-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
1/92
PATOPHYSIOLOGY &PATOPHYSIOLOGY &
MANAGEMENT OF STROKEMANAGEMENT OF STROKE
Abdul GofrAbdul Gofr
Neurology Department oNeurology Department o
Medical FacultyMedical Faculty
Gadjah Mada UniversityGadjah Mada University
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
2/92
Stroke: DefnitionStroke: Defnition
Stroke is clinically defned as aStroke is clinically defned as
aneurologic syndrome characterizedneurologic syndrome
characterizedby acute disruption o blood ow toby acute disruption o
blood ow to
an area o the brain andan area o the brain andcorresponding
onset o neurologiccorresponding onset o neurologicdefcits related
to the concerneddefcits related to the concernedarea o the
brainarea o the brain
Nurs Clin N Am 2002;37:35-57
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
3/92
Causes o StrokeCauses o Stroke
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
4/92
1
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
5/92
Defnition o Ischemic StrokeDefnition o Ischemic Stroke
Almost 80% oAlmost 80% ostrokes are romstrokes are roman emboli
or aan emboli or athrombusthrombus
Embolic &Embolic &ThromboticThromboticstrokes arestrokes
areISCHEICISCHEIC
! "#% o strokes! "#% o strokes
are romare romhemorrha$e ithhemorrha$e ithan e'en smalleran e'en
smaller(ercenta$e(ercenta$ecause) b*cause) b*
h*(o(erusionh*(o(erusion
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
6/92
Dr.J.Husada 11-2003
Apoptotic
Cell Death
Necrotic
Cell Death
Ischemic
Injury
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
7/92
Aterosclerotic is a normal response to arterialendotel
injuryAterosclerotic plaque forming, start in youngClinical
manifestation : acute and tent to occur one
time because sudden plaque rupture
1. Vascular : Aterosclerotic process
2. Biochemistry change /cellular
chemist
2 process in ischemic stroke:2 process in ischemic stroke:
C I h i
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
8/92
Causes o Ischaemic
!"#$%&
Blocka'e o (loo' lo) (y ateroma* em(oli*an' ateroscelerotic
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
9/92
EmbolicEmbolic
+nce in *our+nce in *our
brain thebrain the
embolusembolus
e'entuall* tra'else'entuall* tra'els
to a bloo) 'esselto a bloo) 'essel
small enou$h tosmall enou$h to
block its (assa$eblock its (assa$e
The embolusThe embolus
lo)$es therelo)$es there
blockin$ theblockin$ the
bloo) 'essel an)bloo) 'essel an)
causin$ a strokecausin$ a stroke
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
10/92
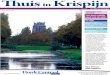
Adapted from Goldstein, et al. Circulation2001;10:1!"1#2.
6! "#ararin$6! "#ararin$%&! "aspirin$%&! "aspirin$
AtrialAtrial
fbrillationfbrillation
"non'valvular$"non'valvular$
%(')(! #ith statins in patients%(')(! #ith statins in
patients#ith *no#n coronary heart disease#ith *no#n coronary heart
disease
H*(erli(i)emiaH*(erli(i)emia
++! reduction in hypertensive++! reduction in hypertensive
diabetics #ith tight blood pressurediabetics #ith tight blood
pressurecontrolcontrol
DiabetesDiabetes
,(! #ithin & year- baseline,(! #ithin & year-
baselineater , yearsater , years
.mo*ing.mo*ing
)(! ' +(!)(! ' +(!/ypertens/ypertensionion
0is* reduction #ith0is* reduction #ithtreatmenttreatment
FactorFactor
Potential Stroke Risk Reduction for IndividualsPotential Stroke
Risk Reduction for Individuals
AHA GuidelinesAHA Guidelines
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
11/92
Stroke: ClassifcationStroke: Classifcation
schemic strokeschemic stroke: Account for 80%. Results from:
Account for 80%. Results fromocclusion in the blood vessel
supplying the brainocclusion in the blood vessel supplying the
brain
hromboti
hromboti : !cclusion due to: !cclusion due to
atherothrombosis of small"large vesselsatherothrombosis of
small"large vessels
supplying the brainsupplying the brain
#mboli
mboli : !cclusion due to embolus arising: !cclusion due to
embolus arising
either from heart $e.g. atrial fibrillationeither from heart
$e.g. atrial fibrillation
valvular disease& or blood vesselvalvular disease& or
blood vessel
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
12/92
'lassification $cont.&'lassification $cont.&
(emorrhagic strokeemorrhagic stroke: Account for )0%. Results
from: Account for )0%. Results fromrupture of blood vessels leading
to bleeding inrupture of blood vessels leading to bleeding in
brainbrain
ntracerebral:
ntracerebral: *leeding +ithin the brain due to*leeding +ithin
the brain due to
rupture of small blood vessels. !ccurs mainlyrupture of small
blood vessels. !ccurs mainly
due to high blood pressuredue to high blood pressure
,ubarachnoid:
ubarachnoid: *leeding around the brain-*leeding around the
brain-
commonest cause is rupture of aneurysm.commonest cause is
rupture of aneurysm.
!ther causes: (ead inury!ther causes: (ead inury
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
13/92
Stroke: ,re)is(osin$ actorsStroke: ,re)is(osin$ actors Age $risk
doubles forAge $risk doubles for
every decade / age &every decade / age &
1ender1ender
$males/females&$males/females& 2amily history of2amily
history of
stroke"IAstroke"IA
(ypertension(ypertension 3iabetes3iabetes
(yperlipidemia(yperlipidemia
(yperhomocysteinemia(yperhomocysteinemia
!besity!besity
,moking,moking
Atrial fibrillation
trial fibrillation
,edentary lifestyle,edentary lifestyle
3rug abuse $e.g.3rug abuse $e.g.
cocaine use&cocaine use&
(ormone(ormonereplacement therapyreplacement therapy
!ral contraceptive!ral contraceptive
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
14/92
0is* Factors or .tro*e0is* Factors or .tro*e
Non+,o'iia(le
#isk -actors or !troke$Age
$%e&$'ace(et)nicity$*amily )istory
Modifable 0is*Modifable 0is*Factors or .tro*eFactors or
.tro*e66
H*(ertensionH*(ertension
DiabetesDiabetes
Smokin$Smokin$
H*(erli(i)emiaH*(erli(i)emia
Caroti) stenosisCaroti) stenosisAtrial fbrillationAtrial
fbrillation
http://www.clevelandclinicmeded.com/diseasemanagement/neurology/stroke/stroke.htmhttp://www.clevelandclinicmeded.com/diseasemanagement/neurology/stroke/stroke.htmhttp://www.clevelandclinicmeded.com/diseasemanagement/neurology/stroke/stroke.htm
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
15/92
Stroke: S*m(tomsStroke: S*m(toms
+nset o stroke s*m(toms+nset o stroke s*m(toms
'aries as (er t*(e o stroke:'aries as (er t*(e o stroke:
- 1hrombotic stro*e1hrombotic stro*e: De'elo(: De'elo(more
$ra)uall*more $ra)uall*
- 2mbolic stro*e2mbolic stro*e: Hits su))enl*: Hits su))enl*
- /emorrhagic stro*e/emorrhagic stro*e: Hits: Hitssu))enl* an)
continues to orsensu))enl* an) continues to orsen
S k SSt k S t
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
16/92
Stroke: S*m(tomsStroke: S*m(toms
.cont/.cont/ 3i44iness3i44iness 'onfusion'onfusion
5oss of balance"coordination5oss of balance"coordination
6ausea"vomiting6ausea"vomiting 6umbness"+eakness on one side of the
body6umbness"+eakness on one side of the body
,ei4ure,ei4ure ,evere headache,evere headache 7ovement
disorder"speech disorder"blindness etc7ovement disorder"speech
disorder"blindness etc
$depending on the area of brain affected&$depending on the
area of brain affected&
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
17/92
,ymptom and ,ign,ymptom and ,ign
'onsider stroke in any patient presenting +ith'onsider stroke in
any patient presenting +ithacuteacute
neurological deficit or any alteration in level ofneurological
deficit or any alteration in level of
consciousness.consciousness.
'ommon signs of stroke include the follo+ing:'ommon signs of
stroke include the follo+ing: Acute hemiparesis or hemiplegiaAcute
hemiparesis or hemiplegia 'omplete or partial hemianopia monocular
or'omplete or partial hemianopia monocular or
binocular visual loss or diplopiabinocular visual loss or
diplopia
3ysarthria or aphasia3ysarthria or aphasia Ataia vertigo or
nystagmusAtaia vertigo or nystagmus ,udden decrease in
consciousness,udden decrease in consciousness
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
18/92
Transient Ischemic Attack .TIATransient Ischemic Attack .TIA
11ini stroke2ini stroke2 Stroke s*m(toms last or less than 34
hoursStroke s*m(toms last or less than 34 hours
.usuall* "0 to "# mins.usuall* "0 to "# mins 5esult as a brie
interru(tion in bloo) 6o to5esult as a brie interru(tion in bloo)
6o to
brainbrain E'er* TIA is an emer$enc*E'er* TIA is an emer$enc*
TIA ma* be a arnin$ si$n o a lar$er strokeTIA ma* be a arnin$ si$n
o a lar$er stroke ,atients ith (ossible TIA shoul) be
e'aluate),atients ith (ossible TIA shoul) be e'aluate)
b* a (h*sicianb* a (h*sician
Diagnosis o acute ischemicDiagnosis o acute ischemic
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
19/92
Diagnosis o acute ischemicDiagnosis o acute ischemic
stro*estro*e
9hysical eamination9hysical eamination 6eurological
6eurological#amination#amination
*rain imaging $cranial ' and"or 7RI&: 3etect*rain imaging
$cranial ' and"or 7RI&: 3etect
small vessel disease. (elps to effectivelysmall vessel disease.
(elps to effectively
discriminate bet+een ischemic and hemorrhagicdiscriminate
bet+een ischemic and hemorrhagic
stroke and stroke from brain tumoursstroke and stroke from brain
tumours
3oppler ultrasonography"Angiography: 3etect3oppler
ultrasonography"Angiography: 3etect
large vessel atherosclerosislarge vessel atherosclerosis
#'1"#chocardiography: 3etect cardiac
embolism#'1"#chocardiography: 3etect cardiac embolism
#clusion of conditions mimicking stroke#clusion of conditions
mimicking stroke$hypoglycemia migraine sei4ure&$hypoglycemia
migraine sei4ure&
Ischemic stroke )ia$nosticIschemic stroke )ia$nostic
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
20/92
Ischemic stroke )ia$nosticIschemic stroke )ia$nostic
al$orithmal$orithmAcute ocal (rain 'eicit
ea' C"
Ischemic !troke
&C
&cho
CA#DIAC&,B$0I!,
0A#& A#"A"$!C0$!I!
!,A00V&!!&0 DI!&A!&
$" D&",IN&DCA!&
Doppler
,#AAngiogram
,#I
C"
Vasculopathy
Coagulopathy
C#3"$&NIC
!"#$%&
&4clu'e' hypoglycemia* migraine
)ith aura* post+sei5ure 'eicit
TIA (if CT/MR brain imaging
)ithout ischemic lesion6
7 1 hour
0acunar syn'romeCorticalsyn'rome
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
21/92
AcuteAcute
TreatmentTreatment
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
22/92
rr77TT,A,A
I a 7hour in)o o treatment canI a 7hour in)o o treatment can
be met thrombol*tic thera(* ithbe met thrombol*tic thera(*
ith
intra'enous t7,A can be benefcial orintra'enous t7,A can be
benefcial or
each o the ma9or cate$ories oeach o the ma9or cate$ories
oischemic stroke:ischemic stroke:
atherothromboticatheroembolicatherothromboticatheroembolic
car)ioembolic an) small 'esselcar)ioembolic an) small
'esselocclusi'e .lacunar strokeocclusi'e .lacunar stroke
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
23/92
3ntravenous 1hrombolysis3ntravenous 1hrombolysis
Intra'enous rt,A .0/; m$k$ ma
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
24/92
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
25/92
The intra'enous a)ministration oThe intra'enous a)ministration
o
stre(tokinase or treatment o stroke is notstre(tokinase or
treatment o stroke is not
recommen)e) .Class III =e'el o E'i)encerecommen)e) .Class III
=e'el o E'i)ence
A/A/ &he intra"enous administration o ancrod,&he
intra"enous administration o ancrod,
tenecteplase,reteplase, desmoteplase,tenecteplase,reteplase,
desmoteplase,
urokinase, or other thrombolytic agentsurokinase, or other
thrombolytic agents
outside the setting o a clinical trial is notoutside the setting
o a clinical trial is notrecommended (Class , !e"el o
#"idencerecommended (Class , !e"el o #"idence
C$%C$%
H i C )i b liHe(arin or Car)ioembolic
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
26/92
He(arin or Car)ioembolicHe(arin or Car)ioembolic
Stroke:Stroke:
Stroke recurrence is lo much lessStroke recurrence is lo much
less
than "%)a* in frst 3 eeksthan "%)a* in frst 3 eeks
=ar$e stroke: ait 487>3 hours an)=ar$e stroke: ait 487>3
hours an)
re(eat CTre(eat CT
Small stroke: use 9u)$mentSmall stroke: use 9u)$ment
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
27/92
(eparin
+)ere is no large clinical trial in t)e
literature comparing i.. )eparin as
traditionally administered to placebo-nternational %troe +rial:
compared s.q.
)eparin at comparable doses to asa and
neit)er in 1/ patients: result: )eparinas not beneficial
3ancet. 1//4;/:1!/"#1
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
28/92
(eparinoids
+5A%+ trial: indicated no benefit for a
367 )eparinoid in stroe 85'G 101429
%troe. 1//#;2/:2#!
t tana$ement o acute
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
29/92
ana$ement o acuteana$ement o acute
ischemic strokeischemic stroke .ystemic thrombolysis.ystemic
thrombolysis: Intra'enous: Intra'enous
recombinant tissue (lasmino$en acti'atorrecombinant tissue
(lasmino$en acti'ator
.rt7,A: ?ithin hrs o onset o stroke/.rt7,A: ?ithin hrs o onset o
stroke/
Dose 0/; m$k$ ma< ;0 m$/Dose 0/; m$k$ ma< ;0 m$/
Antiplatelet agentsAntiplatelet agents: As(irin "@0700 m$: As(irin
"@0700 m$
ithin 347 48 hrs .not )urin$ frst 34 hrsithin 347 48 hrs .not
)urin$ frst 34 hrs
olloin$ thrombol*tic thera(*/olloin$ thrombol*tic thera(*/
Clo(i)o$rel a (otential alternati'e/Clo(i)o$rel a (otential
alternati'e/Combination o clo(i)o$rel an) as(irinCombination o
clo(i)o$rel an) as(irin
currentl* bein$ e'aluate)currentl* bein$ e'aluate)
ana$ement o acuteana$ement o acute
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
30/92
ana$ement o acuteana$ement o acute
ischemic stroke .cont)/ischemic stroke .cont)/
AnticoagulantsAnticoagulants: He(arin=?H are not: He(arin=?H are
not
recommen)e) in acute treatment o ischemicrecommen)e) in acute
treatment o ischemicstroke/stroke/ 0ecommended in setting
o0ecommended in setting o atrialatrialfbrillationfbrillation- acute
M3 ris*- prosthetic- acute M3 ris*- prosthetic
valves- coagulopathies and orvalves- coagulopathies and
orprevention o D41prevention o D41//
3ntra'arterial thrombolytics3ntra'arterial thrombolytics: An
o(tion or: An o(tion ortreatment o selecte) (atients ith
ma9ortreatment o selecte) (atients ith ma9or
stroke o ! @ hrs )uration )ue to lar$e 'esselstroke o ! @ hrs
)uration )ue to lar$e 'esselocclusion/occlusion/
E M di lC f N l i
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
31/92
Emergency Medical Care for NeurologicEmergencies
Provide reassurance.
Ensure proper airway and breathing.
Place the patient in a position of comfort.
If you suspect stroke, transport immediately andnotify
hospital.
Assess and care for any injuries if you suspect any
type of trauma.
ana$ement o acuteana$ement o acute
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
32/92
ana$ement o acuteana$ement o acute
ischemic stroke .cont)/ischemic stroke .cont)/
5 management5 management: Shoul) be ke(t ithin hi$her: Shoul) be
ke(t ithin hi$hernormal limits since lo , coul) (reci(itatenormal
limits since lo , coul) (reci(itate(erusion ailure/ arke)l*
ele'ate) ,(erusion ailure/ arke)l* ele'ate) ,.B330""0mmH$ mana$e)
ith nitro$l*cerin.B330""0mmH$ mana$e) ith nitro$l*cerincloni)ine
labetalol so)ium nitro(russi)e/ orecloni)ine labetalol so)ium
nitro(russi)e/ ore
a$$ressi'e a((roach is taken i thrombol*tica$$ressi'e a((roach
is taken i thrombol*ticthera(* is institute)thera(* is institute)
5lood glucose management5lood glucose management: Shoul) be ke(t:
Shoul) be ke(t
ithin (h*siolo$ical le'els usin$ oral or Iithin (h*siolo$ical
le'els usin$ oral or I$lucose .in case o h*(o$l*cemiainsulin
.in$lucose .in case o h*(o$l*cemiainsulin .in
case o h*(er$l*cemiacase o h*(er$l*cemia 2levated body
temperature management2levated body temperature management::
Anti(*retics an) use o coolin$ )e'ice canAnti(*retics an) use o
coolin$ )e'ice canim(ro'e the (ro$nosisim(ro'e the (ro$nosis
UDA12 7N MANAG2M2N1 7FUDA12 7N MANAG2M2N1 7F
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
33/92
UDA12 7N MANAG2M2N1 7FUDA12 7N MANAG2M2N1 7F
38/38/ .,ouratian 300.,ouratian 300
Medical interventionsMedical interventions
' 8ardiopulmonary optimi9ation' 8ardiopulmonary optimi9ation
"A58..$"A58..$' 5lood pressure control' 5lood pressure
control
' 38 reduction' 38 reduction
'' UltraUltra''early hemostatic therapyearly hemostatic
therapy
.urgical interventions.urgical interventions
M2D38A: MANAG2M2N1 7F 38/M2D38A: MANAG2M2N1 7F 38/
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
34/92
"ouratian %(()$"ouratian %(()$
8ardiopulmonary optimi9ation " Air#ay- 5reathing-8ardiopulmonary
optimi9ation " Air#ay- 5reathing-
8irculation8irculation
-s*in- sei9ures-s*in- sei9ures
$$
0eversing coagulation deects "coagulopathies and
platelet0eversing coagulation deects "coagulopathies and
plateletdisorders$disorders$
5lood pressure control ":abetolol ; nicardipine 34-5lood
pressure control ":abetolol ; nicardipine 34-nitroprusside not oten
usednitroprusside not oten used brain edema$s nec* in neutral-
patient>s nec* in neutralpositionposition ma?ma?imi9eimi9e
venous out@o#
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
35/92
5:77D 02..U02 MANAG2M2N1 3N 38/5:77D 02..U02 MANAG2M2N1 3N
38/"5roderic* &BBB$"5roderic* &BBB$
' 3 .5 C %)( mm /g or D5 C' 3 .5 C %)( mm /g or D5 C&+( mm
/g on %&+( mm /g on %readings , minutes apartreadings , minutes
apart nitroprusside (
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
36/92
$$hemorrha$ic strokehemorrha$ic stroke
AnalgesicsAntian?ietyAnalgesicsAntian?ietyagentsagents: To
relie'e: To relie'ehea)ache/ Anal$esics ha'in$ se)ati'ehea)ache/
Anal$esics ha'in$ se)ati'e(ro(erties are benefcial or (atients
ha'in$(ro(erties are benefcial or (atients ha'in$sustaine) trauma
.e/$/ mor(hine sul(hatesustaine) trauma .e/$/ mor(hine sul(hate
AntihypertensivesAntihypertensives:.e/$/ so)ium:.e/$/
so)iumnitro(russi)e labetololnitro(russi)e labetolol
/yperosmotic/yperosmoticagentsagents.e/$/ mannitol.e/$/
mannitol
$l*cerol urosemi)e: To re)uce cerebral$l*cerol urosemi)e: To
re)uce cerebrale)ema an) raise) intracranial (ressure/e)ema an)
raise) intracranial (ressure/
AdeHuate hydration is necessaryAdeHuate hydration is necessary
.urgical intervention may occasionally.urgical intervention may
occasionally
be lie savingbe lie saving
0287MM2NDA137N. F7002 MM2NDA13 N F 0.U0G38A: 102A1M2N1 7F
38/.U0G38A: 102A1M2N1 7F 38/
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
37/92
.U0G38A: 102A1M2N1 7F 38/.U0G38A: 102A1M2N1 7F 38/.ro)erick
";;;.ro)erick ";;;
N7N .U0G38A: 8AND3DA12.N7N .U0G38A: 8AND3DA12.&< .mall
hemorrhages "E&( cm)$ or minimal&< .mall hemorrhages
"E&( cm)$ or minimal
neurological defcits
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
38/92
N2U07:7G38N2U07:7G38
D2120370A137N 3N 38/ ":eiraD2120370A137N 3N 38/ ":eira
%((+$%((+$2arly neurologic deterioration "2ND$ occurred in
%%
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
39/92
770 7U187M2 3N 38/
ouratian %(()ouratian %(()
4olume o the hematoma4olume o the hematoma"" )( cc$ )( cc$
Neurologic status "G8. scoreNeurologic status "G8. score $$
3ntraventricular e?tension o the clot3ntraventricular e?tension
o the clot
/ydrocephalus/ydrocephalus
.ubarachnoid e?tension.ubarachnoid e?tension
Anticoagulation agentsAnticoagulation agents
0elative edema0elative edema
Davis L.8 %((+Davis L.8 %((+OO 3nratentorial lesion3nratentorial
lesion
OO 8oronary heart disease8oronary heart disease
OO /yperthermia/yperthermia
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
40/92
Cerebral oedema This is an abnormal accumulation of fluid
in the cerebral parenchyma.It is usually the result of
breakdown of the bloodbrain barrier, and it may occur
following damage initiated by several different
causes:Ischaemia, e.g. from infarction.Trauma,e.g.
from head injury.Inflammation encephalitis or meningitis.
Oveproduction of !" by choroid ple#us neoplasms
$ack
http://c/Documents%20and%20Settings/SpongeBob/My%20Documents/PRESENTASI%20KASUS%20211205%20baru.ppt#Management%20of%20acute%20ischemic%20strokehttp://c/Documents%20and%20Settings/SpongeBob/My%20Documents/PRESENTASI%20KASUS%20211205%20baru.ppt#Management%20of%20acute%20ischemic%20stroke
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
41/92
E)em serebri 'aso$enik meru(akan akibat (rimer )arimenin$katn*a
(ermeabilitas blood brain barier
2dem serebri sitoto*si* terjadi se*under dari *erusa*anelemen
seluler serebri- terlepasnya a*tor'a*tor to*si*dari netrofl dan
ba*teri< .ehingga terjadi pening*atan*andungan air intraseluler-
dimana terjadi *ebocoranpotasium- glu*osa diguna*an melalui
gli*olisis anae
robi*- produ*sila*tatleated blood pressure usually declines
spontaneously oer t)e first 2 )ours after stroe
onset and oer?ealous use of a calcium antagonistand ot)er
anti)ypertensie drugs s)ould be
aoided because t)ey can furt)er reduce cerebral
perfusion.
Antith*(ertensi'eAntith*(ertensi'e
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
63/92
TreatmentTreatment In)icate) or:In)icate) or:
- aortic )issectionaortic )issection- acute m*ocar)ial
inarctionacute m*ocar)ial inarction- heart ailureheart ailure
- acute renal ailureacute renal ailure- h*(ertensi'e
ence(halo(ath*h*(ertensi'e ence(halo(ath*- thrombol*tic
thera(*thrombol*tic thera(*
?hen s*stolic (ressure is "80 mm H$ or?hen s*stolic (ressure is
"80 mm H$ or
hi$her or the )iastolic (ressure "0# mmhi$her or the )iastolic
(ressure "0# mmH$ or hi$her/H$ or hi$her/
*lood 9ressure and hemorrhage
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
64/92
g
Control of eleated blood pressure )asneer been s)on to decrease
t)e ris
of ongoing or recurrent bleeding in
patients it) intracerebral )emorr)age.'ecommend treatment of
moderate and
seere eleations of blood pressure
8systolic blood pressure of greater t)an1#0 mm =g or mean
arterial pressure of
greater t)an 10 mm =g9.
H*(er$l*cemia & StrokeH*(er$l*cemia & Stroke
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
65/92
H*(er$l*cemia & Stroke*( $ *
'ersistent hyperglycemia ()*+ mgd!$'ersistent hyperglycemia ()*+
mgd!$during the frst -* hours ater stroke isduring the frst -*
hours ater stroke is
associated with poor outcomes%associated with poor outcomes%
!ower serum glucose concentrations!ower serum glucose
concentrations
(possibly )*+ to )./ mgd!$ probably(possibly )*+ to )./ mgd!$
probably
should trigger administration o insulin,should trigger
administration o insulin,
similar to the procedure in other acutesimilar to the procedure
in other acute
situations accompanied by hyperglycemiasituations accompanied by
hyperglycemia(Class a, !e"elo #"idence C$%(Class a, !e"elo #"idence
C$%
Close monitorin$Close monitorin$
Tem(eratureTem(erature
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
66/92
Tem(eratureTem(erature
Increase tem( increases (ercenta$eIncrease tem( increases
(ercenta$eo (oor outcome in strokeo (oor outcome in stroke
Increase cerebral o
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
67/92
2ever
+)ere is general agreement to
recommend treatment of t)e sources of
feer and use of antipyretics to control
an eleated body temperature 83eels of
>idence --- t)roug) , Grade C9. +)ere
are insufficient clinical data about t)e
use of )ypot)ermia to recommend t)ist)erapy.
2ever: reatment
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
68/92
2ever: reatment
+reat any temperature eleations
@ata is not in as to )et)er )ypot)ermia
may be protectie
'#R#*RA5 #3#7A
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
69/92
'#R#*RA5 #3#7A
=ypo"osmolar fluids, suc) as
de&trose in ater, may orsen edema.
1(2B% or B% recommended
7annitol
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
70/92
7annitol
6annitol 80.2 to 0. g(g -9 gien oer
20 minutes rapidly loers intracranial
pressure and can be gien eery !
)ours.4+)e usual ma&imum daily dose
is 2 g(g.4
annitolannitol
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
71/92
a o
Dose: 7 3# to #0 $ I/'/ J 7# hrs/Dose: 7 3# to #0 $ I/'/ J 7#
hrs/ a
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
72/92
2vents Ater .tro*e or 13A
1he combination o aspirin plus dipyridamole is moreeective than
aspirin alone in preventing stro*e and
other serious vascular events in patients #ith minorstro*e and
13As< 1he ris* reduction #as greater andstatistically signifcant
or studies using primarily
e?tended release dipyridamole- #hich may re@ect a
truepharmacological eect or lac* o statistical po#er in
studies using immediate release dipyridamole
This meta-analysis systematically reviewed randomized
controlledtrials comparing aspirin plus dipyridamole #ith aspirin
alone inpatients #ith stro*e and 13A to determine the ecacy o
these
agents in preventing recurrent cerebral and systemic vascular
events
0ehabilitation rogram=0ehabilitation rogram=
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
73/92
hysical therapy =hysical therapy = Mobili9ationMobili9ation
Lal*ingLal*ing Major motor or sensory impairment o theMajor motor
or sensory impairment o the
limbslimbs rescription o devices- such as a cane orrescription o
devices- such as a cane or
#al*er#al*er
7ccupational 1herapy =7ccupational 1herapy = Fine movements o
the handFine movements o the hand
Arm unctionArm unction Utili9ation o toolsUtili9ation o tools
Assistive devicesAssistive devices Ability to unction
independentlyAbility to unction independently
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
74/92
American =eart Association. All rig)ts resered.American =eart
Association. All rig)ts resered.
@iagnosis And +reatment 5f @i??iness-n Cerebroascular
@isease
Ab)ul ofr
Knit Stroke 5S Sar)9ito a$ian Ilmu ,en*akit Saraakultas
e)okteran Kni'ersitas a)9ah a)a Lo$*akarta
DiMMinessDiMMiness
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
75/92
,re'alence,re'alence
- " in # a)ults re(ort )iMMiness in last month" in # a)ults
re(ort )iMMiness in last month
- Increases in el)erl*Increases in el)erl*
- ?orsene) b* )ecrease) 'isual acuit*?orsene) b* )ecrease)
'isual acuit*
(ro(rioce(tion an) 'estibular in(ut(ro(rioce(tion an) 'estibular
in(ut DiMMinessDiMMiness
- Gon7s(ecifc termGon7s(ecifc term
- DiNerent meanin$s to )iNerent (eo(leDiNerent meanin$s to
)iNerent (eo(le
Coul) meanCoul) mean
7 erti$oerti$o 7 S*nco(e7 S*nco(e 7 ,res*nco(e7 ,res*nco(e
7 ?eak?eak 7 i))iness7 i))iness 7 An
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
76/92
Cerebroascular @isease
E i) i l C b lE(i)emiolo$* o Cerebro'ascular
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
77/92
E(i)emiolo$* o Cerebro'ascularE(i)emiolo$* o Cerebro'ascular
DiseaseDisease ##00000 stroke sur'i'ors are ali'e to)a*##00000
stroke sur'i'ors are ali'e to)a*
>00000 each *ear>00000 each *ear
- #00000 o these are frst attacks#00000 o these are frst
attacks- 300000 are recurrent attacks/300000 are recurrent
attacks/
0% to #0% o stroke sur'i'ors )o not re$ain0% to #0% o stroke
sur'i'ors )o not re$ain
unctional in)e(en)enceunctional in)e(en)ence
"#% to 0% o all stroke sur'i'ors are"#% to 0% o all stroke
sur'i'ors are
(ermanentl* )isable)(ermanentl* )isable)
I i) C b lI i) C b l
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
78/92
Inci)ence o Cerebro'ascularInci)ence o Cerebro'ascular
DiseaseDisease Increases ith a$eIncreases ith a$e
38% are less than @# *rs ol)38% are less than @# *rs ol)
80% o cerebrob'ascular )isease80% o cerebrob'ascular )isease
are (re'entableare (re'entable
";% $reater in men than omen";% $reater in men than omen
?omen B @# ha'e hi$her inci)ence?omen B @# ha'e hi$her
inci)ence
than menthan men
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
79/92
ertebrobasilar insuOcienc*ertebrobasilar insuOcienc*
DiMMiness )i(lo(ia )*sarthria $aitDiMMiness )i(lo(ia )*sarthria
$ait
ata
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
80/92
American =eart Association. All ri )ts resered.American =eart
Association. All ri )ts resered.
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
81/92
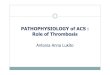
Arise rom the subcla'ianArise rom the subcla'ian
arteriesarteries
5un alon$si)e the5un alon$si)e the
me)ullame)ulla loo) su((l* orloo) su((l* or
brainstem an) cerebellumbrainstem an) cerebellum
e* unctional Areas:e* unctional Areas:
T S(inal cor) tracts7(*rami)alS(inal cor) tracts7(*rami)al
an) s(inothalamican) s(inothalamicT Cranial ner'es 7"3Cranial
ner'es 7"3
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
82/92
"7 ,osterior Cerebral"7 ,osterior Cerebral
37 Su(erior Cerebellar37 Su(erior Cerebellar
7 ,ontine ranches o7 ,ontine ranches o
asilarasilar
47 Anterior Inerior Cerebellar47 Anterior Inerior Cerebellar
#7 Internal Au)itor*#7 Internal Au)itor*
@7 ertebral@7 ertebral
>7 ,osterior Inerior>7 ,osterior Inerior
CerebellarCerebellar87 Anterior S(inal87 Anterior S(inal
;7 asilar;7 asilar
DiMMinessDiMMiness
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
83/92
,eri(heral causes,eri(heral causes
- canalithiasis .,,7#0%canalithiasis .,,7#0%
- 'estibular neuronitis'estibular
neuronitis.lab*rinthitis73#%.lab*rinthitis73#%
- enierePs )isease7"0%enierePs )isease7"0%
- traumatrauma
- )ru$s .amino$l*cosi)es)ru$s .amino$l*cosi)es
Central causesCentral causes
- Cerebro'ascular )iseaseCerebro'ascular )isease
.'ertebrobasilar insuOcienc*7#0.'ertebrobasilar insuOcienc*7#0-
)em*elinatin$ .multi(le sclerosis)em*elinatin$ .multi(le
sclerosis
- )ru$s .anticon'ulsants alcohol)ru$s .anticon'ulsants
alcohol
h*(noticsh*(notics
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
84/92
erti$o 's/ other t*(es oerti$o 's/ other t*(es
o)iMMiness)iMMiness
TimeTimecoursecourse77 'erti$o is ne'er continuous77 'erti$o is
ne'er continuous
,ro'okin$,ro'okin$actorsactors77 s(ontaneousl* or ith77
s(ontaneousl* or ith(ositional chan$es(ositional chan$es
A$$ra'atin$A$$ra'atin$actorsactors77 all 'erti$o is ma)e77 all
'erti$o is ma)eorse b* mo'in$ the hea)orse b* mo'in$ the hea)
E t bli hi th E t bli hi th
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
85/92
Establishin$ the cause oEstablishin$ the cause o
)iMMiness)iMMinessTime courseTime course
- ,,: lasts less than one minute sel7limite),,: lasts less than
one minute sel7limite)
res(on)s (oorl* to anti7'erti$o )ru$sres(on)s (oorl* to
anti7'erti$o )ru$s
- ascular: sin$le e(iso)e lastin$ minutes toascular: sin$le
e(iso)e lastin$ minutes to
hoursQ usuall* )ue to mi$raine or to transienthoursQ usuall* )ue
to mi$raine or to transient
ischemia o the lab*rinth or brainstemQischemia o the lab*rinth
or brainstemQ
occasionall* enierePs )iseaseoccasionall* enierePs )isease
- 5ecent onset o more (rolon$e) e(iso)es5ecent onset o more
(rolon$e) e(iso)escharacteristic o 'estibular neuronitis
multi(lecharacteristic o 'estibular neuronitis multi(le
sclerosis 'ertebrobasilar ischemiasclerosis 'ertebrobasilar
ischemia
E t bli hi th E t bli hi th
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
86/92
Establishin$ the cause oEstablishin$ the cause o
)iMMiness)iMMiness
Associate) s*m(tomsAssociate) s*m(toms
- ertebrobasilar )isease stroke: )i(lo(iaertebrobasilar )isease
stroke: )i(lo(ia)*sarthria )*s(ha$ia eakness numbness)*sarthria
)*s(ha$ia eakness numbness
- enierePs )isease: aural ullness )eanessenierePs )isease: aural
ullness )eaness
tinnitustinnitus
- ,s*ch,anic attack: S+ (al(itations,s*ch,anic attack: S+
(al(itations)ia(horesis)ia(horesis
- ulti(le sclerosis: 'erti$o (rece)e) b* otherulti(le sclerosis:
'erti$o (rece)e) b* other
neurolo$ic )*sunctionneurolo$ic )*sunction
Establishin$ the cause oEstablishin$ the cause o
)iMMiness)iMMiness
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
87/92
)iMMiness)iMMiness
,rior risk actors,rior risk actors
- i$rainei$raine
- H*(ertension Diabetes ellitusH*(ertension Diabetes ellitus
smokin$ ,eri(heral ascular Diseasesmokin$ ,eri(heral ascular
Disease
- Hea) in9ur*Hea) in9ur*
- ,s*chiatric illness,s*chiatric illness
,h*sical e
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
88/92
estibular e
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
89/92
urther stu)ies to e'aluateurther stu)ies to e'aluate
)iMMiness)iMMiness 5I5A5I5A 77 )istin$uishin$ central causes77
)istin$uishin$ central causes
TCDTCD Au)iometr*Au)iometr* 77 )istin$uishin$ (eri(heral77
)istin$uishin$ (eri(heral
causescauses
- rainstem e'oke) au)iometr*rainstem e'oke) au)iometr* 77
;07;#%77 ;07;#%sensiti'it* or )etectin$ acoustic neuromasensiti'it*
or )etectin$ acoustic neuroma
Transient Ischaemic AttackTransient Ischaemic Attack
.TIA mana$ement.TIA mana$ement
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
90/92
$ The risk o stroke (ost TIA is hi$himme)iatel* ater an e'entQ
u( to #%in the frst 3 )a*s an) "0% ithin the
frst eek
$ Those at hi$h risk can be
)iscriminate) rom those at lo riskb* means o clinical assessment
.the
ACD3 score/
ContRR//ContRR//
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
91/92
$ The ACD3 scale is a >7(oint scalebase) on clinical )ata
a'ailable
beore neuroima$in$ hich can beuse) to estimate the risk o
stroke
ater TIA
0ohnston et al, !ancet -++1
ana$ement o TIAana$ement o TIA
-
7/24/2019 Patophysiology and Management of Stroke-Okt2014
92/92
E'aluation ithin hours ater onsetE'aluation ithin hours ater
onseto s*m(tomso s*m(toms
CT scan is necessar* in all (atientsCT scan is necessar* in all
(atients
Anti(latelet thera(* ith as(irin .#07Anti(latelet thera(* ith
as(irin .#073# m$) consi)er use o3# m$) consi)er use oclo(i)o$rel
ticlo(i)ine or as(irin7clo(i)o$rel ticlo(i)ine or
as(irin7)i(*ri)amole in (atients ho are)i(*ri)amole in (atients ho
are
intolerant to as(irin or those hointolerant to as(irin or those
hoe