Embed Size (px)
Citation preview

191
chapter 8
Alterations in Fluid,Electrolyte, andAcid-Base Balance
LEARNING OUTCOMES
1. Define and use the key terms listed in this chapter.
2. Compare and contrast the distribution of fluid in bodycompartments.
3. Differentiate between cations and anions, including expectedconcentrations within specific body compartments.
4. Identify the influences that promote fluid movement between andwithin compartments.
5. Outline the critical components that determine pH.
6. List four potential sources of body fluid loss.
7. Describe the clinical implications of alterations in electrolytebalance.
8. Compare and contrast mechanisms characterizing metabolicacidosis and metabolic alkalosis.
9. Apply concepts of altered fluid, electrolyte, and acid-base balance toselected clinical models.
90309 ch08 (191-216).ps 8/10/06 11:16 AM Page 191

192 Chapter 8
Introduction•
and form molecules. An example of this is the bonding ofthe cation Na� to the anion Cl� to form the moleculeNaCl, or sodium chloride.
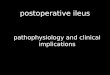
The plasma within the vascular space and the intersti-tial fluid of the extracellular compartment are high insodium, chloride, and calcium; low in potassium, magne-sium, and phosphate; and contain moderate levels of bi-carbonate. The intracellular fluid contains extremely lowlevels of calcium, small amounts of sodium, bicarbonate,and chloride, and moderate amounts of phosphate andmagnesium. Potassium is found in greatest concentra-tions in the intracellular fluid. Figure 8.2 illustrates theconcentrations of electrolytes inside and outside of a cell.
Interstitial volume: 14%
Plasma volume: 5%
Transcellular volume: 1%
Ext
race
llula
r w
ater
: 20
% o
f bod
y w
eigh
t In
trac
ellu
lar
wat
er:
40%
of b
ody
wei
ght
Tota
l bo
dy
wat
er: 6
0% o
f b
od
y w
eig
ht
Tota
l bo
dy
wei
gh
t
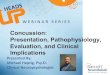
FIGURE 8.1 Body fluid compartments. Extracellular water makes up20% of body weight, and intracellular water makes up 40% of bodyweight.
Remember This?• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
One liter of water weighs 1 kg or 2.2 lb. Fluid gain orloss can be measured by serial (repeated) measures of bodyweight.
Review of Fluid andElectrolyte Balance
The body is mostly fluid, accounting for a significantpercentage of body weight. Total body water can vary bygender, age, and amount of body fat. Sixty percent of thebody is comprised of fluids distributed between twocompartments: 40% is located in the intracellular com-partment and 20% is located in the extracellular com-partment (Fig. 8.1). The intracellular compartmentconsists of the fluid inside the cells, containing approxi-mately two thirds of the body water and accounting for40% of body weight. The smaller extracellular com-partment contains the remaining one third, or 20%, ofbody fluid in the interstitial tissue and plasma outside thecells. Fluid in the plasma compartment accounts for 5%of body weight, and the interstitial fluid accounts for 14%of body weight. A third, minor extracellular compart-ment is the transcellular compartment, separated by alayer of endothelium. The fluid in this compartment iscontained in body spaces such as the spinal cord, peri-toneal, pleural, pericardial, and joint spaces. This rela-tively small compartment of fluid is often referred to as a“third space” because it is unavailable for exchange be-tween the other extracellular compartments.
ELECTROLYTE BALANCE
Body fluid contains dissolved particles known as elec-trolytes. Electrolytes are electrically charged particles,or ions. Ions with a positive charge are called cationsand include sodium (Na�), calcium (CA2�), hydrogen(H�), and potassium (K�). Negatively charged ions arecalled anions, and include chloride (Cl�), bicarbonate(HCO3
�), sulfate (SO42�), and phosphate (PO4
3�).Ions with opposite charges are attracted to each other
Have you ever been thirsty on a hot, sunny day? Whatabout after a long workout or after eating a bag of pret-zels? Thirst is the way the body communicates the needto increase fluid intake. Fluid intake must make up forfluid lost through sweating, breathing, and urinating. Inaddition to fluids, electrolytes and specialized com-pounds that control acid-base balance are necessary for
cell and organ functioning. This chapter reviews themechanisms involved in the regulation of fluid, elec-trolyte, and acid-base balance. It also covers alterations inthe regulation of these mechanisms and the clinical con-sequences that may result. Selected clinical models thathighlight specific alterations are presented to allow thestudent to apply the learned concepts.
90309 ch08 (191-216).ps 8/10/06 11:16 AM Page 192

Alterations in Fluid, Electrolyte, and Acid-Base Balance 193
Anion Gap
The anion gap is a calculation of the major measuredcations and anions in the plasma, providing an indicationof electrolyte and acid-base balance. The clinical calcula-tion of anion gap uses sodium (major measurable cation),chloride, and bicarbonate (major measurable anions), andit reflects the difference between the unmeasurable anions,including phosphates, sulfates, organic acids, and pro-teins. The difference in the concentrations of the cationsodium (140 mEq/L) and the anions chloride (102mEq/L) and bicarbonate (26 mEq/L) in the blood isknown as the anion gap. In other words, Na� � (Cl� �HCO3
�) � 140 mEq/L � (102 mEq/L � 26 mEq/L) �anion gap. Therefore, the anion gap is 12 mEq/L with avariation of 2 mEq/L, which results in a normal range of10 to 14 mEq/L. The anion gap serves as a measurementof acid-base balance. Occasionally, other electrolytes maybe considered, resulting in a different reference range dis-tinguishing a normal from an abnormal value. An exam-ple of this variation includes the addition of the cationpotassium to sodium, which changes the anion gap to 16mEq/L (range 14 to 18 mEq/L).
Electrolyte Transport
The cell membrane forms a barrier between the intracel-lular and extracellular compartments. Movement ofelectrolytes across the cell barrier occurs by transportmechanisms, some that require energy (active transport)and others that follow gradients determined by charge/electrical or concentration (passive transport), asdetailed in Chapter 2.
Stop and Consider
Calcium is one of the electrolytes important in muscle contrac-tion. Large amounts of calcium must be available inside the cell topromote the development of tension in muscle cells. What musthappen to intracellular calcium levels for this to occur?
Remember This?• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
Laboratory analysis requires plasma or serum formany diagnostic tests. Plasma is the noncellular portion ofcirculating blood, containing nutrients, electrolytes, gases,albumin, clotting factors, wastes, and hormones. Serum isthe fluid portion of the blood that remains after removal ofthe fibrin clot and blood cells. Serum retains antibodies butno blood cells, platelets, or fibrinogen.
From the Lab
The amount of electrolytes in body fluids is describedby the concentration of solute in a particular volume of fluid.Measurements are often described as milligrams perdeciliter (mg/dL), the solute weight in one-tenth of a liter(dL), also equivalent to 100 microliters (�l) of solution. Elec-trolytes can also be expressed in measurements of mil-liequivalents per liter (mEq/L), which considers the chargeequivalency for a specific weight of electrolyte. Based onelectroneutrality, cations and anions must be balanced inthe body. The combination of anions and cations resultsfrom the attraction based on ionic charge rather thanmolecular weight. Therefore, 1 mEq of sodium has the samenumber of charges as 1 mEq of chloride. Clinical measure-ments of electrolytes are determined by their concentrationin the plasma.
+ – +
+ +
+ + + +
+ +
+
+
+ + +
+ +
+
+ +
+ +
+
+ + +
+
– –
–
–
–
–
–
– –
–
– –
–
–
– – – –
– –
–
–
– –
–
– –
+
+
–
+ –
+ –
+ –
+ –
+ –
Equal +,–
Cytosol Extracellular fluid
Membrane
Equal +,–
Equal +,–
Distribution of electrical charge across the membrane. Electroneu-trality of cations and anions promote balanced charges across themembrane. (Image from Bear MF, Connors BW, Paradiso MA. Neu-roscience: Exploring the Brain. 3rd Ed. Baltimore: LippincottWilliams & Wilkins, 2006.)
135-145 mEq/L 10-14 mEq/L
98-106 mEq/L 3-4 mEq/L
7-10 mEq/L 24-31 mEq/L
8.5-10.5 mg/dL < 1 mEq/L
140-150 mEq/L 3.5-5 mEq/L
Na+
K+
Cl-
Ca2+ HCO3
-
Extracellular
Intracellular
FIGURE 8.2 Intracellular and extracellular distribution of ions.
90309 ch08 (191-216).ps 8/10/06 11:16 AM Page 193

194 Chapter 8
FLUID BALANCE
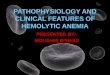
Body fluid volume is regulated directly in the extracellu-lar compartment and indirectly in the intracellular com-partment by the kidneys. This process involves water andion movement across the cell membranes of the renaltubules and close association with the vasculature of thekidneys (Fig. 8.3).
Fluid Transport
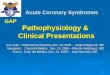
Water is able to move between compartments throughspecial channels in the cell membrane, called aquapor-ins. Movement of water is stimulated by a concentrationgradient, moving to an area of higher concentration ofparticles (less water content) from an area of lowerconcentration of particles (more water content). Thisprocess, osmosis, is regulated by the concentration ofparticles that do not diffuse across the semipermeablemembrane. Some characteristics that make particlesnondiffusible include large size or lipid solubility. Os-motic pressure is generated as water moves through themembrane. Table 8.1 summarizes active and passivetransport mechanisms.
Fluid also moves between extracellular compart-ments, with forces promoting fluid movement balance.Hydrostatic forces (pressure of fluid) can promote
movement of fluid based on the pressure gradient, alsoknown as filtration pressure. The pressure of the bloodon the capillary walls (semipermeable membranes) canforce fluid movement from within the vessel to the inter-stitial space; this movement is called filtration. Capillaryfiltration pressure is countered by interstitial fluid pres-sure, which opposes fluid movement out of the capillary.Conversely, capillary osmotic pressure caused by pro-teins or other molecules can pull fluid from the intersti-tial space into the intravascular space; this movement iscalled reabsorption. This force is countered by tissue os-motic pressure, which opposes such movement (Fig.8.4). In vessels with intact endothelial cells, fluid movesout of the capillary at the arteriolar end of the capillary
Glomerular capillaries
Efferent arteriole
Afferent arteriole
Venule
Cells and protein remain in blood
Proximal convoluted tubule
Distal convoluted tubule
Collecting duct
Drugs
(Aldosterone effect) Bicarbonate
Water (ADH effect)
Water (by osmosis)
Peritubular capillaries
Glucose
Amino acids
Na+
Na+
Na+
H+ K+
Cl-
Water
Filtration
Reabsorption
Reabsorption Secretion
Des
cend
ing
loop
Thi
ck a
scen
ding
loop
Loop of Henle
FIGURE 8.3 Renal regulation of fluid and electrolytes. Filtration, reabsorption, and secretion processes are illustrated between the renal structures andassociated vasculature. Note the movement of ions and water along the tubules. ADH, antidiuretic hormone. (Image modified from Premkumar K. TheMassage Connection: Anatomy and Physiology. Baltimore: Lippincott Williams & Wilkins, 2004.)
Remember This?• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
An osmole is the unit of measure reflecting the os-motic activity that nondiffusible particles exert in pullingwater from one side of the semipermeable membrane tothe other. Osmolarity is the osmolar concentration in 1 Lof solution (mOsm/L) and is used when referring to fluidsoutside the body. Osmolality is the osmolar concentra-tion in 1 kg of water (mOsm/kg of H2O), and is used to de-scribe fluids within the body.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 194

Alterations in Fluid, Electrolyte, and Acid-Base Balance 195
Water
A B
ATP
ADP
TABLE 8.1
Mechanisms of Membrane Transport
Type of Stimulus for Outcome ofTransport Mechanism Transport Transport Transport
Diffusion Passive Chemical or electrical Particles are evenlygradient distributed across the
membrane
Osmosis Passive Concentration gradient Flow of water is directedby osmotically activeparticles
Facilitated Diffusion Passive Binding of substance A carrier system movesto transporter particles across the
membrane
Active Transport Active Proteins using energy Energy (ATP) movesto pump ions across particles against athe membrane gradient across the
membrane
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 195

196 Chapter 8
bed where the hydrostatic pressure is greater, and itmoves back in at the venous end where oncotic pressureis greater. The small amount of fluid that remains in theinterstitium is removed by the lymphatic system and re-turned to the circulation.
Fluid Regulation
Mechanisms regulating total body water include thosethat promote thirst and water excretion. Neural and hor-monal mechanisms work in concert to attain or maintainfluid balance.
Mechanisms to Promote Fluid Intake
Thirst is an important mechanism contributing to in-creased fluid intake. Thirst is characterized by a desire todrink fluids high in water content, which is prompted byuncomfortable sensations in the mouth and pharynx.1
The sensory neurons known as osmoreceptors in thehypothalamic thirst center that promote thirst are acti-vated by:
• Cellular dehydration resulting from increased extra-cellular osmolality
• Decrease in blood volume
Stop and Consider
Are there any risks to drinking too much water?
Stretch receptors in the carotid and aorta (high-pres-sure baroreceptors) and the left atrium (low-pressurebaroreceptors) sense change in arterial blood pressure
and contribute to the development of thirst. The hor-mone, angiotensin II, also indirectly contributes to thirstin response to low blood volume and low blood pressure.The renal hormone, renin, is released from the kidneysand serves as an enzyme, converting angiotensinogen toangiotensin I. Angiotensin I is converted to angiotensin IIby angiotensin-converting enzyme, primarily in thelungs. Angiotensin II also regulates aldosterone, a hor-mone produced in the adrenal cortex. The increase insodium retention that results from the effects of aldos-terone may have the indirect effect of increasing thirst.
Antidiuretic hormone (ADH) regulates fluid volumeby controlling excretion of total body water. Produced inthe hypothalamus, ADH is transported to the posteriorpituitary where it is stored until needed. Production andrelease of ADH is stimulated by hypothalamic osmore-ceptor detection of increased blood osmolality. Alsoknown as vasopressin, ADH works at the level of the kid-ney to promote the reabsorption of water via aquaporinsfrom the renal-collecting ducts into the vasculature, re-ducing fluid loss through decrease in urine output. Themechanisms that promote fluid intake are illustrated inFigure 8.5.
Mechanisms to Promote Fluid Excretion
The most common method for increasing fluid excretionis the use of diuretics. Diuretics are drugs that increaseurine production. The kidneys are the target of the ef-fects of diuretics, which are designed to decrease reab-sorption of sodium in the kidney. This mechanism iseffective because water moves together with sodium.
Different types of diuretics work on different struc-tures of the kidney. The loop diuretics reduce reab-sorption of sodium in the thick ascending loop of Henle,causing a decreased osmolality in the interstitial fluid ofthe collecting ducts and impair the ability to concentrateurine at the loop. Thiazide diuretics prevent NaCl re-absorption in the distal convoluted tubule. This action iscoupled with increased potassium loss in the urine anduric acid retention. Potassium-sparing diuretics, alsoknown as aldosterone antagonists, reduce sodium reab-sorption in the late distal tubule and collecting tubule,functions regulated by aldosterone. The effects of aldos-terone at this site are inhibited, promoting excretion of
Filtration Reabsorption
Pif Pif
Pc Pc
Capillary
Interstitium
Lymphatics
Vein Artery
FIGURE 8.4 Forces for fluid movement across the capillary. Pc is the cap-illary lumen hydrostatic pressure, and Pif is the interstitial hydrostatic pres-sure. When Pc is greater then Pif, filtration processes are dominant. WhenPif is greater than Pc, reabsorption processes are “favored” or dominant.
RESEARCH NOTES In addition to chemical diuretics, cer-tain foods can have diuretic effects. The American Heart As-sociation has long advocated the Dietary Approaches toStop Hypertension (DASH) diet for blood pressure-loweringeffects. The DASH diet is rich in fruits and vegetables. Al-though it was recognized that the DASH diet lowered bloodpressure, the explanation for these effects was unknown un-til a group of researchers determined that the DASH dietpromoted salt excretion and increased urine production,similar to the mechanism of action of diuretic drugs.2
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 196

Alterations in Fluid, Electrolyte, and Acid-Base Balance 197
sodium and water. The simultaneous effect of increasedpotassium reabsorption prevents the potential for exces-sive loss associated with other types of diuretics. The se-cretion of hydrogen ions may be altered, increasing therisk for metabolic acidosis, discussed later in this chapter.
TONICITY
The osmotic pressure or tension of a solution is known astonicity.1 Tonicity is determined by solutes that cannotcross the semipermeable cell membrane, producing anosmotic force that transports water. Cell size can be af-fected by tonicity, promoting fluid movement in or out ofcells. Hypertonic solutions have a greater osmolality
than the intracellular fluid (ICF). When cells are in a hy-pertonic solution in which the extracellular osmotic forceis greater, water moves out of the cell causing cells toshrink. Hypotonic solutions have a lower osmolalitythan the ICF. The osmotic forces outside the cells are lessthan that of the intracellular environment, promoting wa-ter movement into the cell and causing cells to swell. Anexample of cellular changes in response to sodium con-centration is shown in Figure 8.6, with hypernatremiaserving as an example of a hypertonic solution, and hy-ponatremia representing a hypotonic solution. Cells in anisotonic solution, which has the same osmolality as theICF, are unchanged with osmotic forces balanced withinand outside of the cell.
Blood volume Serum osmolality
( Thirst and water intake)
Arterial BP (stimulates baroreceptors)
Sympathetic discharge
Renal perfusion
Renin release ( GFR) H2O & Na+
filtered by kidney
Angiotensin I & II
Aldosterone by adrenal cortex
ADH release into bloodstream from storage
in posterior pituitary
Reabsorption of H2O by kidneys
Urine excretion Na+ & H2O excretion; blood pressure
Circulating volume of H2O & Na+ (loss of K+)
ADH production in hypothalamus (osmoreceptors)
Blood volume Serum osmolality
Concentratedurine excreted
Diuresis results
Stimulates
Inhi
bits
Stim
ulates
FIGURE 8.5 Fluid regulation cycle. Negative feedback mechanisms promote regulation of body fluid. Decreased blood volume and increased serumosmolality promote water intake via thirst. Decreased blood pressure (BP) increases sympathetic nervous stimulation, triggering reduced renal perfu-sion and the renin-angiotensin-aldosterone system (RAAS). Reabsorption of water through the actions of antidiuretic hormone (ADH) combined withreduced sodium and water secretion through the effects of aldosterone leads to increased circulating volume of water and sodium. Increased bloodvolume and low serum osmolality inhibit ADH production, promoting diuresis. (Image from Smeltzer SC, Bare BG. Textbook of Medical-Surgical Nurs-ing. 10th Ed. Philadelphia: Lippincott Williams & Wilkins, 2003.)
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 197

198 Chapter 8
Review of Acid-Base Balance
Regulation of acids and bases is critical to the meta-bolic activities of the body. A narrow physiologic pHrange is required for the function of cells, tissues, andorgans.
REGULATION OF ACID AND BASE
Acids are substances that donate hydrogen ions, andbases are substances that accept hydrogen ions. Weakacids in plasma include albumin and inorganic phospho-rus. Strong ions almost completely dissociate, or sepa-rate, when in solution. In plasma, the strong cationsinclude Na�, K�, Ca2�, and Mg2�. The strong anionsare Cl� and lactate.3 The ratio between acids and basesin the extracellular fluid of the body are closely regulatedto provide a favorable environment for metabolic cellularfunctions. The clinical measurement of this balance isknown as pH. Hydrogen ion concentration representsthe inverse of the pH, so that when the pH is low, thereis a high amount of H�; when the pH is high, there is alow amount of H�.
Buffer Systems
The balance of pH involves buffer systems (mixing ofacid and base to resist pH change), which are responsi-ble for trading stronger acids and bases for weaker vari-eties. Acid-base balance is regulated by the actions ofthree major buffer systems, working together to respondto conditions threatening acid-base balance. The onset ofaction in each system varies, leading to rapid responsesto correct acute insults, followed by more prolonged cor-rection via a slower onset of action. These buffer systemsinclude:
1. Plasma buffer system: Reacts within seconds inresponse to hydrogen ion concentration
2. Respiratory buffer system: Reacts within minutes toexcrete CO2 through change in respiratory rate
3. Renal buffer system: Reacts within hours to daysthrough the production, absorption, and excretionof acids, bases, and ions
The kidneys are the primary regulators of the balancebetween acids and bases. This regulation is accom-plished through generating, buffering, and eliminatingacids and bases. The secretion of hydrogen ions, reab-sorption of sodium, and production of ammonium ionscontribute acids. Reabsorption of basic bicarbonate ionsare among the ways the kidneys work to obtain a pH be-tween 7.35 and 7.45, thereby promoting optimal cellularfunctioning. A pH of 7.4 requires a 20:1 ratio of bicar-bonate (HCO3
�) base to carbonic acid (H2CO3). Ratherthan the absolute concentration of a substance, the ratioof substances provides the balance, which serves as thedeterminant of pH.
H2CO3 is an acid that is balanced with carbon dioxide(CO2) gas; both are considered volatile because theycan be excreted by the lungs. Because CO2 is excreted bythe lungs, respiratory function contributes to H2CO3
levels. The respiratory regulation of acid-base balance isdiscussed in detail in Chapter 12. Circulating fixed acidsare considered nonvolatile because they are unable to beexcreted by the lungs and require buffering and excre-tion by the kidneys. The kidneys contribute to plasmaregulation of HCO3
� by the reabsorption of HCO3�
from the urine into the bloodstream, or by the elimina-tion of buffered hydrogen ions.
The ions involved in acid-base balance are reflected inthe determination of the anion gap, despite the actualcalculation being limited to measurable ions, cations, and
A. Hyponatremia: Na+ less than 130 mEq/L
B. Hypernatremia: Na+ greater than 150 mEq/L
H2O
FIGURE 8.6 Effect of tonicity on cell size. A. The cell swells as water ispulled in from extracellular fluid. B. The cell shrinks as water is pulled outinto extracellular fluid.
Remember This?• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
The calculation of pH is based on the Hendersonequation, using the negative logarithm of the dissociationconstant and the logarithm of HCO3
� to H2CO3 ratio to cal-culate pH. The equation reads pH � 6.1 � log10 (ratioHCO3
�: H2CO3).
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 198

Alterations in Fluid, Electrolyte, and Acid-Base Balance 199
anions, including sodium, chloride, bicarbonate, and, oc-casionally, potassium. An increased anion gap (morethan 12 mEq/L) may indicate acidosis due to the buildupof anions or metabolic acids in the plasma. Alkalosis maybe detected by an anion gap of less than 10 mEq/L be-cause of a decrease in unmeasured anions (i.e., albumin)or an increase in unmeasured cations. A more specificdetermination of acid-base balance can be made by de-termining the strong ion difference (SID). Three com-ponents that determine SID are:
1. CO2 tension2. Strong ion difference (fully dissociated ions at
physiologic pH) equaling the sum of sodium,potassium, calcium, and magnesium minus thesum of chloride, lactate, sulphate, ketoacids, andfatty acids
3. Titratable anions at physiologic pH, includingphosphate, albumin, and globulins
The strong ion difference considers the same param-eters as with the calculation of anion gap, but it also in-cludes other variables that may influence pH and alsopoint to the underlying cause of the imbalance.
Protein Buffer System
Buffer systems must respond to the moment-to-momentchanges to retain pH in the narrow range necessary foroptimal cell function. Proteins serve as the largest buffer-ing system and mainly involve the proteins albumin andplasma globulins in the vascular compartment. Able tofunction as either acid or base, proteins are referred to asamphoteric. These protein buffers that can both acceptor donate H� ions are often found intracellularly. TheH� and CO2 ions that are released because of these re-actions can then freely diffuse across cell membranes.
Bicarbonate Buffer System
The weak acid H2CO3 and the weak base sodium bicar-bonate (NaHCO3) are the primary substances involvedin the bicarbonate buffer system (Fig. 8.7). The kidneycan regulate the amount of HCO3
�, conserving it whenexcess acid is added and excreting it in the presence ofexcess base.
Potassium-Hydrogen Exchange
Ionic exchange of the potassium (K�) and hydrogen (H�)cations contributes to regulation of acid-base balance. Ex-cess H� in the extracellular compartment can diffuseacross the cell membrane inside the cell for buffering. Theentry of H� prompts the exit of K� from within the cell tothe extracellular space, potentially resulting in hyper-kalemia. Conversely, if the extracellular level of K� falls, asin the case of hypokalemia, K� then moves out of the cellin parallel with H� entry into the cell, decreasing extracel-lular concentrations of H�, thereby increasing pH. Theregulation of acid-base and electrolyte balance is closelytied in an effort to maintain homeostasis.
Tubular Buffer Systems
The tubule structures of the kidney are protected by theregulation of urine pH. Intratubular buffers bind un-buffered H� to maintain local pH for kidney cell func-tion. The phosphate buffer system uses HPO4
2� to bindH�, resulting in H2PO4
�, allowing the kidney to secreteH� ions. The ammonia buffer system promotes excre-tion of H� and generates HCO3
� in a series of ion ex-changes between ammonium (NH4
�) and HCO3�. The
secreted H� ions combine with ammonia (NH3) and arethen eliminated in the urine as NH4Cl.
Stop and Consider
What other organ systems are important in the regulation of fluid,electrolyte, and acid-base balance?
A. HCL + NaHCO3 H2CO3 + NaCl
B. NaOH + H2CO3 NaHCO3 + H2O
FIGURE 8.7 Bicarbonate buffer systems. A. The strong acid HCl is substi-tuted for the weaker acid H2CO3 through a reaction with the weak baseNaHCO3. B. The strong base sodium hydroxide (NaOH) is substituted forthe weak base NaHCO3 through a reaction with the weak acid H2CO3.
From the Lab
Arterial blood gas (ABG) analysis is the lab test used todetermine acid-base balance. Anion gap, base excess ordeficit, CO2 and HCO3
� levels, and pH can be measured in anarterial blood sample. These variables not only determinebalance but point to causes that might result in altered bal-ance. Base excess or deficit represents the amount offixed acid or base needed to achieve a pH of 7.4 in the bloodsample.
RECOMMENDED REVIEW
To apply concepts of altered fluid, electrolyte, and acid-basebalance, review the role of the kidney in regulation of thisprocess in your anatomy and physiology textbook. Pay spe-cial attention to the anatomy of the kidney and the special-ized functions of these structures. Mechanisms involvingfluid and electrolyte transport within and between com-partments should also be reviewed.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 199

200 Chapter 8
Altered Fluid Balance
The imbalance of hydrostatic and osmotic forces can re-sult in alterations in fluid balance. Total body fluid canalso be altered by increases or decreases in fluid ingestionand excretion. Excretion of bodily fluids, such as urine,emesis, sweat, or blood, as well as insensible fluid lossduring respiration, can significantly alter fluid balance.
WATER CONTENT
Alterations in water and sodium can affect total bodyfluid balance. Hypervolemia is an excessive increase offluid in the extracellular compartment. Decreased vascu-lar volume is known as hypovolemia, often the result ofinadequate fluid intake or excessive excretion.
Hypovolemia
Hypovolemia is a deficit of body fluid volume. Causes ofhypovolemia can be attributed to excessive body fluidloss, reduction of fluid intake, or loss of fluid to a thirdspace resulting in decreased extracellular fluid volume.Decreased intravascular volume results in decreased cap-illary hydrostatic pressure. Blood circulation and trans-port of oxygen and nutrients to tissues may be impaired.
Clinical manifestations of hypovolemia, from least tomost severe, include:
• Thirst
• Dry mucous membranes
• Weight loss
• Flattened neck veins
• Diminished skin turgor (fullness) (Fig. 8.8)
• Prolonged time for capillaries to refill after blanch-ing (more than 3 seconds)
• Decreased urine output
• Increased heart rate
• Decreased blood pressure
• Altered level of consciousness
The body attempts to compensate with physiologic re-sponses to counter the manifestations of hypovolemia.Decreased blood flow to the kidneys triggers the activationof the renin-angiotensin-aldosterone system (RAAS), in-creasing sodium and water reabsorption. Decreased bloodpressure sensed by baroreceptors stimulates the sympa-thetic nervous system to increase heart rate, constrict ar-teries, and increase contractility of the heart. The expectedresponse to compensate for decreased intravascular fluidvolume is increased cardiac output and mean arterial pres-sure. Antidiuretic hormone and aldosterone work togetherto decrease urine output and increase fluid intake by stim-ulating thirst. Failure to compensate adequately mayimpair cellular function significantly, resulting in multisys-tem failure.
The type of fluid loss that leads to hypovolemia mayaffect tonicity of the extracellular fluid. The diagnosisand management of alterations in fluid balance may de-pend on the circumstances contributing to hypovolemia.Laboratory testing of hemoglobin, hematocrit, bloodurea nitrogen (BUN), serum creatinine, urine specificgravity, blood glucose, electrolytes, and plasma proteinscan provide additional information to guide treatmentstrategies.
Hemorrhage
Hemorrhage, or excessive bleeding, may result in hypo-volemia. Because water and sodium are lost at compara-ble rates, this condition is isotonic. Hemoglobin andhematocrit are decreased and BUN may be increasedearly in hemorrhage. Damage to other organ systemsmay be evident if hypovolemia is not corrected. Fluid re-placement for volume expansion is often necessary and is
FIGURE 8.8 Skin turgor evaluation. After squeezing the skin together,release should result in the ridges immediately returning to a normal ap-pearance. Dehydration should be suspected when evidence of ridges re-main after release. (Image reprinted with permission from Lesha Studios.)
Remember This?• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •
Hematocrit is a common laboratory analysis used todetermine the percentage of the volume of a blood sampleoccupied by cells. Hematocrit is an indirect measure of theviscosity or concentration/dilution of the blood reported asthe percentage of the volume of a blood sample occupiedby red blood cells.1
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 200

Alterations in Fluid, Electrolyte, and Acid-Base Balance 201
determined by the amount of blood loss. Replacement ofvolume with blood products, either whole blood orpacked (concentrated) red blood cells, provides the nec-essary extracellular fluid expansion as well as the cellularcomponents lost with bleeding. The crystalloid solutionRinger’s lactate intravenous fluid contains sodium,chloride, potassium, calcium, and lactate in concentra-tions that mirror those found in plasma and may also bean appropriate treatment in large-volume fluid resuscita-tion.3 Fluid replacement with osmotically active fluidshelps promote the movement of fluid from the interstitialspace to the intravascular space.
Dehydration
Dehydration is the result of decreased extracellularfluid volume or increased sodium content in relation towater content, representing a hypertonic condition.Excessive watery diarrhea, sweating, and insensiblerespiratory water loss during hyperventilation or fevermay lead to dehydration. Intravascular volume may be-come viscous, with evidence of an increase in hemat-ocrit caused by hemoconcentration. Thirst may bestimulated, and urinary output decreased. Movementof fluid from the intracellular to the extracellular com-partment promotes cell shrinkage. Dehydration of brainand nerve cells may result in headache, decreased re-flexes, seizures, and coma. Expansion of extracellularvolume with oral or intravenous rehydration, such asRinger lactate, is indicated to prevent organ damage.When chloride loss complicates dehydration, intra-venous replacement with an isotonic solution of normalsaline may be indicated to address the underlying ionicalteration.
Water Intoxication
Hypotonic hypovolemia, also known as water intoxica-tion, results from decreased sodium concentration, oftenthe result of water replacement after strenuous activity orexcessive loss of sodium from diuretic therapy inhibitingADH. Cellular swelling occurs because of movement ofwater from the extracellular space to the intracellularspace. Increases in cellular water trigger clinical manifes-tations, including muscle weakness, cramps, and fatigue,and central nervous system involvement such asheadache, confusion, and depression of deep tendon re-flexes (DTRs). Treatments including limiting water orincreasing sodium intake target the underlying cause ofthe condition. Hypertonic saline solutions and loop di-uretics to increase water elimination are also optionaltreatments.
Hypervolemia
Hypervolemia is an expansion of extracellular volumeinvolving the interstitial or vascular space.
When excess sodium and water are retained in similarproportions, the increased volume is isotonic. Causes ofhypervolemia include:
• Heart failure
• Cirrhosis of the liver
• Kidney failure
• Excessive fluid replacement
• Administration of osmotically active fluids
Mean arterial blood pressure is increased in hyper-volemia, inhibiting the secretion of ADH and aldos-terone, resulting in increased urinary sodium and waterelimination. In individuals who are unable to mountthese compensatory mechanisms, heart failure and pul-monary edema may result.
Edema
Edema results from increases in the extracellular com-partment of the interstitial fluid. Movement of fluid intothe interstitial compartment can be driven by:
• Increased capillary filtration pressure: hydrostaticpressure forces water from capillaries into intersti-tial fluid
• Decreased capillary osmotic pressure: fluid movesto the interstitium across the concentration gradient
• Increased capillary permeability: altered integrity ofthe capillary wall allows proteins to leak from thecapillaries into the interstitial space, increasing in-terstitial osmotic pressure
• Obstructed lymph flow (lymphedema): fluid inthe interstitium cannot be returned to the systemiccirculation
The mechanisms for the development of edema aredepicted in Figure 8.9. Edematous tissues may be at riskfor damage because of the resulting increased distancefor diffusion and the compression of the vasculaturesupplying oxygen and removing waste. The clinicalmanifestations of edema are determined by the sites ofoccurrence. When located in the joints, pain and im-paired movement may result. When located in the brainor lungs, function may be so impaired that death may re-sult. When fluid accumulation in the peripheral intersti-tium exceeds the tissues’ ability for absorption, the fluidbecomes mobile when pressure is exerted upon it. Whenpressure over an edematous area forces fluid movementand leaves an indentation, the edema is referred to as pit-ting (Fig. 8.10). Edema may be recognized as a localarea of swelling, increased body weight, and pain.
Body weight measurements provide an effective eval-uation of edema, with increased body weight reflectingan increase in total body fluid. Visual inspection of ex-tremities helps to identify peripheral edema. Evaluationof edema within organ systems not readily visible de-pends on the involved tissues. Auscultation of heart andlungs may reveal excessive fluid.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 201

202 Chapter 8
Capillary Normal
Interstitial space
12 mL/min
Lymphatic
2mL/min
Venule
Arterial
Increased hydrostatic pressure Decreased oncotic pressure
Increased permeability Lymphatic obstruction
Edema Edema
Edema
Edema
Tumor
B
A
C
D E
FIGURE 8.9 Mechanisms of edema in the capillary system. A. Normal. The differential between the hydrostatic and oncotic pressures at the arterialend of the capillary system is responsible for the filtration into the interstitial space of approximately 14 mL of fluid per minute. The fluid is reabsorbedat the venous end at the rate of 12 mL/min. Lymphatic capillaries drain fluid at a rate of 2 mL/min. B. Edema caused by increased hydrostatic pressure.Elevation at the venous end of the capillary decreases reabsorption. If the lymphatic capacity to drain fluid is exceeded, fluid accumulates. C. Edemacaused by decreased oncotic pressure. Decreased oncotic pressure in the vascular space promotes reduced fluid reabsorption. D. Edema caused by in-creased permeability results from endothelial injury, allowing fluid to leak from the vascular space. E. Lymphedema results from accumulation of fluidcaused by lymphatic obstruction. (Image from Rubin E, Farber JL. Pathology. 4th Ed. Philadelphia: Lippincott Williams & Wilkins, 2005.)
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 202

Alterations in Fluid, Electrolyte, and Acid-Base Balance 203
Altered Electrolyte Balance
Similar to acid-base balance, regulation of electrolytebalance is critical to metabolic function of cells. Alter-ations in electrolytes can disrupt many processes, includ-ing generation of action potentials and maintenance offluid balance.
ALTERED SODIUM BALANCE
Sodium is the most abundant cation in the extracellularcompartment and serves as the primary determinant ofblood osmolarity. Transport of sodium out of the cell
occurs against its concentration gradient, requiring activetransport through the energy-dependent Na�/K��ATP-ase membrane pump (Fig. 8.11). Alterations in sodiumbalance can alter acid-base balance, fluid balance, andneural conduction. Dietary sources provide sodium,which is excreted mainly by the kidneys, along with water.
Hyponatremia
Hyponatremia is characterized by decreased levels ofsodium in the blood. Sodium loss most often occursthrough vomiting, diarrhea, and sweating. Blood sodiumlevels of less than 135 mEq/L are diagnostic of hypona-
FIGURE 8.10 Pitting edema. Palpation causes a depression when released because of movement of fluid in the interstitium. (Image from Rubin E,Farber JL. Pathology. 4th Ed. Philadelphia: Lippincott Williams & Wilkins, 2005.)
NaNa+ +
NaNa+ +
NaNa+ +
K+ +
K+ +
NaNa+ +
NaNa+ +
NaNa+ +
K+ +
K+ +
Sodium-potassium pumps Extracellular fluid
Membrane
Cytosol
K+
Na+ Na+
Na+
Na+
Na+
Na+
K+ K+
K+ FIGURE 8.11 The sodium-potassium pump.This membrane-associated ion pump uses en-ergy in the form of ATP to transport sodium andpotassium across the membrane against theirconcentration gradient. (Image from Bear MF,Connors BW, Paradiso MA. Neuroscience: Explor-ing the Brain. 3rd Ed. Baltimore: LippincottWilliams & Wilkins, 2006.)
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 203

204 Chapter 8
tremia. Osmotic swelling of cells contributes to muscletwitching and weakness. Reduced extracellular circulat-ing volume may lead to hypotension, tachycardia, andreduced or absent urine output (oliguria and anuria, re-spectively). Altered neuronal function may lead to nau-sea and vomiting, lethargy, confusion, seizures, or coma.
Stop and Consider
Why is sodium balance especially critical to fluid balance?
Hypernatremia
Excessive dietary intake of sodium and loss of body wa-ter are the primary causes of hypernatremia. Hyperna-tremia is characterized by blood sodium levels of greaterthan 145 mEq/L. Cell metabolism is altered, as evi-denced by agitation, restlessness, and decreased levels ofconsciousness. Fluid shifts caused by hypernatremia mayresult in thirst, hypertension, tachycardia, edema, andweight gain.
ALTERED POTASSIUM BALANCE
Potassium is the most abundant intracellular cation. Be-cause most potassium is found in muscle, total bodypotassium is determined in large part by body size andmuscle mass.
Hypokalemia
Loss of potassium may result from excessive loss due todiuretic use, severe vomiting, or diarrhea. Potassiumlevels of less than 3.5 mEq/L in the blood indicatehypokalemia. These levels of potassium alter mem-brane potential, which may result in dizziness, hypoten-sion, cardiac arrhythmias, muscle weakness, and legcramps. Decreased smooth muscle motility contributesto nausea, anorexia (loss of appetite), and abdominaldistention.
Hyperkalemia
Potassium levels of more than 5 mEq/L in the blood arediagnostic of hyperkalemia. Causes of hyperkalemia areoften iatrogenic; that is, caused by inappropriate use ofdrugs or their management, leading to increased potas-sium levels. Movement of potassium from the intracellu-lar to the extracellular space may also lead to hyper-kalemia. Inadequate excretion of potassium, as in renalfailure (see Chapter 15), can also lead to hyperkalemia.These levels can alter membrane potential and are asso-ciated with the development of cardiac arrest, abdominalcramping, and flaccid paralysis because of their effectson sodium channels.
ALTERED CHLORIDE BALANCE
Chloride is a major extracellular anion. Chloride move-ment is often associated with sodium and plays a role inregulation of acid-base balance.
Hypochloremia
Hypochloremia is determined when blood chloride lev-els are less than 98 mEq/L. Common reasons for chlorideloss include vomiting, diarrhea, and the use of diuretics.Hypochloremia is often associated with hyponatremia,hypokalemia, and metabolic alkalosis. Muscle effects in-clude excessive tone and tetany (sustained contraction),weakness, and twitching. Shallow, depressed breathing,paralysis, or mental confusion may result.
Hyperchloremia
Hyperchloremia can result from severe dehydration,kidney failure, hemodialysis, and traumatic brain injury.Diagnosed by blood chloride levels of more than 108mEq/L, hyperchloremia may result in hyperchloremicmetabolic acidosis. Deep rapid breathing, weakness,headache, diminished cognitive ability, and cardiac arrestmay result from hyperchloremia.
ALTERED CALCIUM BALANCE
Most calcium is contained within bones and teeth; only asmall fraction is located in the extracellular fluid.Although the concentration of calcium in the extracellu-lar fluid is relatively small, calcium plays an essential rolein many metabolic processes, including activity of en-zyme systems, generation of action potentials, and mus-cle contraction.
Hypocalcemia
Calcium blood levels of less than 8.5 mg/dL, indicative ofhypocalcemia, lead to enhanced neuromuscular irri-tability. Medications, such as heparin and glucagon, cancause decreased blood calcium levels. In addition, thy-roid disorders, severe burns (see Chapter 13), kidneyfailure, vitamin D deficiency (see Chapter 16), and sep-sis may lead to hypocalcemia. Clinical manifestations in-clude anxiety, irritability, muscle twitching, cramps,spasms, tetany, laryngospasm, and seizure. Hypotensionand cardiac arrhythmia may occur because of decreasedcalcium entry into the cell.
Hypercalcemia
Blood calcium levels greater than 10.5 mg/dL indicatehypercalcemia. Increased blood calcium levels may re-sult from excessive bone breakdown, thyroid disease,and excessive intake of calcium supplements, includingcalcium-containing antacids. Decreased neuromuscularirritability caused by increased threshold accounts for the
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 204

Alterations in Fluid, Electrolyte, and Acid-Base Balance 205
main manifestations of hypercalcemia. These manifesta-tions include confusion, fatigue, constipation, nauseaand vomiting, muscle weakness, cardiac arrhythmia,headaches, and irritability.
ALTERED MAGNESIUM BALANCE
Magnesium has functions similar to the cations calciumand potassium. Much of the body’s magnesium iscontained in bone, similar to calcium. Soft tissues andmuscle cells also contain significant concentrations ofmagnesium.
Hypomagnesemia
Hypomagnesemia, characterized by blood levels lessthan 1.5 mEq/L, usually occurs in association withhypokalemia and hypocalcemia. Inadequate intake ofmagnesium because of malnutrition, malabsorption syn-dromes, severe burns, or alcoholism is the most commoncause of hypomagnesemia. Diuretic use is also associatedwith a risk of hypomagnesemia. Tetany, muscle cramp-ing, and seizures are possible manifestations resultingfrom altered neuromuscular transmission. Cardiac ar-rhythmia and hypotension occur from the alteration ofelectrical currents because of the concurrent effects ofsodium, potassium, and calcium imbalances.
Hypermagnesemia
Magnesium levels greater than 2.5 mEq/L measured inthe blood define hypermagnesemia. This imbalanceoccurs with less frequency than other electrolyte imbal-ances, and it often results from excessive intake of mag-nesium-containing products or supplements or fromend-stage renal disease. Neuromuscular transmissionand cell excitability are reduced, resulting in hypoten-sion, diminished reflexes, muscle weakness, flaccidparalysis, and respiratory depression. Cardiac arrhyth-mia and bradycardia may result, secondary to decreasedmovement of sodium into the cell.
ALTERED PHOSPHATE BALANCE
A component of ATP, phosphate is essential to cellularmetabolism. Cellular functions of glycolysis and manyenzyme reactions depend on phosphate. The major in-tracellular anion phosphate is stored in bones and teeth,in conjunction with calcium.
Hypophosphatemia
Blood phosphate levels less than 2.5 mg/dL are associatedwith hypophosphatemia. Often associated with hypo-magnesemia and hypokalemia, hypophosphatemia mayresult from severe burns, malnutrition, malabsorption,alcoholism, kidney disease, vitamin D deficiency, or pro-longed diuretic use. Manifestations of hypophosphatemia
include muscle weakness, tremor, paresthesia (abnormalsensation such as tingling or burning), weight loss, andbone deformities.
Hyperphosphatemia
Hyperphosphatemia occurs when blood phosphate lev-els rise above 4.5 mg/dL, and it often occurs in tandemwith hypocalcemia. Conditions resulting in hyperphos-phatemia include fractures, bone disease, hypoparathy-roidism, acromegaly (see Chapter 2), systemic infection(see Chapter 5), and intestinal obstruction (see Chapter15). There are no associated symptoms of hyperphos-phatemia, unless it is accompanied by other electrolyteimbalances.
Manifestations of electrolyte imbalances are summa-rized in Table 8.2.
Altered Acid-BaseBalance
Acid and base disorders can be respiratory or metabolic inorigin. Respiratory acidosis is described in detail in Chap-ter 12. This chapter focuses on metabolic alterations.Metabolic disorders result in an alteration in bicarbonatecaused by the addition or loss of nonvolatile acid or basein the extracellular fluid. Metabolic acidosis results in areduction of HCO3
�, prompting a decrease in pH. In-creased levels of HCO3
� result in an increase of pH,known as metabolic alkalosis. Initiating events thatcause altered HCO3
� levels trigger compensatory mech-anisms to maintain acid-base balance. Kidneys compen-sate efficiently by conserving HCO3
� or H� ions until thepH has returned to normal. These compensatory mecha-nisms adjust pH without altering underlying cause.
METABOLIC ACIDOSIS
A base deficit of HCO3� characterizes metabolic acido-
sis. Metabolic acidosis may occur secondary to an in-crease in strong anions (Cl�) or to an increase in weakacids. The levels of circulating albumin must also be con-sidered when determining the presence of metabolic aci-dosis. Hypoalbuminemia may mask the presence ofmetabolic acidosis caused by an alkalizing effect.4 Mech-anisms contributing to the development of metabolic aci-dosis include:
• Increased production of nonvolatile acids; causedby fasting, ketoacidosis, and lactic acidosis
• Decreased secretion of acids by the kidneys; leads torenal failure
• Increased loss of bicarbonate; caused by diarrhea,gastrointestinal suction
• Increase in Cl�; caused by excessive chloride reab-sorption in the kidney, sodium chloride infusion
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 205

206 Chapter 8
TABLE 8.2
Manifestations of Electrolyte Imbalances
Electrolyte Blood Level Imbalance Manifestations
Sodium �135 mEq/L Hyponatremia Muscle cramps, twitching, weaknessVolume deficit, hypotension, oliguriaHeadache, anxiety, altered consciousness
�145 mEq/L Hypernatremia Thirst, dry skin and mucous membranesDecreased excretionsHeadache, restlessness, altered consciousness
Potassium �3.5 mEq/L Hypokalemia Dizziness, muscle weakness, leg crampsCardiac arrhythmia, hypotensionThirst, nausea, anorexiaPoorly concentrated urine, polyuria
�5 mEq/L Hyperkalemia Cardiac arrestAbdominal cramping, flaccid paralysis
Chloride �98 mEq/L Hypochloremia Increased muscle tone, twitching, weakness, tetanyShallow, depressed breathing, respiratory arrestMental confusion
�108 mEq/L Hyperchloremia Hyperchloremic metabolic acidosisDeep, rapid breathingWeakness, headache, diminished cognitive abilityCardiac arrest
Calcium �8.5 mg/dL Hypocalcemia Enhanced neuromuscular irritabilityAnxiety, irritability, seizureMuscle twitching, cramps, spasm, tetany, laryngospasmHypotension, cardiac arrhythmia
�10.5 mg/dL Hypercalcemia Decreased neuromuscular irritabilityConfusion, fatigue, headache, irritabilityConstipation, nausea, vomitingCardiac arrhythmia
Magnesium �1.5 mEq/L Hypomagnesemia Tetany, muscle crampingSeizuresCardiac arrhythmia, hypotension
�2.5 mEq/L Hypermagnesemia Reduced neuromuscular transmission and cell excitabilityFlaccid paralysis, diminished reflexes, muscle weaknessHypotension, respiratory depression
Phosphate �2.5 mg/dL Hypophosphatemia Muscle weakness, tremor, paresthesiaWeight loss, bone deformity
�4.5 mg/dL Hyperphosphatemia No associated manifestations
The clinical manifestations of metabolic acidosis in-clude anorexia, nausea, vomiting, weakness, lethargy,confusion, coma, vasodilation, decreased heart rate, andflushed skin. Decreased neural activity results from re-duced neuronal excitability. Laboratory findings includedecreased pH (less than 7.35) and HCO3
� (less than 24mEq/L). The anion gap may increase when the cause ofthe metabolic acidosis is due to excess metabolic acids.
Change in HCO3� levels and base excess are useful be-
cause they account for buffering in the nonbicarbonatesystems.4 When acidosis is caused by increased chloride,the anion gap remains normal. Compensatory mecha-nisms include increased breathing rate and depth, hyper-kalemia, and increased ammonia in urine. Treatment isaimed to correct the primary cause, replace fluid andelectrolytes, and correct the pH.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 206

Alterations in Fluid, Electrolyte, and Acid-Base Balance 207
Fluid
Intracellular compartment
Extracellular compartment
Na+
K+
Mg+
Ca2+
Cl-
Phos-
HCO3-
Movement
Diffusion Osmosis Facilitated diffusion
Active transport
Acids
Bases
pH
Vascular space
Interstitium
Hydrostatic forces Osmotic pressure
Acidosis
Plasma
Respiratory
Renal
Alkalosis
Buf
fer
syst
em <
7.35
> 7.45
FIGURE 8.12 Concept map. Fluid, electrolyte,and acid-base balance.
balance. Each concept is individually highlighted, al-though clearly each is related to the other. When review-ing the clinical models, the student should apply the con-cepts he or she has learned about these alterations. Anoverview of the relationship between fluid, electrolyte,and acid-base balance is shown in Figure 8.12.
ALTERED FLUID BALANCE: CIRRHOSIS
Chapter 5 introduced the liver disease known as cirrho-sis. In this chapter, the discussion of cirrhosis focuses onthe implications of this disease related to alterations influid balance.
Pathophysiology
As previously discussed, cirrhosis is a form of liver dis-ease characterized by the interference of local blood flowand hepatocyte damage. Cirrhosis is often (but notalways) the result of hepatitis and liver damage from al-cohol exposure. The most common complication of cir-rhosis is ascites, accumulation of fluid in the peritonealcavity. This is an example of fluid loss to a “third space,”making it unavailable for use in the remaining extracellu-lar or intracellular compartments.
Cirrhosis and chronic liver disease represent lead-ing causes of mortality, although the rates are decreas-ing. From 1980 to 1989, hospitalization rates for womenwere less than that for men by one third. Hospitalizationrates were 20 to 30% lower in Whites as compared to
Blacks. Increasing age was associated with increaseddeath rates in men (15.2 to 49 in 100,000) and in women(4.8 to 26.7 in 100,000) when rates for age groups in the35 to 44 and 65 to 74 (men) and 75 to 84 (women) rangewere compared.5
TRENDS
METABOLIC ALKALOSIS
Increased pH caused by plasma excess of HCO3� char-
acterizes metabolic alkalosis. Mechanisms contributingto the development of metabolic alkalosis include:
• Decreased H� ions
• Increased HCO3� ions
• Loss of Cl� ions
Impaired excretion of excess HCO3� may be promoted
by contraction of extracellular fluid volume, hypokalemia,and hypochloremia.
Stop and Consider
Why can excessive, prolonged vomiting promote the develop-ment of metabolic alkalosis?
Clinical Models
The clinical models presented in this chapter incorporatethe concepts of altered fluid, electrolyte, and acid-base
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 207

208 Chapter 8
Ascites is the manifestation of the combination of hy-drostatic pressure, oncotic pressure, and capillary per-meability, similar to other forms of edema. Examples ofconditions leading to ascites and the underlying causesinclude:
• Increased hydrostatic pressure• Budd-Chiari syndrome (hepatic vein obstruc-
tion)• Congestive heart failure
• Decreased colloid osmotic pressure• Malnutrition• Nephrotic syndrome
• Increased capillary permeability• Malignancy• Bacterial peritoneal infection
Increased vascular resistance to blood flow in the livercauses a condition known as portal hypertension, ele-vation in the portal (hepatic) pressure of the liver. In-creased pressure promotes movement of fluid out ofcapillaries through hydrostatic mechanisms. The move-ment of fluid into the interstitium exceeds the ability ofthe lymphatic system to recirculate fluid to the systemiccirculation, leading to accumulation. Increased vascularresistance triggers the production of vasodilators to de-crease vascular resistance and increase blood flow. Thedilation of the portal arteries eventually results in a de-crease in blood volume and a drop in arterial pressure.To compensate for the drop in blood pressure, arterialpressure is maintained by activating mechanisms, whichresults in sodium and water retention and expandsplasma volume. Intestinal capillary pressure and perme-ability are altered by the combination of portal hyper-tension and arterial dilation, promoting the transport offluid to the abdominal cavity. In the advanced state, cir-rhosis is associated with protein wasting. This leads toloss of albumin in the circulation, further altering fluidbalance through loss of fluid to the extravascular space.
Progressive pathology may lead to renal impairment,including impaired free water excretion that leads to dilu-tional hyponatremia and renal vasoconstriction, which in-creases the risk of hepatorenal syndrome (renal failurecaused by severe renal vasoconstriction). Increased levelsof renin and aldosterone further contribute to altered fluidbalance.
Clinical Manifestations
The severity of ascites is related to the manifestation ofclinical signs and symptoms (Fig. 8.13). Ascites can bedescribed based on volume of fluid in the peritoneum(moderate to large volume) and is often associated withthe following manifestations:
• Moderate to severe abdominal discomfort
• Increased abdominal girth
• Increased weight
Tympany
Dullness
Bulging flank
FIGURE 8.13 Clinical evidence of ascites. Fluid accumulation in the ab-dominal cavity causes distention and bulging flanks and umbilicus. Tym-pany over the intestines and dullness over fluid in abdomen and flanksare also noted.
• Severe sodium retention
• Dilutional hyponatremia
• Renal failure (oliguria and increase in serum crea-tinine
Diagnostic Criteria
Physical examination and change in body weight areused to diagnose ascites. Measurement of abdominalgirth or circumference may be useful. Evaluation of liver,renal, and cardiac function should be completed to de-termine systemic damage or dysfunction.
Treatment
The volume of ascites is a primary determinant of treat-ment. Diuretics are often used to promote ascitic fluid lossand normalize sodium balance. Caution must be used toavoid excessive diuresis, which results in hypovolemia andincreases risk of renal failure. In severe cases, paracentesismay be necessary. Paracentesis is the insertion of a can-nula into the peritoneal cavity to remove ascitic fluid (Fig.8.14). Intravenous albumin may be administered to ex-pand plasma volume in individuals who have had a largevolume of fluid removed to reduce the risk of circulatorydysfunction and rapid recurrence of ascites.
Stop and Consider
Why does ascites often return after fluid removal by paracentesis?
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 208

Alterations in Fluid, Electrolyte, and Acid-Base Balance 209
ALTERED ELECTROLYTE BALANCE:RENAL TUBULOPATHY
Hypokalemic salt-losing tubulopathies (SLTs) are agroup of autosomal recessive disorders characterized bymetabolic alkalosis. Many of the same physiologic ab-normalities are common between the groups, althoughthe age of onset varies between conditions. Four variantsof this disorder are known:
1. Classic Bartter syndrome (cBS)2. Gitelman syndrome (GS)3. Hyperprostaglandin-E syndrome (HPS), also
known as antenatal Bartter syndrome (aBS)4. Hyperprostaglandin-� syndrome with sensorineu-
ral deafness (HPS � SND)
Bartter and Gitelman syndromes are characterized byhypokalemia and hypochloremic metabolic alkalosis.7
From the Lab
Urinary sodium concentration provides a measure-ment of renal sodium retention. In patients with large-vol-ume ascites, urine sodium concentrations of 10 mmol/L areconsistent with severe sodium retention. Analysis of asciticfluid should be done to help determine etiology. Asciticfluid analysis involves:
• Determination of serum-ascitic albumin gradient (SAAG):calculated from the difference between ascitic fluid albu-min concentration and serum albumin concentration
• Gradients greater than or equal to 1.1 g/dL indicateportal hypertension or transudative ascites
• Gradients lesser than 1.1 g/dL indicate exudativeascites
• Amylase concentration: elevated in ascites of pancreaticorigin
• White blood cell (WBC) count: increase indicatesinfection
• Predominantly polymorphonuclear WBC indicatesbacterial infection
• Predominantly mononuclear WBC indicates fungal ortuberculin infection
• Red blood cell (RBC) count: increased concentration indi-cates hemorrhagic ascites, often caused by malignancy
• Gram stain and culture: determination of pathogeninvolved in infection
• Cytology: examination of cells for signs of malignancy
Rectus abdominis in sheath
External oblique
Internal oblique
Transverse abdominis
Transverse fascia
Extraperitoneal fat
Parietal peritoneum
Peritoneal cavity
Coils of small intestine
Skin
Superficial fascia
A
B
FIGURE 8.14 Paracentesis of the abdominalcavity. A. Midline approach. B. Lateral approach.(Image from Snell MD. Clinical Anatomy. 7th Ed.Philadelphia: Lippincott Williams & Wilkins,2003.)
RESEARCH NOTES Ascites can lead to the developmentof shock, renal failure, respiratory failure, and hypoperfusionas a result of abdominal pressure. In a recent case report, a67-year-old woman came into the emergency room who re-ported mild difficulty breathing. Her abdomen was obeseand tense on examination. While being evaluated in theemergency room, the patient developed severe hypoten-sion, oliguria (decreased urine output), and an increasedserum creatinine level consistent with acute onset renal fail-ure. She required ventilatory support because of decreasedoxygen saturation of her tissues. An ultrasound revealed se-vere ascites. Paracentesis was done with removal of 4,500mL of fluid, reducing abdominal pressure.6
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 209

210 Chapter 8
Pathophysiology
In SLTs, electrolyte reabsorption in the renal tubules isimpaired because of a gene defect altering five renalmembrane proteins. The effects are related to specificprotein alterations characteristic of each condition andhave been likened to the effects of diuretics.9 The cBSand HPS syndromes manifest alterations similar tothose induced by the loop diuretics, inhibiting reab-sorption of sodium and chloride in the loop of Henle.GS-associated electrolyte alterations mimic those in-duced by thiazide diuretics, also blocking sodium reab-sorption in the distal renal tubule. Inhibition of sodiumreabsorption is desirable because excretion of sodium inthe urine is accompanied by the excretion of water.Potassium may also be excreted, resulting in hy-pokalemia. Excessive loss of the strong cations sodiumand potassium lead to the development of metabolicalkalosis.
Clinical Manifestations
Manifestation of HPS occurs in utero; neonates presentwith severe effects. The initial manifestation is maternalhydramnios (excessive amniotic fluid) due to increased fe-tal urine output. Bartter syndrome and Gitelman syn-drome often present in early infancy through childhoodand adolescence. The neonatal (first 28 days of life)course is complicated by polyuria (excessive urine out-put), hypercalciuria (excessive calcium excreted in urine),and affects from increased levels of prostaglandin, includ-ing fever, vomiting, and diarrhea, further contributing toaltered fluid and electrolyte balance.10
Metabolic alkalosis is associated with contracted extra-cellular fluid volume because of sodium chloride loss.This decreased intravascular volume limits the space fordistribution of bicarbonate, amplifying the hyperbicar-bonatemia. Sodium chloride loss also contributes potas-sium loss and increased renal reabsorption of bicarbonate,further increasing blood pH and worsening metabolicalkalosis.11
Diagnostic Criteria
Renal structures can be evaluated with ultrasound. De-termination of electrolyte and fluid imbalances can beevaluated by measurements of electrolytes in serum andurine. Arterial blood gasses, anion gap, and base excess
The prevalence of Bartter syndrome worldwide isnot currently known. Studies have been conducted in Aus-tralia, Europe, the Middle East, and the United States. Astudy of patients in Costa Rica revealed a high frequency of
Bartter syndrome (1.2 cases per 100,000 live births). Theincidence of Bartter syndrome was estimated to be 25.4cases per 100,000 in preterm births.8
TRENDS
measures can be used to determine the presence ofmetabolic alkalosis and to guide treatment strategies.Fluid balance may be determined by urine-specificgravity measurement. Laboratory evaluations to detectrenal failure (discussed in more detail in Chapter 15)are done serially in these chronic conditions. In familieswith known risk for these disorders, DNA testing forthe genetic defect located on chromosome number 1can be accomplished on amniotic fluid in the antenatalperiod or from a cell sample taken directly from theneonate after birth.
Treatment
Treatment strategies are focused on the correction ofrenal salt and fluid losses. Sodium and potassium sup-plements are used to correct hyponatremia and hy-pokalemia. Diuretics that spare potassium excretion,including spironolactone and amiloride, may also beused. Indomethacin, a prostaglandin inhibitor, may beused to reduce prostaglandin production. Calcium andmagnesium supplements may also be used to correcthypocalcemia and hypomagnesemia.
Stop and Consider
Why are potassium-sparing diuretics the preferred treatment offluid and electrolyte imbalances associated with Bartter syndrome?
From the Lab
Urine-specific gravity measures the concentration ofparticles in the urine, comparing the weight of urine to theweight of water. A value between 1.010 and 1.025 suggestsfluid balance. Concentrated urine contains more particlesand has a higher specific gravity (more than 1.025). Diluteurine has a lower concentration of particles and has a lowerspecific gravity (less than 1.010). Urine osmolality measuresindicate the kidney’s ability to excrete or conserve water, orthe ability to concentrate urine, providing additional infor-mation on the renal contributions to fluid and electrolytebalance.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 210

Alterations in Fluid, Electrolyte, and Acid-Base Balance 211
ALTERED ACID-BASE BALANCE: HIGHLY ACTIVE ANTIRETROVIRALTHERAPY (HAART)-ASSOCIATEDACIDOSIS
As discussed in Chapter 4, the treatment of HIV has beeneffective in prolonging life and decreasing the incidenceand severity of many HIV-associated pathologies. Al-though HIV treatments have improved outcomes, thereare known drug-related adverse effects. The use of nucle-oside-analogue reverse transcriptase inhibitors (NRTIs)for the treatment of HIV has improved morbidity andmortality significantly. As more infected individuals takeNRTIs and are on them for longer periods, some signifi-cant adverse drug effects are being uncovered. Amongthem is the development of hyperlactatemia, or an ele-vation of lactic acid in the blood. Many individuals whodevelop hyperlactatemia, also known as lactic acidemia,are not symptomatic, and they experience subclinicalepisodes that are self-limiting. Other individuals sufferfrom a life-threatening form of metabolic acidosis knownas lactic acidosis that results from hyperlactatemia13, arare, but serious, complication of NRTI use.
Pathophysiology
Inhibition of the enzyme DNA polymerase by NRTIsmay lead to mitochondrial dysfunction and is believedto be responsible for the development of hyperlac-tatemia. Loss of this mitochondrial DNA prevents pro-duction of the necessary components of the electrontransport chain in the mitochondria. Oxidative phos-phorylation is impaired, promoting the formation oflactic acid for use by the cells for energy. Lactic acid isquickly converted to lactate through loss of a hydrogenatom in the blood. The buildup of lactate in the blood
reduces pH and predisposes affected individuals todeveloping lactic acidosis.
Clinical Manifestations
Symptoms are related to the severity of the metabolic aci-dosis developing from hyperlactatemia. Most individualswith hyperlactatemia are asymptomatic and do notdemonstrate any clinical manifestations.16 Mild hyperlac-tatemia can induce symptoms such as nausea, vomiting,abdominal discomfort, and weight loss. Hepatic steato-sis (fatty liver) is often associated with symptomatichyperlactatemia, resulting from NRTI-stimulated fatdeposition in the liver. Severe hyperlactatemia is the dis-ease subtype associated with a form of metabolic acidosisknown as lactic acidosis syndrome (LAS). Lactic acidosisis associated with pH levels of less than 7.3.14 Liverinvolvement, including hepatomegaly (enlarged liver),elevated liver enzymes, and hepatic failure, is often associ-ated with LAS. LAS may potentially result in coma andmultiorgan failure.
Diagnostic Criteria
Early recognition and treatment of hyperlactatemia inHIV-infected individuals taking NRTIs are critical fac-tors in decreasing morbidity and mortality due to thisadverse drug effect. The clinical manifestations and lab-oratory determination of the amount of lactate in theblood assist in the diagnosis and form the basis of treat-ment strategies. Liver function tests may be completed toidentify hepatic dysfunction. Electrolyte and blood pHlevels may also be analyzed.
RESEARCH NOTES Salt transport depends on the recy-cling of potassium in the thick ascending limb of the loop ofHenle. The genetic alterations associated with Bartter syn-drome contribute to the loss of potassium channel secretoryactivity, accounting for the alteration in electrolytes charac-teristic of the syndrome.12
HIV patients who take NRTIs are at increased riskfor the development of hyperlactatemia syndromes.Asymptomatic lactic acidemia associated with elevated
lactate levels and normal pH affects approximately 8 to21% of individuals taking at least one NRTI, with lactic aci-dosis occurring in about 1.5 to 2.5%.14
TRENDS
RESEARCH NOTES The influence of mitochondrial DNAdepletion and increases in serum lactate levels vary amongdifferent NRTIs. A study was done on patients taking NRTIsto determine the origin of hyperlactatemia. Blood sampleswere taken to determine serum lactate levels, and mito-chondrial DNA concentrations were determined from liverbiopsy samples. Depletion of mitochondrial DNA was in-creased by 47% in individuals taking the NRTIs zalcitabine,didanosine, and stavudine when compared to patients tak-ing zidovudine, lamivudine, and abacavir. Increased lactatelevels were also associated with the use of the drugs, whichdepleted mitochondrial DNA at a higher rate.15
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 211

212 Chapter 8
Treatment
Subclinical hyperlactatemia requires no treatment. Thiscondition is usually transient and resolves without inter-vention. Drug selection may influence the developmentof hyperlactatemia; certain drugs deplete mitochondrialDNA more than others. Stavudine and didanosine aremore often associated with the development of hyperlac-tatemia and lactic acidosis than are other NRTIs.17
NRTI treatment may be stopped or altered in individu-als who develop symptoms of hyperlactatemia, but havenot developed metabolic acidosis, in an attempt to pre-vent the development of LAS. NRTI treatment isstopped in individuals with LAS, although recovery can-not be assured. Intravenous administration of fluids canbe used to expand intravascular volume, prevent cardio-vascular collapse, and promote renal clearance of lactate.A period of weeks may be needed before lactate levelsreturn to normal. Resolution of LAS is confirmed by:
• Normalization of sodium bicarbonate
• Normalization of pH
• Serum lactate of less than 3.0 mmol/L
• Normalization of liver function
Stop and Consider
How is lactic acidosis different from other types of metabolicacidosis?
ALTERED SODIUM BALANCE: DEHYDRATION
Dehydration is characterized by negative fluid balance.Diarrhea is the most common cause of dehydration,although a variety of other conditions can lead todehydration.
Pathophysiology
Fluid deficit associated with dehydration involves bothintracellular and extracellular volume. Causes of dehy-dration resulting in fluid depletion include:
• Decreased fluid intake
• Increased fluid output• Renal• Gastrointestinal• Insensible
• Fluid shift between compartments• Ascites• Capillary leakage (burns and sepsis)
Dehydration is categorized based on blood sodiumconcentration, providing information about the type offluid loss and the potential complications associated withcoexisting electrolyte imbalance. Categories of dehydra-tion are described in Table 8.3. Volume deficit coupledwith altered sodium balance stimulates further fluidshifts, determined by the amount of circulating sodiumin the blood. In hyponatremic dehydration, the fluid lostcontains more sodium than the amount contained in theblood, leading to a hypotonic state. Seeking equilibrium,fluid shifts from the intravascular compartment to theextravascular compartment because of the low level ofsodium in the blood. This step results in further volumedepletion of the intravascular space, exaggerating the ef-fect of actual volume loss. Conversely, hypernatremicdehydration is associated with hypotonic fluid loss. Be-cause less sodium is lost relative to the fluid amount, lossof hypotonic fluid leads to a hypertonic state, promotingfluid movement from the extravascular space to the in-travascular space. This type of fluid shift actually mini-mizes the effects of the fluid loss, maintaining vascularvolume and potential for perfusion.18
According to the World Health Organization,dehydration secondary to diarrheal illness is the leadingcause of infant and child mortality. It was estimated thatbetween 2000 and 2003, diarrhea was the cause of deathin 17% of children younger than 5 years and in 3% of
babies younger than 28 days of age. A worldwide prob-lem linked to 4% of all deaths, diarrhea kills approxi-mately 2.2 million people in the world each year, mostlyaffecting children in developing countries.
TRENDS
From the Lab
Lactate levels can be measured in the blood to supporta diagnosis of hyperlactatemia. Lactate levels of more than2.1 mmol/L are diagnostic of hyperlactatemia, although in-dividuals may still be asymptomatic. Lactate levels of 5.0mmol/L or more are consistent with severe lactic acidemia.The diagnosis of lactic acidosis can be made when the arte-rial pH level falls below normal in the presence of elevatedlactate levels.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 212

Alterations in Fluid, Electrolyte, and Acid-Base Balance 213
Clinical Manifestations
Identification of clinical manifestations of dehydrationhelps to determine dehydration severity. Estimates offluid deficit are based on age and body size. In newborns,dehydration is classified by loss of body weight, with 5%considered mild, 10% considered moderate, and 15%considered severe. In children who weigh more than 10kg, mild dehydration is associated with a 3% weight loss,moderate is associated with a 6% loss, and severe equatesto a 9% loss. Mild dehydration is associated with mildmanifestations, with signs and symptoms worsening asthe severity of dehydration increases. Manifestations ofdehydration include:
• Decreased level of consciousness
• Prolonged capillary refill time
• Dry mucous membranes
• Decreased or absent tears
• Change in vital signs• Increased respiratory rate• Decreased blood pressure• Weak pulse
• Depressed fontanel (areas not enclosed by cranium,or “soft spots” on infants heads)
• Sunken eye
• Decreased or absent urine output
Diagnostic Criteria
A recent history helps determine the cause and severityof dehydration. Fluid intake, including volume and type(hypertonic or hypotonic), as well as fluid output, quan-tity, and characteristics (urine, stools, emesis, andsweat), are important in determining fluid balance. Ap-petite patterns and recent weight loss may provide an in-dication of malnutrition. Underlying medical condition,recent exposure to illness, or recent travel may point toan infectious cause of fluid imbalance.
History and evaluation of clinical manifestations pro-vide the basis of diagnosis. Laboratory analyses are gen-erally reserved for severe cases of dehydration. Bloodconcentrations of sodium, potassium, and chloride mayindicate associated electrolyte and acid-base imbalances.Poor perfusion may promote buildup of lactic acid, con-suming bicarbonate. Measures of circulating bicarbonatemay provide another indication of acid-base balance.Hypoperfusion may also lead to renal damage, which canbe determined by evaluation of blood urea nitrogen(BUN) and creatinine. Urine can be evaluated for con-centration by measurement of specific gravity and forelectrolyte content (see From the Lab box, below).Results of the laboratory evaluation may assist in thetreatment plan.
TABLE 8.3
Classifications of Dehydration: Sodium Considerations
Dehydration Sodium Frequency of Type of FluidCategory Concentration Diagnosis Loss Fluid Shifts
Hyponatremic �130 mEq/L 5–10% Hypertonic Intravascular to Extravascular
Isonatremic 130–150 mEq/L 80% Isotonic None
Hypernatremic �150 mEq/L 5–10% Hypotonic Extravascular to Intravascular
RESEARCH NOTES Hyponatremia is becoming an in-creasing concern for marathon runners, contributing torace-related morbidity and mortality.19 In a recent study of488 athletes participating in the Boston Marathon, re-searchers found that 13% had hyponatremia and 0.6% hadcritical hyponatremia with extremely low serum sodiumconcentrations. Excessive fluid intake during the race wasthe strongest single predictor for the development of hy-ponatremia. The researchers found no association with thetype of fluid intake among the runners (plain water or elec-trolyte solutions) and the risk for hypovolemia, emphasizingthe greater role of volume in the development of fluid im-balance. The risk was significantly increased in women andin individuals with extremes of body mass index.
From the Lab
As in evaluation of ascites, urinary sodium concentra-tion can be used to provide a measurement of renal sodiumretention. In patients with dehydration, urine sodium con-centrations help determine etiology. Urinary sodium con-centrations of less than 20 mEq/L indicate a nonrenal causeof fluid loss, such as ascites, vomiting, or diarrhea. Hypov-olemia associated with urinary sodium concentration ofmore than 20 mEq/L indicates fluid loss of renal origin. Fluidloss of renal origin may be caused by drugs such as thiazidediuretics because they alter urine concentration. Renalcauses of hypovolemia can also include excessive salt lossdue to renal failure.
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 213

214 Chapter 8
Treatment
Oral rehydration for mild to moderate dehydration helpsrestore fluid balance. Fluids intended for rehydrationcontain sodium, potassium, and glucose in the appropri-ate proportions, promoting ready absorption from thegastrointestinal system into the circulation. Rehydrationfluids must be administered frequently and in smallamounts. Severe dehydration with hypovolemia requiresintravenous administration of Ringer’s lactate or isotonicsaline solution to promote intravascular volume. Ideally,volume replacement should be determined based oncalculation of fluid deficit. Care must be taken to avoidrapid correction of hyponatremia, which is associatedwith neurologic complications. Rapid rehydration inhypernatremia may cause cellular swelling to the point ofcellular rupture.
Summary
Fluid, electrolyte, and acid-base balance are impor-tant to homeostasis and cellular function.
Fluid represents 60% of body weight, with two thirdsof body fluids contained in the intracellular compartmentand the remaining one third contained in the extracellu-lar compartment.
Fluid transport is accomplished based on concentra-tion and chemical gradients. Osmotic pressure is gener-ated by charged particles and pressure gradients aregenerated by hydrostatic forces.
Thirst, stimulated by hormonal mechanisms, isimportant in the regulation of fluid intake. Diureticsstimulate excretion of fluid through actions within thekidneys.
Alterations in fluid balance may result from imbal-ance between hydrostatic and osmotic forces and fromaltered capillary permeability. Hypervolemia and hypov-olemia are examples of altered fluid balance.
Alterations in fluid, electrolyte, or acid-base balancecan occur because of other diseases or can cause illness.
Electrolytes contain positive charges (cations) or neg-ative charges (anions) that determine attractive forcesand movement caused by differing concentrations be-tween compartments.
Alterations in electrolyte balance may affect acid-baseregulation, fluid balance, and neural conduction.
Low blood levels of electrolytes are indicated by theprefix “hypo”; increased blood levels of electrolytes areindicated by the prefix “hyper”, followed by the termfor the specific electrolyte involved (i.e., -natremia[sodium], -kalemia [potassium], and -phosphatemia[phosphate]).
Anion gap, based on calculation of measurable cationsand anions, provides an indication of acid-base balance.
Metabolic acidosis is characterized by a deficit inbase. Metabolic alkalosis is characterized by an excess inbase.
Acid-base balance is regulated by buffer systems,working in concert to maintain pH balance.
Correction of imbalances is critical to the mainte-nance of bodily functions.
To correct imbalances in fluid, electrolyte, and acid-base, careful consideration must be given to the potentialimpact of one system on the other.
Case Study
Jenny, a 19-year-old college student, was injuredin a fire resulting from a car accident. She experiencedfull-thickness burns over approximately 10% of herbody. Consider the clinical model that is most relatedto this process. From your reading related to fluid,electrolyte, and acid-base balance, answer the follow-ing questions:
1. What anatomic problem would most likely lead tofluid shifts because of burn injury?
2. What is the cause of fluid shifts in burn injury?
3. How would you manage fluid shifts in burn injury?
4. What would you expect for clinical manifestations?
5. What diagnostic tests might be used?
Log onto the Internet. Search for a relevant journalarticle or Web site that details fluid resuscitation afterburn injury to confirm your predictions.
Practice Exam Questions
1. Which of the following is an example of a strong acid?
a. Albuminb. Inorganic phosphorusc. Sodiumd. Lactate
2. An anion gap of 16 can be calculated by which of thefollowing scenarios?
a. Sodium 146, chloride 102, bicarbonate 26 mEq/Lb. Sodium 140, chloride 102, bicarbonate 26 mEq/Lc. Sodium 136, chloride 122, bicarbonate 30 mEq/Ld. Sodium 148, chloride 100, bicarbonate 28 mEq/L
3. Fluid loss in response to hypervolemia is promotedby:
a. Stimulating secretion of ADH, promoting urinarysodium and water elimination
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 214

Alterations in Fluid, Electrolyte, and Acid-Base Balance 215
RESOURCES
AIDSinfo (a service of the U.S. Department of Health andHuman Services):http://aidsinfo.nih.gov
American Burn Association:http://www.ameriburn.org/
REFERENCES
1. Stedman’s Electronic Dictionary. Philadelphia: LippincottWilliams & Wilkins, 2004.
2. Akita S, Sacks FM, Svetkey LP, et al. Effects of the Dietary Ap-proaches to Stop Hypertension (DASH) diet on the pressure-na-triuresis relationship. Hypertension 2003;42(1):8–13.
3. Leblanc M. Acid-base balance in acute renal failure and renal re-placement therapy. Best Pract Res Clin Anaesthesiol 2004;18(1):113–127.
4. Levraut J, Grimaud D. Treatment of metabolic acidosis. CurrOpin Crit Care 2003;9(4):260–265.
5. Centers for Disease Control and Prevention (CDC). Deaths andhospitalizations from chronic liver disease and cirrhosis—UnitedStates, 1980–1989. MMWR Morb Mortal Wkly Rep 1993;41(52–53):969–973.
6. Etzion Y, Barski L, Almog Y. Malignant ascites presenting as ab-dominal compartment syndrome. Am J Emerg Med 2004;22(5):430–431.
7. Naesens M, Steels P, Verberckmoes R, et al. Bartter’s and Gitel-man’s syndromes: from gene to clinic. Nephron Physiol 2004;96(3):65–78.
8. Madrigal G, Saborio P, Mora F, et al. Bartter syndrome in CostaRica: a description of 20 cases. Pediatr Nephrol 1997;11(3):296–301.
9. Reinalter SC, Jeck N, Peters M, Seyberth HW. Pharmacotyping ofhypokalaemic salt-losing tubular disorders. Acta Physiol Scand2004;181(4):513–521.
10. Jeck N, Reinalter SC, Henne T, et al. Hypokalemic salt-losingtubulopathy with chronic renal failure and sensorineural deafness.Pediatrics 2001;108(1):E5.
11. Adrogue HJ, Madias NE. Management of life-threatening acid-base disorders. Second of two parts. N Engl J Med 1998;338(2):107–111.
12. Lu M, Wang T, Yan Q, et al. ROMK is required for expression ofthe 70-pS K channel in the thick ascending limb. Am J Physiol Re-nal Physiol 2004;286(3):F490–F495.
13. Ogedegbe AE, Thomas DL, Diehl AM. Hyperlactataemia syn-dromes associated with HIV therapy. Lancet Infect Dis 2003;3(6):329–337.
14. Monier PL, Wilcox R. Metabolic complications associated with theuse of highly active antiretroviral therapy in HIV-1-infected adults.Am J Med Sci 2004;328(1):48–56.
15. Walker UA, Bauerle J, Laguno M, et al. Depletion of mitochondrialDNA in liver under antiretroviral therapy with didanosine, stavu-dine, or zalcitabine. Hepatology 2004;39(2):311–317.
16. McComsey GA, Yau L. Asymptomatic hyperlactataemia: predic-tive value, natural history and correlates. Antivir Ther 2004;9(2):205–212.
17. Department of Health and Human Services (DHHS). Guidelinesfor the Use of Antiretroviral Agents in HIV-Infected Adults andAdolescents. Rockville, MD: AIDSinfo; 2006.
18. Ellsbury DL, George CS (2006). Dehydration. EMedicine. Re-trieved from http://www.emedicine.com/ped/topics556.htm onJune 7, 2006.
19. Almond CS, Shin AY, Fortescue EB, et al. Hyponatremia amongrunners in the Boston Marathon. N Engl J Med 2005;352(15):1550–1556.
b. Inhibiting the secretion of aldosterone, promotingurinary sodium and water elimination
c. Lowering mean arterial pressured. Administering osmotically active fluids
4. Which of the following ions is most closely related towater movement?
a. Potassiumb. Sodiumc. Chlorided. Calcium
5. A pH of 7.5 is defined as
a. Alkalosisb. Acidosisc. Acidemiad. Alkalemia
DISCUSSION AND APPLICATION
1 What did I know about alterations in fluid, elec-trolyte, and acid-base balance before today?
2 What body processes are affected by alterations influid, electrolyte, and acid-base balance? How dofluid, electrolyte, and acid-base imbalances affectthose processes?
3 What are the potential etiologies for alterations influid, electrolyte, and acid-base balance? How dofluid, electrolyte, and acid-base imbalancesdevelop?
4 Who is most at risk for developing fluid, elec-trolyte, and acid-base imbalances? How can thesealterations be prevented?
5 What are the human differences that affect theetiology, risk, or course of alterations in fluid,electrolyte, and acid-base balance?
6 What clinical manifestations are expected duringfluid, electrolyte, and acid-base imbalances?
7 What special diagnostic tests are useful in deter-mining the diagnosis and course of alterations influid, electrolyte, and acid-base balance?
8 What are the goals of care for individuals whohave alterations in fluid, electrolyte, and acid-basebalance?
9 How does the concept of alterations in fluid, elec-trolyte, and acid-base balance build on what I havelearned in the previous chapter and in the previouscourses?
10 How can I use what I have learned?
90309 ch08 (191-216).ps 8/10/06 11:17 AM Page 215