Embed Size (px)
Citation preview

Patient pathways and clinical governance: Patient flow knowledge
generation and clinical practice
Jean-Yves Blay
(coordinator ERN EURACAN)

Eur J Cancer 2011;47:2493
1 in 5 cancers is rare…

Rare cancers have worse prognosis
0
20
40
60
80
100
120
0 1 2 3 4 5 6
rare
common
years

• promote good quality and safe care to patients by fostering proper diagnosis, treatment,follow-up and management of patients across the Network
• empower and involve patients
• offer and promote multi-disciplinary advice for complex cases
• develop and implement clinical guidelines and cross-border patient pathways
• exchange, gather and disseminate knowledge, evidence and expertise within andoutside the Network
• promote collaborative research within the Network
• reinforce research and epidemiological surveillance, through setting up of sharedregistries
• exchange and disseminate knowledge and best practices, in particular by supportingnational centres and networks

EURACAN governance EURACAN General Assembly
Board of all HCP members andassociate/affiliate partners
Domains(Clinical action)
Guidelines
Research
Training/Education
Funding/sustainability plan
Communication/ Interaction with PAGs
G1
Sar
com
a
G2
Rar
e G
YN
G3
Rar
e G
U
G4
NET
G5
Rar
e G
I
G6
En
do
crin
e
G7
Rar
e H
&N
G8
Rar
e T
ho
raci
c
G9
Rar
e S
kin
G1
0 R
are
Bra
in
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
Transversal Task Forces
Steering CommitteeCoordinator
10 Group leaders+ 1 representative/country not already
represented7 task force leaders
Patient Advocacy groups
Scientific Advisory Board6 independent experts
Rare/frequent cancer/diseases Outside / inside EU
Decisions for key questions
Decisions for daily management
Dissemination
Quality control

Diagnosis

0 0.2 0.4 0.6 0.8 1 1.2 1.4
GISTLiposarcomasSarcoma NOS
Leiomyos non ut.Kaposi
DermatofibroSUterine LMS
MFH
MyxofibrosarcomasRhabdomyosarcomas
Synovialosarcomas
Ewing sarcomasAngiosarcomas
LG Fibromyxoid Sarcomas
MPNST
FibrosarcomasSolitary fibrous tumors
OsteoS
Incidence / 100,000 / yr
Others
Over 80 histotypes of sarcomas…

GIST
Sarcomas and
aggressive connective
tissue tumors
Mutations
kinases
G5
Ntl
Group
Translocations
DFSP
SyS
Ewing
Mutations
APC/bCat
Desmoids
WD/DDLPSAmplification
12q13-15
MDM2/CDK4
MPNST
PEComas
TSG loss
NF1, TSC1/2
Genomique
complexe
LMS, UPS

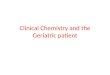
For 35 % the diagnosis is not totally correct
Rate of concordance by patient sub-group
188
Second opinion requested
53 (28%)
Total
discordance
53 (28%)
Partial
concordance
82 (44%)
Total
concordance
178
Second opinion not requested
17 (10%)
Total
discordance
44 (25%)
Partial
concordance
117 (65%) Total
concordance
For 56 % the diagnosis is not totally correct
Accuracy of histological diagnosis
Ducimetière F, et al. PLoS One. 2011;6(8):e20294.
Cassier PA, etal. Br J Cancer. 2010 Jul 13;103(2):165-70.
Lurkin A, et al. BMC Cancer. 2010 Apr 19;10:150.

Histological discordances

Guidelines

• Biopsy first
– Assessment by an experienced team
• Adequate preop imaging
• En bloc surgical resection
– Planning R0
– If R1, consider re resection
• Post operative radiotherapy
– (G2-3 and/or deep seated, and/or >5cm)
• Preoperative radiotherapy


Research

Research in rare cancers
• Increasing burden of clinical research
• Refined biological understanding
• Rare tumors are good models for PoC
• Numbers: new designs needed
• Health technology assessment : which rules?
• Association of reference networks with research consortium


Clinical research in rare cancers?
Histological
classification
IHC/
single gene
Gene
panelWES WGS

Patient flow knowledge generation and clinical
practice

3 networks of reference for sarcomas
Label by INCa
Review
diagnosis
Mandatory
Review of
discordant
cases
Evaluation :
-activity,
-discrepancies
-delays,
-technics used,
-Frozen/FFPE
Database shared via Internet
Structuration
of MDTB
sarcoma in
France
Organisation of
third level
MDTB
Activity of MDTB :
-new patients / Fup Patients
-Description traitements
local phase
advanced phase
-inclusions trials,
Réseau de Référence en
Pathology des Sarcomes
Tissus mous / viscères
RRePS
Pr Jean-Michel COINDRE
BERGONIE
NetSarc
Pr Jean-Yves BLAY
CENTRE LEON BERARD
Réseau de Référence Clinical
des Sarcomes
Tissus mous / viscères
ResOsPr François GOUIN
CHU Nantes
Pr Gonzague DE PINIEUX
CHU Tours
Réseau de référence
Pathology/clinical
Sarcomes osseux

Jean-Yves Blay, Axel Le Cesne, Nicolas Penel, Emmanuelle Bompas, Florence Duffaud, Christine Chevreau, Maria Rios, Pierre Kerbrat, Didier Cupissol, Philippe Anract, Jean-Emmanuel Kurtz, Celeste Lebbe, Nicolas Isambert, Francois Bertucci, Antoine Thyss, Sophie Piperno-Neumann,
Pascale Dubray-Longeras, Francoise Ducimetiere, Jean-Michel Coindre, Antoine Italiano;
Universite Claude Bernard & Centre Léon Bérard, Lyon, France; Gustave Roussy Cancer Campus, Villejuif, France; Centre Oscar Lambret, Lille, France; Department of Medical Oncology, Centre René Gauducheau, Nantes St. Herblain, France; La Timone University Hospital, Marseilles, France; Institut Claudius Regaud, Toulouse, France; Centre Alexis Vautrin, Vandoeuvre-lès-Nancy, France; Medical Oncology Eugene Marquis Comprehensive Cancer Center, Rennes, France; Centre Val d'Aurelle, Montpellier, France; Hopital Cochin Saint Vincent de Paul, Paris, France;
Hôpitaux Universitaires de Strasbourg, Strasbourg, France; Dermatology Department, Saint Louis Hospital, Paris, France; Centre Georges François Leclerc, Dijon, France; Institut Paoli Calmettes, Marseille, France; Centre Antoine-Lacassagne, Nice, France; Institut Curie, Paris,
France; Centre Jean Perrin/ERTICa EA 4677, Clermont-Ferrand, France; Centre Léon Bérard, Lyon, France; Institut Bergonié, Department of Pathology, Bordeaux, France; Institut Bergonié, Department of Medical Oncology, Bordeaux, France
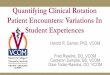
The nationwide cohort of 26883 patients with sarcomas & connective tissue tumors treated in NETSARC reference
network between 2010 and 2015 in France: major impact of multidisciplinary board presentation prior to first
treatment

Bone
Soft tissue
Visceral
Patients in MDT of NetSARC

Results (3)Better management when MDT before
treatment
• A higher number of pts presented in Netsarc MDTB had
– Adequate imaging of the tumor before treatment/ surgery (87,9% vs 67,8%, p<0.0001)
– Biopsy prior the first resection (87,% vs 55,0%, p<0.0001).

24%
33%
26%24%
38%
23%24%
37%
23%
30%33%
22%
28%
34%
25%
51%
31%
8%
54%
30%
6%
55%
29%
7%
55%
31%
7%
58%
29%
6%
R0 R1 R2
2011 N=724 2012 N=824 2013 N=791 2014 N=888 2015 N=668
2011 N=712 2012 N=806 2013 N=941 2014 N=923 2015 N=670
Outside Outside OutsideNetSarc NetSarc NetSarc
R0 R1 R2
1%
16%
1%
14%
2%
14%
1%
14%
1%
11%
1%
8%
1%
9%
1%
9%
1%
6%
1%
6%
Non évaluable Inconnu
Quality of initial surgery, incident patients (STS & visceral sarcomas operated)
Non evaluable Unknown
ASCO16

Local relapse free and relapse free survival

Needed
• Improved education of practitionners and health care workers
• Easily accessible informations
• Communication tools
• Continuous medical education
• Real life analysis of the outcome of patients
• Databases
• Simple and efficient access to MDT
• Referral system intra /extra country

EURACANWhat are the objectives
• Improving the quality of care of patients with Rare cancers in EU
• Guidelines
• Communication
• Patient pathways
• Expertise for all
• Cross border
• Research

EURACAN governance EURACAN General Assembly
Board of all HCP members andassociate/affiliate partners
Domains(Clinical action)
Guidelines
Research
Training/Education
Funding/sustainability plan
Communication/ Interaction with PAGs
G1
Sar
com
a
G2
Rar
e G
YN
G3
Rar
e G
U
G4
NET
G5
Rar
e G
I
G6
En
do
crin
e
G7
Rar
e H
&N
G8
Rar
e T
ho
raci
c
G9
Rar
e S
kin
G1
0 R
are
Bra
in
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
LeaderSecret.
Transversal Task Forces
Steering CommitteeCoordinator
10 Group leaders+ 1 representative/country not already
represented7 task force leaders
Patient Advocacy groups
Scientific Advisory Board6 independent experts
Rare/frequent cancer/diseases Outside / inside EU
Decisions for key questions
Decisions for daily management
Dissemination
Quality control

EURACAN – Domain leaders
• G1 : Sarcoma : Paolo Casali <[email protected]>
• G2: Rare GYN: Michael Seckl ([email protected])
• G3: Rare GU: Pr J.A. Gietema, ([email protected])
• G4: NET : Martyn Caplin, ([email protected])
• G5: GI: Lucjan Wyrwicz; ([email protected])
• G6: Endocrine: Eric Baudin ([email protected])
• G7: Rare Head and Neck: Lisa Licitra <[email protected]>
• G8: Rare Thoracic : Nicolas Girard <[email protected]>
• G9: Rare Skin/Eye melanoma: Dirk Schadendorf [email protected]
• G10 : Brain tumors: Martin J van den Bent [email protected]

EURACAN domains and subdomains
EURACAN
G1 Sarcoma
G2Rare female
genital organ / placenta
G3Rare
male genital organ / urinary
tract
G4Rare neuroendocrine
system
G5Rare
Digestive tractG6
Rare Endocrine organs
G7Rare
Head and neck
G8Rare
thorax
G9Rare skin / eye
melanoma
G10Rare brain /
spinal cords / meninges /
cranial nerves
G1 Soft tissue /
visceralsarcoma
G1 Bone
SarcomaG2
Trophoblastic disease
G2Rare ovarian
G3Testis
G5Peritoneal
G5Biliary tract
G5Anal
G9Skin
G9Eye melanoma
Domains Sub domains

Distribution of centres by country
Endorsement process –member state
Minimal set of criteria:- Expertise- N of patients
N=5
N=4..N=3..
.N=10
N=1N=6 N=1
N=12.
N=6
N=8
N=2
N=2N=2
NO, SW, FI, DK , (n=8)
N=1
N=1
N=1

…….

Conclusions
• Patient pathways must be carefully monitored
• Patients empowerment
• Communication, education
• Webbased tools
• Clinical governance
• Monitoring patient outcome in exhaustive real life populations enables measuring the impact of our action and open now questions
• The missions of the ERNs

Patient pathways and clinical governance: Patient flow knowledge
generation and clinical practice
Jean-Yves Blay
(coordinator ERN EURACAN)