Embed Size (px)
Citation preview

9/12/2019
1/21
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 69: Acute Asthma Rita K. Cydulka
FIGURE 69-1.
INTRODUCTION AND EPIDEMIOLOGY
Asthma is a chronic inflammatory disorder characterized by increased responsiveness of the airways to multiple stimuli. Insusceptible individuals, the inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, andcoughing, particularly at night or in the early morning. These episodes usually are associated with widespread and varyingairflow obstruction.
Although most acute attacks are reversible and improve spontaneously or within minutes to hours with treatment withsymptom-free intervals in between, many asthmatic patients develop chronic airflow limitation. This impacts the diagnosis of,management of, and attempts to prevent acute exacerbations.
Asthma a�ects approximately 8% of the U.S. population, is the most common chronic disease of childhood (9% prevalence),
a�ects 7% of the elderly, and has a similar prevalence in developed nations around the world.1,2,3 Approximately one half ofcases of asthma develop before the age of 10 years old, and another one third develop before the age of 40 years old.
PATHOPHYSIOLOGY
Asthma is characterized by an abnormal accumulation of eosinophils, lymphocytes, mast cells, macrophages, dendritic cells,and myofibroblasts in airways. The pathophysiologic hallmark of asthma is a reduction in airway diameter caused by smoothmuscle contraction, vascular congestion, bronchial wall edema, and thick secretions. These changes are reflected in pulmonaryfunction changes, increased work of breathing, and abnormal distribution of pulmonary blood flow (Table 69-1). Large andsmall airways contain plugs composed of mucus, serum proteins, inflammatory cells, and cellular debris. On a microscopiclevel, airways are infiltrated with eosinophils and mononuclear cells. Evidence of microvascular leakage, epithelial disruption,and vasodilation is frequently noted. The airway smooth muscle is hypertrophied and characterized by new vessel formation,an increased number of epithelial goblet cells, and deposition of interstitial collagen beneath the epithelium. Inflammationa�ects all bronchial pulmonary structures.

9/12/2019
2/21
TABLE 69-1
Physiologic Consequences of Airflow Obstruction
Increased airway resistance
Decreased maximum expiratory flow rates
Air trapping
Increased airway pressure
Barotrauma
Adverse hemodynamic e�ects
Ventilation–perfusion imbalance
Hypoxemia
Hypercarbia
Increased work of breathing
Pulsus paradoxus
Respiratory muscle fatigue with ventilatory failure
Asthma is a continuum from acute bronchospasm to airway inflammation to permanent airway remodeling. The structuralchanges associated with airway remodeling, such as sub–basement membrane thickening, subepithelial fibrosis, airwaysmooth muscle hypertrophy and hyperplasia, angiogenesis, and mucous gland hyperplasia and hypersecretion are associated
with nonreversible loss of lung function.4 Acute allergic bronchoconstriction results from immunoglobulin E–dependent releaseof mediators from mast cells. These mediators include histamine, leukotrienes, tryptase, and prostaglandins that directly
contract airway smooth muscle.4 Bronchospasm induced by aspirin and other nonsteroidal anti-inflammatory drugs also
involves mediator release from airway cells.4
Inflammation plays a key role in the pathophysiology of asthma regardless of disease severity. Inhaled antigens activateimmunoglobulin E, mast cells, and T helper cells in the airway and induce the production of inflammatory mediators andcytokines. In turn, this initiates a cascade of reactions involving lymphocytes, mast cells, eosinophils, dendritic cells,macrophages, resident airway cells, and epithelial cells that perpetuate the inflammatory response, with further release ofchemokines, cytokines, cysteinyl leukotrienes, and nitric oxide. The inflammatory process is multicellular, redundant, and self-amplifying.
Numerous host and environmental factors, such as number and type of infections in childhood, frequent antibiotic use,Western lifestyle, and repeated exposures to allergens, may contribute to the development of allergic asthma. Viral respiratory
infections are among the most common of the stimuli that invoke acute asthma exacerbation.5 Increased airway
responsiveness secondary to infection may last anywhere from 2 to 8 weeks.5 Exercise is another common precipitant of acuteasthma. Environmental conditions, such as atmospheric pollutants and antigens noted in heavy industrial or densely populatedurban areas, or increased indoor antigens, such as mold, house dust mites, cockroaches, and animal dander, are associatedwith higher incidence and severity of asthma. Occupational exposures, such as metal salt, wood and vegetable dust,pharmaceuticals, industrial chemicals, plastics, biological enzymes, vapors, gases, and aerosols, also may stimulate an asthmaattack. Agents such as aspirin, β-blockers (including topical β-blockers), nonsteroidal anti-inflammatory drugs, sulfating agents,tartrazine dyes, and food additives and preservatives may trigger acute asthma. Exposure to cold air alone can induce acutebronchospasm. Endocrine factors, such as changing levels of estradiol and progesterone during the normal menstrual cycle and
pregnancy, contribute to the level of airway reactivity.6 Emotional stress also can produce an asthma attack.
CLINICAL FEATURES

9/12/2019
3/21
The symptoms of asthma include dyspnea, wheezing, and cough. Many, but not all, patients will relay the history of asthmaupon presentation. Early in the attack, patients will complain of a sensation of chest constriction and cough. As theexacerbation progresses, wheezing becomes apparent, expiration becomes prolonged, and accessory muscle use may ensue. A
thorough history can be helpful in guiding care for asthma exacerbations7,8,9,10 (Table 69-2). Acute asthma exacerbations are
categorized based on clinical features7,8,9,10 (Table 69-3).
TABLE 69-2
Key History Points for Acute Asthma Exacerbation7,8,9,10
Symptoms Pattern Disease History Risk Factors for Death from Asthma
Cough Perennial and/or seasonal Age at onset Past history of severe exacerbation
Wheezing Continual or episodic Present management and medications ≥2 hospitalizations for asthma in the
past year
Shortness of
breath
Onset Medication regimen adherence >3 ED visits for asthma in the past year
Chest
tightness
Duration History of corticosteroid use (chronic
and/or intermittent)
>2 canisters per month of inhaled
short-acting β2-agonist
Sputum
production
Frequency Intensive care admissions Di�iculty perceiving airflow
obstruction or its severity
Fever Aggravating factors History of intubation Low socioeconomic status or inner-city
resident
Usual pattern of
exacerbation and outcome
Best spirometry measures Illicit drug use
Psychiatric disease or medical
comorbidities

9/12/2019
4/21
*The presence of several parameters, but not necessarily all, indicates the general classification of the exacerbation. Many of these
parameters have not been systemically studied, so they serve only as general guides.
Abbreviations: FEV1 = forced expiratory volume in 1 second; PEF = peak expiratory flow; SABA = short-acting β2 agonist.
Source: www.nhlbi.nih.gov/files/docs/guidelines/asthsumm.pdf (National Heart, Lung, and Blood Institute; National Institutes of Health;
U.S. Department of Health and Human Services: NIH Publication Number 08-5846, October 2007, Fig. 20). Accessed November 18, 2014.
TABLE 69-3
Classifying Severity of Asthma Exacerbations in Patients >12 Years Old and Adults*
Symptoms and Signs Initial PEF (or FEV1) Clinical Course
Mild Dyspnea only with
activity
PEF ≥70% predicted
or personal best
Prompt relief with inhaled SABA.
Moderate Dyspnea interferes with
or limits usual activity
PEF 40%–69%
predicted or personal
best
Relief from frequent inhaled SABA. Symptoms for 1–2 d a�er
oral corticosteroids begun.
Severe Dyspnea at rest;
interferes with
conversation
PEF <40% predicted
or personal best
Partial relief from frequent inhaled SABA. Symptoms for ≥3 d
a�er oral corticosteroids begun.
Subset:
life-
threatening
Too dyspneic to speak;
perspiring
PEF <25% predicted
or personal best
Minimal or no relief from frequent inhaled SABA; IV steroids;
adjunctive therapy; needs ED or intensive care unit.
Physical examination findings are variable. Patients presenting with a severe asthma attack may be in respiratory distress, withrapid breathing and loud wheezing, whereas patients with mild exacerbation may present with only cough and end-expiratorywheezing. At times, wheezing may be audible without a stethoscope. Other conditions may present with wheezing and mimicasthma (Table 69-4). The use of accessory muscles of inspiration indicates diaphragmatic fatigue. The appearance ofparadoxical respiration, which is chest deflation and abdominal protrusion during inspiration followed by chest expansion andabdominal deflation during expiration, is a sign of impending ventilatory failure. Alteration in the mental status (e.g., lethargy,exhaustion, agitation, or confusion) also heralds respiratory arrest.

9/12/2019
5/21
TABLE 69-4
Important Asthma Mimickers
Acute heart failure ("cardiac asthma")
Upper airway obstruction
Multiple pulmonary emboli
Aspiration of foreign body or gastric acid
Tumors/disorders causing endobronchial obstruction
Interstitial lung disease
Vocal cord dysfunction
Directed physical examination reveals hyperresonance to percussion, decreased intensity of breath sounds, and prolongation ofthe expiratory phase, usually with wheezing. Although wheezing results from the movement of air through narrowed airways,the intensity of the wheeze may not correlate with the severity of airflow obstruction. The "silent chest" reflects very severeairflow obstruction, with air movement insu�icient to promote an audible wheeze. A pulsus paradoxus (change in bloodpressure during inspiration) >20 mm Hg is also indicative of severe asthma, although it is not specific for asthma. Althoughtachycardia and tachypnea are usually seen with acute asthma, a normal heart rate, a normal respiratory rate, and the absenceof a pulsus paradoxus do not indicate complete relief of airway obstruction.
DIAGNOSIS AND PATIENT MONITORING
Bedside spirometry provides a rapid, objective assessment of patients and guides therapy. The forced expiratory volume in 1second (FEV1) and the peak expiratory flow rate (PEFR) rate directly measure the degree of large airway obstruction. Sequential
measurements help assess severity and determine response to therapy. A flow-volume loop can help distinguish asthma fromvocal cord dysfunction; the latter is o�en treated as asthma, sometimes with repeated visits. Vocal cord dysfunction responds tothe moisture, not the drug, in a nebulized treatment, and "fails" metered-dose inhaler outpatient therapy because moisture isnot a part of that delivery system. If not documented, obtain a full spirometry assessment only in patients with frequentoutpatient failures.
Signs on physical examination and the subjective symptoms do not necessarily correlate well with the severity of airflowobstruction, making objective measures valuable. Patient cooperation is essential for these tests to be reliable, limiting the
value of spirometry in severe exacerbations or in noncooperative patients.7,8,9,10
Pulse oximetry assesses oxygen saturation during treatment. Arterial blood gas measurement is not needed in most patientswith mild to moderate asthma exacerbation, and it should be reserved for suspected hypoventilation with carbon dioxideretention and respiratory acidosis. With acute attacks, ventilation is stimulated, resulting in a decrease in partial pressure ofarterial carbon dioxide (Paco2). Therefore, a normal or slightly elevated Paco2 (e.g., >42 mm Hg) indicates extreme airway
obstruction and fatigue and may herald the onset of acute ventilatory failure. Patients with impending respiratory failure almost
always have clinical evidence of severe attacks or spirometry demonstrating a PEFR or FEV1 <25% predicted.11 The use of
capnography in acute asthma management is unclear. One small study reported good concordance between expired carbon
dioxide levels measured by capnography and arterial carbon dioxide concentration,12 but another reported di�erences of up to
10 mm Hg or more between the two measurements.13
Radiography is indicated only if there is clinical suspicion of pneumothorax, pneumomediastinum, pneumonia, or other causefor symptoms (e.g., acute heart failure) or complication of asthma. For admitted asthma patients, less than one third of patients
have an abnormal chest radiograph.14

9/12/2019
6/21
A CBC is not routinely needed and likely will show modest leukocytosis secondary to administration of β-agonist therapy orcorticosteroids. For those few patients taking theophylline, measure the serum level. Routine ECG is also unnecessary but mayreveal right ventricular strain, abnormal P waves, or nonspecific ST- and T-wave abnormalities, which resolve with treatment.Older patients, especially those with coexisting heart disease, should have cardiac monitoring during treatment.
STANDARD TREATMENT
The goal is rapid reversal of airflow obstruction by repetitive or continuous administration of inhaled β2-agonists, ensuring
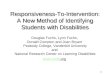
adequate oxygenation, and relieving inflammation.7,8,9,10 Figure 69-1 shows the National Asthma Education and Prevention
Program Expert Panel ED treatment algorithm.10 The following categories of medications are used in the treatment of acuteasthma: β-adrenergic agonists, anticholinergics, and glucocorticoids. Treatments for impending or actual respiratory arrest arediscussed below in "Status Asthmaticus."
FIGURE 69-1.
Management of asthma exacerbations: ED and hospital-based care. FEV1 = forced expiratory volume in 1 second; ICS = inhaled
corticosteroid; MDI = metered-dose inhaler; PEFR = peak expiratory flow rate; SABA = short-acting β2-agonist; Sao2 = oxygen
saturation by pulse oximetry. [Source: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf (National Heart, Lung, andBlood Institute; National Institutes of Health; U.S. Department of Health and Human Services: National Asthma Education andPrevention Program, Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Publication No. 08-4051.Bethesda, MD, National Institutes of Health, 2007.) Accessed November 18, 2014.]

9/12/2019
7/21
ADRENERGIC AGENTS

9/12/2019
8/21
β-Adrenergic agonists with rapid onset are the preferred initial rescue medication for acute bronchospasm (Table 69-5).Stimulation of β1-receptors increases rate and force of cardiac contraction and decreases small intestine motility and tone,
whereas β2-adrenergic stimulation promotes bronchodilation, vasodilation, uterine relaxation, and skeletal muscle tremor.

9/12/2019
9/21
TABLE 69-5
β-Adrenergic, Anticholinergic, and Steroid Dosages of Drugs for Asthma
Medication Dose Comments
Inhaled β2-Agonists
Albuterol
Nebulizer solution (0.63
milligram/3 mL, 1.25
milligrams/3 mL, 2.5
milligrams/3 mL, 5.0
milligrams/mL)
2.5–5 milligrams every 20 min for
three doses, then 2.5–10
milligrams every 1–4 h, as needed,
or 10–15 milligrams/h as
continuous nebulization.
Only selective β2-agonists are recommended. For optimal
delivery, dilute aerosols to minimum of 3 mL at gas flow of 6–8
L/min. Use large-volume nebulizers for continuous
administration. May mix with ipratropium nebulizer solution.
MDI (90 micrograms/pu�) 4–8 pu�s every 20 min up to 4 h,
then every 1–4 h as needed.
In mild-to-moderate exacerbations, MDI plus valved holding
chamber is as e�ective as nebulized therapy with appropriate
administration technique and coaching by trained personnel.
Bitolterol
Nebulizer solution (2
milligrams/mL)
See albuterol dose. Has not been studied in severe asthma exacerbations. Do not
mix with other drugs.
MDI (370
micrograms/pu�)
See albuterol MDI dose. Has not been studied in severe asthma exacerbations.
Levalbuterol (R-albuterol)
Nebulizer solution (0.63
milligram/3 mL, 1.25
milligrams/3 mL)
1.25–2.5 milligrams every 20 min
for three doses, then 1.25–5
milligrams every 1–4 h, as needed.
Levalbuterol administered in one half the milligram dose of
albuterol provides comparable e�icacy and safety. Has not
been evaluated by continuous nebulization.
MDI (45 micrograms/pu�) See albuterol MDI dose.
Pirbuterol
MDI (200
micrograms/pu�)
See albuterol MDI dose. Has not been studied in severe asthma exacerbations.
Systemic (Injected) β2-Agonists
Epinephrine
1:1000 (1 milligram/mL) 0.3–0.5 milligram every 20 min for
three doses SC.
No proven advantage of systemic therapy over aerosol.
Terbutaline

9/12/2019
10/21
Medication Dose Comments
(1 milligram/mL) 0.25 milligram every 20 min for
three doses SC.
No proven advantage of systemic therapy over aerosol.
Anticholinergics/Combinations
Ipratropium bromide
Nebulizer solution (0.25
milligram/mL)
0.5 milligram every 20 min for
three doses, then as needed.
May mix in same nebulizer with albuterol. Should not be used
as first-line therapy; should be added to SABA therapy for
severe exacerbations. The addition of ipratropium has not
been shown to provide further benefit once the patient is
hospitalized.
MDI (18 micrograms/pu�) Eight pu�s every 20 min, as
needed, up to 3 h.
Should use with valved holding chamber and face mask for
children <4 y. Studies have examined ipratropium bromide
MDI for up to 3 h.
Ipratropium with albuterol
Nebulizer solution (each 3-
mL vial contains 0.5
milligram of ipratropium
bromide and 2.5
milligrams of albuterol.)
3 mL every 20 min for three doses,
then as needed.
May be used for up to 3 h in the initial management of severe
exacerbations. The addition of ipratropium has not been
shown to provide further benefit once the patient is
hospitalized.
MDI (each pu� contains 18
micrograms of
ipratropium bromide and
90 micrograms of
albuterol.)
Eight pu�s every 20 min as
needed up to 3 h.
Should use with valved holding chamber and face mask for
children <4 y.
Systemic Corticosteroids Applies to all three corticosteroids for oral medications.
Prednisone For inpatients: oral "burst," use
40–80 milligrams/d in one or two
divided doses until PEFR reaches
70% of predicted or personal best.
For outpatients: oral "burst," use 40–60 milligrams in single or
two divided doses for 5–10 d.
Methylprednisolone IV: 1 milligram/kg every 4–6 h. For outpatients: a single IM dose of 150 milligrams depot
methylprednisolone may be used.19
Prednisolone 1–2 milligrams/kg/d for 5–10 d;
may be divided twice daily.
More frequently used over prednisone in children due to
increased palatably of available liquid formulations.

9/12/2019
11/21
Notes: There is no known advantage for higher doses of corticosteroids in severe asthma exacerbations, nor is there any advantage for IV
administration over oral therapy provided GI transit time or absorption is not impaired.
The course of systemic corticosteroids for an asthma exacerbation requiring an ED visit or hospitalization may last from 3 to 10 days. For
corticosteroid courses of <1 week, there is no need to taper the dose. For slightly longer courses (e.g., up to 10 days), there probably is no
need to taper, especially if patients are concurrently taking inhaled corticosteroids.
Inhaled corticosteroids can be started at any point in the treatment of an asthma exacerbation.
Abbreviations: MDI = metered-dose inhaler; PEFR = peak expiratory flow rate.
Source: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf (National Heart, Lung, and Blood Institute; National Institutes of Health;
U.S. Department of Health and Human Services: National Asthma Education and Prevention Program, Expert Panel Report 3: Guidelines for
the Diagnosis and Management of Asthma. Publication No. 08-4051. Bethesda, MD, National Institutes of Health, 2007.) Accessed November
18, 2014.
β-Adrenergic drugs cause bronchodilation by stimulation of the enzyme adenyl cyclase, which converts intracellular adenosinetriphosphate into cyclic adenosine monophosphate. This action enhances the binding of intracellular calcium to cellmembranes, reducing the myoplasmic calcium concentration, and results in relaxation of bronchial smooth muscle. β-Adrenergic drugs also inhibit mediator release and promote mucociliary clearance.
The most common side e�ect of β-adrenergic drugs is skeletal muscle tremor. Patients also may experience nervousness,anxiety, insomnia, headache, hyperglycemia, palpitations, tachycardia, and hypertension. Clinical toxicity is rare and lesscommon than undertreatment complications. Provoking dysrhythmias or myocardial ischemia is rare, especially in thosewithout a prior history of coronary artery disease. The older catecholamine bronchodilators, such as epinephrine, are not β2
specific and have a short duration of action.
Albuterol is a 50:50 racemic mixture (equal amounts of le� and right isomers); it is now available in the hydrofluoroalkaneformulation, which has increased the cost and the e�ectiveness. The R isomer has great binding a�inity for the β2-receptor and
is responsible for bronchodilation. The S isomer has no bronchodilatory e�ect but has a long half-life (12 hours); this isomer
may be responsible for late paradoxical bronchospasm in some patients. Levalbuterol (Xopenex®) is the pure R isomer form ofthe drug, intended to improve e�ectiveness and limit side e�ects such as tachycardia and rhythm change. Both racemicalbuterol and levalbuterol can be given as intermittent or continuous nebulizations. Levalbuterol costs 5 to 25 times more than
albuterol, and it has no clear advantage over albuterol regarding symptom change, admission, or tachycardia.15,16,17
Nonprescription racemic epinephrine (Asthmanefrin®) replaced Primatene® as an over-the-counter medication, and the cost is
less than for prescription β2-adrenergics. Asthmanefrin® contains 11.25 milligrams of racemic epinephrine/0.5 mL. In one study,
subjects recruited through local pharmacies reported no worse asthma outcomes than individuals treated with prescription β-
agonists.18 No other data exist to guide use of Asthmanefrin® versus prescribed agents.
Aerosol therapy with β2-adrenergic drugs produces excellent bronchodilation and is favored over oral or parenteral routes. The
aerosol route achieves topical administration of a relatively small dose of drug, thereby producing local e�ects with minimumsystemic absorption and fewer side e�ects. Aerosol delivery occurs with a metered-dose inhaler coupled to a spacing device or
with a compressor-driven nebulizer.20 A spacing device attached to the inhaler improves drug deposition; when optimally used,metered-dose inhaler therapy delivers the most drug to target airways, better than nebulized therapy. Even with optimumtechnique, a maximum of 15% of the drug dose is retained in the lungs, regardless of the aerosol method used.
Aerosol treatments may be administered every 15 to 20 minutes or on a continuous basis.21 Subcutaneous epinephrine andterbutaline are options for patients unable to coordinate aerosolized or metered-dose inhaler treatments, seen o�en in severe

9/12/2019
12/21
airflow-limited states. IV β-agonist infusions o�er no advantage over aerosolized or metered-dose inhaler–delivered agents and
carry increased risk.22
Salmeterol xinafoate and formoterol are β2-adrenoreceptor agonists that bind with greater a�inity to the β2-receptor site than
albuterol. They are indicated for twice-daily maintenance therapy. Neither drug should be used for acute asthma exacerbations.Bronchodilator e�ects last at least 12 hours, and tachyphylaxis has not been reported with long-term use. The number ofasthma-related deaths among patients receiving salmeterol, especially in African Americans, has increased for unknownreasons, although this may be due to failure to recognize the need for or use rescue short-acting agents and to seek careappropriately. Long-acting β2-adrenoreceptor agonists are an e�ective treatment for long-term control of asthma, especially in
conjunction with inhaled corticosteroids. Short-acting β2-adrenoreceptor agonists are used for infrequent or breakthrough
symptoms that occur despite the use of long-acting β2-adrenoreceptor agonists.7,8,9,10,21
CORTICOSTEROIDS
Corticosteroids are a cornerstone of asthma treatment. Steroids produce beneficial e�ects by restoring β-adrenergicresponsiveness and reducing inflammation. The peak anti-inflammatory e�ect occurs at least 4 to 8 hours a�er IV or POadministration, but early use is wise to enhance care quickly; corticosteroids given within 1 hour of arrival in the ED reduce the
need for hospitalization.23 Although there is disagreement over the optimal dose in acute asthma, an initial dose of POprednisone of 40 to 60 milligrams or IV methylprednisolone of 1 milligram/kg is su�icient, and higher-dose corticosteroid
therapy o�ers no advantage.24 Admitted patients should receive additional daily corticosteroids until subjective and objectiveimprovements are achieved. Patients who are being discharged home with an FEV1 or PEF of <70% predicted a�er aggressive
ED treatment should be prescribed a 5- to 10-day nontapering course of prednisone (40 to 60 milligrams/d in a single daily dose
or its equivalent) or a 2-day course of oral dexamethasone (16 milligrams/d in a single daily dose).7,8,9,10,19,25,26 A single dose of
depot methylprednisolone, 150 milligrams IM, is another option if compliance is a concern.27
Current recommendations favor inhaled corticosteroids for all patients with mild persistent asthma or more severe
asthma.7,8,9,10 This means discharging patients with mild persistent or more severe asthma on maintenance inhaled
corticosteroids in addition to any systemic bursts.28,29,30,31 Inhaled corticosteroid options are beclomethasone, 80 to 240micrograms/d; budesonide, 180 to 600 micrograms/d; flunisolide, 500 to 1000 micrograms/d; fluticasone, 88 to 264micrograms/d; mometasone, 200 micrograms/d; and triamcinolone acetonide, 300 to 750 micrograms/d.
ANTICHOLINERGICS
The e�ects of anticholinergics used in combination with β-adrenergic agents are additive. Anticholinergics a�ect large, centralairways, whereas β-adrenergic drugs dilate smaller airways. Anticholinergic drugs competitively antagonize acetylcholine at thepostganglionic junction between the parasympathetic nerve terminal and e�ector cell. This process blocks thebronchoconstriction induced by vagal cholinergic-mediated innervation to the larger central airways. In addition,anticholinergics reduce concentrations of cyclic guanosine monophosphate in airway smooth muscle, further promotingbronchodilation.
The anticholinergic commonly used is inhaled ipratropium bromide. Ipratropium is available as a nebulized solution and a
metered-dose inhaler or in combination with albuterol7,8,9,10 (Table 69-5). Use an aerosolized ipratropium bromide solution, 0.5
milligrams, in patients with moderate to severe exacerbation.7,8,9,10 Adding multiple doses of ipratropium bromide to a short-acting selective β-agonist may improve bronchodilation and decrease the need for hospitalization among severely obstructed
asthmatics,32 although this benefit is not universal.33 Potential side e�ects with anticholinergics include dry mouth, thirst, and

9/12/2019
13/21
di�iculty swallowing. Less commonly, tachycardia, restlessness, irritability, confusion, di�iculty in micturition, ileus, blurring ofvision, or an increase in intraocular pressure can occur. Long-acting anticholinergic agents have no role in acute care.
STATUS ASTHMATICUS (ACUTE SEVERE ASTHMA)
Status asthmaticus is an acute severe asthma attack that does not improve with usual doses of inhaled bronchodilators andsteroids. Signs and symptoms include hypoxemia, tachypnea, tachycardia, accessory muscle use, and wheezing. Wheezing maybe absent when airflow is severely reduced. Rapid treatment is the key to preventing cardiopulmonary arrest. In addition tousual and ongoing bronchodilators coupled with early steroids, other treatment adjuncts exist.
MAGNESIUM
IV magnesium sulfate is indicated in the management of acute, very severe asthma (FEV1 <25% predicted).34 The magnesium
dose is 1 to 2 grams IV over 30 minutes. Nebulized magnesium is e�ective and may also improve pulmonary function in severe
asthma when it follows aggressive β-agonist and steroid therapy.34,35,36 Dosing regimens vary; one regimen is 95 milligrams ofnebulized magnesium sulfate in four divided doses 20 minutes apart, and another is 384 milligrams of nebulized magnesium
sulfate in sterile water.37 When using magnesium in any form, monitor blood pressure and deep tendon reflexes during
administration37 because hypotension or neuromuscular blockade may occur, although this is exceptionally rare in the dosesrecommended.
NONINVASIVE POSITIVE-PRESSURE VENTILATION
Noninvasive positive-pressure ventilation (see chapter 28, "Noninvasive Airway Management") improves airflow andrespirations compared with usual care, and despite little research, it is commonly used in clinical practice for acute life-
threatening asthma.38,39 Noninvasive positive-pressure ventilation decreases the need for intubation, results in clinical
improvement, and decreases the need for hospitalization.39 Do not institute noninvasive positive-pressure ventilation ifintubation is indicated or in patients with suspected pneumothorax.
KETAMINE
Ketamine inhibits reuptake of noradrenaline and thus increases circulating catecholamines, aiding some with severe asthma.
An IV bolus dose of 0.2 milligram/kg followed by an infusion of 0.5 milligram/kg/h is sometimes used;40 higher doses are
validated.41 If intubation is needed, ketamine is a good agent to aid during the procedure and a�er mechanical ventilationstarts. Controlled trials substantiating ketamine's e�icacy in treating severe acute asthma are lacking.
EPINEPHRINE
Although epinephrine is standard treatment for anaphylactic asthma, it is overlooked as an adjunct to treat status asthmaticus.
Epinephrine can be given SC or IM, 0.5 milligram in adults (standard adult EpiPen® dose), in refractory situations.41
MECHANICAL VENTILATION
If the patient manifests progressive hypercarbia or acidosis or becomes exhausted or confused, intubation and mechanicalventilation (see chapter 29, "Intubation and Mechanical Ventilation") are necessary to prevent respiratory arrest. Mechanicalventilation does not relieve the airflow obstruction—it merely eliminates the work of breathing and enables the patient to restwhile the airflow obstruction is resolved.

9/12/2019
14/21
The potential complications of mechanical ventilation in asthmatic patients include extremely high peak airway pressures withsubsequent barotrauma and hemodynamic impairment. Mucous plugging is frequent, leading to increased airway resistance,atelectasis, and pulmonary infection. Due to the severity of airflow obstruction during the early phases of treatment, the tidalvolume may be larger than the returned volume, leading to air trapping and increased residual volume (intrinsic positive end-expiratory pressure). Using rapid inspiratory flow rates at a reduced respiratory frequency (12 to 14 breaths/min) and allowingadequate time for the expiratory phase can mitigate these e�ects. Also, it is reasonable to target adequate arterial oxygensaturation (≥90%) without concern for "normalizing" the hypercarbic acidosis. This approach is called controlled mechanicalhypoventilation or permissive hypoventilation.
Ventilation of asthmatic patients requires sedation. Neuromuscular blocking agents may be required, but extended use may
cause postextubation muscle weakness.42 See chapter 111, Intubation and Ventilation in Infants and Children for furtherdiscussion.
AGENTS OF UNCERTAIN OR NO BENEFIT IN STATUS ASTHMATICUS
Heliox
A mixture of 80% helium and 20% oxygen (heliox) can lower airway resistance and act as an adjunct in the treatment of severe
asthma exacerbations.43 Heliox does not reliably avert tracheal intubation, change intensive care and hospital admission rates
and duration, or decrease mortality in severe asthma.43
Methylxanthines
Aminophylline is no longer a first- or second-line treatment for acute asthma.44 The most common side e�ects ofmethylxanthines are nervousness, nausea, vomiting, anorexia, and headache. At plasma levels >30 milligrams/mL, there is arisk of seizures and cardiac arrhythmias.
Other Agents
Mast cell modifiers, such as cromolyn and nedocromil, exert their anti-inflammatory action by blockage of chlorine channels,modulating mast cell mediator release and eosinophil recruitment. These agents also inhibit early and late responses toallergen challenge and exercise. Neither is indicated for treatment of acute bronchospasm.
Leukotrienes are potent proinflammatory mediators that contract airway smooth muscle, increase microvascular permeability,stimulate mucus secretion, decrease mucociliary clearance, and recruit eosinophils into the airway. Several leukotrienemodifiers, namely montelukast, zafirlukast, and zileuton, are available as oral tablets for the treatment of asthma. Leukotrienemodifiers improve lung function, diminish symptoms, and diminish the need for short-acting β2-agonists. They may be used as
an alternative to low-dose inhaled corticosteroid therapy in mild persistent asthmatics and as steroid-sparing agents with
inhaled corticosteroids in moderate persistent asthmatics.7,8,9,10 Despite one trial with adjuvant IV montelukast for acute
asthma,45 there is no indication for the use of any of the leukotriene modifiers in the ED.
DISPOSITION AND FOLLOW-UP
Disposition decisions should take into account a combination of subjective parameters, such as resolution of wheezing andimprovement in air exchange, as assessed by auscultation and patient opinion; objective measures, such as normalization ofFEV1 or PEFR; and historical factors, such as compliance, history of ED use, and hospitalization. Some degree of residual airflow
obstruction, airway lability, and inflammation persists a�er treatment and discharge from the ED.

9/12/2019
15/21
Advise discharged patients to use a short-acting β-agonist on a scheduled basis for several days and to complete any oralcorticosteroids regimens. Add inhaled corticosteroids in patients with a history of persistent asthma who are not already using
this regimen.28,29,30
A good response to treatment resolves symptoms and results in a PEFR or FEV1 of >70% predicted; these patients can be safely
discharged home. Patients with a poor response to treatment have persistent symptoms and FEV1 or PEFR of <40% predicted;
these patients are usually best observed or admitted. An incomplete response to treatment, the middle ground, is defined assome persistence of symptoms and a PEF or FEV1 between 40% and 69% predicted. Most asthmatics treated in the ED fall into
this category and may be discharged home safely, although some benefit from prolonged observation or admission7,8,9,10
(Table 69-2).
Patients who fail to improve adequately over a period of several hours because they are in the late phase of their exacerbationand those with significant risk factors for death from asthma are best placed in an observation unit or hospital bed. Many
patients can be successfully treated in an ED observation unit with evidence-based care protocols.46 Intubated patients requireintensive care unit admission.
Arrange follow-up care to ensure resolution and to review the long-term medication plan for the chronic management of
asthma. High previous relapse rates suggest the need for follow-up within 1 to 4 weeks of the ED visit.7,8,9,10 Deliver anappropriate written discharge plan of action that addresses routine care and care of worsening symptoms (Table 69-6). Educatepatients on asthma triggers, and review all discharge medications and the correct use of the inhaler and a peak flow meter (fordaily tracking).

9/12/2019
16/21
Abbreviation: MDI = metered dose inhaler.
Source: National Heart, Lung, and Blood Institute; National Institutes of Health; U.S. Department of Health and Human Services.
1.
TABLE 69-6
Checklist for ED Discharge
Intervention Dose/Timing Education/AdviceMD/RN
Initials
Inhaled medications
(e.g., MDI with valved
holding chamber;
nebulizer)
Select agent, dose, and frequency (e.g.,
albuterol).
Teach purpose.
Short-acting β2-
agonist
2–6 pu�s every 4 h for __ days. Teach and check technique.
Corticosteroids Low to medium dose for patients with
chronic persistent asthma.
For MDIs, emphasize the importance of using a
spacing device or holding chamber.
Oral medications Select agent, dose, and frequency (e.g.,
prednisone 40 milligrams once a day for
10 d).
Teach purpose.
Teach side e�ects.
Peak flow meter For selected patients: measure a.m. and
p.m. peak expiratory flow, and record
best of three tries each time.
Teach purpose.
Teach technique.
Distribute peak flow diary.
Follow-up visit If possible, make appointment for
follow-up care with primary clinician or
asthma specialist or advise patient to
make appointment.
Advise patient (or caregiver) of date, time, and
location of appointment, ideally within 7 d of
hospital discharge.
Action plan Before or at discharge. Instruct patient (or caregiver) on simple plan for
actions to be taken when symptoms, signs, and
peak expiratory flow values suggest recurrent
airflow obstruction.
REFERENCES
Blackwell DL, Lucas JW, Clarke TC: Summary health statistics for U.S. adults: National Health Interview Survey, 2012.National Center for Health Statistics. Vital Health Stat 10: 260, 2014. [PubMed: 24819891]

9/12/2019
17/21
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Bloom B, Jones LI, Freeman G: Summary health statistics for U.S. children: National Health Interview Survey, 2012. NationalCenter for Health Statistics. Vital Health Stat 10: 258, 2013. [PubMed: 22338334]
Oraka E, Kim HJ, King ME et al.: Asthma prevalence among U.S. elderly by age groups: age still matters. J Asthma 49: 593,2012. [PubMed: 22765313]
Kudo M, Ishigatsubo Y, Aoki I: Pathology of asthma. Front Microbiol 4: 263, 2013. [PubMed: 24032029]
Saraya T, Kurai D, Ishii H et al.: Epidemiology of virus-induced asthma exacerbations: with special reference to the role ofhuman rhinovirus. Front Microbiol 5: 226, 2014. [PubMed: 24904541]
Bonds RS, Midoro-Horiuti T: Estrogen e�ects in allergy and asthma. Curr Opin Allergy Clin Immunol 13: 92, 2013. [PubMed: 23090385]
Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma [GINA] 2014.http://www.ginasthma.org/. Accessed July 31, 2014.
British Guideline on the Management of Asthma: A National Guideline, 2012. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-guideline-on-the-management-of-asthma/. Accessed July 31, 2014.
National Asthma Council Australia: Australian Asthma Handbook, Version 1.0. Melbourne, 2014.http://www.asthmahandbook.org.au. Accessed August 21, 2014.
National Asthma Education and Prevention Program, Expert Panel Report 3: Guidelines for the Diagnosis and Managementof Asthma. Publication No. 08-4051. Bethesda, MD: National Institutes of Health, 2007.http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed November 18, 2014.
Martin TG, Elenbaas RM, Pingleton SH: Use of peak expiratory flow rates to eliminate unnecessary arterial blood gases inacute asthma. Ann Emerg Med 11: 70, 1982. [PubMed: 6814315]
Corbo J, Bijur P, Lahn M et al.: Concordance between capnography and arterial blood gas measurements of carbon dioxidein acute asthma. Ann Emerg Med 46: 323, 2005. [PubMed: 16187465]
Delerme S, Freund Y, Renault R et al.: Concordance between capnography and capnia in adults admitted for acute dyspneain an ED. Am J Emerg Med 28: 711, 2010. [PubMed: 20637388]
Beng Leong L, Vasu A, Cham Wai Ming G: Identifying adult asthmatic patients with an abnormal chest radiograph in theemergency department. Eur J Emerg Med 19: 95, 2012. [PubMed: 21730867]

9/12/2019
18/21
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
Kim HN: Xopenex: is it worth the money? Clinical Correlations. The NYU Langone Online Journal of Medicine. August 16,2012. www.clinicalcorrelations.org/?p=5705. Accessed November 18, 2014.
Wilkinson M, Bulloch B, Garcia-Filion P et al.: E�icacy of racemic albuterol versus levalbuterol used as a continuousnebulization for the treatment of acute asthma exacerbations: a randomized, double-blind, clinical trial. J Asthma 48: 188,2011. [PubMed: 21275850]
Khorfan FM, Smith P, Watt S et al.: E�ects of nebulized bronchodilator therapy on heart rate and arrhythmias in critically illadult patients. Chest 140: 1466, 2011. [PubMed: 21960699]
Douglass JA, Goeman DP, McCarthy EA et al.: Over-the-counter B2 agonist purchase versus script: a cross-sectional study.Respir Med 106: 223, 2012. [PubMed: 22040532]
Kravitz J, Dominici P, Ufberg J et al.: Two days of dexamethasone versus 5 days of prednisolone in the treatment of acuteasthma: a randomized controlled trial. Ann Emerg Med 58: 200, 2011. [PubMed: 21334098]
Cates CJ, Welsh EJ, Rowe BH: Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma.Cochrane Database Syst Rev 9: CD000052, 2013. [PubMed: 24037768]
Papi A, Corradi M, Pigeon-Francisco C: Beclomethasone-formoterol as maintenance and reliever treatment in patients withasthma: a double-blind, randomised controlled trial. Lancet Respir Med 1: 23, 2013. [PubMed: 24321801]
Travers AH, Milan SJ, Jones AP: Addition of intravenous beta(2)-agonists to inhaled beta(2)-agonists for acute asthma.Cochrane Database Syst Rev 12: CD010179, 2012. [PubMed: 23235685]
Rowe BH, Spooner C, Ducharme FM et al.: Early emergency department treatment of acute asthma with systemiccorticosteroids. Cochrane Database Syst Rev 1: CD002178, 2001. [PubMed: 11279756]
Emerman CL, Cydulka RK: A randomized comparison of 100-milligrams vs 500-milligrams dose of methylprednisolone inthe treatment of acute asthma. Chest 107: 1559, 1995. [PubMed: 7781346]
Cossette B, Beauchesne MF, Forget A et al.: Systemic corticosteroids for the treatment of asthma exacerbations during andoutside of pregnancy in an acute-care setting. Respir Med 108: 1260, 2014. [PubMed: 25060542]
Rowe BH, Spooner CH, Ducharme FM et al.: Corticosteroids for preventing relapse following acute exacerbations ofasthma. Cochrane Database Syst Rev 3: CD000195, 2007. [PubMed: 17636617]

9/12/2019
19/21
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
Lahn M, Bijur P, Gallagher EJ: Randomized clinical trial of intramuscular vs oral methylprednisolone in the treatment ofasthma exacerbations following discharge from an emergency department. Chest 126: 362, 2004. [PubMed: 15302718]
Cydulka RK, Tamayo-Sarver JH, Wolf C et al.: Inadequate follow-up controller medications among patients with asthmawho visit the emergency department. Ann Emerg Med 46: 316, 2005. [PubMed: 16187464]
Price D, Fletcher M, van der Molen T: Asthma control and management in 8,000 European patients: the REcognise Asthmaand LInk to Symptoms and Experience (REALISE) survey. NPJ Prim Care Respir Med 24: 14009, 2014. [PubMed: 24921985]
Williams LK, Peterson EL, Wells K et al.: Quantifying the proportion of severe asthma exacerbations attributable to inhaledcorticosteroid nonadherence. J Allergy Clin Immunol 128: 1185, 2011. [PubMed: 22019090]
Filiatrault L, Harriman D, Abu-Laban RB et al.: Compliance with the Canadian Association of Emergency Physicians'asthma clinical practice guidelines at a tertiary care emergency department. CJEM 14: 224, 2012. [PubMed: 22813396]
Rodrigo GJ, Castro-Rodriguez JA: Anticholinergics in the treatment of children and adults with acute asthma: a systematicreview with meta-analysis. Thorax 60: 740, 2005. [PubMed: 16055613]
Cydulka RK, Emerman CL, Muni A: Levalbuterol versus levalbuterol plus ipratropium in the treatment of severe acuteasthma. J Asthma 47: 1094, 2010. [PubMed: 20923385]
Kew KM, Kirtchuk L, Michell CI: Intravenous magnesium sulfate for treating adults with acute asthma in the emergencydepartment. Cochrane Database Syst Rev 5: CD010909, 2014. [PubMed: 24865567]
Blitz M, Blitz S, Hughes R et al.: Aerosolized magnesium sulfate for acute asthma: a systematic review. Chest 128: 337,2005. [PubMed: 16002955]
Goodacre S, Cohen J, Bradburn M et al.: Intravenous or nebulised magnesium sulphate versus standard therapy for severeacute asthma (3Mg trial): a double-blind, randomised controlled trial. Lancet Respir Med 1: 293, 2013. [PubMed: 24429154]
Shirk MB, Donahue R, Shirvani J: Unlabeled uses of nebulized medications. Am J Health Syst Pharm 63: 1704, 2006. [PubMed: 16960254]
Pallin M, Naughton M: Noninvasive ventilation in acute asthma. J Crit Care 29: 586, 2014. [PubMed: 24735521]
Lim WJ, Mohammed AR, Carson KV: Non-invasive positive pressure ventilation for treatment of respiratory failure due tosevere acute exacerbations of asthma. Cochrane Database Syst Rev 12: CD004360, 2012.

9/12/2019
20/21
40.
41.
42.
43.
44.
45.
46.
[PubMed: 23235608]
Shenvi C: Getting creative with ketamine. EPM September 2014. http://www.epmonthly.com/features/current-features/getting-creative-with-ketamine/. Accessed November 18, 2014.
Management of life-threatening asthma in the emergency department. http://emupdates.com/wp-content/uploads/2011/12/MOLTAITEDv6.pdf. Accessed November 18, 2014.
Adnet F, Dhissi G, Borron SW et al.: Complication profiles of adult asthmatics requiring paralysis during mechanicalventilation. Intensive Care Med 27: 1729, 2001. [PubMed: 11810115]
Colebourn CL, Barber V, Young, JD: Use of helium–oxygen mixture in adult patients presenting with exacerbations ofasthma and chronic obstructive pulmonary disease: a systematic review. Anaesthesia 62: 34, 2007. [PubMed: 17156225]
Nair P, Milan SJ, Rowe BH: Addition of intravenous aminophylline to inhaled beta(2)-agonists in adults with acute asthma.Cochrane Database Syst Rev 12: CD002742, 2012. [PubMed: 23235591]
Camargo CA, Smithline HA, Malice MP et al.: A randomized controlled trial of intravenous montelukast in acute asthma. AmJ Respir Crit Care Med 167: 528, 2003. [PubMed: 12456380]
Leykum LK, Huerta V, Mortensen E: Implementation of a hospitalist-run observation unit and impact on length of stay(LOS): a brief report. J Hosp Med 5: E2, 2010. [PubMed: 20717893]
USEFUL WEB RESOURCES
American Lung Association—http://www.lungusa.org
British Thoracic Society, British Guidelines on the Management of Asthma— https://www.brit-thoracic.org.uk/guidelines-and-quality-standards/asthma-guideline/
Canadian Thoracic Society—http://www.respiratoryguidelines.ca/guideline/asthma
Global Initiative For Asthma—http://www.ginasthma.org
National Asthma Council Australia—http://www.nationalasthma.org.au/handbook
National Asthma Education and Prevention Program, Expert Panel Report 3: Guidelines—http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
National Asthma Education Program and Prevention Program. Working Group Report on -Managing Asthma During Pregnancy—http://www.nhlbi.nih.gov/health/prof/lung/asthma/astpreg/astpreg_full.pdf

9/12/2019
21/21
McGraw HillCopyright © McGraw-Hill EducationAll rights reserved.Your IP address is 75.148.241.33 Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair