Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 8 , N O . 1 0 , 2 0 1 6
ª 2 0 1 6 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 5 . 0 8 6
REVIEW TOPIC OF THE WEEK
PCI Strategies in Patients WithST-Segment Elevation MyocardialInfarction and MultivesselCoronary Artery Disease
Eric R. Bates, MD,a Jacqueline E. Tamis-Holland, MD,b John A. Bittl, MD,c Patrick T. O’Gara, MD,dGlenn N. Levine, MDe
ABSTRACT
Fro
ArcM
Int
Me
to
Ma
Recent randomized controlled trials have suggested that patients with ST-segment elevation myocardial infarction and
multivessel coronary artery disease may benefit more from multivessel percutaneous coronary intervention (PCI)
compared with culprit vessel-only primary PCI. The American College of Cardiology, American Heart Association, and
Society for Cardiovascular Angiography and Interventions recently published an updated recommendation on this topic.
The purpose of this State-of-the-Art Review is to accurately document existing published reports, describe their limi-
tations, and establish a base for future studies. (J Am Coll Cardiol 2016;68:1066–81)
© 2016 by the American College of Cardiology Foundation.
A pproximately 50% of patients with ST-segment elevation myocardial infarction(STEMI) have multivessel (MV) coronary ar-
tery disease (CAD) (1). The short-term prognosis afterSTEMI is worse with MV CAD than with single-vesselCAD (2–4), perhaps because of additional plaqueinstability (5,6); impaired myocardial perfusioncaused by endothelial dysfunction, microvascularspasm, or inflammation (7); or decreased contractilityin noninfarct zones (2,8). The long-term prognosis isalso worse because of older age, more atheroscleroticrisk factors, higher atherosclerotic disease burden,and lower left ventricular ejection fraction in patientswith MV CAD (9).
The 2011 American College of Cardiology Founda-tion (ACCF)/American Heart Association (AHA)/Society for Cardiac Angiography and Interventions
m the aDivision of Cardiovascular Diseases, Department of Internal Me
bor, Michigan; bDivision of Cardiology, Department of Internal Medicine, M
unroe Heart and Vascular Institute, Munroe Regional Medical Center, Oca
ernal Medicine, Brigham and Women’s Hospital, Boston, Massachusetts;
dical Center, Baylor College of Medicine, Houston, Texas. The authors ha
the contents of this paper to disclose.
nuscript received March 3, 2016; revised manuscript received April 19, 20
(SCAI) guideline for percutaneous coronary inter-vention (PCI) and the 2013 ACCF/AHA guideline forSTEMI recommended that primary PCI should not beperformed (Class III, Harm) in a noninfarct artery inpatients with STEMI who are hemodynamically stable(10,11). Additionally, the American College of Cardi-ology (ACC) Appropriate Use Criteria Task Forcelabeled PCI of a noninfarct artery at the time ofprimary PCI as “inappropriate” (12). These recom-mendations arose from historical safety concernsthat included an increased potential for proceduralcomplications, contrast nephropathy, and stentthrombosis. However, more complete acute revascu-larization in patients with STEMI may be safer in thecurrent era due to advances in stent technology andantiplatelet therapy; might decrease mortality, rein-farction, and repeat revascularization rates; and
dicine, University of Michigan Medical Center, Ann
ount Sinai St. Luke’s Hospital, New York, New York;
la, Florida; dCardiovascular Division, Department of
and the eSection of Cardiology, Michael E. DeBakey
ve reported that they have no relationships relevant
16, accepted May 10, 2016.

AB BR E V I A T I O N S
AND ACRONYM S
ACC = American College of
Cardiology
ACCF = American College of
Cardiology Foundation
AHA = American Heart
Association
BCI = Bayesian confidence
interval
CAD = coronary artery disease
CI = confidence interval
CVO = culprit-vessel only
ESC = European Society of
Cardiology
FFR = fractional flow reserve
MACE = major adverse
cardiovascular event(s)
MV = multivessel
OR = odds ratio
PCI = percutaneous coronary
intervention
SCAI = Society for
Cardiovascular Angiography
and Interventions
STEMI = ST-segment elevation
myocardial infarction
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1067
could reduce hospital length of stay, resource utili-zation, and cost. In fact, several recent randomizedcontrolled trials and meta-analyses have supportedthis strategy (see later discussion). In response tothese reports, the ACC removed the 2012 proscriptionagainst MV primary PCI from the American Board ofInternal Medicine Foundation Choosing WiselyCampaign in 2014 (13). Additionally, the 2014 Euro-pean Society of Cardiology (ESC)/European Associa-tion for Cardio-Thoracic Surgery (EACTS) Guidelineson Myocardial Revascularization and the 2015 ACC/AHA/SCAI Focused Update on Primary PCI committeeassigned a new Class IIb recommendation,concluding that MV primary PCI may be considered inselected hemodynamically stable patients with sig-nificant noninfarct artery stenoses (14,15).
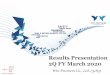
Nevertheless, the best strategy for the treatment ofthe noninfarct artery in patients with STEMI and MVCAD remains an unresolved issue, with importantimplications for potentially improving clinical out-comes in these patients. PCI strategies include: 1)culprit vessel-only (CVO) primary PCI with continuedmedical management and PCI of noninfarct arteriesonly for spontaneous angina or myocardial ischemiaon stress testing; 2) MV PCI at the time of primary PCI;or 3) CVO primary PCI, followed by staged PCI ofnoninfarct arteries later during the index hospitali-zation or soon after hospital discharge (CentralIllustration). This review summarizes the data on PCIfor patients with STEMI and MV CAD (15).
The terms preventive angioplasty (16) and completerevascularization (17–20) have previously been usedto describe what we are presently naming MV primaryPCI and staged PCI. We prefer these terms becausethe term preventive has traditionally been used todescribe noninvasive interventions that attempt toprevent invasive interventions or major adversecardiovascular events (MACE), and because completerevascularization was not routinely attempted in pa-tients with chronic total occlusions, other complexlesions, or smaller arteries.
METHODS
A search of the published reports was performed us-ing the PubMed database through December 2015. Weincluded in our analysis previously published reportsthat were cited in previous publications andany additional studies that were independentlyidentified. When possible, we excluded patients withnon–ST-segment elevation myocardial infarction,hemodynamic instability, prior fibrinolytic therapy,and prior coronary artery bypass surgery. We docu-mented study design and enrollment periods,
primary endpoints, and quantitative mortal-ity results; and separated MV primary PCI andstaged PCI results. Qualitative results forMACE, reinfarction, and repeat revasculari-zation were tabulated because the studieswere too heterogeneous to permit an accuratequantitative analysis. Twelve reports wereexcluded from this analysis: 4 included pa-tients with non–ST-segment elevation acutecoronary syndromes (21–24); 3 did not sepa-rate MV primary PCI from staged PCI (25–27);2 compared complete versus incompleterevascularization (28,29); 2 studied patientswith heart failure and cardiogenic shock(30,31); and 1 compared MV primary PCI withsingle-vessel primary PCI (32).
To illustrate the relative effectiveness ofCVO versus MV PCI, we used conventionalstatistical methods to create forest plots toillustrate differences in mortality rates, arelevant endpoint reported in all trialscomparing primary PCI strategies in patientswith STEMI and MV CAD. We applied arandom effects model to acknowledge thevariation in study design, treatment dura-tion, and length of follow-up among thestudies. For inductive inference and to
emulate the random effects model, we used hierar-chical Bayesian meta-analysis. In the absence ofstrong evidence for the superiority of 1 strategy overanother, we used noninformative priors defined by atreatment effect of 0.00 and precision of 0.0001 toensure that the posterior inference would be domi-nated by the likelihood of the data (33,34). All ana-lyses were intention-to-treat. Standard meta-analysiswas performed using the open-source statistical pro-gram R 3.0.2 and the library package meta 3.8-0 (35).Bayesian computations were run with the open-source program OpenBUGS 3.2.3 (Open BayesianInference Using Gibbs Sampling), using Markov chainMonte Carlo modeling (34,36), linked to R with BRugs(37).CVO VERSUS MV PRIMARY PCI. We identified 6single-center (38–43), 8 multicenter (44–51), and 3case-controlled (52–54) observational reports thatcompared CVO versus MV primary PCI (Table 1). Ingeneral, in the current era with new-generation stentimplantation and dual antiplatelet therapy, thereappeared to be no increased risk for reinfarction whenasymptomatic periprocedural myocardial biomarkerelevations were not counted as events. The risk forrepeat revascularization was inconsistently lowerwith MV primary PCI in these studies, but was never

CENTRAL ILLUSTRATION PCI Strategies in Patients With STEMI and MV Disease: CVO Primary PCI Versus MV PCI
Strategies
Initial procedure
Days−weeks later
Culprit vessel-only primary PCI
Culprit vessel-only PCI Culprit vessel PCIand non-culprit vessel PCI
Non-culprit vessel PCIfor spontaneous ischemia
or intermediate/high risk findingson noninvasive testing
Non-culprit vessel PCI
Culprit vessel-only PCI
Multivessel primary PCI Staged PCI
Pros
Reduced contrast volumeReduced risk of
PCI complications
Decreased repeatrevascularization
Decreased hospital length of stay
Time to assess benefit vs. riskof non-culprit vessel PCI
Increased repeatrevascularization risk
Potential reduction in LV recovery
Prolonged procedure timeIncreased contrast volume
Increased periprocedural MI riskPotentially unnecessary PCI of
functionally insignificant stenosis
Additional PCI access riskAdditional procedure costsCons
Bates, E.R. et al. J Am Coll Cardiol. 2016;68(10):1066–81.
Patients with ST-segment elevation myocardial infarction (STEMI) and multivessel (MV) coronary artery disease may undergo percutaneous coronary intervention (PCI)
using 1 of 3 strategies: 1) culprit vessel–only (CVO) primary PCI; 2) primary PCI followed by MV intervention of additional noninfarct lesions at the time of the primary
procedure; or 3) CVO primary PCI followed by staged PCI of noninfarct lesions later during the index hospitalization or after hospital discharge. Advantages and dis-
advantages of each strategy are illustrated. LV ¼ left ventricular.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1068
contrasted with the total number of additional non-infarct artery PCI procedures performed initiallyto obtain that result. We observed a nonsignificantreduction in long-term mortality with CVO comparedwith MV primary PCI using both traditional statisticalapproaches (odds ratio [OR]: 0.83; 95% confidenceinterval [CI]: 0.62 to 1.09) and Bayesian approaches(posterior median OR: 0.83; 95% Bayesian confidenceinterval [BCI]: 0.59 to 1.15) (Figure 1).
Four randomized trials (16–19) compared CVO toMV primary PCI (Table 2). MACE, reinfarction, andrepeat revascularization rates were lower with MVprimary PCI. We observed a nonsignificant increasein long-term mortality with CVO compared with MVprimary PCI using both traditional statistical ap-proaches (OR: 1.69; 95% CI: 0.98 to 2.89) and Bayesianapproaches (OR: 1.66; 95% BCI: 0.84 to 3.28)(Figure 2).
The HELP-AMI (Hepacoat for Culprit or MultivesselStenting for Acute Myocardial Infarction) trial ran-domized 69 patients in a 3:1 ratio to MV or CVO pri-mary PCI (17). There was a nonsignificant reductionin repeat revascularization with MV primary PCI
(17% vs. 35%), but no differences in death or rein-farction rates.
Politi et al. (18) randomized 214 patients to CVOprimary PCI, MV primary PCI, or staged PCI. Again,repeat revascularization rates were lower with MVprimary PCI, but there were no differences in death orreinfarction rates.
The PRAMI (Preventive Angioplasty in AcuteMyocardial Infarction) trial screened 1,922 patientsand enrolled 465 patients at 5 sites over 5 years (16).Recruitment was stopped prematurely by the datasafety and monitoring board with a mean follow-up of23 months due to significant differences betweengroups. The sample size was on the basis of an ex-pected annual MACE rate of 20% for CVO primary PCIand a 30% risk reduction for MV primary PCI at 80%power. Thirteen patients did not receive assignedtherapy, and 18 were lost to follow-up. The compositeprimary outcome of cardiac death, nonfatal reinfarc-tion, or refractory angina occurred in 21 (9%) patientstreated with MV primary PCI compared with 53 (22%)patients treated with CVO primary PCI (hazard ratio[HR]: 0.35; 95% CI: 0.21 to 0.58; p < 0.001). There

TABLE 1 Observational Trials of CVO Versus MV Primary PCI
First Author (Ref. #)Year Design CVO MV
PrimaryEndpoint
Follow-Up(Months)
Mortality,n (%)
Outcomes forMV
Roe (52)2001
Case-controlledMulticenter1995–1999
61 68 D, MI, revasc 6 CVO: 10 (16)MV: 17 (25)
MACE, MI, revasc similarMortality similar
Corpus (38)2004
RegistrySingle-center1998–2002
354 26 D, MI, revasc 12 CVO: 42 (12)MV: 5 (19)
MACE, MI, revasc similarMortality similar
Khattab (39)2008
Sequential cohortSingle-center2004–2005
45 28 D, MI, revasc 12 CVO: 3 (7)MV: 2 (8)
MACE, MI, revasc similarMortality similar
Qarawani (40)2008
RetrospectiveSingle-center2001–2004
25 95 D, MI, CHF, ischemia 12 CVO: 2 (8)MV: 9 (9.4)
MACE, MI, revasc lowerMortality similar
Varani (41)2008
RegistrySingle-center2004–2007
156 147 Mortality 1 CVO: 10 (6.6)MV: 15 (9.9)
Mortality similar
Cavender (44)2009
RegistryMulticenter2004–2007
23,146 2,701 Mortality In-hospital CVO: 586 (2.5)MV: 88 (3.3)
MACE similarMortality similar*
Hannan (53)2010
Case-controlledMulticenter2003–2006
458 458 Mortality 42 CVO: 31 (6.7)MV: 48 (10.4)
Mortality similar
Toma (45)2010
SubgroupMulticenter2004–2007
1,984 217 Mortality 3 CVO: 111 (5.6)MV: 27 (12.5)
Mortality higher
Dziewierz (46)2010
RegistryMulticenter2005–2007
707 70 Mortality 12 CVO: 57 (8.1)MV: 11 (15.7)
Mortality similar*
Mohamad (42)2011
RetrospectiveSingle-center2002–2006
30 7 Mortality 12 CVO: 3 (10)MV: 2 (28.6)
MACE similarMortality similar
Bauer (47)2013
RegistryMulticenter2005–2008
2,118 419 Mortality In-hospital CVO: 72 (3.4)MV: 6 (1.4)
MI higherMortality similar*
Jaguszewski (48)2013
RegistryMulticenter2005–2012
3,833 1,108 Mortality In-hospital CVO: 68 (4.4)MV: 81 (7.3)
MI similarMortality similar*
Santos (49)2014
RegistryMulticenter2010–2011
180 77 Mortality In-hospital CVO: 14 (7.8)MV: 2 (2.6)
MI similarMortality similar*
Jeger (50)2014
RegistryMulticenter2005–2012
1,467 442 Mortality 12 CVO: 40 (2.7)MV: 12 (2.7)
MI similarRevasc lowerMortality similar
Kim (43)2014
RegistrySingle-center2006–2009
155 67 D, MI, revasc 36 CVO: 15 (9.7)MV: 5 (7.4)
MACE, MI, revasc similarMortality similar
Manari (51)2014
RegistryMulticenter2002–2010
706 367 D, MI, TVR 24 CVO: 127 (18.0)MV: 26 (7.1)
MI, MACE lowerRevasc similarMortality lower
Iqbal (54)2014
Case-controlledMulticenter2004–2011
2,418 403 Mortality 12 CVO: 164 (6.8)MV: 41 (10.2)
MACE (in-hospital) higherMortality higher*
*Adjusted mortality rates.
CHF ¼ congestive heart failure; CVO ¼ culprit vessel-only; D ¼ death; MACE ¼ major adverse cardiovascular events; MI ¼ myocardial infarction; MV ¼ multivessel; PCI ¼percutaneous coronary intervention; revasc ¼ repeat revascularization; TVR ¼ target vessel revascularization.
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1069
were statistically significant reductions in the com-posite of death and myocardial infarction, and in re-fractory angina and repeat revascularization rates infavor of MV primary PCI.
The CvLPRIT (Complete Versus Culprit-LesionOnly Primary PCI) trial screened 850 patients andenrolled 296 patients at 7 sites over 2 years (19).The sample size was calculated on the basis of an
expected MACE rate of 37% for CVO primary PCI and22% for MV PCI at 80% power. Eighteen patientscrossed over, and 19 were lost to follow-up. MV pri-mary PCI was performed in 97 patients, and stagedPCI was performed in 42 patients. The compositeprimary outcome of all-cause death, reinfarction,heart failure, and ischemia-driven revascularizationat 12 months occurred in 15 (10%) patients with

FIGURE 1 Forest Plot of Mortality in Observational Studies Comparing CVO With MV Primary PCI
Study
Fixed effect modelRandom effects modelHeterogeneity: I−squared=76.6%, tau−squared=0.1929, p<0.0001
Roe (2001)Corpus (2004)Qarawani (2008)Khattab (2008)Varani (2008)Cavender (2009)Hannan (2010)Toma (2010)Dziewierz (2010)Mohamad (2011)Bauer (2013)Jaguszewski (2013)Santos (2014)Jeger (2014)Kim (2014)Manari (2014)Iqbal (2014)
Events
2214
13 42 2 3 8
1321 54 111 57 3
72 168 14
40 15
127 164
Total
40562
79 354 25 45 156
25802 503
1984 707 30
2118 3833 180 1467 155
706 2418
CULPRIT MULTIVESSELEvents
565
19 5 9 2 12
246 59 27 11 2 6 81 2 12 5
26 41
Total
7189
79 26 95 28 147
3134 503 217 70 7
4191108
77 442 67
367 403
0.1 0.2 0.5 1 5 10
Odds Ratio (OR)
CVO Better
OR
0.750.83
0.620.570.830.930.610.630.910.420.470.282.420.583.161.001.332.880.64
95%−CI
[0.67; 0.82][0.62; 1.09]
[0.28; 1.37][0.20; 1.58][0.17; 4.11][0.15; 5.93][0.24; 1.53][0.55; 0.73][0.61; 1.34][0.27; 0.65][0.23; 0.95][0.04; 2.11][1.05; 5.61][0.44; 0.76][0.70; 14.27][0.52; 1.93][0.46; 3.82][1.85; 4.48][0.45; 0.92]
Bayesian hierarchical meta-analysis 0.83 [0.59; 1.15]
2MV Better
Mortality rates at longest follow-up are obtained from the studies described in Table 1 comparing culprit vessel–only (CVO) to multivessel (MV)
coronary intervention in patients with ST-segment elevation myocardial infarction (STEMI) and MV coronary artery disease (CAD). CI ¼ con-
fidence interval.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1070
MV PCI compared with 31 (21%) patients with CVOprimary PCI (HR: 0.45; 95% CI: 0.24 to 0.84;p ¼ 0.009). There were no statistically significantdifferences in death, reinfarction, heart failure, orrepeat revascularization rates, although the trendsfavored MV PCI.
TABLE 2 Randomized Controlled Trials of CVO Versus MV Primary PC
First Author (Ref. #)Year Design
CVO(n)
MV(n)
PrimaryEndpoint
Di Mario (17)2004
Randomizedmulticenter2004
17 52 Revasc
Politi (18)2010
Randomizedsingle-center2003–2007
84 65* Death, MI, rehosfor ACS, reva
Wald (16)2013
Randomizedmulticenter2008–2013
231 234 CV death,MI,refractory an
Gershlick (19)2015
Randomizedmulticenter2011–2013
146 150† Death, MI, HF, re
Pooled 478 501
*Excludes 65 patients randomized to staged PCI. †Includes 42 patients who underwent
ACS ¼ acute coronary syndrome; CV ¼ cardiovascular; HF ¼ heart failure; rehosp ¼ r
It should be noted that 2 of the randomized trialsthat tested CVO versus MV primary PCI includedpatients with staged PCI (18,19), with the resultsoften included as MV primary PCI in meta-analyses.Four other randomized trials have tested CVO pri-mary PCI versus staged PCI (20,55–58), with 2 using
I
Follow-Up(Months)
Mortality(n)
CV Death(n)
MI(n)
Revasc(n)
12 0 vs. 1 0 vs. 1 1 vs. 1 6 vs. 9
psc
30, mean 13 vs. 6 10 vs. 4 7 vs. 2 28 vs. 6
gina
23, mean 16 vs. 12 10 vs. 4 20 vs. 7 46 vs. 16
vasc 12 10 vs. 4 7 vs. 2 4 vs. 2 16 vs. 8
39 vs. 23 27 vs. 11 32 vs. 12 96 vs. 39
staged PCI.
ehospitalization; other abbreviations as in Table 1.

FIGURE 2 Forest Plot of Mortality in Randomized Controlled Trials Comparing CVO With MV Primary PCI
Study
Fixed effect modelRandom effects modelHeterogeneity: I−squared=0%, tau−squared=0, p=0.8056
Di Mario (2004)Politi (2010)Wald (2013)Gershlick (2014)
Events
39
0131610
Total
478
17 84231146
CULPRITEvents
23
1 612 4
Total
501
52 65
234150
0.1 0.2 0.5 1 5 10
Odds Ratio (OR)
CVO Better
OR
1.701.69
0.981.801.382.68
95%−CI
[1.00; 2.91][0.98; 2.89]
[0.04; 25.20][0.64; 5.03][0.64; 2.98][0.82; 8.76]
Bayesian hierarchical meta-analysis 1.66
MULTIVESSEL
[0.84; 3.28]
2MV Better
Mortality rates at longest follow-up are obtained from trials described in Table 2 comparing CVO with MV and noninfarct coronary intervention
in patients with STEMI and MV CAD. Abbreviations as in Figure 1.
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1071
fractional flow reserve (FFR) measurements to guiderevascularization decisions (20,55,56) (Table 3).Additionally, 2 small, randomized trials havecompared MV primary PCI with staged PCI (59,60).
TABLE 3 Randomized Controlled Trials of Staged PCI Versus CVO or
First Author (Ref. #)Year Design
Staged PCI(n)
CVO(n)
MV(n)
TiSta
Staged PCI vs. CVO primary PCI
Politi (18)2010
RandomizedSingle-center2003–2007
65 84 — 57 d
Ghani (56)2012
Randomizedsingle-center2004–2007
80 41 — <3
Engstrøm (20)2015
RandomizedMulticenter2011–2014
314 313 — 2
Hlinomaz (57)2015
RandomizedMulticenter2009–2013
106 108 — 3–4
Henriques (58)2015
RandomizedMulticenter2008–2015
148 154 — <
Pooled 715 700
Staged PCI vs. MV primary PCI
Ochala (59)2004
RandomizedSingle-centerN/A
44 — 48 27 d
Politi (18)2010
RandomizedSingle-center2003–2007
65 — 65 57 d
Tarasov (60)2014
RandomizedSingle-center2011–2013
43 — 46 8 da
Pooled 152 159
*Included 5 periprocedural MI.
IRA ¼ infarct-related artery; LVED ¼ left ventricular end-diastolic diameter; LVEF ¼ l
The ACC/AHA/SCAI Focused Update recommendationdoes not distinguish between MV primary PCI andstaged PCI, but rather gives 1 recommendation for MVPCI (15).
MV Primary PCI
ming ofged PCI
PrimaryEndpoint
Follow-Up(Months)
Mortality(n)
CV Death(n)
MI(n)
Revasc(n)
ays, mean Death, MI, rehospfor ACS, revasc
30, mean 4 vs. 13 12 vs. 10 4 vs. 7 8 vs. 28
weeks LVEF 36 4 vs. 0 N/A 14* vs. 0 27 vs. 14
days D, MI, non-IRArevasc
27, mean 15 vs. 11 5 vs. 9 15 vs. 16 17 vs. 52
0 days D, MI, stroke 38, mean 6 vs. 7 N/A 11 vs. 8 N/A
7 days LVEF, LVED 4 4 vs. 0 4 vs. 0 5 vs. 3 0 vs. 1
33 vs. 31 21 vs. 19 49 vs. 34 52 vs. 95
ays, mean LVEF 6 0 vs. 0 0 vs. 0 4 vs. 3 10 vs. 12
ays, mean Death, MI, rehospfor ACS, revasc
30, mean 4 vs. 6 2 vs. 4 4 vs. 2 8 vs. 6
ys, mean D, MI, revasc 6 1 vs. 0 N/A 0 vs. 3 0 vs. 2
5 vs. 6 2 vs. 4 8 vs. 8 18 vs. 20
eft ventricular ejection fraction; N/A ¼ not available; other abbreviations as in Tables 1 and 2.

TABLE 4 Observational Trials of CVO Primary PCI Versus Staged PCI
First Author (Ref. #)Year Design
CVO(n)
Staged PCI(n)
Timing ofStaged PCI
PrimaryEndpoint
Follow-Up(Months)
Mortalityn (%)
Outcomes forStaged PCI
Corpus (38)2004
RegistrySingle-center1998–2002
354 126 In-hospital D, MI, revasc 12 CVO: 42 (12)Staged: 12 (9.5)
MACE, MI, revasc higherMortality similar
Rigattieri (61)2008
RetrospectiveSingle-center2004–2006
46 64 In-hospital D, stroke, stentthrombosis,
Revasc,ACS hosp
13, mean CVO: 7 (15.2)Staged: 1 (1.5)
MACE similarPeriprocedural MI higherMortality lower
Varani (41)2008
RegistrySingle-center2004–2007
156 96 In-hospital Mortality 1 CVO: 10 (6.6)Staged: 2 (2.1)
Mortality similar
Han (62)2008
RetrospectiveSingle-centerN/A
149 93 7–15 days Cardiac D, MI, TVR 12 CVO: 4 (2.7)Staged: 3 (3.2)
MACE, revasc similarMortality similar
Hannan (53)2010
Case-controlledMulticenter2003–2006
538 538 <60 days Mortality 42 CVO: 40 (7.4)Staged: 30 (5.6)
Mortality similar
Chen (63)2010
RegistrySingle-center2002–2009
351 60150
<1 month1–6 months
Mortality 12 CVO: 66 (18.8)Staged: 13 (6.2)
Mortality lower
Mohamad (42)2011
RetrospectiveSingle-center2002–2006
30 12 In-hospital Mortality 12 CVO: 3 (10)Staged: 2 (16.7)
MACE similarMortality similar
Barringhaus (66)2011
RegistryMulticenter1999–2007
1,345 173130
In-hospitalOutpatient
Mortality 6 CVO: 106 (7.9)Staged: 4 (2)
Periprocedural MI higherMortality lower
Lee (67)2012
RegistryMulticenter2005–2007
1,106 538 In-hospital D, MI, revasc 12 CVO: 25 (2.3)Staged: 9 (1.7)
MACE, MI, revasc similarMortality similar
Kim (43)2014
RegistrySingle-center2006–2009
155 252 In-hospital D, MI, revasc 36 CVO: 15 (9.7)Staged: 11 (4.4)
MACE lowerMI, revasc similarMortality similar
Manari (51)2014
RegistryMulticenter2002–2010
706 988 <60 days D, MI, TVR 24 N/A MACE, MI lowerRevasc similarMortality lower
Ma (64)2015
RegistrySingle-center2008–2011
246 201 7 days D, MACE 55 CVO: 41 (16.7)Staged: 13 (6.5)
MACE, MI, revasc lowerMortality lower
Russo (65)2015
RegistrySingle-center2004–2011
779 259 In-hospital Mortality 6 CVO: 38 (5.0)Staged: 2 (0.8)
Mortality lower
Toyota (68)2016
RegistryMulticenter2005–2007
630 681 <90 days Mortality 60 CVO: 95 (16.0)Staged: 59 (9.5)
MI, revasc similarMortality lower
hosp ¼ hospitalization; other abbreviations as in Tables 1 and 3.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1072
CVO PRIMARY PCI VERSUS STAGED PCI. We identi-fied 9 single-center (38,41–43,61–65), 4 multicenter(51,66–68), 1 case-controlled (53), and 5 randomizedtrial (18,20,55–58) reports that compared CVO primaryPCI versus staged PCI (Tables 3 and 4). Similar to theresults comparing CVO with MV primary PCI, therewere no obvious differences in reinfarction or repeatrevascularization rates. In the 13 observationalstudies, we observed a significant increase in long-term mortality with CVO primary PCI compared withstaged PCI using traditional statistical approaches(OR: 2.18; 95% CI: 1.58 to 3.01) and Bayesian ap-proaches (OR: 2.09; 95% BCI: 1.54 to 2.88) (Figure 3).In 5 randomized trials, mortality rates with CVO pri-mary PCI were no different than staged PCI using
traditional statistical methods (OR: 0.92; 95% CI: 0.40to 2.12) and Bayesian approaches (OR: 0.94; 95% BCI:0.31 to 2.09) (Figure 4).
The DANAMI 3-PRIMULTI (Third Danish Study ofOptimal Acute Treatment of Patients with STEMI:Primary PCI in Multivessel Disease) trial screened2,212 patients and randomized 627 patients to CVOprimary PCI or FFR-guided staged revascularizationbefore hospital discharge at 4 sites over 4 years (20).The sample size was calculated on the basis of anexpected annual MACE rate of 18% for CVO primaryPCI and a predicted 30% risk reduction for FFR-guided staged PCI at 80% power. In the staged PCIgroup, 97 patients did not undergo PCI because FFRvalues were >0.80, 6 were referred for coronary

FIGURE 3 Forest Plot of Mortality in Observational Studies Comparing CVO Primary PCI With Staged PCI
Study
Fixed effect modelRandom effects modelHeterogeneity: I−squared=50.1%, tau−squared=0.1466, p=0.02
Corpus (2004)Rigattieri (2008)Varani (2008)Han (2008)Hannan (2010)Chen (2010)Mohamad (2011)Barringhaus (2011)Lee (2012)Kim (2014)Ma (2015)Russo (2015)Toyota (2016)
Events
492
42 7
10 4
40 66 3
106 25 15 41 38 95
Total
5885
354 46 156 149 538 351 30
13451106 155
246 779 630
CULPRIT STAGEDEvents
161
12 1 2 3
30 13 2 4 9 11 13 2
59
Total
3373
126 64 96 93
538 210 12
303 538 252 201 259 681
0.1 0.2 0.5 1 5 10
Odds Ratio (OR)
CVO Better Staged Better
OR
2.20 2.18
1.2811.31 3.22 0.83 1.36 3.51 0.56 6.40 1.36 2.35 2.89 6.59 1.87
95%−CI
[1.82; 2.67][1.58; 3.01]
[0.65; 2.52][1.34; 95.44][0.69; 15.02][0.18; 3.78][0.83; 2.22][1.88; 6.54][0.08; 3.83][2.34; 17.49][0.63; 2.93][1.05; 5.25][1.50; 5.57][1.58; 27.51][1.33; 2.64]
Bayesian hierarchical meta-analysis 2.09 [1.54; 2.88]
2
Mortality rates at longest follow-up are obtained from studies described in Table 4 comparing CVO with staged coronary intervention of
noninfarct lesions in patients with STEMI and MV CAD. Staging occurred either in hospital or after hospital discharge. Abbreviations as in
Figure 1.
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1073
artery bypass graft surgery, and 19 other patients didnot undergo PCI for other reasons. The compositeprimary outcome of all-cause mortality, reinfarction,and ischemia-driven revascularization at a medianfollow-up of 27 months occurred in 40 (13%) patientswho had FFR-guided staged PCI and 68 (22%) patientswho had CVO primary PCI (HR: 0.56; 95% CI: 0.38 to0.83; p ¼ 0.004). The improvement in outcomeappeared to be entirely related to a lower rate ofroutine and urgent repeat revascularization. Therewere no differences in mortality or reinfarction rates.
Three smaller randomized controlled trials testedCVO PCI versus staged PCI. Dambrink et al. (55,56)randomized 120 patients to a strategy of CVO pri-mary PCI or FFR-guided staged PCI. There was nosignificant difference in left ventricular ejectionfraction measured at 6 months, nor was there a dif-ference in the composite endpoint of mortality,reinfarction, and repeat revascularization at 3 years(35.0% vs. 35.4%; p ¼ 0.96). The PRAGUE-13 (Multi-vessel Disease Diagnosed at the Time of PPCI forSTEMI: Complete Revascularization Versus Conser-vative Strategy) trial randomized 214 patients over a4-year period to undergo CVO primary PCI or stagedPCI at 3 to 40 days (57). The primary compositeendpoint of all-cause mortality, reinfarction, or
stroke at 38 months was not significantly different(13.9% vs. 16.0%; p ¼ 0.41). The EXPLORE (EvaluatingXience V and Left Ventricular Function in Percuta-neous Coronary Intervention on Occlusions AfterST-Elevation Myocardial Infarction) trial randomized302 patients with a chronic total occlusion to stagedPCI of the occluded noninfarct artery within 7 days ormedical therapy (58). There were no differences inleft ventricular ejection fraction, left ventricular end-diastolic volume, or clinical events at 4 months.
The 2013 ACCF/AHA STEMI guideline recommendsPCI of a noninfarct artery before hospital dischargeonly in patients with spontaneous symptoms ofmyocardial ischemia (Class I), or in patients with in-termediate- or high-risk findings on noninvasivetesting (Class IIa) (11). Similarly, the 2014 ESC/EACTSguidelines on myocardial revascularization give aClass IIa recommendation for staged PCI for symp-toms or ischemia within days to weeks after primaryPCI (14). The 2015 ACC/AHA/SCAI Focused Updategives a Class IIb recommendation for anatomy-basedstaged PCI (15).
MV PRIMARY PCI VERSUS STAGED PCI. We identi-fied 5 single-center (38,41–43,69), 3 multicenter(51,70,71), and 3 randomized (18,59,60) trials that

FIGURE 4 Forest Plot of Mortality in Randomized Controlled Trials Comparing CVO Primary PCI With Staged PCI
Study
Fixed effect modelRandom effects modelHeterogeneity: I−squared=43.6%, tau−squared=0.3606, p=0.1314
Politi (2010)Ghani (2012)Engstrom (2015)Hinomaz (2015)Henriques (2015)
Events
31
13 011 7 0
Total
700
84 41313108154
CULPRITEvents
33
4 415 6 4
Total
713
65 80314106148
STAGED
0.1 0.2 0.5 10
Odds Ratio (OR)
CVO Better Staged Better
OR
0.910.92
2.790.200.731.160.10
95%−CI
[0.55; 1.51][0.40; 2.12]
[0.87; 9.01][0.01; 3.90][0.33; 1.61][0.38; 3.56][0.01; 1.95]
Bayesian hierarchical meta-analysis 0.94 [0.31; 2.09]
1 2 5
Mortality rates at longest follow-up are obtained from trials described in Table 3 comparing CVO with staged coronary intervention of
noninfarct lesions in patients with STEMI and MV CAD. Staged procedures occurred 2 to 57 days after the primary intervention. Abbreviations as
in Figure 1.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1074
compared MV primary PCI to staged PCI (Tables 3and 5). There were no obvious differences in MACE,reinfarction, or repeat revascularization. In the7 observational studies with evaluable data, weobserved a significant increase in long-term mortalitywith MV primary PCI compared with staged PCI usingboth traditional statistical approaches (OR: 3.89; 95%CI: 2.65 to 5.70) and Bayesian approaches (OR: 3.59;95% BCI: 2.04 to 5.56) (Figure 5). However, a morecritical clinical condition may have biased the selec-tion of patients for MV primary PCI, despite the ClassIII proscription against that strategy. There were nodifferences in the randomized trials, but the samplesizes and event rates were quite small.
META-ANALYSES
Meta-analysis in the absence of an adequately pow-ered trial must be viewed as hypothesis-generating,given the limitations of the assumptions requiredfor pooling data, as well as the limitations of the in-dividual studies. This is particularly true in this evi-dence base, with variable study populations, studydesigns, analytical methods, and clinical endpoints. Itis widely recognized that the results of meta-analysisincluding small trials or observational studiesfrequently yield findings that are not definitiveand are contradictory to well-conducted largermulticenter randomized trials (72). The conclusionsof 25 meta-analyses (73–97) on the role of PCI in pa-tients with STEMI and MV CAD have been remarkablydiscordant, reflecting the inclusion of different trialsin different meta-analyses and the absence of a
definitive large randomized trial (Table 6). To sum-marize, 6 meta-analyses showed increased mortality,10 showed similar mortality, and 9 showed decreasedmortality after MV PCI. Therefore, it is easy for anauthor to selectively cite a meta-analysis to support aconclusion or position on this topic for a publication,but our complete review of these meta-analyses il-lustrates the limitations of using meta-analysis as aprimary source for evidence-based guideline recom-mendations (15).
ADVANTAGES AND DISADVANTAGES OF
MV PRIMARY PCI
There are several potential advantages to performingMV primary PCI (Central Illustration). First, acuteoptimization of myocardial blood supply may in-crease myocardial salvage in hibernating myocardiumor watershed areas of infarction, improving left ven-tricular ejection fraction, although there areconflicting reports on benefit (55,58,59). Second, MVprimary PCI may decrease the compounded risk ofvascular complications from the repeat vascularpunctures required in a staged procedure.Third, MV primary PCI may decrease hospitallength of stay and use fewer resources, increasingcost-effectiveness. Finally, complete revasculariza-tion may decrease the risk of a future acute coronarysyndrome or revascularization procedure andimprove prognosis.
There are several potential disadvantages toperforming MV primary PCI (Central Illustration).First, procedure times are prolonged, and there is

TABLE 5 Observational Trials of MV Primary PCI Versus Staged PCI
First Author (Ref. #)Year Design
MV(n)
Staged(n)
Timing ofStaged PCI
PrimaryEndpoint
Follow-Up(Months)
Mortalityn (%)
Outcomes forMV
Corpus (38)2004
RegistrySingle-center1998–2002
26 126 In-hospital D, MI, revasc 12 MV: 5 (19)Staged: 12 (9.5)
MACE, MI, revasc higherMortality similar
Varani (41)2008
RegistrySingle-center2004–2007
147 96 In-hospital Mortality 1 MV: 15 (9.9)Staged: 2 (2.1)
Mortality higher
Mohamad (42)2011
RetrospectiveSingle-center2002–2006
7 12 In-hospital Mortality 12 MV: 2 (28.6)Staged: 2 (16.7)
MACE similarMortality similar
Maamoun (69)2011
SequentialSingle-center2007–2008
42 36 <7 days D, MI, ACS hosp, stroke 12 MV: 2 (4.8)Staged: 1 (2.8)
MACE, MI, revasc similarMortality similar
Kornowski (70)2011
SubsetMulticenter2005–2007
275 393 30 days, mean D, MI, revasc, stroke 12 MV: 25 (9.2)Staged: 9 (2.3)
MACE, MI, revasc similarMortality higher
Jensen (71)2012
RegistryMulticenter2002–2009
354 820 <60 days Mortality 12 MV: 36 (10.2)Staged: 16 (2.0)
Mortality higher
Kim (43)2014
RegistrySingle-center2006–2009
67 252 In-hospital D, MI, revasc 36 MV: 5 (7.4)Staged: 11 (4.4)
MI, revasc similarMortality similar
Manari (51)2014
RegistryMulticenter2002–2010
367 988 <60 days D, MI, revasc 24 N/A MI, revasc similarMortality similar
Abbreviations as in Tables 1 and 4.
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1075
increased radiation exposure. Second, higher contrastmedia volume increases the risk for contrast ne-phropathy and acute volume overload, potentiallyincreasing hospital morbidity and mortality (98).Third, noninfarct artery stenosis severity may beacutely exaggerated as the result of circulatingcatecholamine-mediated vasoconstriction, and resultin PCI of functionally insignificant stenoses (99).Fourth, the risk of jeopardizing remote viablemyocardium during PCI of noninfarct artery stenoses(distal embolization, no-reflow, side branch occlu-sion, loss of collateral circulation) could result inhemodynamic instability. Finally, there may beincreased risk for acute and subacute stent throm-bosis in a prothrombotic and proinflammatory state.The advantage of the staged PCI strategy is more timeto appropriately decide on the risks and benefits ofadditional revascularization, perhaps resulting inbetter patient selection (12).
LIMITATIONS OF THE EVIDENCE BASE
There has been significant heterogeneity in the pub-lished studies, with great variability in reportingbaseline variables, follow-up duration, and outcomemeasures. Important patient-, operator-, and center-related factors have not been detailed, potentiallycausing inclusion and exclusion selection bias. Dataon lesion location or complexity, percent diameter
stenosis, resolution of ST-segment elevation, finalThrombolysis In Myocardial Infarction (TIMI) flow,and procedure success rates were usually omitted.Neither have the indications, timing, and complete-ness of revascularization been clearly documented.Moreover, MV primary PCI cohorts have sometimesincluded patients undergoing staged PCI, andCVO primary PCI cohorts have usually included pa-tients undergoing staged PCI, ischemia-driven PCI, orcoronary bypass graft surgery at undocumented times.A review of the patient enrollment dates demonstratesthat many of the reports are older and may not reflectimprovements in clinical practice over the lastseveral years. Also, prospective and retrospective,single-center and multicenter, and observational andrandomized reports have been variably pooled inmeta-analyses, with discordant conclusions.
Additionally, observational studies are known tobe limited by ascertainment bias, unmeasured con-founders, failure to monitor or adjudicate events,and lack of adequate risk adjustment. There wasusually a large imbalance in cohort size in theobservational studies, with only a small proportion ofpatients undergoing MV PCI. Conversely, the largebenefit with MV primary PCI in the randomized trialsmost likely overestimates the true benefit becausethe trials were underpowered to detect a clinicallymeaningful difference in outcomes, few endpointsoccurred, and the patients were selected for

FIGURE 5 Forest Plot of Mortality in Observational Studies Comparing MV Primary PCI With Staged PCI
Study
Fixed effect modelRandom effects modelHeterogeneity: I−squared=0%, tau−squared=0, p=0.4953
Corpus (2004)Varani (2008)Mohamad (2011)Maamoun (2011)Kornowski (2011)Jensen (2012)Kim (2014)
Events
90
515 2 2
2536 5
Total
918
26147
7 42275354 67
MULTIVESSELEvents
53
12 2 2 1 91611
Total
1735
126 96 12 36
393 820 252
STAGED Odds Ratio (OR)
MV Better
OR
3.993.89
2.265.342.001.754.275.691.77
95%−CI
[2.74; 5.80][2.65; 5.70]
[0.72; 7.09] [1.19; 23.9] [0.21; 18.7] [0.15; 20.1][1.96; 9.29] [3.11; 10.4][0.59; 5.27]
Bayesian hierarchical meta-analysis 3.59 [2.04; 5.56]
0.1 0.2 0.5 101 2 5Staged Better
Mortality rates at longest follow-up are obtained from studies in Table 5 comparing MV PCI with staged MV PCI in patients with STEMI.
Staged procedures took place during the index hospitalization or up to 60 days after the primary intervention. PCI ¼ percutaneous coronary
intervention; other abbreviations as in Figure 1.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1076
randomization. The randomized trials are alsolimited by open-label design, premature cessation in2 trials (16,55,56), and lack of information on clinicalor lesion selection criteria. What has really beentested in these trials is a strategy of early invasivetherapy versus early noninvasive therapy for non-infarct artery stenoses, not 2 distinct treatments,because patients frequently crossed over to the otherstrategy or were lost to follow-up.
FRACTIONAL FLOW RESERVE
It has been suggested that adding a physiologicalassessment of ischemia during coronary angiographyusing FFR measurements might avoid the limitationsof anatomy-guided decision making and be morecompatible with existing revascularization recom-mendations supporting documentation of ischemiabefore PCI. However, the FAME-2 (Fractional FlowReserve Versus Angiography for Multivessel Evalua-tion 2) trial found no differences in death or rein-farction rates with FFR-guided PCI compared withmedical therapy in 888 patients with stable CAD,despite the fact that 23% of patients had class III/IVangina, and 14% of lesions were >90% diameter ste-nosis (100). Additionally, FFR measurements may beincreased during primary PCI due to acutelydecreased coronary blood flow (7), although 1 reportdemonstrated good FFR reproducibility with serialmeasurements (101). The FFR benefit is also not clearas part of a staged PCI strategy. As previously
outlined, Dambrink et al. (55) and Ghani et al. (56)randomized 121 patients to FFR-guided staged PCIor medical therapy after primary PCI and found nodifference in MACE rates (55,56). Similarly, theDANAMI 3-PRIMULTI trial randomized 627 patientsafter primary PCI to FFR-guided staged PCI versusmedical therapy and found no differences in death orreinfarction rates (20). Only repeat revascularizationevents were reduced, a preordained outcome whennoninfarct artery stenoses meeting revascularizationguidelines are not treated during the initial hospi-talization. It may be that lesion stability and severityhave more prognostic value after STEMI than docu-mentation of ischemia.
FUTURE STUDIES
There are at least 8 randomized clinical trials inprogress evaluating the role of PCI in patient withSTEMI and MV CAD (Table 7). The study designs vary,so complementary data will be added that will not beeasily aggregated by meta-analysis. Several publica-tions have suggested that the COMPLETE (Completevs Culprit-Only Revascularization to Treat Multi-vessel Disease After Primary PCI for STEMI) trial willclarify the debate, but this trial randomized patientsto CVO primary PCI versus staged PCI, not MV pri-mary PCI. Although many physicians are eager tohave a guideline recommendation for staged PCI, itwill not clarify the debate on anatomy-guided versusFFR-guided revascularization because FFR is only

TABLE 6 Meta-Analyses of CVO Primary PCI Versus MV Primary PCI or Staged PCI
First Author (Ref. #)Year
RCT(n)
Observational(n)
Abstracts(n)
Patients(n)
Short-TermMV PCI F/U
Long-TermMV PCI F/U
Sethi (73)2011
2 9 0 CVO: 27,394MV PCI: 4,640
Mortality similar MACE, revasc similarMortality similar
Navarese (74)2011
2 8 0 CVO: 27,047MV PCI: 4,118
Mortality similar MI similarRevasc lowerMortality similar
Bangalore (75)2011
2 10 7 CVO: 52,074MV PCI: 9,690
MACE, revasclower
MI similarMortality similar
MACE, revasc lowerMI similarMortality lower
Vlaar (76)2011
2 16 0 CVO: 34,295MV PCI: 5,985
Mortality higher Mortality higher
Takagi (77)2011
4 7 0 36,689 Mortality higher Mortality higher
Lu (78)2013
3 8 2 CVO: 51,998MV PCI: 8,240
Mortality higher MACE, MI similarRevasc lowerMortality higher
Bagai (79)2013
3 11 0 CVO: 30,492MV PCI: 4,747
MI, revasc similarMortality higher
Revasc lowerMortality higher
Bainey (80)2014
3 17 6 CVO: 38,438MV PCI: 7,886
Mortality similar Revasc lowerMortality lower
Pandit (81)2014
3 0 0 CVO: 332MV PCI: 416
N/A MI, revasc lowerMortality lower
Zhang (82)2014
4 14 0 CVO: 33,594MV PCI: 5,796
Mortality higher MI similarRevasc lowerMortality higher
Sekercioglu (83)2014
3 0 0 CVO: 324MV PCI: 341
N/A MI, revasc lowerMortality lower
Dahal (84)2014
4 0 0 CVO: 332MV PCI: 573
N/A MACE, MI, revasc lowerMortality similar
Moretti (85)2015
4 9 0 N/A N/A MI similarRevasc lowerMortality similar
Briasoulis (86)2015
5 0 0 CVO: 522MV PCI: 612
N/A MI, revasc lowerMortality lower
Sardar (87)2015
5 0 0 CVO: 522MV PCI: 549
N/A MI, revasc lowerMortality lower
Song (88)2015
7 23 0 CVO: 36,169MV PCI: 8,087
N/A MACE, MI similarRevasc lowerMortality similar
Rasoul (89)2015
5 10 0 CVO: 30,939MV PCI: 5,109
N/A MACE similarMI, revasc lowerMortality higher
Bangalore (90)2015
5 0 0 CVO: 519MV PCI: 646
N/A MI similarRevasc lowerMortality lower
Sarathy (91)2015
4 0 0 CVO: 376MV PCI: 399
N/A MI, revasc lowerMortality lower
Bittl (92)2015
4 14 0 CVO: 40,180MV PCI: 7,588
N/A Mortality similar
El-Hayek (93)2015
4 0 0 CVO: 478MV PCI: 566
N/A MI, revasc lowerMortality lower
Kowalewski (94)2015
7 0 0 CVO: 666MV PCI: 637
N/A MI, revasc lowerMortality similar
Elgendy (95)2015
7 0 0 CVO: 939MVI: 1,000
N/A MACE, revasc lowerMI similarMortality similar
Spencer (96)2015
5 0 0 CVO: 775MV PCI: 793
N/A MI, revasc lowerMortality similar
Bajaj (97)2015
8 0 0 CVO: 919MV PCI: 1,054
N/A MACE, revasc lowerMI similarMortality similar
F/U ¼ follow-up; RCT ¼ randomized controlled trials; other abbreviations as in Table 1.
J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1077

TABLE 7 Future Randomized Clinical Trials
RandomizedControlled Trial Design Size (N) Composite Primary Endpoint
COCUANCT01180218
CVO primary PCI vs.MV primary PCI
646 1-yr cardiac death, STEMI,ischemia-driven TVR
ASSIST-MINCT01818960
CVO primary PCI vs.MV primary PCI
250 90-day infarct size by CMR
CULPRIT SHOCKNCT01927549
CVO primary PCI vs.MV primary PCI incardiogenic shock
706 30-day death or acute kidneyinjury requiring renalreplacement therapy
FITNCT01160900
CVO primary PCI vs.staged PCI
180 30-day death, MI1-yr stent thrombosis, TVR
COMPLETENCT01740479
CVO primary PCI vs. stagedPCI (<72 h) with FFR forlesions 50%–70% DS
3,900 4-yr death, MI
ZES for STEMINCT01781715
MV primary PCI vs. staged(3–15 days) PCI
120 1-yr death, MI, revascularization
CompareAcuteNCT01399736
MV primary PCI with FFR vs.ischemia-guided PCI
885 1-yr death, MI, cerebrovascularevents, revascularization
CROSS-AMINCT01179126
Staged PCI (indexhospitalization) vs.ischemia-guided PCI
400 1-yr cardiovascular death, MI,revascularization, HFhospitalization
ASSIST-MI ¼ Revascularization Strategies for ST Elevation Myocardial Infarction Trial; CMR ¼ cardiac magneticresonance; COCUA ¼ Complete Lesion Versus Culprit Lesion Revascularization; CompareAcute ¼ ComparisonBetween FFR Guided Revascularization Versus Conventional Strategy in Acute STEMI Patients With MVD;COMPLETE ¼ Complete vs Culprit-Only Revascularization to Treat Multi-vessel Disease After Primary PCI forSTEMI; CROSS-AMI¼ Strategies of Revascularization in Patients With ST-Segment Elevation Myocardial Infarction(STEMI) and Multivessel Disease; CULPRIT SHOCK ¼ Culprit Lesion Only PCI Versus Multivessel PCI in CardiogenicShock; CVO¼ culprit-only; DS¼ diameter stenosis; FIT¼ Fast Infarction Treatment; FFR¼ fractional flow reserve;STEMI ¼ ST-segment elevation myocardial infarction; ZES for STEMI ¼ Multivessel Stenting Versus StagedRevascularization With Zotarolimus-Eluting Stent for STEMI; other abbreviations as in Tables 1 and 2.
Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1078
being performed for lesions with 50% to 70% diam-eter stenosis. Similarly sized randomized trials areneeded to compare CVO to MV primary PCI and MVprimary PCI to staged PCI.
CONCLUSIONS
Compared with CVO PCI, MV PCI, either at thetime of primary PCI or as a staged procedure inselected patients who are hemodynamically stable,appears to be safe and may result in better out-comes. Whether MV primary PCI or staged PCI issuperior remains to be demonstrated. Indicationsfor noninfarct artery PCI should match elective PCIstandards, with routine PCI of intermediate orcomplex stenoses at time of primary PCI discour-aged. Until more definitive studies are available,physicians should integrate clinical status andcomorbidities, lesion complexity, and clinicaljudgment to determine the optimal strategy andtiming for PCI in patients with STEMI and MV CAD.Demonstration of myocardial ischemia, multidisci-plinary evaluation by the heart team, and stagedPCI (or coronary artery bypass graft surgery)following appropriate use criteria has been themore traditional approach to pursuing MV revas-cularization. More studies are needed to clarify theindications for and timing of noninfarct artery PCI,and to determine whether MACE are more affectedby baseline characteristics than by the additionalPCI procedure.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Eric R. Bates, CVC Cardiovascular Medicine, 1500 EastMedical Center Drive, Ann Arbor, Michigan 48109-5869. E-mail: [email protected].
RE F E RENCE S
1. Park DW, Clare RM, Schulte PJ, et al. Extent,location, and clinical significance of non-infarct-related coronary artery disease among patientswith ST-elevation myocardial infarction. JAMA2014;312:2019–27.
2. Muller DW, Topol EJ, Ellis SG, et al., Throm-bolysis and Angioplasty in Myocardial Infarction(TAMI) Study Group. Multivessel coronary arterydisease: a key predictor of short-term prognosisafter reperfusion therapy for acute myocardialinfarction. Am Heart J 1991;121:1042–9.
3. Jaski BE, Cohen JD, Trausch J, et al. Outcome ofurgent percutaneous transluminal coronary an-gioplasty in acute myocardial infarction: compari-son of single-vessel versus multivessel coronaryartery disease. Am Heart J 1992;124:1427–33.
4. Sorajja P, Gersh BJ, Cox DA, et al. Impact ofmultivessel disease on reperfusion success andclinical outcomes in patients undergoing primarypercutaneous coronary intervention for acutemyocardial infarction. Eur Heart J 2007;28:1709–16.
5. Goldstein JA, Demetriou D, Grines CL, et al.Multiple complex coronary plaques in patients
with acute myocardial infarction. N Engl J Med2000;343:915–22.
6. Asakura M, Ueda Y, Yamaguchi O, et al.Extensive development of vulnerable plaques as apan-coronary process in patients with myocardialinfarction: an angioscopic study. J Am Coll Cardiol2001;37:1284–8.
7. GibsonCM,RyanKA,MurphySA, et al., TIMI StudyGroup. Impaired coronary blood flow in nonculpritarteries in the setting of acutemyocardial infarction.J Am Coll Cardiol 1999;34:974–82.
8. Grines CL, Topol EJ, Califf RM, et al., TAMIStudy Group. Prognostic implications and pre-dictors of enhanced regional wall motion of thenoninfarct zone after thrombolysis and angio-plasty therapy of acute myocardial infarction.Circulation 1989;80:245–53.
9. Parodi G, Mernisha G, Valenti R, et al. Five yearoutcome after primary coronary intervention foracute ST elevationmyocardial infarction: results froma single centre experience. Heart 2005;91:1541–4.
10. Levine GN, Bates ER, Blankenship JC, et al.2011 ACCF/AHA/SCAI guideline for percutaneouscoronary intervention. A report of the American
College of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines andthe Society for Cardiovascular Angiography andInterventions. J Am Coll Cardiol 2011;58:e44–122.
11. O’Gara P, Kushner FG, Ascheim DD, et al. 2013ACCF/AHA guideline for the management of ST-elevation myocardial infarction. a report of theAmerican College of Cardiology Foundation/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2013;61:485–510.
12. Patel MR, Dehmer GJ, Hirshfeld JW, et al.ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012appropriate use criteria for coronary revasculariza-tion focused update: a report of the AmericanCollege of Cardiology Foundation Appropriate UseCriteria Task Force, Society for CardiovascularAngiography and Interventions, Society of ThoracicSurgeons, American Association for Thoracic Sur-gery, American Heart Association, American Societyof Nuclear Cardiology, and the Society of Cardio-vascular Computed Tomography. J Am Coll Cardiol2012;59:857–81.
13. American College of Cardiology. American Col-lege of Cardiology Updates Heart Attack Recom-mendations. September 19, 2014. Available at:

J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1079
http://www.acc.org/latest-in-cardiology/articles/2014/09/19/16/03/american-college-of-cardiology-updates-heart-attack-recommendations. AccessedJune 22, 2016.
14. Windecker S, Kolh P, Alfonso F, et al. 2014ESC/EACTS guidelines on myocardial revasculari-zation. Eur Heart J 2014;35:2541–619.
15. Levine GN, O’Gara PT, Bates ER, et al. 2015ACC/AHA/SCAI focused update on primary percu-taneous coronary intervention for patients withST-elevation myocardial infarction: an update ofthe 2011 ACCF/AHA/SCAI Guideline for Percuta-neous Coronary Intervention and the 2013ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J Am Coll Cardiol2016;67:1235–50.
16. Wald DS, Morris JK, Wald NJ, et al., PRAMIInvestigators. Randomized trial of preventive an-gioplasty in myocardial infarction. N Engl J Med2013;369:1115–23.
17. Di Mario C, Mara S, Flavio A, et al. Single vsmultivessel treatment during primary angioplasty:results of the multicentre randomised HEpacoatfor cuLPrit or multivessel stenting for AcuteMyocardial Infarction (HELP AMI) study. Int JCardiovasc Intervent 2004;6:128–33.
18. Politi L, Sgura F, Rossi R, et al. A randomisedtrial of target-vessel versus multi-vessel revascu-larisation in ST-elevation myocardial infarction:major adverse cardiac events during long-termfollow-up. Heart 2010;96:662–7.
19. Gershlick AH, Khan JN, Kelly DJ, et al. Ran-domized trial of complete versus lesion-onlyrevascularization in patients undergoing primarypercutaneous coronary intervention for STEMI andmultivessel disease: the CvLPRIT trial. J Am CollCardiol 2015;65:963–72.
20. Engstrøm T, Kelbæk H, Helqvist S, et al.,DANAMI 3-PRIMULTI Investigators. Completerevascularisation versus treatment of the culpritlesion only in patients with ST-segment elevationmyocardial infarction and multivessel disease(DANAMI 3-PRIMULTI): an open-label, randomisedcontrolled trial. Lancet 2015;386:665–71.
21. Ijsselmuiden AJ, Ezechiels J, Westendorp IC,et al. Complete versus culprit vessel percutaneouscoronary intervention in multivessel disease: a ran-domized comparison. Am Heart J 2004;148:467–74.
22. Chen LY, Lennon RJ, Grantham JA, et al. In-hospital and long-term outcomes of multivesselpercutaneous coronary revascularization afteracute myocardial infarction. Am J Cardiol 2005;95:349–54.
23. Lee HJ, Song YB, Hahn JY, et al. Multivessel vssingle-vessel revascularization in patients withnon-ST-elevation acute coronary syndrome andmultivessel disease in the drug-eluting stent era.Clin Cardiol 2011;3:160–5.
24. Kong JA, Chou ET, Minutello RM, et al. Safetyof single versus multi-vessel angioplasty for pa-tients with acute myocardial infarction and multi-vessel coronary artery disease: report from theNew York State Angioplasty Registry. Coron ArteryDis 2006;17:71–5.
25. Jo HS, Park JS, Sohn JW, et al. Culprit-lesion-only versus multivessel revascularization usingdrug-eluting stents in patients with ST-segment
elevation myocardial infarction: a Korean AcuteMyocardial Infarction Registry-based analysis.Korean Circ J 2011;41:718–25.
26. Abe D, Sato A, Hoshi T, et al. Initial culprit-only versus initial multivessel percutaneous coro-nary intervention in patients with ST-segmentelevation myocardial infarction: results from theIbaraki Cardiovascular Assessment Study registry.Heart Vessels 2014;29:171–7.
27. Ryu KS, Park HW, Park SH, et al., other KoreaAcute Myocardial Infarction Registry Investigators.Comparison of clinical outcomes betweenculprit vessel only and multivessel percutaneouscoronary intervention for ST-segment elevationmyocardial infarction patients with multivesselcoronary diseases. J Geriatr Cardiol 2015;12:208–17.
28. Poyen V, Labrunie P, Silvestri M, et al. [Com-plete revascularization of multivessel coronaryartery disease during acute myocardial infarction.Results following hospitalization and after 30months. Series of 86 interventions carried outwith 167 multivessel disease patients; causes offailure]. Arch Mal Coeur Vaiss 2003;96:1149–56.
29. Kalarus Z, Lenarczyk R, Kowalczyk J, et al.Importance of complete revascularization in pa-tients with acute myocardial infarction treatedwith percutaneous coronary intervention. AmHeart J 2007;153:304–12.
30. Katayama N, Horiuchi K, Nakao K, et al. [Doespercutaneous coronary intervention in non-culpritvessels improve the prognosis of acute myocardialinfarction complicated by pump failure?]. J Cardiol2005;46:1–8.
31. van der Schaaf RJ, Claessen BE, Vis MM, et al.Effect of multivessel coronary disease with orwithout concurrent chronic total occlusion on one-year mortality in patients treated with primarypercutaneous coronary intervention for cardio-genic shock. Am J Cardiol 2010;105:955–9.
32. Xu F, Chen YG, Li JF, et al. Multivesselpercutaneous coronary intervention in Chinesepatients with acute myocardial infarction andsimple nonculprit arteries. Am J Med Sci 2007;333:376–80.
33. He Y, Bittl JA, Wouhib A, Normand SLT. Casestudy in cardiovascular medicine: unprotected leftmain coronary artery disease. In: Biondi-Zoccai G,editor. Network Meta-Analysis: Evidence Synthe-sis With Mixed Treatment Comparison.Hauppauge, NY: Nova Science Publishers, 2014:285–306.
34. Spiegelhalter DJ, Abrams KR, Myles JP.Bayesian Approaches to Clinical Trials and HealthCare Evaluations. Chichester, England: Wiley,2004.
35. Schwarzer G. Package ’meta’. Freiburg, Ger-many: version 3.8–0, 2012.
36. Kruschke JK. Doing Bayesian Data Analysis: ATutorial With R and BUGS. Oxford, UK: Elsevier,2011.
37. Thomas A, O’Hara B, Ligges U, et al. MakingBUGS Open. R News 2006;6:12–7.
38. Corpus RA, House JA, Marso SP, et al. Multi-vessel percutaneous coronary intervention in pa-tients with multivessel disease and acute
myocardial infarction. Am Heart J 2004;148:493–500.
39. Khattab AA, Abdel-Wahab M, Röther C. Multi-vessel stenting during primary percutaneous cor-onary intervention for acute myocardial infarction.A single-center experience. Clin Res Cardiol 2008;97:32–8.
40. Qarawani D, Nahir M, Abboud M, et al. Culpritonly versus complete coronary revascularizationduring primary PCI. Int J Cardiol 2008;123:288–92.
41. Varani E, Balducelli M, Aquilina M, et al. Singleor multivessel percutaneous coronary interventionin ST-elevation myocardial infarction patients.Catheter Cardiovasc Interv 2008;72:927–33.
42. Mohamad T, Bernal JM, Kondur A, et al. Cor-onary revascularization strategy for ST elevationmyocardial infarction with multivessel disease:experience and results at 1-year follow-up. Am JTher 2011;18:92–100.
43. Kim MC, Jeong MH, Park KH, et al. Three-yearoutcomes of staged, ad hoc, and culprit-onlypercutaneous coronary intervention in patientswith ST-segment elevation myocardial infarctionand multivessel disease. Int J Cardiol 2014;176:505–7.
44. Cavender MA, Milford-Beland S, Roe MT, et al.Prevalence, predictors, and in-hospital outcomesof non-infarct artery intervention during primarypercutaneous coronary intervention for ST-segment elevation myocardial infarction (fromthe National Cardiovascular Data Registry). Am JCardiol 2009;104:507–13.
45. Toma M, Buller CE, Westerhout CM, et al.,APEX-AMI Investigators. Non-culprit coronary ar-tery percutaneous coronary intervention duringacute ST-segment elevation myocardial infarction:insights from the APEX-AMI trial. Eur Heart J2010;31:1701–7.
46. Dziewierz A, Siudak Z, Rakowski T, et al.Impact of multivessel coronary artery disease andnoninfarct-related artery revascularization onoutcome of patients with ST-elevation myocardialinfarction transferred for primary percutaneouscoronary intervention (from the EUROTRANSFERregistry). Am J Cardiol 2010;106:342–7.
47. Bauer T, Zeymer U, Hochadel M, et al. Prima-vista multi-vessel percutaneous coronary inter-vention in haemodynamically stable patients withacute coronary syndromes: analysis of over 4,400patients in the EHS-PCI registry. Int J Cardiol 2013;166:596–600.
48. Jaguszewski M, Radovanovic D,Nallamothu BK, et al., AMIS Plus Investigators.Multivessel versus culprit vessel percutaneouscoronary intervention in ST-elevation myocardialinfarction: is more worse? EuroIntervention 2013;9:909–15.
49. Santos AR, Piçarra BC, Celeiro M, et al.,Investigadores do Registo Nacional de SíndromesCoronárias Agudas. Multivessel approach inST-elevation myocardial infarction: impact on in-hospital morbidity and mortality. Rev Port Car-diol 2014;33:67–73.
50. Jeger R, Jaguszewski M, Nallamothu BN,et al., AMIS Plus Investigators. Acute multivesselrevascularization improves 1-year outcome in ST-

Bates et al. J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6
PCI Strategies in Patients With STEMI and MV CAD S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1
1080
elevation myocardial infarction: a nationwidestudy cohort from the AMIS Plus registry. Int JCardiol 2014;172:76–81.
51. Manari A, Varani E, Guastaroba P, et al. Long-term outcome in patients with ST segmentelevation myocardial infarction and multivesseldisease treated with culprit-only, immediate, orstaged multivessel percutaneous revascularizationstrategies: insights from the REAL registry. Cath-eter Cardiovasc Interv 2014;84:912–22.
52. Roe MT, Cura FA, Joski PS, et al. Initial expe-rience with multivessel percutaneous coronaryintervention during mechanical reperfusion foracute myocardial infarction. Am J Cardiol 2001;88:170–3.
53. Hannan EL, Samadashvili Z, Walford G, et al.Culprit vessel percutaneous coronary interventionversus multivessel and staged coronary interven-tion for ST-segment elevation myocardial infarc-tion patients with multivessel disease. J Am CollCardiol Intv 2010;3:22–31.
54. Iqbal MB, Ilsley C, Kabir T, et al., London HeartAttack Centre (HAC) Group Investigators. Culpritvessel versus multivessel intervention at the timeof primary percutaneous coronary intervention inpatients with ST-segment–elevation myocardialinfarction and multivessel disease: real-worldanalysis of 3984 patients in London. Circ Car-diovasc Qual Outcomes 2014;7:936–43.
55. Dambrink JH, Debrauwere JP, van ’t Hof AW,et al. Non-culprit lesions detected during primaryPCI: treat invasively or follow the guidelines?EuroIntervention 2010;5:968–75.
56. Ghani A, Dambrink JH, van ’t Hof AW, et al.Treatment of non-culprit lesions detected duringprimary PCI: long-term follow-up of a randomisedclinical trial. Neth Heart J 2012;20:347–53.
57. Hlinomaz O. Multivessel coronary diseasediagnosed at the time of primary PCI for STEMI:complete revascularization versus conservativestrategy: the PRAGUE 13 trial. Paper presented at:EuroPCR; May 19, 2015; Paris, France.
58. Henriques JPS. EXPLORE: a prospective ran-domized trial of chronic total occlusion interven-tion versus medical therapy after successfulprimary angioplasty in patients with ST-segmentelevation. Paper presented at: TCT ScientificSymposium; October 11-15, 2015; San Francisco,CA. Available at: http://www.tctmd.com/show.aspx?id¼131921. Accessed June 22, 2016.
59. Ochala A, Smolka GA, Wojakowski W, et al. Thefunction of the left ventricle after complete mul-tivessel one-stage percutaneous coronary inter-vention in patients with acute myocardialinfarction. J Invasive Cardiol 2004;16:699–702.
60. Tarasov RS, Ganyukov VI, Protopopov AV,et al. Six month results of randomized clinical trial:multivessel stenting versus staged revasculariza-tion for ST-elevation myocardial infarction pa-tients with second generation drug eluting stents.Clin Med Res 2014;3:125–9.
61. Rigattieri S, Biondi-Zoccai G, Silvestri P, et al.Management of multivessel coronary disease afterST elevation myocardial infarction treated by pri-mary angioplasty. J Interv Cardiol 2008;21:1–7.
62. Han YL, Wang B, Wang XZ, et al. Comparativeeffects of percutaneous coronary intervention for
infarct-related artery only or for both infarct- andnon-infarct-related arteries in patients with ST-elevation myocardial infarction and multi-vesseldisease. Chin Med J (Engl) 2008;121:2384–7.
63. Chen HC, Tsai TH, Fang HY, et al. Benefit ofrevascularization in non-infarct-related artery inmultivessel disease patients with ST-segmentelevation myocardial infarction undergoing pri-mary percutaneous coronary intervention. IntHeart J 2010;51:319–24.
64. Ma LX, Lu ZH, Wang L, et al. Culprit vesselonly versus “one-week” staged percutaneouscoronary intervention for multivessel disease inpatients presenting with ST-segment elevationmyocardial infarction. J Geriatr Cardiol 2015;12:226–31.
65. Russo JJ, Wells GA, Chong AY, et al., CAPITALInvestigators. Safety and efficacy of stagedpercutaneous coronary intervention during indexadmission for ST-elevation myocardial infarctionwith multivessel coronary disease (insights fromthe University of Ottawa Heart Institute STEMIregistry). Am J Cardiol 2015;116:1157–62.
66. Barringhaus KG, Park KL, McManus DD, et al.,GRACE Investigators. Outcomes from patientswith multi-vessel disease following primary PCI:staged PCI imparts very low mortality. CatheterCardiovasc Interv 2011;77:617–22.
67. Lee HW, Hong TJ, Yang MJ, et al., Korea AcuteMyocardial Infarction Registry Investigators.Comparison of infarct-related artery vs multi-vessel revascularization in ST-segment elevationmyocardial infarction with multivessel disease:analysis from Korea Acute Myocardial Infarctionregistry. Cardiol J 2012;19:256–66.
68. Toyota T, Shiomi H, Taniguchi T, et al. Culpritvessel-only vs. staged multivessel percutaneouscoronary intervention strategies in patients withmultivessel coronary artery disease undergoingprimary percutaneous coronary intervention forST-segment elevation myocardial infarction. Circ J2016;80:371–8.
69. Maamoun W, Elkhaeat N, Elarasy R. Safety andfeasibility of complete simultaneous revasculari-zation during primary PCI in patients with STEMIand multi-vessel disease. Egyptian Heart J 2011;63:39–43.
70. Kornowski R, Mehran R, Dangas G, et al.,HORIZONS-AMI Trial Investigators. Prognosticimpact of staged versus “one-time” multivesselpercutaneous intervention in acute myocardialinfarction: analysis from the HORIZONS-AMI(Harmonizing Outcomes with Revascularizationand Stents in Acute Myocardial Infarction) trial.J Am Coll Cardiol 2011;58:704–11.
71. Jensen LO, Thayssen P, Farkas DK, et al. Culpritonly multivessel coronary interventions in patientswith ST-segment elevation myocardial infarctionand multivessel disease. EuroIntervention 2012;8:456–64.
72. LeLorier J, Grégoire G, Benhaddad A, et al.Discrepancies between meta-analyses and subse-quent large randomized, controlled trials. N Engl JMed 1997;337:536–42.
73. Sethi A, Bahekar A, Bhuriya R, et al. Completeversus culprit only revascularization in acute ST
elevation myocardial infarction: a meta-analysis.Catheter Cardiovasc Interv 2011;77:163–70.
74. Navarese EP, De Servi S, Buffon A, et al.Clinical impact of simultaneous complete revas-cularization vs. culprit only primary angioplasty inpatients with ST-elevation myocardial infarctionand multivessel disease: a meta-analysis.J Thromb Thrombolysis 2011;31:217–25.
75. Bangalore S, Kumar S, Poddar KL, et al. Meta-analysis of multivessel coronary artery revascu-larization versus culprit-only revascularization inpatients with ST-segment elevation myocardialinfarction and multivessel disease. Am J Cardiol2011;107:1300–10.
76. Vlaar PJ, Mahmoud KD, Holmes DR Jr., et al.Culprit vessel only versus multivessel andstaged percutaneous coronary intervention formultivessel disease in patients presenting withST-segment elevation myocardial infarction: apairwise and network meta-analysis. J Am CollCardiol 2011;58:692–703.
77. Takagi H, Umemoto T. Multi- versus single-vessel percutaneous coronary intervention forST-elevation myocardial infarction with multi-vessel disease. Int J Cardiol 2011;152:97–9.
78. Lu C, Huang H, Li J, et al. Complete versusculprit-only revascularization during primarypercutaneous coronary intervention in ST-elevation myocardial infarction patients withmultivessel disease: a meta-analysis. Kaohsiung JMed Sci 2013;29:140–9.
79. Bagai A, Thavendiranathan P, Sharieff W, et al.Non-infarct-related artery revascularization dur-ing primary percutaneous coronary interventionfor ST-segment elevation myocardial infarction: asystematic review and meta-analysis. Am Heart J2013;166:684–93.e1.
80. Bainey KR, Mehta SR, Lai T, et al. Complete vsculprit-only revascularization for patients withmultivessel disease undergoing primary percuta-neous coronary intervention for ST-segmentelevation myocardial infarction: a systematic re-view and meta-analysis. Am Heart J 2014;167:1–14.e2.
81. Pandit A, Aryal MR, Aryal Pandit A, et al. Pre-ventive PCI versus culprit lesion stenting duringprimary PCI in acute STEMI: a systematic reviewand meta-analysis. Open Heart 2014;1:e000012.
82. Zhang D, Song X, Lv S, et al. Culprit vesselonly versus multivessel percutaneous coronaryintervention in patients presenting with ST-segment elevation myocardial infarction andmultivessel disease. PLoS One 2014;9:e92316.
83. Sekercioglu N, Spencer FA, Lopes LC, et al.Culprit vessel only vs immediate complete revas-cularization in patients with acute ST-segmentelevation myocardial infarction: systematic re-view and meta-analysis. Clin Cardiol 2014;37:765–72.
84. Dahal K, Rijal J, Panta R, et al. Multi-vesselversus culprit-vessel and staged percutaneouscoronary intervention in STEMI patients withmultivessel disease: a meta-analysis of random-ized controlled trials. Cardiovasc Revasc Med2014;15:408–13.
85. Moretti C, D’Ascenzo F, Quadri G, et al. Man-agement of multivessel coronary disease in STEMI

J A C C V O L . 6 8 , N O . 1 0 , 2 0 1 6 Bates et al.S E P T E M B E R 6 , 2 0 1 6 : 1 0 6 6 – 8 1 PCI Strategies in Patients With STEMI and MV CAD
1081
patients: a systematic review and meta-analysis.Int J Cardiol 2015;179:552–7.
86. Briasoulis A, Afonso L, Palla M, et al. Culprit-vessel versus complete revascularization duringprimary angioplasty in ST-elevation myocardialinfarction: an updated meta-analysis. Int J Cardiol2015;178:171–4.
87. Sardar P, Chatterjee S, Giri J, et al. Interven-tion strategies for multi-vessel disease in patientswith ST-segment elevation myocardial infarction:a meta-analysis of randomized trials. Int J Cardiol2015;179:225–7.
88. Song YJ, Shin HC, Yang JI, et al. Preven-tive versus culprit-only percutaneous coronaryintervention in ST-elevation myocardial infarctionpatients with multivessel disease: a meta-analysis.J Interv Cardiol 2015;28:1–13.
89. Rasoul S, van Ommen V, Vainer J, et al. Multi-vessel revascularisation versus infarct-related ar-tery only revascularisation during the index primaryPCI in STEMI patients with multivessel disease: ameta-analysis. Neth Heart J 2015;23:224–31.
90. Bangalore S, Toklu B, Wetterslev J. Completeversus culprit-only revascularization for ST-segment–elevation myocardial infarction andmultivessel disease. A meta-analysis and trialsequential analysis of randomized trials. Circ Car-diovasc Interv 2015;8:e002142.
91. Sarathy K, Nagaraja V, Kapur A, et al. Target-vessel versus multivessel revascularisation in ST-elevation myocardial infarction: a meta-analysis
of randomised trials. Heart Lung Circ 2015;24:327–34.
92. Bittl JA, Tamis-Holland JE, Lang CD, et al.Outcomes after multivessel or culprit-vesselintervention for ST-elevation myocardial infarc-tion in patients with multivessel coronary dis-ease: a Bayesian cross-design meta-analysis.Cathet Cardiovasc Interv 2015;86 Suppl 1:S15–22.
93. El-Hayek GE, Gershlick AH, Hong MK, et al.Meta-analysis of randomized controlled trialscomparing multivessel versus culprit-only revas-cularization for patients with ST-segment eleva-tion myocardial infarction and multivessel diseaseundergoing primary percutaneous coronary inter-vention. Am J Cardiol 2015;115:1481–6.
94. Kowalewski M, Schulze V, Berti S, et al.Complete revascularization in ST-elevationmyocardial infarction and multivessel disease:meta-analysis of randomized controlled trials.Heart 2015;101:1309–17.
95. Elgendy IY, Wen X, Mahmoud A, Bavry AA.Complete versus culprit-only revascularization forpatients with multi-vessel disease undergoingprimary percutaneous coronary intervention: anupdated meta-analysis of randomized trials.Catheter Cardiovasc Interv 2015 Nov 3 [E-pubahead of print].
96. Spencer FA, Sekercioglu N, Prasad M, et al.Culprit vessel versus immediate complete revas-cularization in patients with ST-segment
myocardial infarction-a systematic review. AmHeart J 2015;170:1133–9.
97. Bajaj NS, Kalra R, Aggarwal H, et al. Com-parison of approaches to revascularization inpatients with multivessel coronary artery diseasepresenting with ST-segment elevation myocardialinfarction: meta-analyses of randomized controltrials. J Am Heart Assoc 2015;4:e002540.
98. Marenzi G, Assanelli E, Campodonico J, et al.Contrast volume during primary percutaneouscoronary intervention and subsequent contrast-induced nephropathy and mortality. Ann InternMed 2009;150:170–7.
99. Hanratty CG, Koyama Y, Rasmussen HH, et al.Exaggeration of nonculprit stenosis severity dur-ing acute myocardial infarction: implications forimmediate multivessel revascularization. J Am CollCardiol 2002;40:911–6.
100. De Bruyne B, Pijls NH, Kalesan B, et al., FAME2 Trial Investigators. Fractional flow reserve-guided PCI versus medical therapy in stable cor-onary disease. N Engl J Med 2012;367:991–1001.
101. Ntalianis A, Sels JW, Davidavicius G, et al.Fractional flow reserve for the assessment ofnonculprit coronary artery stenoses in patientswith acute myocardial infarction. J Am Coll CardiolIntv 2010;3:1274–81.
KEY WORDS myocardial ischemia,myocardial revascularization, outcomeassessment