Embed Size (px)
DESCRIPTION
Patient Safety Walk-Rounds
Citation preview

We are all responsible…and together we are creating a safer healthcare system
An initiative of the Quality and Patient Safety Directorate, Health Service Executive, May 2013 ©
Toolkit
Quality and SafetyWalk-rounds
THERAPY PROFESSIONS COMMITTEE

2
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
© Health Service ExecutiveQuality and Patient Safety DirectorateMay 2013ISBN 978-1-906218-60-7Quality and Patient Safety DirectorateHealth Service ExecutiveDr Steevens’ HospitalDublin 8Ireland
Telephone: +353 1 6352344Email : [email protected] Web : http://www.hse.ie
Adapted from: Institute for Healthcare Improvement (2004), Patient Safety First UK (2009), Great Ormond Street Hospital for Children, NHS Trust (2011) and The Scottish Patient Safety Programme (2011).
This forms part of a series of supports developed by the HSE Quality and Patient Safety Directorate:■ Quality and Patient Safety Clinical Governance Information Lea� et (2012);
■ The Safety Pause (2013): Information Sheet;
■ Quality and Safety Committee(s): Guidance and Sample Terms of Reference;
■ Quality and Patient Safety Clinical Governance Development Assurance Check
for Health Service Providers (2012);
■ Quality and Safety Prompts for Multidisciplinary Teams (2012);
■ Achieving Excellence in Clinical Governance: Towards a Culture of Accountability (2010); and
■ Integrated Framework for Quality Safety and Risk Management (2009).
Copies of the documents can be located at www.hse.ie/go/clinicalgovernance
All of the above will assist organisations in demonstrating their commitment to sta� engagement, building
relationships, trust and patient service quality and safety. Along with working to meet the National Standards for
Safer Better Healthcare (2012), the Quality Framework for Mental Health Services in Ireland (2007) and preparing for the
new governance arrangements within the health system.

1
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Foreword
The Quality and Patient Safety Directorate in the HSE is constantly seeking ways to support health service
providers to improve the way they work and thus deliver a safer high quality experience to patients and people
who access our services. To that end we are seeking to promote leadership for high quality compassionate
care. Ultimately we are seeking to nurture a culture where problems in care are openly discussed and solutions
identi� ed, where hierarchies are � attened and all sta� feel that they can speak up and contribute to improving
the services we provide.
In a systematic review leadership walk-rounds and multi-faceted unit-based strategies are the two strategies
with some stronger evidence to support a positive impact on patient safety culture in hospitals1. The purpose
of this Quality and Safety Walk-round Toolkit is to provide a structured process to bring senior managers and
front line sta� together to have conversations about quality and safety with the intention to prevent, detect and
mitigate patient/sta� harm.
The guidance document is one of a series with the tag line ‘we are all responsible … and together we are creating
a safer healthcare system’. While the health system is under signi� cant pressure we would intend this to not be
an additional burden but a practical toolkit. The walk-round can be focused on any location or service that may
a� ect patient care and safety of the organisation.
I would like to thank the quality and safety clinical governance development steering group, working group,
international reference panel, colleges and associations for preparing and endorsing our approach.
I would like to strongly recommend that our senior leaders and managers would embrace the style of leadership
embedded in the concept of quality and safety walk-round many already do. This will form a key element in our
model for service delivery where we really listen to front line sta� and ensure that quality and safety is at the top
of all our agendas.
I would welcome feedback and learning from the system from the practical application of this approach and we
will develop the document further based on your experience.
Dr. Philip Crowley
National DirectorQuality and Patient Safety Directorate
1 Morello, R., Lowthian, J., Barker, A., McGinnes, R., Dunt, D., and Brand, C. (2012), ‘Strategies for improving patient safety culture in hospitals: a systematic review.’ British Medical Journal Quality and Safety, on line published on 21st July 2012 as 10.1136/bmjqs-2011-000582.

2
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

3
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Table of Contents
Foreword 1
1. Introduction 4
2. Approach to: Quality and Safety Walk-rounds 5
2.1 Aims 6
2.2 Setting the Scene 6
2.3 Who 6
2.4 When 7
2.5 Where 7
2.6 How 7
2.7 Tracking Mechanism 8
3. Communication 9
3.1 At the start 9
3.2 Before the Walk-round 9
3.3 Follow up after the Walk-round 9
3.4 On-going 9
4. Sample Guide for Discussion with Patients 10
5. Sample Guide for Discussion with Staff 11
6. Impact of Quality and Safety Walk-rounds 13
7. Summary 13
Toolkit: Quality and Safety Walk-rounds 14
Appendix 1: Sample Quality and Safety Walk-rounds Contact Information 15
Appendix 2: Sample Executive/Senior Management Team: Quality and Safety the Walk-round Members 16
Appendix 3: Sample Communication Prior to the Walk-round 17
Appendix 4: Sample Quality and Safety Walk-round Notice 18
Appendix 5: Sample Walk-round Leafl et 19
Appendix 6: Sample Preparation for the Senior Managers Leading the Quality and Safety Walk-round Team 20
Appendix 7: Sample Communication after the Quality and Safety Walk-round 21
Appendix 8: Sample Final Communication after the Quality and Safety Walk-round 22
Appendix 9: Sample Quality and Safety Walk-round Action Plan Template 23
Appendix 10: Sample Quality and Safety Walk-round Schedule 25

4
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
1 Morello, R., Lowthian, J., Barker, A., McGinnes, R., Dunt, D., and Brand, C. (2012), ‘Strategies for improving patient safety culture in hospitals: a systematic review.’ British Medical Journal Quality and Safety, on line published on 21st July 2012 as 10.1136/bmjqs-2011-000582.
2 Frankel, A., Graydon-Baker, E., Neppl, C., Simmonds, T., Gustafson, M., Gandhi, TK., (2003), ‘Patient Safety Ledrship Walk-rounds ’. Joint Commission Journal on Quality and Safety 29(1): 16-26.
3 Institute for Healthcare Improvement (2004), Patient Safety Leadership Walk-rounds . Boston: Institute for Healthcare Improvement 4 Healthcare Improvement Scotland (2011), Leadership Walk-rounds Fact Sheet. Edinburgh: Scottish Patient Safety Programme5 Patient Safety First (2009), Leadership for Safety Patient Safety Walk-rounds . London: Patient Safety First 6 Feitelberg, S. (2006), 'Patient Safety Executive Walkarounds.' The Permante Journal 10(2), 29-367 O'Connor, P. (2011), 'Looking for Harm in Healthcare: Can Patient Safety Leadership Walk Rounds Help to detect and prevent harm in NHS hospitals? A Case Study of NHS Tayside', PhD Thesis: University of St. Andrews, Scotland.
1. Introduction This document provides a short guide and toolkit aimed at helping organisations start out on this
important initiative. Safety walk-rounds have helped many organisations make a signi� cant impact on
their safety culture.1 Quality and safety walk-rounds allow executive/senior management team members
to have a structured conversation around safety with frontline sta� and patients. The walk-round can
be focused on any location or service that may a� ect patient care and safety of the organisation.
Central to the success of walk-rounds is a collaborative open approach. Visits are intended to be helpful
opportunities to share ideas and provide immediate feedback without taking responsibility away from
line managers.
Strong e� ective leadership is essential to build a safety-orientated organisational culture, as evidence suggests, that
without this, many other interventions are likely to fail. Senior managers have a lead role in:
Creating a culture where quality and safety is everybody’s primary goal
Patient safety walk-rounds are a way of ensuring that senior managers can build relationships and trust so they are
informed and can exchange views, regarding the safety concerns of units/teams. They provide an opportunity for
frontline sta� to identify and discuss their safety concerns. They are also a way of demonstrating visible commitment
by listening to and supporting sta� when issues of safety are raised. Walk-rounds can be instrumental in developing
an open culture where the safety of patients is seen as the priority of the organisation.
As a more formalised framework, patient safety walk-rounds were initially introduced by Allan Frankel, MD2,
have since been developed by the Institute for Healthcare Improvement,3 Governments4 5 and hospitals6 as a
tool to engage senior managers and frontline staff in a meaningful discussion of patient safety concerns with
agreed actions7.
Quality and safety walk-round
Structured process to bring senior managers and front line sta� together to have quality and safety
conversations with a purpose to prevent, detect and mitigate patient/sta� harm.
Quality and safety walk-rounds can be conducted in any setting such as wards, departments, operating theatres,
clinics, general practice and community settings, but are not limited to these. They are also useful in services such
as pathology and portering or other areas that may a� ect patient care or the safety of the organisation such as
information communication technology (ICT) and � nance. They provide a formal process for members of the
executive/senior management team/members of the board to talk with sta� about safety issues in their unit or
team and show their support of sta� for reporting errors/near misses.

5
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
2. Approach to: Quality and Safety Walk-rounds Being clear on the why, who, when, where and how is central to the success of quality and safety walk-rounds.
Consideration of the context and culture will inform the decision on the best approach and level of organisation.
Algorithm: Quality and Safety Walk-rounds
AIMSDemonstrate senior manager’s commitment to quality and safety for patients, sta� and the public
Increase sta� engagement and a culture of open communicationIdentify, acknowledge and share good practice
Support a proactive approach to minimising risk, timely reporting and feedbackStrengthen commitment and accountability for quality and safety
WHOLed by CEO/General Manager/Service Manager
To ensure continuity a named person for all Quality and Safety Walk-rounds is identi�ed by the CEO/GM/Service ManagerRepresentatives nominated by the Senior Management Team and the Unit/Team participate in the walk-round
WHENThe Walk-rounds occur at an agreed frequency
Dates and times are arranged, in consultation with area, and communicated by the named person coordinating the Quality and SafetyWalk-round, who will schedule all dates and areas to be visited for the year
COMMUNICATIONA clear communication plan for the Quality and Safety Walk-round initiative
All sta� are briefed about the initiative and the aimsGeneral sta� brie�ngs, newsletters and intranet communication should be used to promote the initiative
Providing feedback and follow up with the unit/team within agreed time frames
WHEREWalk-rounds start with a tour of the unit and meeting with patients and sta�
A meeting venue close to the patient /service area (o�ce, seminar room) is used for the discussion
HOWThe team in the area being visited are asked to think of a recent example of a patient safety incident they have experienced and share this at the meeting so
that discussion can take place on - what is working well, how this was managed by the team and how the senior management team can help
SETTING THE SCENEAgreed and con�rmed at the start of the walk-round
The walk-round is an opportunity for an open discussion on quality and safety and is not an assessment or inspectionAll information discussed in a walk-round is con�dential
SENIOR MANAGEMENT WALK-ROUND TEAM– Senior management team lead. For example, one of the following will be designated lead: ■ CEO/GM /Service Manager ■ Lead/Executive/Clinical Director/Director of Quality and Safety ■ Health and Social Care Professional Lead ■ Director of Nursing/Midwifery ■ Head of Finance or Human Resources or ICT– Accompanied by (where possible): ■ Patient representative/advocate or patient liaison o�cer ■ A member of the board ■ A note taker
WARD/DEPARTMENT/UNIT TEAM– Ward/Department/Unit manager (identi�ed lead)– Medical Leads– On the day there may be a number of other sta� present For example: ■ Junior doctors ■ Consultants ■ Health and Social Care Professionals ■ Clerical Sta� ■ Catering Sta� ■ Nurses/Midwives ■ Health Care Assistants and other Support Sta�

6
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
2.1 AimsThe aims in introducing Quality and Safety Walk-rounds are:■ Demonstrate senior managers’ commitment to quality and safety for patients, sta� and the public;
■ Increase sta� engagement and develop a culture of open communication;
■ Identify, acknowledge and share good practice;
■ Support a proactive approach to minimising risk, timely reporting and feedback; and
■ Strengthen commitment and accountability for quality and safety.
2.2 Setting the SceneIt is helpful to clarify ground rules in advance and re con� rm this at the start of the walk-round. Some suggestions
for successful walk-rounds are:■ Understanding that the walk-round is an opportunity for an open discussion on quality and safety. It is not an
assessment or inspection and can provide the opportunity for sta� to express concerns on behalf of patients;
■ Actively listening and a proactive approach to identifying and minimising risk;
■ Con� dentiality of information discussed in a walk-round and patient safety disclosure requirements;
■ Agreeing times and location of walk-rounds an agreed period in advance;
■ Sharing key learning from walk-rounds with other units/teams; and
■ Prompt feedback from the senior management team with follow up.
2.3 Who To ensure continuity, it is advised that a named person be identi� ed by the CEO/General Manager/Service Manager
to coordinate all Quality and Safety walk-rounds. It is important for the individual to have appropriate authority,
resources and time to e� ectively manage the process.
To assist with planning, it is advised that a list of contacts for each participating executive/senior management team
member and the relevant unit/team be maintained (see Toolkit).
Unit teamFor each walk-round a lead is identi� ed from the unit/team being visited, usually the senior accountable person
responsible for the area visited. The unit/team manager and medical leads are each invited to attend. On the day,
there may be a number of other sta� present such as junior doctors, consultants, health and social care professionals,
clerical, catering, nurses/midwives and health care assistants. The priority is to have an opportunity to talk to both
patients and sta� .

7
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Senior Management Walk-round teamThe senior most accountable person (CEO/General Manager/Service Manager) leads each walk-round. Other
members of the executive/senior management team may be involved, for example:■ Lead/Executive/Clinical Director/Director Quality and Safety;
■ Director of Nursing/Midwifery;
■ Chief Operating O� cer;
■ Health and Social Care Professional Lead;
■ Head of Finance;
■ Head of Human Resources; and
■ Head of ICT.
The walk-round lead may be accompanied by (where possible):■ A patient representative/advocate or patient liaison o� cer;
■ A nominated note taker (normally from the executive/senior management teams administrative sta� ); 8 and
■ Non-Executive Director (member of the Board) – on occasions arranged through the CEO/General Manager/
Service Manager’s o� ce.
Advice may be sought from quality improvement, risk management, health and safety, healthcare records manager,
or technical services/estates/facilities sta� prior to, or following on from, the visit. To support dialogue and positive
relationships it is important that the Quality and Safety Walk-round numbers are kept small and never outnumber
the front line team. The maximum number visiting an area should be agreed.
Members of the walk-round team may be identi� ed, based on their experience and personal strengths, as being
prepared to provide further development and support to other team members. Some members of the executive/
senior management team may feel apprehensive about leading quality and safety oriented discussions and a
shadowing system among the executive/senior management team may be useful at the initial stages.
2.4 WhenThe Walk-rounds occur at an agreed frequency (at least monthly or as designated by the executive/senior
management team). Dates and times (most suitable for sta� and the service) are arranged and communicated by
the named Quality and Safety Walk-round person, who will schedule all dates and areas to be visited for the year.
2.5 WhereIt is useful for the walk-rounds to start with a tour of the unit/team and meeting with patients (where possible). It
is better to focus the walk-round rather than a formal meeting. A meeting area as close to the patient/service area
(as possible) such as an o� ce or seminar room can be used for the discussion. It is best to agree a time limit (for
example maximum one hour).
2.6 HowThe team in the area being visited is asked to describe what is working well or a change that was brought in at
local level that might also work in other locations. They may also be asked to think of a recent example of a risk or
patient safety incident they have experienced. The quality improvement plan or any challenges can be shared with
the executive/senior managment team.
8 The note taker should not be a member of the walk-round team as this impedes active participation in the discussion

8
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
It can be helpful to ask probing questions and all members of sta� are actively encouraged to participate. A number
of issues that might be considered are: ■ Identifying and acknowledging good practice;
■ Communication e.g. within teams and with patients;
■ Teamwork e.g. how the team operates;
■ Risk management e.g. the experience of the team in reporting incidents or near misses;
■ Prevention and control of HCAI e.g. standard of cleaning and compliance with hand-washing;
■ Environment e.g. changes to the physical environment;
■ Equipment e.g. new safety devices or maintenance and access to equipment;
■ Process e.g. medication reconciliation, drug errors or delays in prescribing medication, clinical audits, missing
or incomplete healthcare records;
■ Continuing Professional Development e.g. safety education and training speci� c to the area; and
■ Leadership e.g. key quality improvements plans to address National Standards.
At the end of the walk-round, everyone agrees the safety issues identi� ed, if any. The aim is for the safety issues
to be dealt with at a local level with the support of the executive/senior management team. If the ward/area is a
'productive ward' site, this is an opportunity to discuss progress with other improvement initiatives and update the
'visit pyramid'.
The � ndings of the walk-round can be circulated and discussed at the appropriate line management forum. By
exception they may be circulated also to the executive/senior management team. Responsibility is delegated to
address issues arising.
This will also provide evidence, for assurance. The aim is to complete these actions within an agreed timeframe. This
does not prevent all sta� from addressing the risks identi� ed and recording these on the unit/team risk register,
where appropriate.
2.7 Tracking MechanismFor e� ective use and follow up, the executive/senior management team normally commits to maintaining a record
of the process. A tracking mechanism (electronic) can then be used to monitor progress while at the same time
providing reports on issues identi� ed, actioned, escalated and resolved. The nominated Quality and Safety Walk-
round person will be responsible for maintaining the record.

9
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
3. Communication A strong communication plan is essential to the success of any Quality and Safety Walk-round initiative. This is informed by the approach adopted by the organisation. Brie� ng sta� so they know about the initiative and understand the aims is really important. General sta� brie� ngs, newsletters, notice boards, team meetings, and intranet communication may be used to promote the initiative (see suggested lea� et in the toolkit).
The nominated Quality and Safety Walk-round person arranges all communication and follow up as follows by:
3.1 At the start■ Creating the schedule for Quality and Safety Walk-rounds for the year; and
■ Distributing the schedule to all executive/senior management team members, heads of departments,relevant others and unit/team being visited with requests for the dates to be con� rmed in relevant diaries.
3.2 Before the Walk-round■ Issuing email reminder to the unit/team (the week before the scheduled visit).
■ Issuing email reminder to walk-round team (four days before the visit). It can be useful to include prompts of the information to be reviewed in preparation for the visit. These may include (but are not limited to):
❙ Relevant quality and performance indicators;
❙ Unit/team risk register;
❙ Infection prevention and control issues;
❙ Patient feedback about their experience (compliments/complaints);
❙ Incidents/near misses;
❙ Quality improvements;
❙ Sta� ng complements/absenteeism;
❙ Health and safety issues;
❙ Copy of the outstanding actions from the previous Walk-round visit; and
❙ Preparing material for the note taker to take on the walk-round.
3.3 Follow up after the Walk-round■ Updating the Quality and Safety Walk-round Database;
■ Preparing and circulating to all those present at the walk-round the draft action plan for comment and approval (within an agreed timeframe of the visit where possible);
■ Circulating the � nal action plan (within an agreed timeframe); and
■ Following up progress on the issues being actioned by the executive/senior management team.
3.4 On-going■ Creating the schedule for Quality and Safety Walk-rounds for each subsequent year;
■ Updating the Quality and Safety Walk-round Database on an on-going basis; and
■ Preparing reports as required.

10
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
4. Sample Guide for Discussion with PatientsThe prompts below are examples that may be used in the walk-round conversation with patients. The principles of the
National Healthcare Charter (2012) 'You and your health service' may be of assistance in preparing for the discussion.
These are: access, dignity and respect, safe and e� ective service, communication and information, participation,
privacy, improving health and accountability. See further information at http://www.hse.ie/eng/services/ysys/National_Healthcare_Charter
The questions are designed to promote constructive feedback. People often feel concerned about making a
complaint, therefore, if we invite them to make a positive statement it is easier to suggest improvements.
SUGGESTED QUESTIONS
1. How are you today?
2. Is there anything that we could do better?
3. If you were in-charge here, what would you do to make things work better?
During the discussion, there may be a chance to highlight some of the opportunities for patients to provide further
feedback, for example using the lea� et ‘You and your health service: tell us….your feedback’.
11
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
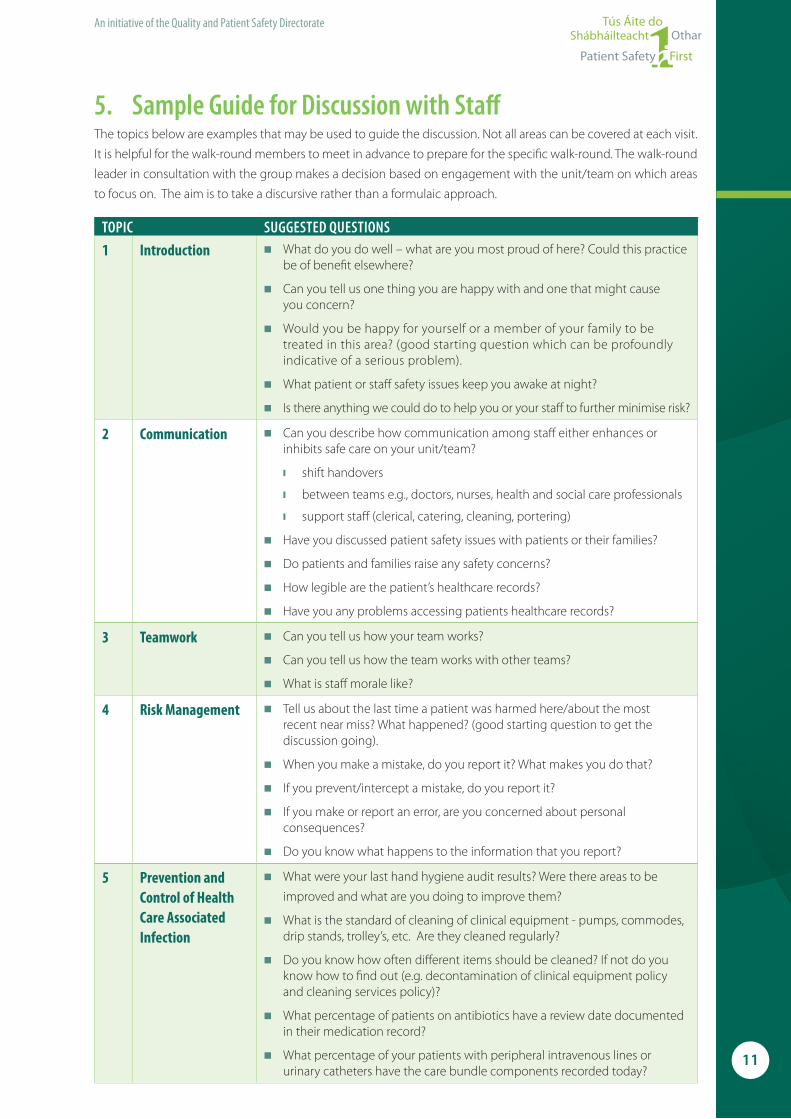
5. Sample Guide for Discussion with Staff The topics below are examples that may be used to guide the discussion. Not all areas can be covered at each visit.
It is helpful for the walk-round members to meet in advance to prepare for the speci� c walk-round. The walk-round
leader in consultation with the group makes a decision based on engagement with the unit/team on which areas
to focus on. The aim is to take a discursive rather than a formulaic approach.
TOPIC SUGGESTED QUESTIONS
1 Introduction ■ What do you do well – what are you most proud of here? Could this practice be of bene� t elsewhere?
■ Can you tell us one thing you are happy with and one that might causeyou concern?
■ Would you be happy for yourself or a member of your family to be treated in this area? (good starting question which can be profoundly indicative of a serious problem).
■ What patient or sta� safety issues keep you awake at night?
■ Is there anything we could do to help you or your sta� to further minimise risk?
2 Communication ■ Can you describe how communication among sta� either enhances or inhibits safe care on your unit/team?
❙ shift handovers
❙ between teams e.g., doctors, nurses, health and social care professionals
❙ support sta� (clerical, catering, cleaning, portering)
■ Have you discussed patient safety issues with patients or their families?
■ Do patients and families raise any safety concerns?
■ How legible are the patient’s healthcare records?
■ Have you any problems accessing patients healthcare records?
3 Teamwork ■ Can you tell us how your team works?
■ Can you tell us how the team works with other teams?
■ What is sta� morale like?
4 Risk Management ■ Tell us about the last time a patient was harmed here/about the mostrecent near miss? What happened? (good starting question to get the discussion going).
■ When you make a mistake, do you report it? What makes you do that?
■ If you prevent/intercept a mistake, do you report it?
■ If you make or report an error, are you concerned about personal consequences?
■ Do you know what happens to the information that you report?
5 Prevention and Control of Health Care Associated Infection
■ What were your last hand hygiene audit results? Were there areas to be
improved and what are you doing to improve them?
■ What is the standard of cleaning of clinical equipment - pumps, commodes, drip stands, trolley’s, etc. Are they cleaned regularly?
■ Do you know how often di� erent items should be cleaned? If not do you know how to � nd out (e.g. decontamination of clinical equipment policy and cleaning services policy)?
■ What percentage of patients on antibiotics have a review date documented in their medication record?
■ What percentage of your patients with peripheral intravenous lines or urinary catheters have the care bundle components recorded today?

12
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
TOPIC SUGGESTED QUESTIONS
6 Environment ■ What aspects of the environment are likely to lead to the next patientharm? Examples:
❙ Broken sinks, taps, bedpan washers, scales, ligature points, etc
❙ Not enough information available (e.g. building works a� ecting care)
7 Equipment ■ Do you have regular maintenance of your equipment? Do you have service notices on your equipment?
■ Do you have access to all the equipment you need to care for yourpatients safely?
8 Process ■ What audits (both clinical and non clinical) does your area undertake or lead?
■ Today, are you able to care for your patients as safely as possible? If not, why not?
■ Have there been any near misses that nearly caused patient harm butdidn’t? Examples:
❙ Taking a drug to give to a patient and then realising it is incorrect
❙ Mis-programming a pump, but having an alert that warns you
❙ Incorrect prescriptions/orders caught by nurses/midwives or other sta�
9 Continuingprofessional development
■ What incident, risk management, quality improvement and clinical governance training have you had?
■ What infection prevention and control and medication management training have you had?
■ Are your team up to date with mandatory training, for example, Basic Life Support, Moving and Handling, Fire Training, Hand Hygiene?
10 Leadership ■ Do you feel supported when you make a mistake or things go wrong?
■ Who leads your team?
■ What speci� c intervention from senior management would make the work you do safer for patients and sta� ? Examples:
❙ Organise multi-disciplinary groups to evaluate a speci� c problem
❙ Facilitate in changing the attitude of a particular group
❙ Facilitating interaction between two speci� c groups
■ What would make these Quality and Safety Walk-rounds more e� ective?
■ Have you found participation in these Quality and Safety Walk-rounds bene� cial?

13
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
6. Impact of Quality and Safety Walk-roundsIt is important to build a process to demonstrate the impact of the Quality and Safety Walk-rounds. One targeted
measure might be considered. Some examples are:■ Number of problems identi� ed by sta� which are addressed within a certain time period;
■ Number of safety-based changes made by sta� by units/teams per year;
■ Percent changes in overall surveillance data (for example, infection rates);
■ Number of compliments/complaints received per month (outcome measure); and
■ Response to patient safety culture survey (process measure).
7. SummaryIn summary, walk-rounds can: ■ Demonstrate top level commitment to improving safety and quality of care;
■ Provide opportunity for direct engagement and communication with patients about safety
and their experience;
■ Establish lines of communication about patient safety among frontline sta� and managers throughout all
departments within the organisation;
■ Provide opportunities for sta� to raise concerns and suggest improvements;
■ Identify opportunities with sta� concerned for improving safety;
■ Encourage reporting of issues, errors, and near misses;
■ Promote a culture for change pertaining to patient safety;
■ Establish local solutions to minimise risk; and
■ Demonstrate accountability.

14
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Toolkit: Quality and Safety Walk-rounds
Patientfirst
Openculture
Supportingperformanceperformance
Personalresponsibilityresponsibilityresponsibility
Definedauthority
Leadership
ClearaccountabilityaccountabilityMultidisciplinaryMultidisciplinary
working
Continuousquality
improvementimprovementimprovementimprovementimprovementquality
improvementquality Safety

15
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
An initiative of the Quality and Patient Safety Directorate
Appe
ndix
1: Sa
mpl
e Qua
lity a
nd Sa
fety
Wal
k-ro
unds
Cont
act i
nfor
mat
ion
– as
of XX
(mon
th/y
ear)
UNIT
/TEA
MDI
RECT
ORAT
E/
DIVI
SION
NURS
E/M
IDW
IFE L
EAD
MED
ICAL
LEA
DPH
ONE
EMAI
L
1 2 3 4 5 6 7 8 9 10 11 12

16
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
It is useful to maintain a listing of the identi� ed senior sta� who lead or participate in Quality and Safety Walk-rounds.
Executive/Senior Managers (one lead for each walk-round):
NAME TITLE POINT OF CONTACT
[insert details] CEO/General Manager/Service Manager[insert email and phone contact details]
Lead/Executive/Clinical Director/Director of Quality and Safety
Chief Operating O� cer
Head of Finance
Head of Human Resources
Head of ICT
Quality Improvement/Risk Management/Health and Safety/Technical Services/Estates/Facilities (May be involved in the visit or provide advice and support in follow up to the visit)
NAME TITLE POINT OF CONTACT
Occasionally, a Non-Executive Director (Board Member) may accompany the Walk-round team. This is arranged
through the CEO/General Manager/Service Manager O� ce. These are as follows:
Non-Executive Directors
NAME
Appendix 2: Sample Executive/Senior Management Team: Quality and Safety the Walk-round Members

17
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Appendix 3: Sample Communication Prior to the Walk-round
An email reminder can be sent to the unit/team the week before their Walk-round visit. An example template
is as below:
Dear all [insert date]
XXXX ward has been scheduled for a Quality and Safety Walk-round on the dd/mm/yyyy from XX:XX am to XX:XX am.
XXXX (Senior Manager) will be accompanied by XXXX Plus any other member
The aim of the Walk-round is to allow the senior management team to learn about safety issues on the unit/team that are of concern to staff or patients.
They will ask questions to which there are no right or wrong answers. The senior team would like to use the visit as an opportunity to speak to all staff of any grade or profession. Please inform staff members of the walk-round and their opportunity to engage in the process. The senior managers would also welcome the opportunity to speak with patients if possible, at the start of the visit, and would therefore appreciate it if you could kindly arrange this on the day (if appropriate).
If you have any queries or require further clarifi cation, please contact me via email or contact details be-low. Attached is a leafl et, which explains the purpose and process of the visit. You may wish to bring it to the attention of all your team to help them understand the purpose of the visit. A notice is also attached.
Many thanks and kind regards,
A copy of the Quality and Safety Walk-round lea� et and notice can be attached.
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
17

18
An initiative of the Quality and Patient Safety Directorate
Appendix 4: Sample Quality and Safety Walk-round Notice
Quality and Safety Walk-round
XXX Unit/TeamXXX DateXXX Time
Walk-round Senior Management Team:
XXXX (Senior Manager lead)
Notetaker :
XXXX
Unit/Team:
XXXXXXXX (CN/MM)
XXXX (Assistant Director/ Directorate Nurse/Midwife Manager)
XXXX (Business/Programme Manager)
XXXX (Medical Lead)
XXXX (specialty/ward overview):
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

19
An initiative of the Quality and Patient Safety Directorate
Appendix 5: Sample Walk-round Leafl et
Quality and Safety Walk-rounds What is the aim of the Walk-round?The aims in introducing Quality and Safety Walk-rounds are:■ Demonstrate senior managers’ commitment to quality and
safety for patients, sta� and the public;
■ Increase sta� engagement and develop a culture of open
communication;
■ Identify, acknowledge and share good practice;
■ Support a proactive approach to minimising risk, timely
reporting and feedback; and
■ Strengthen commitment and accountability for quality
and safety.
How do they fi t in with the quality and safety programme?Our aim is to minimise harm – that is, we want to ensure that all
preventable harm is eliminated and this will need the help of all
members of sta� and of patients and the public.
Quality and Safety Walk-rounds will assist organisations in
demonstrating their commitment to sta� engagement, building
relationships, trust and patient service quality and safety. They
will also assist in working to meet the National Standards for Safer
Better Healthcare (2012), the Quality Framework for Mental Health
Services in Ireland (2007) and preparing for the new governance
arrangements within the health system.
Who is involved?You and a member of the senior management team: CEO/GM/
Service Manager, Chief Operating O� cer, Head of Finance, Director
of Nursing/Midwifery, Lead/ Executive Clinical Director, and Head
of Human Resources or ICT. A member of the senior management
team will visit each area accompanied by a patient representative/
advocate or patient liaison o� cer (where possible) as well as a
administrative support to record key issues discussed.
Where does the walk-round take place?It is useful for the walk-rounds to start with a tour of the unit/team
and meeting with patients (where possible). It is better to focus on
the walk-round rather than a formal meeting. The walk-round team
and the sta� can meet and hold the discussions in any area that
suits the local team. This may be in the patient areas or in a quiet
room within the main clinical area.
What happens at the Walk-round?A member of the walk-round team will explain and introduce the
process including the agreements for con� dentiality and patient
safety disclosures. Members of the visiting walk-round team will
then ask some questions to start a dialogue. All members of sta�
who participate are encouraged to respond and participate in the
discussion.
Issues that can be raised may include: ❙ Good practice and safety developments;
❙ Your key patient safety concerns;
❙ What can we do together to improve?;
❙ How does your local team operate?;
❙ Communication – within teams and with patients;
❙ How can the senior management team help?; and
❙ Incident reporting & safety culture in the organisation.
At the end of the process, we will agree the actions to be taken
forward together to make the area safer for patients.
We ask sta� to think of an example of good practice and a patient
safety experience that they have addressed and bring this to the
meeting to share with us, e.g. patients not getting their medications
on time, patients not being reviewed when required, etc.
What will happen to the information we gather?Senior managers will respond to the local team within an agreed
time frame, thanking all individuals for their participation and
highlighting the main areas discussed actions agreed.
ReferencesFrankel, A., Graydon-Baker, E., Neppl, C., Simmonds, T., Gustafson,
M., and Gandhi, T. (2003) “Patient Safety Leadership Workarounds”
Joint Commission Journal on Quality and Safety 29 (1):16-26
Leonard M, Frankel A, Simmonds T, Vega K.: Achieving (2004) Safe
and Reliable Healthcare Strategies and Solutions. Chicago: Health
Administration Press.
For Information Contact:[insert details
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

20
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Appendix 6: Sample Preparation for the Senior Managers Leading the Quality and Safety Walk-round
Dear All , [insert date]
The Quality and Safety Walk-round visit which you are leading is scheduled to visit XXXX unit/team on dd/mm/yyyy from xx:xx am to xx:xx am.
Please fi nd attached a sample question guide. This information serves as background material to assist you in preparing for the conversation with the unit/team. Following this rigidly, on the walk-round may distract from the fl ow of the discussion. An open dialogue is more eff ective.
The information you might consider reviewing, in existing reports, in preparation for visit might include:
■ Relevant quality and performance indicators;
■ Unit/team risk register;
■ Infection prevention and control issues;
■ Complaints/compliments;
■ Incidents/near misses;
■ Quality improvements;
■ Staffi ng complements/absenteeism; and
■ Health and safety issues.
If you require any further details or clarifi cation about the visit, please do not hesitate to contact me.
Best wishes,
Attach the Action Plan report from the last walk-round (if relevant) and the Quality and Safety Walk-round
Discussion Guide.

21
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Appendix 7: Sample Communication after the Quality and Safety Walk-round
A copy of the draft Action Plan is circulated to all those present at the walk-round for comment and approval. All
positive feedback and suggestions for improvements are also noted and these are included in the email sent to the
team following the walk-round (see below).
In some instances, it can be useful to focus on a small number of high priority issues identi� ed on a Quality and
Safety Walk-round.
A suggested email template is as below:
Dear XXXX, [insert date]
Thank you for investing the time and participating in the Quality and Safety Walk-round to XXXX unit/team on dd/mm/yyyy.
As agreed, please fi nd attached a draft version of the action plan that highlights safety action points that together we will take forward with the intention of resolving or raising further awareness on the issue.
In addition, we would like to note the positive feedback we received during the visit:-
1.2.3.
Suggestions for unit/team to consider as part of promoting further good practice are:
1.2.3.
If you wish to make any amendments to the attached report or to the comments above, I would be grateful if you could please let me know by XXX 20XX. The fi nal action plan will then be emailed to all concerned to ensure agreed actions are taken forward.
Kind regards and many thanks
It is good practice to distribute the draft action plan within an agreed time frame.

22
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Appendix 8: Sample Final communication after the Quality and Safety Walk-round
The � nal action plan is circulated to all participants in the walk-round within an agreed timeframe.
An example email template is as below:
Dear All, [insert date]
Thank you for participating in the Quality and Safety Walk-round to XXXX unit/team ondd/mm/yyyy. Further to my email (dated XXX) please fi nd attached the fi nal action plan that takes account of your comments and highlights the agreed priority issues that will be taken forward.
Again, we would like to note the positive feedback we received during the visit:
1.2.3.
Suggestions for unit/team to consider as part of promoting further good practice are:
1.2.3.
Our agreed time scale for addressing the issues is dd/mm/yyyy. Please keep me briefed on the progress to enable me to update the Quality and Safety Walk-round database.
Thank you.
Kind regards,
The named person for coordinating the Quality and Safety Walk-rounds takes responsibility for following up progress
on the action plans as the deadlines approach. Progress on all other issues are normally captured at the next walk-
round visit for that particular area (or as agreed by the executive/senior management team).

23
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
An initiative of the Quality and Patient Safety Directorate
Appe
ndix
9: Sa
mpl
e Qua
lity a
nd Sa
fety
Wal
k-ro
und A
ctio
n Pl
an Te
mpl
ate
TOPI
CIS
SUE O
R CO
NCER
N RA
ISED
WHA
T HAS
ALR
EADY
BEE
N DO
NE TO
AD
DRES
S ISS
UEAC
TION
TO B
E TAK
EN FO
LLOW
ING
WAL
KRO
UND
PERS
ON
RESP
ONSI
BLE
DUE D
ATE
Are
as:
Inci
dent
Rep
ortin
g; C
omm
unic
atio
n; E
nviro
nmen
t; Eq
uipm
ent;
Proc
ess;
Team
wor
k; P
reve
ntio
n an
d co
ntro
l of H
CAI;
Cont
inui
ng P
rofe
ssio
nal D
evel
opm
ent;
Lead
ersh
ip.

24
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
An initiative of the Quality and Patient Safety Directorate
Appe
ndix
9: Sa
mpl
e Qua
lity a
nd Sa
fety
Wal
k-ro
und A
ctio
n Pl
an Te
mpl
ate (
cont
inue
d)
FEED
BACK
SUGG
ESTI
ONS
Are
as:
Inci
dent
Rep
ortin
g; C
omm
unic
atio
n; E
nviro
nmen
t; Eq
uipm
ent;
Proc
ess;
Team
wor
k; P
reve
ntio
n an
d co
ntro
l of H
CAI;
Cont
inui
ng P
rofe
ssio
nal D
evel
opm
ent;
Lead
ersh
ip
25
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
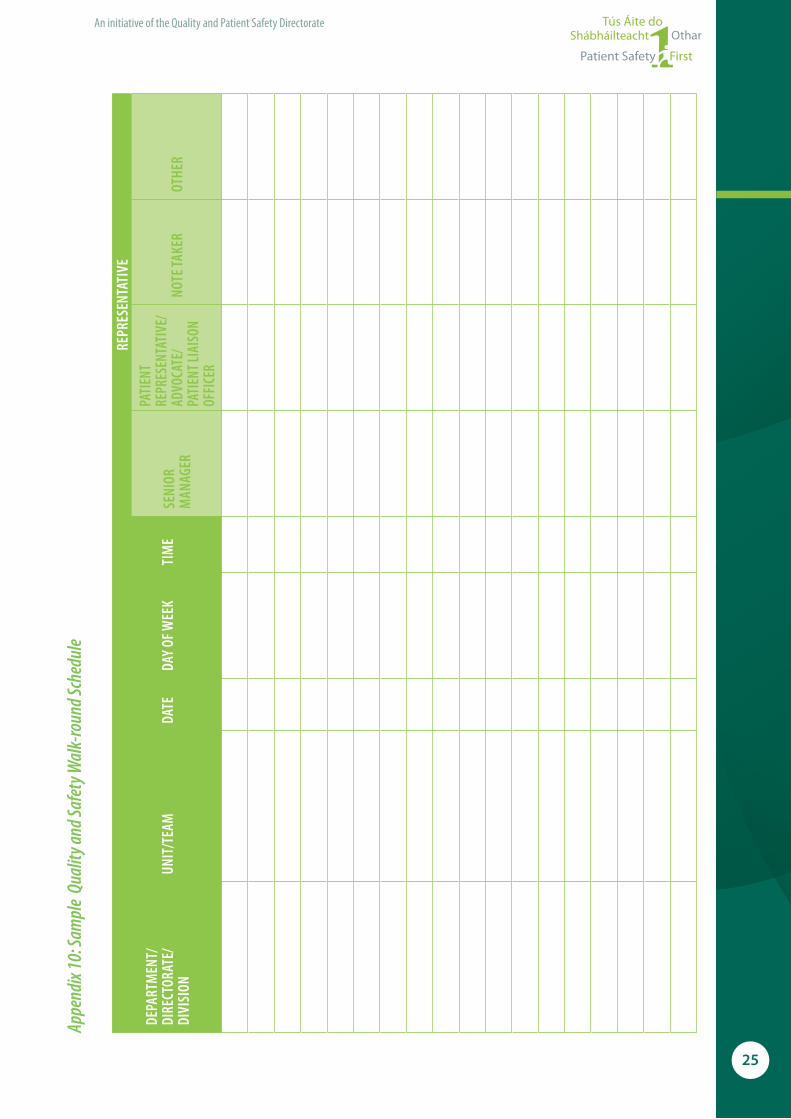
An initiative of the Quality and Patient Safety Directorate
Appe
ndix
10: S
ampl
e Qu
ality
and S
afet
y Wal
k-ro
und S
ched
ule
DEPA
RTM
ENT/
DIRE
CTOR
ATE/
DIVI
SION
UN
IT/T
EAM
DATE
DAY
OF W
EEK
TIM
E
REPR
ESEN
TATI
VE
SENI
OR
MAN
AGER
PATI
ENT
REPR
ESEN
TATI
VE/
ADVO
CATE
/PA
TIEN
T LIA
ISON
OF
FICE
R
NOTE
TAKE
ROT
HER

26
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

27
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

28
An initiative of the Quality and Patient Safety Directorate
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…

About the Quality and Patient Safety DirectorateThe Quality and Patient Safety (QPS) Directorate of the Health Service Executive (HSE) was established in January 2011, on the appointment of the National Director, Dr. Philip Crowley. The national director is a member of both the HSE Senior Management Team and the Board of the HSE.
The role of the QPS Directorate is to provide leadership and be a driving force by supporting the statutory and voluntary services of the HSE in providing high quality and safe services to patients, their families and members of the public.
The National Director for Quality and Patient Safety has responsibility for leading and supporting:
– Capacity and capability - developing a strong system of integrated corporate and clinical governance. Strengthening and embedding the role of clinical directors. Achieving a critical mass of senior healthcare sta� with a knowledge and understanding of improvement science through the Diploma in Leadership and Quality in Healthcare.
– Clinical e� ectiveness and audit - providing systems and tools to assist service providers in embedding national standards and HSE recommended practices. Supporting the National O� ce of Clinical Audit and undertaking a planned programme of QPS audits providing independent assurance on safety and quality.
– Information management - monitoring and analysing data to provide information to support the quality improvement process and learning. Widening the use of the Health Intelligence Ireland information system and National Quality Assurance Intelligence System (NQAIS) to help drive quality, safety, and e� ciency of health services.
– Learning and sharing information - innovating and improving how we share learning. Enhancing the way we manage and learn from incidents through revised incident management policies and guidelines.
– Patient and public involvement – Continually involving service users in improving care delivery and developing systems for listening to and seeking their feedback.
– Quality and performance indicators - measurement of quality and safety through the adoption and development of indicators in collaboration with the national clinical programmes.
– Patient safety and risk management - promoting risk management as everyday practice. Advocating and designing patient safety initiatives, e.g. Health Care Acquired Infection programme. Designing a framework for quality and safety to cover all stages of the chain from organ donation to transplantation.
– Sta� ng and sta� management – appreciating the importance of caring for the morale of front line sta� . Designing systems for measuring sta� perceptions of the patient safety culture. Leading the HSE relationship with regulatory and statutory.
While it is the QPS Directorate role to determine and de� ne systems and processes for quality and safety within the HSE, implementation is the responsibility of and achieved by the Integrated Services, Clinical Strategy and Programmes, Cancer Control, Children and Families, Finance, Communication, Human Resource, and Corporate Planning and Corporate Performance, Directorates.
Contact Details Quality and Patient Safety Directorate, Health Service Executive, Room 1.51, Dr. Steevens, Dublin 8Tel: +353 (0)1 6352038email: [email protected] For further information please see www.hse.ie/go/qps
The HSE is a signatory to Patient Safety First - the initiative through which healthcare organisations declare their commitment to patient safety. Through participation in this initiative, those involved aspire to play their part in improving the safety and quality of healthcare services. This commitment is intended to create momentum for positive change towards increased patient safety. For further information see www.patientsafety� rst.ie
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
Clinical Governance: we are all responsible…
We are all responsible…and together we are creating a safer healthcare system

We are all responsible…and together we are creating a safer healthcare system
An initiative of the Quality and Patient Safety Directorate, Health Service Executive, May 2013 ©
Toolkit
Quality and SafetyWalk-rounds
THERAPY PROFESSIONS COMMITTEE
© Health Service ExecutiveQuality and Patient Safety DirectorateMay 2013ISBN 978-1-906218-60-7
Quality and Patient Safety DirectorateHealth Service ExecutiveDr Steevens’ HospitalDublin 8Ireland
Telephone: +353 1 6352344Email : [email protected] Web : http://www.hse.ie