Embed Size (px)
Citation preview

Patient Specific QA for Monte Carlo Lung SBRT on Cyberknife:
Is It Necessary?J. Fabien, MS; Y. Zhang, MS; J. Brindle, PhD; D. Dobbins, CMD;
T. Podder, PhD; B. Wessels, PhD
University Hospitals Seidman Cancer CenterCase Western Reserve University Medical Center

The Lung SBRT Issue
• Originally, all Cyberknife planning used Ray Tracing algorithm
• 2012: Started using Monte Carlo algorithm
• RTOG clinical trials exclude Ray Tracing
• Realized a 10-20% deficiency in dose and resulting loss of prescription coverage
• After dosimetry effects were seen, ALL lung and T-spine patients were calculated with MC

Monte CarloRay Tracing
The Lung SBRT Issue
54 Gy
Ray Tracing
The Lung SBRT Issue
Monte CarloRay Tracing
The Lung SBRT Issue
Ray Tracing
The Lung SBRT Issue
Monte CarloRay Tracing
The Lung SBRT Issue

Monte CarloRay Tracing
PTV = 98.6%CTV = 100%
PTV = 2.2%CTV = 19.8%
The Lung SBRT Issue
Ray Tracing
The Lung SBRT Issue
Monte CarloRay Tracing
The Lung SBRT Issue

Ray Tracing
Ray tracing calculation using equivalent path length:
• TPR (FS, Deff)
• OCR (FS, R800, Deff)
• OF (FS, SAD)
OFTPRSAD
OCRMUD
2800

Ray TracingSecond check using MuCheck (Oncology Data Systems):
Ray Tracing dose = 6000 cGyMuCheck dose = 6026 cGy
Ray Tracing
Ray Tracing dose = 6000 cGyMuCheck dose = 6026 cGy

• Much more complex
• Much more accurate with heterogeneities
• No software second check exists
• Phantom measurement is necessary to verify dose
Monte Carlo

The Method
• Use heterogeneous phantom
• Overlay chamber position in low gradient area
• Calculate mean MC dose to chamber volume
• Deliver patient plan to phantom, measure dose to chamber

1. Transfer patient plan onto hetero phantom

2. Calculate low resolution dose to check & adjust chamber position

3. Calculate high resolution

4. Calculate with Monte Carlo
MC chamber mean dose = 85.30 Gy

5. Deliver patient plan to hetero phantom with ion chamber
MC chamber mean dose = 85.30 GyMeasured chamber dose = 84.14 Gy -1.4%

-10.00%-9.00%-8.00%-7.00%-6.00%-5.00%-4.00%-3.00%-2.00%-1.00%0.00%1.00%2.00%3.00%4.00%5.00%6.00%7.00%8.00%9.00%
10.00%
0 5 10 15 20 25 30 35 40 45 50 55 60
Pt #
% D
iffer
ence
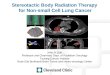
Delivery QA Results
Avg. MC delivery % Error = -2.50%
N = 60
Measured dose vs. MC calculated dose for 60 patients, % difference:

Is it necessary?
• Patient specific QA varies across Cyberknife users• We sought verification of MC accuracy using
chamber measurements• Use hetero phantom to simulate patient anatomy
to uncover dose discrepancies• Reduce frequency once baseline is established
Yes … initially.

Current Clinical Implementation
• Verified sufficiently the MC algorithm is working, and more accurate for hetero anatomy
• 60 patients measured, average difference -2.5%• In radiation oncology we nominally require a 2nd
check calculation• Currently we use a calculated MC vs. RT QA in a
homogenous phantom to identify gross planning, collimator or alignment errors
• 20 patients calculated, average difference -2.0%

Calculated QA Method
• Use homogenous phantom
• Overlay patient plan in center of phantom
• Calculate max point dose with RT, then MC for same point
• Export RT beam list for 2nd check

1. Transfer patient plan onto homog. phantom

2. Calculate low resolution to verify position

RT Max dose = 85.30 Gy
3. Calculate high resolution Ray Tracing dose

RT Max dose = 85.30 GyMC (RT Max) dose = 83.03 Gy
4. Calculate Monte Carlo dose
-2.7%

5. Compare with MUCheck results
% Diff. = +0.1%
MC dose = 83.03 GyRT dose = 85.30 Gy
MUCheck dose = 85.41 Gy
% Diff. = -2.7%

Monte Carlo Calculated QA Results
-10.00%-9.00%-8.00%-7.00%-6.00%-5.00%-4.00%-3.00%-2.00%-1.00%0.00%1.00%2.00%3.00%4.00%5.00%6.00%7.00%8.00%9.00%
10.00%
0 5 10 15 20
Pt #
% D
iffer
ence
Monte CarloMuCheck
Avg. MuCheck % Error = +0.07%
Avg. MC-RT % Error = -2.07%
N = 20
Calculated QA ResultsRT vs. MC calculated dose & RT vs. MuCheck 2nd check
% difference (20 patients):