Embed Size (px)
DESCRIPTION
PART II. Obstructive Airway Diseases. Obstructive Lung Diseases. Chronic Bronchitis. Emphysema. Cystic Fibrosis. Asthma. Bronchiectasis. The most common obstructive lung diseases. Chapter 11 Chronic Obstructive Pulmonary Disease (COPD) Chronic Bronchitis and Emphysema. - PowerPoint PPT Presentation
Citation preview
1Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
PART IIPART II
Obstructive Airway Obstructive Airway DiseasesDiseases
2Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Asthma
Chronic Bronchitis
Emphysema
Obstructive Lung Diseases
Cystic Fibrosis
Bronchiectasis
The most common obstructive lung diseases
3Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chapter 11Chapter 11
Chronic Obstructive Pulmonary Chronic Obstructive Pulmonary Disease (COPD) Chronic Bronchitis Disease (COPD) Chronic Bronchitis
and Emphysemaand Emphysema
4Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
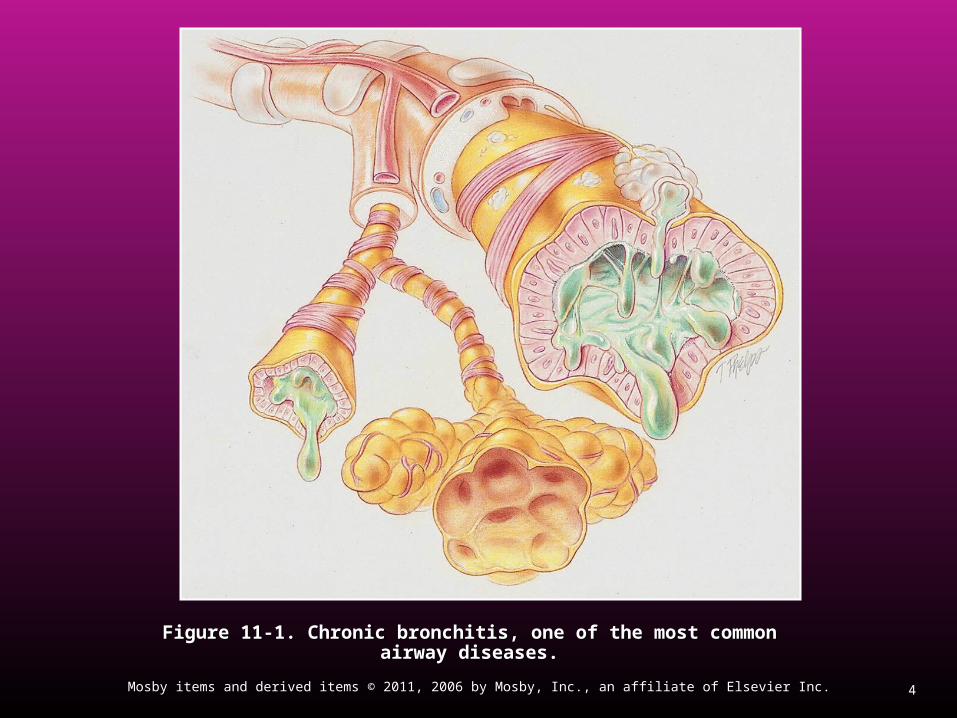
Figure 11-1. Chronic bronchitis, one of the most common airway diseases.Figure 11-1. Chronic bronchitis, one of the most common airway diseases.

5Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 11-2. Panlobular emphysema. A, Normal alveoli for comparison purposes. B, Panlobular Figure 11-2. Panlobular emphysema. A, Normal alveoli for comparison purposes. B, Panlobular emphysema. C, Excessive bronchial secretions from bronchitis, a common alteration of the emphysema. C, Excessive bronchial secretions from bronchitis, a common alteration of the
lungs.lungs.
A
B
C
6Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
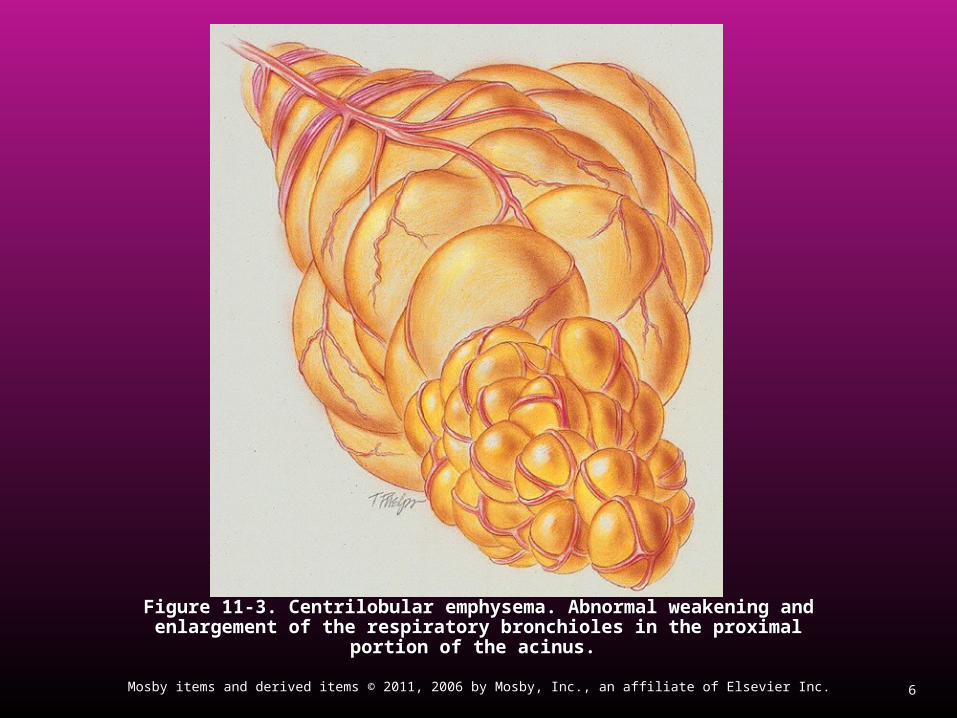
Figure 11-3. Centrilobular emphysema. Abnormal weakening and enlargement Figure 11-3. Centrilobular emphysema. Abnormal weakening and enlargement of the respiratory bronchioles in the proximal portion of the acinus. of the respiratory bronchioles in the proximal portion of the acinus.
7Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
The American Thoracic Society The American Thoracic Society (ATS)(ATS)
Guidelines for Guidelines for Chronic obstructive pulmonary disease (COPD)Chronic obstructive pulmonary disease (COPD) Chronic bronchitis, Chronic bronchitis, EmphysemaEmphysema

8Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chronic Obstructive PulmonaryChronic Obstructive Pulmonary DiseaseDisease
Is a preventable and treatable disease state Is a preventable and treatable disease state characterized by airflow limitation that is not characterized by airflow limitation that is not fully reversible. fully reversible.
The airflow limitation is usually progressive The airflow limitation is usually progressive and is associated with an abnormal and is associated with an abnormal inflammatory response of the lungs to inflammatory response of the lungs to noxious particles or gases, primarily caused noxious particles or gases, primarily caused by cigarette smoking. by cigarette smoking.
Although COPD affects the lungs, it also Although COPD affects the lungs, it also produces significant systemic consequences.produces significant systemic consequences.

9Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chronic BronchitisChronic Bronchitis
Is defined clinically as chronic productive Is defined clinically as chronic productive cough for 3 months in each of 2 successive cough for 3 months in each of 2 successive years in a patient in whom other causes of years in a patient in whom other causes of productive chronic cough have been productive chronic cough have been excluded.excluded.

10Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
EmphysemaEmphysema
Is defined pathologically as the presence of Is defined pathologically as the presence of permanent enlargement of the airspaces permanent enlargement of the airspaces distal to the terminal bronchioles, distal to the terminal bronchioles, accompanied by destruction of their walls accompanied by destruction of their walls and without obvious fibrosis. and without obvious fibrosis.

11Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
In patients with In patients with COPD:COPD:
Either or both of those conditions may be Either or both of those conditions may be present. present.
However, the relative contribution of each to However, the relative contribution of each to the disease process is often difficult to the disease process is often difficult to discern.”discern.”

12Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Note that the ATS’s definition forNote that the ATS’s definition for
Chronic bronchitisChronic bronchitis is based on the major is based on the major ""clinical manifestationsclinical manifestations" associated with the " associated with the disease. disease.
EmphysemaEmphysema is based on the pathology, or is based on the pathology, or the "the "anatomic alterations of the lung,anatomic alterations of the lung," " associated with the disorder. associated with the disorder.
13Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
The The GGlobal Initiative for Chronic lobal Initiative for Chronic OObstructive bstructive LLung ung DDisease (isease (GOLDGOLD) )
provides this working definition:provides this working definition:

14Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chronic Obstructive Pulmonary Chronic Obstructive Pulmonary Disease (COPD)Disease (COPD) is….. is…..
A preventable and treatable disease with A preventable and treatable disease with some significant extrapulmonary effects that some significant extrapulmonary effects that may contribute to the severity in individual may contribute to the severity in individual patients. patients.
Its pulmonary component is characterized by Its pulmonary component is characterized by airflow limitation that is not fully reversible. airflow limitation that is not fully reversible.
The airflow limitation is usually progressive The airflow limitation is usually progressive and associated with an abnormal and associated with an abnormal inflammatory response of the lung to noxious inflammatory response of the lung to noxious particles or gases.particles or gases.

15Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
The bottom line is this:The bottom line is this:
Even though chronic bronchitis and Even though chronic bronchitis and emphysema can each develop alone, they emphysema can each develop alone, they often occur together as one disease often occur together as one disease complex.complex.
When this happens, the disease entity is When this happens, the disease entity is called called chronic obstructive pulmonary chronic obstructive pulmonary disease (COPD)disease (COPD)..

16Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
GOLD Website Address
http://www.goldcopd.org

17Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Anatomic Alterations of the LungsAnatomic Alterations of the LungsAssociated with Chronic BronchitisAssociated with Chronic Bronchitis
Chronic inflammation and swelling of the Chronic inflammation and swelling of the peripheral airwaysperipheral airways
Excessive mucus production and Excessive mucus production and accumulationaccumulation
Partial or total mucus plugging of the airwaysPartial or total mucus plugging of the airways Smooth muscle constriction of bronchial Smooth muscle constriction of bronchial
airways (bronchospasm)airways (bronchospasm) Air trapping and hyperinflation of alveoli—Air trapping and hyperinflation of alveoli—
occasionally in the late stagesoccasionally in the late stages
18Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Anatomic Alterations of the Lungs Anatomic Alterations of the Lungs Associated with EmphysemaAssociated with Emphysema
Permanent enlargement and deterioration of Permanent enlargement and deterioration of the air spaces distal to the terminal the air spaces distal to the terminal bronchiolesbronchioles
Destruction of pulmonary capillariesDestruction of pulmonary capillaries Weakening of the distal airways, primarily the Weakening of the distal airways, primarily the
respiratory bronchiolesrespiratory bronchioles Air trapping and hyperinflation of alveoli (air-Air trapping and hyperinflation of alveoli (air-
trapping)trapping)
19Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
EpidemiologyEpidemiology
It is estimated that between 10 and 15 million It is estimated that between 10 and 15 million people in the United States either have people in the United States either have chronic bronchitis, emphysema, or a chronic bronchitis, emphysema, or a combination of both. combination of both.
Most authorities agree that COPD is under-Most authorities agree that COPD is under-diagnosed.diagnosed.

20Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Risk FactorsRisk FactorsAccording to GOLDAccording to GOLD
Tobacco smokeTobacco smoke Occupational dusts and chemicalsOccupational dusts and chemicals Indoor air pollutionIndoor air pollution Outdoor air pollutionOutdoor air pollution Conditions that affect normal lung growthConditions that affect normal lung growth Genetic predispositionGenetic predisposition
Alpha 1-antitrypsin deficiencyAlpha 1-antitrypsin deficiency
21Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Diagnosis of COPDDiagnosis of COPDAccording to GOLDAccording to GOLD
Key Indicators for Considering a COPD Key Indicators for Considering a COPD Diagnosis:Diagnosis: DysypneaDysypnea Chronic coughChronic cough Chronic sputum productionChronic sputum production History of exposure to risk factorsHistory of exposure to risk factors
22Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Pulmonary Function Study in the Pulmonary Function Study in the Diagnosis of COPDDiagnosis of COPD
According to GOLDAccording to GOLD The three main spirometry tests for COPD The three main spirometry tests for COPD
are the :are the : FVCFVC FEVFEV11
FEVFEV11/FVC ratio/FVC ratio
23Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
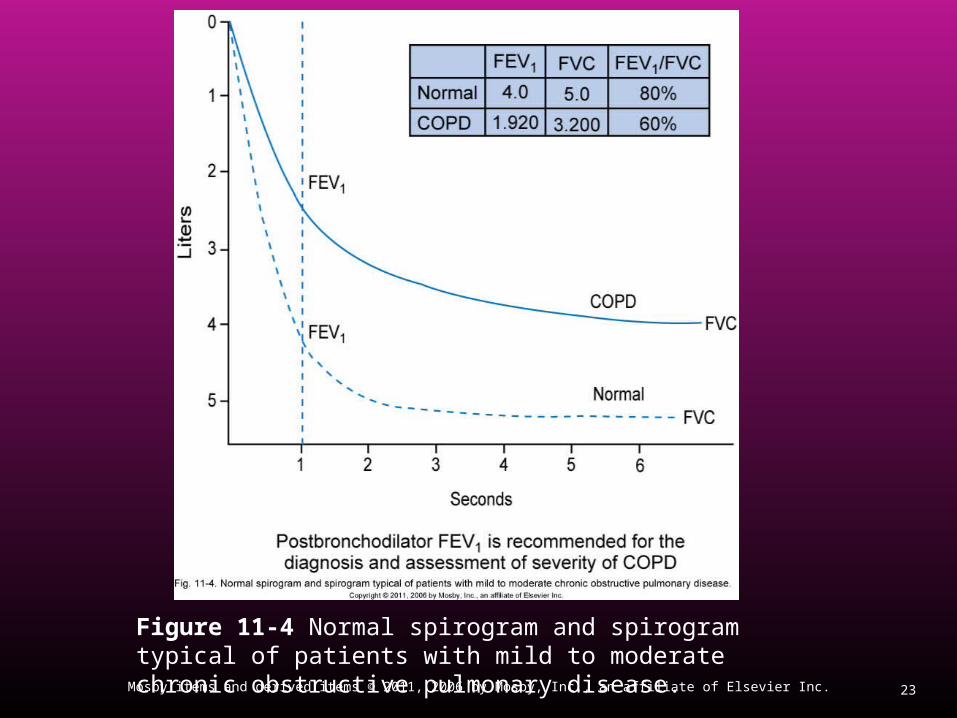
Figure 11-4 Normal spirogram and spirogram typical of patients with mild to moderate chronic obstructive pulmonary disease.
24Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Pulmonary Function Study in the Pulmonary Function Study in the Diagnosis of COPD (Cont’d)Diagnosis of COPD (Cont’d)
The presence of COPD is confirmed when The presence of COPD is confirmed when both the FEVboth the FEV11 and FEV and FEV11/FVC ratio are /FVC ratio are
decreaseddecreased
25Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Stages of COPDStages of COPDAccording to GOLDAccording to GOLD
Stage I: Mild COPDStage I: Mild COPD Stage II: Moderate COPDStage II: Moderate COPD Stage III: severe COPDStage III: severe COPD Stage IV: Very severe COPDStage IV: Very severe COPD
26Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Additional Diagnostic Studies of COPDAdditional Diagnostic Studies of COPDAccording to GOLDAccording to GOLD
Bronchodilator reversibility testingBronchodilator reversibility testing Chest x-rayChest x-ray Arterial blood gas measurementArterial blood gas measurement AlphaAlpha11 antitrypsin deficiency screening antitrypsin deficiency screening
27Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
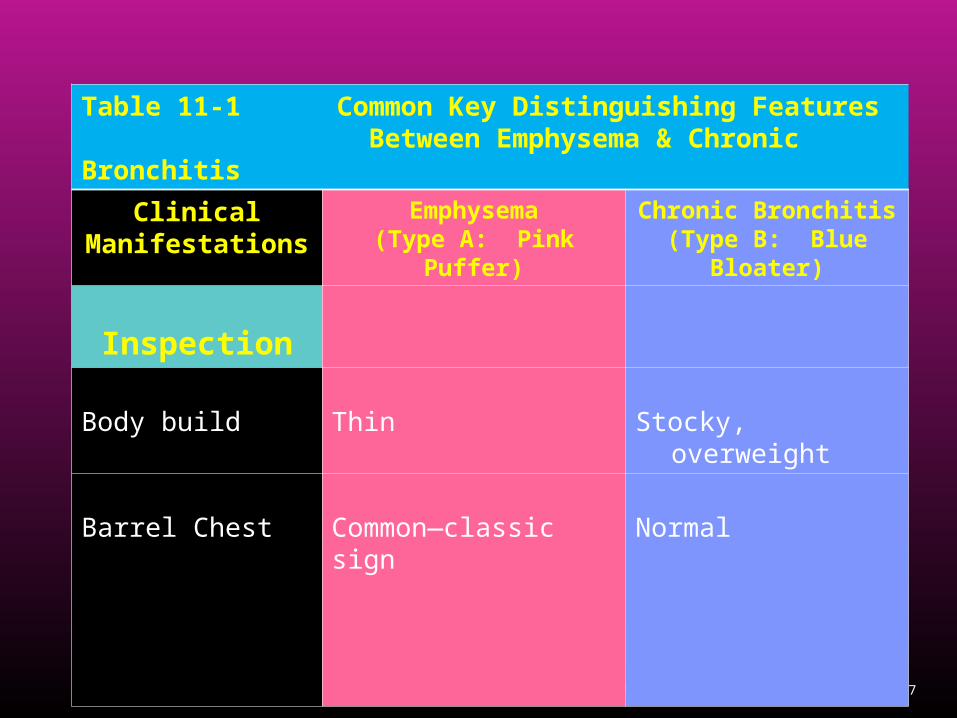
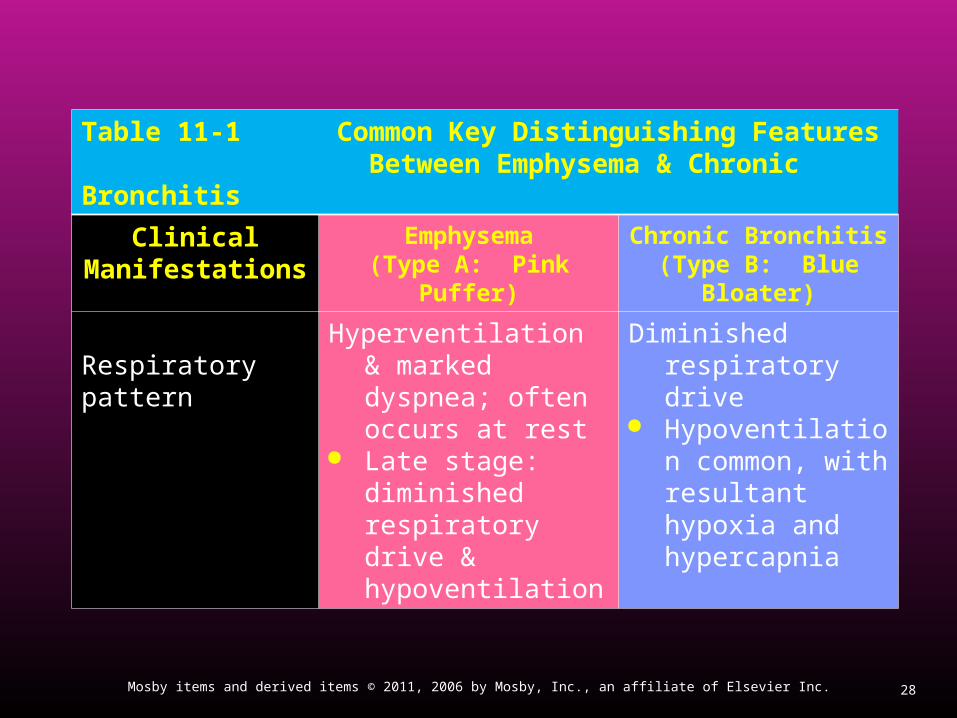
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Inspection
Body build Thin Stocky, overweight
Barrel Chest Common—classic sign Normal
28Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Respiratory patternHyperventilation &
marked dyspnea; often occurs at rest
Late stage: diminished respiratory drive & hypoventilation
Diminished respiratory drive
Hypoventilation common, with resultant hypoxia and hypercapnia

29Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis (Cont’d)
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Pursed-lip breathing
Common Uncommon
Cough Uncommon Common—classic sign
Sputum Uncommon Common—classic sign
Copious amounts, purulent
30Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
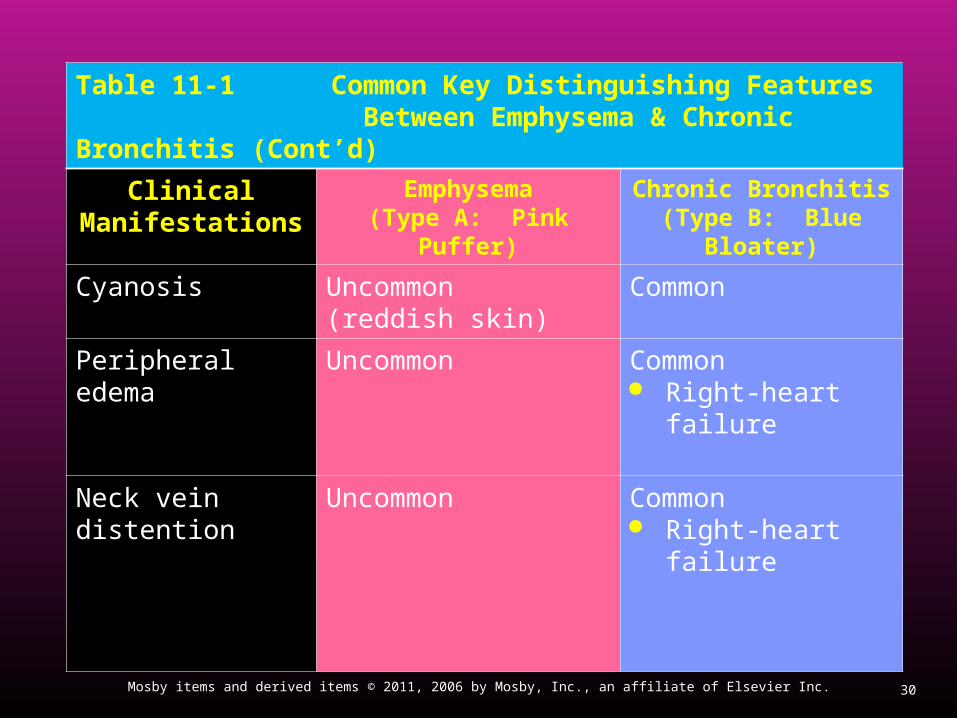
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis (Cont’d)
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Cyanosis Uncommon (reddish skin)
Common
Peripheral edema Uncommon Common Right-heart failure
Neck vein distention
Uncommon Common Right-heart failure
31Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
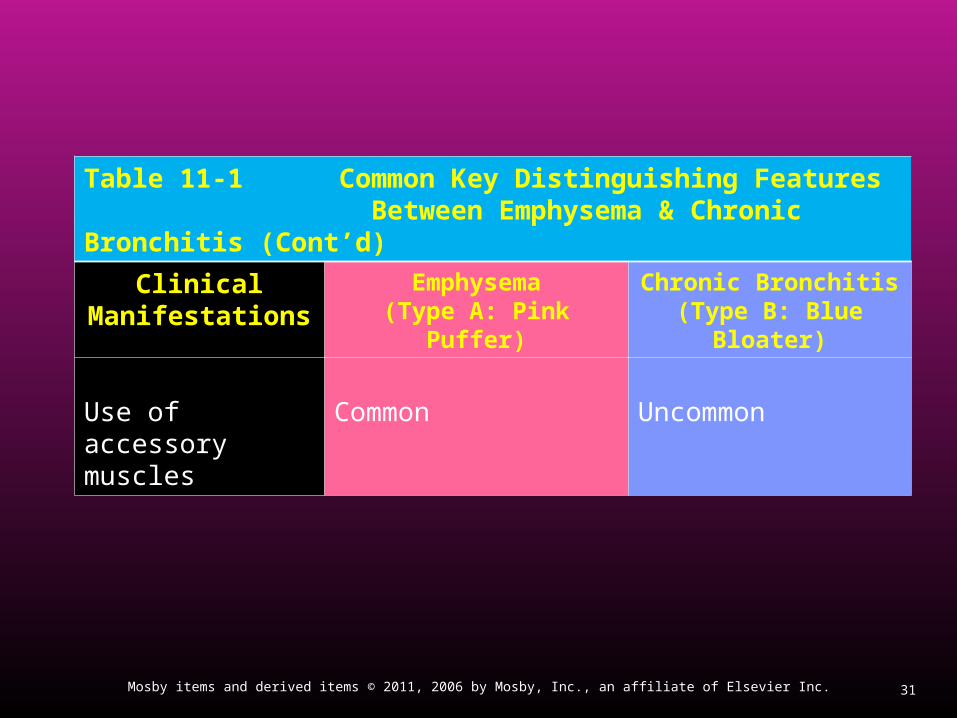
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis (Cont’d)
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Use of accessory muscles
Common Uncommon

32Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Auscultation Decreased breath
sounds, decreased heart sounds; prolonged expiration
Wheezes, crackles, rhonchi, depending on severity of disease
Percussion Hyperresonance Normal
33Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
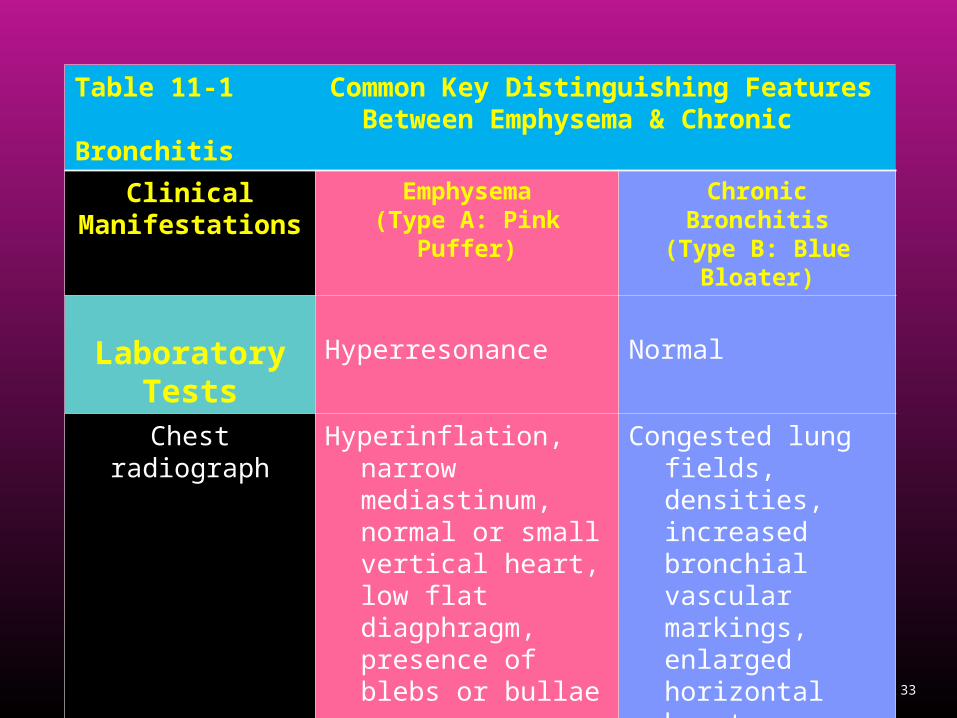
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Laboratory Tests
Hyperresonance Normal
Chest radiograph Hyperinflation, narrow mediastinum, normal or small vertical heart, low flat diagphragm, presence of blebs or bullae
Congested lung fields, densities, increased bronchial vascular markings, enlarged horizontal heart
Polycythemia Uncommon Common

34Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Infections Occasionally Common
Polycythemia Uncommon Common

35Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-1 Common Key Distinguishing Features Between Emphysema & Chronic Bronchitis
Clinical Manifestations
Emphysema(Type A: Pink Puffer)
Chronic Bronchitis(Type B: Blue Bloater)
Pulmonary Function Study
DLCO and DLCO/VA Decreased Often normal
Other
Pulmonary hypertension
Uncommon Common
Cor pulmonale Uncommon Common Right-heart failure

36Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
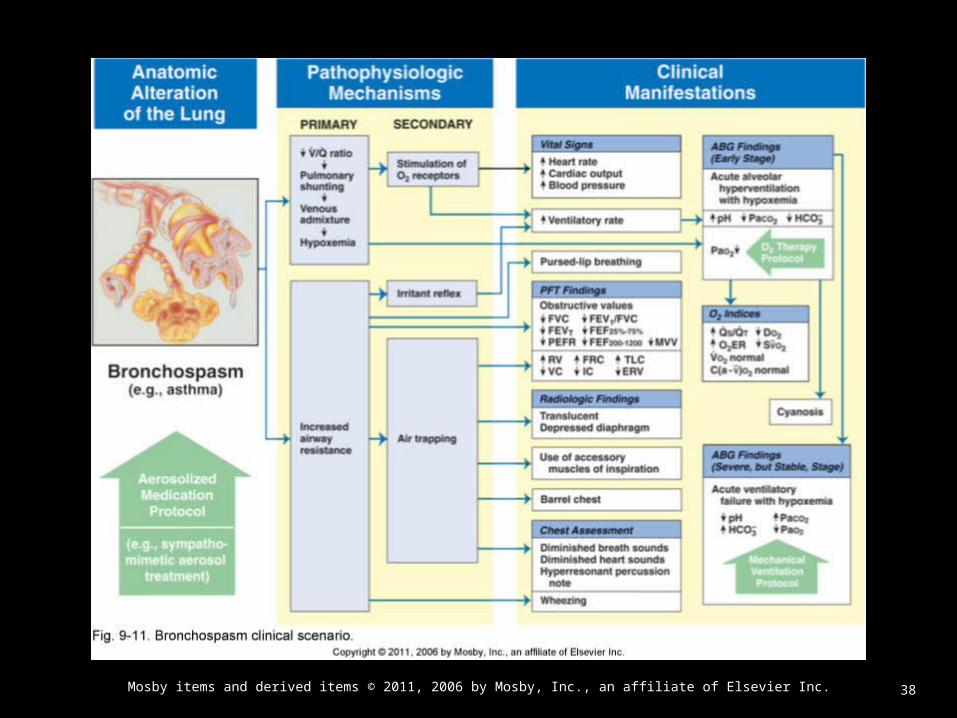
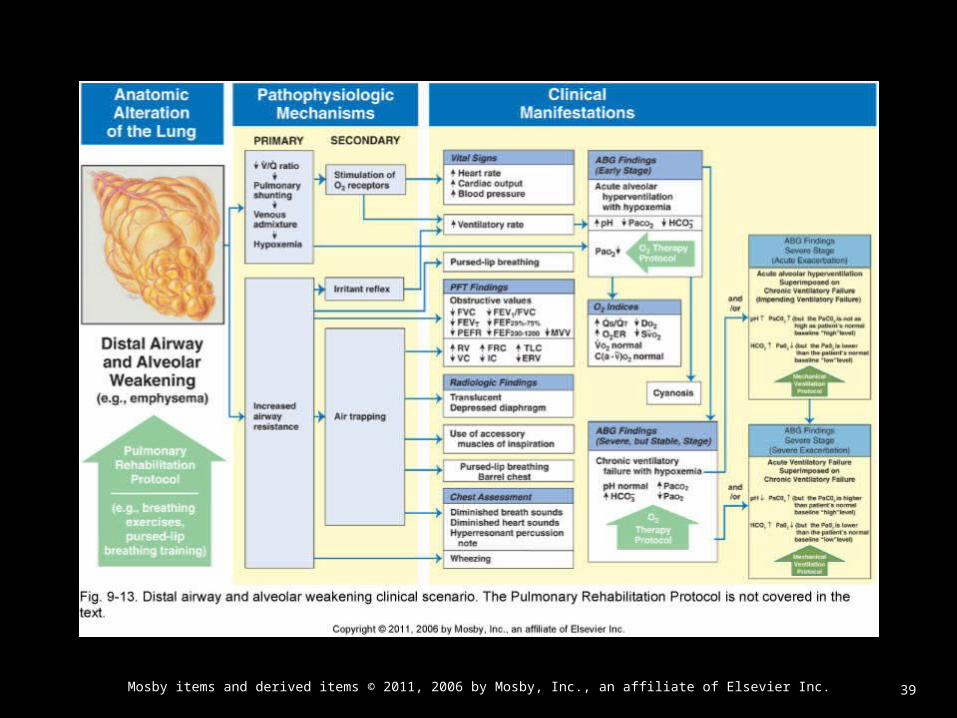
Overview Overview of the Cardiopulmonary Clinical Manifestations of the Cardiopulmonary Clinical Manifestations
Associated with Associated with Chronic Bronchitis and Emphysema (COPD)Chronic Bronchitis and Emphysema (COPD)
The following clinical manifestations result from the The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) pathophysiologic mechanisms caused (or activated) by by
Excessive Bronchial Secretions Bronchospasm Distal Airway and Alveolar Weakening

37Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
38Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
39Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

40Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Clinical Data Obtained at the Clinical Data Obtained at the Patient’s BedsidePatient’s Bedside
Vital Signs Chronic Bronchitis & Emphysema
Heart rate and respiratory rate
Stable patients: normal vital signs Exacerbations: Usually acute
increase in heart rate and respiratory rate (Tachypnea)
Classic sign of hypoxemia
41Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
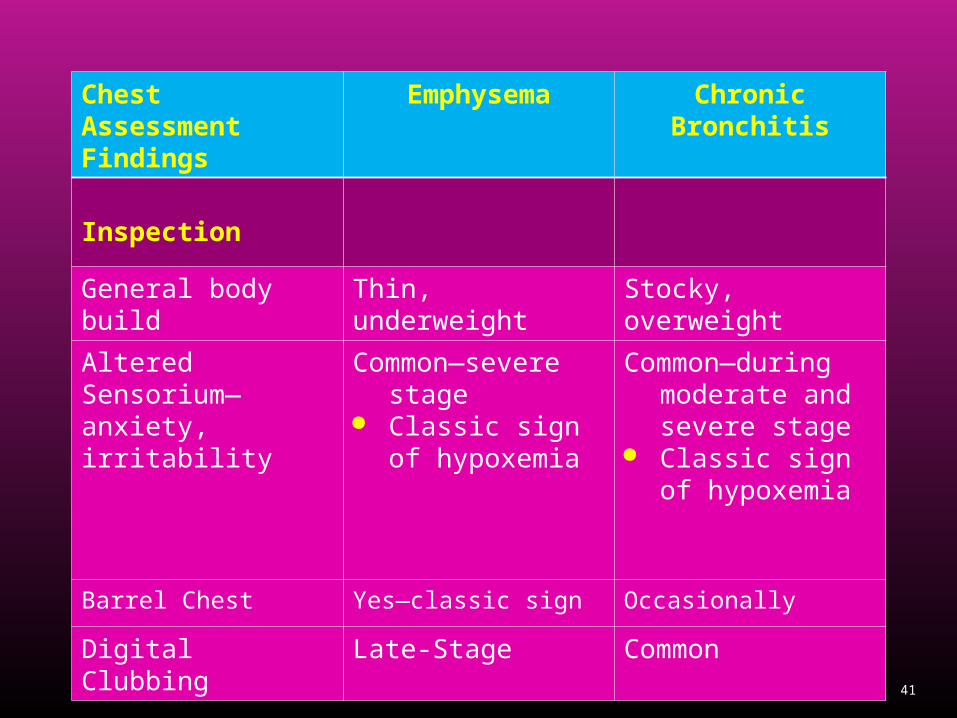
Chest Assessment Findings
Emphysema Chronic Bronchitis
Inspection
General body build Thin, underweight Stocky, overweight
Altered Sensorium—anxiety, irritability
Common—severe stage
Classic sign of hypoxemia
Common—during moderate and severe stage
Classic sign of hypoxemia
Barrel Chest Yes—classic sign Occasionally
Digital Clubbing Late-Stage Common
42Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
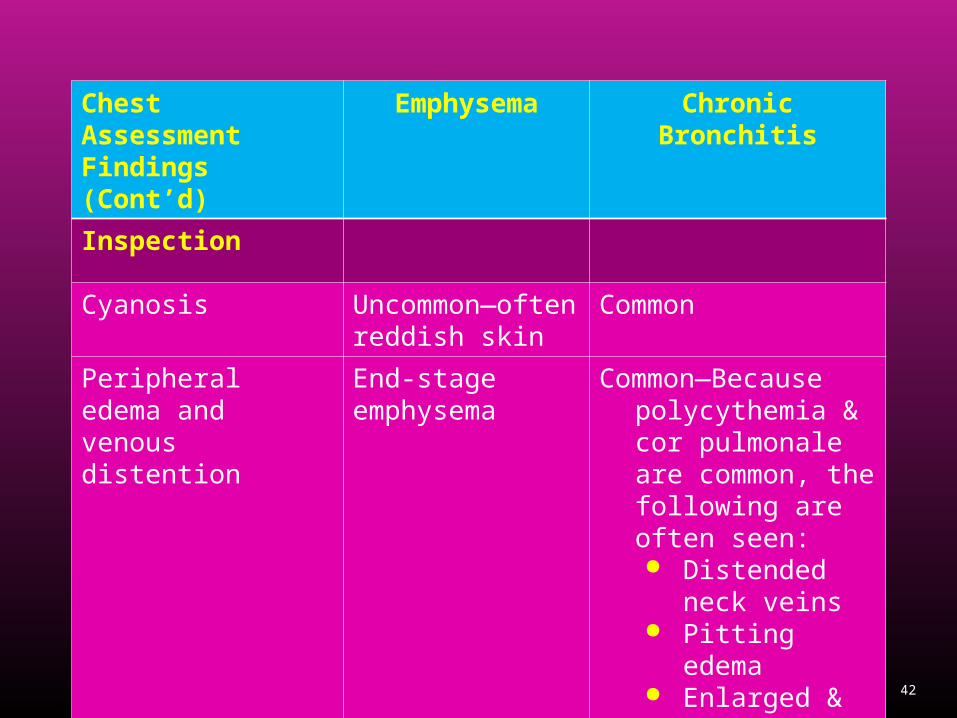
Chest Assessment Findings (Cont’d)
Emphysema Chronic Bronchitis
Inspection
Cyanosis Uncommon—often reddish skin
Common
Peripheral edema and venous distention
End-stage emphysema
Common—Because polycythemia & cor pulmonale are common, the following are often seen:
Distended neck veins
Pitting edema Enlarged &
tender liver
43Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
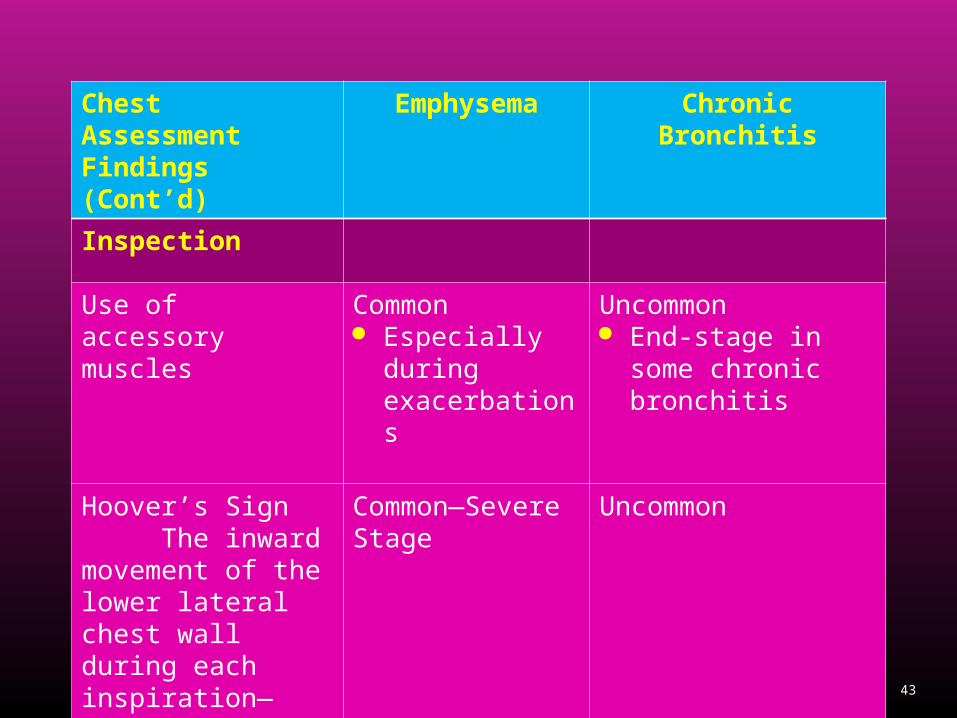
Chest Assessment Findings (Cont’d)
Emphysema Chronic Bronchitis
Inspection
Use of accessory muscles
Common Especially
during exacerbations
Uncommon End-stage in some
chronic bronchitis
Hoover’s Sign The inward movement of the lower lateral chest wall during each inspiration—indicates severe hyperinflation
Common—Severe Stage
Uncommon

44Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Assessment Findings (Cont’d)
Emphysema Chronic Bronchitis
Inspection
Pursed-lip breathing Common Uncommon
Cough Uncommon during mild and moderate stage Some coughing
during severe-stage with infection
Classic sign More severe in the
mornings
Sputum Uncommon Little, mucoid
Common Classic sign;
copious amounts, purulent
45Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
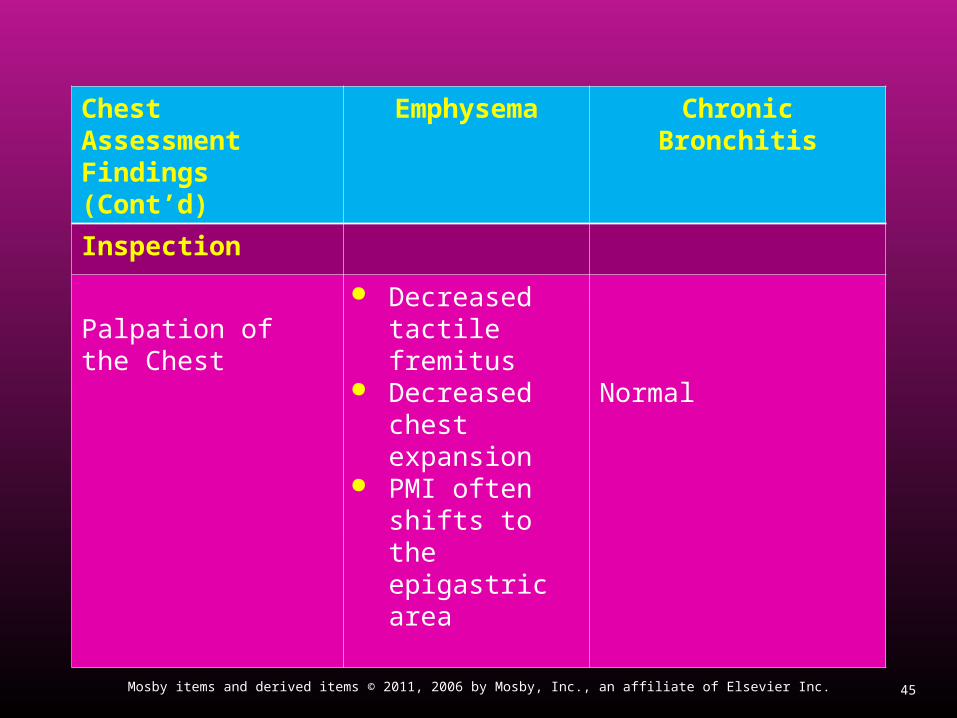
Chest Assessment Findings (Cont’d)
Emphysema Chronic Bronchitis
Inspection
Palpation of the Chest
Decreased tactile fremitus
Decreased chest expansion
PMI often shifts to the epigastric area
Normal

46Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Chest Assessment Findings (Cont’d)
Emphysema Chronic Bronchitis
Inspection
Percussion of the Chest
Hyperresonance Decreased
diaphragmatic excursion
Normal
Auscultation of the Chest
Diminished breath sounds
Prolonged expiration
Diminished heart sounds
Rhonchi Crackles Wheezes
47Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Clinical Data Obtained from Clinical Data Obtained from Laboratory Tests and Special Laboratory Tests and Special
ProceduresProcedures
48Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
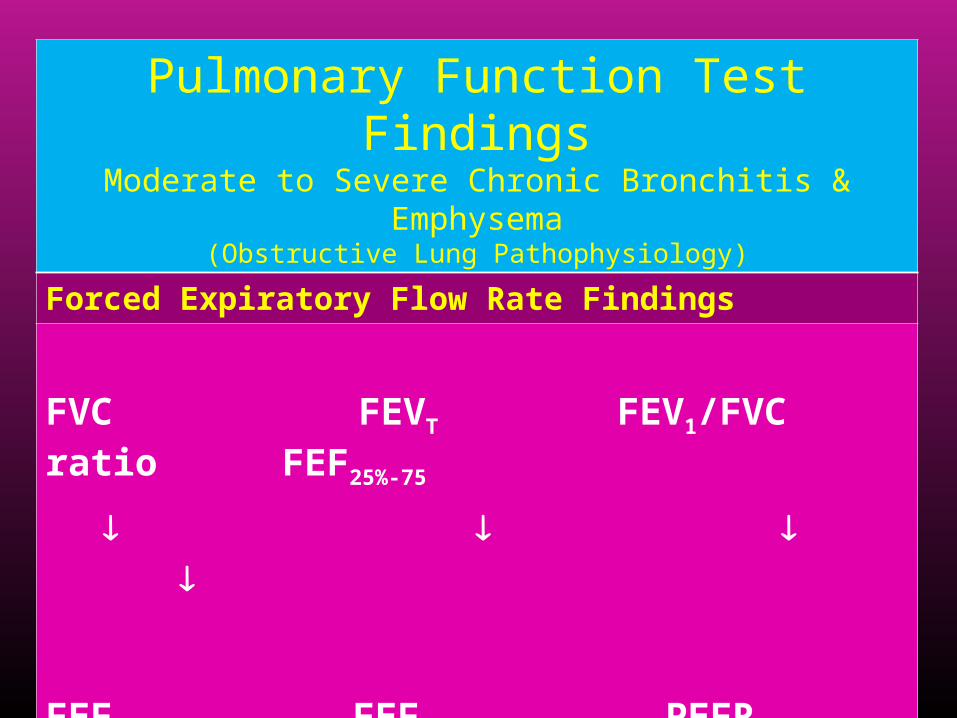
Pulmonary Function Test FindingsModerate to Severe Chronic Bronchitis & Emphysema
(Obstructive Lung Pathophysiology)
Forced Expiratory Flow Rate Findings
FVC FEVT FEV1/FVC ratio FEF25%-75
FEF50% FEF200-1200 PEFR MVV
49Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
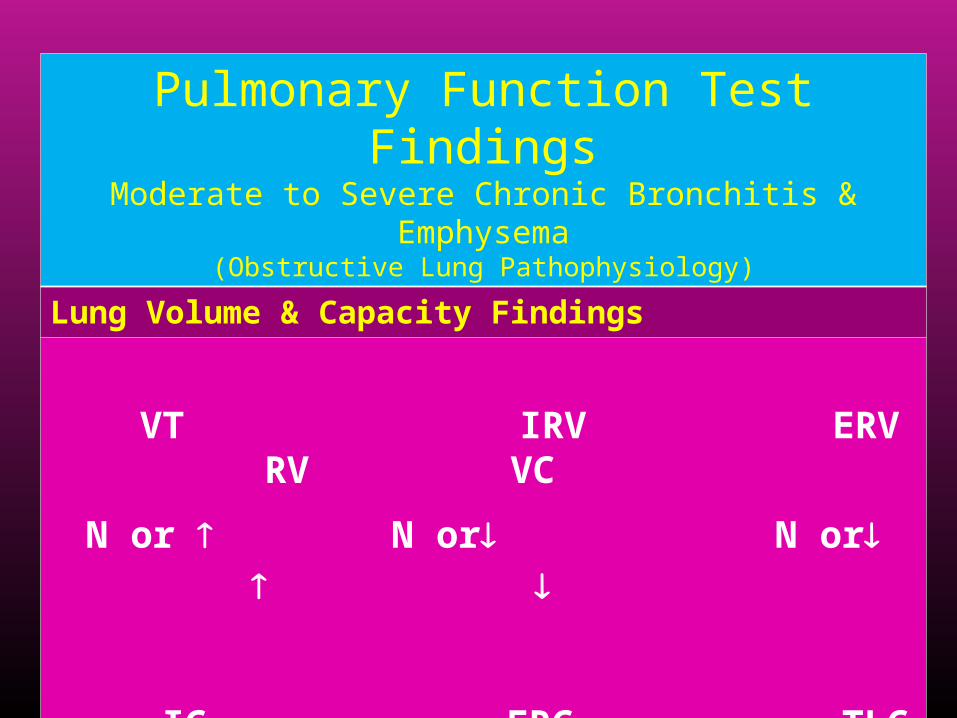
Pulmonary Function Test FindingsModerate to Severe Chronic Bronchitis & Emphysema
(Obstructive Lung Pathophysiology)
Lung Volume & Capacity Findings
VT IRV ERV RV VC
N or N or N or
IC FRC TLC RV/TLC ratio
N or N or N or

50Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Diffusion Capacity (DLCO)Emphysema Chronic Bronchitis
Decreased A decreased DLCO is
a classic diagnostic sign of emphysema
Normal
51Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
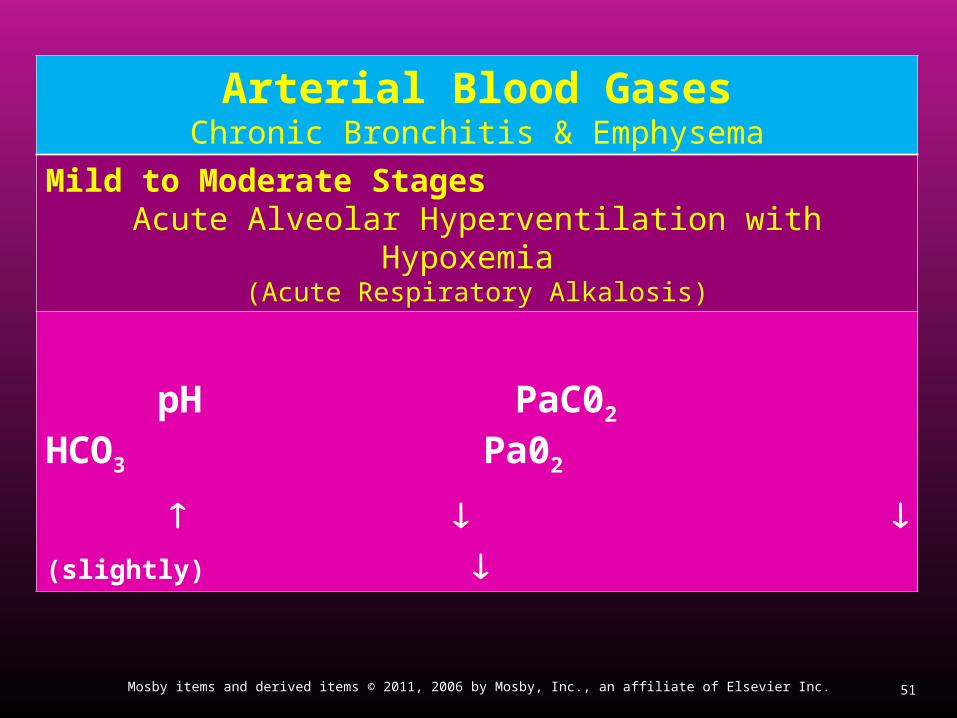
Arterial Blood GasesChronic Bronchitis & Emphysema
Mild to Moderate StagesAcute Alveolar Hyperventilation with Hypoxemia
(Acute Respiratory Alkalosis)
pH PaC02 HCO3 Pa02
(slightly)
52Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
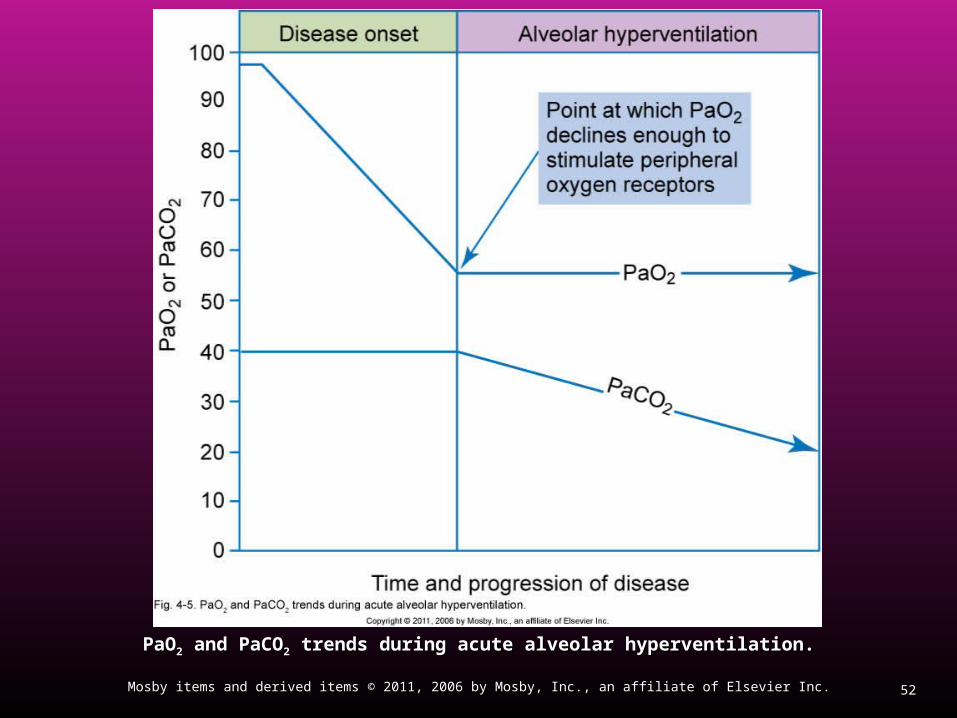
PaOPaO22 and PaCO and PaCO22 trends during acute alveolar hyperventilation. trends during acute alveolar hyperventilation.
53Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
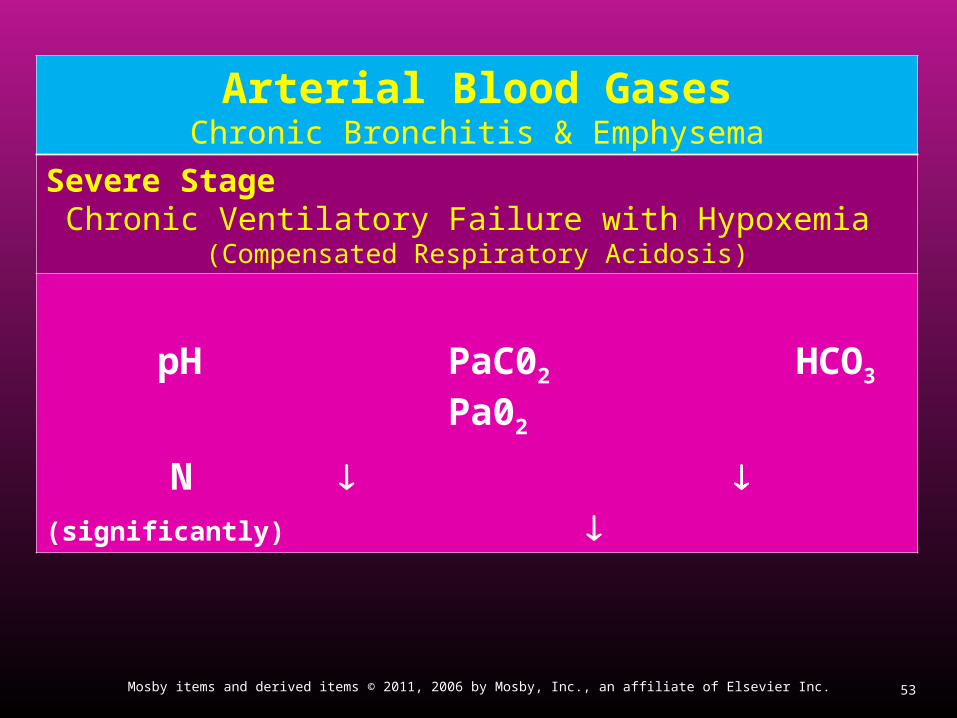
Arterial Blood GasesChronic Bronchitis & Emphysema
Severe StageChronic Ventilatory Failure with Hypoxemia
(Compensated Respiratory Acidosis)
pH PaC02 HCO3 Pa02
N (significantly)

54Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
PaOPaO22 and PaCO and PaCO22 trends during acute or chronic ventilatory failure. trends during acute or chronic ventilatory failure.
55Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Arterial Blood GasesChronic Bronchitis & Emphysema
Acute Ventilatory Changes Superimposed On Chronic Ventilatory Failure
Because acute ventilatory changes are frequently seen in patients with chronic ventilatory failure, the respiratory care practitioner must be familiar with and alert for the following: Acute alveolar hyperventilation superimposed on chronic
ventilatory failure Acute ventilatory failure (acute hypoventilation)
superimposed on chronic ventialtory failure.

56Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Oxygenation IndicesChronic Bronchitis and Emphysema
Moderate to Severe Stages
QS/QT D02 V02 C(a-v)02 02ER Sv02
N N
57Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
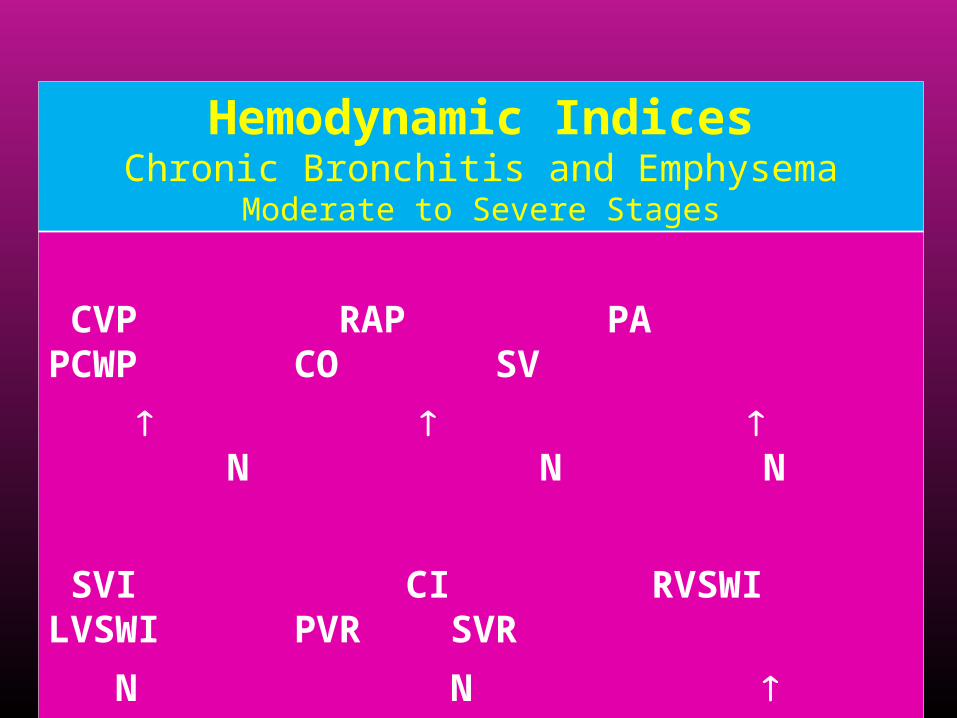
Hemodynamic IndicesChronic Bronchitis and Emphysema
Moderate to Severe Stages
CVP RAP PA PCWP CO SV
N N N
SVI CI RVSWI LVSWI PVR SVR
N N N N
58Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
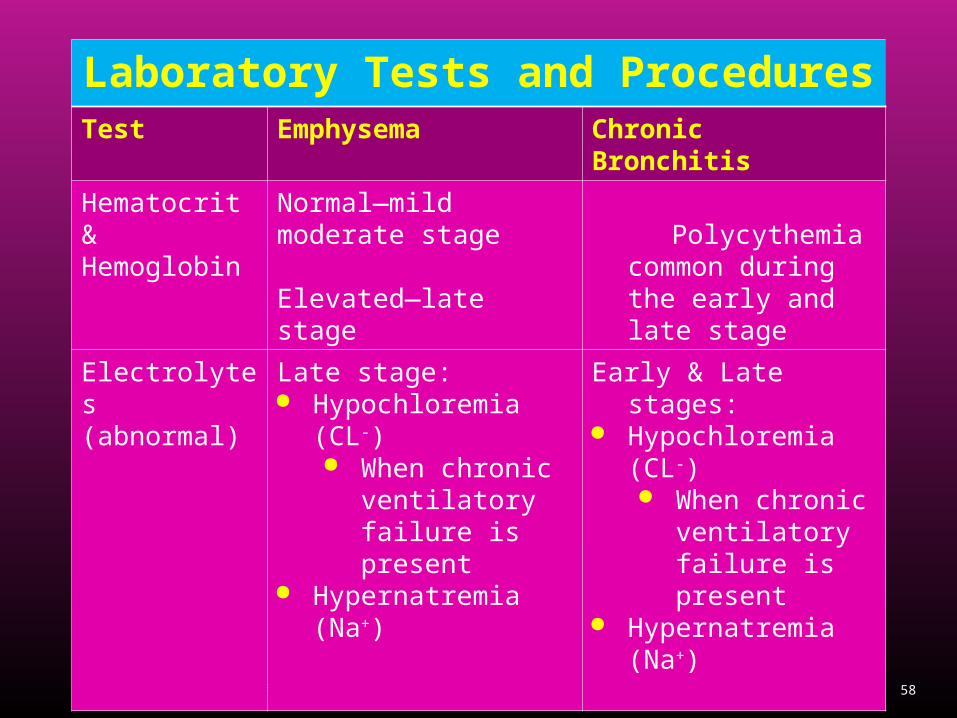
Laboratory Tests and ProceduresTest Emphysema Chronic Bronchitis
Hematocrit & Hemoglobin
Normal—mild moderate stage
Elevated—late stage
Polycythemia common during the early and late stage
Electrolytes(abnormal)
Late stage: Hypochloremia (CL-)
When chronic ventilatory failure is present
Hypernatremia (Na+)
Early & Late stages: Hypochloremia (CL-)
When chronic ventilatory failure is present
Hypernatremia (Na+)

59Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory Tests and Procedures (Cont’d)
Test Emphysema Chronic Bronchitis
Sputum examination(culture)
Normal Streptococcus pneumoniae
Haemophilus influsenzae
Moraxella catarrhalis
60Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
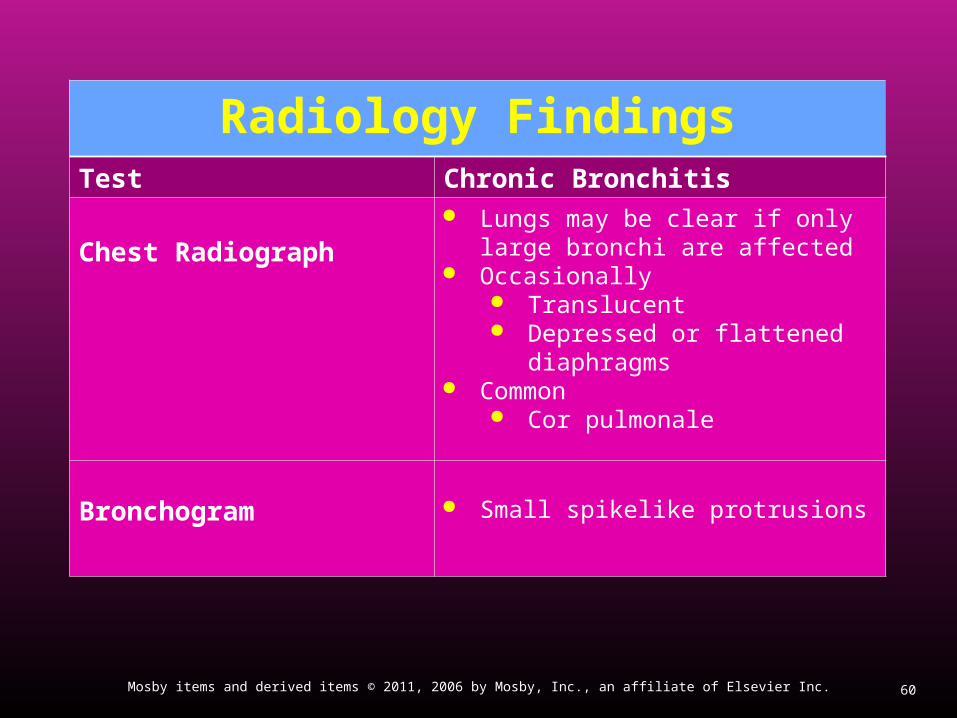
Radiology FindingsTest Chronic Bronchitis
Chest Radiograph
Lungs may be clear if only large bronchi are affected
Occasionally Translucent Depressed or flattened
diaphragms Common
Cor pulmonale
Bronchogram Small spikelike protrusions

61Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 11-5 Chest X-ray film from a patient with chronic bronchitis. Note the translucent (dark) lung fields at the bases, depressed diaphragms, and long and narrow heart.
62Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
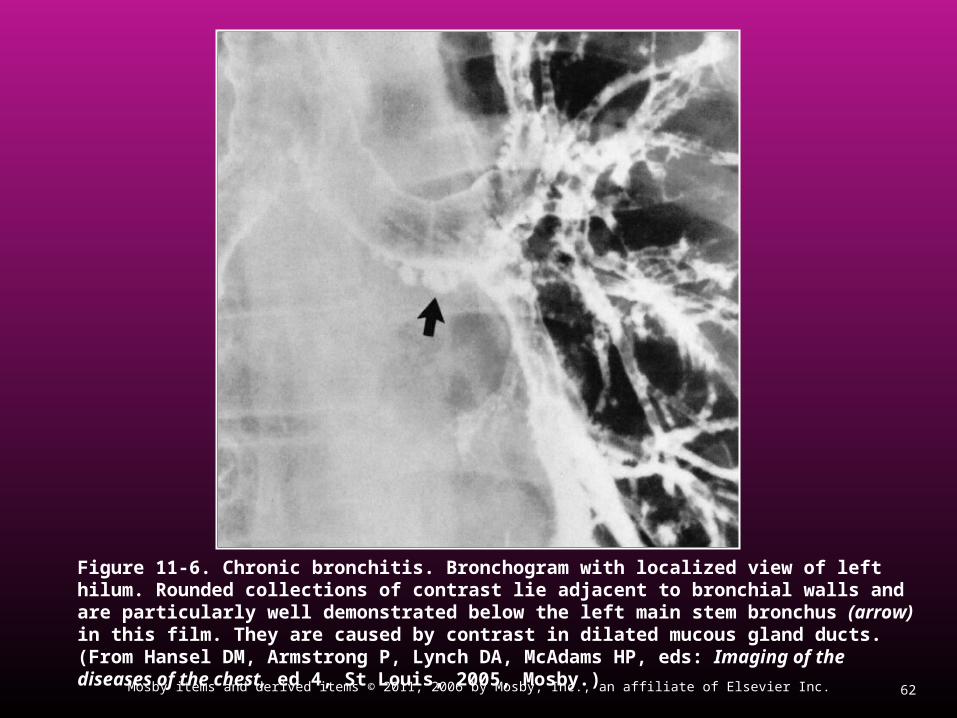
Figure 11-6. Chronic bronchitis. Bronchogram with localized view of left hilum. Rounded collections of contrast lie adjacent to bronchial walls and are particularly well demonstrated below the left main stem bronchus (arrow) in this film. They are caused by contrast in dilated mucous gland ducts. (From Hansel DM, Armstrong P, Lynch DA, McAdams HP, eds: Imaging of the diseases of the chest, ed 4, St Louis, 2005, Mosby.)

63Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Radiology Findings (Cont’d)Test Emphysema
Chest RadiographCommon Translucent Depressed or flattened diaphragms Long & narrow heart Increased retrosternal air spaceOccasionally cor pulmonale
64Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
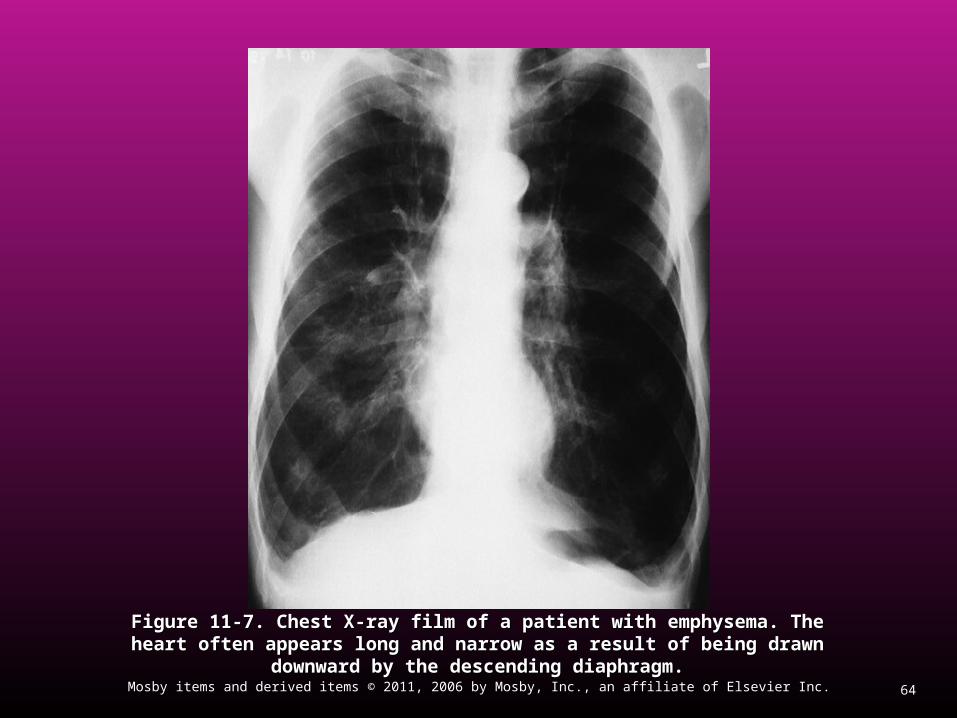
Figure 11-7. Figure 11-7. Chest X-ray film of a patient with emphysema. The heart often appears Chest X-ray film of a patient with emphysema. The heart often appears long and narrow as a result of being drawn downward by the descending diaphragm.long and narrow as a result of being drawn downward by the descending diaphragm.
65Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
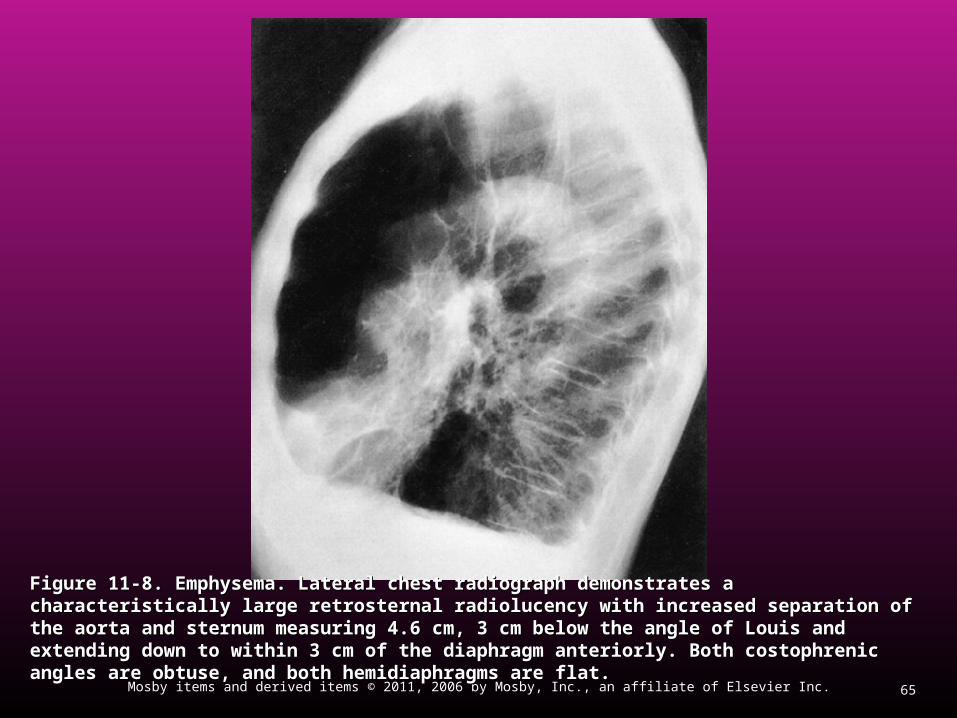
Figure 11-8. Emphysema. Lateral chest radiograph demonstrates a characteristically large Figure 11-8. Emphysema. Lateral chest radiograph demonstrates a characteristically large retrosternal radiolucency with increased separation of the aorta and sternum measuring 4.6 cm, 3 retrosternal radiolucency with increased separation of the aorta and sternum measuring 4.6 cm, 3 cm below the angle of Louis and extending down to within 3 cm of the diaphragm anteriorly. Both cm below the angle of Louis and extending down to within 3 cm of the diaphragm anteriorly. Both costophrenic angles are obtuse, and both hemidiaphragms are flat.costophrenic angles are obtuse, and both hemidiaphragms are flat.
66Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
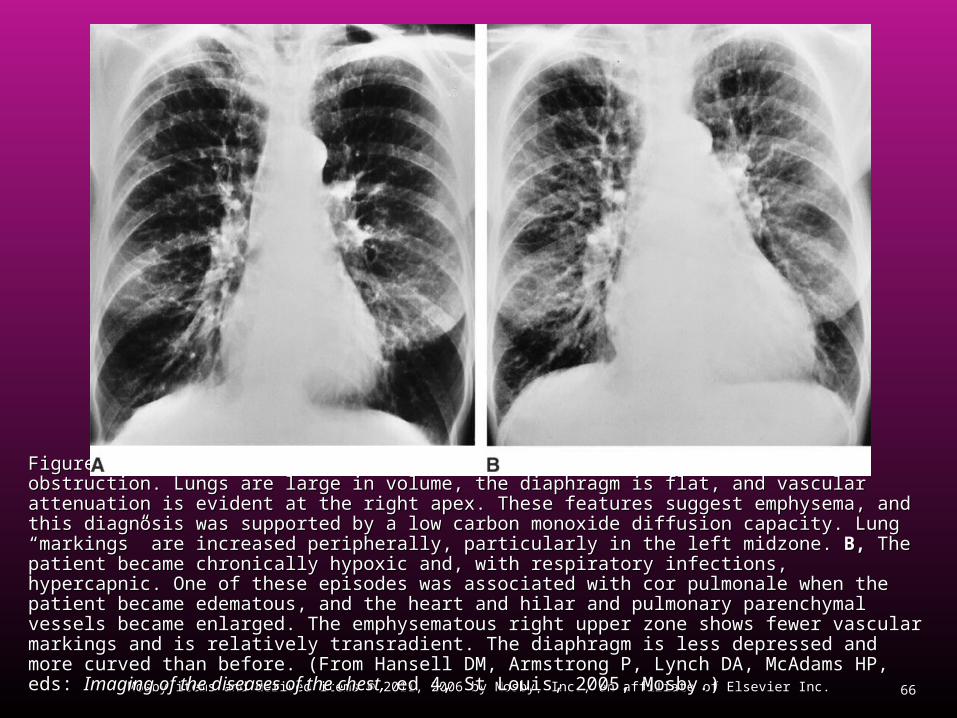
Figure 11-9. Figure 11-9. Cor pulmonale. Cor pulmonale. A,A, A 50-year-old man with chronic airflow obstruction. Lungs are large in A 50-year-old man with chronic airflow obstruction. Lungs are large in volume, the diaphragm is flat, and vascular attenuation is evident at the right apex. These features suggest volume, the diaphragm is flat, and vascular attenuation is evident at the right apex. These features suggest emphysema, and this diagnosis was supported by a low carbon monoxide diffusion capacity. Lung emphysema, and this diagnosis was supported by a low carbon monoxide diffusion capacity. Lung “markings” are increased peripherally, particularly in the left midzone. “markings” are increased peripherally, particularly in the left midzone. B,B, The patient became chronically The patient became chronically hypoxic and, with respiratory infections, hypercapnic. One of these episodes was associated with cor hypoxic and, with respiratory infections, hypercapnic. One of these episodes was associated with cor pulmonale when the patient became edematous, and the heart and hilar and pulmonary parenchymal pulmonale when the patient became edematous, and the heart and hilar and pulmonary parenchymal vessels became enlarged. The emphysematous right upper zone shows fewer vascular markings and is vessels became enlarged. The emphysematous right upper zone shows fewer vascular markings and is relatively transradient. The diaphragm is less depressed and more curved than before. (From Hansell DM, relatively transradient. The diaphragm is less depressed and more curved than before. (From Hansell DM, Armstrong P, Lynch DA, McAdams HP, eds: Armstrong P, Lynch DA, McAdams HP, eds: Imaging of the diseases of the chest,Imaging of the diseases of the chest, ed 4, St Louis, 2005, ed 4, St Louis, 2005, Mosby.)Mosby.)
67Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Global Initiative for Chronic
Obstructive
Lung
Disease
GOLD StandardsGOLD Standards(Excerpts)(Excerpts)
68Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Components of Care: A COPD Management Program
The goals of COPD management include: Relieve symptoms Prevent disease progression Improve exercise tolerance Improve health status Prevent and treat complications Prevent and treat exacerbations Reduce mortality Prevent or minimize side effects from treatment
69Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
A COPD Management Program with Four Components
Assess and Monitor Disease Reduce Risk Factors Manage Stable COPD Manage Exacerbations

70Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 1: Assess and Monitor Disease
Exposure to risk factors, including intensity and duration
Past medical history, including asthma, allergy, sinusitis or nasal polyps, respiratory infections in childhood, and other respiratory diseases
Family history of COPD or other chronic respiratory disease
Pattern of symptom development History of exacerbations or previous hospitalizations
for respiratory disorder.
71Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 1: Assess and Monitor Disease (Cont’d)
Presence of comorbidities, such as obesity, heart disease, malignancies, osteoporosis, and musculoskeletal disorders, which may also contribute to restriction of activity.
Appropriateness of current medical treatments.

72Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 1: Assess and Monitor Disease (Cont’d)
Impact of disease on patient’s life, including limitation of activity; missed work and economic impact; effect on family routines; and feelings of depression or anxiety.
Social and family support available to the patient. Possibilities for reducing risk factors, especially
smoking cessation.

73Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 2: Reduce Risk Factors
Counseling to quit smoking Pharmacotherapy Smoking prevention Occupational exposures Indoor and outdoor air pollution
74Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 11-2: Strategy to Help a Patient Quit Smoking, excerpts
Ask—Systematically identify all tobacco users at every visit.
Advise—Strongly urge all tobacco users to quit. Assess—Determine willingness to make a quit
attempt. Assist—Aid the patient in quitting. Arrange—Schedule follow-up contact.
75Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD, excerpts
Management of stable COPD should be guided by the following general principles:
Determine disease severity Implement a stepwise treatment plan that reflects
this assessment of disease severity Choose treatments according to national and
cultural preferences, the patient’s skills and preferences, and local availability of medications
76Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD excerpts (Cont’d)
Patient education
77Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts
Pharmacologic treatments (Table 11-3 excerpts) β2-agnoists
Short-acting Fenoterol Levalbuterol Salbutamol Terbutaline

78Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Long-acting Formoterol Saleterol
Anticholinergics Short-acting
Ipratropium bromide Oxitropium bromide
Long-acting Tiotropium
79Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Combination short-acting β2-agonists plus anticholinergic in one inhaler Fenoterol/Ipratropium Oxitropium bromide

80Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Methylxanthines Aminophylline Theophylline
81Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Inhaled glucocorticosteroids Beclomethasone Budesonide Flutcasone Triamcinolone
82Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Combination long-acting β2-agonists plus glucocorticosteroids in one inhaler Formoterol/Budesonide Salmeterol/Fluticasone
83Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD Table 11-3 excerpts (Cont’d)
Systemic glucocorticosteroids Prednisone Methyl-prednisolone

84Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 3: Manage Stable COPD excerpts (Cont’d)
Glucocorticosteroids Vaccines Antibiotics Mucolytic Antitussives Non-pharmacologic treatment Rehabilitation Oxygen therapy Surgical treatment
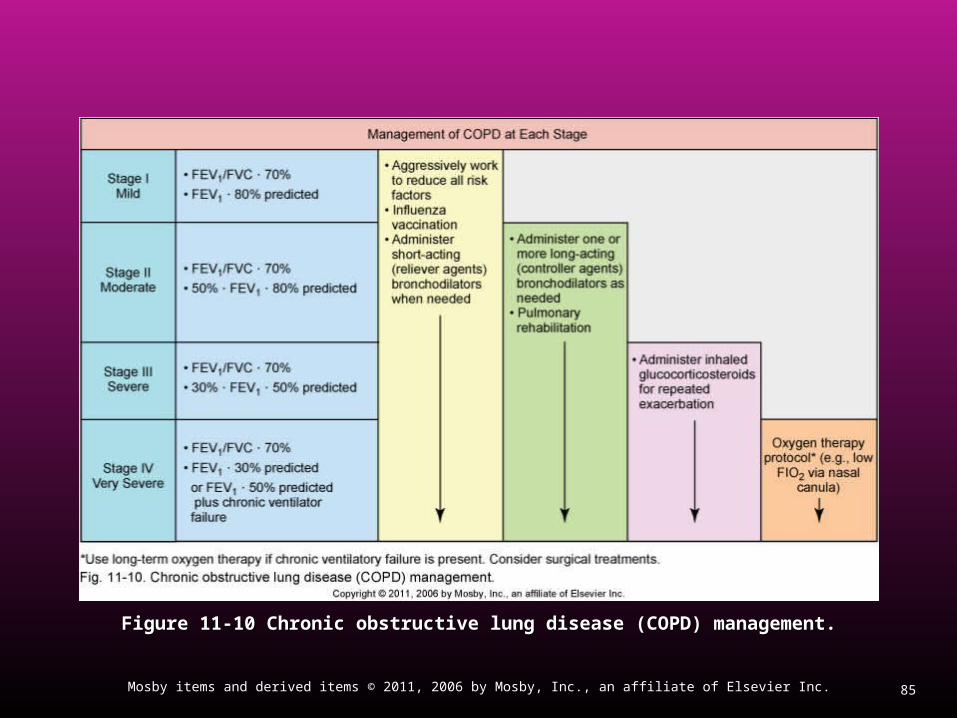
85Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 11-10 Chronic obstructive lung disease (COPD) management.Figure 11-10 Chronic obstructive lung disease (COPD) management.
86Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Component 4: Manage Exacerbation
Exacerbation of COPD is defined as an event in the natural course of the disease characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal-day-to-day variations, is acute in onset, and may warrant a change in regular medication in a patient with underlying COPD
87Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Additional Treatment Considerations for Emphysema
Alpha1 antitrypsin therapy Lung volume reduction surgery Lung transplantation
88Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Classroom DiscussionClassroom Discussion
Case Study 1: Chronic BronchitisCase Study 1: Chronic Bronchitis
89Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Classroom DiscussionClassroom Discussion
Case Study 2: EmphysemaCase Study 2: Emphysema
90Mosby items and derived items © 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Classroom Discussion
Case Study 3: COPD





























