Embed Size (px)
Citation preview

A review of Parry-Romberg syndrome
Jessica El-Kehdy, MD, Ossama Abbas, MD, and Nelly Rubeiz, MD
Beirut, Lebanon
From
Fund
Conf
Acce
Repr
A
PO
Parry-Romberg syndrome, also known as progressive hemifacial atrophy, is a rare disorder characterizedby unilateral facial atrophy affecting the skin, subcutaneous tissue, muscles, and sometimes extending tothe osteocartilaginous structures. It has been associated with various systemic manifestations, particularlyneurologic, ophthalmologic and maxillofacial. In this article, we review Parry-Romberg syndrome with itsassociated findings (neurologic, ophthalmologic, cardiac, rheumatologic, endocrinologic, infectious,orthodontic and maxillofacial, and autoimmune), underlying cause, differential diagnoses (en coup desabre, scleroderma, and Rasmussen encephalitis), and therapeutic options. ( J Am Acad Dermatol2012;67:769-84.)
Key words: en coup de sabre; morphea; Parry-Romberg; progressive hemifacial atrophy; Rasmussenencephalitis; scleroderma.
Abbreviations used:
CT: computerized tomographyLSCS: linear scleroderma en coup de sabreMRI: magnetic resonance imagingPHA: progressive hemifacial atrophyPRS: Parry-Romberg syndromeRE: Rasmussen encephalitis
Parry-Romberg syndrome (PRS) is an infre-quent, acquired disorder characterized byprogressive hemiatrophy of the skin and soft
tissue of the face and, in some cases, results inatrophy of muscles, cartilage, and the underlyingbony structures.1,2 It was first described by Parry in1825 and Romberg in 1846.3,4 However, it was notuntil 1871 that Eulenberg gave the disease its currentnomenclature: progressive hemifacial atrophy(PHA).5
PRS slowly progresses over 2 to 20 years beforestabilizing.1-9 It is typically restricted to one half ofthe face but occasionally involves the arm, trunk, andleg.2,10-12 Bilateral progressive atrophies have beendescribed13-17; however, some references classifythem under the Barraquer-Simons syndrome ratherthan PRS.18
PRS usually begins in the first decade of life,1,2,19,20
although some cases with a late onset have beendescribed.10,21 It is more common in females,10,22-24
and is believed to be sporadic, although some rarefamilial cases have been reported.25-28
CUTANEOUS MANIFESTATIONS,PATHOLOGY, AND DERMATOLOGICASSOCIATIONS
Commonly affecting dermatomes of one or mul-tiple branches of the trigeminal nerve, PRS is
the American University of Beirut Medical Center.
ing sources: None.
licts of interest: None declared.
pted for publication January 27, 2012.
int requests: Nelly Rubeiz, MD, Department of Dermatology,
merican University of Beirut Medical Center, Riad El Solh St,
Box 11-0236, Beirut, Lebanon. E-mail: [email protected].
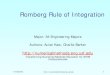
clinically characterized by mostly unilateral facialatrophy of the skin, soft tissues, muscles, and under-lying bony structures that may be preceded bycutaneous induration.1,2 Skin discoloration (eg, hy-perpigmentation or depigmentation) and cicatricialalopecia may also be observed in the affected areas.Intraoral involvement with tongue hemiatrophy mayoccur. There is progressive shrinking and deforma-tion of one side of the face, resulting in unilateralfacial atrophy, ipsilateral enophthalmos, and devia-tion of the mouth and nose toward the affected side(Fig 1). The final degree of deformity may depend onthe duration of the disease. The condition affects notonly the aesthetic, but also the functionality of theface.
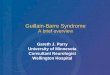
Histopathological examination of affected PRSskin usually reveals atrophy of the epidermis, der-mis, subcutaneous tissue, skin adnexa, vessels, and/or hair follicles,24,29,30 and skin fibrosis with collagen
Published online March 9, 2012.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2012.01.019
769

J AM ACAD DERMATOL
OCTOBER 2012770 El-Kehdy, Abbas, and Rubeiz
fiber thickening and skin edema29 (Fig 2).Inflammation in the form of lymphocytic infiltratesis variably present.8,24,29,30 Degenerative alterationsof vascular endothelia have been identified on elec-tron microscopy.24
PRS has been associated with bandlike alopecia,31
homolateral segmental vitiligo,32 hyperpigmenta-
CAPSULE SUMMARY
d Parry-Romberg syndrome is a raredisorder characterized by unilateral facialatrophy affecting the skin, subcutaneoustissue, muscles, and sometimesextending to the osteocartilaginousstructures in addition to variousassociated systemic manifestations.
d There is a close relationship betweenParry-Romberg syndrome and linearscleroderma en coup de sabre.
d This review provides an overview of theclinical picture of Parry-Rombergsyndrome, underlying cause, and currenttreatment options.
tion,20,33 port-wine stain,14
Klippel-Tr�enaunay syn-drome,14 lupus profundus,34
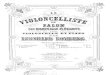
morphea,35-37 and linear scle-roderma en coup de sabre(LSCS) (Fig 3)14,16,28,38-44
(Table I).
ORIGINThe pathogenesis of PRS
is not well understood andseems to be heterogeneous;trauma, infection, cranialvascular malformation, im-mune-mediated processes,disturbance of fat metab-olism, and sympatheticdysfunction have beenproposed.
Trauma has been hypoth-
esized to be at the origin of PRS in 24% to 34% ofpatients,45,46 whether accidental traumas,47 opera-tive traumas such as thyroidectomy or dental avul-sion,48 or obstetric traumas such as forceps orvacuum maneuvers.18PHA as a manifestation of scleroderma has alsobeen proposed because of their similar histology andfrequent coexistence in the same subjects.41,48-50
Occasional PRS cases are familial and point to agenetic predisposition.25-28,49 Some authors havesuggested the mode of inheritance to be autosomaldominant with incomplete penetrance.51
The autoimmune hypothesis is based on thefrequent association of PRS with autoimmune dis-eases.18 Moreover, the occasional finding of autoan-tibodies41,52-55 such as antinuclear antibodies,1,2,28,53
antidouble-stranded DNA,54 anticentromere anti-bodies,53 antihistone antibodies,53 anticardiolipinantibodies,1 rheumatoid factor,53 and cerebrospinalfluid oligoclonal bands1 in the sera of patients withPRS would support this hypothesis.
Infections by slow viruses or bacteria have alsobeen hypothesized as a possible causative factor inPRS,56 although no organism could be extractedfrom the cerebrocerebellar tissue.18 Among the or-ganisms are herpes and Borrelia burgdorferi (Lymedisease),57 although their causality is questioned.29,58
Associated general infectious processes such as
otitis, dental infections, diphtheria, syphilis, rubella,and tuberculosis have also been noted.18,59,60
The association of hemifacial atrophy with benigntumors such as orbital neuromas, mandibular odon-togenic fibromas, and hamartomas, along with mi-graine and intracranial aneurysms has raised thepossibility of a neural crest migration disorder, from
which craniofacial cartilageand bone, smooth muscles,frontonasal masses, and cra-nial vessels take origin.18,61
The coexistence of PRSand paroxysmal kinesigenicdyskinesia, a movement dis-order thought to be theresult of a channelopathy,had the authors hypothesizea common mechanism toboth diseases through achannelopathy.62
The facial atrophy, lipo-dystrophy, and dienceph-alic tissue melting wasalso attributed to a meta-bolic disorder affecting theadipose tissues, probablyhyperthyroidism.49,63
Hyperactivity of the brain stem center has alsobeen suggested to be a cause of PRS.64
Trophic malformation of the cervical sympathetictrunk leading to sympathetic dysfunction is thoughtto play a pathogenic role in PHA.48 This hypothesishas found some confirmation because ablation of thesuperior cervical ganglion in animals has reproducedthe principal clinical manifestations of PHA: hemifa-cial atrophy, enophthalmos, and bone atrophy onthe side of the sympathectomy.47,48,60 Nevertheless,although some patients have clear evidence of con-comitant autonomic dysfunction such as ipsilateralHorner syndrome,41,65 others give completely nor-mal responses to standard autonomic function test-ing.48 Finally, many authors have, in fact, suggestedthat sympathetic irritation leads to facial hemiatro-phy, and, as a result, sympathectomy would and has,in some cases, halted the progression of the facialatrophy.66
Whatever the origin of PHA, there is evidence thatthis disorder has been present for more than 2000years. Indeed, in a study of 200 mummy portraitspainted in color at the beginning of the first millen-nium, two were found to have the disease.67 Thediagnosis was based on facial features suggestinglocalized atrophy of the skin and subcutaneoustissues. Three-dimensional computerized tomogra-phy (CT) of the skull also revealed atrophy of the

Fig 2. Histology of Parry-Romberg syndrome reveals epidermal atrophy, dermal sclerosis,entrapment of eccrine coils, and sparse inflammatory infiltrate. Findings are similar to thoseseen in scleroderma. (A and B, Hematoxylin-eosin stain; original magnifications: A, 3100; B,3200.)
Fig 1. A and B, Patient with Parry-Romberg syndrome. (Photographs courtesy of Dr ShukrallahZaynoun.)
J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 771
underlying bony structures and a smaller ipsilateralorbit, attesting to the asymmetry of facial bones andconfirming the diagnosis.
SYSTEMIC ASSOCIATIONSPRS has also been linked with neurologic, oph-
thalmologic, cardiac, rheumatologic, infectious,endocrine, maxillofacial, and orthodontic manifes-tations. It has also been associated with autoimmunediseases, congenital diseases, and pregnancy(Table I).
Neurologic manifestationsClinical manifestations. Given that the most
frequent systemic manifestations associated withPRS are neurologic (affecting around 15% of thePRS population), some authors have proposed thatPRS be regarded as a neurocutaneous syndrome.68,69
Seizures are the most common neurologic manifes-tation.10,16,38,69-76 Other associations include mi-graines,10,61,77 that sometimes lead tohemiplegia,78,79 aneurysms,61,80-83 brain atro-phy,38,71,74,75,84 limb atrophy,2,10,11,85 intracranialvascular malformations, and others (Table II).86-97
Imaging, other diagnostic modalities, andtherapy. CT and magnetic resonance imaging(MRI) are the two most common modalities used inthe diagnosis of the neurologic manifestations inPRS.29 In some cases, abnormalities are detectedyears after the onset of cutaneous lesions.98
A common MRI finding is ipsilateral white-matterhigh signal intensity,1,30,69,99-101 with occasionalhyperintensities in the gray matter as well.69 CranialCT and MRI findings in patients with PRS andneurologic disease are usually ipsilat-eral,30,69,90,102,103 supporting the theory that these

Fig 3. Patient with en coup de sabre morphea (A and C) and hemifacial atrophy on left side(B). (Photographs courtesy of Dr Shukrallah Zaynoun.)
J AM ACAD DERMATOL
OCTOBER 2012772 El-Kehdy, Abbas, and Rubeiz
neurologic manifestations may be directly linked tothe cutaneous disease.14 However, contralateral find-ings on imaging have also been documented.102
Other findings are listed in Table II.104-109
Histopathologic findings of brain specimens andtreatment options are listed in Table II.56,76,106,110-112
Ophthalmologic manifestationsClinical manifestations. PRS has been associ-
ated with multiple ophthalmologic manifestations.The most common are enophthalmos,87,113-117
uveitis,113,118-120 retinal vasculitis,118,120,121 ipsilateral16
and contralateral13,65,119 third nerve paresis, glau-coma,119,122,123 and eyelid atrophy (Table III).41,115,124
Other findings are listed in Table III.124-135
Imaging, other diagnostic modalities, andtherapy. Few reports have discussed the resultsobtained on imaging and pathology of the ophthal-mologic manifestations.85,116,121,133,136 As for treat-ment, few were reported to have improved theophthalmologic symptoms, except for Disuloneused in the treatment of a patient with bilateralpapillitis and contralateral nerve palsy, whichshowed no improvement.65
Maxillofacial and orthodontic manifestationsClinical manifestations. Mandibular and teeth
involvement are common in PRS.137-140 Accordingto some sources, teeth anomalies help to identifythe age of onset of PRS.18 Communication

Table
I.Derm
atologic,cardiologic,endocrinologic,infectious,au
toim
mune,congenital,andacquiredconditionsassociatedwithParry-Romberg
syndrome
Derm
atologic
manifestations
Card
iologic
manifestations
Endocrinologic
manifestations
Infectiousmanifestations
Autoim
munemanifestations
Congenitaldisease
manifestations
Pregnancy10,122,123
Ban
dlikealopecia3
1
Homolateralsegmental
vitilig
o32
Hyp
erpigmentation20,33
Port-w
inestain14
Klip
pel-Tr� en
aunay
syndrome14
Raynau
dphenomenon36
Lupusprofundus3
4
Morphea3
5-37
Linear
scleroderm
aen
coupde
sabre
8,14,16,43,44
Hyp
ertrophic
cardiomyo
pathy1
85
Hyp
erthyroidism
63
Hyp
othyroidism
38
Lipodystrophy1
4
Borrelio
sis(Borrelia
burgdorferi)14,57,186-189
Herpes1
8
Generalinfectious
processes1
8,59,60:
Otitis
Dentalinfection
Diphtheria
Syphilis
Rubella
Tuberculosis
Hashim
oto
thyroiditis63
Grave
disease63
Primarybiliarycirrhosis1
8
Vitiligo32
Inflam
matory
bowel
disease10
Rheumatoid
arthritis1
0
Ankylosingspondylitis10
Multiple
sclerosis1
0
Sj€ ogrendisease18
Autoim
munehemolytic
anemia18
Lupuserythematosus1
8
Scleroderm
a14,16,28,43,44
ContralateralPoland
syndrome190
Congenital
lowerlim
bhyp
oplasia1
91
Congenital
ipsilateral
cerebralatrophy8
2
Supernumerary
nipple18
Microphthalmia18
Congenital
torticollis1
8
Renal
malform
ation18
WorseningofPRS
duringpregnan
cyan
dafterdelivery
7
PRS,
Parry-Romberg
syndrome.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 773
disorders and dysphonia have also been reported(Table IV).141,142
Imaging, other diagnostic modalities, andtreatment. Cone beam CT, along with the mirrorimage of the unaffected side superimposed on theaffected side, were found to be very helpful inmaking clear linear, angular, and volumetric mea-surements and assess the degree of asymmetry,giving the orthodontist insight to the therapeuticpossibilities.143 Orthodontic rehabilitation144 and theuse of prophylactic orthodontic appliances weredescribed with good results.145
DIFFERENTIAL DIAGNOSISLinear scleroderma en coup de sabre
LSCS is a variant of localized scleroderma of theface and skull.88,146 It presents as an area of mixedhypopigmented and hyperpigmented skin overlyingthe frontoparietal area, usually unilateral, restrictedto the forehead, and associated with a deep para-median forehead scar separating atrophic from nor-mal tissue (Fig 4). It is often preceded by indurationof the skin.2,42 Scarring alopecia may be present onthe affected side.88 The disease usually starts inchildhood and predominantly affects females.14,147
The clinical course is slow and progressive over 2 to20 years, after which it becomes stable.88 Neurologicand ophthalmologic complications have been re-ported.148-150 The origin of LSCS remains unclear;however, autoimmunity, disturbed peripheral sym-pathetic nervous system, disturbed trigeminal nerve,and early cerebral inflammation have all beenproposed.64,101,146
Differentiating PRS from LSCS is very challeng-ing.2 Indeed, both diseases have a similar age ofonset (mean age of 11 years), predominantly affectwomen, and present as lesions that progressover time until they reach stability few yearslater.147 Moreover, both disorders have comparableneurologic and ophthalmologic findings,147 andboth may respond to immunosuppressive treat-ment.76,112,151,152 Furthermore, both conditions mayshow overlap or transition14,17,28,43,44,58; althoughLSCS and PRS were found to coexist in manypatients,153-156 some have described patients withLSCS converting with time to PHA (Fig 4).155,157 Theprevalence of LSCS in conjunction with PRS isuncertain, but has been reported to range from36.6% to 53.6%.14,58
There are no definite criteria generally agreedupon to differentiate PRS from linear scleroderma.88
The most accepted differentiating factors cited inthe literature are the presence or absence of inflam-mation/induration, the site affected, and the severityof atrophy.12,40,42 Duymaz et al2 have come up with

Table II. Neurologic Parry-Romberg syndrome associations, diagnostic features, pathology, and therapy
Neurologic manifestations Imaging and diagnostic modalities Pathology Therapy
Seizure10,16,38,69-76
Migraine10,61,77
Hemiplegia78,79,89
Aneurysm61,80-83
Brain atrophy (cerebellar, congenitalipsilateral cerebral, progressive cerebral,hemiatrophy of brain)38,71,74,75,84
Limb atrophy (contralateral, ipsilateral)2,10,11,85
Intracranial vascular malformations (left andright internal carotid, middle cerebral,anterior cerebral, posteriorcommunicating, posterior cerebral,vertebral arteries)86,87
Status migrainosus88
Headaches78
Facial pain10,90
Cerebral microhemorrhage91
Paroxysmal kinesigenic dyskinesia62
Rasmussen syndrome92
Trigeminal neuralgia77,90,93
Cystic leukoencephalopathy72
Dura matter atrophy72
Subdural hygroma73
Torticollis94
Syringomyelia95
Sympathetic hyperactivity77,96
Cerebellar syndrome74
Agenesis of head of caudate nucleus27
Trunk atrophy2,10
Amnesic aphasia89
Mental retardation89
Unilateral alien hand syndrome97
Mandibular cramps93
Bilateral pyramidal tract involvement89
Hemianesthesia70
Oculomotor nerve palsy16
Facial nerve palsy16
CT and MRIIpsilateral white-matter high signal
intensity1,30,69,99,100
Hyperintensities in gray matter69
Mild cortical thickening30,42
Leptomeningeal enhancement30,69
Dense mineral deposition orcalcification30,69,102-104
Intracerebral atrophy19,30,38,69,71,74,75,84,99
Dilatation of lateral ventricles69
Microscopic vascular malformations68,86,87
Hamartomas105
Homolateral porencephaly30
Unilateral focal corpus callosum infarctions30
Loss of cortical gyration69
Gyral enhancement42
Meningocortical dysmorphism30
Ipsilateral infarcts in amygdaloid body30
Ipsilateral meningeal and basal ganglialesions106
Ipsilateral contrast hypercaptation75
Diffusion tensor imaging and fibertractography
Fiber derangement, especially in sensorytract of cerebral white matter108
ElectroencephalogramLentification75
Depression75
Slowing of frontal lobe conduction14
Slowing of facial velocity conduction75
Ipsilateral multifocal sharp waves19
Frontal, temporal and frontotemporaldischarges14
Generalized abnormalities14
Single-photon emission tomographyIncreased perfusion in cortex of affected
hemisphere100
Leptomeningeal fibrosis56,110
Degenerative cortical changes56,110
Microvascular malformations56,110
Ipsilateral gray- and white-matterperivascular lymphocytic infiltration, withpial and glial proliferation49
Small groups of ectopic cells, neuronal loss,gliosis, activated microglial cells, synapseformation in dentate gyrusein patientwith temporal lobe resection forintractable seizures111
Immunosuppressive drugs79,112
Prednisone and methotrexate106
Antiepileptic therapy76
Surgery111
JAM
ACADD
ERM
ATOL
OCTOBER20
12774
El-K
ehdy,
Abbas,andRubeiz

Central
nervoussystem
tumor29
Cortical
depression75
Fatalbrain
stem
invo
lvement71
Hyp
eractivityofbrain
stem
center64
Blinkreflexandtrigeminalevoked
potential
Abnorm
alitiesin
brain
stem
109
Cerebralangiography
Ipsilateralintracranialan
eurysm
s61,81-83
Ipsilateralarteriovenousfistulas8
3
Ipsilateralreversible
vesselcalib
erchan
ges7
9
CT,
Computerizedtomography;
MRI,mag
neticresonan
ceim
aging.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 775
an oversimplified guideline to distinguish the twodiseases. They suggest that the diagnosis of PRSshould be made if the patient presents with aunilateral atrophy involving the entire side of theface, usually deeper and less bound down than theone in LSCS, with absent or minimal precedingsigns of inflammation or induration.2 The overlyingskin is usually thin and soft, with normal hair andabsent sclerosis. Unilateral dysplasia of underlyingbone, skull, tongue, gingival, and palate could bepresent.42 As for LSCS, they propose that the diag-nosis should be based on the presence of a unilat-eral bandlike sclerotic scar with hyperpigmentationon the frontoparietal area, restricted to the areaabove the eyebrow and most often preceded byinduration of the skin.2 Cutaneous sclerosis in theform of hard, depressed, hyperpigmented, shiny,and hairless skin is usually present. Progressivesoftening of the lesions would take place overtime.42
There is still considerable debate over the rela-tionship between LSCS and PRS, with some authorsbelieving that they are separate entities, whereasothers endorse that progressive facial hemiatrophy isa form of scleroderma,66,104,147 part of a spectrumranging from linear scleroderma through PRS tosystemic sclerosis.10,40,42,108,155,156
The most frequently cited associations with LSCSare, as with PRS, neurologic and ophthal-mic.2,42,148-150 However, compared with patientswith LSCS, more patients with PRS have beenreported with neurologic findings.88 The most com-mon neurologic symptoms reported in LSCS are, asfor PRS, seizures.10,42,88,156-159 Headache has alsobeen reported.42,88 Findings on brain MRI in patientswith LSCS are also similar to patients with PRS,consisting of ipsilateral intracerebral calcifica-tions,160,161 ipsilateral hyperintense intracerebral le-sions,162 and occasional contralateral frontal brainlesions.150
Rasmussen syndromeRasmussen encephalitis (RE) is a rare, chronic
inflammatory disease, presenting as progressive fo-cal cortical inflammation and tissue destruction usu-ally involving a single brain hemisphere.1,42 REgenerally begins in the first decade of life, with rarereported onset in adolescence and early adulthood.Neurologic symptoms include intractable seizures,progressive hemiplegia, and mental deterioration,that patients usually experience over the first 8 to 12months, before entering a phase of deficient, butstable, neurologic state.1 Its origin is yet unclear;however, autoimmunity and viral infections such as

Table III. Ophthalmologic Parry-Romberg syndrome associations, diagnostic features, pathology, and therapy
Ophthalmologic manifestations Imaging and diagnostic features Pathology Therapy
Enophthalmos87,113-117
Uveitis14,118-120
Retinal vasculitis118-120
Third nerve paresis (ipsilateral,contralateral)13,16,65,119
Glaucoma119,122,123
Eyelid atrophy41,115,124
Amblyopia94 leading to progressive visualloss when anisometropic125
Exotropia94
Hypotropia126
Esotropia126
Increase in pre-existing hyperopia119
Diplopia127
Restrictive strabismus119
Cataract119
Miosis41
Retinal pigment changes13,119
Chorioretinal lesions128
Extraocular muscle thinning116
Contralateral extraocular muscleimpairment129
Eyelid alterations (upper eyelidretraction)113,130
Decreased corneal sensitivity114
Band keratopathy114
Loss of cilia38,115
Papillitis65,113
Episcleritis114
Bilateral vitreitis 115
Iridocyclitis87
Neuroretinitis115,131
Retinal telangiectasis116,132
Orbital neurinomas105
Phthisis bulbi86
Pseudoptosis132
Profound ocular hypotony133
Nocturnal lagophthalmos130
Blepharoptosis70
OCT angiographyIn patient with vitreoretinal interface
abnormality:Retinal nerve, fiber layer edema, diffuse
retinal edema136
Fluorescein angiographyIn patient with vitreoretinal interface
abnormality:Optic disc swelling, engorgement of retinal
vessels, mottling of pigmentepithelium136
In patient with enophthalmous andhyperopia:
Telangiectasis116
Ultrasound biomicroscopyIpsilateral ciliary muscle inflammation133
EchographyIn patient with enophthalmous and
hyperopia:Shrinkage of eyeball, thinning of extraocular
muscles, telangiectasis116
Right temporalis muscle biopsy and needleelectromyography of masseter muscle
In patient with retinal vasculitis:Large fibrosis with focal lymphohistiocytic
infiltration of muscle fibers121
Anterior orbital fat and lacrimal glandbiopsy
In patient with iridocyclitis:Fibrosis and chronic inflammation87
Immunosuppressive therapy121
Steroids113,115
Cyclosporine A132
Disulone65
Laser therapy121,132
Dissimilar trifocals117
Orbital floor implants132
Recession of levator muscle130
JAM
ACADD
ERM
ATOL
OCTOBER20
12776
El-K
ehdy,
Abbas,andRubeiz

Lightstainingofretina1
16
Shrinkageofeyeball116
Retinal
detachment124
Corneal
exp
osure
130
Blin
dness
119,120
Adie
pupil6
9
Coat
syndrome124,134
Duan
eretractionsyndrome135
Fuchssyndrome
65
Hornersyndrome41,65
OCT,
Opticalcoherence
tomography.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 777
Epstein-Barr virus, cytomegalovirus, and herpeshave been suggested.1
CT scan findings in RE are often normal in theearly stages.1 In the active phase of the disease,however, MRI shows sporadic, patchy gyriformcortico-pial enhancement and areas of unilateralhyperintensity corresponding to cytotoxic edema.Ipsilateral brain atrophy occurs afterward.
RE and PRS were found to coexist, however veryrarely.92 Nevertheless, in some patients with PRS andneurologic symptoms, RE was considered in thedifferential diagnosis.19,42 Indeed, according to somereports, these two disorders would share a commonautoimmune cause given the presence of autoanti-bodies and the reaction to immunosuppressive ther-apies.42 Moreover, their similar neurologic findings,unilateral involvement, early onset, and stabilizationof the disease over time render them quite similarand would explain the diagnostic confusion.
TREATMENTTreatment of PRS aims first at halting the disease
process and improving some symptoms of the dis-ease. Immunosuppressive drugsmight be consideredin some patients especially in the case of cerebralinvolvement (TableV).14,29,79,112Once thediseasehasstabilized, aesthetic treatments of the hemifacial atro-phy consisting of augmentation of the atrophic regionand restoration of the symmetry of the face can beinitiated with a recommended pause of 1 to 2 yearsbefore proceeding with the reconstruction.1,29,163
These consist of single therapies for facial recontour-ing or volumetric regeneration and combined thera-pies.163-184 The latter are considered by somesurgeons to be the mainstay of treatments for facialatrophy.179,180 However, some authors suggest theuse of either single or combined therapies accordingto the severity of the atrophy.184Whatever the option,these treatment modalities resolve only momentarilythe good appearance, and are lost in time as a result ofgravity, and the patient would need a newintervention.20
CONCLUSIONIn conclusion, PRS, although rare, has been
reported in the literature quite abundantly, and hasbeen associated with multiple findings. The treat-ment options offered in the literature for both diseaseprogression and cosmetic appearance are diversebut not curative. Althoughmany theories concerningits origin have been proposed, none has beenuniversally accepted. A close relationship existsbetween PRS and LSCS; PRS appears to belong tothe broad spectrum of scleroderma.

Table IV. Maxillofacial and orthodontic associations, diagnostic features, and therapy
Maxillofacial and orthodontic
manifestations Imaging and diagnostic modalities Therapy
Mandibular odontogenousfibroma105
Odontogenic cyst137
Odontoma of mandible138
Teeth involvementRoot resorption139,140
Delayed eruption140
Dilaceration140
Ipsilateral reduction in heightand width of mandible140
Communication disorders141
Dysphonia
RadiographyMandible and teeth anomaliesCone beam computerized tomography and mirror image of
unaffected side superimposed on affected side143
/ Make clear linear, angular, and volumetric measurements/ Assess degree of asymmetry
Orthodonticrehabilitation144
Prophylactic orthodonticappliances145
Fig 4. A and B, Patients with linear scleroderma en coup de sabre. (Photographs courtesy of DrShukrallah Zaynoun.)
J AM ACAD DERMATOL
OCTOBER 2012778 El-Kehdy, Abbas, and Rubeiz
REFERENCES
1. Longo D, Paonessa A, Specchio N, Delfino LN, Claps D, Fusco
L, et al. Parry-Romberg syndrome and Rasmussen encepha-
litis: possible association; clinical and neuroimaging features.
J Neuroimaging 2009;20:1-6.
2. Duymaz A, Karabekmez FE, Keskin M, Tosun Z. Parry-Rom-
berg syndrome: facial atrophy and its relationship with other
regions of the body. Ann Plast Surg 2009;63:457-61.
3. Parry CH. Collections from the unpublished medical writings
of the late Caleb Hillier Parry. London: Underwoods; 1825;
478-80.
4. Romberg HM. Krankheiten des nervensystems (IV: Tropho-
neurosen) (in German). Klinische Ergebnisse. Berlin: Forrtner;
1846; 75-81.
5. Eulenberg A. Hemiatrophia facialis progressiva (in German).
Lehrbuch der functionellen nervenkrankheiten auf physiolo-
gischer basis. Berlin: Verlag von August Hirschwald; 1871;
712-26.
6. Mazzeo N, Fisher JG, Mayer MH, Mathieu GP. Progressive
hemifacial atrophy (Parry-Romberg syndrome). Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 1995;79:30-5.
7. Moore MH, Wong KS, Proudman TW, David DJ. Progressive
hemifacial atrophy (Romberg’s disease): skeletal involvement
and treatment. Br J Plast Surg 1993;46:39-44.
8. Neville BW, Damm DD, Allen CN, Bouquout JE, editors.
Patologia oral e Maxilofacial. Rio de Janeiro: Guanabara
Koogan; 1998. p. 35.
9. Roddi R, Riggio E, Gilbert PM, Hovius SE, Vaandrager JM, van
der Meulen JC. Clinical evaluation of techniques used in the
surgical treatment of progressive hemifacial atrophy.
J Craniomaxillofac Surg 1994;22:23-32.
10. Stone J. Parry-Romberg syndrome: a global survey of 205
patients using the Internet. Neurology 2003;61:674-6.
11. Chapman MS, Peraza JE, Spencer SK. Parry-Romberg syn-
drome with contralateral and ipsilateral extremity involve-
ment. J Cutan Med Surg 1999;3:260-2.
12. Rees TD. Facial atrophy. Clin Plast Surg 1976;3:637-46.
13. Miller MT, Sloane H, Goldberg MF, Grisolano J, Frenkel
M, Mafee MF. Progressive hemifacial atrophy (Parry-
Romberg disease). J Pediatr Ophthalmol Strabismus 1987;
24:27-36.
14. Tollefson MM, Witman PM. En coup de sabre morphea and
Parry-Romberg syndrome: a retrospective review of 54
patients. J Am Acad Dermatol 2007;56:257-63.
15. Rai R, Handa S, Gupta S, Kumar B. Bilateral en coup de
sabreea rare entity. Pediatr Dermatol 2000;17:222-4.
16. Gambichler T, Kreuter A, Hoffmann K, Bechara FG, Altmeyer
P, Jansen T. Bilateral linear scleroderma ‘‘en coup de sabre’’

Table V. Therapeutic options for Parry-Romberg syndrome
Systemic therapy Local therapy Single surgical procedure Combined surgical procedures
Procaine penicillin29
D-penicillamine14
Antimalarials(hydroxychloroquine)14,29
Corticosteroids14,29,112
Vitamin E14
Retinoids29
Cyclosporine29
Tetracycline14
Cyclophosphamide29,112
Methotrexate14,29,112
Methotrexate 1pulse oral steroids14
Emollients29
Vitamin D analog29
Vitamin D analog 1PUVA14
Topical steroids14
Botulinum toxininjections14
Phototherapy29,188
Facial reconstructionLipofilling165,184
Polyethylene implant165
Medpor implant166
Cell-assisted lipotransfer169
Flaps and graftsMicrosurgical tissue transfer with
free anterolateral thighfascioadipose flap174
Pedicled superficial temporalfascia sandwich flap175
Perforator-based anterolateralthigh flaps176
Vascularized serratus anteriormuscle flap177
Free vascular parascapulargraft113
Thoracodorsal flaps178
Free groin flaps166
Composite galeal frontalis flap172
Volume regenerationAutologous fat
transplantation169-171
Expandedpolytetrafluoroethylene167
Poly-L-lactic acid168
Poly-L-lactic acid 1 lipofilling 1intense pulse light therapy181
Superficial temporal fascial flap1 lipofilling163
Revascularized free flap(anterolateral thighadipofascial flaps or latissimusdorsi flaps) 1 dermisgrafting179
Revascularized free flap(anterolateral thighadipofascial flaps or latissimusdorsi flaps) 1 lipoinjection179
Revascularized free flap(anterolateral thighadipofascial flaps or latissimusdorsi flaps) 1 Medporimplant (Porex Surgical/Stryker Corporation, Newman,GA)179
Revascularized free flap(anterolateral thighadipofascial flaps or latissimusdorsi flaps) 1 genioplasty179
Revascularized free flap(anterolateral thighadipofascial flaps or latissimusdorsi flaps) 1 liposuctionrevision179
Coleman lipoinjection 1 de-epithelialized freeparascapular flap transfer180
Coleman lipoinjection 1polyglactic acid182
Coleman lipoinjection 1 bloodplatelet gel183
Lipoinjection 1 galeal flaps 1free dermis-fat grafts 1 boneand cartilage grafts184
PUVA, Psoralen plus ultraviolet A.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 779
associated with facial atrophy and neurological complica-
tions. BMC Dermatol 2001;1:9.
17. Dilley JJ, Perry HO. Bilateral linear scleroderma en coup de
sabre. Arch Dermatol 1968;97:688-9.
18. Ruhin B, Bennaceur S, Verecke F, Louafi S, Seddiki B, Ferri J.
Progressive hemifacial atrophy in the young patient: physi-
opathologic hypotheses, diagnosis and therapy. Rev Stoma-
tol Chir Maxillofac 2000;101:287-97.
19. Carre~no M, Donaire A, Barcel�o MI, Rumi�a J, Falip M. Parry
Romberg syndrome and linear scleroderma in coup de sabre
mimicking Rasmussen encephalitis. Neurology 2007;68:
1308-10.
20. Pinheiro TP, Silva CC, Silveira CS, Botelho PC, Pinheiro MG.
Progressive hemifacial atrophyecase report. Med Oral Patol
Oral Cir Bucal 2006;11:E112-4.
21. Mendonca J, Viana SL, Freitas F, Lima G. Late-onset progress-
ive facial hemiatrophy (Parry-Romberg syndrome). J Postgrad
Med 2005;51:135-6.
22. Jurkiewicz MJ, Nahai F. The use of free revascularized grafts
in the amelioration of hemifacial atrophy. Plast Reconstr Surg
1985;76:44-55.
23. Finesilver B, RosowHN. Total hemiatrophy. JAMA1938;5:366-8.
24. Pensler JM, Murphy GF, Muliken JB. Clinical and
ultra-structural studies of Romberg’s hemifacial atrophy.
Plast Reconstr Surg 1990;85:669-76.
25. Anderson PJ, Molony D, Haan E, David DJ. Familial
Parry-Romberg disease. Int J Pediatr Otorhinolaryngol 2005;
69:705-8.
26. Ignatowicz R, Micha1owicz R, Kmie�c T, J�o�zwiak S. Familial
form of Parry-Romberg syndrome. Pol Tyg Lek 1985;40:47-9.

J AM ACAD DERMATOL
OCTOBER 2012780 El-Kehdy, Abbas, and Rubeiz
27. Le€ao M, da Silva ML. Progressive hemifacial atrophy with
agenesis of the head of the caudate nucleus. J Med Genet
1994;31:969-71.
28. Lewkonia RM, Lowry RB. Progressive hemifacial atrophy
(Parry-Romberg syndrome) report with review of genetics
and nosology. Am J Med Genet 1983;14:385-90.
29. Bergler-Czop B, Lis-Swiety A, Brzezi�nska-Wcis1o L. Sclero-
derma linearis: hemiatrophia faciei progressiva (Parry-Rom-
berg syndrome) without any changes in CNS and linear
scleroderma ‘‘en coup de sabre’’ with CNS tumor. BMC
Neurol 2009;9:39.
30. Cory RC, Clayman DA, Faillace WJ, McKee SW, Gama CH.
Clinical and radiologic findings in progressive facial hemiat-
rophy (Parry-Romberg syndrome). AJNR Am J Neuroradiol
1997;18:751-7.
31. Thapa R, Ghosh A, Dhar S. Parry-Romberg syndrome with
band-like alopecia. Indian J Pediatr 2009;76:760.
32. Creus L, Sanchez-Rega~na M, Salleras M, Chaussade V, Umbert
P. Parry-Romberg syndrome associated with homolateral
segmental vitiligo. Ann Dermatol Venereol 1994;121:710-1.
33. Moseley BD, Burrus TM, Mason TG, Shin C. Contralateral
cutaneous and MRI findings in a patient with
Parry-Romberg syndrome. J Neurol Neurosurg Psychiatry
2010;81:1400-1.
34. Grossberg E, Scherschun L, Fivenson DP. Lupus profundus:
not a benign disease. Lupus 2001;10:514-6.
35. Lane TK, Cheung J, Schaffer JV. Parry-Romberg syndrome
with coexistent morphea. Dermatol Online J 2008;14:21.
36. Rischebieth RH. Progressive facial hemiatrophy (Parry-
Romberg syndrome). Proc Aust Assoc Neurol 1976;13:
109-12.
37. Al-Khenaizan S, Al-Watban L. Parry-Romberg syndrome:
overlap with linear morphea. Saudi Med J 2005;26:317-9.
38. Klene C, Massicot P, Ferri�ere-Fontan I, Sarlangue J, Fontan D,
Guillard JM. ‘‘Saber-cut’’ scleroderma and Parry-Romberg
facial hemiatrophy, nosologic problems, neurologic compli-
cations. Ann Pediatr (Paris) 1989;36:123-5.
39. Wakhlu A, Agarwal V, Aggarwal A, Misra R. Parry Romberg
syndrome: a close differential diagnosis of linear sclero-
derma en coup de sabre. J Assoc Physicians India 2003;51:
980.
40. Lehman TJ. The Parry Romberg syndrome of progressive
facial hemiatrophy and linear scleroderma en coup de sabre:
mistaken diagnosis or overlapping conditions? J Rheumatol
1992;19:844-5.
41. Auvinet C, Glacet-Bernard A, Coscas G, Cornelis P, Cadot M,
Meyringnac C. Parry-Romberg progressive facial hemiatrophy
and localized scleroderma: nosologic and pathogenic prob-
lems [in French]. J Fr Ophtalmol 1989;12:169-73.
42. Paprocka J, Jamroz E, Adamek D, Marszal E, Mandera M.
Difficulties in differentiation of Parry-Romberg syndrome,
unilateral facial sclerodermia, and Rasmussen syndrome.
Childs Nerv Syst 2006;22:409-15.
43. Slimani S, Hounas F, Ladjouze-Rezig A. Multiple linear scle-
rodermas with a diffuse Parry-Romberg syndrome. Joint
Bone Spine 2009;76:114-6.
44. Maletic J, Tsirka V, Ioannides P, Karacostas D, Taskos N.
Parry-Romberg syndrome associated with localized sclero-
derma. Case Rep Neurol 2010;2:57-62.
45. Asher SW, Berg BO. Progressive hemifacial atrophy: report of
three cases, including one observed over 43 years, and
computed tomographic findings. Arch Neurol 1982;39:44-6.
46. Delaire J, Lumineau JP, Mercier J, Plenier V. Romberg’s
syndrome: progressive facial hemiatrophy. Rev Stomatol
Chir Maxillofac 1983;84:313-21.
47. Claudy AL, Segault D, Rousset H, Moulin G. Facial hemiatro-
phy, homolateral cervical linear scleroderma and thyroid
disease. Ann Dermatol Venereol 1992;119:543-5.
48. Archambault L, Fromm NK. Progressive facial hemiatrophy;
report of three cases. Arch Neurol Psychiatry 1932;27:529-84.
49. Wartenberg R. Progressive facial hemiatrophy. Arch Neurol
Psychiatry 1945;54:75-96.
50. Lapresle J, Desi M. Scleroderma with progressive facial
hemiatrophy and atrophy of the other side of the body.
Rev Neurol (Paris) 1982;138:815-25.
51. Johnson RH, Spalding JMK. Disorders of the autonomic
nervous system. Oxford: Blackwell; 1974.
52. Kayanuma K, Oguchi K. A case of progressive hemifacial
atrophy associated with immunological abnormalities. Rin-
sho Shinkeigaku 1994;34:1058-60.
53. Garcia-de la Torre I, Castello-Sendra J, Esgleyes-Ribot T,
Martinez-Bonilla G, Guerrerosantos J, Fritzler MJ. Autoanti-
bodies in Parry-Romberg syndrome: a serologic study of 14
patients. J Rheumatol 1995;22:73-7.
54. Gonul M, Dogan B, Izci Y, Varol G. Parry-Romberg syndrome
in association with anti-dsDNA antibodies: a case report.
J Eur Acad Dermatol Venereol 2005;19:740-2.
55. Blaszczyk M, Jablonska S. Linear scleroderma en coup de
sabre: relationship with progressive facial hemiatrophy (PFH).
Adv Exp Med Biol 1999;455:101-4.
56. Wolf SM, Verity MA. Neurological complications of progress-
ive facial hemiatrophy. J Neurol Neurosurg Psychiatry 1974;
37:997-1004.
57. Sahin MT, Baris S, Karaman A. Parry-Romberg syndrome: a
possible association with borreliosis. J Eur Acad Dermatol
Venereol 2004;18:204-7.
58. Sommer A, Gambichler T, Bachrach-Buhles M, von Rothen-
burg T, Altmayer P, Kreuter A. Clinical and serological
characteristics of progressive facial hemiatrophy: a case of
12 patients. J Am Acad Dermatol 2006;54:227-33.
59. Stern HS, Elliott LF, Beegle PH Jr. Progressive hemifacial
atrophy associated with Lyme disease. Plast Reconstr Surg
1992;90:479-83.
60. Resende LA, Dal Pai V, Alves A. Experimental study of
progressive facial hemiatrophy: effects of cervical sympa-
thectomy in animals. Rev Neurol (Paris) 1991;147:609-11.
61. Pichiecchio A, Uggetti C, Grazia Egitto M, Zappoli F.
Parry-Romberg syndrome with migraine and intracranial
aneurysm. Neurology 2002;59:606-8.
62. Mrabet Khiari H, Masmoudi S, Mrabet A. Association of
Parry-Romberg syndrome and paroxysmal kinesigenic dyski-
nesia. Rev Neurol (Paris) 2009;165:489-92.
63. Decourt J, Aubry M, Blanchard J. Hemiatrophie faciale lingual
et velopalatine et maladie de Basedow associee. Revue
Neurol (Paris) 1941;34:135-40.
64. Lonchampt P, Emile J, P�elier-Cady MC, Cadou B, Barthelaix A.
Central sympathetic dysregulation and immunological ab-
normalities in a case of progressive facial hemiatrophy
(Parry-Romberg disease). Clin Auton Res 1995;5:199-204.
65. Garcher C, Humbert P, Bron A, Chirpaz L, Royer J. Optic
neuropathy and Parry-Romberg syndrome: apropos of a case
[in French]. J Fr Ophtalmol 1990;13:557-61.
66. Rogers BO. Progressive facial hemiatrophy: Romberg’s dis-
ease, a review of 772 cases. In: Broadbent TR, Anderson B.
Transactions of the third international congress of plastic
surgery. International congress series 66. Amsterdam: Ex-
cerpta Medica; 1963. p. 681-9.
67. Appenzeller O, Stevens JM, Kruszynski R, Walker S. Neurology
in ancient faces. J Neurol Neurosurg Psychiatry 2001;70:
524-9.

J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 781
68. Taylor HM, Robinson R, Cox T. Progressive facial hemiatro-
phy: MRI appearances. Dev Med Child Neurol 1997;39:484-6.
69. Aynaci FM, Sen Y, Erd€ol H, Ahmeto�glu A, Elmas R. Parry-
Romberg syndrome associated with Adie’s pupil and radio-
logic findings. Pediatr Neurol 2001;25:416-8.
70. Aktekin B, Oguz Y, Aydin H, Senol U. Cortical silent period in a
patient with focal epilepsy and Parry-Romberg syndrome.
Epilepsy Behav 2005;6:270-3.
71. Sathornsumetee S, Schanberg L, Rabinovich E, Lewis D Jr,
Weisleder P. Parry-Romberg syndrome with fatal brain stem
involvement. J Pediatr 2005;146:429-31.
72. Casta~neda-Reyna MA, Galarza-Manyavi C. Parry Romberg
syndrome associated with refractory epilepsy, atrophy of
the dura mater and cystic leukoencephalopathy. Rev Neurol
2003;37:941-5.
73. Sandhu K, Handa S. Subdural hygroma in a patient with
Parry-Romberg syndrome. Pediatr Dermatol 2004;21:48-50.
74. Speciali JG, Resende LA. Progressive facial hemiatrophy:
report of a case. Arq Neuropsiquiatr 1984;42:166-70.
75. Duro LA, de Lima JM, dos Reis MM, da Silva CV. Progressive
hemifacial atrophy (Parry-Romberg disease): study of a case.
Arq Neuropsiquiatr 1982;40:193-200.
76. Yano T, Sawaishi Y, Toyono M, Takaku I, Takada G. Progress-
ive facial hemiatrophy after epileptic seizures. Pediatr Neurol
2000;23:164-6.
77. Drummond PD, Hassard S, Finch PM. Trigeminal neuralgia,
migraine and sympathetic hyperactivity in a patient with
Parry-Romberg syndrome. Cephalalgia 2006;26:1146-9.
78. Ong B, Chong PN, Yeo PP. Progressive hemifacial atrophyea
report of 2 cases. Singapore Med J 1990;31:497-9.
79. Woolfenden AR, Tong DC, Norbash AM, Albers GW. Progress-
ive facial hemiatrophy: abnormality of intracranial vascula-
ture. Neurology 1998;50:1915-7.
80. Aoki T, Tashiro Y, Fujita K, Kajiwara M. Parry-Romberg
syndrome with a giant internal carotid artery aneurysm.
Surg Neurol 2006;65:170-3.
81. Bosman T, Van Bei Jnum J, Van Walderveen MA, Brouwer PA.
Giant intracranial aneurysm in a ten-year-old boy with
Parry-Romberg syndrome: a case report and literature re-
view. Interv Neuroradiol 2009;15:165-73.
82. Catala M. Progressive intracranial aneurysmal disease in a
child with progressive hemifacial atrophy (Parry-Romberg
disease): case report. Neurosurgery 1998;42:1195-6.
83. Schievink WI, Mellinger JF, Atkinson JL. Progressive intracra-
nial aneurysmal disease in a child with progressive hemifacial
atrophy (Parry-Romberg disease): case report. Neurosurgery
1996;38:1237-41.
84. Chang SE, Huh J, Choi JH, Sung KJ, Moon KC, Koh JK.
Parry-Romberg syndrome with ipsilateral cerebral atrophy of
neonatal onset. Pediatr Dermatol 1999;16:487-8.
85. Lakhani PK, David TJ. Progressive hemifacial atrophy with
scleroderma and ipsilateral limb wasting (Parry-Romberg
syndrome). J R Soc Med 1984;77:138-9.
86. Qureshi UA, Wani NA, Altaf U. Parry-Romberg syndrome
associated with unusual intracranial vascular malformations
and Phthisis bulbi. J Neurol Sci 2010;291:107-9.
87. Miedziak AI, Stefanyszyn M, Flanagan J, Eagle RC Jr.
Parry-Romberg syndrome associated with intracranial vascu-
lar malformations. Arch Ophthalmol 1998;116:1235-7.
88. Menascu S, Padeh S, Hoffman C, Ben-Zeev B. Parry-Romberg
syndrome presenting as status migrainosus. Pediatr Neurol
2009;40:321-3.
89. Miao J, Liu R, Lin H, Su C, Li H, Lei G, et al. Severe bilateral
pyramidal tract involvement in a patient with Parry-Romberg
syndrome. Am J Med Sci 2009;337:212-4.
90. Kumar AA, Kumar RA, Shantha GP, Aloogopinathan G.
Progressive hemifacial atrophyeParry-Romberg syndrome
presenting as severe facial pain in a young man: a case
report. Cases J 2009;2:6776.
91. Blitstein MK, Tung GA. MRI of cerebral microhemorrhages.
AJR Am J Roentgenol 2007;189:720-5.
92. Straube A, Padovan CS, Seelos K. Parry-Romberg syndrome
and Rasmussen syndrome: only an incidental similarity?
Nervenarzt 2001;72:641-6.
93. Brito JC, Holanda MM, Holanda G, da Silva JA. Progressive
facial hemiatrophy (Parry-Romberg disease): report of two
cases associated with trigeminal neuralgia and cramps. Arq
Neuropsiquiatr 1997;55:472-7.
94. Kee C, Hwang JM. Parry-Romberg syndrome presenting with
recurrent exotropia and torticollis. J Pediatr Ophthalmol
Strabismus 2008;45:368-70.
95. Kaci�nski M, Biedro�n A, Zajac A, Steczkowska M. Diagnostic
difficulties of paroxysmal symptoms in a boy with
Parry-Romberg syndrome. Neurol Neurochir Pol 2010;44:
297-303.
96. Scope A, Barzilai A, Trau H, Orenstein A, Winkler E, Haik J.
Parry-Romberg syndrome and sympathectomyea coinci-
dence? Cutis 2004;73:343-4, 346.
97. Takenouchi T, Solomon GE. Alien hand syndrome in
Parry-Romberg syndrome. Pediatr Neurol 2010;42:280-2.
98. Menni S, Marzano AV, Passoni E. Neurologic abnormalities in
two patients with facial hemiatrophy and sclerosis coexisting
with morphea. Pediatr Dermatol 1997;14:113-6.
99. Moko SB, Mistry Y, Blandin de Chalain TM. Parry-Romberg
syndrome: intracranial MRI appearances. J Craniomaxillofac
Surg 2003;31:321-4.
100. Okumura A, Ikuta T, Tsuji T, Kato T, Fukatsu H, Naganawa S,
et al. Parry-Romberg syndrome with a clinically silent white
matter lesion. AJNR Am J Neuroradiol 2006;27:1729-31.
101. Fry JA, Alvarellos A, Fink CW, Blaw ME, Roach ES. Intracranial
findings in progressive facial hemiatrophy. J Rheumatol 1992;
19:956-8.
102. Aher SW, Berg BO. Progressive hemifacial atrophy: report of 3
cases, including one observed over 43 years, and CT findings.
Arch Neurol 1992;39:44-6.
103. Sagild JC, Alving J. Hemiplegic migraine and progressive
hemifacial atrophy. Ann Neurol 1985;17:620.
104. Merritt KK, Faber HK, Bruch H. Progressive facial hemiatrophy:
report of two cases with cerebral calcifications. J Pediatr
1937;10:374-95.
105. Derex L, Isnard H, Revol M. Progressive facial hemiatrophy
with multiple benign tumors and hamartomas. Neuropedi-
atrics 1995;26:306-9.
106. Goldberg-Stern H, deGrauw T, Passo M, Ball WS Jr. Parry-
Romberg syndrome: follow-up imaging during suppressive
therapy. Neuroradiology 1997;39:873-6.
107. Terstegge K, Kunath B, Felber S, Speciali JG, Beckert M,
Henkes H, et al. Magnetic resonance of brain involvement
in progressive facial hemiatrophy (Romberg’s disease):
reconsideration of a syndrome. Arq Neuropsiquiatr 1995;
53:98-113.
108. Moon WJ, Kim HJ, Roh HG, Oh J, Han SH. Diffusion tensor
imaging and fiber tractography in Parry-Romberg syndrome.
AJNR Am J Neuroradiol 2008;29:714-5.
109. Aleem MA, Meikandan D, Raveendran S, Ramasubramanian
D. Parry Romberg syndrome: newer concepts in pathophys-
iology. Neurol India 1999;47:342-3.
110. Verity C, Firth H, ffrench-Constant C. Congenital abnormal-
ities of the central nervous system. J Neurol Neurosurg
Psychiatry 2003;74(Suppl):i3-8.

J AM ACAD DERMATOL
OCTOBER 2012782 El-Kehdy, Abbas, and Rubeiz
111. DeFelipe J, Segura T, Arellano JI, Merch�an A, DeFelipe-Or-
oquieta J, Mart�ın P, et al. Neuropathological findings in a
patient with epilepsy and the Parry-Romberg syndrome.
Epilepsia 2001;42:1198-203.
112. Korkmaz C, Adapinar B, Uysal S. Beneficial effect of immuno-
suppressive drugs on Parry-Romberg syndrome: a case report
and review of the literature. South Med J 2005;98:940-2.
113. Dawczynski J, Thorwarth M, Koenigsdoerffer E, Schultze-Mos-
gau S. Interdisciplinary treatment and ophthalmological find-
ings in Parry-Romberg syndrome. J Craniofac Surg 2006;17:
1175-6.
114. Aracena T, Roca FP, Barragan M. Progressive hemifacial
atrophy (Parry-Romberg syndrome): report of two cases.
Ann Ophthalmol 1979;11:953-8.
115. Karim A, Laghmari M, Ibrahimy W, Essakali HN, Mohcine Z.
Neuroretinitis, Parry-Romberg syndrome, and scleroderma [in
French]. J Fr Ophtalmol 2005;28:866-70.
116. Bandello F, Rosa N, Ghisolfi F, Sebastiani A. New findings in
the Parry-Romberg syndrome: a case report. Eur J Ophthal-
mol 2002;12:556-8.
117. Brown WL, Bite U. Use of dissimilar trifocals to equalize fields
of view for asymmetric orbital positions secondary to
progressive facial hemiatrophy. Ophthal Plast Reconstr Surg
2011;27:e23-5.
118. Yildirim O, Dinc E, Oz O. Parry-Romberg syndrome associated
with anterior uveitis and retinal vasculitis. Can J Ophthalmol
2010;45:289-90.
119. MillerMT, SpencerMA. Progressivehemifacial atrophy: a natural
history study. Trans Am Ophthalmol Soc 1995;93:203-15.
120. Ong K, Billson FA, Pathirana DS, Clifton-Bligh P. A case of
progressive hemifacial atrophy with uveitis and retinal vas-
culitis. Aust N Z J Ophthalmol 1991;19:295-8.
121. Bellusci C, Liguori R, Pazzaglia A, Badiali L, Schiavi C, Campos
EC. Bilateral Parry-Romberg syndrome associated with retinal
vasculitis. Eur J Ophthalmol 2003;13:803-6.
122. L�opez-Leyva E, Due~nas-Arias E, Ju�arez-Azpilcueta A, Monta-~no-Uzcanga A, Ortiz-Pav�on A. Parry-Romberg syndrome con
glaucoma and pregnancy: first case in the literature. Gac Med
Mex 2001;137:65-6.
123. Ibarra P�erez C. Parry-Romberg syndrome with glaucoma and
pregnancy. Gac Med Mex 2001;137:289.
124. Nasser O, Greiner K, Amer R. Unilateral optic atrophy
preceding Coats disease in a girl with Parry-Romberg syn-
drome. Eur J Ophthalmol 2010;20:221-3.
125. Finley TA, Siatkowski RM. Progressive visual loss in a child
with Parry-Romberg syndrome. Semin Ophthalmol 2004;19:
91-4.
126. Khan AO. Restrictive strabismus in Parry-Romberg syndrome.
J Pediatr Ophthalmol Strabismus 2007;44:51-2.
127. Zubcov-Iwantscheff AA, Thomke F, Goebel HH, Bacharach-
Buhles M, Cordey A, Constantinescu CS, et al. Eyemovement
involvement in Parry-Romberg syndrome: a clinicopathologic
case report. Strabismus 2008;16:119-21.
128. Detilleux JM, Zanen J. Progressive facial hemiatrophy (Par-
ry-Romberg disease) with chorioretinal lesions. Bull Soc Belge
Ophtalmol 1970;156:608-18.
129. Johnson RV, Kennedy WR. Progressive facial hemiatrophy
(Parry-Romberg syndrome): contralateral extraocular muscle
impairment. Am J Ophthalmol 1969;67:561-4.
130. Galanopoulos A, McNab AA. Hemifacial atrophy: an unusual
cause of upper eyelid retraction. Ophthal Plast Reconstr Surg
1995;11:278-80.
131. de Crecchio G, Forte R, Strianese D, Rinaldi M, D’Aponte A.
Clinical evolution of neuroretinitis in Parry-Romberg syn-
drome. J Pediatr Ophthalmol Strabismus 2008;45:125-6.
132. Ousterhout DK. Correction of enophthalmos in progressive
hemifacial atrophy: a case report. Ophthal Plast Reconstr
Surg 1996;12:240-4.
133. Hung S, Rutar T, Lin S, Wong IG. Severe hypotony associated
with Parry-Romberg syndrome. Ophthalmic Surg Lasers
Imaging 2010;9:1-3.
134. Park DH, Kim IT. Patient with Parry-Romberg syndrome
complicated by Coats’ syndrome. Jpn J Ophthalmol 2008;
52:520-2.
135. Sharma DC, Parihar PS, Kumawat DC, Ramakrishnan S, Dave
R, Bhatnagar HN, et al. Duane’s retraction syndrome with
facial hemiatrophy (a case report). J Postgrad Med 1990;36:
51-3.
136. Theodossiadis PG, Grigoropoulos VG, Emfietzoglou I, Papas-
pirou A, Nikolaidis P, Vergados I, et al. Parry-Romberg
syndrome studied by optical coherence tomography. Oph-
thalmic Surg Lasers Imaging 2008;39:78-80.
137. Beluffi G, Bassi L, Vitali MC, Meloni G, Caselli D. Parry-Rom-
berg syndrome and odontogenic cyst: a case report. Radiol
Med 2001;101:88-90.
138. Fietta M, Gennari PU. Observations on a case of odontoma of
the mandible associated with Parry-Romberg syndrome. Riv
Anat Patol Oncol 1963;24(Suppl):763-80.
139. Fayad S, Steffensen B. Root resorptions in a patient with
hemifacial atrophy. J Endod 1994;20:299-303.
140. O’Flynn S, Kinirons M. Parry-Romberg syndrome: a report of
the dental findings in a child followed up for 9 years. Int J
Paediatr Dent 2006;16:297-301.
141. Pruszewicz A, Wojnowski W, Walczak M, Zebryk-Stopa A.
Parry-Romberg syndrome: communication disorders in a
12-year-old boy. Otolaryngol Pol 2003;57:715-7.
142. Rafai MA, Boulaajaj FZ, El Moutawakil B, Bourezgui M, Sibai M,
Mahtar M, et al. Parry-Romberg syndrome with dysphonia.
Rev Neurol (Paris) 2007;163:1246-8.
143. Oosterkamp BC, Damstra J, Jansma J. Facial asymmetry: the
benefits of cone beam computerized tomography. Ned
Tijdschr Tandheelkd 2010;117:269-73.
144. de Vasconcelos Carvalho M, do Nascimento GJ, Andrade E,
Andrade M, Sobral AP. Association of aesthetic and ortho-
dontic treatment in Parry-Romberg syndrome. J Craniofac
Surg 2010;21:436-9.
145. Grippaudo C, Deli R, Grippaudo FR, Di Cuia T, Paradisi M.
Management of craniofacial development in the
Parry-Romberg syndrome: report of two patients. Cleft Palate
Craniofac J 2004;41:95-104.
146. Marzano AV, Menni S, Parodi A, Borghi A, Fuligni A, Fabbri P,
et al. Localized scleroderma in adults and children: clinical
and laboratory investigations on 239 cases. Eur J Dermatol
2003;13:171-6.
147. Kister I, Inglese M, Laxer RM, Herbert J. Neurologic manifes-
tations of localized scleroderma: a case report and literature
review. Neurology 2008;71:1538-45.
148. Hickman JW, Sheils WS. Progressive facial hemiatrophy:
report of a case with marked homolateral involvement.
Arch Intern Med 1964;113:716-20.
149. Donley DE. Facial hemiatrophy associated with epilepsy:
report of a case. J Nerv Ment Dis 1935;82:33-9.
150. Obermoser G, Pfausler BE, Linder DM, Sepp NT. Sclero-
derma en coup de sabre with central nervous system and
ophthalmologic involvement: treatment of ocular symp-
toms with interferon gamma. J Am Acad Dermatol 2003;49:
543-6.
151. Grosso S, Fioravanti A, Biasi G, Conversano E, Marcolongo R,
Morgese G, et al. Linear scleroderma associated with pro-
gressive brain atrophy. Brain Dev 2003;25:57-61.

J AM ACAD DERMATOL
VOLUME 67, NUMBER 4El-Kehdy, Abbas, and Rubeiz 783
152. Kreuter A, Gambichler T, Breuckmann F, Rotterdam S, Freitag
M, Stuecker M, et al. Pulsed high-dose corticosteroids com-
bined with low-dose methotrexate in severe localized scle-
roderma [Erratum in Arch Dermatol 2005;141:1091]. Arch
Dermatol 2005;141:847-52.
153. Falanga V, Medsger TA Jr, Reichlin M, Rodnan GP. Linear
scleroderma: clinical spectrum, prognosis, and laboratory
abnormalities. Ann Intern Med 1986;104:849-57.
154. Jablonska S, Blaszczyk M, Rosinka D. Progressive facial
hemiatrophy and scleroderma en coup de sabre: clinical
presentation and course as related to the onset in early
childhood and young adults. Arch Argent Dermatol 2007;56:
257-63.
155. Orozco-Covarrubias L, Guzm�an-Meza A, Ridaura-Sanz C,
Carrasco Daza D, Sosa-de-Martinez C, Ruiz-Maldonado R.
Scleroderma ‘en coup de sabre’ and progressive facial
hemiatrophy. Is it possible to differentiate them? J Eur
Acad Dermatol Venereol 2002;16:361-6.
156. Blaszczyk M, Kr�olicki L, Krasu M, Glinska O, Jablonska S.
Progressive facial hemiatrophy: central nervous system in-
volvement and relationship with scleroderma en coup de
sabre. J Rheumatol 2003;30:1997-2004.
157. Chbicheb M, Gelot A, Rivier F, Roubertie A, Humbertclaude V,
Coubes P, et al. Parry-Romberg’s syndrome and epilepsy [in
French]. Rev Neurol (Paris) 2005;161:92-7.
158. Holland KE, Steffes B, Nocton JJ, Schwabe MJ, Jacobson RD,
Drolet BA. Linear scleroderma en coup de sabre with
associated neurologic abnormalities. Pediatrics 2006;117:
e132-6.
159. Zulian F, Athreya BH, Laxer R, Nelson AM, Feitosa de Oliveira
SK, Punaro MG, et al. Juvenile localized scleroderma: clinical
and epidemiological features in 750 children, an international
study. Rheumatology (Oxford) 2006;45:614-20.
160. Chung MH, Sum J, Morrell MJ, Horoupian DS. Intracerebral
involvement in scleroderma en coup de sabre: report of a case
with neuropathologic findings. Ann Neurol 1995;37:679-81.
161. Liu P, Uziel Y, Chuang S, Silverman E, Krafchik B, Laxer R.
Localized scleroderma: imaging features. Pediatr Radiol 1994;
24:207-9.
162. Stone J, Franks AJ, Guthrie JA, Johnson MH. Scleroderma ‘‘en
coup de sabre’’: pathological evidence of intracerebral
inflammation. J Neurol Neurosurg Psychiatry 2001;70:382-5.
163. Ye XD, Li CY, Wang C, Yu YS. Superficial temporal fascial flap
plus lipofilling for facial contour reconstruction in bilateral
progressive facial hemiatrophy. Aesthetic Plast Surg 2010;34:
534-7.
164. Berenguer B, Gallo H, Rodr�ıguez Urcelay P, Mar�ın Guztke M,
Gonz�alez Meli B, Enr�ıquez de Salamanca J. Free fat flap for
the treatment of Parry-Romberg disease in children. Cir
Pediatr 2005;18:49-51.
165. Ozturk S, Acarturk TO, Yapici K, Sengezer M. Treatment of ‘en
coup de sabre’ deformity with porous polyethylene implant.
J Craniofac Surg 2006;17:696-701.
166. Palmero ML, Uziel Y, Laxer RM, Forrest CR, Pope E. En coup
de sabre scleroderma and Parry-Romberg syndrome in
adolescents: surgical options and patient-related outcomes.
J Rheumatol 2010;37:2174-9.
167. Saccomanno F, Bernardi C, Vittorini P. The expanded poly-
tetrafluoroethylene (ePTFE) in the surgical treatment of
Parry-Romberg syndrome: case report. Aesthetic Plast Surg
1997;21:342-5.
168. Onesti MG, Troccola A, Scuderi N. Volumetric correction
using poly-L-lactic acid in facial asymmetry: Parry Romberg
syndrome and scleroderma. Dermatol Surg 2009;35:
1368-75.
169. Yoshimura K, Sato K, Aoi N, Kurita M, Inoue K, Suga H, et al.
Cell-assisted lipotransfer for facial lipoatrophy: efficacy of
clinical use of adipose-derived stem cells. Dermatol Surg
2008;34:1178-85.
170. Sterodimas A, Huanquipaco JC, de Souza Filho S, Bornia FA,
Pitanguy I. Autologous fat transplantation for the treatment
of Parry-Romberg syndrome. J Plast Reconstr Aesthet Surg
2009;62:e424-6.
171. Clauser LC, Tieghi R, Consorti G. Parry-Romberg syndrome:
volumetric regeneration by structural fat grafting technique.
J Craniomaxillofac Surg 2010;38:605-9.
172. Duymaz A, Karabekmez FE, Tosun Z, Keskin M, Karamese M,
Savaci N. Reconstruction with galeal frontalis flap of de-
pressed forehead region in progressive hemifacial atrophy.
J Craniofac Surg 2008;19:1104-6.
173. Avelar RL, G€oelzer JG, Azambuja FG, de Oliveira RB, de
Oliveira MP, Pase PF. Use of autologous fat graft for correc-
tion of facial asymmetry stemming from Parry-Romberg
syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2010;109:e20-5.
174. Wang XC, Qiao Q, Liu ZF, Feng R, Zhang HL, Yan YJ, et al.
Microsurgical tissue transfer for the reconstruction of hem-
ifacial atrophy (Parry-Romberg syndrome). Zhonghua Zheng
Xing Wai Ke Za Zhi 2006;22:433-5.
175. Zhang Y, Jin R, Shi Y, Sun B, Zhang Y, Qian Y. Pedicled
superficial temporal fascia sandwich flap for reconstruction
of severe facial depression. J Craniofac Surg 2009;20:505-8.
176. Wolff KD, Kesting M, L€offelbein D, H€olzle F. Perforator-based
anterolateral thigh adipofascial or dermal fat flaps for facial
contour augmentation. J Reconstr Microsurg 2007;23:
497-503.
177. Cheng J, Shen G, Tang Y, Zhang Z, Qiu W, Lu X. Facial
reconstruction with vascularized serratus anterior muscle flap
in patients with Parry-Romberg syndrome. Br J Oral Max-
illofac Surg 2010;48:261-6.
178. Malakhovskaia VI, Nerobeev AI, Osipov GI. The thoracodorsal
flap in facial reconstruction. Stomatologiia (Mosk) 1995;74:
40-5.
179. Yu-Feng L, Lai G, Zhi-Yong Z. Combined treatments of facial
contour deformities resulting from Parry-Romberg syn-
drome. J Reconstr Microsurg 2008;24:333-42.
180. Vaienti L, Soresina M, Menozzi A. Parascapular free flap and
fat grafts: combined surgical methods in morphological
restoration of hemifacial progressive atrophy. Plast Reconstr
Surg 2005;116:699-711.
181. Onesti MG, Monarca C, Rizzo MI, Mazzocchi M, Scuderi N.
Minimally invasive combined treatment for Parry-Romberg
syndrome. Aesthetic Plast Surg 2009;33:452-6.
182. Grimaldi M, Gentile P, Labardi L, Silvi E, Trimarco A, Cervelli V.
Lipostructure technique in Romberg syndrome. J Craniofac
Surg 2008;19:1089-91.
183. Cervelli V, Gentile P. Use of cell fat mixed with platelet gel in
progressive hemifacial atrophy. Aesthetic Plast Surg 2009;33:
22-7.
184. Guerrerosantos J, Guerrerosantos F, Orozco J. Classification
and treatment of facial tissue atrophy in Parry-Romberg
disease. Aesthetic Plast Surg 2007;31:424-34.
185. Behera M, Nimkhedkar K, Gupta RS, Hassadi MF, Mousa ME.
Facial hemiatrophy (Parry-Romberg syndrome) and hyper-
trophic cardiomyopathy. J Assoc Physicians India 1988;36:
394-5.
186. Esgleyes-Ribot T, Garcia-De la Torre I, Gonzalez-Mendoza A,
Guerrerosantos J, Barcelo R. Progressive facial hemiatrophy
(Parry-Romberg syndrome) and antibodies to Borrelia. J Am
Acad Dermatol 1991;25:578-9.

J AM ACAD DERMATOL
OCTOBER 2012784 El-Kehdy, Abbas, and Rubeiz
187. Abele DC, Bedingfield RB, Chandler FW, Given KS. Progressive
facial hemiatrophy (Parry-Romberg syndrome) and borrelio-
sis. J Am Acad Dermatol 1990;22:531-3.
188. Baskan EB, Kacar SD, Turan A, Saricaoglu H, Tunali S, Adim
SB. Parry-Romberg syndrome associated with borreliosis:
could photochemotherapy halt the progression of the
disease? Photodermatol Photoimmunol Photomed 2006;22:
259-61.
189. Abele DC, Anders KH. The many faces and phases of
borreliosis II. J Am Acad Dermatol 1990;23:401-10.
190. Dintiman BJ, Shapiro RS, Hood AF, Guba AM. Parry-Romberg
syndrome in association with contralateral Poland syndrome.
J Am Acad Dermatol 1990;22:371-3.
191. Zambelis T, Tsivgoulis G, Kokotis P, Spengos K, Karandreas N.
Electrophysiological findings in a case of congenital lower
limb hypoplasia. Neurol Sci 2008;29:177-9.