Embed Size (px)
Citation preview
Polyuria
Nocturia
Urinary frequency
Normal urine output ? 800 – 2500 ML/Day
Physiological - primary polydipsia
Pathological – diabetes insipidus
Burning micturition
Increased frequency
increased Urgency
A/W disorders of urinary tract
Inability to retain urine in bladder
Neurogenic incontinence
Stress incontinence
Mechanical incontinence
Overflow incontinence
Psychogenic incontinence
Functional incontinence
Enuresis
Oliguria
Anuria
Diuresis
Natriuresis
Deterioration of renal functions resulting in
reduced GFR leading to accumulation of
urea ,creatinine , electrolytes ,and non
nitrogenous substances
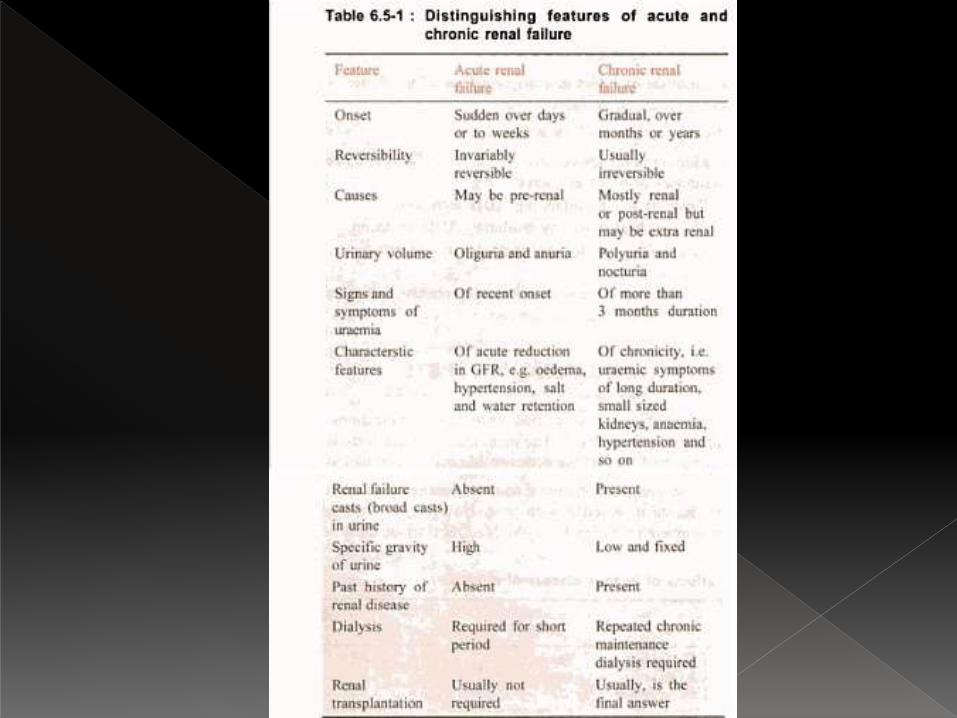
ARF
CRF
Oliguria
Anuria
Volume overload
Hyperkalemia
Metabolic acidosis
Hypoalcemia
Anorexia , nausea , vomiting , muscle
twitching , fits , coma
Sudden reduction in function of kidney A/w
rapid rise in urea and creatinine
Pre renal
Renal
Post renal
Pre renal – severe hemorrhage , shock ,
hypovolemia , burns , septicaemia
Renal – glomerulonephritis , acute tubular
necrosis
Post renal – urinary tract obstruction
Slow insidious onset
Irreversible loss of renal functions
Leading to uremia
Manifesting as excretory , metabolic ,
hematological , endocrinal functional
abnormalities
Maintenance of adequate water and
electrolyte balance
Control of infection
Control of BP
Acid base balance
Diet
Dialysis
Congenital disorders
Vascular disorders
Glomerular disorders
Tubulointestitial disorders
Obstructive disorders
Massive proteinuria and associated
complications
Hypoalbuminemia
Edema
Hyperlipidemia
Lipiduria
Hypercoagulability
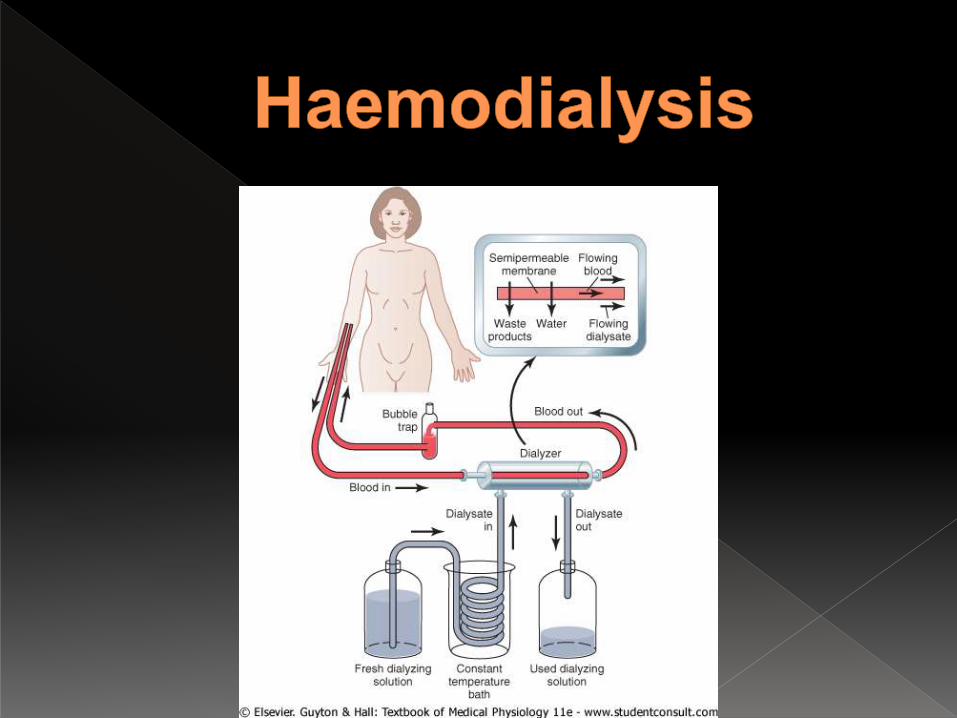
Haemodialysis
Peritoneal dialysis
Functions as artificial kidney in patients with
non functional kidneys
To treat patients in uremic coma
Uses the principle of diffusion of solutes
through a semi-permeable membrane
Can never replace a normal kidney
Does not provide endocrinal , hematological
function of kidney
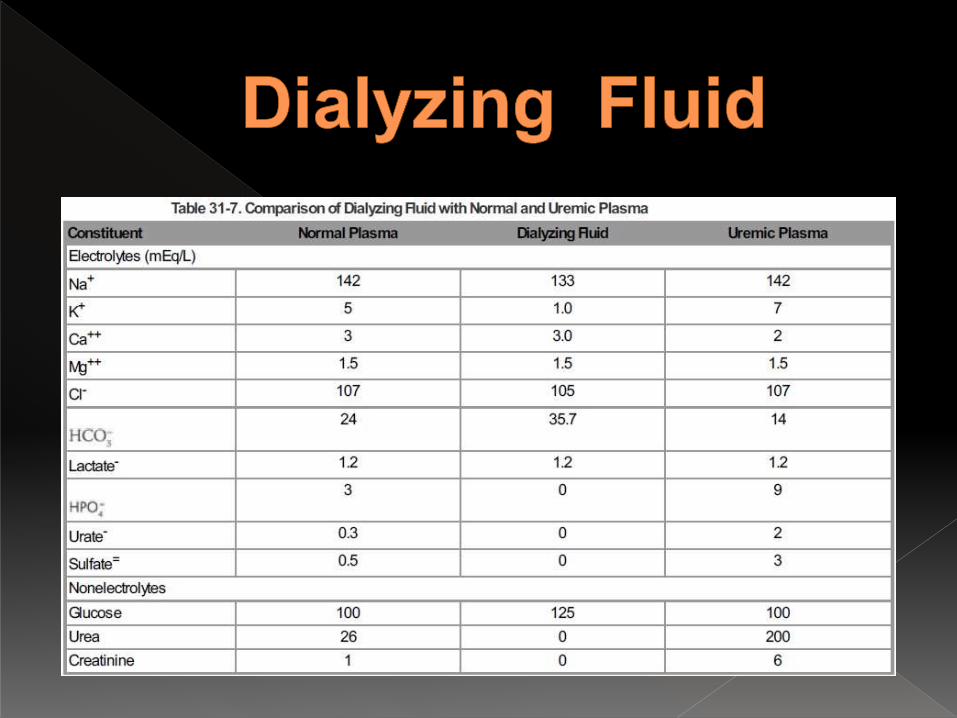
Dialyzing fluid
Uses heparin as an anti-coagulent
Drains blood from the patient through AV
fistula or large veins
Semi-permeable membrane allows passage
of all solutes except proteins
At any given time artificial kidney contains
500ml of blood
Used in both ARF and CRF
Needs hospitalization and monitoring
Needs AV fistula in CRF for repeated uses
One cycle runs for 4- 6 hours
Clears urea at the rate of 100 – 225 ml/min
Peritoneal membrane is used as dialyzing
membrane
No need for hospitalization
Used in young children and older individuals
Also known as CAPD
Two liters of dialyzing fluid is injected into the
peritoneum
Placement of permanent peritoneal catheter
Exchange happens for 15 min
Dialyzing fluid drained out and measured
One cycle for every 6 hours
Strict i/o chart is maintained
Irreversible or terminally damaged kidneys
ESRD
Donor – cadaveric
sibling
isogenic or allogenic
Left kidney is preferred
Rt iliac fossa is preferred
Immunosupression needed- prednisolone , cyclosporine
Substances increasing urine output
By increasing water excretion
Diuresis occurs along with natriuresis
Loss of both water and solutes
Used to reduce ECF volume
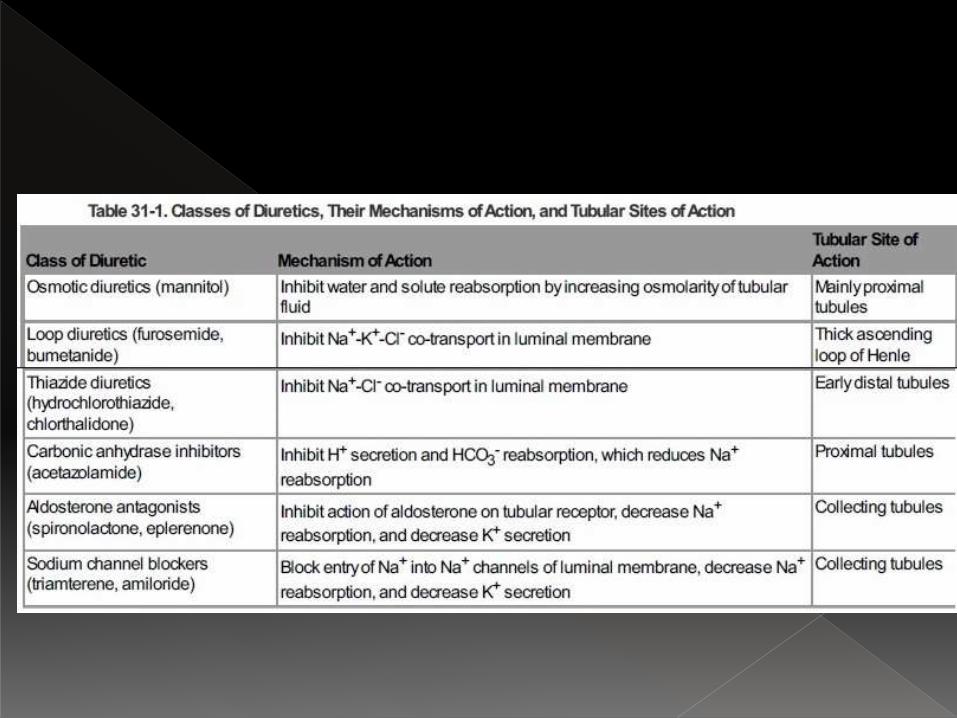
Depending upon their ability (effectiveness) they are classified under
High efficacy diuretics - Loop diuretics
Medium efficacy – Thiazides
Weak diuretic -
Osmotic diuretic
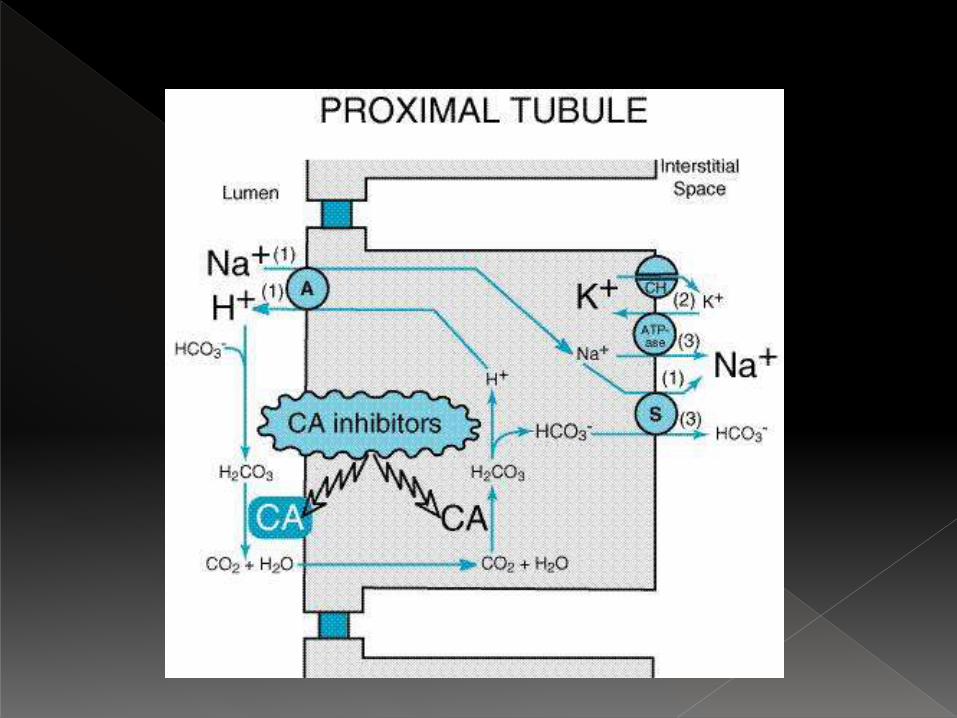
Carbonic anhydrase inhibitors
Aldosterone antagonist
Sodium channel blockers
Diuretics acting on PCT
Diuretics acting on loop of henle
Diuretics acting on DCT and CD
Potassium sparing diuretics
Acting on loop of TAL
Inhibiting Na- k- 2cl symporter
High efficacy diuretiics
Furosemide , bumetanide
Acts on early DCT
Inhibits Na –Cl symport
Medium efficacy drugs
Hydrochlorthiazide
Site of action is PCT
Inhibits H+ secretion thro Na H antiport
Causes loss of Na and bicarbonate
Acetazolamide ..
Mannitol , glycerol , isosorbide
Major site of action PCT
Causes increased osmolarity in the tubules
Loss of water through diffusion
Aldosterone antagonist
EnaC inhibitors
Acts on DT ,CD
Spironolactone , amiloride ,