Embed Size (px)
Citation preview

Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. PA
RA
DO
XIC
AL EM
BO
LISM
1571
Paradoxical Embolism: Role of Imaging in Diagnosis and Treat-ment Planning1
Paradoxical embolism (PDE) is an uncommon cause of acute arterial occlusion that may have catastrophic sequelae. The pos-sibility of its presence should be considered in all patients with an arterial embolus in the absence of a cardiac or proximal arterial source. Despite advancements in radiologic imaging technology, the use of various complementary modalities is usually necessary to exclude other possibilities from the differential diagnosis and achieve an accurate imaging-based diagnosis of PDE. In current practice, the imaging workup of a patient with symptoms of PDE usually starts with computed tomography (CT) and magnetic resonance (MR) imaging to identify the cause of the symptoms and any thromboembolic complications in target organs (eg, stroke, peripheral arterial occlusion, or visceral organ ischemia). Additional imaging studies with modalities such as peripheral venous Doppler ultrasonography (US), transcranial Doppler US, echocardiography, and CT or MR imaging are required to detect peripheral and central sources of embolism, identify cardiac and/or extracardiac shunts, and determine whether arterial disease is present. To guide radiologists in selecting the optimal modalities for use in various diagnostic settings, the article provides detailed information about the imaging of PDE, with numerous radiologic and pathologic images illustrating the wide variety of features that may accompany and contribute to the pathologic process. The roles of CT and MR imaging in the diagnosis and exclusion of PDE are described, and the use of imaging for planning surgical treatment and interventional procedures is discussed.
©RSNA, 2014 • radiographics.rsna.org
Farhood Saremi, MD Neelmini Emmanuel, MD Philip F. Wu, BS Lauren Ihde, MD David Shavelle, MD John L. Go, MD Damián Sánchez-Quintana, MD, PhD
Abbreviations: DVT = deep venous thrombo-sis, IVC = inferior vena cava, PDE = paradoxical embolism, PFO = patent foramen ovale
RadioGraphics 2014; 34:1571–1592
Published online 10.1148/rg.346135008
Content Codes: 1From the Departments of Radiology (F.S., N.E., P.F.W., L.I., J.L.G.) and Cardiovascular Medicine (D.S.), University of Southern Califor-nia, USC University Hospital, 1500 San Pablo St, Los Angeles, CA 90033; and Department of Human Anatomy, University of Extremadura, Badajoz, Spain (D.S.Q.). Recipient of a Cer-tificate of Merit award for an education exhibit at the 2012 RSNA Annual Meeting. Received January 3, 2013; revision requested April 4 and received July 13; accepted July 19. For this journal-based SA-CME activity, the authors, editor, and reviewers have disclosed no relevant relationships. Address correspondence to F.S. (e-mail: [email protected]).
After completing this journal-based SA-CME activity, participants will be able to: ■ Describe the causes of PDE and se-
quelae in target organs.
■ Discuss the specific uses of various im-aging modalities in the diagnosis of PDE.
■ Recognize CT and MR imaging fea-tures that are pertinent for the diagnosis of PDE and for posttreatment evaluation.
See www.rsna.org/education/search/RG.
SA-CME LEARNING OBJECTIVES
IntroductionParadoxical embolism (PDE) is usually definitively diagnosed at autopsy or at radiologic imaging when a thrombus that crosses an intracardiac defect is seen in the setting of arterial embolic damage in end organs (eg, stroke). Imaging evaluation of patients in whom the presence of PDE is suspected usually necessitates the use of more than one modality. Peripheral Doppler ultrasonography (US) and echocardiography are well-established methods for assessing thromboembolic processes. Although echocardiography is the prime modality for depicting a shunt across a patent foramen ovale (PFO), no single modality can cover the whole spectrum of findings in the imaging workup of PDE.

1572 October Special Issue 2014 radiographics.rsna.org
target organs. Additional imaging studies, includ-ing peripheral venous Doppler US, transcranial Doppler US, echocardiography, and CT, are used to detect peripheral and central sources of embo-lism, arterial disease, and cardiac or extracardiac shunts. Further diagnostic testing often includes continuous long-term electrocardiographic re-cordings, blood chemistry panels, and coagula-tion tests.
Types of EmbolismThrombi from tributaries of the IVC are the major sources of embolism, but emboli of fat, air, amniotic fluid, and tumor tissue have also been described (10–15). Fat embolism syndrome is primarily a pulmonary disease (10). Shunt-ing of fat or other material across a PFO can be precipitated by increased right atrial pressure for a variety of reasons, including changes in body position, breathing patterns, and intrathoracic pressure. Paradoxical air embolism can lead to cerebral lesions in scuba divers (11). Cerebral air embolism can occur through central venous catheters (12). Patients undergoing neurosurgery in a sitting position have a risk for paradoxical air embolism (13). In these cases, preoperative detection of PFO and additional monitoring and special care during surgery are advised. Amni-otic fluid embolism can rarely be complicated by PDE resulting from increased pressure in the right side of the heart due to the release of vaso-active substances when amniotic fluid enters the pulmonary circulation (14).
Imaging findings of PDE complications in the brain are probably similar for different types of embolism, and the clinical history is important for final diagnosis. Air emboli absorb quickly and are best depicted in an early stage at CT.
Peripheral Sources of Venous Thromboembolism
Venous thrombosis in the legs may be the most common source of embolus. Approximately 90% of symptomatic pulmonary emboli arise from thrombi located in the leg veins (8,16). In most
The article outlines the optimal imaging ap-proach in various clinical settings and the value contributed by each imaging modality for accu-rate diagnosis of PDE. The current roles of com-puted tomography (CT) and magnetic resonance (MR) imaging in identifying cardiac and extra-cardiac abnormalities known to contribute to the development of PDE and detecting sequelae in target organs are emphasized, and the utility of supplemental US studies is reviewed. Strategies for treating PDE, including interventional tech-niques, also are described.
Historical Background and Definitions
In 1877, Cohnheim (1) reported the first case of PDE by describing the path of an embolus through a septal defect in the heart. In 1881, Zahn (2) reported an autopsy study in which thrombosis of the uterine vein, multiple systemic emboli, and a branched thrombus within a PFO were seen in the same cadaver. Later, in 1885, he used the term paradoxical embolism to describe a condition in which emboli derived from the ve-nous system reached the systemic arterial system through an abnormal communication between the heart chambers (3).
Four essential elements contribute to the devel-opment of PDE: systemic embolism, an embolic source, a right-to-left shunt, and a pressure gradi-ent across the shunt (Table 1) (3–6). The diagnosis of PDE is considered definitive when it is based on a finding at autopsy or at imaging of a thrombus that crosses an intracardiac defect in the setting of an arterial embolus (4). A diagnosis of PDE in the absence of these findings is considered presump-tive (4,6). The triad of systemic embolism, venous thrombosis, and intracardiac communication defines the clinical diagnosis of PDE and allows treatment with a high level of confidence (7,8). The diagnosis of PDE is termed “possible” if an arterial embolus and PFO are detected; many phy-sicians treat patients on the basis of a diagnosis of “possible PDE” (9).
Most early case reports of paradoxical embolus were based on autopsy findings (4). Later, an in-tracardiac right-to-left shunt was demonstrated in a living patient when dye injected into the inferior vena cava (IVC) appeared earlier than expected at the left brachial artery (6). Limited catheter-ization of the right side of the heart was proposed as a method for excluding an intracardiac shunt in patients with coexistent venous thrombosis or pulmonary embolism and arterial embolism.
In current practice, the imaging workup of a patient for PDE usually starts with CT and MR imaging. These modalities are used to diagnose thromboembolic sequelae of arterial embolism in
Table 1: Essential Elements of PDE
Systemic embolism confirmed by clinical, an-giographic, or pathologic findings without an apparent source on the left side of the heart or in the proximal arterial tree (ascending aorta)
Embolic source within the venous systemAbnormal intracardiac or intrapulmonary commu-
nication between the right and left circulationsPressure gradient that promotes a right-to-left shunt
at some point during the cardiac cycle

RG • Volume 34 Number 6 Saremi et al 1573
venography for evaluation after a stroke, DVT was found within 3.25 days after the occurrence of a stroke in 27% of those with cryptogenic brain ischemia and an interatrial communica-tion, half of the thrombi being isolated within a calf or pelvic vein (25). In a related multicenter study, pelvic DVT was found at MR venography performed within 3 days after the occurrence of a cryptogenic stroke in 20% of 46 patients with a PFO or atrial septal defect (26). With the use of MR venography, Kiernan et al (27) found pelvic venous thrombosis (May-Thurner syndrome) in 6.3% of patients who underwent PFO closure after a cryptogenic stroke. Eighty percent of the patients were female, and 54% of the female patients were receiving oral con-traceptive therapy. Overall, the results of the preceding studies show that (a) PDE from the lower extremity and possibly the pelvis is one mechanism that accounts for ischemia related to systemic embolization in a subset of patients and (b) pelvic CT or MR imaging may be useful for determining whether pelvic DVT is present in patients in whom findings are negative for DVT of the lower extremities.
Upper-extremity sources of PDE include spontaneous DVT (Paget-Schroetter syndrome) and catheter-related DVT. The occurrence of PDE as a complication of Paget-Schroetter syndrome is rare, but at least one case has been reported (28). Catheter-related thrombosis ac-counts for approximately 80% of cases of upper-extremity DVT (29). Thrombogenesis associated with catheters has been well documented, with an incidence ranging from 2% to 67%, depend-ing on the catheter type and location, diagnostic criteria, and population studied (29,30). The published literature about catheter-associated paradoxical thromboembolus is limited to case reports of coronary arterial, limb, or brain in-volvement (31,32).
Sequelae of PDE in Target Organs
Although PDE is an uncommon cause of acute arterial occlusion, it can have catastrophic se-quelae, and the possibility that it is present should be considered in all patients with an arte-rial embolus in the absence of a cardiac or proxi-mal arterial source. PDE is frequently associated with cryptogenic stroke and peripheral embolism (33) (Fig 1). Uncommon complications include brain abscess (34), decompression sickness in underwater divers (11), myocardial infarction (35), and mesenteric infarction (7). Hypoxemia due to a transient right-to-left shunt is also pos-sible. In Loscalzo’s (7) study based on findings in 30 patients, the five sites of arterial emboli
studies, the prevalence of deep venous thrombo-sis (DVT) in patients with acute pulmonary em-bolism appears to be higher than that in patients with a cryptogenic stroke and PFO (16,17). In many cases of PDE, the source of the embolus in peripheral veins cannot be found (8). The report-edly low rate of DVT in patients with a PFO and cryptogenic stroke may be an effect of the delay between the initiation of anticoagulation therapy and the imaging evaluation, complete thrombus migration, inability to detect residual thrombus, or undetected thrombosis in a calf or pelvic vein (10%) (8,18). Another possibility is that the embolic source remains undetected in the upper-extremity veins (19).
Duplex US is the most common method for evaluating DVT. Most US studies of the lower extremity are limited to veins at or above the level of the popliteal veins, which may lead to underes-timation of the true incidence of venous throm-bosis (20).
US is more accurate than venography for de-picting peripheral DVT but is much less accurate for showing central (ie, pelvic) DVT (20,21). A small proportion (2%–7%) of thrombi that can be diagnosed at venography or CT venography are limited to the pelvic veins or vena cava and may therefore remain undetected at US (22). Contrast material–enhanced MR venography seems to be more accurate than color Doppler US in depicting a central (toward the pelvis) extension of DVT (23). Nonenhanced balanced steady-state free precession MR venography is more accurate than US for the diagnosis of lower-extremity DVT and is capable of depicting greater central extension of the thrombus (24). Nonenhanced MR venography can be performed when intravenous administration of gadolinium-based contrast material is contraindicated.
The reported incidence of DVT associated with PFO and PDE ranges widely between dif-ferent patient series (8,17,25), depending on the imaging modality used, anatomic location of the venous thrombus, time interval between the onset of symptoms and imaging, and dura-tion of anticoagulation therapy before imaging. For example, Stöllberger et al (8) reported that DVT was found at lower-extremity venography performed within 90 days after symptom onset in 57% of patients with a PFO and arterial em-boli without evident arterial or cardiac sources. By contrast, in a study by Lethen et al (17), venography depicted DVT in only 10% of pa-tients with a PFO as the sole identifiable cardiac risk factor for PDE; most of those patients had undergone heparin therapy before venography. In a recent study of 37 patients who underwent duplex US of the lower extremity and pelvic MR

1574 October Special Issue 2014 radiographics.rsna.org
were peripheral (49%), cerebral (37%), coronary (9%), renal (1%), and splenic (1%). Among cases of PDE reported by Travis et al (9), the most frequent clinical manifestations were (in order of decreasing frequency) lower-extremity ischemia, upper-extremity ischemia, respiratory distress, cerebral infarction or amaurosis fugax, and ab-dominal and/or flank pain.
Cryptogenic StrokeIschemic strokes can be classified into two ma-jor categories: (a) those due to a known cause such as large-artery atherosclerosis, intracardiac thrombus, or small-artery occlusion and (b) those due to an undetermined cause or cryptogenic infarction (36,37). One-third of ischemic strokes
are cryptogenic in origin (38). The cause of cryp-togenic stroke remains undetermined in most cases because the event is transitory or reversible, investigators cannot look for all possible causes, and some causes remain unknown. The detection of a PFO in a patient with a confirmed stroke does not necessarily mean that the cause of the stroke has been identified. Establishing a causal relation-ship between the presence of a PFO and the oc-currence of a stroke remains the crucial point in the diagnosis of PDE. The four criteria described earlier for the diagnosis of PDE may not always be met. The presence of other contributing fac-tors, such as the morphologic characteristics of the PFO and associated structures, may increase the probability that PDE is present (37,38).
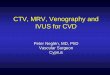
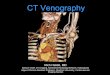
Figure 1. Axial diffusion-weighted MR images demonstrate paradoxical embolic infarcts. (a) Multiple bilateral nonterritorial subcortical infarcts (light gray foci) are seen in a patient with tetralogy of Fallot and an anomalous connection of a left-sided su-perior vena cava with the left atrium. (b) A single territorial infarct (arrow) that origi-nated from right subclavian venous throm-bus is depicted in a patient with a PFO. (c) A large lobar infarct (light gray–whitish area) is evident in the right temporoparietal region in a patient with an atrial septal defect.

RG • Volume 34 Number 6 Saremi et al 1575
Embolic and Nonembolic InfarctsPFO is thought to be an important causal mecha-nism of embolic stroke in young patients (38,39). Some investigators believe that various imaging patterns can support a diagnosis of PDE (40). Theoretically, paradoxical emboli are expected to cause brain infarcts with an imaging appearance resembling that of brain infarcts due to other (cardiac or arterial) embolic causes. At brain imaging, the occlusion of a superficial arterial branch or the presence of a large infarct involv-ing more than one lobe is strongly suggestive of embolic infarction (40). Scattered lesions or cor-tical-subcortical territorial lesions also are indica-tive of embolic infarction (Fig 1). Multiple acute infarcts, especially those that are bilateral and affect various networks of cerebral circulation, are strong indicators of a proximal embolic source or a systemic cause, and diffusion-weighted imaging is an excellent MR imaging technique for depict-ing multiple small infarcts (40,41).
Patients with a large PFO are more likely to demonstrate embolic infarcts after a cryptogenic stroke than are patients with a small or no PFO (42). Patients with a medium or large PFO more frequently have occipital and infratentorial (pos-terior circulation) strokes than do patients with a small PFO (57% versus 27%) (42,43) or patients with a history of atrial fibrillation; they also tend to have multiple infarcts (44). Cryptogenic stroke with an “embolic” pattern is more common when PFO and atrial septal aneurysm coexist (45). Although the presence of hemorrhagic transfor-mation is a strong indicator of embolic infarction, published data do not demonstrate an association between PFO and hemorrhagic infarcts (42).
Anatomic and Physiologic Con-siderations in Patients with a PFO
Potential routes of PDE are classified in Table 2. Both intracardiac and extracardiac shunts can lead
to PDE. However, intracardiac causes are more common; of these, most arise from the presence of a PFO. In Loscalzo’s (7) series of cases with a clinical diagnosis of PDE, 72% had a PFO, and the remaining potential routes included atrial sep-tal defect, pulmonary arteriovenous malformation, and ventricular septal defect. Some shunts, such as those produced by muscular and membranous ventricular septal defects, may be small and found incidentally at clinical and imaging examinations (Fig 2).
A PFO has been known to be a common find-ing since 1930, when Thompson and Evans (4) identified a “probe patent” foramen (0.2–0.5 cm in diameter) in 29% of unselected autopsy cases and a “pencil patent” defect (0.6–1.0 cm in di-ameter) within the atrial septum in 6%.
Hagen et al (46) found a PFO in 27% of 965 autopsied hearts. The prevalence of PFO and the size of the defect did not differ significantly ac-cording to sex but varied significantly with age: 34% of PFOs were found in those who had died in the first 3 decades of life; 25% of PFOs, in those who had died in the 4th to 8th decades of life; and 20% of PFOs, in those who had died in the 9th or 10th decade of life. The size of the PFOs seen in the cadavers ranged from 1 to 19 mm (mean, 4.9 mm), increasing progressively from a mean of 3.4 mm in those who had died in the 1st decade of life to 5.8 mm in those who had died in the 10th decade of life, perhaps because smaller PFOs close spontaneously with age.
PFO has been implicated in the pathogenesis of many diseases (11,37). The precise frequency with which PDE complicates PFO is unknown; PDE occurs in a minority of patients with ve-nous thromboembolic disease who also have a PFO. This is thought to be because the foramen ovale is normally closed by the higher left-to-right atrial pressure gradient. Case control stud-ies that demonstrate a higher prevalence of PFO
Table 2: Potential Routes of PDE (Right-to-Left Shunt)
Intracardiac PFO Iatrogenic connection (baffle defect, Fontan conduit, Rashkind device) Enlarged thebesian veins (ie, interatrial muscle bundle)
Congenital anomaly (atrial septal defect, unroofed coronary sinus, ventricu- lar septal defect, atrioventricular septal defect)
Extracardiac Pulmonary arteriovenous malformation (congenital, secondary to cavopul-
monary shunts) Systemic to pulmonary venous communication (congenital, acquired) Arterioarterial communication (patent ductus arteriosus) or venovenous
communication

1576 October Special Issue 2014 radiographics.rsna.org
among patients with cryptogenic strokes led to the acceptance of PFO as a potential risk factor for stroke (38,39). However, whether a PFO has a direct causal role in the occurrence of stroke or whether the relationship is merely an associa-tion remains controversial. In support of a causal relationship, case reports have described direct visualization of thrombus in migration through a PFO tunnel (47) (Fig 3). The proportion of cryptogenic strokes due to PDE is believed to be around 20% (48). Obviously this proportion may vary, depending on patient age and the presence of predisposing factors (Table 3).
Hemodynamic Parameters That In- fluence PFO-related Right-to-Left ShuntThe etiology of a right-to-left shunt through a PFO despite normal intracardiac pressures and normal or near-normal pulmonary function has not yet been completely elucidated. The results of population-based studies suggest that the annual risk of cryptogenic stroke in otherwise healthy
people with a PFO may be as low as 0.1% (49). This observation suggests that other factors con-tribute to the increased risk of stroke in people with a PFO. Diagnostic studies performed with contrast agent–enhanced echocardiography while the patient performed the Valsalva maneuver dem-onstrated pressure-dependent shunts in 50%–60% of all patients with a detectable PFO (50). Con-current risk factors for venous thromboembolism, such as trauma, recent surgery, use of oral contra-ceptives, and various hypercoagulable states, also influence the clinical relevance of a PFO.
A transient spontaneous physiologic reversal of the pressure gradient between the left and right atria is present during early diastole and during isovolumetric contraction of the right ventricle during each cardiac cycle (51,52). This so-called reversal gradient may increase when the patient performs physiologic maneuvers leading to increased right atrial pressure, such as postural changes, inspiration, vigorous cough-ing, or the Valsalva maneuver. The reversal gra-
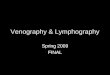
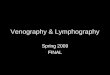
Figure 2. Still MR images from a cine sequence depict interventricular membra-nous septal aneurysm and defect. LV = left ventricle. (a) Coronal view shows an aneu-rysm of the interventricular membranous septum (arrow). (b, c) Three-chamber views obtained during systole (b) and dias-tole (c) show the same aneurysm (arrow in b), along with a linear region void of signal in diastole (arrow in c). The latter finding is suggestive of a small ventricular septal defect, a potential cause of PDE. The ven-tricular portion of the membranous septum may become aneurysmal, usually bulging toward the right. The protruding aneurysm may limit intracardiac shunting, with resul-tant spontaneous closure of the ventricular septal defect.

RG • Volume 34 Number 6 Saremi et al 1577
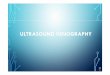
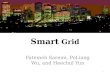
Figure 3. Thrombus in migration through a PFO tunnel (black arrows) in a 43-year-old woman. (a) CT angiography of the chest demonstrates multiple pulmonary emboli (arrowheads). (b) The presence of a thrombus (arrow) was confirmed at transthoracic four-chamber echocardiography, which provided better depiction. LA = left atrium, RA = right atrium.
dient also may be increased in the presence of a pathologic condition that results in high pulmo-nary vascular resistance (eg, acute pulmonary embolism, hypoxemia due to obstructive sleep apnea, severe chronic obstructive pulmonary disease, right ventricular infarction, and positive end-expiratory pressure during neurosurgical procedures performed with the patient in a sit-ting position) (13,51,52).
Another mechanism that helps explain a transient right-to-left shunt is preferential di-rectionality of blood flow from the IVC toward the interatrial septum (53). The IVC flow enters
from the posterior of the right atrium and is directed upward and backward through the flap valve of the fossa ovalis (Fig 4). The eustachian valve plays a crucial role in deflecting the flow through the PFO. Horizontal reorientation of the plane of the interatrial septum may facilitate flow from the IVC directly into the left atrium through the PFO. This reorientation of the sep-tum has been observed in patients with a right pneumonectomy, aortic aneurysm, or large pleu-ral effusion (54,55).
In patients with a PFO, pulmonary embolism is thought to be associated with a small but defi-nite risk for PDE and with findings of silent brain infarcts at MR imaging (56). Patients with a PFO and hemodynamically important pulmonary em-bolism are more likely to experience an ischemic stroke (13% vs 2.2%), peripheral arterial embo-lism (15% vs 0%) (57), and arterial hypoxemia possibly due to PDE (58).
Effect of PFO Morph- ology on Right-to-Left ShuntThe functional and morphologic characteristics of a PFO are closely related. The magnitude of a shunt through a PFO depends not only on he-modynamic parameters but also on the anatomy of the PFO (Fig 5). These include the size of the opening into the right atrium, length of the PFO tunnel, and extent of excursion of the flap mem-brane. The magnitude of a shunt through a PFO appears to be directly related to the degree of risk for a first stroke (42). Medium to large PFOs are found more often in patients with cryptogenic
Table 3: Predisposing Factors for Right-to-Left Shunt through a PFO or for Intracardiac Shunt
Increased pressure in the right side of the heart Physiologic cause (eg, Valsalva maneuver,
coughing) Chronic obstructive pulmonary disease Extensive pulmonary embolism Primary pulmonary hypertensionIntracardiac anatomic factors Chiari network Septal aneurysm (atrial, interventricular) Large eustachian valvePFO morphologic features Short flap length Large openingGross anatomic position Supine more than sitting

1578 October Special Issue 2014 radiographics.rsna.org
3–9 microbubbles; a moderate shunt, by 10–30 microbubbles; and a severe shunt, by more than 30 microbubbles. Patients with a cryptogenic stroke had a larger PFO with a more severe right-to-left interatrial shunt than did patients with a stroke of determined cause (59).
PFO tunnel length is another important de-terminant of the presence and severity of a right-to-left shunt (60,61). In a study performed by Natanzon and Goldman (62), the magnitude of the right-to-left shunt in patients with a stroke was greater than that in control subjects, but no signifi-cant difference was found between the two groups with regard to entry zone diameter (mean ± stan-dard deviation, 2.5 mm ± 2.0 vs 1.9 mm ± 1.6 for patients vs control subjects). This finding led Na-tanzon and Goldman to speculate about whether other measures could also affect the presence and magnitude of a shunt through a PFO. They reported a shorter flap length in patients with a
Figure 4. IVC flow and the eustachian valve. (a) Short-axis CT image shows prefer-ential IVC flow toward the fossa ovalis (FO) and eusta-chian valve (EV). In the pos-terior half of the right atrial (RA) chamber, blood enters from the IVC, flowing up-ward through the flap valve of the fossa ovalis and backward through the eustachian valve. The eustachian valve plays a crucial role in deflecting blood flow toward a PFO. LA = left atrium, SVC = superior vena cava. (b) Axial CT image demonstrates a prominent eu-stachian valve (EV) guarding the anterior ostial margin of the IVC. RV = right ventricle. (c, d) Axial MR images ac-quired at end diastole (c) and systole (d) show dynamic movement of the eustachian valve (arrow) during the car-diac cycle.
infarcts than in those with infarcts with a known cause (26% vs 6%) (42). Moreover, the risk of stroke appears to be increased in the presence of structures that direct flow toward a PFO (eg, a prominent eustachian valve) or hemodynamic changes that increase right-sided pressure (eg, a large pulmonary embolism) (Table 3).
Homma et al (59) characterized PFOs in pa-tients with findings of cryptogenic stroke to as-sess morphologic factors that might be conducive to the development of PDE. PFO size was mea-sured as the maximum separation of the septum primum and septum secundum in millimeters. A PFO was classified as large when the separation was 2 mm or greater and small when the separa-tion was less than 2 mm. The severity of a shunt was classified as mild, moderate, or severe on the basis of the number of microbubbles appearing in the left atrium during an agitated saline study: a mild shunt was characterized by the presence of

RG • Volume 34 Number 6 Saremi et al 1579
cryptogenic stroke than in those with incidental detection of a PFO at transesophageal echocar-diography (7.5 mm ± 3.4 vs 9.9 mm ± 6.0). We have observed similar findings at cardiac CT (Fig 6). In a recent study performed with multidetector CT in asymptomatic individuals with a PFO, 92% of shunts occurred in the presence of a PFO tun-nel length of 6 mm or less (60). Such information may be important for determining the feasibility of percutaneous closure of a PFO.
PDE is more common in patients with a bi-directional shunt through a PFO than in those with a right-to-left shunt only (Fig 6). However, a bidirectional shunt is a relatively uncommon finding (50). When the flap length is very short, a bidirectional shunt is more probable. Patients with an atrial septal aneurysm also have a very short PFO tunnel length. In a recent postmor-tem study, Ho et al (61) described two types of PFO: valve competent and valve incompetent.
Figure 5. CT angiography demonstrates components of the interatrial septum in three different patients. Magnified view for each case is pre-sented in the right column. (a, b) Four-chamber views show a small fossa ovalis (FO) with fatty infiltration of the interatrial groove and the atrioventricular sandwich (AVS). IVS = interventricular septum, mAV = muscular atrioventricular septum, MV = mitral valve, P = posterior margin of the fossa ovalis, RA = right atrium, SI = sep-tal isthmus, STV = septal leaflet of the tricuspid valve. (c–f) Short-axis images show a PFO (c, d) and a large fossa ovalis (FO) with a short interatrial groove (e, f). The septum secundum forms the interatrial groove, which cov-ers the superior (S), posterior, and inferior (I) margins of the fossa ovalis. Blue line denotes the septum primum. LA = left atrium, RA = right atrium.

1580 October Special Issue 2014 radiographics.rsna.org
Figure 6. Valve-incompetent PFO at CT angiography. (a) Short-axis CT image shows the free flap of the PFO valve (arrowheads), which is too short to cover the superior rim of the septum secundum and form a PFO tunnel (black arrow). Note the free flow of contrast mate-rial through the PFO (white arrows). (b) Short-axis CT image from another patient shows an atrial septal aneurysm (arrowheads) and a very short PFO tunnel (black arrow) causing a left-to-right shunt (white arrow). LA = left atrium, RA = right atrium.
PFOs with a short overlapping flap in the pres-ence of an atrial septal aneurysm were classified as incompetent, with a high likelihood of bidirec-tional flow. Similar morphologic features of valve incompetence observed at multidetector CT in patients with a PFO included a short PFO tunnel length and an atrial septal aneurysm (Fig 6) (60).
Effect of Structures Occur- ring in Association with a PFOThe presence of one or more aberrant ana-tomic structures in association with a PFO can increase the probability that PDE will occur. These abnormal structures include a Chiari net-work, an atrial septal aneurysm, and a persistent eustachian valve.
Chiari Network.—The Chiari network consists of coarse or fine fibers within the right atrium, arising from the eustachian or thebesian valve and con-necting them with the crista terminalis, right atrial wall, or interatrial septum (Fig 7a). This structure is a remnant of the embryonic right valve of the sinus venosus (63) and should be differentiated from a large eustachian valve by looking care-fully for attachments to other parts of the right atrium. A Chiari network has been reported in 2%–4% of autopsy studies (63) and is generally thought to have no clinical significance. In rare instances, however, a Chiari network may be the site of thrombus formation (64) (Fig 7b, 7c). In a large patient series, a Chiari network diagnosed at transesophageal echocardiography was seen in 2%
of patients (64). This feature was more frequently seen in patients with a PFO (83%) and a right-to-left shunt (55%) than in subjects within the con-trol group. A Chiari network was also frequently associated with an atrial septal aneurysm, which was seen in 24% of patients. Fine Chiari networks may be difficult to visualize at CT or MR imaging. However, a dedicated multidetector CT study of the right side of the heart may produce artifact-free images of the right atrium that depict a Chiari network (Fig 7b, 7c).
Atrial Septal Aneurysm.—An atrial septal aneu-rysm is another important anatomic feature to consider when evaluating PFO. An atrial septal aneurysm is defined as a bulge that protrudes more than 15 mm beyond the plane of the atrial septum (65). Pearson et al (66) used the Han-ley diagnostic criteria (65) to classify findings of atrial septal aneurysm into two groups on the basis of the direction and timing of the protru-sion. Generally, right atrial protrusion is the most common (76%) direction and is followed by tran-sient motion toward the left atrium during systole or with the Valsalva maneuver (65) (Fig 8). In-creased interatrial septal mobility is believed to increase the probability of PDE by mechanically redirecting blood flow from the IVC through the PFO into the left atrium.
The detection rate for atrial septal aneurysm is 4.6%–10% at transesophageal echocardiogra-phy (67,68). An atrial septal aneurysm associ-ated with a PFO has a prevalence of 30%–60%

RG • Volume 34 Number 6 Saremi et al 1581
(67,68) and is most likely associated with an increased rate of embolic events (67). Among patients with normal patency of the carotid arter-ies, atrial septal aneurysm is more prevalent in those with cerebral ischemia (28%) than in those without cerebral ischemia (10%) (67). An atrial septal aneurysm can easily be assessed at CT and MR imaging. In one study performed with mul-tidetector CT, an atrial septal aneurysm was seen in 4% of patients, and 63% of patients with an atrial septal aneurysm were found to have a left-to-right shunt (60) (Fig 6).
Persistent Eustachian Valve in Adults.—The eustachian valve, which guards the anteroinferior aspect of the IVC, is a remnant of the embryonic right valve of the sinus venosus (Fig 9a). During embryonic development, the eustachian valve directs oxygenated blood from the IVC through the PFO into the systemic circulation (69). By directing the blood from the IVC toward the interatrial septum, a persistent eustachian valve may prevent spontaneous closure of the PFO af-
ter birth and thereby indirectly contribute to the development of PDE. A prominent eustachian valve is a common finding at cardiothoracic CT and MR imaging (Fig 9b). In echocardiographic studies performed by Schuchlenz et al (69), a persistent eustachian valve was seen in 57% of patients, with a mean valve diameter of 1.0 cm ± 0.4 (range, 0.5–2.0 cm). Seventy percent of patients with a eustachian valve also had a PFO. A persistent eustachian valve was more common in patients with presumed PDE than in control subjects (68% vs 33%), but there was no signifi-cant difference in the size of the eustachian valve between the two groups.
Imaging-based Diag- nosis of Intracardiac ShuntsVarious imaging modalities can be used to diag-nose an intracardiac shunt either directly or in-directly (Table 4). Echocardiography is the most popular modality for this purpose; it is widely available, noninvasive, accurate, and relatively in-expensive. An intracardiac shunt can be directly
Figure 7. Chiari network. (a) Photo-graph of a cadaveric heart provides a four-chamber view of the right atrium (RA), with the Chiari network (*) in the anatomic region of the eustachian valve, anterior to the IVC and extending to the ostium of the coronary sinus (CS). (b, c) Axial (b) and two-chamber (c) CT angiograms of the right ventricle (RV) in a live patient show rounded and bandlike structures (arrows) attached to the walls of the IVC and coronary sinus (CS) ostium at the inferior cavoatrial junction. This finding was confirmed at echocardiography, which showed a pos-sible thrombus covering the Chiari net-work. The patient had a history of right ventricular endocardial pacemaker. FO = fossa ovalis, LA = left atrium, TV = tricuspid valve.

1582 October Special Issue 2014 radiographics.rsna.org
assessed with echocardiography and MR imaging; to evaluate extracardiac shunts, CT or MR imag-ing is commonly performed. However, given the widespread use of cardiac CT for other indica-tions, CT is increasingly relevant for assessments of intracardiac shunt and PFO as well. An intra-cardiac shunt may also be indirectly diagnosed on the basis of findings at transcranial Doppler US.
MR imaging enables direct flow quantification and provides valuable information about the size,
shape, and location of the PFO and its spatial relationship to other structures (70). Mohrs et al (70) found a good correlation between dynamic contrast-enhanced MR angiography and trans-esophageal echocardiography in the grading of PFO shunts. In their study, a right-to-left shunt through the PFO was demonstrated by compar-ing time-intensity curves for contrast material arrival in the left atrium and in a pulmonary vein. However, contrast-enhanced MR angi-
Figure 8. Atrial septal aneurysm. LA = left atrium, RA = right atrium. (a, b) Short-axis CT angiograms demonstrate an atrial septal aneurysm (arrow) pro-truding into the right atrium in diastole (a) and toward the left atrium in systole (b). Right atrial protrusion of an atrial septal aneurysm is the most common morphologic feature, whereas motion toward the left atrium during systole or with the Valsalva maneuver is transient. (c–e) Transesophageal echocardiograms obtained during an agitated saline contrast-enhanced CT study show the atrial septal aneurysm (arrow in c and e) with right-to-left shunting visible in d and e.

RG • Volume 34 Number 6 Saremi et al 1583
Figure 9. Eustachian valve or ridge. (a) Photograph of a cadaveric heart shows the right atrium, with a large eustachian valve or ridge (*) extending between the IVC and the coronary sinus (CS) ostium. C = crista terminalis, FO = fossa ovalis, TV = tricuspid valve. (b) Long-axis two-chamber black-blood MR image of the right ventricle (RV) shows a large eustachian valve (arrows) in the anteroinferior ostial margin of the IVC. RA = right atrium.
ography may be inferior to contrast-enhanced transesophageal echocardiography for detecting a right-to-left shunt and identifying an atrial septal aneurysm (71).
Electrocardiographically gated multidetector CT is a fast and easy method that may obviate invasive imaging studies by depicting a com-pletely closed interatrial septum. Demonstration of a PFO tunnel at multidetector CT may help predict the presence of a shunt. Only a limited number of studies have involved comparison of multidetector CT with transesophageal echocar-diography (60,72). Current CT techniques for coronary angiography are capable of showing a left-to-right shunt. This can be important because the demonstration of a left-to-right shunt, partic-ularly when a short flap valve length or atrial sep-tal aneurysm exists, is indicative of an incompe-tent valve mechanism and a high likelihood that the shunt is bidirectional. No provocative test is necessary to demonstrate a left-to-right shunt at multidetector CT.
For CT evaluation of intracardiac shunts, data must be collected for the entire cardiac cycle. This requires radiation-intensive retrospec-tive electrocardiographic gating. Detection of a small right-to-left shunt at the level of the PFO indicates a need for dedicated retrospectively gated right atrial CT angiography, preferably performed while the patient performs the Valsalva maneuver. The acquisition of high-quality right atrial CT angiograms is challenging and requires homogeneous enhancement of the right atrium, correct scanning timing, a small field of view lim-ited to the atria, and a heart rate of less than 70 beats per minute. Homogeneous enhancement of the right atrium can be obtained with simul-
taneous injections of moderately concentrated contrast material into the antecubital and femoral veins (73).
Transcranial Doppler US of the middle ce-rebral artery performed during the injection of contrast material can be used as an alternative method for indirect detection of a PFO or shunt (Fig 10). If both echocardiography and tran-scranial Doppler US are performed when the presence of a PFO is suspected, the PFO detec-tion rate is higher than that with either method used alone (74). Results of comparative studies with transesophageal echocardiography suggest that the sensitivity of transcranial Doppler US is higher than 90% but the specificity is low (ap-proximately 65%–90%). The low specificity of transcranial Doppler US may be due to technical limitations of the study or the presence of extra-cardiac shunts.
Imaging for Percutaneous PFO ClosureTable 5 lists the anatomic information required to prepare for percutaneous PFO closure. Cur-rent techniques for placement of PFO closure devices rely on fluoroscopic landmarks combined with either transesophageal or intracardiac echo-cardiographic guidance. Transesophageal echo-cardiography for device closure usually involves conscious sedation but may require general an-esthesia in patients with airway issues or a body habitus that makes transesophageal access dif-ficult. CT has been used for localization of the fossa ovalis to aid in transseptal catheterization (75). Given that a PFO is a three-dimensional structure with dynamic opening and closing, as well as a channel-like structure in some pa-tients, one-dimensional measurements may not

1584 October Special Issue 2014 radiographics.rsna.org
Tab
le 4
: Co
mp
aris
on
of
Dif
fere
nt
Imag
ing
Mo
dal
itie
s fo
r C
linic
al W
ork
up
of
PD
E
Mod
alit
yIm
agin
g W
orku
pO
ptim
al U
ses
Adv
anta
ges
Lim
itat
ions
Mul
tide
tect
or C
TIn
itia
l ass
essm
ent
of t
arge
t or
gan
dam
age
(ie,
per
iph-
er
al e
mbo
li an
d in
farc
-ti
on);
su
pp
lem
enta
l st
ud
ies
Det
ecti
on o
f in
trac
ar-
diac
and
ext
raca
rdia
c sh
unts
, dir
ect
depi
c-ti
on o
f th
rom
bus
Non
inva
sive
, rap
idly
per
form
ed s
tudy
of t
he c
hest
, abd
omen
, an
d pe
lvis
tha
t m
ay e
xclu
de p
redi
spos
ing
fact
ors
and
othe
r ca
uses
of e
mbo
lic e
vent
s; p
rovi
des
info
rmat
ion
abou
t P
FO
si
ze, w
hich
is im
port
ant
to a
void
inad
vert
ent
punc
ture
of t
he
sept
um s
ecun
dum
wit
h re
sult
ant
extr
acar
diac
per
fora
tion
; sh
ows
com
plet
e cl
osur
e of
the
inte
ratr
ial s
eptu
m o
r a
PF
O
tunn
el, fi
ndin
gs p
redi
ctiv
e of
the
pro
babi
lity
of a
n in
trac
ar-
diac
shu
nt (
pres
ence
of c
ompl
ete
clos
ure
may
obv
iate
mor
e in
vasi
ve im
agin
g st
udie
s); s
how
s ca
rdia
c an
d ex
trac
ardi
ac
anat
omic
pat
hway
s fo
r pr
epro
cedu
ral t
rans
atri
al in
terv
enti
on
asse
ssm
ent;
depi
cts
acut
e pu
lmon
ary
embo
lism
Rad
iati
on d
ose;
infe
rior
ity
to
tran
seso
phag
eal e
choc
ar-
diog
raph
y fo
r de
tect
ing
a ri
ght-
to-l
eft
shun
t th
roug
h a
PF
O
MR
imag
ing
Init
ial a
sses
smen
t of
tar
get
orga
n da
mag
e (i
e, b
rain
em
boli
and
infa
rcti
on)
Intr
acar
diac
and
ext
ra-
card
iac
shun
ts, d
irec
t th
rom
bus
imag
ing
Use
d to
ass
ess
card
iac
or e
xtra
card
iac
shun
ts a
nd q
uant
ify
di-
rect
flow
; dep
icts
ano
mal
ous
veno
us d
rain
age;
allo
ws
excl
u-
sion
of
pred
ispo
sin
g fa
ctor
s an
d d
iffe
ren
tiat
ion
of
poss
ible
ca
uses
of
embo
lic e
vent
s; p
rovi
des
deta
iled
info
rmat
ion
on
size
, sha
pe, a
nd s
pati
al r
elat
ions
hip
to o
ther
str
uctu
res
Infe
rior
to
tran
seso
phag
eal
echo
card
iogr
aphy
for
the
de
tect
ion
of a
rig
ht-t
o-le
ft
PF
O s
hunt
; inf
erio
r to
tra
ns-
esop
hage
al e
choc
ardi
ogra
-ph
y fo
r th
e id
enti
ficat
ion
of
atri
al s
epta
l ane
urys
ms
Tra
nses
opha
geal
ec
hoca
rdio
grap
hyS
uppl
emen
tal
Intr
acar
dia
c sh
un
t,
dir
ect
thro
mbu
s
imag
ing
Bes
t m
odal
ity
for
depi
ctin
g a
left
atr
ial a
ppen
dage
thr
ombu
s;
whe
n u
sed
in c
onju
nct
ion
wit
h tr
ansc
ran
ial D
oppl
er U
S,
the
PF
O d
etec
tion
rat
e is
hig
her
Inva
sive
; lim
ited
aco
usti
c w
in-
dow
s; p
atie
nt m
ust
perf
orm
th
e V
alsa
lva
man
euve
r to
al-
low
iden
tific
atio
n of
a s
hunt
Per
iphe
ral v
enou
s
Dop
pler
US
Sup
plem
enta
lE
xtra
card
iac
embo
lic
sour
ces
Eas
iest
mea
ns fo
r di
rect
ly d
epic
ting
thr
ombi
in t
he e
xtre
mit
ies
Low
sen
siti
vity
for
det
ecti
on o
f in
trap
elvi
c th
rom
biT
rans
cran
ial
Dop
pler
US
Sup
plem
enta
lIn
dire
ct e
valu
atio
n of
sh
unt
Whe
n pe
rfor
med
wit
h an
inje
ctio
n of
mic
robu
bble
con
tras
t m
ater
ial,
it c
an b
e a
relia
ble
alte
rnat
ive
met
hod
for
dete
ctio
n of
PF
O o
r in
trac
ardi
ac s
hunt
; whe
n us
ed in
con
junc
tion
with
ec
hoca
rdio
grap
hy, t
he P
FO
det
ecti
on r
ate
is h
ighe
r
Spe
cific
ity
for
dete
ctio
n of
in
trac
ardi
ac s
hunt
s m
ay
be lo
w in
pat
ient
s w
ith
an
extr
acar
diac
shu
nt

RG • Volume 34 Number 6 Saremi et al 1585
Figure 10. (a, b) Transcranial Doppler US was performed for PFO in two patients after injection of agitated saline and during the Valsalva maneuver. (a) Doppler waveform from the first patient shows a positive test result, with a mild to moderate shunt (“shower” effect). (b) Doppler waveform from the second patient shows a moderate to severe shunt (“curtain” effect). At transcranial Doppler US, passage of a single bubble leads to an instantaneous increase in signal amplitude. A diagnosis of PFO is based on the number of Doppler signals detected and the time elapsed between the end of the contrast material injection and the appearance of signal.
be accurate. With CT, detailed three-dimensional information can easily be obtained (Fig 11a). CT can demonstrate the relationship of important cardiac structures to the PFO and allows a deter-mination of the length of the interatrial groove, distance to the aortic root, anomalous coronary arterial course, and location of the coronary sinus ostium. Knowledge of the length of the interatrial groove and distance to the aortic root is crucial when planning the placement of a closure de-vice (60). The presence of a markedly thickened (eg, in lipomatosis) or unusually short interatrial groove may interfere with appropriate placement
of the PFO closure device and may increase the likelihood of complications such as dislodgment of the closure device or injury of adjacent struc-tures such as the aortic root.
The criteria for PFO closure are not standard-ized (76). Some authors recommend PFO clo-sure in the presence of a large PFO, a permanent right-to-left shunt (versus a Valsalva maneuver–induced shunt), or an atrial septal aneurysm (76). In this regard, cardiac CT can provide important information about the morphologic characteris-tics of the PFO; a permanent right-to-left shunt is less likely to be present when the PFO tunnel
Table 5: Imaging Analysis before Percutaneous PFO Closure
Imaging Features Sought and Assessed Figure(s) Showing the Feature
PFO morphology: size of opening, tunnel length, patency
Figures 5, 6
Thickness and length of superior interatrial groove (septum secundum)
Figure 11
Dimensions of fossa ovalis on short-axis and four-chamber views
Figures 5, 11
Presence of atrial septal aneurysm Figures 6, 8Distance between the PFO and both the vena cava
and the aortic root Figures 5, 11
Presence of atrial septal and sinus venosus defects …Integrity of pulmonary venous anatomy seen on
axial CT or MR images…
Presence of an anatomic abnormality that could interfere with device placement (eg, eustachian valve, Chiari network)
Figures 4, 7, 9
Presence of thrombus in the left atrial appendage …

1586 October Special Issue 2014 radiographics.rsna.org
Figure 11. Percutaneous closure of PFO. (a) Short-axis preprocedural reformatted CT image of the IVC at the level of the fossa ovalis (fo) shows the most important parameters of mea-surement (bidirectional arrows): the length of the superior interatrial groove (s) and the length of the membranous flap covering the fossa ovalis. AA = ascending aorta, LA = left atrium, RA = right atrium. (b) Postprocedural transesophageal echocardiogram shows septal occlusion (Amplatzer Septal Occluder; AGA Medical, Golden Valley, Minn) (arrows). LA = left atrium. (c, d) Short-axis (c) and four-chamber (d) postprocedural CT images show occlusion of a PFO (Cardioseal; NMT Medical, Boston, Mass) (arrows) in a patient with an atrial septal aneurysm. Inset in d shows an axial view of the occlusive device. LA = left atrium.
is well formed and narrow (Fig 5). CT and MR imaging are complementary to transesophageal echocardiography for assessing the effective-ness of a percutaneously placed occlusive device (77,78) (Fig 11b, 11c). However, a small residual shunt is common after placement of an occlusive device, and complete endothelialization of the device takes 3–6 months, so early postprocedural imaging may not be relevant.
Congenital Heart Malfor- mations and the Risk of PDE
The presence of an intracardiac shunt due to an atrial or ventricular septal defect can increase the risk of thromboembolism especially in patients with a permanent pacemaker, because the pace-
maker leads create a predisposition to thrombus formation (79). Patients with transposition of the great arteries and a concomitant baffle leak may also have an increased risk of PDE (Fig 12). For this reason, patients who require pacemaker im-plantation typically undergo a thorough prepro-cedural imaging evaluation to determine whether a baffle leak is present (79). Potential pathways of interatrial communication that may be seen at cardiac CT are enlarged thebesian veins pass-ing along the superior interatrial muscle bundle (Bachmann bundle) between the right and left atrial appendages (73). Pulmonary arteriovenous communications are a known complication after some types of cavopulmonary anastomoses be-cause of the diversion of normal hepatic venous

RG • Volume 34 Number 6 Saremi et al 1587
flow from the pulmonary circulation, which may lead to additional complications, including PDE.
Extracardiac Causes of Right-to-Left Shunt
Abnormal Venous ReturnThe source of cryptogenic stroke remains unex-plained in approximately 50% of patients who undergo imaging to determine whether PDE is present (80). One important role of CT or MR imaging in the evaluation of PDE is to exclude any anomalous venous drainage that may have gone undetected at previous echocardiography. Among the possible congenital causes of a right-to-left shunt, anomalous drainage of the left superior vena cava into the left atrium and fenestrated coronary sinus should be investigated. In less than 10% of patients with a persistent left superior vena cava, that vein drains into the left atrium either directly or through an unroofed coronary sinus, creating a right-to-left shunt (81) (Fig 13).
Large collateral mediastinal veins may cause a visible right-to-left shunt (systemic-to-pulmonary
venous shunt). PDE can develop with stenosis, thrombosis, or absence of the left brachiocephalic vein and severe stenosis or occlusion of the supe-rior vena cava (81). Collateral venous pathways frequently extend between the left brachioce-phalic vein and left atrium, through an arcade comprising the left superior intercostal vein or left vertical vein and a pulmonary vein, to the left atrium. These collateral pathways are best appre-ciated at CT (Fig 14).
Arteriovenous MalformationsParadoxical neurologic complications can occur in patients with a pulmonary arteriovenous mal-formation, a defect most often associated with Osler-Weber-Rendu disease or hereditary hem-orrhagic telangiectasia (82) (Fig 15). These pa-tients should be screened for lung arteriovenous malformations by using MR imaging or CT. It is inevitable that some of these patients will have a pulmonary arteriovenous malformation, with or without an associated PFO (which may be the sole cause of PDE), and that the malformation may remain a source of continued embolization
Figure 12. Mustard procedure for transposi-tion of the great arteries in a 24-year-old man. PDE-related embolic events caused infarc-tions in the spleen, brain, and left kidney. (a) Short-axis MR image shows a large baffle defect (arrow). RA = right atrium, SVC = su-perior vena cava. (b) Axial abdominal CT im-age shows splenic infarction (arrow). (c) Axial CT image shows the cardiac appearance after closure of the baffle defect with an occlusive device (Amplatzer Septal Occluder) (arrow).

1588 October Special Issue 2014 radiographics.rsna.org
Figure 14. Coronal CT image obtained after contrast material injection into the left arm of a 17-year-old female patient with hemoptysis, hypoxemia, and mild cyanosis after a Fontan procedure for a double-outlet right ventricle demonstrates an extracardiac cause of PDE: partial occlusion of the left brachiocephalic vein and extensive mediastinal venous collateral (Collat.) formation. A relatively large network of collateral vessels connected to the right superior pulmonary vein (RSPV) causes early filling of the left atrium (LA), an indication of a right-to-left shunt. Venous thrombosis combined with the right-to-left shunt led to the development of PDE. RPA = right pulmonary artery.
Figure 13. Extracardiac causes of PDE in a patient with repaired tetralogy of Fallot and multiple episodes of PDE-related brain infarction. (a) MR angiographic image obtained after contrast material was injected into the patient’s left arm demonstrates a right-to-left shunt due to direct communication of the left superior vena cava (arrow) with the left atrium (LA). (b) Transesophageal echocardiogram obtained after injection of agitated saline into the patient’s left arm shows bubbles (arrows) entering the left atrium (LA), a finding that confirms the presence of the right-to-left shunt. Images obtained after an agi-tated saline injection into the patient’s right arm showed no evidence of a PFO. Emboliza-tion of the left-sided communication was performed with a coil device. RA = right atrium.
even after PFO closure (82). Echocardiography would not be adequate for identifying such ab-normalities, and CT might be more reliable.
Differential DiagnosisWhen evaluating patients in whom the presence of PDE is suspected, it is important to determine whether other possible causes of embolic events are present. CT or MR imaging is helpful for identifying predisposing conditions such as aortic atherosclerotic disease, aortic dissection, intracar-diac masses, and intracardiac thrombi. An associ-ated acute pulmonary embolism is an important finding that is easily detected at CT. Cardiac sources of non-PDE-related embolic events are generally located in the left side of the heart. Em-bolic sources in the left side of the heart include a left atrial appendage thrombus associated with atrial fibrillation, left ventricular mural clot oc-curring in the setting of myocardial infarction, mitral or aortic valve vegetation, and tumor (83). Embolic phenomena are indicated by present-ing symptoms in as many as 20% of patients and may be caused by detached tumor fragments or thrombi (83). Atherosclerotic plaques of the aor-tic arch are an important source of extracardiac thromboembolism. The highest risk is associated with proximal arch plaques with a maximal diam-eter of more than 4 mm (84).
Nonvalvular atrial fibrillation is a common cause of embolic brain infarction in the elderly
(85). A left atrial appendage thrombus might occur in patients of any age, and every imaging study obtained for evaluation of PDE should be inspected carefully. At present, for the exclusion of thrombus in the left atrial appendage, MR

RG • Volume 34 Number 6 Saremi et al 1589
Figure 15. Axial CT image shows an extracardiac cause of PDE in a patient with Osler-Weber-Rendu disease: multiple pulmonary arteriovenous malforma-tions (arrows).
imaging and CT cannot replace transesopha-geal echocardiography (86). However, both MR imaging and CT may be attractive noninvasive alternatives if transesophageal echocardiography is technically unfeasible or is declined by the patient (77,86). If the left atrial appendage has a normal appearance at CT (a finding with a nega-tive predictive value of >95%), transesophageal echocardiography may not be needed (86). In-complete mixing of contrast material with blood in the left atrial appendage, especially in patients with atrial fibrillation, may result in many false-positive findings at CT. However, in a study in which transesophageal echocardiography was compared with CT, a two-phase CT protocol (an early arterial phase and a phase delayed after 30 seconds) was found to have high sensitivity and specificity for the diagnosis of left atrial append-age thrombus (87).
ConclusionImaging assessment for PDE usually requires complementary use of different modalities to al-low an accurate diagnosis excluding various dif-ferential possibilities. No single imaging modality is capable of depicting the entire spectrum of possible findings in PDE.
MR imaging plays a primary role in the di-agnosis of target lesions in the brain, and CT can easily show these lesions in other parts of the body. An embolic source in the peripheral veins can be detected with high sensitivity with US, whereas MR imaging and CT are better for the diagnosis of central venous thrombosis. An intracardiac shunt through a PFO, and the as-sociated anatomic details, is best depicted with transesophageal echocardiography. Electrocardio-graphically gated CT also can show the anatomic details of a PFO and may be helpful in selected
cases. MR imaging is not an ideal modality for assessing a PFO. In patients with a large intracar-diac shunt, MR imaging and echocardiography play a major role and can be used to quantify the shunt and demonstrate its exact location. In pa-tients with an extracardiac shunt, the use of echo-cardiography is limited; in this setting, CT and MR angiography are better choices because they provide valuable data about extracardiac lesions such as anomalous venous return and pulmonary arteriovenous malformation. MR angiography can provide additional functional information about vascular malformations (eg, the direction, amount, and rapidity of flow through the vessel) without exposing the patient to iodinated con-trast agents and ionizing radiation.
In summary, the following algorithm may be followed for the diagnostic imaging evalua-tion of patients in whom the presence of PDE is suspected. First, initial studies are performed to detect target lesions: MR imaging or CT of the brain, heart, abdomen, or extremities may be used, depending on the clinical manifestations. Second, predisposing intracardiac abnormalities are sought by performing contrast-enhanced echocardiogra-phy (preferably with a transesophageal approach) to identify PFO, intracardiac shunt, left-heart thrombus or mass, or aortic or mitral valve veg-etation. Cardiac MR imaging or CT should be performed if echocardiography is not feasible or if the echocardiographic findings are not convincing. Third, if the presence of DVT is suspected, Dop-pler US of the lower or upper extremity is per-formed. Fourth, if the presence of arterial lesions is indicated, additional studies with Doppler US, CT, or MR angiography of the aorta and carotid arteries are performed. Last, if there is evidence of a possible extracardiac predisposing cause, CT is performed to allow the detection of anomalous venous return and arteriovenous malformation.
References 1. Cohnheim J. Thrombose und embolie. In: Vorlesun-
gen über allgemeine pathologie. Vol. 1. Berlin, Ger-many: Hirschwald, 1877.
2. Zahn FW. Thrombose de plusieurs branches de la veine cave inférieure avec embolies consécutives dans les artères. Rev Med Suisse Rom, 1881;1: 227–237.
3. Zahn FW. Beiträge zur geschwustlehre. Dtsch Z Chir 1885;22(1-2):1–35.
4. Johnson BI. Paradoxical embolism. J Clin Pathol 1951;4(3):316–332.
5. Thompson T, Evans W. Paradoxical embolism. Q J Med 1930;os-23(90):135–150.
6. Swan HJ, Burchell HB, Wood EH. The presence of venoarterial shunts in patients with interatrial com-munications. Circulation 1954;10(5):705–713.
7. Loscalzo J. Paradoxical embolism: clinical presenta-tion, diagnostic strategies, and therapeutic options. Am Heart J 1986;112(1):141–145.

1590 October Special Issue 2014 radiographics.rsna.org
8. Stöllberger C, Slany J, Schuster I, Leitner H, Win-kler WB, Karnik R. The prevalence of deep venous thrombosis in patients with suspected paradoxical embolism. Ann Intern Med 1993;119(6):461–465.
9. Travis JA, Fuller SB, Ligush J Jr, Plonk GW Jr, Geary RL, Hansen KJ. Diagnosis and treatment of paradoxical embolus. J Vasc Surg 2001;34(5): 860–865.
10. Nijsten MW, Hamer JP, ten Duis HJ, Posma JL. Fat embolism and patent foramen ovale. Lancet 1989;1(8649):1271.
11. Gerriets T, Tetzlaff K, Hutzelmann A, et al. Associa-tion between right-to-left shunts and brain lesions in sport divers. Aviat Space Environ Med 2003;74 (10):1058–1060.
12. Han SS, Kim SS, Hong HP, Lee SY, Lee SJ, Lee BK. Massive paradoxical air embolism in brain occurring after central venous catheterization: a case report. J Korean Med Sci 2010;25(10):1536–1538.
13. Engelhardt M, Folkers W, Brenke C, et al. Neuro-surgical operations with the patient in sitting position: analysis of risk factors using transcranial Doppler sonography. Br J Anaesth 2006;96(4):467–472.
14. Kumar S, Wong G, Maysky M, et al. Amniotic fluid embolism complicated by paradoxical embolism and disseminated intravascular coagulation. Am J Crit Care 2010;19(4):379–382.
15. Horowitz MB, Carrau R, Crammond D, Kanal E. Risks of tumor embolization in the presence of an unrecognized patent foramen ovale: case report. AJNR Am J Neuroradiol 2002;23(6):982–984.
16. van Rossum AB, van Houwelingen HC, Kieft GJ, Pattynama PM. Prevalence of deep vein throm-bosis in suspected and proven pulmonary embo-lism: a meta-analysis. Br J Radiol 1998;71(852): 1260–1265.
17. Lethen H, Flachskampf FA, Schneider R, et al. Frequency of deep vein thrombosis in patients with patent foramen ovale and ischemic stroke or tran-sient ischemic attack. Am J Cardiol 1997;80(8): 1066–1069.
18. Cogo A, Lensing AW, Prandoni P, Hirsh J. Distribu-tion of thrombosis in patients with symptomatic deep vein thrombosis: implications for simplifying the diagnostic process with compression ultrasound. Arch Intern Med 1993;153(24):2777–2780.
19. Erharhaghen J, Bartz M, Di Giovanni S, Melms A, Haarmeier T, Sieverding L. An unusual location of deep venous thrombosis associated with ischemic stroke and persistent foramen ovale. Case Rep Neurol 2011;3(2):160–164.
20. Wells PS, Lensing AW, Davidson BL, Prins MH, Hirsh J. Accuracy of ultrasound for the diagnosis of deep venous thrombosis in asymptomatic patients after orthopedic surgery: a meta-analysis. Ann In-tern Med 1995;122(1):47–53.
21. Kassaï B, Boissel JP, Cucherat M, Sonie S, Shah NR, Leizorovicz A. A systematic review of the ac-curacy of ultrasound in the diagnosis of deep venous thrombosis in asymptomatic patients. Thromb Hae-most 2004;91(4):655–666.
22. Cham MD, Yankelevitz DF, Shaham D, et al. Deep venous thrombosis: detection by using indirect CT venography. The Pulmonary Angiography-Indirect CT Venography Cooperative Group. Radiology 2000;216(3):744–751.
23. Laissy JP, Cinqualbre A, Loshkajian A, et al. As-sessment of deep venous thrombosis in the lower limbs and pelvis: MR venography versus duplex
Doppler sonography. AJR Am J Roentgenol 1996; 167(4):971–975.
24. Lindquist CM, Karlicki F, Lawrence P, Strzelczyk J, Pawlyshyn N, Kirkpatrick ID. Utility of balanced steady-state free precession MR venography in the diagnosis of lower extremity deep venous thrombosis. AJR Am J Roentgenol 2010;194(5):1357–1364.
25. Cramer SC, Maki JH, Waitches GM, et al. Paradoxi-cal emboli from calf and pelvic veins in cryptogenic stroke. J Neuroimaging 2003;13(3):218–223.
26. Cramer SC, Rordorf G, Maki JH, et al. Increased pelvic vein thrombi in cryptogenic stroke: results of the Paradoxical Emboli from Large Veins in Isch-emic Stroke (PELVIS) study. Stroke 2004;35(1): 46–50.
27. Kiernan TJ, Yan BP, Cubeddu RJ, et al. May-Thurner syndrome in patients with cryptogenic stroke and patent foramen ovale: an important clinical associa-tion. Stroke 2009;40(4):1502–1504.
28. Aoyama T, Suehiro S, Shibata T, Sasaki Y, Fujii H. Paradoxical cerebral embolism in a patient with Paget-Schroetter syndrome. Ann Thorac Cardiovasc Surg 2005;11(6):429–431.
29. Rooden CJ, Tesselaar ME, Osanto S, Rosendaal FR, Huisman MV. Deep vein thrombosis associated with central venous catheters: a review. J Thromb Hae-most 2005;3(11):2409–2419.
30. Ong B, Gibbs H, Catchpole I, Hetherington R, Harper J. Peripherally inserted central catheters and upper extremity deep vein thrombosis. Australas Radiol 2006;50(5):451–454.
31. Petrea RE, Koyfman F, Pikula A, et al. Acute stroke, catheter related venous thrombosis, and paradoxical cerebral embolism: report of two cases. J Neuroim-aging 2013;23(1):111–114.
32. From AH, Wang Y, Eliot RS, Edwards JE. Coronary arterial embolism in persistent truncus arteriosus: report of a case following cardiac catheterization. N Engl J Med 1965;272:1204–1207.
33. Hausmann D, Mügge A, Becht I, Daniel WG. Di-agnosis of patent foramen ovale by transesophageal echocardiography and association with cerebral and peripheral embolic events. Am J Cardiol 1992;70 (6):668–672.
34. Dethy S, Manto M, Kentos A, et al. PET findings in a brain abscess associated with a silent atrial septal defect. Clin Neurol Neurosurg 1995;97(4): 349–353.
35. Wöhrle J, Kochs M, Hombach V, Merkle N. Preva-lence of myocardial scar in patients with cryptogenic cerebral ischemic events and patent foramen ovale. JACC Cardiovasc Imaging 2010;3(8):833–839.
36. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial—TOAST. Trial of Org 10172 in Acute Stroke Treat-ment. Stroke 1993;24(1):35–41.
37. De Castro S, Cartoni D, Fiorelli M, et al. Morpho-logical and functional characteristics of patent fora-men ovale and their embolic implications. Stroke 2000;31(10):2407–2413.
38. Lechat P, Mas JL, Lascault G, et al. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 1988;318(18):1148–1152.
39. Webster MW, Chancellor AM, Smith HJ, et al. Pat-ent foramen ovale in young stroke patients. Lancet 1988;2(8601):11–12.
40. Wessels T, Röttger C, Jauss M, Kaps M, Traupe H, Stolz E. Identification of embolic stroke patterns by

RG • Volume 34 Number 6 Saremi et al 1591
diffusion-weighted MRI in clinically defined lacunar stroke syndromes. Stroke 2005;36(4):757–761.
41. Kang DW, Chalela JA, Ezzeddine MA, Warach S. Association of ischemic lesion patterns on early diffusion-weighted imaging with TOAST stroke subtypes. Arch Neurol 2003;60(12):1730–1734.
42. Steiner MM, Di Tullio MR, Rundek T, et al. Patent foramen ovale size and embolic brain imaging find-ings among patients with ischemic stroke. Stroke 1998;29(5):944–948.
43. Venketasubramanian N, Sacco RL, Di Tullio M, Sherman D, Homma S, Mohr JP. Vascular distribu-tion of paradoxical emboli by transcranial Doppler. Neurology 1993;43(8):1533–1535.
44. Jauss M, Wessels T, Trittmacher S, Allendörfer J, Kaps M. Embolic lesion pattern in stroke patients with patent foramen ovale compared with patients lacking an embolic source. Stroke 2006;37(8): 2159–2161.
45. Santamarina E, González-Alujas MT, Muñoz V, et al. Stroke patients with cardiac atrial septal ab-normalities: differential infarct patterns on DWI. J Neuroimaging 2006;16(4):334–340.
46. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 de-cades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc 1984;59(1):17–20.
47. Dörr M, Hummel A. Images in clinical medicine: paradoxical embolism—thrombus in a patent fora-men ovale. N Engl J Med 2007;357(22):2285.
48. Thaler DE, Di Angelantonio E, Di Tullio MR, et al. The Risk of Paradoxical Embolism (RoPE) Study: initial description of the completed database. Int J Stroke 2012 Aug 9. [Epub ahead of print]
49. Lock JE. Patent foramen ovale is indicted, but the case hasn’t gone to trial. Circulation 2000;101(8): 838.
50. Lynch JJ, Schuchard GH, Gross CM, Wann LS. Prevalence of right-to-left atrial shunting in a healthy population: detection by Valsalva maneuver contrast echocardiography. Am J Cardiol 1984;53 (10):1478–1480.
51. Zanchetta M, Rigatelli G, Ho SY. A mystery featur-ing right-to-left shunting despite normal intracar-diac pressure. Chest 2005;128(2):998–1002.
52. Langholz D, Louie EK, Konstadt SN, Rao TL, Scanlon PJ. Transesophageal echocardiographic demonstration of distinct mechanisms for right to left shunting across a patent foramen ovale in the absence of pulmonary hypertension. J Am Coll Car-diol 1991;18(4):1112–1117.
53. Gallaher ME, Sperling DR, Gwinn JL, Meyer BW, Fyler DC. Functional drainage of the inferior vena cava into the left atrium: three cases. Am J Cardiol 1963;12:561–566.
54. Laybourn KA, Martin ET, Cooper RA, Holman WL. Platypnea and orthodeoxia: shunting associ-ated with an aortic aneurysm. J Thorac Cardiovasc Surg 1997;113(5):955–956.
55. Smeenk FW, Postmus PE. Interatrial right-to-left shunting developing after pulmonary resection in the absence of elevated right-sided heart pres-sures: review of the literature. Chest 1993;103(2): 528–531.
56. Clergeau MR, Hamon M, Morello R, Saloux E, Viader F, Hamon M. Silent cerebral infarcts in pa-tients with pulmonary embolism and a patent fora-men ovale: a prospective diffusion-weighted MRI study. Stroke 2009;40(12):3758–3762.
57. Konstantinides S, Geibel A, Kasper W, Olschewski M, Blümel L, Just H. Patent foramen ovale is an important predictor of adverse outcome in patients with major pulmonary embolism. Circulation 1998; 97(19):1946–1951.
58. Kasper W, Geibel A, Tiede N, Just H. Patent fo-ramen ovale in patients with haemodynamically significant pulmonary embolism. Lancet 1992;340 (8819):561–564.
59. Homma S, Di Tullio MR, Sacco RL, Mihalatos D, Li Mandri G, Mohr JP. Characteristics of patent foramen ovale associated with cryptogenic stroke: a biplane transesophageal echocardiographic study. Stroke 1994;25(3):582–586.
60. Saremi F, Channual S, Raney A, et al. Imaging of patent foramen ovale with 64-section multidetector CT. Radiology 2008;249(2):483–492.
61. Ho SY, McCarthy KP, Rigby ML. Morphologi-cal features pertinent to interventional closure of patent oval foramen. J Interv Cardiol 2003;16(1): 33–38.
62. Natanzon A, Goldman ME. Patent foramen ovale: anatomy versus pathophysiology—which determines stroke risk? J Am Soc Echocardiogr 2003;16(1): 71–76.
63. Bhatnagar KP, Nettleton GS, Campbell FR, Wagner CE, Kuwabara N, Muresian H. Chiari anomalies in the human right atrium. Clin Anat 2006;19(6): 510–516.
64. Schneider B, Hofmann T, Justen MH, Meinertz T. Chiari’s network: normal anatomic variant or risk factor for arterial embolic events? J Am Coll Cardiol 1995;26(1):203–210.
65. Hanley PC, Tajik AJ, Hynes JK, et al. Diagnosis and classification of atrial septal aneurysm by two-dimensional echocardiography: report of 80 consecutive cases. J Am Coll Cardiol 1985;6(6): 1370–1382.
66. Pearson AC, Nagelhout D, Castello R, Gomez CR, Labovitz AJ. Atrial septal aneurysm and stroke: a transesophageal echocardiographic study. J Am Coll Cardiol 1991;18(5):1223–1229.
67. Mattioli AV, Aquilina M, Oldani A, Longhini C, Mattioli G. Atrial septal aneurysm as a cardioem-bolic source in adult patients with stroke and nor-mal carotid arteries: a multicentre study. Eur Heart J 2001;22(3):261–268.
68. Mügge A, Daniel WG, Angermann C, et al. Atrial septal aneurysm in adult patients: a multicenter study using transthoracic and transesophageal echocardiography. Circulation 1995;91(11): 2785–2792.
69. Schuchlenz HW, Saurer G, Weihs W, Rehak P. Per-sisting eustachian valve in adults: relation to patent foramen ovale and cerebrovascular events. J Am Soc Echocardiogr 2004;17(3):231–233.
70. Mohrs OK, Petersen SE, Erkapic D, et al. Diagnosis of patent foramen ovale using contrast-enhanced dynamic MRI: a pilot study. AJR Am J Roentgenol 2005;184(1):234–240.
71. Nusser T, Höher M, Merkle N, et al. Cardiac mag-netic resonance imaging and transesophageal echo-cardiography in patients with transcatheter closure of patent foramen ovale. J Am Coll Cardiol 2006;48 (2):322–329.
72. Kim YJ, Hur J, Shim CY, et al. Patent foramen ovale: diagnosis with multidetector CT—compari-son with transesophageal echocardiography. Radiol-ogy 2009;250(1):61–67.

1592 October Special Issue 2014 radiographics.rsna.org
73. Saremi F, Kang J, Rahmanuddin S, Shavelle D. As-sessment of post-atrial switch baffle integrity using a modified dual extremity injection cardiac computed tomography angiography technique. Int J Cardiol 2013;162(2):e25–e27.
74. Droste DW, Schmidt-Rimpler C, Wichter T, et al. Right-to-left-shunts detected by transesophageal echocardiography and transcranial Doppler sonog-raphy. Cerebrovasc Dis 2004;17(2-3):191–196.
75. Graham LN, Melton IC, MacDonald S, Crozier IG. Value of CT localization of the fossa ovalis prior to transseptal left heart catheterization for left atrial ablation. Europace 2007;9(6):417–423.
76. Rigatelli G, Dell’Avvocata F, Cardaioli P, et al. Permanent right-to-left shunt is the key factor in managing patent foramen ovale. J Am Coll Cardiol 2011;58(21):2257–2261.
77. Mohrs OK, Petersen SE, Erkapic D, et al. Dynamic contrast-enhanced MRI before and after transcath-eter occlusion of patent foramen ovale. AJR Am J Roentgenol 2007;188(3):844–849.
78. Lee T, Tsai IC, Fu YC, et al. MDCT evaluation af-ter closure of atrial septal defect with an Amplatzer septal occluder. AJR Am J Roentgenol 2007;188(5): W431–W439.
79. Kuppahally SS, Litwin SE, Green LS, Ishihara SM, Freedman RA, Michaels AD. Utility of intracardiac echocardiography for atrial baffle leak closure in repaired transposition of the great arteries. Echocar-diography 2010;27(8):E90–E93.
80. Kristensen B, Malm J, Carlberg B, et al. Epidemiol-ogy and etiology of ischemic stroke in young adults
aged 18 to 44 years in northern Sweden. Stroke 1997;28(9):1702–1709.
81. Gilkeson RC, Nyberg EM, Sachs PB, Wiant AM, Zahka KG, Siwik ES. Systemic to pulmonary ve-nous shunt: imaging findings and clinical presenta-tions. J Thorac Imaging 2008;23(3):170–177.
82. Kjeldsen AD, Oxhøj H, Andersen PE, Green A, Vase P. Prevalence of pulmonary arteriovenous malfor-mations (PAVMs) and occurrence of neurological symptoms in patients with hereditary haemorrhagic telangiectasia (HHT). J Intern Med 2000;248(3): 255–262.
83. Burke A, Jeudy J Jr, Virmani RA. Cardiac tumours: an update. Heart 2008;94(1): 117–123.
84. Tenenbaum A, Garniek A, Shemesh J, et al. Dual-helical CT for detecting aortic atheromas as a source of stroke: comparison with transesophageal echocardiography. Radiology 1998;208(1):153–158.
85. Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gen-der of patients with atrial fibrillation: analysis and implications. Arch Intern Med 1995;155(5):469–473.
86. Feuchtner GM, Dichtl W, Bonatti JO, et al. Diag-nostic accuracy of cardiac 64-slice computed to-mography in detecting atrial thrombi: comparative study with transesophageal echocardiography and cardiac surgery. Invest Radiol 2008;43(11):794–801.
87. Hur J, Kim YJ, Lee HJ, et al. Left atrial appendage thrombi in stroke patients: detection with two-phase cardiac CT angiography versus transesoph-ageal echocardiography. Radiology 2009;251(3): 683–690.
This journal-based SA-CME activity has been approved for AMA PRA Category 1 CreditTM. See www.rsna.org/education/search/RG.

Teaching Points October Special Issue 2014
Paradoxical Embolism: Role of Imaging in Diagnosis and Treatment PlanningFarhood Saremi, MD • Neelmini Emmanuel, MD • Philip F. Wu, BS • Lauren Ihde, MD • David Shavelle, MD • John L. Go, MD • Damián Sánchez-Quintana, MD, PhD
RadioGraphics 2014; 34:1571–1592 • Published online 10.1148/rg.346135008 • Content Codes:
Page 1572The diagnosis of PDE is considered definitive when it is based on a finding at autopsy or at imaging of a thrombus that crosses an intracardiac defect in the setting of an arterial embolus. A diagnosis of PDE in the absence of these findings is considered presumptive. The triad of systemic embolism, venous thrombosis, and intracardiac communication defines the clinical diagnosis of PDE and allows treatment with a high level of confidence. The diagnosis of PDE is termed “possible” if an arterial embolus and PFO are detected; many physicians treat patients on the basis of a diagnosis of “possible PDE.”
Page 1573Overall, the results of the preceding studies show that (a) PDE from the lower extremity and possibly the pelvis is one mechanism that accounts for ischemia related to systemic embolization in a subset of patients and (b) pelvic CT or MR imaging may be useful for determining whether pelvic DVT is pres-ent in patients in whom findings are negative for DVT of the lower extremities.
Page 1574The cause of cryptogenic stroke remains undetermined in most cases because the event is transitory or reversible, investigators cannot look for all possible causes, and some causes remain unknown. The detec-tion of a PFO in a patient with a confirmed stroke does not necessarily mean that the cause of the stroke has been identified. Establishing a causal relationship between the presence of a PFO and the occurrence of a stroke remains the crucial point in the diagnosis of PDE. The four criteria described earlier for the diag-nosis of PDE may not always be met. The presence of other contributing factors, such as the morphologic characteristics of the PFO and associated structures, may increase the probability that PDE is present.
Page 1579–1580When the flap length is very short, a bidirectional shunt is more probable. Patients with an atrial septal aneurysm also have a very short PFO tunnel length. In a recent postmortem study, Ho et al described two types of PFO: valve competent and valve incompetent. PFOs with a short overlapping flap in the presence of an atrial septal aneurysm were classified as incompetent, with a high likelihood of bidirec-tional flow.
Page 1585The criteria for PFO closure are not standardized. Some authors recommend PFO closure in the pres-ence of a large PFO, a permanent right-to-left shunt (versus a Valsalva maneuver–induced shunt), or an atrial septal aneurysm.