Embed Size (px)
Citation preview

Case Report
Paradental Cyst: Report of Two Cases
Claudia M. Kanno,* Jessica L. Gulinelli,† Maria J.H. Nagata,‡ Ana M.P. Soubhia,§
and Marcelo M. Crivelini§
Background: The paradental cyst is an odontogen-ic lesion of inflammatory origin that has few clinicalsigns and symptoms apart from recurring acute epi-sodes. A well-defined radiolucency associated withthe roots or distal to the crown may be seen radio-graphically. The purpose of this article is to report ondifferent aspects of two cases involving paradentalcysts. In the first case, the patient complained aboutrecurring pericoronitis. A semilunar-shaped radiolu-cency on the distal aspect of the mandibular thirdmolar was noted on the periapical radiograph. Inthe second case, the patient’s main complaint waschronic trauma of the overlying mucosa. Radiographsrevealed an enlarged pericoronal space.
Methods: In both cases, the mandibular third molarwas extracted due to a lack of space. Lesional sampleswere sent for histopathologic analysis.
Results: In the first case, the drainage of cystic fluidand a regular concavity were found during tooth re-moval. In the second case, a nodular lesion was foundadhering to the disto-buccal surface of the tootharising from the distal wall of a periodontal pocket.The histopathologic analysis revealed a hyperplasticstratified squamous epithelium with arcading lininga fibrous capsule with inflammatory infiltrate, result-ing in a final diagnosis of a paradental cyst.
Conclusions: The presence of a paradental cystshould be considered when recurrent inflammatoryperiodontal processes are associated with partiallyerupted vital teeth, even when characteristic radio-graphic findings are absent. Definitive diagnosisrequires a clinicopathologic correlation incorporat-ing surgical, radiographic, and histologic findings.J Periodontol 2006;77:1602-1606.
KEY WORDS
Jaw cysts; odontogenic cysts; periodontal diseases.
The reduced enamel epithelium and epithelialrests of Malassez are believed to have the po-tential for proliferation in response to inflam-
matory stimuli and, thus, give rise to several differentodontogenic cysts, such as the paradental cyst.According to the World Health Organization (WHO)Histological Typing of Odontogenic Tumors, the par-adental cyst is defined as ‘‘a cyst occurring near to thecervical margin of the lateral aspect of a root as aconsequence of an inflammatory process in a peri-odontal pocket. A distinctive form of the paradentalcyst occurs on the buccal and distal aspects oferupted mandibular molars, most commonly the thirdmolars, where there is an associated history ofpericoronitis.’’1
The major clinical feature of the paradental cyst isthe presence of a recurring inflammatory periodontalprocess, usually a pericoronitis. Apart from acute ep-isodes, this cyst presents only a few signs and mildsymptoms, including discomfort, tenderness, moder-ate pain, and, in some cases, suppuration through theperiodontal sulcus.2-4 Some cases are asymptomaticand diagnosed incidentally from a radiograph,5
whereas others remain undetected by clinical exami-nation and radiographs.6 The paradental cyst occursmost commonly on the buccal and disto-buccal as-pects of partially or fully erupted vital teeth7-9 andrarely on the mesial aspect.3,10 Most reported caseshave described the paradental cyst in association withthe third mandibular molars,2,3,6,8-13 although it mayoccur less frequently with the second9,14 and firstmolars13,15-18 and rarely with premolars7 or incisors/canines.19
There can be a variety of radiographic presenta-tions, depending on factors such as the superimposi-tion of anatomical structures, presence of infection,and lesion size and location.2 The lesion frequentlyproduces a well-defined radiolucency mimicking per-iapical pathology involving one or both roots of the in-volved tooth6,11 or semilunar-shaped bony resorptionon the distal aspect.10 Characteristically, the peri-odontal ligament space and the lamina dura are intact
* Post-Graduation Program, Dental School of Aracxatuba, Sao Paulo StateUniversity, Sao Paulo, Brazil.
† Faculty of Odontology, Dental School of Aracxatuba, Sao Paulo StateUniversity.
‡ Department of Surgery and Integrated Clinic, Dental School of Aracxatuba,Sao Paulo State University.
§ Department ofOral Pathology, Dental School of Aracxatuba, SaoPaulo StateUniversity. doi: 10.1902/jop.2006.050380
Volume 77 • Number 9
1602

and continuous around the root because the inflam-matory component is not of endodontic origin.
The paradental cyst cannot be differentiated histo-pathologically from other odontogenic cysts of in-flammatory origin.6,7,20 The connective tissuecapsule, with heavy inflammatory infiltrate, is outlinedby a hyperplastic non-keratinized stratified squamousepithelium.2,3,6,7,10-12,21 Foci of hemosiderin pig-ment and cholesterol clefts consistent with inflamma-tory cysts4 can also be found.6,7,10,12
The prevalence of the paradental cyst reported inseveral studies varies from 1% to 5% of all odontogeniccysts,6,10,22 which justifies its inclusion in the group ofrare lesions.7 However, it is possible that the paraden-tal cyst is much more common than previously re-ported,2,10 considering the high incidence of recurringinflammatory periodontal processes.
The purpose of the present article is to report clin-ical, radiographic, and histologic findings in two casesof paradental cysts associated with mandibular thirdmolars. Case 1 was enrolled on March 24, 2004,and case 2 was enrolled on February 18, 2004. In-formed consent was obtained from both patients,and the study was conducted in accordance withthe Helsinki Declaration of 1975, as revised in 2000.
CASE REPORTS
Case 1A 23-year-old man described a recurring spontane-ous pain localized to a vital, right mandibular third mo-lar. Clinically there was mild edema in the overlayingmucosa of the partially erupted tooth in a vertical po-sition. Radiographs disclosed a well-defined semilunar-shaped bony resorption on the distal aspect of thecrown, ending at the level of the cemento-enameljunction (Fig. 1). The tooth and lesional tissue weresurgically removed, exposing a distal bony resorptionas a regular concavity. An enlarged follicular sac, lat-eral dentigerous cyst, and paradental cyst were con-sidered in the differential diagnosis. Microscopicexamination showed a fibrous connective tissue cap-sule invaded by a lymphocytic inflammatory infiltrate,lined by a hyperplastic, non-keratinized, stratifiedsquamous epithelium (Fig. 2), resulting in a final diag-nosis of a paradental cyst.
Case 2A 21-year-old man reported chronic discomfortcaused by occlusal trauma on pericoronal tissues ofthe left mandibular molar, which was partially eruptedin a vertical position. A radiolucency was seen on thedistal aspect of the crown that was interpreted as per-icoronal space enlargement (Fig. 3). Tooth extractionwas indicated because of a lack of space. A nodularlesion of fibrous consistency, 7 mm in diameter, wasencountered adherent to the distal surface of the
Figure 1.Periapical radiograph showing a semilunar-shaped bony resorption onthe distal aspect of the partially erupted third molar.
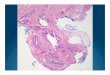
Figure 2.Cystic wall showing the epithelium, with intense chronic inflammationand vascularization in the connective tissue (hematoxylin and eosin[H&E]; original magnification ·200; bar = 50 mm).
Figure 3.Periapical radiograph showing a radiolucency on the distal aspect ofthe crown.
J Periodontol • September 2006 Kanno, Gulinelli, Nagata, Soubhia, Crivelini
1603

tooth, arising from the distal wall of the periodontalpocket (Figs. 4 and 5). Histologically, the cyst cap-sule was lined by a proliferating, non-keratinized,stratified squamous epithelium, showing as arcading.The cystic wall consisted of dense, mature fibrous con-nective tissue, with an intense chronic inflammatory
reaction mainly near the epithelium (Fig. 6), support-ing a definitive diagnosis of a paradental cyst.
DISCUSSION
The paradental cyst is considered a rare lesion. How-ever, it has been speculated that this lesion has beenunderdiagnosed. Lindh and Larsson23 believe that theparadental cyst has been misdiagnosed as a dentiger-ous cyst, lateral radicular cyst, or merely as pericoro-nitis or some other entity related to inflammatoryconditions of the dental follicle. Another fact thatcould result in the underdiagnosis of paradental cystsis that histopathologic analysis of extirpated follicularsacs is rarely done. On the other hand, the relativelyrecent characterization of this cyst can be a contribut-ing factor to its non-recognition. It was included in theWHO Histological Typing of Odontogenic Tumors forthe first time in 1992, although it had been describedin several clinicopathologic studies in specializedjournals since 1970.6,10,11,19 Considering these facts,it seems reasonable that new cases be reported andthe variety of clinical presentations be discussed to in-crease the awareness of this lesion.
Most cases described in the literature to date haveoccurred in mandibular third molars, less frequently insecond9,14 and first molars,13,15-18 and rarely in pre-molars7 or incisors/canines.19 It is interesting that thereported paradental cysts that were located on the dis-tal surface occurred in partially erupted third molars invertical or slightly disto-angular positions, like thepresent cases. In those cases in which the lesionwas located on the mesial aspect, the tooth was in amesio-angular position. It seems that the tooth posi-tion and its relationship with the overlaying mucosadetermine the surface on which the paradental cystwill occur. Colgan et al.24 believe that food impaction
Figure 4.Occlusal view of the lesion adhered to the distal aspect of theextracted tooth. A periodontal pocket can be seen.
Figure 5.Lingual view of the lesion adhered to the distal aspect of theextracted tooth. The relationship between the lesion and theperiodontal pocket can be seen.
Figure 6.Cystic capsule with intense inflammatory reaction and numerousblood vessels lined by stratified squamous epithelium (H&E; originalmagnification ·100; bar = 200 mm).
Paradental Cyst: Report of Two Cases Volume 77 • Number 9
1604

plays an essential role in the pathogenesis of the par-adental cyst by causing an inflammatory reaction.However, the buccal location of the lesion seems tobe related to the presence of an enamel projectionin a great number of cases.6,11
The radiographic aspects of paradental cysts maybe a diagnostic pitfall, as occurred in the second casepresented in which the lesion was not suspected be-fore surgery. The distal radiolucency was interpretedas enlargement of the pericoronal space. It can occurwhen the superimposition of other anatomical struc-tures precludes the visualization of the lesion. An in-triguing question that could be raised is what wouldhave happened if the patient had not accepted toothextraction and the lesion had remained undiagnosed?There is some evidence in the literature indicating thatthe growth of the paradental cyst is self-limiting21 be-cause great dimensions have not been found. There isalso the possibility of spontaneous drainage, leadingto the regression of the lesion.18,21
It has been stated that the radiographic image ofthe paradental cyst is always characterized by a well-defined radiolucency associated with the roots on thebuccal aspect.6,11 Cases in which the lesion is relatedto the distal surface of the crown could represent lat-eral dentigerous cysts.11 In both cases described inthe present article, the radiographs disclosed a distalradiolucency adjacent to the crown, delimited by thecemento-enamel junction. In the first case, the lesionwas fragmented during the tooth extraction becausethe inflammatory process led to tissue damage. Nev-ertheless, the drainage of cystic fluid during tooth ex-traction and bony cavitation distally in the alveolussupport the diagnosis of a cystic lesion.25 The final di-agnosis was strongly suggested based on the histopa-thologic findings, in which the diagnosis of adentigerous cyst was ruled out. Arcading of the hyper-plastic squamous epithelium was seen over an in-flamed connective tissue, among other histologicfeatures. Conversely, the epithelial lining of the den-tigerous cyst consists of two to four layers of cuboidalepithelial cells, with a flat epithelial-connective tissueinterface.26 In case 2, the lesion clearly arose from thewall of the periodontal pocket. In fact, the most ac-cepted theory for the origin of the paradental cyst isfrom the reduced enamel epithelium.6,11 These fea-tures, in conjunction with the location of the bony cav-itation, the partial eruption of the tooth, and thechronic gingival inflammatory process, strongly sug-gested a paradental cyst, which was confirmed by thehistologic analysis. In contrast, the lining of the den-tigerous cyst is comprised of the reduced enamel ep-ithelium, which is always found adhering to thecemento-enamel junction and presents different his-tologic features compared to the sulcular epithelium.Moreover, the bony cavitation of a lateral dentigerous
cyst would be expected to be found around the wholecrown of an unerupted tooth.
In the present cases, an inflamed pericoronal folli-cle was also included in the differential diagnosis.However, the odontogenic keratocyst, dentigerouscyst, lateral radicular cyst, ameloblastoma, gingivalcyst, and some odontogenic tumors should also beconsidered depending on radiographic and clinicalfindings.2,3,20,21 In the first case, pericoronitis wasruled out because bony cavitation, fluid drainage,and a semilunar-shaped radiolucency are character-istics of a cystic lesion. In the second case, the clinicalfeatures of the lesion suggested a paradental cyst.Moreover, the epithelial arcading seen at the micro-scopic level strongly supported the final diagnosis ofa paradental cyst.
The histopathologic features of the paradental cystare identical to the radicular cyst, which makes thepulp vitality test a key factor in the differential diagno-sis. If the paradental cyst can present variable clinicaland radiographic signs,6 in addition to being con-founded with the radicular cyst at the microscopiclevel, it is mandatory to correlate all clinical, radio-graphic, and histologic data to obtain a definitive diag-nosis. Surgical findings, such as bony cavitation,cystic content, and location of lesion adherence, cangive some important clues.
Surgical removal of the tooth and the paradentalcyst has been considered the treatment of choicewhen the involved tooth is a third molar.2,3,12 Enucle-ation of the lesion with the maintenance of the associ-ated tooth can be indicated when the first or secondmolars are involved.2,3,14-16 In all cases, recurrenceis rare, provided that the lesion has been completelyremoved.7,11,12,21,27
The presence of a paradental cyst should be con-sidered when recurrent inflammatory periodontal pro-cesses are associated with partially erupted vitalteeth, especially mandibular molars, even when char-acteristic radiographic findings are absent. A clinico-pathologic correlation, incorporating the surgical,radiographic, and histologic findings, is required toobtain a final diagnosis of paradental cyst. Histopath-ologic examination of every follicular sac could in-crease the frequency of this lesion’s diagnosis.
REFERENCES1. Kramer IRH, Pindborg JJ, Shear M. Histological Typ-
ing of Odontogenic Tumors, 2nd ed. Berlin: Springer-Verlag; 1992:42.
2. Bsoul SA, Flint DJ, Terezhalmy GT, Moore WS.Paradental cyst (inflammatory collateral, mandibularinfected buccal cyst). Quintessence Int 2002;33:782-783.
3. Philipsen HP, Reichart PA, Ogawa I, Suei Y, Takata T.The inflammatory paradental cyst: A critical review of342 cases from a literature survey, including 17 new
J Periodontol • September 2006 Kanno, Gulinelli, Nagata, Soubhia, Crivelini
1605

cases from the author’s files. J Oral Pathol Med 2004;33:147-155.
4. Stoneman DW, Worth HM. The mandibular infectedbuccal cyst: Molar area. Dent Radiogr Photogr 1983;56:1-14.
5. Vedtofte P, Holmstrup P. Inflammatory paradentalcysts in the globulomaxillary region. J Oral PatholMed 1989;18:125-127.
6. Craig GT. The paradental cyst: A specific inflamma-tory odontogenic cyst. Br Dent J 1976;141:9-14.
7. Morimoto Y, Tanaka T, Nishida I, et al. Inflammatoryparadental cyst (IPC) in the mandibular premolarregion in children. Oral Surg Oral Med Oral PatholOral Radiol Endod 2004;97:286-293.
8. Souza SOM, Correa L, Deboni MC, Araujo VC. Clini-copathologic features of 54 cases of paradental cyst.Quintessence Int 2001;32:737-741.
9. Lim AA-T, Peck RH-L. Bilateral mandibular cyst:Lateral radicular cyst, paradental cyst, or mandibularinfected buccal cyst? Report of a case. J Oral Max-illofac Surg 2002;60:825-827.
10. Ackermann G, Cohen M, Altini M. The paradental cyst:A clinicopathologic study of 50 cases. Oral Surg OralMed Oral Pathol 1987;64:308-312.
11. Fowler CB, Brannon RB. The paradental cyst: A clini-copathologic study of six new cases and review of theliterature. J Oral Maxillofac Surg 1989;47:243-248.
12. Vedtofte P, Praetorius F. The inflammatory paradentalcyst. Oral Surg Oral Med Oral Pathol 1989;68:182-188.
13. el-Magboul K, Duggal MS, Pedlar J. Mandibularinfected buccal cyst or a paradental cyst? Report ofcase. Br Dent J 1993;175:330-332.
14. Martinez-Conde R, Aguirre JM, Pindborg JJ. Paraden-tal cyst of the second molar: Report of a bilateral case.J Oral Maxillofac Surg 1995;53:1212-1214.
15. Camarda AJ, Pham J, Forest D. Mandibular infectedbuccal cyst: Report of two cases. J Oral MaxillofacSurg 1989;47:528-534.
16. Packota GV, Hall JM, Lanigan DT, Cohen MA. Para-dental cysts on mandibular first molars in children:Report of five cases. Dentomaxillofac Radiol 1990;19:126-132.
17. Bohay RN, Weinberg S, Thorner PS. The paradental cystof the mandibular permanent first molar: Report of abilateral case. ASDC J Dent Child 1992;59:361-365.
18. Gomez RS, Oliveira JR, Castro WH. Spontaneousregression of a paradental cyst. Dentomaxillofac Ra-diol 2001;30:296.
19. Main DM. Epithelial jaw cysts: A clinicopathologicalreappraisal. Br J Oral Surg 1970;8:114-125.
20. Silva TA, Batista AC, Camarini ET, Lara VS, Con-solaro A. Paradental cyst mimicking a radicular cyston the adjacent tooth: Case report and review ofterminology. J Endod 2003;29:73-76.
21. David LA, Sandor GKB, Stoneman DW. The buccalbifurcation cyst: Is non-surgical treatment an option?J Can Dent Assoc 1998;64:712-716.
22. Kreidler J, Raubenheimer EJ, van Heerden WFP. Aretrospective analysis of 367 cystic lesions of the jaw:The Ulm experience. J Craniomaxillofac Surg 1993;21:339-341.
23. Lindh C, Larsson A. Unusual jaw-bone cysts. J OralMaxillofac Surg 1990;48:258-263.
24. Colgan CM, Henry J, Napier SS, Cowan CG. Paraden-tal cysts: A role for food impaction in the pathogen-esis? Br J Oral Maxillofac Surg 2002;40:162-168.
25. Damante JH, Fleury RN. A contribution to the diag-nosis of the small dentigerous cyst or the paradentalcyst. Pesqui Odontol Bras 2001;15:238-246.
26. Waldron CA. Odontogenic cysts and tumours. In:Neville BW, Damm DD, Allen CM, Bouquot JE, eds.Oral and Maxillofacial Pathology. Philadelphia: W.B.Saunders; 1995:493-540.
27. Pompura JR, Sandor GKB, Stoneman DW. The buccalbifurcation cyst: A prospective study of treatmentoutcomes in 44 sites. Oral Surg Oral Med Oral PatholOral Radiol Endod 1997;83:215-221.
Correspondence: Dr. Claudia M. Kanno, Dental Schoolof Aracxatuba, Sao Paulo State University, Rua JoseBonifacio, 1193, CEP 16015-050, Aracxatuba, Sao Paulo,Brazil. E-mail: [email protected].
Accepted for publication March 30, 2006.
Paradental Cyst: Report of Two Cases Volume 77 • Number 9
1606