Embed Size (px)
Citation preview

[CANCER RESEARCH 43, 5228-5234, November 1983)
Parenteral Level of Glucose Intake on Glucose Homeostasis, Tumor
Growth, Gluconeogenesis, and Body Composition in Normal andTumor-bearing Rats1
Ivan L. Cameron2 and Virginia A. Ord
Department ol Anatomy, The University ol Texas Health Science Center at San Antonio, San Antonio, Texas 78284
ABSTRACT
To determine the effects of different levels of glucose intakeon glucose homeostasis, gluconeogenesis, body composition,and tumor growth, we gave 8 days of total parenteral feeding ofa defined liquid formula diet to groups of Buffalo rats, with andwithout a transplantable Morris 7777 hepatoma. The level ofglucose intake was held at levels which ranged from 0 to 9.5 g/100 body weight per day while the levels of all other nutrientswere held constant. Measurements were made on tumor growthrate, terminal blood plasma glucose and whole blood láclatelevels,gluconeogenesis, body and organ weight, muscle nitrogencontent, liver glycogen, and urine analysis. Tumor-bearing rats(TB) at low glucose intake but not non-tumor-bearing rats (NTB)were found to be dependent on gluconeogenesis for maintenance of blood glucose homeostasis (normoglycemia). Bodyweight was dependent on glucose intake level in both TB andNTB rats with glucose intake rates of 5.7 g/100 g/day being thepoint between weight loss or gain. However, under these feedingconditions, tumor growth rate was not dependent on the glucoseintake rate. The weight of epididymal fat pad and the size of fatcells were positively correlated with glucose intake rate in bothTB and NTB rats, but the fat pad weight in TB rats showed agreater dependence on the rate of glucose intake than it did inthe NTB rats. Glucose intake of 3.8 g/100 g/day or less leads tosignificant loss of muscle mass and loss of muscle nitrogen(protein) in TB but not in NTB rats. Some liver glycogen wasdetected in all groups of rats except those TB rats with zeroglucose intake. TB rats with high glucose intake (5.7 to 9.5 g/100 g/day) had higher blood láclateand lower urine pH than didNTB rats. Thus, TB rats at low glucose intake (3.8 g/100 g/dayor less), as opposed to NTB rats, demonstrated a significantdependence on gluconeogenesis for glucose homeostasis, mobilized more of their liver glycogen, and catabolized more of theirmuscle proteins to supply the increased energy needs of thegrowing tumor and to maintain normoglycemia.
INTRODUCTION
The parenteral delivery by pump of a defined liquid formuladiet allows us to make direct correlations between the glucoseintake rate, which allows precise control over calorie intake, andthe measurement of a number of experimental parameters inTB3and in NTB rats. In this study, the level of glucose was held
constant at levels which ranged from 0 to 9.5 g/100 g/day, while
1Supported by National Cancer Institute Grant CA30956.2To whom requests lor reprints should be addressed.3The abbreviations used are: TB, tumor bearing; NTB, non-tumor-bearing; PAS,
periodic acid-Schiff.Received January 12, 1983; accepted August 2, 1983.
keeping the delivery of the remainder of nutrients constant. Thisexperimental approach allowed us to control nutritional variablesand to get a better understanding of glucose metabolism, gluconeogenesis, and the depletion of adipose and muscle as anenergy source in TB and NTB rats.
It was our hope that the integration of findings from such astudy would give us important new information on the role ofglucose or calorie intake rate on the metabolism of TB and NTBrats. The establishment of significant differences between theTB and the NTB rats should provide us with clues as to how thetumor influences host metabolism, and should also provide basicinformation that can eventually be used to design therapeuticinterventions to prevent the wasting of body mass due to thepresence of the tumor (cancer cachexia), or to suppress tumorgrowth.
The role of nutrition on tumor-host metabolism has been thesubject of several recent symposia and a review article. Theinterested reader is referred to these sources as an excellentbackground summary of this field (3, 12,18,19).
MATERIALS AND METHODS
The dispersing of animals into groups was done by assigning numbersto all rats, then dispersing the animals into groups by selection of randomnumbers from a random-number table. Male Buffalo rats, 7 weeks old,
were initially divided into 2 groups. One group of rats were inoculated inthe right flank with an 0.25-ml suspension of 107 viable Morris 7777
hepatoma cells, as reported previously (9). The Morris 7777 hepatomacells were obtained from Henryka Brania of the McArdle Laboratory forCancer Research in Madison, Wis. The second group of rats were giventhe same volume of lactated Ringer's solution. After 3 weeks, the rats
inoculated with tumor and those not inoculated with tumor cells wererandomly divided into groups to receive different levels of glucose. Theanimals were housed individually in metabolic cages with water available,and were exposed to a 14-hr light and 10-hr dark cycle from the time
they were 7 weeks of age.Animals were fed a liquid diet parenterally (i.V.). The components of
the elemental diet are listed in Table 1. Any other required trace elementsshould be available as diet or environmental contaminants. The glucoselevels in the i.v. solution ranged from 0 to 9.5 g/100 g/day. The i.v.solution was administered at a flow rate of 0.4 ml/hr/100 g the first day,0.6 ml/hr/100 g the second day, and 0.79 ml/hr/100 g from Day 3through the end of the experiment at Day 10.
The cannulation procedure has been described previously (10). Briefly,parenterally fed rats have a Silastic catheter tube inserted into thesuperior vena cava or the right atrium via the external jugular vein. Theother end of the catheter exits the body between the scapulae. The ratswere placed in a padded harness and attached to swivel apparatus(Instec Labs, Philadelphia, Pa.) via a tightly wound steel shielding cable,housing the plastic infusion tubing. The rats were infused at a constantcontinuous rate with a Holter Model 903 peristaltic pump (Critikon, Inc.,Tampa, Fla.).
5228 CANCER RESEARCH VOL. 43
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

Glucose Intake Rate on Tumor-Host Responses
TabtelFormula of the elemental diet
The nutritional composition of the liquid feeding solution is listed in this table.To the formula we add trace elements formula"; cobalt chloride, 56 mg; cupric
sulfate, 86 mg; zinc sulfate, 176 mg; potassium iodide (DSP); 195 mg in 10 mlwater, 1 ml; water, 1000 ml). The salts containing trace elements are dissolved inwater and a 10-ml dose is added to every liter of the standard liquid diet for feeding.
Final concentration
Crystalline aminoacid"Essential
aminoacidL-lsoleucineL-LeucineL-LysineMethionineL-PhenylalanineL-ThreonineL-TryptophanL-ValineNonessential
aminoacidL-AlanineL-ArginineL-HistidineL-ProlineL-SerineGlycineL-CystineTotalNitrogenglitter2.953.853.102.252.401.700.652.803.001.551.204.752.508.50<0.1041.36.25
mEq/liter
ElectrolytesMagnesiumsulfatePotassiumchlorideCalciumchloridePotassiumphosphateSodiumbicarbonateCholine
chlorideMultivitamin
mix (M.V.I.) (5-ml vial, use 0.50ml)0Ascorbic
acid (vitaminC)VitaminA (retinylpalmitate)VitaminD(ergocalciferol)Thiamine
hydrochloride (vitaminB,)Riboflavin(as 5-phosphate) (vitaminB2)Pyridoxinehydrochloride (vitaminB»)NiacmamideDexpanthenolVitamin
E (DL-n-tocopherylacetate)FolieacidcVitaminKc*
Freamine (McGaw Laboratories, Irvine,Calif.)."(USVPharmaceutical Corp., Tuckahoe, N.Y.)c
Sigma Chemical Co. (St. Louis, Mo.).4.0660.363.43.41144.641.7950
mg/liter1000ID/liter100
ID/liter5mg/liter1mg/liter1
.5mg/liter10mg/liter2.5mg/liter0.5Ill/liter2mg/liter0.4
mg/liter
Beginning at the start of the third week after tumor inoculation, whichwas the same time the rats were started on the different i.v. diets, bodyweight, tumor size, water intake, and urine output were measured daily.Tumor size was determined by measuring the long and short axes withvernier calipers; the cross-sectional area of the tumor was calculated by
using the formula for an ellipse. The rate of tumor growth was alsomeasured for each rat, as reported by Cameron ef al. (8). Samples ofurine were analyzed for pH, glucose, and ketone, using BILI-Labstix
(Ames Multistix, Elkhart, Ind.).On Day 10 the rats were anesthetized with an i.p. injection of sodium
pentobarbital (37 mg/kg in 0.9% NaCI solution). Blood samples (0.7 ml)were then obtained from the left external jugular. For blood plasmaglucose determination, 0.2 ml of blood was placed in a test tube with ananticoagulant, sodium heparinate, and centrifuged for 5 min. The plasmawas drawn off, frozen, and later assayed (26). For determination oflactate, 0.5 ml of whole blood was put directly into 1.0 ml of cold 6%HCIO4. The acidified samples were centrifuged for 10 min, and theprotein-free supernatants were neutralized with 0.3 ml 20% KOH. The
samples were placed on ice for 10 min, after which they were centrifuged
to remove the KCIo4 precipitate. Samples of the supernatant wereassayed enzymatically for lactate (16). Immediately after the initial bloodsample was taken the rats were given s.c. injections of sodium 3-
mercaptopicolinate, a gift from Dr. N. DiTullio of Smith Kline & FrenchLaboratories, Philadelphia, Pa., at 15 mg/100 g (75 mg/ml in 0.9% NaCIsolution). A further blood sample was collected from the anesthetizedrats 1 hr after administration of the sodium 3-mercaptopicolinate, and
was subsequently analyzed for glucose and lactate, as described above.To validate the 3-mercaptopicolinate method of assessment of gluco-neogenesis, 2 separate groups of normally fed and 24-hr starved ratswere given injections of this drug. The 24-hr starved rats, but not the
normally fed rats, showed significant increases in whole blood lactate(data not presented). This gives a clear indication that the 24-hr starved
rats, but not the normally fed rats, are dependent on gluconeogenesis.Thus, this method detects and measures gluconeogenesis in our laboratory, as previously reported by others (24).
After the last blood sample was taken, the rats were killed by etheroverdose. The following organs were dissected and weighed at the timethe rats were killed: liver, heart, epididymal fat pad, and gastrocnemiusmuscle. Sections of the liver and the epididymal fat pad were fixed in10% neutral buffered formalin for later histological analysis. The gastrocnemius muscle was frozen on dry ice. To obtain the dry weight themuscles were weighed, then heated in a vacuum oven at 100° at 3
dynes/sq cm until a stable weight was obtained, usually taking between2 and 3 days. The nitrogen concentration of the dried muscle wasdetermined using microdistillation apparatus (Labconco Corp., KansasCity, Mo.) by the micro-Kjeldahl method (2).
RESULTS
Rate of Patenterai Glucose Intake on Tumor Growth Rate.Three weeks after s.c. implantation of tumor cells on the rightflank of each rat, a palpable and measurable tumor was presentin each rat. At this time the TB rats weighed an average of 255±9 (S.E.) g and the NTB rats weighed an average of 255 ±5g. Thus the tumor was found not to have caused a significanteffect on the total body weight at the beginning of the feedingtreatment period (F = 0.0003; p, not significant).
Daily measurements of tumor size during the 8-day course ofthe experiment were made and were subjected to a least-squares linear and to a least-squares logarithmic regression
analysis. The linear regression model showed a higher correlationcoefficient value for 9 of the 10 tumors, as compared to thecorrelation coefficient value for the logarithmic model. The linearregression data were therefore selected for presentation, asshown in Table 2.
Tumor growth under the different rates of glucose intake gavetumor growth rate slopes which range from 122 to 183 sq mmincrease in cross-sectional area per day. The goodness of fit of
the growth slopes to a linear model is indicated by the highcorrelation coefficient values (range, 0.90 to 0.99). The table alsolists the intercept values of each tumor growth slope, whichgives a good measure of the initial cross-sectional area of the
tumor (range, 586 to 1405 sq mm). Past studies from thislaboratory showed a high correlation between cross-sectional
area of the tumor and tumor weight (9). It is therefore possiblefor us to get an accurate estimate of tumor weight based on itscross-sectional area. Using this procedure, we estimated the
mean initial tumor weight to be 18.25 ±1.90 g, which amountedto an average of 7.26% of the body weight. At the terminationof the experiment the mean tumor weight was 46.30 ±1.94 g,which amounted to an average of 18.68% of the initial bodyweight. The data showed that each tumor more than doubled in
NOVEMBER 1983 5229
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

/. L. Cameron and V. A. Ord
Table 2
Effect of 8 days of parenteral glucose intake (ranging from zero to 9.5 g/100 g/day) on tumor growth rate
Glucose intake rate(g/hr/100g)0.00.0
0.03.8385.75.75.79.59.5Least-squares
linear regression analysis of tumorgrowthIntercept,
initial Slope, tumortumor size' (sq growth rate (sq Correlation coef-
mm) mm/day) ficient(/•)1405
155 0.931154 181 0.90
996 177 0.961300 183 0.96925 181 0.94617 137 0.98586 194 0.92
1069 122 0.961050 143 0.94678 1770.99Least
squares linear regression analysis between glucoseintake rate and tumor growthrateSlope,
tumor growth rate/glucose in- rtake-1.7866
0.27
a Length and width measured were used to calculate the cross-sectional area
using the formula for an ellipse.6 Not significantly different from a slope of 0.
size during the parenteral feeding treatment period. This tumornormally causes death of untreated rats between 8 and 10 weeksafter its inoculation. To determine if the glucose intake rateinfluenced the tumor growth rate, a least-squares linear regres
sion analysis was performed and is presented at the bottom ofTable 2. The results of this analysis showed that the glucoseintake rate did not determine or directly correlate with the tumorgrowth rate under these experimental conditions.
Thus tumor growth rate was not found to be dependent onthe glucose intake rate when the intake of all other nutrients inthe liquid formula diet were held constant.
Rate of Parenteral Glucose Intake on Change in BodyWeight and on Terminal Plasma Glucose and Whole BloodLactate Levels in TB and NTB Rats. Table 3 summarizes theresults and the analysis of results of the rats given 8 days ofparenteral feeding at different glucose infusion rates on thepercentage of change in body weight, terminal blood glucoselevel, and terminal blood lactate level for both the TB and NTBrats.
The least-squares linear regression analysis revealed that
glucose intake rate was positively and significantly correlated tobody weight change as a result of the 8-day course of the
parenteral feeding treatments. The intercept values of the regression analysis showed that TB and NTB rats, when placed onzero glucose intake rate, lost between 19 and 20% of their initialweight. Statistical analysis for differences in slope of body weightchanges did not show significant differences between the TBand NTB rats in their weight response to increasing level ofglucose intake. The regression analysis showed that for each gincrease in glucose intake per 100 g per day there resulted a3.47 to 3.59% increase in body weight. It should be noted thatterminal body weight in the TB rats includes the weight of asubstantial tumor mass (average of 46.3 ±1.94 g). Clearly, theterminal body weight of TB rats less the tumor mass would beless than the terminal body weight of NTB rats.
Thus, overall body weight increases in both TB and NTB wasdependent on the glucose intake rate when the intake of all othernutrients was held constant. Under these experimental condi
tions a glucose intake rate of 5.7 g glucose per 100 g/day wasthe transition point between weight loss and weight gain.
Terminal plasma glucose level in either the TB or the NTBrats, as shown in Table 3, when correlated to the glucose intakerate by means of least-squares linear regression analysis were
not found to be significantly correlated. This indicated that glucose homeostasis in the plasma was maintained in both TB andNTB rats, regardless of the rate of glucose infusion. Urinanalysisduring the last 4 days of parenteral feeding showed no indicationof glucose, even in the rats on the highest levels of glucoseinfusion.
The terminal blood lactate level in NTB rats, as shown in Table3, was not significantly correlated with the glucose intake rate,as determined by least-squares linear regression analysis, but
terminal blood lactate level in TB rats was significantly correlatedwith the glucose intake rate. A statistical comparison betweenthe regression analysis slopes of the TB and NTB rats showeda significantly higher slope value in the TB rats (p < 0.005). Itwas also noted that blood lactate level at zero glucose intakewas lower in TB rats (intercept values, 0.448 mw) than in theNTB rats (intercept value, 1.113 mw), as seen by comparison ofthe regression analysis of slope intercept values (Table 3). Thus,terminal lactate level was found to be dependent on the glucoseintake rate in TB but not in NTB rats.
Urine pH might be anticipated to decrease as blood levels oflactate are increased above normal. Regular urine pH measure-
Table3Effect of 8 days of parenteral glucose intake (ranging from Oto 9.5 g¡WOg¡day)on body weight expressed as a percentage of initial body weight, and on terminal
blood plasma glucose and whole blood lactate levels
Rate ofglucose intake (g/hr/
100g)NTB
ratsLeast
squareslinearregressionanalysisSlopeInterceptTB
ratsLeast
squareslinearregressionanalysisSlopeInterceptSignificance
of slope differenceNTB
vs. TB rats0.00.00.00.03.83.83.83.85.75.75.78.90.00.00.03.83.85.75.75.79.59.5Body
wt(g)-20.0-18.7-18.7-19.2-19.2-3.5-6.5-15.02.43.49.68.93.59a-19.51-23.4-17.7-25.0-3.10.5-7.00.87.08.313.23.47a-19.79NS6Terminalglucose(HIM)8.8110.256.237.1213.016.787.349.568.346.495.676.23-0.1868.6245.988.386.417.719.158.988.958.699.777.900.2227.224NSTerminal
lactate(my)0.451.830.771.770.520.810.760.640.741.181.070.74-0.0501.1130.320.670.510.631.320.691.581.022.161.591.38'0.448<0.005
a Significantly different from a slope of 0 (p < 0.01).^ NS. not significant.
5230 CANCER RESEARCH VOL. 43
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

Glucose Intake Rate on Tumor-Host Responses
Table 4
Assessment of gluconeogenesis as measured by the change in blood plasma glucose and blood lactatelevels 1 hr after injection of 3-mercaptopicolinate (expressed as a percentage of initial blood level prior to 3-
mercaptopicolinate injection)
Glucose intake rate (g/
Tumor condì- hr/100 g/Group tion day) n Glucose Lactate Lactate/glucose
1 Notumor0-3.82
Notumor5.7-9.03
Tumor4TumorResults
of analysisofvarianceFP0-3.85.7-9.00-3.85.7-9.0544583.8
±7.0a108.3
±5.681
.5±3.692.2±6.52.826<0.1082.6
±14.888.5
±22.521
4.3±46.5"137.8
+9.64.321<0.051.02
±0.210.85
±0.242.59
±0.49C1.56
±0.215.153<0.025
a Mean ±S.E.0 Significantly different from Groups 1 and 2, p < 0.03.c Significantly different from Groups 1, 2, and 4, p < 0.05.
ments were made on all rats in the study. A statistical analysisof variance of urine pH in TB and NTB rats on either low glucoseintake (0 to 3.8 g/100 g/day) or high glucose intake (5.7 to 9.5g/100 g/day) showed that the TB rats on high glucose had asignificantly (p < 0.001) lower pH (7.07 ±0.15) than the other 3groups of rats (range, 7.86 ±0.14 to 7.91 ±0.16). The other 3groups were not significantly different.
Rate of Patenterai Glucose Intake on Gluconeogenesis inTB and NTB Rats. To help determine the mechanism for maintenance of normoglycemia in the TB and NTB rats, as shown inTable 3, we subsequently measured their gluconeogenesis activity. The assessment of gluconeogenesis was done by inhibitinggluconeogenesis with 3-mercaptopicolinate, and then taking
blood samples for blood glucose and lactate levels 1 hr later.Table 4 summarizes the data and the analysis of the data fromthese measurements. A statistical analysis of variance of thepercentage of change in plasma glucose and blood lactate levelsfrom immediately before to 1 hr after the 3-mercaptopicolinate
injection was performed. The analysis of TB and NTB rats onlow glucose intake (0 to 3.8 g/100 g/day) and those on highglucose intake (5.7 to 9.5 g/100 g/day) revealed that the percentage of change in blood lactate in the TB rats was significantlyhigher than the change in blood lactate in the NTB rats witheither high or low glucose intake. Analysis of the ratio of thechange in lactate to the glucose in each rat showed that the TBrats on low glucose intake have a significantly higher ratio thanall of the other groups of rats. These results gave the indicationthat TB rats on the low glucose intake rates were dependent ongluconeogenesis for glucose homeostasis, whereas the NTBrats on low glucose intake rates were not dependent on gluconeogenesis for maintenance of glucose homeostasis.
Rate of Parenteral Glucose Intake on Organ Weights andBody Composition in TB and NTB Rats. Table 5 summarizesthe data and the analysis of data of 8 days of parenteral feedingat different glucose infusion rates on organ weights, expressedas a percentage of initial body weight for both the TB and NTBrats. Table 5 lists the results of a least-squares linear regression
analysis between the glucose intake rate and the terminal organweights for TB and NTB rats. To determine if the terminal organweights of TB rats showed a different response to glucose intakerate than did the NTB rats, a statistical analysis for differencesin the regression slopes was performed. Statistically differentorgan weight responses to glucose intake were determined to
TablesEffect of 8 days of parenteral glucose intake (ranging from Oto 9.5 g/WO g/day)
on terminal organ weights expressed as a percentage of initial body weight
Rate ofglucose Epididy- Gastroc-(g/hr/ mal fat nemius100g) pad muscle Liver Heart
NTBratsLeast
squareslinearregressionanalysisSlopeIntercept0.00.00.00.03.83.83.83.85.75.75.78.90.2910.3360.4550.3850.7800.5590.5520.4631.0190.5570.5400.4980.0360.4110.4570.5130.4740.4550.5290.5560.5490.4630.5370.5570.5400.4980.0070.4863.322.603.604.002.402.932.972.543.403.452.923.170.0323.2180.2380.3030.2490.3380.3090.3220.3340.3000.3230.4130.3570.3560.0090.298
TB rats 0.00.00.03.83.85.75.75.79.59.5
Least squares linearregression analysis
SlopeIntercept
Significance of slope differences
NTB vs. TB rats
0.4310.3040.4350.7530.6380.7580.7440.8101.2301.050
0.076a
0.381
<0.05
0.3860.3880.3860.4540.4930.5390.5340.5140.4850.612
0.018a
0.399
2.52.73.13.72.93.23.23.16.05.1
0.255a
2.436
<0.05 <0.005
0.2650.2380.2700.3640.3160.2860.3190.3170.3020.357
0.0070.272
NS°
Significantly different from a slope of 0 (p < 0.01).6 NS, not significant.
exist between the TB and the NTB rats in the epididymal fatpad, gastrocnemius muscle, and liver (see the bottom of Table5). The regression slopes of the heart weight were not shown tobe significantly different between the TB and NTB rats.
Specifically, the weights of the fat pad, the gastrocnemius,and the liver in the TB rats were shown to be significantly moredependent on the glucose intake rate than was the case in theNTB rats.
Further assessments were made on the fat pad, the gastro-
NOVEMBER1983 5231
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

/. L Cameron and V. A. Ord
cnemius, and the liver to better understand the nature of differences in the organ weights in TB and NTB rats. Histologicalcross-sections through the middle of the epididymal fat pad were
examined in all rats. The number of fat cells in unit areas nearthe central vessels was scored with a microscope and with theaid of an ocular grid on coded histological slides. A statisticalanalysis of variance of the data showed a significant differenceto exist, and a Student-Newman-Keuls multiple comparison test
showed that a decrease in number of fat cells (adipocytes) perunit area occurred as the glucose intake rate was increased fromzero to 5.7 g/100 g/day. No significant differences in numbersof fat cells occurred at higher glucose intake rates. Histologicalexamination showed that the number of fat cells per unit areawas related to the observed size of the fat cell. These resultsindicated that the individual fat cells of both TB and NTB ratsdecreased their size by loss of stored fat (lipolysis), and that thisloss of fat is dependent on glucose intake at rates below 5.7 g/100 g/day.
Urinalysis showed a significant development of ketonuria inthose TB rats with low glucose intake rates (0 to 3.8/100 g/day)during the last 2 to 3 days of the experiment, compared to TBrats on higher glucose intake or to any of the NTB rats (p <0.001).
To further assess differences in the gastrocnemius musclemass under different levels of glucose intake, the muscle fromeach rat was dried to a constant weight and the water contentwas calculated by subtraction of the dry weight from the wetweight. The results, expressed as percentage of water, are givenin Table 6. Analysis of variance showed no significant differencesin the water content between TB or NTB rats, and no significantdifferences between the low and the high glucose intake rategroups (Table 6). Analysis of the nitrogen content of these samemuscles was performed as a means of determining proteinmetabolism. Table 6 lists the results of this study and a statisticalanalysis of the data. The analysis showed that the muscles fromthe group of TB rats on a low glucose intake (0 to 3.8 g/100 g/day) had significantly less nitrogen than the muscles from any ofthe other groups of rats. The results showed that under theseexperimental conditions, the maintenance of muscle nitrogen(protein) is dependent on adequate glucose intake rate (>3.8 g/100 g/day) in TB rats as compared to the NTB rats.
Histological sections were made on the left lobe of the liver ofall rats in the study. One slide set of histological sections wasdigested with «-amylaseand another set of sections was treatedthe same, except that the «-amylase was omitted from theprocedure. The slide sets were both stained with a PAS-stainingreaction and were coded for analysis. No liver treated with a-amylase was found to have a positive PAS-staining reaction.PAS-positive staining was found in the livers of 3 of 10 TB ratsand in the livers of 9 of 13 NTB rats. A PAS-positive staining
reaction was found in 1 of 5 of the TB rats but in 7 of 9 NTBrats with glucose intake of >3.8 g/100 g/day. A PAS-positive
staining reaction was found in none of the TB rats on zeroglucose intake, but a positive PAS reaction was found in 4 of 5NTB rats on zero glucose (this difference was significant at p <0.05).
Histological evidence of liver cell vacuolization was seen inseveral TB and NTB rats with glucose intake rates >8.92 g/100g/day, but was not observed in the livers of rats with lowerglucose intake rates. Pieces of those livers that showed vacuolization were processed for histological staining with the lipid
Table 6Analysis of nitrogen and water content of the gastrocnemiusmuscle
Glucose intake rate
Tumor condì- (g/hr/100 Nitrogen in wholeGroup tion g/day) n muscle (mg) % of water
1234NotumorNotumorTumorTumor0-3.85.7-8.90-3.85.7-9.584554.31
±0.11"4.60
±0.113.52±0.20*4.50
±0.2974.7
±0.673.8±0.775.6±0.275.7±0.3Results
of analysisofvarianceFP5.06<0.051.9NSC
Mean ±S.E.b Significantlydifferent from Groups 1, 2, and 4.c NS, not significant.
stain, oil red O. The vacuoles gave a positive oil red O stainingreaction, and the vacuolization of the liver cells was attributed tofat.
DISCUSSION
The finding that tumor growth rate was not dependent on theglucose intake rate when all of the other nutrients were heldconstant was unexpected, based on our past studies on the ratMorris 7777 hepatoma system. These past studies repeatedlyshowed that total parenteral feeding of the TB rats stimulatedtumor growth in comparison to TB rats given cereal-based stockchow ad libitum (7-9). Experimental results similar to those
reported here have been reported by Buzby ef al. (6). They, too,found that tumor growth rate was not dependent on the glucoseintake rate when the intake of all other nutrients (amino acidsand minerals) was held constant. Reasons that the tumor growthrate was not dependent on glucose intake rate can be proposed.As our present experimental findings (Table 3) show that thehost maintained normoglycemia regardless of the glucose intakerate, it seems likely that growth of the tumor was not limited bythe availability of blood glucose. Perhaps the ad libitum feedingof TB rats with a large rapidly growing Morris 7777 hepatomawith stock chow, as opposed to the total parenteral alimentationwith high levels of amino acids, did not provide adequate aminoacid intake to meet the needs of the growing tumor.
Further support for this idea is provided in a study by Buzbyef al. (6), which showed that parenteral feeding of amino acidswithout glucose, as compared to a cereal-based stock chow ad
libitum, stimulated tumor growth. It seems likely that when thesize of the tumor and its nutrient demands reach a critical point,the plasma glucose level or perhaps the level of amino acidswould become limiting to tumor growth. Singh ef al. (24) haveshown in rats that when the weight ratio between a transplant-
able sarcoma and the body weight reached a critical ratio of 0.31to 0.50, the blood plasma glucose level became significantlylower. It seems likely that tumor growth rate might be limited byhypoglycemia under such extreme tumor conditions.
Let us briefly review and integrate the tumor-associated
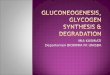
changes in host tissues and the metabolic abnormalities seen inresponse to the level of glucose intake. Drawings to help integrate and explain many of the observed findings of the presentstudy are put forth in Chart 1. This chart depicts the effects ofdifferent levels of glucose intake rate on TB and NTB rats whenthe intake of all other nutrients was held constant. Remember
5232 CANCER RESEARCH VOL. 43
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

Glucose Intake Rate on Tumor-Host Responses
Nutritional Intake
Glucose. Amino acids
Glucose'
homeostasis
Fat storeshpogenesis4
Nutritional Intake
Glucose, Amino acids
^ Liverglycoganesisglycogtn
aciduna
Nutritional Intake
No glucose. Amino acids
Glucosehomeostasis
t
Nutritional Intake
No or low glucose. Amino acids
Liverjglycogenesisglycogen
storage
glycerol-+ é¿
F F A (complete oxidation)
ketonuria
Chart 1. Effects of different levels of glucose intake on glucose homeostasis, gluconeogenesis, and body composition changes in TB and NTB rats as determined inthe present study. Rats with and without a transplantante Morris 7777 hepatoma were parenterally fed different levels of glucose (range, 0 to 9.5 g/100 g/day), whileholding the intake of other nutrients (amino acids, vitamins, and minerals) constant. Key observations showed that plasma glucose homeostasis (normoglycemia) wasmaintained regardless of glucose intake rate or tumor condition. Lipolysis from fat stores occurs in TB and NTB rats at low glucose intake and appears to be a majorsource of energy in these rats. Significant muscle protein catabolism and liver glycogen depletion occurred only in TB rats with little or no glucose intake. Significantgluconeogenesis occurred only in TB rats at low glucose intake, and this gluconeogenesis may be supported by substrates from different sources such as láclate, asshown in the chart. This might explain the low blood lactate levels in the TB rats on tow glucose intake. The increased whole blood lactate levels that occurredpredominantly in TB rats with high glucose intake rates suggest a high rate of tumor glycolysis. which would help to account for the increased lactate levels and theaciduna as was seen in these TB rats. FFA, free fatty acid.
that TB and NTB rats were shown to maintain normoglycemiaregardless of the glucose intake rate. Chart 1 indicates that theweight of the epididymal fat stores decrease by lipolysis in bothTB and NTB rats as the glucose (energy) intake rate drops below5.7 g/100 g/day. Apparently this lipolysis is occurring in responseto the low calorie intake in the diet. That no ketonuria was foundin NTB rats with little or no glucose intake, but was observedduring the last 2 to 3 days in TB rats with no glucose intake,suggests that fatty acid oxidation was complete in NTB rats butmay not have been complete in the TB rats. Perhaps the demandfor glycerol for gluconeogenesis in the TB cachectic host maylimit its availability for lipogenesis and be associated with incomplete oxidation of fatty acids, resulting in ketonuria. In fact it hasbeen previously suggested that suppression of free fatty acidoxidation reflects utilization of glycerol for the acceleration ofgluconeogenesis in cancer patients (21). That gluconeogenesis,as a source of glucose production, is an energy-inefficient proc
ess has been repeatedly suggested in TB individuals (1,4,5,13,14,17, 20, 22-25, 27).
No evidence of significant gluconeogenesis was found in NTBrats with little or no glucose intake, and yet normoglycemia wasmaintained. In this case the NTB rats appear to mobilize andefficiently use lipid stores as a major energy source, and theNTB rats are apparently able to maintain normoglycemia withoutmeasurable gluconeogenesis, probably by lowering their energyrequirements. In other words, glucose utilization may be very
slow in this particular group of NTB rats. The sustained paren-
teral intake of amino acids, even with no glucose intake, supported maintenance of muscle protein in these NTB rats, unlikewhat one expects from NTB rats during sustained total starvation(4,25).
As illustrated in Chart 1, muscle mass and muscle proteincontent (as measured by nitrogen content) were maintained inall TB and NTB rats, except those TB rats on 3.8 g/100 g/dayor less of glucose. An implication of this finding is that the TBrats on low glucose intake have catabolized muscle protein tomobilize amino acids, such as alanine. Such amino acids areutilized for the accelerated gluconeogenesis observed in thesesame TB rats (Table 4), but are also utilized for tumor growth.
What causes the gluconeogenesis seen only in TB rats on lowglucose intake? In addition to the possible control of gluconeogenesis: (a) by substrate levels; (o) by blood plasma glucoselevels; (c) by the extent to which phosphate groups are attached(phosphorylation) to enzymes that synthesize glucose (which isusually controlled by rapidly acting hormones like glucagon); and(d) by effectors of several of the enzymes that synthesize glucose. Cohen ef al. (11 ) have reported evidence that the slow-
acting thyroxine hormone stimulates the rate of glucose production via gluconeogenesis. This stimulation involves the mitochondria! enzyme that converts a-glycerolphosphate to dihydroxyace-
tone (glycerophosphate dehydrogenase), which is the next stepin the gluconeogenic pathway. Studies on the role of thyroxine
NOVEMBER 1983 5233
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

/. L Cameron and V. A. Ord
in the control of gluconeogenesis in TB and NTB individuals maytherefore prove fruitful. Waterhouse (27) has recently reportedthat the metabolism of branched-chain amino acids, such as
leucine, is not under normal control in malnourished cancerpatients, and that this imbalance may be linked to the frequentlyobserved high gluconeogenesis in cancerous individuals.
That uncontrolled gluconeogenesis is an important factor incachectic cancer conditions is suggested by the fact that theblocking of gluconeogenesis in TB rats by an inhibitor of theenzyme phosphoenolpyruvate carboxykinase, combined with total parenteral hyperalimentation, proved successful in preventingcancer cachexia under experimental conditions (7,15). How thehost meets the ever-increasing nutrient needs of the growing
tumor is at least partially explained by our findings; however, themechanism causing these changes remain to be characterized.It is reasonable to expect that elucidation of the control ofgluconeogenesis in TB individuals will add greatly to our understanding and to our treatment of cancer cachexia.
REFERENCES
1. Arbeit. J. M.. Buri. M. E.. Rubenstein, L. V., Gorschboth, C. M., and Braman,M. F. Glucose metabolism and the percentage of glucose derived from alanine:response to exogenous glucose infusion in tumor-bearing and non-tumor-bearing rats. Cancer Res., 42:4936-4942,1982.
2. Archibald, R. M. Nitrogen by the Kjeldahl method. In: 0. Seligson (ed.).Standard Methods of Clinical Chemistry, Vol. 2, pp. 91-98. New York: Academic Press, Inc., 1958.
3. Arno«,M. S., VanEys. J., and Wang, Y.-M. (eds). Molecular Interrelations of
Nutrition and Cancer. New York: Raven Press, 1982.4. Brennan. M. F. Uncomplicated starvation versus cancer cachexia. Cancer
Res., 37: 2359-2364,1977.5. Bun, M. E.. Lowry, S. F., Gorschboth, C . and Brennan, M. F. Metabolic
alterations in a noncachectic animal tumor system. Cancer (Phiia.), 47:2138-
2146,1981.6. Buzby, G. P., Mullen, J. L, Stein, T. P., Miller, E. E., Hobbs, C. L, and Rosato,
E. F. Host-tumor interactions and nutrient supply. Cancer (Phila.), 45: 2940-
2948,1980.7. Cameron, I. L. Effect of total parenteral nutrition on tumor-host responses in
rats. Cancer Treat. Rep., 65 (Suppi. 5V 93-99,1981.
8. Cameron, I. L., Ackley, W. J., and Rogers, W. Responses of hepatoma-bearingrats to total parenteral hyperalimentation and to ad libitum feeding. J. Surg.Res., 23:189-195,1977.
9. Cameron, I. L, and Pavlat, W. A. Stimulation of growth of a transplantablehepatoma in rats by parenteral nutrition. J. Nati. Cancer Inst., 56: 597-602,
1976.10. Camilo, A. J., and Sawyer, C. H. Observations on successive proestrous LH
surges in individual 4-day cycling and post-pseudo-pregnant rats. Acta Endocrino!., 88:274-284,1978.
11. Cohen, S., Ogawa, S., and Shuiman, R. G. "C NMR studies of gluconeo
genesis in rat liver cells: utilization of labeled glycerol by cells from euthyroidand hyperthyroid rats. Proc. Nati. Acad. Sci., 1603-1607,1979.
12. DeWys, W. D. Pediatrie cancer and nutrition workshop. Cancer Res., 42: 695-
782,1982.13. Gold, J. inhibition of gluconeogenesis at the phosphoenolpyruvate carboxyki
nase and pyruvate carboxytase reactions, as a means of cancer chemotherapy.Oncology (Basel). 29:74-89,1974a.
14. Gold, J. Cancer cachexia and gluconeogenesis. Ann. N.Y. Acad. Sci.. 230:103-110,1974b.
15. Grubbs, B., Rogers, W., and Cameron, I. Combining total parenteral nutritionand inhibition of gluconeogenesis to overcome cancer cachexia. Oncology(Basel). 36: 216-223,1979.
16. Gutman, I., and Wanfield, A. W. L-(+)-Lactate determination with lactic dehy-drogenase and NAD. In: H. V. Bergmeyer (ed.), Methods of Enzymatic Analysis,Ed. 2, pp. 1464-1468. New York: Academic Press, Inc., 1974.
17. Hoiroyde, C. P.. and Reichard, G. A. Carbohydrate metabolism in cancercachexia. Cancer Treat. Rep., 65 (Suppl. 5): 55-59,1981.
18. Kisner, D. L, and DeWys, W. 0. The nutrition of the cancer patient. CancerTreat. Rep., 65 (Suppl. 5V 1-158.1981.
19. Lawson. D. H., Richmond, A., Nixon, D. W., and Rudman, D. Metabolicapproaches to cancer cachexia. Annu. Rev. Nutr., 2:277-301.1982.
20. Lundholm. K., Edstrom, S., Ekman, L, Karlberg, I., and Schereten. T. Metabolism in peripheral tissues in cancer patients. Cancer Treat. Rep., 65 (Suppl.5V 79-83,1981.
21. Ruderman, E., Toews, C., and Shafren, E. Rote of free fatty acids in glucosehomeostasis. Arch. Intern. Med., 123:299-313,1969.
22. Sauer, L. A., Stayman, J. W., Ill, and Oauchy, R. T. Amino acid, glucose, andlactic acid utilization in vivo by rat tumors. Cancer Res., 42:4090-4097,1982.
23. Shapot, V. S, and Bhnov. V. A. Blood glucose levels and gluconeogenesis inanimals bearing transplantable tumors. Cancer Res., 34:1827-1832,1974.
24. Singh, J., Grigor, M. R., and Thompson, M. P. Glucose homeostasis in ratsbearing a transplantable sarcoma. Cancer Res., 40:1699-1706,1980.
25. Stein, T. P. Cachexia, gluconeogenesis and progressive weight loss in cancerpatients. J. Theor. Bwl., 73: 51-59,1978.
26. Trinder, P. Determination of glucose in blood using glucose oxidase with analternative oxygen acceptor. Ann. Clin. Biochem., 6: 24-27,1969.
27. Waterhouse, C. Oxidation and metbolic interconversions in malignant cachexia.Cancer Treat. Rep.. 65 (Suppl. 5V 61-66.1981.
5234 CANCER RESEARCH VOL. 43
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

1983;43:5228-5234. Cancer Res Ivan L. Cameron and Virginia A. Ord Normal and Tumor-bearing RatsTumor Growth, Gluconeogenesis, and Body Composition in Parenteral Level of Glucose Intake on Glucose Homeostasis,
Updated version
http://cancerres.aacrjournals.org/content/43/11/5228
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/43/11/5228To request permission to re-use all or part of this article, use this link
on March 11, 2020. © 1983 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from