurgicalRT
Localrecurrence
Lymph nodes METS Distant METS(site)
pTNM FU(mo)
1 51/F 2.00 Yes Severe 9 (1) 75 Yes No NA Liver, lung,bone, brain,spinal cord
T1 (m) NX M1 DOD (6)
2 78/F 4.00 Yes Moderate 4 100 Yes Yes Yes No T3 (m) N1a M0 DOD (10)3 63/F 1.00 Yes Moderate 3 60 No No Yes Lung T1 N1a M1 DOD (31)4 28/F 1.20 No Moderate 3 30 Yes Yes Yes No T3 (m) N0 M0 AND (120)5 58/M 1.80 Yes Moderate 4 75 Yes Yes Yes Shoulder soft
tissue, lung,bone, muscle,pancreas
T3 (m) N1b M1 AWD (87)
6 53/F 3.50 Yes Severe 5 (1) 75 Yes No Yes No T2 N0 M0 AND (236)7 65/F 2.80 Yes Moderate 6 50 Yes No Yes Brain, lung T3 (m) N1b M1 DOD (124)8 65/M 4.00 Yes Severe 3 75 Yes No Yes Epiglottis, larynx,
nasopharynx,base of tongue,tonsils
T3 (m) N1b M1 AWD (4)
9 76/F 5.50 Yes Moderate 3 35 Yes No Yes Brain, lung T3 (m) N1b M1 DOD (16)10 66/F 2.50 No Moderate 4 50 No No No No T3 (m) N0 M0 AND (20)11 66/M 1.70 Yes Moderate 4 40 Yes No Yes Epiglottis,
larynx,nasopharynx
T3 (m) N1a M0 AWD (6)
12 62/F 5.80 Yes Moderate 3 40 Yes No Yes Lung T3 (m) N1a M0 DOD (82)13 74/M 6.00 Yes Moderate 2 10 Yes Yes Yes Lung T3 N1b M0 DOD (163)14 60/M 2.60 No Moderate 1 10 No No No No T2 N0 M0 AND (170)15 48/F 3.50 Yes Moderate 1 10 No No No No T3 (m) N0 M0 DOC (155)16 56/F 1.50 No Moderate 1 10 No No No No T1b N0 M0 AND (274)17 43/F 1.20 No Moderate 1 10 No No No No T1b N0 M0 AND (272)18 57/F 2.50 Yes Moderate 1 10 Yes Yes Yes Bone, neck
soft tissueT3(m) N1b M1 DOD (21)
19 45/M 7.00 Yes Moderate 1 10 Yes No Yes NA T3(m) N1a M0 AND (183)20 52/F 1.00 Yes Moderate 1 10 No No No No T1b N0 M0 AND (202)21 50/F 2.00 No Moderate 1 10 Yes No No No T2 N0 M0 AND (154)22 36/F 3.90 Yes Moderate 2 10 Yes No Yes No T2 N1a M0 AND (75)23 59/F 1.40 Yes Moderate 5 10 Yes No No No T3 (m) N0 M0 AND (22)24 64/F 2.30 No Moderate 2 10 No No No No T2 N0 M0 AND (102)
Abbreviations: F, female; M, male; MP, micropapillary; RT, radiotherapy; METS, metastases; pTNM, pathological Tumor, lymph Nodes, Metastasis status; FU, follow-up; NA, not available; DOD, dead ofdisease; AND, alive with no disease; AWD, alive with disease; DOC, dead of other causes.
322S.
Asioliet
al.

323Hobnail features predict aggressive behavior
Clinicopathologic variables were investigated for theirpossible association with the presence of a micropapillary/hobnail pattern in at least 30% of the tumors. Categoricalvariables were analyzed by Fisher exact tests of contingencytables. Numerical variables were analyzed using the Mantel-Cox log-rank test that compares median differences. Survi-val time was defined as time from the date of first surgery totime of death (or last follow-up). We also looked at 2 otherevents: disease-free survival and time to distant metastasis.The time to events was each compared between groupsinitially with log-rank tests and illustrated using Kaplan-Meier curves. Survival was also compared between groupsusing Cox proportional-hazards regression from whichhazard ratios (HRs) were estimated.
3. Results
3.1. Clinical features
The clinical and pathologic features are summarized inTable 1. The prevalence of PTC with hobnail/micropapillaryfeatures (at least 10% of the tumor) was 0.63% (16/2534) ofall PTC diagnosed at the Mayo Clinic, Rochester, MN,during the period 1955 to 2004 and 0.59% (6/1017) at theMolinette Hospital, University of Turin, Italy, during theperiod 1992 to 2011. The mean patient age was 57.3 years(range, 28-78 years). A female predominance was observed(female/male ratio, 3:1).
All patients underwent total thyroidectomy and cervicallymph node dissection. Radioiodine therapy was given (1-8doses of 131I between 3700 and 7400 MBq) after totalthyroidectomy in 16 patients. Follow-up data were availablefor all 24 patients with a mean of 106 months (range, 4-274months). Clinically aggressive tumors, including those with
Table 2 Clinicopathologic characteristics of study group
Characteristics PTC hobnail/MP b 30% (12 cases) PTC h
Sex (female/male) 9 F:3 M 9 F:3Age (y), mean 54 60.9Tumor size (cm), mean 2.91 2.99Vascular invasionYes 7 10No 5 2Extrathyroid extensionYes 9 5No 3 7Radioactive iodine therapyYes 10 6No 2 6StageI and II 7 2III and IV 5 10Overall survival5-y overall survival rate 91.7% (95% CI, 53.9-98.8) 43.6%10-y overall survival rate 91.7% (95% CI, 53.9-98.8) 32.8%
recurrences or metastatic spread and/or patient death,accounted for 12 (50%) of the 24 tumors. During follow-up,local recurrence was observed in 5 cases, metastases to lymphnodes in 13 cases, and to distant metastases in 10 cases.
The estimated 5- and 10-year survival rates were 69.1%(95% confidence interval [CI], 45.6%-84%) and 64.1% (95%CI, 40.6%-80.3%), respectively (Table 2).
3.2. Pathologic and immunohistochemical features
The mean tumor size was 2.95 cm (range, 1-7 cm). Thetumors were described as multiple nodules present in boththyroid lobes in 58.3% (14/24) of cases. Of 24 patients, 9 hadno evidence of pathologically involved lymph nodes or ofmetastatic disease (stage I or II), whereas 7 cases hadpathologically involved lymph nodes (stage III) and 8 casesdistant metastases at presentation (stage IV).
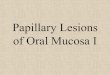
Vascular invasion was identified in 17 (70.8%) of 24patients. Necrosis was absent in all cases. Moderate nuclearatypia was observed in 21 cases, whereas in 3 cases, it wassevere. We observed a mean of 2.9 mitoses per 10 high-powered fields (×400) (range, 1-9), and in 2 cases, atypicalmitoses were present (Fig. 1A-D).
Additional slides from 14 cases were available forimmunohistochemical studies. All of these cases werepositive for thyroglobulin, TTF-1, and p53 (N25% of theneoplastic cell nuclei) in primitive thyroid tumor and inlymph nodes metastases, when present; conversely, distantmetastases showed strong positivity for TTF-1 and p53 in all10 cases, although thyroglobulin was negative in all but 2cases (metastases to the liver in case 1 and to the lung in case9). β-Catenin and E-cadherin showed patchy lateral and orbasolateral membrane positivity in all cases (Fig. 1E).Immunohistochemistry for epithelial membrane antigen was
obnail/MP N 30% (12 cases) Total (24 cases) P
M 18 F:6 M 157.3 .2212.95 .673
17 .3717
14 .21410
16 .1938
9 .08915
(95% CI, 14.41-70.3) 69.1% (95% CI, 45.60-84.0) .026(95% CI, 8.16-60.9) 64.1% (95% CI, 40.6-80.3)

Fig. 1 PTCs with prominent hobnail/micropapillary features. In case 1, the tumor shows a prominent papillary architecture with focalmicropapillary areas (A-D). A, A prominent papillary architecture is noted. B, This included variably sized complex papillary structures withprominent vascular cores. C, Cuboidal or oval epithelium-covered papillary and micropapillary structures with a high N/C ratio and apicallyplaced and occasionally grooved with nuclei that produce a surface bulge leading to a hobnail appearance are present. C, Occasional pinkintranuclear holes are observed (inset). D, Focal areas with micropapillae showed nuclear stratification, and mitotic figures are present.Immunohistochemical analysis for E-cadherin (E) showed patchy lateral and or basolateral membrane positivity (E, inset) in all cases, whereasMUC1 (F) showed the characteristic inside-out staining pattern in the micropapillary component (F, inset).
324 S. Asioli et al.

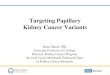
ig. 2 Overall survival (A), distant metastases (B), and disease-ee survival (C) distribution based on the Kaplan-Meier product-mit estimates of hobnail/micropapillary PTC (≥30% of the tumorells) according to the percentage of hobnail/micropapillary
325Hobnail features predict aggressive behavior
present in all cases with nuclear staining in 10 cases andcytoplasm in 4 cases. MUC1 showed the characteristic“inside-out” staining pattern [12] in all cases showing themicropapillary component (Fig. 1F). The proliferative indexevaluated with Ki-67 antibody ranged from 2% to 20% witha mean of 10% of the neoplastic cells. All cases examinedwere negative for antimitochondria antibody.
Based on the percentage of hobnail/micropapillaryfeatures, we divided PTC cases into 2 groups. The firstgroup included 12 (50%) of 24 PTC cases with prominent(≥ 30% of the tumor) hobnail/micropapillary features, andthe other included PTC cases that showed foci of hobnail/micropapillary features in less than 30% of the tumor. Inparticular, in the first group, the proportion of thiscomponent varied between 30% and 100% with a mean of58% of the PTC tumor; conversely, in the other group, itcorresponded to 10% of the tumor area in all cases.
All but 3 cases of PTC, showing 30% or more hobnail/micropapillary features, were associated with an aggressivebehavior during follow-up. In particular, 6 of these patientsdied of disease after a mean of 44.8 months, and 3 patientswere alive with extensive disease involving the epiglottis,larynx, and nasopharynx in 2 cases and the shoulder, lung,bone, muscle, and pancreas in 1 case after a mean follow-up of 32.3 months. Recurrence and metastases to lymphnodes or distant organs showed a predominant hobnailpattern of growth similar to the primary tumor in a similarproportion compared with the corresponding primarytumor. The other 3 patients with prominent hobnail/micropapillary features were alive without evidence ofdisease after a mean follow-up of 125.3 months.
Of the other 12 PTC cases showing focal hobnail/micropapillary features (approximately 10% of the tumor), 9were alive without disease after a mean of 162 months, and 1patient died of sepsis, which was not related to thyroid tumorafter 155 months. Two patients in this group died of diseaseafter 21 and 163 months, respectively.
3.3. Survival analysis
When comparing both groups (Table 2), significantdifferences in overall survival (P = .026) between the PTCcases with focal or predominant hobnail/micropapillary featureswere observed. There was no difference in male/female ratio,age, tumor size, vascular invasion, extrathyroid extension,radioactive iodine therapy, and stage between groups.
The predominant hobnail/micropapillary features in PTCwere associated with an increased risk of death (HR, 2.95; P =.026; Fig. 2A), distant metastases (HR, 3.77; P = .0015;Fig. 2B), and with a decrease of disease-free survival (HR,4.02; P = .0035; Fig. 2C).
atures in the tumor cells (dashed line indicates PTC group with30% of hobnail/micropapillary features; continuous line, PTCroup with ≥30% of hobnail/micropapillary features). Theredominant hobnail/micropapillary features (≥30% of the tumorells) in PTC were associated with an increased risk of death (P =26) and distant metastases (P = .0015).
4. Discussion
A series of 8 cases of PTC with hobnail features wasrecently reported by Asioli et al [1]. A papillary pattern with
Ffrlicfebgpc.0

326 S. Asioli et al.
variably sized papillae and the presence of variable amountsof micropapillary structures and prominent vascular coreswas most common (6/8 cases). Traditional features of PTCwere present in these cases, but these were only focallyrecognized. Nuclei were located in the middle or apex of thecytoplasm, giving a hobnail appearance. This small cohortof patients demonstrated an aggressive clinical course.Distant metastases were present in 5 of 8 patients in variousorgans including the bone and brain. Of this small group,half (4) died of disease in 3.5 years, and 2 were alive withdisease, whereas the other 2 were alive with no evidence ofdisease. The present series of a larger number of hobnail/micropapillary carcinoma extends our knowledge of thisvariant and indicates that even a smaller percentage ofhobnail/micropapillary features can be associated with anaggressive behavior.
A micropapillary pattern of growth in epithelialmalignancies was first described in the breast and ovaryand, subsequently, in other organs, including the bladder,lung, pancreas, salivary glands, and gastrointestinal tract[7-10,13,14].
Cases of pure micropapillary carcinoma were reportedonly in the breast and ovary and are rarely observed [13].Published studies reported that the proportion of micro-papillary component with respect to the entire tumor rangedfrom 5% to 80% but was often less than 30% of the entirelesion [7-10,13,14]. Even if present as a small component inthe primary tumor, a micropapillary growth pattern isimportant to be recognized because in most publishedstudies, this peculiar histology appears to be associated witha poor outcome most likely because of a high stage atpresentation and a high propensity for lymph nodemetastases [7-10,13,14].
The inverted polarity of the cells that compose themicropapillary nests with an inside-out growth pattern [12],which has been shown by immunohistochemical andultrastructural studies [15,16], seems to be most likelyrelated to the high invasive potential and drug resistance ofthese tumors specially in breast carcinoma [17].
The histologic micropapillary carcinoma profile de-scribed in other studies [8,10,18] was characterized bysmall pseudopapillary clusters of cancer cells with invertedcell polarity, which was also confirmed immunohisto-chemically by the membranous staining pattern of MUC1(clone MA695), toward the stromal pole only, in the tumorcell clusters.
In the present case series of hobnail/micropapillaryvariant of PTC, the hobnail cells showed increased N/Cratios, moderately to highly pleomorphic nuclei locatedin the middle or apex of cytoplasm, and abundantcytoplasm with eosinophilia. In our cases of PTC,micropapillary growth pattern and hobnail features seemto overlap even if the micropapillary growth patternseems to be more related with an architectural feature,whereas the hobnail appearance is rather referred to acellular characteristic.
The low proportion of hobnail/micropapillary carcinomacomponent in the global tumor volume and its prognosticrelevance indicate that the number of sections studied iscritical in the evaluation of these tumors. An increase in thenumber of sections routinely studied, especially sampling atthe tumor-infiltrating edge, can likely result in a higherincidence of detection of the hobnail/micropapillary variantof thyroid carcinoma. In the surgical specimens, andprobably also in cytologic samples, it may be importantto report the presence of hobnail/micropapillary featureseven if they constitute a small proportion in the tumorbecause the poor prognosis may not depend on this ratiobut rather on the mere presence of such component(Table 2).
Hobnail/micropapillary variant of PTC in the presentseries showed focal positivity for E-cadherin in thebasolateral or lateral site of tumor cells with loss ofexpression of this protein in most of the tumors. This partialloss of E-cadherin expression in hobnail/micropapillaryPTC cells could be a step toward the epithelial tomesenchymal transition (EMT) that has recently beenrecognized as an important mechanism of epithelial tumorprogression, local invasion, and metastasis. In particular,the E-cadherin repressor Slug and the basic helix-loop-helixtranscription factor Twist inhibit E-cadherin expression inpoorly differentiated malignancies, acting as EMT inducers[19]. Very little is known about the expression of EMTregulators in thyroid cancer. Recently, Buehler et al [19]reported that the EMT regulators Slug and Twist areexpressed in anaplastic thyroid carcinomas and areassociated with absence of E-cadherin, supporting the roleof EMT in this cancer.
In addition, changes in cell orientation with loss ofpolarity highlighted by hobnail features of the tumor cellsand possibly alterations in specific glycoproteins such asMUC1 [15] may contribute to the higher propensity tometastasize to sites uncommon for conventional PTCs.
Thus, molecular changes such as p53 overexpression andB-type Raf kinase (BRAF) mutations that we describedpreviously [1] may be important parameters to explain themore aggressive behavior of the tumors in our series.
Some other variants of PTC such as tall and columnarcells may behave more aggressively than classical PTCs[20]. Tall cell variant of PTC is one of the more commonaggressive types of PTC. It is important to recognize the tallcell variant because of a worse prognosis and a higherrecurrence rate associated with this variant. This tumorvariant usually affects older men, is often large at the time ofpresentation, and is accompanied by vascular and extrathy-roidal extensions. In the histology, at least 50% of theneoplastic cells must be characterized by cells with granulareosinophilic cytoplasm whose height are at least twice theirwidth. Predominance of these features is necessary fordiagnosing such variants. Nevertheless, it is suggested thatpathologists should indicate whether there is a significantamount of tall cells in a PTC in their reports. Recently,

327Hobnail features predict aggressive behavior
Ganly et al [21] reported that consideration should be givento use a 30% tall cell threshold to diagnose tall cell variantof PTC such as that previously suggested by Asioli et al [1]for PTC with hobnail features. Moreover, Dettmer et al [22]suggested that 10% of tall cell quantity within a PTC isstrongly associated with an adverse clinical outcome andshould therefore be reported. The cells can form papillary ortrabecular structures with characteristic nuclear featuresincluding exaggerated grooves. Necrosis, pleomorphism,and mitoses are not uncommon in this variant, whereas PTCwith hobnail/micropapillary features showed high pleomor-phism and mitotic figures, including atypical mitosis. Tallcell variant shows more aggressive behavior regardless ofsize, sex, and age. Even tumors confined to the thyroidshow a higher rate of lymph node metastases, as observed inthe present series [23]. Some studies suggest that molecularfactors are responsible for aggressive biological behavior ofthis variant such as high expression of MUC1 [24,25]. Inaddition, a higher prevalence of BRAF mutation incomparison with classic PTC could also have a role in theaggressive biological behavior of this variant. All of theseimmunohistochemical and molecular features overlap withour hobnail/micropapillary PTC [26-29].
The columnar cell PTC is a rare variant of PTC that isalso apparently associated with a more aggressivebehavior, and patients usually present with extrathyroidalextension at the time of diagnosis as observed in thepresent cases of PTC with hobnail/micropapillary features.However, Gaertner et al [30] reported that the morpho-logical designation of columnar variant is not a significantfactor predicting biological behavior compared with thepredictive role of clinical stage. To diagnose this variant,most of the tumor should be composed of pseudostratifiedcolumnar cells with elongated hyperchromatic nuclei andsupranuclear and subnuclear cytoplasmic vacuoles. Intra-cytoplasmic vacuoles are periodic acid-Schiff positive,diastase sensitive, and negative for mucicarmine. Thecharacteristic nuclear features of PTC are usually lessapparent in this variant. If the tumor metastasizes to alymph node, it might be confused with a colonic orendometrial adenocarcinoma. Immunohistochemical stainsfor TTF-1 and thyroglobulin can be helpful in thedifferential diagnosis [31].
In conclusion, thyroid PTC with hobnail/micropapillaryfeatures appears to be more aggressive than conventionalPTC, regardless of the proportion of hobnail/micropapillaryfeatures. In particular, all the cases in this series had hobnailhistology, but only 50% had micropapillary features, so wethink that the hobnail features are more important in thediagnosis and prognosis of these carcinomas (as well as thepreferred designation as hobnail). In addition, both of thesemorphological features (micropapillary and hobnail) corre-late with the loss of polarity that is present in thesecarcinomas. More studies are needed to better define themolecular significance of hobnail/micropapillary compo-nents in PTC.
References[1] Asioli S, Erickson LA, Sebo TJ, et al. Papillary thyroid carcinoma with
prominent hobnail features: a new aggressive variant of moderatelydifferentiated papillary carcinoma. A clinicopathologic, immunohis-tochemical, and molecular study of eight cases. Am J Surg Pathol2010;34:44-52.
[2] Motosugi U, Murata S, Nagata K, Yasuda M, Shimizu M. Thyroidpapillary carcinoma with micropapillary and hobnail growth pattern: ahistological variant with intermediate malignancy? Thyroid 2009;19:535-7.
[3] Bai Y, Kakudo K, Nakamura M, et al. Loss of cellular polarity/cohe-siveness in the invasive front of papillary thyroid carcinoma andperiostin expression. Cancer Letters 2009;281:188-95.
[4] Liu Z, Kakudo K, Bai Y, et al. Loss of cellular polarity/cohesiveness inthe invasive front of papillary thyroid carcinoma, a novel predictor forlymph node metastasis; possible morphological indicator of epithelialmesenchymal transition. J Clin Pathol 2011;64:325-9.
[5] Liu Z, Bai Y, Li Y, et al. Non-solid type thyroid carcinoma: a casereport of moderately differentiated adenocarcinoma of the thyroid.Pathol Int 2010;60:524-7.
[6] Lino-Silva LS, Domínguez-Malagón HR, Caro-Sánchez CH, Salcedo-Hernández RA. Thyroid gland papillary carcinomas with “micropapil-lary pattern,” a recently recognized poor prognostic finding: clinico-pathologic and survival analysis of 7 cases. HUM PATHOL 2012;43:1596-600.
[7] Amin MB, Ro YJ, el-Sharkawy T, et al. Micropapillary variant oftransitional cell carcinoma of the urinary bladder. Histologic patternresembling ovarian papillary carcinoma. Am J Surg Pathol 1994;18:1224-32.
[8] Ueng SH, Mezzetti T, Tavassoli FA. Papillary neoplasms of the breast:a review. Arch Pathol Lab Med 2009;133:893-907.
[9] Travis WD, Brambilla E, Noguchi M, et al. International Associationfor the Study of Lung Cancer/American Thoracic Society/EuropeanRespiratory Society International Multidisciplinary Classification ofLung Adenocarcinoma. J Thorac Oncol 2011;6:244-85 [Review].
[10] Nassar H. Carcinomas with micropapillary morphology: clinicalsignificance and current concepts. Adv Anat Pathol 2004;11:297-303[Review].
[11] Edge SBBD, Byrd DR, Compton CC, et al. Cancer Staging Handbook(from the AJCC Cancer Staging Manual). 7th ed. New York, NY:Springer-Verlag; 2010.
[12] Peterse JL. Breast carcinoma with an unexpected inside out pattern.Rotation of polarization associated with angioinvasion. Path Res Pract1993;189:780.
[13] Verdú M, Román R, Calvo M, et al. Clinicopathological and molecularcharacterization of colorectal micropapillary carcinoma. Mod Pathol2011;24:729-38.
[14] Ushiku T, Matsusaka K, Iwasaki Y, et al. Gastric carcinoma withinvasive micropapillary pattern and its association with lymph nodemetastasis. Histopathology 2011;59:1081-9.
[15] Nassar H, Pansare V, Zhang H, et al. Pathogenesis of invasivemicropapillary carcinoma: role of MUC1 glycoprotein. Mod Pathol2004;17:1045-50.
[16] Li YS, Kaneko M, Sakamoto DG, et al. The reversed apical pattern ofMUC1 expression is characteristics of invasive micropapillarycarcinoma of the breast. Breast Cancer 2006;13:58-63.
[17] Doublier S, Belisario DC, Polimeni M, et al. HIF-1 activation inducesdoxorubicin resistance in MCF7 3-D spheroids via P-glycoproteinexpression: a potential model of the chemo-resistance of invasivemicropapillary carcinoma of the breast. BMC Cancer 2012;12:4.
[18] Kim MJ, Hong SM, Jang SJ, et al. Invasive colorectal micropapillarycarcinoma: an aggressive variant of adenocarcinoma. HUM PATHOL2006;37:809-15.
[19] Buehler D, Hardin H, Shan W, Rehrauer W, Chen H, Lloyd RV.Expression of epithelial-mesenchymal transition regulators Slug andTwist in thyroid carcinomas. Mod Pathol 2012;25:142A.

328 S. Asioli et al.
[20] Rosai J, Carcangui ML, DeLellis RA. Tumors of the Thyroid Gland.Atlas of Tumor Pathology. Third Series. Fascicle 5. Washington, DC:Armed Forces Institute of Pathology; 1992.
[21] Ganly I, Ibrahimpasic T, Rivera M, et al. Prognostic implications ofpapillary thyroid carcinoma with tall cell features. Mod Pathol2012;25:144A.
[22] Dettmer MS, Schmitt A, Steinert H, Moch H, Komminoth P, Perren A.Tall cell variant of papillary thyroid carcinoma—how many tall cellsare needed? Mod Pathol 2012;25:143A.
[23] Ghossein RA, Leboeuf R, Patel KN, et al. Tall cell variant of papillarythyroid carcinoma without extrathyroid extension: biologic behaviorand clinical implications. Thyroid 2007;17:655-61.
[24] Wreesmann VB, Sieczka EM, Socci ND, et al. Genomewide profilingof papillary thyroid cancer identifies MUC1 as an independentprognostic marker. Cancer Res 2004;64:3780-9.
[25] Campo E, Merino MJ, Liotta L, et al. Distribution of the 72-kd type IVcollagenase in nonneoplastic and neoplastic thyroid tissue. HUM PATHOL1992;23:1395-401.
[26] Kebebew E, Weng J, Bauer J, et al. The prevalence and prognosticvalue of BRAFmutation in thyroid cancer. Ann Surg 2007;246:466-70.
[27] Lupi C, Giannini R, Ugolini C, et al. Association of BRAF V600Emutation with poor clinicopathological outcomes in 500 consecutivecases of papillary thyroid carcinoma. J Clin Endocrinol Metab2007;92:4085-90.
[28] Nikiforova MN, Kimura ET, Gandhi M, et al. BRAF mutations inthyroid tumors are restricted to papillary carcinomas and anaplastic orpoorly differentiated carcinomas arising from papillary carcinomas.J Clin Endocrinol Metab 2003;88:5399-404.
[29] Riesco-Eizaguirre G, Gutierrez-Martinez P, Garcia-Cabezas MA, et al.The oncogene BRAF V600E is associated with a high risk ofrecurrence and less differentiated papillary thyroid carcinoma due tothe impairment of Na +/I- targeting to the membrane. Endocr RelatCancer 2006;13:257-69.
[30] Gaertner EM, Davidson M, Wenig BM. The columnar cell variant ofthyroid papillary carcinoma: case report and discussion of an unusuallyaggressive thyroid papillary carcinoma. Am J Surg Pathol 1995;19:940-7.
[31] Chen JH, Faquin WC, Lloyd RV, Nosé V. Clinicopathological andmolecular characterization of nine cases of columnar cell variant ofpapillary thyroid carcinoma. Mod Pathol 2011;24:739-49.