Embed Size (px)
Citation preview

Thorax 1989;44:960-970
Review
Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigationG J GIBSON
The function of the diaphragm has been the subject ofintense study over the past 15 years. As a result itscomplex actions in normal subjects are now betterunderstood and it is increasingly clear that impairmentof diaphragmatic function may contribute to thepathophysiology of various conditions, not onlyprimary neuromuscular diseases, but also skeletalabnormalities and pulmonary diseases such as asthmaand chronic airways obstruction. This article is con-cerned with the presentation, consequences, investi-gation, and treatment of bilateral and unilateraldiaphragmatic paralysis; it is prefaced by a briefreview of current structural and functional conceptsand an account of the methods available for clinicalinvestigation of the diaphragm.
Hemidiaphragmatic paralysis is a conditionfamiliar to chest physicians and its implications interms of the likely underlying mediastinal lesions havebeen well known for many years.' The functional andsymptomatic consequences have been less generallyagreed, but several recent studies2"7 have helped toclarify the picture. Bilateral diaphragmatic paralysis isa much less familiar condition, which had beenreported only occasionally'89 until the series ofNewsom Davis et al in 1976.'0 With the increasing useof measurements of transdiaphragmatic pressure anddiaphragmatic electromyography, bilateral diaphrag-matic paralysis or severe weakness is now increasinglyrecognised. As an isolated abnormality, however, itremains a very rare occurrence, and recent evidence"suggests that if the function of the other respiratorymuscles is normal bilateral diaphragmatic paralysismay have less profound consequences than haveformerly been described.
Structure and function of the diaphragm
Standard anatomical texts'2 describe the structure ofthe diaphragm in terms of its central tendon andmuscular domes with attachments to the lower six ribs,
Address for correspondence: Dr G J Gibson, Departmentof Respiratory Medicine, Freeman Hospital, Newcastle upon Tyne,NE7 7DN.
to the xiphisternum and pericardium, and, via thearcuate ligaments and diaphragmatic crura, to thelumbar vertebrae. Clear understanding of its actionhas, however, been elusive and the reasons were wellstated by Briscoe in 1925:'
We have not to deal with a simple muscle exerting astraightforward easily ascertained action upon fixedpoints, but with a double sheet of complex fibres hiddendeep in the body, the actions ofwhich are far from simpleand only to be recognised by effects which are not only forthe most part indirectly produced, but are always com-plicated by the interfering action of other muscles.
This remains true in 1989 but understanding of themechanisms of action of the diaphragm has beenimproved by a clearer perception of its topographyand anatomical relations and by measurements ofchest wall motion, transdiaphragmatic pressure, andelectromyography.
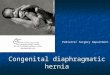
ACTIONS OF THE DIAPHRAGM ON THE RIB CAGEIn 1973 Goldman and Mead '3 pointed out that duringquiet tidal breathing, particularly in the supine pos-ture, the upper surface of the diaphragm is in directrelation not to the lung but to the inner surface of therib cage; there exists a large circumferential surfacebelow the lungs where the two layers of parietal pleuralining respectively the superior surface of the dia-phragm and the inner surface of the rib cage are inintimate contact (fig 1). With a moment's thought thisimportant point is self evident, but until then itssignificance had not been generally appreciated, per-haps because the clinician is used to examining chestradiographs taken after full inspiration when this"zone of apposition" is minimal. The functionalconsequence is that, particularly in the supine posi-tion, the lower rib cage behaves during tidal breathingas if it is driven by transabdominal rather thantransthoracic pressure.'3 During inspiration the dia-phragmatic muscle fibres shorten and the diaphragmas a whole moves caudally in piston like fashion; thedome ofthe diaphragm normally changes size or shapevery little during tidal breathing and the changes inmuscle length are accommodated mainly by increasingand decreasing the area of apposition. As the dia-
960
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigation
Pleural,/t space
Rib cage
Lung
Diaphragm
"Zone of Pabapposition"Lo
Fig 1 Diagrammatic representation of the "zone ofapposition," where the lower rib cage is effectively exposed toabdominal pressure (Pab) as there is no lung interveningbetween the two layers ofparietal pleura. These conditionsapply particularly at low lung volumes and in the supineposition.
phragm contracts it lowers pleural pressure andincreases abdominal pressure. The reduction in pleuralpressure produces an inflationary effect on the lungsbut, if no other force were active, its effect on the ribcage would be deflationary. This is, however, morethan countered by the accompanying effects of in-creasing abdominal pressure, which tends to expand
RC
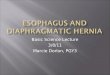
the rib cage via the zone of apposition, and by thedirect insertional effect of the diaphragm on the lowerribs, again tending to expand the rib cage (fig 2). In thehyperinflated chest of a patient with airways obstruc-tion the zone of apposition is greatly diminished orabsent, so that the inflationary effect of increasingabdominal pressure on the rib cage is no longeroperative; in addition, the insertional effect is modifiedso that direct traction by the flattened diaphragmresults in paradoxical inspiratory indrawing of thelower costal margin (Hoover's sign'4).
INTERACTION OF DIAPHRAGM AND OTHERRESPIRATORY MUSCLESAlthough the diaphragm is the most important in-spiratory muscle, it is not the only one active duringquiet breathing. The presence of phasic electricalactivity in the inspiratory intercostal muscles has longbeen recognised and similar activity has more recentlybeen reported in the scalene muscles, which are moreappropriately regarded as primary inspiratory musclesrather than as accessory muscles of inspiration.'5During deeper or more forceful inspiratory effortsother muscles, such as the sternomastoids, are re-cruited. In lung disease resting ventilation is usuallyincreased and the impedance to breathing may beabnormally high, so that coordinated contraction ofboth the primary and the accessory muscles of inspira-tion is necessary.
In bilateral diaphragmatic paralysis inspiration isachieved by the inspiratory intercostal and accessorymuscles, which lower pleural pressure and expand the
L
3
1 Dl
Fig 2 Normal effects ofthe diaphragm on the rib cage(RC). The lower rib cage is expanded (1) by directinsertions, the diaphragm (DI) using the abdominal contentsas afulcrum, and (2) by the effect ofincreasing abdominalpressure (Pab) via the zone ofapposition; these effects arecountered (3) by the deflating effect ofpleuralpressure(Ppl) as it becomes more negative. The net effect isinspiratory but mechanisms (1) and (2) becomeprogressively less effective as lung volume increases.
Pab t
INSPIRATORY by direct insertions
INSPIRATORY by increasing Pab
EXPIRATORY by lowering Ppi
2
1
2
3
961
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

962INSPIRATION WITHDIAPHRAGM ALONE
Movemenits
INSPIRATION WITHOUTDIAPHRAGM
I-
Gibsonexercise; their activation in late expiration passivelyraises and stretches the diaphragm, in effect "priming"it for the subsequent inspiration.'7 A further exampleof compensatory action by a different group ofrespiratory muscles in the face of diaphragmaticparalysis is glottal closure at end inspiration, whichallows maintenance of lung volume without continu-ing contraction of the inspiratory muscles.'6
l; I
Magnetometry
RC el
AB
Pressu res
pp,N' Pab
+ve -vePressure Pressure
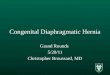
Fig 3 Comparison of chest wall motion andpleuralabdominal pressure changes when inspiration is achiethe diaphragm (left) andby other inspiratory musclecomplete diaphragmatic paralysis (right); withdiaphragmatic contraction both rib cage (RC) andabdominal (AB) dimensions increase and abdominal(Pab) becomes more positive. With bilateral diaphraparalysis the rib cage and abdomen move out ofphaseach other-that is, abdominalparadox occurs andabdominal pressure passively follows pleuralpressure
rib cage. The flaccid diaphragm moves craniasubdiaphragmatic abdominal pressure becomlnegative, rather than more positive as occunormal diaphragmatic contraction (fig 3). The iof the abdominal wall, which are normally expmay also act as accessory muscles of inspExpiratory abdominal muscle contraction is c(in patients with bilateral diaphragmatic weaknit has been suggested that use of these muscleaid inspiration by producing ascent of the padiaphragm at the end of expiration, so thaabdominal contraction ceases the diaphragm dipassively at the onset of inspiration.'""6 This nism operates effectively only in the upright pwhere gravity aids passive diaphragmatic cSimilar use of the abdominal muscles to aidtion has been demonstrated in normal subjects
INDEPENDENCE OF RIGHT AND LEFTHEMIDIAPHRAGMSAs the diaphragm forms one continuous musculo-tendinous sheet between the thorax and the abdomen,it is at first sight surprising that each hemidiaphragmcan apparently operate independently; paralysis ofone phrenic nerve might be expected to have littleeffect because tension in the whole diaphragm shouldbe maintained by activity in the contralateral phrenicnerve. Clearly this is not the case, however, and anelegant computed tomography reconstruction of thehuman diaphragm in vivo obtained in one normal
Volume subject by Whitelaw'8 has helped understanding ofhow the two halves of the diaphragm can operaterelatively independently when one half is paralysed.In particular, the reconstruction emphasises the pos-terior indentation of the central saddle shaped area ofthe diaphragm by the spinal column and aorta, which
+ve together extend approximately half way across theanteroposterior diameter (fig 4). As a result, fibres
and project from the centre of each dome to the ipsilateral!ved by hemithorax round more than 2700. The very limited7 in projection to the contralateral hemithorax would have
the effect that tension on one side was not well!nr.ovsa transmitted to the other, so would allow relativelyI,,a-urrgmaticre with
e (Ppl).
llfy andes moreurs withmusclesPiratory,liration.ommonless ands mightiralysed.t whenlescendsnechan-oosition,descent.inspira-s during
Fig 4 Direction oflines oftensionfrom the centre ofeachhemidiaphragmatic dome tofixed attachments, based on thecomputed tomography reconstruction by Whitelaw.'8 Becauselines oftension project to the opposite hemidiaphragm onlyvia the narrow isthmus between the spine and the xiphoidprocess tension on one side is not well transmitted to theother. (Reproduced by courtesy ofthe Journal ofAppliedPhysiology.)
-ve
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigationindependent operation of the two halves of thediaphragm.
COSTAL AND CRURAL PORTIONS: THE CONCEPTOF "TWO DIAPHRAGMS"A further important conclusion on structure-function relationships of the diaphragm has comerecently from studies in dogs'9 showing that stimula-tion of the costal and crural portions individuallyproduces very different effects: in the supine animalcontraction of the costal fibres at resting lung volumeincreased rib cage dimensions but contraction of thecrural fibres did not; at higher lung volumes, or whenthe abdomen was opened to the atmosphere (so thatthe inflating effect on the rib cage of increasingabdominal pressure could no longer operate), stimula-tion of the crural diaphragm led to diminution of ribcage dimensions. The concept of the diaphragm as twofunctionally independent muscles has an embryo-logical counterpart as the costal diaphragm developsfrom the lateral body wall whereas the crural portiondevelops in the dorsal mesentery of the oesophagus.'2This finding has led to a more complex but morerealistic model of inspiratory muscle actions'; theimplications for diaphragmatic function in healthyman or in disease remain to be explored.
Methods of assessment
CLINICAL METHODSClinical assessment of diaphragmatic function is atbest crude. The effect of the diaphragm on tidalbreathing is most apparent in the supine posture,where the abdominal muscles are usually least active;the normal forward motion of the anterior abdominalwall results directly from displacement of theabdominal contents by contraction of the diaphragm.Patients with bilateral diaphragmatic paralysis com-plain of extreme orthopnoea and (if they can toleratebeing examined supine) there is obvious inspiratoryparadoxical motion of the abdominal wall, resultingfrom passive transmission of the negative pleuralpressure generated by the other inspiratory muscles.Palpation of the abdominal wall allows this effect tobe distinguished from active contraction of theabdominal muscles themselves. In unilateral paralysisasymmetry of abdominal wall motion or diminutionof expansion of the ipsilateral costal margin during adeep inspiration can sometimes be detected but thesesigns are insensitive and unreliable. The maximumexcursion of the diaphragm between full inspirationand full expiration can be assessed approximately bypercussion, but this is of limited value. Reducedmotion on one side is very non-specific and occurswith localised disease above or below the diaphragm;
occasionally the paradoxical movement of unilateralparalysis can be detected.
IMAGING TECHNIQUESNormal ranges have been established for the radio-graphic position and degree of curvature of thediaphragm,2' but use is made of these mainly inrecognition and assessment of hyperinflation of thelungs associated with airways obstruction. Anunusually high position of one or both hemidia-phragms is less specific. Provided that the patient hastaken a full inspiration, bilateral elevation of thediaphragms implies one of the following: a reductionin pulmonary compliance, reduction in abdominalcompliance, pleural adhesions, or weakness of thediaphragmatic muscle itself. Unilateral elevation isseen with local lesions above or below the diaphragm,with hemidiaphragmatic weakness or paralysis, orother abnormalities of the diaphragm such as eventra-tion.
Fluoroscopy is the best established method ofassessing diaphragmatic function and it retains itsvalue in the recognition of hemidiaphragmaticparalysis. In a classic study Alexander22 investigateddiaphragmatic movements in a large number ofnormal subjects and showed that over the full vitalcapacity range there were appreciable differences inmost individuals between the excursions of the left andright hemidiaphragms, with movement of the leftusually exceeding that of the right. He also establishednormal ranges for the "sniff" test: out of 776 normalsubjects as many as 88 showed paradox ofone or bothhalves of the diaphragm during sniffing. Lateralfluoroscopy showed that in some individuals theparadoxical motion was confined to the anterior partof the diaphragmatic dome with normal movementposteriorly. After exclusion of these subjects, and alsoany who showed paradoxical motion of both hemi-diaphragms, there were still 6% of normal subjects inthis series with paradoxical motion of one completehemidiaphragm during the sniff test; this was seenmore commonly on the right side. Results of fluoro-scopy therefore have to be interpreted with somecaution; paradoxical motion should be at least 2 cmfor the confident recognition of abnormality. Withbilateral paralysis fluoroscopy is less helpful, at least inthe upright posture, as apparently normal inspiratorymovement may be seen with passive descent afterrelaxation of the abdominal wall muscles, which havecontracted during the previous expiration.23
Ultrasonography shows the right dome of thediaphragm well, but the left hemidiaphragm is visual-ised less clearly as the underlying bowel transmitsultrasound less well than does the liver. Mostultrasonic images of the diaphragm are obtainedincidentally during investigation of possible ab-
963
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

964dominal or pleural abnormalities. Parasagittal imagesare obtained by scanning in B mode with the subject inthe supine position; the transducer is placed sub-costally and directed towards the head as a gentle arc issectored.24 Normal values for the range of displace-ment of the right hemidiaphragm between functionalresidual capacity (FRC) and total lung capacity (TLC)in supine subjects have been established.25 In manysubjects three distinct echogenic lines are seen in theregion of the right hemidiaphragm, particularly athigh lung volumes: the inferior of these lines has beenshown to represent the liver capsule and diaphragmand the middle line the lung and visceral pleura, andthe superior line to be a mirror image artefact of theinferior line.26 Little use has so far been made ofultrasonography in clinical assessment of the dia-phragm, but it has been used in combination withphrenic nerve stimulation as a means of following therecovery of diaphragmatic paralysis in infants.27Computed tomography has been used to estimate
the thickness of the diaphragmatic leaves and theheight of the dome; both show large ranges in normalsubjects.' Conventional computed tomographyimages obtained in transverse section show the dia-phragmatic crura well; reconstructions of images inthe sagittal or coronal planes give more accurateinformation on the thickness and composition of thediaphragmatic dome and have been used in detailedreconstruction of diaphragmatic topography'8 (seeabove). So far no clinical use appears to have beenmade of this approach, nor has the possible role ofmagnetic resonance imaging been evaluated.
VOLUME AND PRESSURE MEASUREMENTSEarlier reports drew attention to the substantialchange in vital capacity (VC) between erect and supinepositions as an indicator of bilateral diaphragmaticparalysis.910 In such patientsVC characteristically fallsby half or more when the subject is lying supine.Normal subjects, however, also show a reduction ofVC in the supine posture, which is reported to be asmuch as 20%.29 Differences of 20-50% suggest dia-phragmatic weakness and indicate the need for furtherassessment. Measurements of the expansion of the ribcage and abdomen individually give indirect informa-tion about the contribution of the diaphragm to tidalbreathing. The ratio of rib cage and abdominaldisplacement (measured by magnetometers or induc-tance plethysmography) has been used as an index ofdiaphragmatic function. With complete bilateralparalysis the ratio is negative as the abdomen movescompletely out of phase with the rib cage (fig 3).Displacements of the rib cage and abdomen are not,however, specific as they are influenced also bycontraction ofthe other groups of respiratory muscles
Gibson(intercostal and accessory muscles, abdominalmuscles).The tension developed by the diaphragm cannot be
measured directly but the pressure generated by itscontraction is readily accessible. Measurements oftransdiaphragmatic pressure (Pdi) were introducedby Agostoni and Rahn.30 Pleural pressure (Ppl) isestimated from oesophageal pressure measured in theconventional way with an oesophageal balloon; sub-diaphragmatic abdominal pressure (Pab) is derivedfrom gastric pressure (Pga) measured by a secondballoon in the stomach. Pga is consistently morepositive than Pab, partly because of the hydrostaticpressure gradient and partly because of tone in thegastric wall. Most investigators assume that Pdi atFRC is zero-that is, Ppl = Pab; hence Pab duringbreathing is derived from Pga by subtracting thedifference between Pga and Ppl recorded with thesubject relaxed at FRC.The value of Pdi recorded during a maximum static
inspiratory effort is not necessarily the highest value asubject can attain as the pattern of performing aforceful inspiratory effort shows considerable vari-ation between subjects.3' 32 Some subjects activate therib cage and accessory muscles to a relatively greaterextent than the diaphragm so that Pab tends tobecome more negative during the effort and dia-phragmatic strength may be underestimated, whereasin other subjects Pab becomes strongly positive. Thisvariability limits the clinical usefulness of maximumPdi measured during such manoeuvres.
Miller et al" showed in normal subjects thatmeasurement of Pdi during maximal sniffs at FRCproduced consistently larger values than those recor-ded during sustained maximum static inspiratoryefforts at residual volume and the resulting normalrange showed less variation between subjects. Evenduring sniffs, however, the associated change in Pabhas been shown to contribute a proportion of therecorded Pdi, varying in normal subjects from 14% to80%.3 In some subjects the greatest value of Pdi maybe found during expulsive manoeuvres30 or during the"diaphragmatic Muller manoeuvre"-that is, whenthe subject performs a maximum inspiratory effort atthe same time concentrating on producing forwardabdominal motion." The maximum values achievedcan be increased by providing visual feedback infor-mation to the subject with an oscilloscope displayingPpl and Pab to encourage maximal effort.36 The mostappropriate method of assessing maximal diaphrag-matic activation in clinical practice is not universallyagreed. The sniff technique requires least training,whereas the static feedback method36 tends to give thegreatest values pf Pdi and the subject's spontaneousinspiratory effort consistently produces the mostnegative pleural pressure.
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigationDiaphragmatic contraction during quiet tidal
breathing is normally associated with an increase inPab and reduction in Ppl so that the contribution ofthe diaphragm can be assessed semiquantitatively byexamining the ratio APab:APpl." This analysis is validonly if other respiratory muscles do not contributeappreciably to the pressures generated. The ratio isnormally negative as Ppl and Pab move in oppositedirections (fig 3, left); it becomes positive if Pab falls(that is, becomes more negative) during inspiration.The ratio has a maximum value of + I when thediaphragm makes no contribution to the breath-thatis, if APpl and APab are equal (fig 3, right). Themeasurement is of particular value in patients who areunable or unwilling to perform maximal efforts.7
Electrophysiological techniques
Electromyographic activity in the diaphragm can berecorded with either oesophageal or surface elec-trodes. The former is less convenient but can becombined with measurements of transdiaphragmaticpressure with a single catheter system.38 Surface elec-trodes are more generally used. Recordings are madeduring spontaneous breathing or during electricalstimulation of the phrenic nerve in the neck.39 Thelatter is subject to the theoretical disadvantage thatlack of response may represent failure to locate thephrenic nerve, but in practice this is rarely a problemwith an experienced operator.' The normal phrenicnerve conduction time in adult subjects is less than9 5 ms.4' Phrenic nerve stimulation can be combinedwith measurement of transdiaphragmatic pressure toassess the mechanical response to neural excitation.4243Stimulation may be unilateral or simultaneously bi-lateral; it may use either a single "twitch" or asustained tetanic discharge, but the latter is rarely usedas it causes discomfort. The values of Pdi resultingfrom phrenic nerve stimulation are appreciably lowerthan those obtained by voluntary efforts; the pressureduring bilateral stimulation exceeds the sum of thevalues recorded with sequential unilateral stimulation,and that obtained with a tetanic discharge is greaterthan with a twitch. This approach has a role indistinguishing diaphragmatic paresis due to uppermotor and lower motor neurone lesions"; in theformer a disproportionate reduction of voluntary Pdiwould be expected, whereas in the latter case valuesobtained after stimulated and voluntary contractionshould be impaired to a similar degree.
Bilateral diaphragmatic paralysis
Paralysis or severe weakness of both hemidiaphragmsis seen usually in the context of severe generalisedrespiratory muscle weakness, but in occasional
patients the diaphragm is specifically or dispropor-tionately affected. Conditions that are particularlyassociated with bilateral diaphragmatic paralysis arelisted in the table. Most are rare and the associationwith bilateral diaphragmatic paralysis is in manyinstances based only on isolated case reports, but a fewof these conditions merit individual mention.
In motor neurone disease of the common adult type(amytrophic lateral sclerosis) the respiratory musclesare usually affected in proportion to the extent of thedisease elsewhere,' but occasionally early paralysis ofthe diaphragm presents diagnostic difficulty.' Thephrenic nerves are probably affected quite commonlyin generalised polyneuropathies but often this is notapparent unless phrenic nerve function is specificallystudied, as recently with hereditary peroneal muscularatrophy (Charcot-Marie-Tooth syndrome)."5 Withacute infective (Guillain-Barre) polyneuropathyrecovery of phrenic nerve function is not alwayscomplete and this may become apparent as difficultyin weaning a patient from ventilatory support whenneural function elsewhere appears to be recovering.The syndrome of neuralgic amyotrophy ("paralyticbrachial neuritis") is one of the more common causesof isolated bilateral diaphragmatic paralysis" " 5; it isassociated with pain, muscle wasting, and sensory lossin the shoulder or arm; again, recovery of diaphrag-matic function is often incomplete.'5 Phrenic nerveinjury by cold (the "frostbitten phrenic") has beenreported on several occasions after open heart sur-
Conditions particularly associated with bilateraldiaphragmatic paresis
Site oflesion(s) Condition References
Spinal cord Transection above C5 45Multiple sclerosis 46
Motor neurones PoliomyelitisAmyotrophic lateral sclerosis 47,48Spinal muscular atrophy 16,49,50
Cervical nerveroots Severe spondylosis 51
Phrenic nerves Tetanus antitoxin 8Guillain-Barre polyneuropathy 41, 52Charcot-Marie-Tooth polyneuropathy 53, 54Neuralgic amyotrophy 11, 55,56Unclassified phrenic neuropathy 57, 58, 59Trauma: blunt chest injury 60
cold injury 41, 61,62Malignant invasion 63Paraneoplastic lesion 64Hypothyroidism 65,66
Diaphragmatic Limb girdle dystrophy 10,67muscle Acid maltase deficiency 68,69
Systemic lupus erythematosus 70-74Mixed connective tissue disease 75Dermatomyositis 76Systemic sclerosis 77Amyloid infiltration 78
965
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

966
gery61 62; it results from ice used in the pericardium toproduce topical cardiac cooling. The condition comesto light with postoperative difficulty in weaning fromventilatory support; recovery is usual but may takeseveral months.62The diaphragm is likely to be affected in virtually
any generalised disease of skeletal muscle: conditionswith a propensity to cause disproportionate dia-phragmatic weakness are the late onset form ofmuscular dystrophy (limb girdle dystrophy)'067 andacid maltase deficiency." 6 In the more commonjuvenile form of muscular dystrophy, Duchennemuscular dystrophy, diaphragmatic paralysis tends tobe a late feature. Respiratory muscle function isaffected in many systemic conditions, particularly thecollagen diseases and thyroid disease. Occasionalpatients with systemic lupus erythematosus developthe interesting "shrinking lung" syndrome, character-ised by dyspnoea, orthopnoea, and radiographic ele-vation of the hemidiaphragms, which on screening aresaid to move "sluggishly." Several studies7"74 havesuggested that this syndrome results most commonlyfrom severe diaphragmatic weakness; extensivefibrosis and atrophy of the diaphragm was found atnecropsy in one case.72 The condition deteriorateswhen the disease is active generally but may stabiliseduring prolonged periods of chronic disability.
Patients with bilateral diaphragmatic paralysisusually complain of breathlessness but in the presenceof severe generalised muscle weakness the capacity toperform exercise may be so limited that this is not amajor feature. Orthopnoea is a more specific symptomand is sometimes so severe that the patient is unable tolie completely supine. There is associated tachypnoea,respiratory distress, and abdominal wall paradox inthe supine position. The chest radiograph typicallyshows elevation of both hemidiaphragms, though thisis not always present; atelectasis may be evident at thelung bases. Fluoroscopy may show apparently dimin-ished movement but is generally unhelpful, at least inthe upright posture23; if it is performed with the subjectsupine diaphragmatic paradox is more readilydetected.Newsom Davies et al 0 drew attention to the
elevation of arterial carbon dioxide tension in theirpatients, particularly in the supine position, and thearterial blood gases showed striking deteriorationwhen the subjects were asleep. Similar findings werereported by Skatrud et a167 in one patient with limbgirdle dystrophy studied in detail during sleep, whenthere was considerable hypoventilation during rapideye movement (REM) sleep. As in normal subjectsventilation during REM sleep is dependent on activityof the diaphragm, because the intercostal and acces-sory muscles are then inactive,80 it was suggested thatpatients with diaphragmatic paralysis would be
Gibson
unusually vulnerable to hypoventilation or apnoea,particularly during REM sleep. Recently, however,Laroche et al," studying six carefully chosen patientsin a stable state with severe and apparently isolatedbilateral diaphragmatic weakness, found neitherchronic hypercapnia nor abnormal nocturnal hypo-ventilation. They therefore argued that the nocturnalhypoventilation reported in other studies was depen-dent on the presence of generalised respiratory muscleweakness and that bilateral diaphragmatic paralysisalone does not lead to important nocturnal hypo-ventilation or chronic respiratory failure. This con-troversy is not completely resolved as there are otherwell documented cases with apparently isolated bi-lateral diaphragmatic paralysis where hypercapniawas present.663
Because in most patients bilateral diaphragmaticparalysis occurs in the context of global respiratorymuscle weakness, many patients are adequately asses-sed by simple measurements of maximum static res-piratory pressures at the mouth. In the occasionalpatient in whom specific or disproportionate weaknessof the diaphragm is suspected measurements of Pdiare indicated. When the diaphragms are completelyparalysed the exact manoeuvres used to detect Pdi arenot critical; with weakness, however, measurements ofPdi, especially during forceful efforts, may need to beinterpreted cautiously. Mier et al8' investigated theinterrelations of various indices of diaphragmaticfunction in 30 patients with varying degrees of dia-phragmatic weakness; they showed general correla-tions between maximum inspiratory pressure (Pimax)measured at the mouth (an index of global inspiratorymuscle function) and Pdi during forceful sniffing.Reduction ofthe latter was also related to the presenceof abdominal paradox and to JVC in the supineposture. When sniff Pdi was less than 30 cm H20orthopnoea and abdominal paradox were alwayspresent. Although these clinical features are, ofcourse,not specific, the presence of severe bilateral dia-phragmatic weakness is likely to be detected by acombination of clinical examination and measure-ments of aVc and Pimax; measurement of Pdi isavailable for confirmation if necessary. If the cause ofthe paralysis is uncertain phrenic nerve stimulationwith measurement of the electromyographic or pres-sure (Pdi) response and phrenic nerve conduction timemay be helpful in locating the site and nature of thelesion or lesions.The management of patients with bilateral dia-
phragmatic paralysis is determined by the nature ofthe underlying condition. Occasionally, as in the caseof infective polyneuropathy, the paresis is reversible;but more often recovery cannot be expected. Inoccasional patients, where the cause is situated prox-imally in the upper cervical cord or brainstem, pacing
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigationof the distal phrenic nerves may be appropriate.82 Inthe context of generalised muscle disease ventilatoryassistance may be indicated particularly during sleep,and this may lead to an improvement in daytimerespiratory function. Traditionally this has beenachieved by negative pressure ventilation using acuirass,83 but more recently the technique of intermit-tent positive pressure ventilation via a nasal mask hasproved successful in many patients and seems likely tobecome the treatment of choice.'85
Unilateral diaphragmatic paralysis
Hemidiaphragmatic paralysis is much more familiarto the chest physician than is bilateral paralysis. Inmany cases the cause is immediately evident from thehistory or chest radiograph. Formerly therapeuticphrenicotomy was a common cause and the effects ofthis procedure are still seen in a few patients who weretreated for tuberculosis in the preantibiotic era. Thecommonest single identifiable cause nowadays ismalignant infiltration due to a bronchial carcinoma.This was the diagnosis in one third of 105 patients withparalysis of identifiable cause reported by Piehler etal.3 A further third of these patients had a history ofthoracic or neck operations resulting in intentional oraccidental phrenic nerve injury, and the remainingthird had diaphragmatic paralysis related to trauma,infection, or neurological disease. Most of the causesof bilateral paralysis listed in the table may present asapparent unilateral paralysis: cases have been repor-ted, for instance, with spinal cord injury,8" cervicalspondylosis,8" poliomyelitis,88 neuralgic amyotrophy,55and late onset muscular dystrophy.89 Other specificcauses of unilateral paralysis include pneumonia,88trauma resulting from cannulation of the subclavianvein,90 and herpes zoster affecting the cervical nerveroots and associated with a characteristic vesicularrash over the appropriate dermatomes.9' 9
Whether hemidiaphragmatic paralysis in itself is asufficient explanation for breathlessness during exer-tion has been a matter of some dispute, but in a seriesof 142 such patients with no identifiable cause 24%complained ofshortness ofbreath and in most this waspersistent.3 If there is concomitant obesity or lungdisease, such as airflow obstruction, the symptomaticimpact is greater. Orthopnoea is also a frequentcomplaint,2 but it is less dramatic than in patients withbilateral paralysis. The physical signs are usually non-specific; occasionally paradoxical motion of theparalysed diaphragm may be suspected by percussionand there is a reduction in breath sounds at theaffected lung base. Asymmetrical motion of theabdominal wall in the supine posture is occasionallydetectable.'5The functional effects of hemidiaphragmatic
paralysis are in general similar to, but less strikingthan, those of bilateral paralysis. There are reductionsin ventilation and perfusion of the lower lobe on theaffected side,493' leading to some mismatching andwidening of the alveolar-arterial oxygen differenceand mild hypoxaemia.'
Indices of diaphragmatic function give values inter-mediate between those of bilateral paralysis andnormality. Some reduction in vital capacity in thesitting position is the rule but this is rarely severe, withmean values reported of 74%5 and 81%2 predicted.The fall in vital capacity when the supine position isassumed is greater than normal but less than is seen inbilateral paralysis. In one subject studied in detailbefore and after crushing of the right phrenic nervebecause of intractible hiccups Easton et a14 showed anincrease in aVC from 0 47 to I 0 1. Clague and Hall2 infour patients with right hemidiaphragmatic paralysisshowed a mean aVC of 19%, compared with 10% infour subjects with left sided paralysis; the greater fall inthe individuals with right sided lesions was attributedto the weight of the liver. Pimax is reduced; Laroche etal' found a mean value of 62% predicted. MaximumPdi is also reduced, by about half both during staticefforts5 and during sniffing.6 The wide normal range ofPdi during maximum static efforts, however, reducesits discriminatory value and measurements in half thepatients studied by Lisboa et al6 were in the lownormal range. During tidal breathing the changes ingastric pressure show a reduced amplitude, the pres-sure sometimes becoming more negative during ins-piration. The latter is particularly evident with lefthemidiaphragmatic paralysis, as might be expectedfrom the normal position of the gastric air bubbleunder the left hemidiaphragm.6 As a result, JPab/zlPplduring tidal breathing is more positive than normal.67The relation between zPab/JPpl and maximum Pdi issimilar in patients with unilateral and bilateralparalysis.7The common clinical concern is whether there is an
underlying serious condition in a patient who presentswith hemidiaphragmatic paralysis with no causeimmediately evident on the chest radiograph. Thepublished evidence on this point is generally reassur-ing: in the study of Piehler et al' bronchoscopy wasperformed in 53 such cases with negative results. Noris it likely that a cause will become evident on followup8 88; Piehler et al' followed 142 such patients for amean of 8 7 years and a specific cause becameapparent in only six. It was, however, noteworthy thattwo of these patients presented with paralysis of boththe left hemidiaphragm and the left vocal cord, and ineach case a carcinoma in the left lung with spread tothe mediastinal nodes was subsequently diagnosed.
In patients with persisting symptoms attributable tohemidiaphragmatic palsy diaphragmatic plication is
967
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

968sometimes performed and considerable improvementin shortness of breath, together with an increase in VCand reduction in aVC, has been reported." Shorteningand stiffening of the diaphragm restores a morenormal position and reduces paradoxical motion95"';ventilation of the adjacent lower lobe is presumablyimproved and this leads to an increase in Pao2.95 Dataon diaphragmatic function are sparse, but one patientstudied before and after plication showed an increasein Pdimax from 33 to 53 cm H2O and more negativeAPab/APpl, falling from -0-83 to - 1-33.7The term diaphragmatic eventration is sometimes
used interchangeably with diaphragmatic paralysisbut is more appropriately reserved for a congenitalfailure of muscular development of part or all of thehemidiaphragm. It is usually left sided and presentsmost characteristically in infancy, when there may beassociated respiratory distress requiring surgical treat-ment. Occasionally it is found incidentally in adult life,when it is usually asymptomatic. The distinction isreadily evident at surgery, where the reduction inmuscle fibres and membranous nature of the dia-phragmatic partition are apparent.9597
Conclusions
Bilateral diaphragmatic paresis has been recognisedfor more than 60 years but only in recent years has itbeen generally acknowledged as an important, albeitrare, cause of respiratory disability. Its presenceshould be suspected by the combination of extremeorthopnoea, inspiratory abdominal paradox in thesupine position, and a substantial postural fall in VC.In most cases it is seen in the context of a generalisedneuromuscular disease and adequate assessment isobtained by measurements of maximum inspiratorypressure at the mouth. In a few patients measurementof Pdi or phrenic nerve conduction (or both) isjustified, especially when diaphragmatic paralysisappears to be disproportionate or isolated.
Unilateral diaphragmatic paralysis is relativelycommon; the long established fluoroscopic sniff testremains the investigation of choice, but valid inter-pretation of the results requires an experiencedobserver and the application of certain minimumcriteria for paradoxical ascent of the affected hemi-diaphragm. If the likely cause is not evident from thehistory or chest radiograph at presentation it isunlikely to become apparent later. Many patients withhemidiaphragmatic paralysis are breathless and thiscan be improved by diaphragmatic plication.References
1 Briscoe C. Diagnosis of unilateral phrenic nerveparalysis: important point in mediastinal localization.Lancet 1925;i:376-81.
Gibson
2 Clague HW, Hall DR. Effect of posture on lung volume:airway closure and gas exchange in hemidiaphragmaticparalysis. Thorax 1979;34:523-6.
3 Piehler JM, Pairolero PC, Gracey DR, Bernatz PE.Unexplained diaphragmatic paralysis: a harbinger ofmalignant disease? J Thorac Cardiovasc Surg 1982;84:861-4.
4 Easton PA, Fleetham JA, De La Rocha A, AnthonisenNR. Respiratory function after paralysis of righthemidiaphragm. Am Rev Respir Dis 1983;127:125-8.
5 Lisboa C, Pare PD, Pertuze J, et al. Inspiratory musclefunction in unilateral diaphragmatic paralysis. Am RevRespir Dis 1986;134:488-92.
6 Laroche C, Mier AK, Moxham J, Green M. Diaphragmstrength in patients with recent hemidiaphragmparalysis. Thorax 1988;43:170-4.
7 Hillman DR, Finucane KE. Respiratory pressure parti-tioning during quiet inspiration in unilateral andbilateral diaphragmatic weakness. Am Rev Respir Dis1988;137:1401-5.
8 Comroe JH, Wood FC, Kay CP, et al. Motor neuritisafter tetanus anti-toxin with involvement of themuscles of respiration. Am J Med 1951;10:786-9.
9 McCredie M, Lovejoy FW, Kaltreider NL. Pulmonaryfunction in diaphragmatic paralysis. Thorax 1962;17:213-7.
10 Newsom Davis J, Goldman M, Loh L, Casson M.Diaphragm function and alveolar hypoventilation. Q JMed 1976;45:87-100.
11 Laroche CM, Carroll N, Moxham J, Green M. Clinicalsignificance of severe isolated diaphragm weakness.Am Rev Respir Dis 1988;138:862-6.
12 Williams PL, Warwick R, eds. Gray's Anatomy. 36th ed.London: Churchill Livingstone, 1980.
13 Goldman MD, Mead J. Mechanical interaction betweenthe diaphragm and rib cage. J Appl Physiol 1973;35:197-204.
14 Hoover CF. Diagnostic significance of inspiratorymovements ofcostal margins. Am JMed Sci 1920;159:633-46.
15 De Troyer A, Estenne M. Coordination between rib cagemuscles and diaphragm during quiet breathing inhumans. JAppl Physiol 1984;57:899-906.
16 Grinman S, Whitelaw WA. Pattern of breathing in a caseof generalized respiratory muscle weakness. Chest1983;84:770-2.
17 Grimby G, Goldman M, Mead J. Respiratory muscleaction inferred from rib cage and abdominal V-Ppartitioning. J Appl Physiol 1976;41:739-51.
18 Whitelaw WA. Shape and size of the human diaphragmin-vivo. JAppl Physiol 1987;62:180-6.
19 De Troyer A, Sampson M, Sigrist S, MacklemIPT. Actionof costal and crural parts of the diaphragm on the ribcage in dog. J Appi Physiol 1982;53:30-9.
20 Macklem PT, Macklem DM, de Troyer A. A model ofinspiratory muscle mechanics. J Appl Physiol 1983;55:547-57.
21 Lennon EA, Simon G. The height ofthe diaphragm in thechest radiograph of normal adults. Br J Radiol 1965;38:937-43.
22 Alexander C. Diaphragm movements and the diagnosisofdiaphragm paralysis. Clin Radiol 1966;17:79-83.
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

Diaphragmatic paresis: pathophysiology, clinicalfeatures, and investigation23 Loh L, Goldman MD, Newsom Davis J. The assessment
ofdiaphragm function. Medicine (Baltimore) 1977;56:165-9.
24 Haber K, Asher WM, Freimanis AK. Echographicevaluation of diaphragmatic motion in intraabdominal diseases. Radiology 1975;114:141-4.
25 Harris RS, Giovannetti M, Kim BK. Normal ventilatorymovement of the right hemidiaphragm studied byultrasonography and pneumotachography. Radiology1983;146:141-4.
26 Lewandowski BJ, Winsberg F. Echographic appearanceof the right hemidiaphragm. J Ultrasound Med 1983;2:243-9.
27 McCauley RG. Diaphragmatic paralysis evaluated byphrenic nerve stimulation during fluoroscopy or real-time ultrasound. Radiology 1984;153:33-6.
28 Patterson NW, Teates CD. CT measurements of theanterior portions of the diaphragm with illustrativeabnormal cases. Comput Radiol 1985;9:61-5.
29 Allen SM, Hunt B, Green M. Fall in vital capacity withposture. Br JDis Chest 1985;79:267-71.
30 Agostoni E, Rahn H. Abdominal and thoracic pressuresat different lung volumes. J Appl Physiol 1960;15:1087-92.
31 Gibson GJ, Clark E, Pride NB. Static transdiaphragmaticpressures in normal subjects and in patients withchronic hyperinflation. Am Rev Respir Dis 1981;124:685-9.
32 De Troyer A, Estenne M. Limitations ofmeasurement oftransdiaphragmatic pressure in detecting diaphrag-matic weakness. Thorax 1981;36:169-74.
33 Miller JM, Moxham J, Green M. The maximal sniffin theassessment of diaphragm function in man. Clin Sci1985;69:91-6.
34 Esau SA, Bye PTB, Pardy RL. Changes in rate ofrelaxation of sniffs with diaphragmatic fatigue inhumans. J Appl Physiol 1983;55:731-5.
35 Roussos CS, Macklem PT. Diaphragmatic fatigue inman. J Appi Physiol 1977;43:189-97.
36 Laporta D, Grassino A. Assessment of transdiaphrag-matic pressure in humans. J Appl Physiol 1985;58:1469-76.
37 Macklem PT, Gross D, Grassino A, Roussos C.Partitioning of inspiratory pressure swings betweendiaphragm and intercostal/accessory muscles. J AppiPhysiol 1978;44:200-8.
38 Onal E, Lopata M, Ginzburg AS, O'Connor TD.Diaphragmatic EMG and transdiaphragmatic pres-sure measurement with a single catheter. Am RevRespir Dis 1981;124:563-5.
39 Newsom Davis J. Phrenic nerve conduction in man. JNeurol Neurosurg Psychiatry 1967;30:420-6.
40 Mier A, Brophy C, Moxham J, Green M. Phrenic nervestimulation in normal subjects and in patients withdiaphragmatic weakness. Thorax 1987;42:885-8.
41 Markland DN, Kincaid JC, Pourmand RA, etal. Electro-physiologic evaluation of diaphragm by trans-cutaneous phrenic nerve stimulation. Neurology1984;34:604-14.
42 Bellemare F, Bigland-Ritchie B. Assessment of humandiaphragm strength and activation using phrenic nervestimulation. Respir Physiol 1984;58:263-7.
43 Aubier M, Murciano D, Lecocguic Y, Viires N, ParienteR. Bilateral phrenic stimulation: a simple technique toassess diaphragmatic fatigue in humans. JAppl Physiol1985;58:58-64.
44 Mier-Jedrzejowicz A, Green M. Respiratory muscleweakness associated with cerebellar atrophy. Am RevRespir Dis 1988;137:673-7.
45 Ledsome JR, Sharp JM. Pulmonary function in acutecervical cord injury. Am Rev Respir Dis 198 1;124:41-4.
46 Cooper CB, Trend PstJ, Wiles CM. Severe diaphragmweakness in multiple sclerosis. Thorax 1985;40:633-4.
47 Parhad IM, Clark AW, Barron KD, Staunton SB.Diaphragmatic paralysis in motor neurone disease.Neurology 1978;28:18-22.
48 Serisier DE, Mastaglia FL, Gibson GJ. Respiratorymuscle function and ventilatory control. I. In patientswith motor neurone disease. II. In patients withmyotonic dystrophy. Q J Med 1982;51:205-26.
49 Haas H, Johnson LR, Gill TH, Armentrout TS.Diaphragm paralysis and ventilatory failure in chronicproximal spinal muscular atrophy. Am Rev Respir Dis1981;123:465-76.
50 McWilliam RC, Gardner-Medwin D, Doyle D,Stephenson JBP. Diaphragmatic paralysis due tospinal muscular atrophy. An unrecognized cause ofrespiratory failure in infancy? Arch Dis Child 1985;60:145-9.
51 Spiteri MA, Mier AK, Brophy CJ, Pantin CFA, GreenM. Bilateral diaphragm weakness. Thorax 1985;40:631-2.
52 Gracey DR, McMichan JC, Divertie MB, et al.Respiratory failure in Guillain-Barre syndrome. MayoClin Proc 1982;57:742-6.
53 Chan CK, Mohensin V, Loke J, Virgulto J, Sipski L,Ferranti R. Diaphragmatic dysfunction in siblings withhereditary motor and sensory neuropathy (Charcot-Marie-Tooth disease). Chest 1987;91:567-70.
54 Laroche CM, Carroll N, Moxham J, Stanley NN,Courtenay Evans RJ, Green M. Diaphragm weaknessin Charcot-Marie-Tooth disease. Thorax 1988;43:478-9.
55 Cape CA, Fincham RW. Paralytic brachial neuritis withdiaphragmatic paralysis. Neurology 1965;15:191-3.
56 Graham AN, Martin PD, Haas LF. Neuralgic amyo-trophy with bilateral diaphragmatic palsy. Thorax1985;40:635-6.
57 Spitzer SA, Korczyn AD, Kalaci J. Transient bilateraldiaphragmatic paralysis. Chest 1973;64:355-7.
58 Blythe JA, Griffin JP, Gonyea EF. Bilateral diaphrag-matic paralysis in association with neurogenic disease.Arch Intern Med 1977;137:1455-7.
59 Camfferman F, Bogaard JM, van der Meche FGA,Hilvering C. Idiopathic bilateral diaphragmaticparalysis. Eur J Respir Dis 1985;67:65-71.
60 Sandham JD, Shaw DT, Guenter CA. Acute supinerespiratory failure due to bilateral diaphragmaticparalysis. Chest 1977;72:96-8.
61 Chandler KW. Bilateral diaphragmatic paralysis com-plicating local cardiac hypothermia during open heartsurgery. Am J Med 1984;77:243-9.
62 Kohorst RW, Schonfeld SA, Altman M. Bilateral dia-phragmatic paralysis following topical cardiac hypo-
969
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from

970thermia. Chest 1984;85:65-8.
63 Kreitzer SM, Feldman NT, Saunders NA, Ingram RH.Bilateral diaphragmatic paralysis with hypercapnicrespiratory failure. Am J Med 1978;65:89-95.
64 Thomas NE, Passamonte PM, Sunderrajan EV, AndelinJB, Ansbacher LE. Bilateral diaphragmatic paralysisas a possible paraneoplastic syndrome from renal cellcarcinoma. Am Rev Respir Dis 1984;129:507-9.
65 Hamly FH, Timins RN, Minh VD, Moser KM. Bilateralphrenic paralysis in myxedema. Am Rev Respir Dis1975;111:911-2.
66 Laroche CM, Cairns T, Moxham J, Green M. Hypo-thyroidism presenting with respiratory muscle weak-ness. Am Rev Respir Dis 1988;138:472-4.
67 Skatrud J, Iber C, McHugh W, Rasmussen H, NicholasD. Determination of hypoventilation during wakeful-ness and sleep during diaphragmatic paralysis. Am RevRespir Dis 1980;121:587-93.
68 Sivak ED, Salanga VD, Wilbourn AJ, Mitsumoto H,Golish J. Adult-onset acid maltase deficiency present-ing as diaphragmatic paralysis. Ann Neurol 1981;9:613-5.
69 Trend PstJ, Wiles CM, Spencer GT, Morgan-Hughes JA,Lake BD, Patrick AD. Acid maltase deficiency inadults. Brain 1985;108:845-60.
70 Gibson GJ, Edmunds JP, Hughes GRV. Diaphragmfunction and lung involvement in systemic lupuserythematosus. Am J Med 1977;63:926-32.
71 Martens J, Demedts M, Vanmeenen MT, Dequeker J.Respiratory muscle dysfunction in systemic lupuserythematosus. Chest 1983;84:170-5.
72 Rubin LA, Urowitz MB. Shrinking lung syndrome inSLE: a clinical pathological study. J Rheumatol1983;10:973-6.
73 Jacobelli S, Moreno R, Massardo L, Rivero S, Lisboa C.Inspiratory muscle dysfunction and unexplaineddyspnoea in systemic lupus erythematosus. ArthRheum 1985;28:781-8.
74 Wilcox PG, Stein HB, Clarke SD, Pare PD, Pardy RC.Phrenic nerve function in patients with diaphragmaticweakness and systemic lupus erythematosus. Chest1988;93:352-8.
75 Martens J, Demedts M. Diaphragm dysfunction in mixedconnective tissue disease. Scand J Rheumatol 1982;11:165-7.
76 Schiavi EA, Roncoroni AJ, Puy RJM. Isolated bilateraldiaphragmatic paresis with interstitial lung disease. Anunusual presentation of dermatomyositis. Am RevRespir Dis 1984;129:337-9.
77 Illiffe GD, Pettigrew NM. Hypoventilatory respiratoryfailure in generalized scleroderma. Br Med J 1983;286:337-8.
78 Streeten EA, de la Monte SM, Kennedy TM. Amyloidinfiltration of the diaphragm as a cause of respiratoryfailure. Chest 1986;89:760-2.
Gibson79 Nightingale S, Bates D, Bateman DE, Hudgson P, Ellis
DA, Gibson GJ. Enigmatic dyspnoea: an unusualpresentation of motor neurone disease. Lancet 1982;i:933-5.
80 Tabachnik E, Muller NL, Bryan AC, Levison H.Changes in ventilation and chest wall mechanics duringsleep in normal adolescents. J Appi Physiol 1981;51:557-64.
81 Mier-Jedrzejowicz A, Brophy C, Moxham J, Green M.Assessment of diaphragm weakness. Am Rev RespirDis 1988;137:877-83.
82 Moxham J, Potter D. Diaphragmatic pacing. Thorax1988;43: 161-2.
83 Sawicka EH, Loh L, Branthwaite MA. Domiciliaryventilatory support: an analysis of outcome. Thorax1988;43:31-5.
84 Kerby GR, Mayer LS, Pingleton SK. Nocturnal positivepressure ventilation via nasal mask. Am Rev Respir Dis1987;135:738-40.
85 Carroll N, Branthwaite MA. Control of nocturnalhypoventilation by nasal intermittent positive pressureventilation. Thorax 1988;43:349-53.
86 Carter RE. Unilateral diaphragmatic paralysis in spinalcord injury patients. Paraplegia 1980;18:267-74.
87 Buszek MC. Hemidiaphragmatic paralysis: an unusualcomplication of cervical spondylosis. Arch Phys MedRehabil 1983;64:601-3.
88 Riley EA. Idiopathic diaphragmatic paralysis: a report ofeight cases. Am J Med 1962;32:404-16.
89 Wolf E, Shochina M, Ferber I, Gonen B. Phrenic nerveand diaphragmatic involvement in progressivemuscular dystrophy. Electromyogr Clin Neurophysiol1981;21:35-53.
90 Obel IWP. Transient phrenic nerve paralysis followingsubclavian venipuncture. Anesthesiology 1970;33:369-70.
91 Anderson JP, Keal EE. Cervical herpes zoster anddiaphragmatic paralysis. Br JDis Chest 1969;63:222-6.
93 Derveaux L, Lacquet LM. Hemidiaphragmatic paresisafter cervical herpes zoster. Thorax 1982;37:870-1.
93 Arborelius M, Lilja B, Senyk J. Regional and total lungfunction in patients with hemidiaphragmatic paralysis.Respiration 1975;32:253-64.
94 Ridyard JA, Stewart RM. Regional lung function inunilateral diaphragmatic paralysis. Thorax 1976;31:438-42.
95 Wright CD, Williams JG, Ogilvie CM, Donnelly RJ.Results of diaphragmatic plication for unilateral dia-phragmatic paralysis. J Thorac Cardiovasc Surg 1985;90:195-8.
96 Marcos JJ, Grover FL. Trinkle JK. Paralyzed dia-phragm: effect of plication on respiratory mechanics. JSurg Res 1974;16:523-6.
97 Thomas TV. Congenital eventration of the diaphragm.Ann Thorac Surg 1970;10:180-92.
copyright. on D
ecember 16, 2021 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.44.11.960 on 1 N
ovember 1989. D
ownloaded from