Embed Size (px)
Citation preview

11/16/2011
1
THE GESTATION AND BIRTH OF A
PROVINCIAL LABOUR PARTOGRAM
Partnering for Change
PEI Reproductive Care Program
Partners
Leeanne Lauzon
Perinatal Nurse Consultant
Reproductive Care Program of Nova Scotia
Lily Lee
Provincial Lead, Surveillance
Perinatal Services BC
Diane Boswall
Clinical Specialist – Public Health Nursing
Health PEI

11/16/2011
2
• Descr ibe advantages to shar ing ideas , s t ra teg ies , and
processes (e .g . use o f na t iona l fo rum – Canad ian
Per inata l Programs Coal i t i on)
• Compare exper iences o f p rov inc ia l p rogram
representa t i ves
• Developing, trialing, implementing revised labour partogram
• Descr ibe respec t ive cha l lenges faced & lessons learned
Objectives
Canadian
Perinatal
Programs
Coalition
CPPC
A national organisation of perinatal/reproductive care programs and associations
Committed to fostering and supporting optimal care of childbearing families to facilitate the best possible outcomes for all mothers and babies.
Informal meeting in Nov/1988
Formal meetings since Nov/1989
„National Regionalization Group‟ & „Canadian Perinatal Database Committee‟ formed
1990 – „Canadian Perinatal Regionalization Coalition‟(CPRC)
2000 – „Canadian Perinatal Programs Coalition‟ (CPPC)

11/16/2011
3
CPPC
Voluntary participation
Multidisciplinary
Vehicle for HCPs involved in provincial/regional
reproductive care programs/associations to exchange
ideas and share information:
Database management – health status and performance
measurement (e.g. perinatal audit, benchmarking projects)
Evidence-based practice/policy guidelines
Interdisciplinary professional development
IT accessibility – web-based linkages
Lily’s
experience
•44,000 births per
year
• 50+ sites with
maternity care
11/16/2011
4
Lily’s
experience
The beginning is important
• Setting the stage
• Clarify objectives for the project
• Identify assumptions and expectations
• Review key project deliverables
• Regional representation and champions
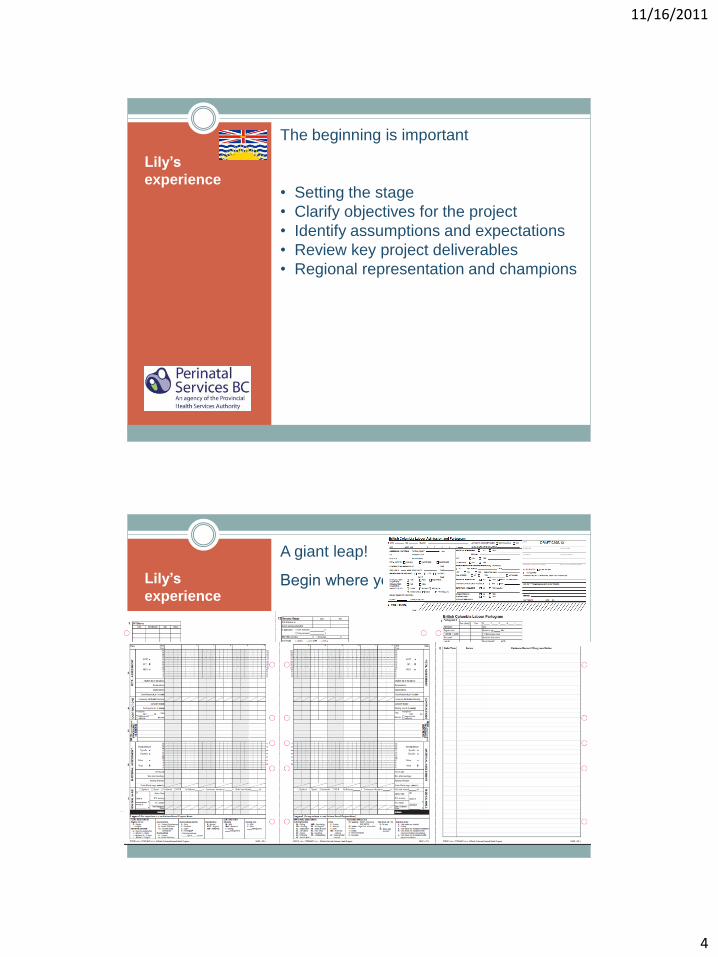
Lily’s
experience
A giant leap!
Begin where you intend to go….

11/16/2011
5
Guiding Principles
Apply to all provincial sites
Incorporate evidence-based care for labour & birth
FHS guidelines
Core competencies and DSTs (CRNBC)
Support normal birth
Adapt to variance charting
Reduce duplication
Enhance early recognition, timely communication and
interventions for changing conditions
Articulate seamlessly with other provincial records
Facilitate data collection and electronic records
Bundle admission and labour charting

11/16/2011
6
Pilot for success Provide tools for learners
Engage the users
Challenges
Context of practice is important
Provincial standardization vs. locally developed forms
Institutional culture and leadership
Feedback from different end users
sometime conflicts

11/16/2011
7
Leeanne’s
experience
9,500 births per
year
10 sites, 3 levels
NS Hospitals where Maternity Care is provided
Leeanne’s
experience
Organization of program:
• clinical
• data collection and management
Focus – work directly with health care
facilities and hospital and community-based
health professionals to promote excellence
in the provision of reproductive care.
Mandatory participation?
11/16/2011
8
Leeanne’s
experience
October 2008 Revisions needed!
Last revision 2000
New evidence for BF and FHS
IWK partogram adapted/adopted by others across province
SCIL elements
Support RNs to narrative charting
Efficient, consistent, legal
Minor revisions made to IWK partogram – beta testing Spring 2009
content
format
Leeanne’s
experience
June 2009
CPPC Halifax
Draft BC partogram shared by Lily
RCP partogram revised over summer
Sept 2009
Beta testing Sept
Format completely changed
Use of abbreviations (pt. safety)
3 month trial at 4 sites
July 2010 – final version
11/16/2011
9
OCTOBER 2011
Feedback one year later…
Leeanne‟s experience
Diane’s
experience
PEI Reproductive Care Program
Prince Edward Island

11/16/2011
10
PEI
PEI Reproductive Care Program
1,400 – 1,500 births per year
2 hospitals where births take place
Births are attended by obstetricians
High risk pregnancies and preterm
babies (< 32 weeks gestation or
requiring complex care) are transferred
to Halifax, NS or Moncton, NB
PEI
PEI Reproductive Care Program
Membership in the Canadian
Perinatal Program Partnership has
been invaluable
“Maternal Database Labour Graphic”
in use since 1996
SOGC‟s Fetal Health Surveillance
(FHS) Guidelines 2007
FHS workshop May 2008
FHS workshop April 2009

11/16/2011
11
PEI
PEI Reproductive Care Program
BC had made many of the edits being
requested by PEI nurses
Supporting document “A Guide to
Completion of the British Columbia
Labour Partogram”
BC developing a Postpartum Clinical
Path and a Newborn Clinical Path –
continuum…
Met with Lily at CPPC meeting
Back to the hospitals
PEI
PEI Reproductive Care Program
Another pilot test
Both hospitals are now using an
adopted, with permission, version of
the February 2010 - British Columbia
Labour Partogram
Moving toward implementation of the
Postpartum Clinical Path and a
Newborn Clinical Path
11/16/2011
12
PEI
PEI Reproductive Care Program
Change is a process & takes time
Be clear: why is change is needed?
More than one change was being
implemented
Engaging staff –finding the
„Champions‟
Adapting if & when possible and
having an „acceptable‟ explanation
when „staying the course‟
Some challenges …
Challenges faced Lessons learned
Getting meaningful, timely
feedback
Consensus is elusive
Outright rejection
Tools may reflect practice
changes/terminology not
yet embraced
Consult, consult, consult,
but place limits on
revisions
Documentation tools
should not take time away
from care provision
Appreciate change theory
Don’t overlook ‘good’ in
the pursuit of ‘perfect’
Post - Partogram Reflections

11/16/2011
13
Thank you!









![HCAHPS and HR: Partnering for Change [webcast]](https://img.pdfslide.net/doc/110x75/5877c8ae1a28ab39588b625f/hcahps-and-hr-partnering-for-change-webcast.jpg)