-
8/21/2019 Renal Vascular Diseases
1/56
RENAL VASCULAR DISEASES
-
8/21/2019 Renal Vascular Diseases
2/56
2
DEFINITION (K/DOQI)
Renal artery disease (RAD) is defined as astenosis of the main
renal artery or its proximalbranches.
Significant RAD anatomicallyif there is a >50% stenosis of
the lumen
hemodynamicallyif the stenosis exceeds 75%. clinically
significant stenosis
RVHT - systemic hypertension due tohemodynamically significant
RAD.
Ischemic nephropathy decreased GFR due to hemodynamically
significant
RAD (K/DOQI)
impairment of renal function beyond occlusive diseaseof the main
renal arteries (Textor).
-
8/21/2019 Renal Vascular Diseases
3/56
3
SIGNIFICANCE
The prevalence and incidence of chronic kidneydisease (CKD) are
increasing.
ESRD incidente patients rates are 168 in Canada,1 250 in the USA
and 85.7 in Romania.
It is of importance to search for reversible causes
of CKD. Renal artery stenosis (RAS) may account for 5
22% of patients with ESRD who are older than 50years;
Correction of ischemic lesions can reversedecrease in renal
function and improve CVoutcomes.
-
8/21/2019 Renal Vascular Diseases
4/56
4
PREVALENCE
RAS due to:
Atherosclerotic renovascular disease (ARVD >90%)
Fibromuscular disease (FMD).
Takayashus arteritis up to 60% (Indian subcontinent
and the Far East)
autopsy studies- 450% of subjects, (16.4 vs. 5.5% > 60 vs
< 60 years)aortic angiography- 38% of patients with aortic
aneurysm,
- 33% in those with aortic occlusive disease- 39% lower limb
occlusive disease.cardiac catheterization- 1429% prevalence in
coronary disease- < 10% in normal coronary arteries .
-
8/21/2019 Renal Vascular Diseases
5/56
5
PATHOGENY (1)
ARVD is associated with three major clinical
syndromes:
ischemic renal disease
hypertension.
Renal failure (acute and chronic)
-
8/21/2019 Renal Vascular Diseases
6/56
6
PATHOGENY (2)
Interrelation among Renal-Artery Stenosis, Hypertension, and
Chronic Renal Failure
Robert D. Safian, M.D., and Stephen C. Textor, M.DNEJM, Nr 6,
vol 344:431-442,
2001
-
8/21/2019 Renal Vascular Diseases
7/56
7
RAS AND KIDNEY FUNCTION (1)
27% of those with RAS develop chronic renal failure within 6
years.
Nephrol Dial Transplant (2007) 22: 10021006; Atherosclerotic
renovascular
disease: beyond the renal artery stenosis; Pascal Meier, Jerome
Rossert,
Pierre-Francois Plouin ,Michel Burnier
-
8/21/2019 Renal Vascular Diseases
8/56
8
ISCHAEMIC NEPHROPATHY(1)
Interstitial fibrosis,
tubular atrophy,
glomerulosclerosis (including focal segmental
glomerulosclerosis),
periglomerular fibrosis
arteriolar abnormalities (hialinosclerosis,
atheroembolism).
atherosclerotic nephropathy
-
8/21/2019 Renal Vascular Diseases
9/56
9
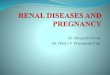
ISCHAEMIC NEPHROPATHY(2)
Histologic studies of interstitial fibrosis (Trichrome stain,
left two (a) low magnification and high magnification (b) and
immunohistochemistry for NF-kappa-B (NFkB, right) in swine. The
presence of renal artery stenosis (RAS) induces both
interstitial fibrosis and NFkB), which is accelerated by the
presence of high cholesterol levels (HC). (Chade AR,
Rodriguez-Porcel M, Grande JP, Krier JD, Lerman A, Romero JC,
Napoli C, Lerman LO: Distinct renal injury in earlyatherosclerosis
and renovascular disease. Circulation106: 11651171, 2002)
-
8/21/2019 Renal Vascular Diseases
10/56
10
ISCHAEMIC NEPHROPATHY(3)
Acu te renal fai lure
bilateral renal arterial occlusion (RAO)
intra-renal cholesterol atheroembolization damage from
radiocontrast agents during intra-
arterial angiography
hypovolaemia, often with concurrent diuretic use
concurrent use of angiotensin-converting enzymeinhibitors
(ACE-I) or angiotensin II receptor blockers(AII-RBs).
-
8/21/2019 Renal Vascular Diseases
11/56
11
ARVD AND ITS ASSOCIATION WITH
HEART AND OTHER VASCULAR
DISEASES (1)
Coronary artery disease
RAS is associated with more severe and
extensive coronary artery disease
? effects of renal ischemia or is a marker
for advanced atherosclerosis and
cardiovascular risk?
-
8/21/2019 Renal Vascular Diseases
12/56
12
ARVD AND ITS ASSOCIATION WITH
HEART AND OTHER VASCULAR
DISEASES (2)Cardiac dysfunction including flash pulmonary
oedema
presenting clinical syndrome in 41% of patients withbilateral
ARAS and in 12% of patients with unilateral ARAS.
angiotensin II promoted sodium retention and increase
inpulmonary microcirculation permeability
ARVD patients were found to have significantly
higherprevalence
left ventricular hypertrophy (78.5% compared with46.0%)
left ventricular diastolic dysfunction (40.5% comparedwith
12.0%),
greater left ventricular mass index (183 74 g/m2compared with
116 33 g/m2).
-
8/21/2019 Renal Vascular Diseases
13/56
13
ARVD AND ITS ASSOCIATION WITH
HEART AND OTHER VASCULAR
DISEASES (3)Ao rt ic aneurysm and per ipheral vascular
disease
Prevalence of ARVD in patients undergoing aortographyfor
intermittent claudication varying from 33%, 39%,
44.9%;Cerebrovascu lar disease
The coexistence of ARVD in patients who have strokeand/or
carotid stenoses In an autopsy series of 346cases of brain infarcts
>75% RAS was found in 10.4%of subjects and carotid artery
stenosis in 33.6%.
Patients with carotid stenosis were more likely to haveARVD than
those without carotid disease.
Conversely, ARVD patients are more likely to have
carotid disease.
-
8/21/2019 Renal Vascular Diseases
14/56
14
ARVD AND ITS ASSOCIATION WITH
HEART AND OTHER VASCULARDISEASES (4)
ARVD and hypertension ARVD is found in 25% of all cases of
hypertension
90% of patients with ARVD are hypertensive.
hypertension precedes ARVD development in many
cases.
-
8/21/2019 Renal Vascular Diseases
15/56
15
DIAGNOSIS OF ARVD (1)Clinical features suggestive of
renovascular disease
Hypertension
Abrupt onset of hypertension in patients aged 50 years
(suggestive of ARVD)
Absent family history of hypertension
Accelerated or malignant hypertension
Resistance to therapy (3 drugs)
Hypertension may be absent, particularly in patients with
chronic
cardiac disfunction.
Renal abno rmali t ies Unexplained renal failure in patients
aged >50 years
Elevation in plasma creatinine level after the initiation of
ACE-I or AII-RB
therapy (> 30% increase in serum creatinine)
Asymmetrical kidneys on imaging
-
8/21/2019 Renal Vascular Diseases
16/56
16
DIAGNOSIS OF ARVD (2)
Other
Unexplained acute pulmonary oedema or
congestive cardiac failure
Femoral, renal, aortic or carotid bruits
Severe retinopathy
History of extra-renal vascular disease
Hypokalaemia
Neurofibromatosis
-
8/21/2019 Renal Vascular Diseases
17/56
17
DIAGNOSIS OF ARVD (3)
DRASTIC
The most powerful predictors for detecting lesions ofat least
50%:
age,
symptomatic vascular disease,
elevated cholesterol the presence of an abdominal bruit.
-
8/21/2019 Renal Vascular Diseases
18/56
18
DIAGNOSIS OF ARVD (4)
Investigation of ARVDDuplex ultrasonography
widely available, noninvasive, and
inexpensive.
First line screening test
sensitivity of 85% and specificity of 92%.
peak systolic velocity, has the highest
performance characteristics;
-
8/21/2019 Renal Vascular Diseases
19/56
19
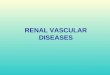
DIAGNOSIS OF ARVD (6)Magnetic resonance imaging the favoured
imaging method for the proximal renal vasculature
The sensitivity ranges from 83% to 100% and specificity from 92%
to97%.
Gadolinium is non-nephrotoxic at low doses;
MR renal angiogram showing tight stenosis of the right renal
artery and occlusion of the leftrenal artery
-
8/21/2019 Renal Vascular Diseases
20/56
20
DIAGNOSIS OF ARVD (7)
Computed tomography angiography
Sensitivity and specificity of 95%
Best for aortorenal calcification (utility in
stentplacement);
Visualise main and accesory renal arteries.
Limitations
risk of contrast nephropathy poor visualization of the distal
main renal
artery and segmental branches.
-
8/21/2019 Renal Vascular Diseases
21/56
21
DIAGNOSIS OF ARVD (8)
Renal scintigraphy and measurement of individualkidney
function
the captopril test unravel the degree of renin activation
Asymmetric result of a functional test RAS Sensitivity and
specificity variable: 43% - 93%
Insufficient sensitivity in:
Renal failure;
Renin independent hypertension
-
8/21/2019 Renal Vascular Diseases
22/56
22
DIAGNOSIS OF ARVD (9)
Renal Arteriography
the gold standard diagnostic test. risks of contrast nephropathy
andatheroembolic renal disease
-
8/21/2019 Renal Vascular Diseases
23/56
23
TREATMENT OPTIONS IN ARVD (1)
Few topics provoke more controversy between
nephrologists and interventional cardiologiststhan management of
atherosclerotic renovascular
disease
-
8/21/2019 Renal Vascular Diseases
24/56
24
TREATMENT OPTIONS IN ARVD (2)
Medical treatment
Limiting the progression of atheromatous diseaseand chronic
kidney disease
vigorous control of hypertension and hyperlipidemia,
diabetes control
use of antiplatelet agents,
cessation of smoking
lifestyle modification (including reduced dietary intakeof salt
and increased exercise).
attention to the complications of renal insufficiency
-
8/21/2019 Renal Vascular Diseases
25/56
25
TREATMENT OPTIONS IN ARVD (3)
CORAL study (Cardiovascular Outcomes in Renal
AtheroscleroticLesions)
-
8/21/2019 Renal Vascular Diseases
26/56
26
TREATMENT OPTIONS IN ARVD (4)
Antihypertensive therapy
Is there an ideal blood pressure targetthat confersmaximal
cardiovascular protection?
In CORAL, the target blood pressure is 140/ 90 mmHg ; 130/80 mm
Hg is recommended for patientswith hypertension and diabetes or
renal disease.
Is there a specificantihypertensive regimenthatprovides
cardiovascular benefits beyond just loweringblood pressure?
-
8/21/2019 Renal Vascular Diseases
27/56
27
TREATMENT OPTIONS IN ARVD (5)
First-line agent
Angiotensin receptor antagonist First-line agent if ARB not
tolerated - ACE inhibitor
especially for those with proteinuric chronic parenchymal
disease,
and those with coexisting coronary artery disease and
cardiac dysfunction.Second-line agent Thiazide diuretic
Combinations with ARB/ACE may be available
Use loop diuretics for patients with serum creatinine 2
mg/dL
Third-line agents (function of comorbidities) Calcium channel
blocker
Beta Blocker
Alfa Blocker
Vasodilator
-
8/21/2019 Renal Vascular Diseases
28/56
28
TREATMENT OPTIONS IN ARVD (6)
Dyslipidemia Treatment in terms of cardiovascular risk RAS is
considered a
coronary artery disease equivalent. Third Report of theExpert
Panel on Detection, Evaluation, and Treatment of High
BloodCholesterol in Adults (Adult Treatment Panel III)
Goal of therapy
low-density lipoprotein cholesterol
-
8/21/2019 Renal Vascular Diseases
29/56
29
TREATMENT OPTIONS IN ARVD (7)
Diabetes Mellitus
HbA1c of
-
8/21/2019 Renal Vascular Diseases
30/56
30
TREATMENT OPTIONS IN ARVD (8)
Effect of the Medical Therapy Intervention
reduce cardiovascular risk
progression to end-stage renal disease actuallydoes not respond
very well to medical therapy
-
8/21/2019 Renal Vascular Diseases
31/56
31
TREATMENT OPTIONS IN ARVD (9)
Surgical treatment
revascularization nephrectomy of small kidneys with relatively
complete
arterial occlusion.
-
8/21/2019 Renal Vascular Diseases
32/56
32
TREATMENT OPTIONS IN ARVD (9)
Evidence for renal revascularization
Randomized Trials in Renal Artery Stenosis Intervention
Year n Medical Balloon Stent End Points
Weibull 1993 58 X X BP/renal function
Plouin 1998 49 X X BP
Webster 1998 55 X X BP/renal function
van de Ven 1999 84 X X Patency/BP/renal function
van Jaarsveld 2000 106 X X BP/renal function
Benefits: A modest improvement in blood pressure control
no improvement in renal function.
-
8/21/2019 Renal Vascular Diseases
33/56
33
TREATMENT OPTIONS IN ARVD (10)
Definite indications for renal revascularization
Recurrent flash pulmonary oedema
Severe hypertension resistant to all medical therapy.
When a patient who requires ACE-I or AII-RB
therapy (e.g. for cardiac failure) presents with
significant ACE-I-related uraemia.
RAO in a reasonably sized kidney
-
8/21/2019 Renal Vascular Diseases
34/56
34
TREATMENT OPTIONS IN ARVD (11)
CONTROVERSIES
Effect of Revascularization on Blood Pressure
Revascularization may fail to cure hypertension
In long-standing hypertension, secondary processesthat sustain
hypertension
Vascular remodeling,
atherosclerosis, ischemic damage to the poststenotic kidney,
hypertensive injury to the nonstenotic kidney
-
8/21/2019 Renal Vascular Diseases
35/56
35
PROGNOSIS OF PATIENTS WITH
ARVD (1)
Major mortality from cardiovascular
complications; risk of death is almost sixtimes that of
developing ESRD
-
8/21/2019 Renal Vascular Diseases
36/56
36
NEPHROSCLEROSIS
-
8/21/2019 Renal Vascular Diseases
37/56
37
Definition
clinical syndrome characterized by long-
term essential hypertension, hypertensive
retinopathy, left ventricular hypertrophy,
minimal proteinuria, and progressive renalinsufficiency
-
8/21/2019 Renal Vascular Diseases
38/56
38
Pathophysiology
glomerular ischemia:chronic hypertension
result in narrowing of preglomerular
arteries and arterioles, with a consequent
reduction in glomerular blood flow
Glomerulosclerosis induce by glomerular
hypertension and glomerular hyperfiltration
-
8/21/2019 Renal Vascular Diseases
39/56
39
Genetics
a significant loss in kidney function was
observed in black people despite similar
levels of BP control
polymorphism in the angiotensin-
converting enzyme (ACE) gene, the DD
genotype
increased angiotensinogen mutations
-
8/21/2019 Renal Vascular Diseases
40/56
40
Frequency
USA: 1985-2005, adjusted rates of ESRD
caused by hypertension increased 140%
Hypertensive nephrosclerosis accounts formore than one third of
patients on
hemodialysis.
Europe: 12% of new patients starting renalreplacement
therapy
-
8/21/2019 Renal Vascular Diseases
41/56
41
Race
In black people, hypertensive
nephrosclerosis occurs earlier, is moresevere, and more often
causes ESRD
(36.8% in black patients vs 26% in white
patients).
-
8/21/2019 Renal Vascular Diseases
42/56
42
Age
The diagnosis of hypertensive
nephrosclerosis increases with advancing
age. The peak age for the development of
ESRD in white patients is 65 years and
older, while the peak age is 45-65 years inblack people
-
8/21/2019 Renal Vascular Diseases
43/56
43
DIAGNOSIS
Long-standing or very severe hypertension Black race
Hypertension preceding renal dysfunction
Hypertension diagnosed prior to the onset ofproteinuria
No evidence of another renal disease
Biopsy findings compatible with the diagnosis
Proteinuria less than 0.5 g/d
Hypertensive retinal changes
Left ventricular hypertrophy
-
8/21/2019 Renal Vascular Diseases
44/56
44
Lab Studies
(I)
Baseline complete blood cell count
Creatinine level
Electrolyte status Urinalysis
Either a spot urine test for albumin or
creatinine ratio or a 24-hour urinecollection - To determine
total protein
excretion
S
-
8/21/2019 Renal Vascular Diseases
45/56
45
Lab Studies
(II)
urine protein excretion of lower than 1 g/d;
in some patients a 24-hour urinary proteinexcretion greater than
1 g/d has been
described. When secondary changes of focal
segmental glomerulosclerosis (FSGS)
related to hyperfiltration develop,proteinuria can increase to
the nephroticrange.
-
8/21/2019 Renal Vascular Diseases
46/56
46
Imaging Studies
echocardiogram to assess left ventricular size.
Renal imaging with either an ultrasound or anintravenous
pyelogram reveals that kidney size is usuallysymmetric and may be
normal or modestly reduced.
The renal calices and pelves are normal. Renal asymmetry or
irregularities in the contour raise the
possibility that hypertension could be secondary to renalartery
stenosis or reflux nephropathy
ECG typically shows left ventricular hypertrophy; thesensitivity
of ECG in helping to detect left ventricularhypertrophy may be as
low as 22%.
-
8/21/2019 Renal Vascular Diseases
47/56
47
Histologic Findings(I)
medial and intimal thickening with intimal
fibrosis of preglomerular arterioles
hyalinosis of afferent arterioles
secondary tubular atrophy
interstitial fibrosis
malignant hypertension Fibrinoid necrosis
microinfarcts
-
8/21/2019 Renal Vascular Diseases
48/56
48
Histologic Findings (II)
GLOMERULAR CHANGES
Obsolescent glomeruli were defined as glomeruli in
which Bowman's space was occupied by collagenous,PAS positive
material, and the tuft was retracted
Solidified glomeruli were defined as glomeruli in
which the entire tuft was solidified, in the absence of
the collagenous change in the capsular space
Disappearing glomeruli were identified as globally
sclerotic glomeruli where there was an absence or
partial disappearance of Bowman's capsule
-
8/21/2019 Renal Vascular Diseases
49/56
49
TREATMENT (I)
-
8/21/2019 Renal Vascular Diseases
50/56
50
TREATMENT (I) BP goal of less than 130/80 mm Hg to preserve
renal function and to reduce
cardiovascular events in patients with hypertension and
diabetes.
Lower BPs are recommended for patients with proteinuria greater
than 1 g/d
and renal insufficiency, regardless of etiology
ACE inhibitors
Effects and indications
Reduce proteinuria
Specific renal protective effect both in diabetic and
nondiabetic renal impairment
Reduce morbidity and mortality rates in congestive heart failure
Monotherapy less effective in older patients (>50 y)
Larger doses required in black patients
Inhibit or blunt all adverse metabolic effects of thiazides
Dose reduction required in renal failure
Reduce left ventricular hypertrophy and thirst
Adverse effects Cough (approximately 10%)
Angioedema (rare)
Hyperkalemia (especially in renal tubular acidosis type IV)
GFR reduction in patients with impaired renal function
May precipitate acute renal failure in patients with renal
artery stenosis
Interfere with breakdown of bradykinin
Contraindicated in pregnancy
-
8/21/2019 Renal Vascular Diseases
51/56
51
TREATMENT (II) Angiotensin II receptor antagonists
Effects and indications Reduce proteinuria
Indicated in patients intolerant of ACE inhibitors
Can be used in combination with an ACE inhibitor
Do not cause cough
Reduce left ventricular hypertrophy and thirst similarly to
ACEinhibitors
Do not interfere with breakdown of bradykinin
Adverse effects
Hyperkalemia
May reduce GFR in patients with impaired renal function May
precipitate acute renal failure in patient with renal artery
stenosis
Angioedema (rare)
Contraindicated in pregnancy
Data in black patients limited
-
8/21/2019 Renal Vascular Diseases
52/56
52
TREATMENT (III)
Calcium channel blockers Effects and indications
Effective as monotherapy in black patients and elderly
patients
Potentiate ACE inhibitor effects
Renal protection not proven
Reduce morbidity and mortality rates in congestive heart failure
Indicated in patients with diastolic dysfunction
No change in dose with renal failure
Adverse effects
Possible increase in cardiovascular mortality rate with
short-actingdihydropyridines
Edema
Constipation (verapamil)
Profound bradycardia possible when verapamil and diltiazem
usedin combination with a beta-blocker
-
8/21/2019 Renal Vascular Diseases
53/56
53
Malignant hypertension(1)
1% of patients with hypertension;
It may occur in patients with preexisting hypertension orin a
previously normotensive patient
Systolic BP can range from 150-290 mm Hg while
diastolic BP can vary from 100-180 mm Hg. Keith-Wagener grade
III (hemorrhages and exudates)
and grade IV retinal changes (papilledema) are thehallmarks of
malignant hypertension.
Acute heart failure: pulmonary edema can be thepresenting signs
in approximately 10% of patients.
Left ventricular hypertrophy is present in as many as75% of
patients at presentation
-
8/21/2019 Renal Vascular Diseases
54/56
54
Malignant hypertension (2)
60% of patients complain of headaches
5-10% cerebrovascular event (eg, focalcerebral ischemia,
cerebral/subarachnoid
hemorrhage) hypertensive encephalopathy is
characterized by headache, nausea,vomiting, and visual blurring,
together withimpaired cognitive function, generalizedseizures, or
cortical blindness.
-
8/21/2019 Renal Vascular Diseases
55/56
55
Malignant hypertension (3)
microangiopathic hemolytic anemia
(schistocytes,thrombocytopenia, increased fibrin degradation
products,and increased fibrinogen) is frequently present
Renal involvement is common, but the degree of
severity varies Proteinuria is common, but overt nephrotic
syndrome is
unusual
30% of patients will have an elevated serum creatininelevel at
presentation
Other symptoms include weakness, malaise, fatigue,and weight
loss
TREATMENT OF MALIGNANT
-
8/21/2019 Renal Vascular Diseases
56/56
56
TREATMENT OF MALIGNANT
HYPERTENSION
Malignant hypertension complicated by organ
failure is a medical emergency and requires
rapid reduction in BP
In uncomplicated malignant hypertension, rapid
BP reduction is not as critical as in the previous
group with BP reduction by up to 20% of the
presenting values, or a systolic BP of greaterthan 170 mm Hg in
the first 24 hours has been
an acceptable target.