Embed Size (px)
Citation preview

C
1494
• Rarelyparathyroidadenomaspresentasapalpablemass.
• Radiology:m Several imaging methods have been used for
localization of hyperfunctioning parathyroidtissue, including retrograde phlebotomy fordeterminationofserumparathormonelevels,CTscanning, ultrasonography, magnetic resonanceimaging (MRI), thallium subtraction scanning,andtechnetium-99msestamibiimaging.
m Technetium-99msestamibiimagingappearstobethemost useful,with localizationofmore than90% of adenomas, and has been most widelyusedinpatientswithanatomicdistortionduetoprevious surgery and in patient who are highsurgical risks;however,more routineutilizationhasgainedsupport.
m Multidimensional CT (referred to as 4D-CT)emerging technique used in detection when alesionisnotidentifiedbymoreconventionaltech-niques(e.g.,ultrasonography,sestamibiimaging)
• May be associated with hyperparathyroidism-jawtumorsyndrome(HPT-JT):m Autosomal-dominant disorder with germline
mutation in HRPT-2 gene on chromosome1q25-31
m Characterizedby:– Parathyroidadenomaorcarcinoma– Fibro-osseouslesionsofthejaw(e.g.,ossifying
fibromaofmandibleormaxilla):30%ofcases– Renal cyst, hamartoma, carcinoma: 20% of
casesm Approximately 80% of patients develop
hyperparathyroidism:– Usuallypresentslateinadolescence– Hypercalcemiatendstobesevere.
m Higher incidence of parathyroid carcinoma incomparison with patients with MEN-1 andMEN-2A
m Renallesionsmayinclude:– Renal cysts, polycystic renal disease, renal
hamartoma– Papillary renal cell carcinoma, renal cortical
adenomas,Wilmstumor• 90%ofadenomasarefoundinparathyroidglands
intheirusuallocations:m Lowerglandsaremorecommonlyinvolved.
Chapter
Neoplasms of the Parathyroid Glands
CLASSIFICATION OF NEOPLASMS OF THE PARATHYROID GLANDS (Box 33-1)
33
BOX 33-1 Neoplasms of the Parathyroid Glands
• Parathyroid adenoma• Parathyroid carcinoma• Secondary neoplasms
PARATHYROID ADENOMA (Figs. 33-1 through 33-22, Table 33-1)
Definition:Benignneoplasmoftheparathyroidparen-chymalcells,includingchiefcellsand/oroncocyticcells.
Clinical• Morecommoninfemales(F:M=3to4:1);occur
overabroadagerangebutaremostfrequentlydis-coveredinthefourthandfifthdecades.
• Represents the major cause of primaryhyperparathyroidism
• Clinical findings are essentially the same as thoseassociatedwithprimaryhyperparathyroidismduetohyperplasia(seeChapter32).
• Asinprimaryhyperparathyroidismduetohyperpla-sia, the symptomatology in patients with parathy-roid adenomas is changing as a result of routinebiochemicalscreeningandearlydetection:m Hypercalcemiamaybeincidentallydiscoveredin
asymptomaticpatients,andmanypatientscom-plainonlyoffatigue,weakness,ordepression.
m Nephrolithiasis is documented in 69% of menand in 36% of women with adenomas overall,but the incidence has been decreasing in recentyearstobetween5%and20%.
m Severe bone disease, once a common complica-tion, is now rare; however, osteopenia is oftenpresent,andjointdiseasesimilartothatfoundinpatientswithparathyroidhyperplasiaoccurs.
• Serum calcium levels are generally higher than inpatientswithprimarychiefcellhyperplasiabutnotusuallyashighasinparathyroidcarcinoma.
• Hypophosphatemia, hyperphosphaturia, and ele-vatedserumparathormonelevelsarefound.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
b0010
p0015u0015u0020
c00034
s0010
p0010
s0015
p0035
s0025
p0040
u0030
u0035
u0040
u0045
u0050
u0055
u0060
u0065
u0070
u0075u0080
u0085
u0090
u0095
u0100
u0105u0110u0115
u0120
u0125
u0130u0135u0140
u0145u0150
u0155
u0160
u0165
Wenig_Chapter 33_main.indd 1494 4/29/2015 5:28:36 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1495
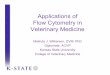
Fig. 33-1.Classic parathyroid adenoma identified on ultrasonography.
A,Sagittalultrasonographicimageshowsahypoechoic,well-definedmass(A)justbelowtheinferiorpoleoftherightthyroidgland(*).B,TransverseultrasonographicimagewithcolorflowDopplershowstheincreasedperipheralarchofvascularityofthemassfrequentlyseenwithadenomas(A).(From Som PM, Curtin HD: Head and neck imaging, ed 5, Philadelphia, 2011, Elsevier, Fig. 41-95, p 2663.)
A
* *A
B
A
• Ectopicparathyroidadenomas:m Parathyroidadenomasmayoccurinanylocation
inwhichparathyroidtissuemaybefound,includ-ingectopicsitessuchasthemediastinum,retro-esophagealsofttissue,withinthethyroidgland,orinthymictissue
m Ectopicadenomas,especiallyintrathyroidalones,maybemissedbyclinicalevaluationand/orsurgi-calexploration:– Intrathyroidal parathyroid adenomas may be
misinterpreted by pathologic evaluation as athyroid follicular lesion or medullary thyroidcarcinoma.
m Reportsofadenomasoccurringinsupernumeraryglands include tumors arising in the vagusnerve, pericardium, or other soft tissue sites intheneck.
PathologyCytology• Occasionally enlarged parathyroid glands, either
hyperplastic or, more commonly, adenomatous,have been serendipitously subjected to fine-needleaspirationasaclinicallysuspected“solitarythyroidnodule”;reportsofultrasonicallyguidedfine-needleaspirationforlocalizationandconfirmationofpara-thyroidproliferativediseasehaveappeared.
• Anawarenessofthetypicalcytologicappearanceofparathyroidtissuecanbehelpfulduringintraopera-tiveexaminationofbiopsiesduringaneckexplora-tion for hyperparathyroidism, as examination oftouchpreparationsprovidesa rapidmeansofcon-firmingthepresenceofparathyroidtissue.
• Aspirates of parathyroid tissue typically containnumerous naked nuclei, as well as small sheets ofcells, sometimes forming acinar or follicular struc-tures;smallaggregatesofdensecolloid-likematerialmaybeseenbutarenotnumerous.
• The cells are generally small, with predominantlyround nuclei; anisonucleosis in scattered cells andoccasionallarge,atypical,nakednucleiarecommon.
• Thecytoplasmisgranularandmayexhibitscatteredlarge metachromatic granules with a May-Grünwald-Giemsa or Romanowsky stain;Papanicolaou-stainedcellshavecleartofinelygranu-larcytoplasm.
• Thenucleiaregenerallyhyperchromaticwithcoarsechromatintypicalofneuroendocrinecells.
• The distinction from follicular epithelium of thethyroidmaybedifficult,althoughthecellsareusuallysmallerthanthoseofthethyroid:m Immunohistochemical staining for PTH, parafi-
bromin,chromogranin,thyroglobulin,andTTF1maybehelpfulinthisdifferentialdiagnosis.
Gross• Adenomasarealmostalwayssolitary(seebelowfor
DoubleAdenoma).• Adenomashaveroundedborders,arefirm,brownto
tan,andarecontainedwithinadelicatecapsule;theymaybeovoidorlobulated.
• A remnant of uninvolved parathyroid tissue at theperipheryofthetumormaybevisible.
• Cystic change may be present, and when markedmaymasktheneoplasticnatureoftheproliferation;markedcysticdegeneration is frequentlyassociatedwithscarringandcalcification.
• There is significant variation in weight, with mostbetween0.3and1.0g.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0010
u0170u0175
u0180
u0185
u0190
s0030
s0035
p0215
u0200
u0205
u0210
u0215
u0220
u0225
u0230
s0040
p0260
u0240
u0245
u0250
u0255
Wenig_Chapter 33_main.indd 1495 4/29/2015 5:28:37 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1496 SECTION 9 ParathyroidGlands
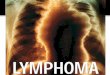
Fig. 33-2.Parathyroid adenoma.
Parathyroidadenomadetectedby201Tl/99mTc-pertechnetatesubtractionimaging(AtoC)andby99mTc-sestamibisubtractionimagingwith123I(D).A,99mTc-pertechnetateconcentratedwithinthethyroidgland.B,201Tlconcentratedwithinthyroidandparathyroidglands.C,Computertechniquesallowtechnetiumconcentratedinthethyroidglandtobesubtractedfromthalliumthataccumulateswithinthyroidandparathyroidtissue.Afterthyroidsubtraction,aparathyroidadenomaisnotedasafocusofincreasedthalliumuptake(arrows).D,99mTc-sestamibisubtractionimagingwith123Ishowsanadenomabelowtheinferiorpoleoftheleftlobeofthethyroidgland.(From Som PM, Curtin HD: Head and neck imaging, ed 5, Philadelphia, 2011, Elsevier, Fig. 41-103, p 2669.)
A B
C D
Histology• Wellcircumscribedanduncommonlysurroundedby
athinfibrouscapsule:m Completeencapsulationnotcommonlyseen
• Hypercellular proliferation lacking intraparenchy-mal fat cellswithdiffusegrowth;vaguenodularitymaybepresentandrarelymaybemultinodular.
• A rim of non-neoplastic parathyroid tissue foundin association with only about half of theadenomas:m Very helpful finding, if present, in making the
distinctionbetweenadenomaandhyperplasiam “Rim” generally contains abundant stromal fat
cells,incontrasttotheverycellularadenoma.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0015
s0045
p0290
u0265u0270
u0275
u0280
u0285
Wenig_Chapter 33_main.indd 1496 4/29/2015 5:28:38 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1497
B
*
A
C
D
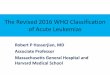
Fig. 33-3.4D-CT in the detection of a small adenoma.
A,UnenhancedCTscanatthelevelofthelowerpolesofthethyroidglandshowsnodiscreteadenoma.B,Immediatefirst-passimagefollowingcontrastadministrationshowsatiny,avidlyenhancingadenomaintherightparaesophagealregion(anteriorto*).C,Secondpassat60secondsshowssomewashoutofenhancement,whichisclearlylessthanontheimmediatepostcontrastscan.D,Lastpassdelayedimageat90secondsshowslittleenhancementoftheadenoma,whichisstillreadilyidentifiable.Onanotherpatient:E,CoronalreconstructedCTimagefromimmediatefirst-passenhancedCTscanshowsalargeadenomabelowtheinferiorpoleoftheleftthyroidlobe(arrow).
E
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0020
Wenig_Chapter 33_main.indd 1497 4/29/2015 5:28:40 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1498 SECTION 9 ParathyroidGlands
Fig. 33-4.Parathyroid adenoma.
Parathyroidadenomaappearingasalargeencapsulatedlesionbulgingintotheoperativefield.Adenomasaretypicallyeasilydissectedfreeofadjacentstructures;difficultyinremovingaparathyroidtumorshouldraisesuspicionforaparathyroidcarcinoma.
Fig. 33-5.Parathyroid adenoma.
Cutsectionofaparathyroidadenomashowsahomogeneous,lighttanappearance;adelicateinconspicuouscapsuleispresent.Aremnantofuninvolvedparathyroidtissueisnotgrosslyvisible.
F G
**
F,Coronalmaximumintensityprojectionimageinanteriorprojectionshowstheadenoma(arrow).G,Coronalmaximumintensityprojectionimageintheposteriorprojectionshowstheadenoma(*)posteriortothecommoncarotidartery.(Cases courtesy of Dr. Lawrence Ginsberg. From Som PM, Curtin HD: Head and neck imaging, ed 5, Philadelphia, 2011, Elsevier, Fig. 41-101, p 2667.)
Fig. 33-3, cont’d
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0025
f0030
Wenig_Chapter 33_main.indd 1498 4/29/2015 5:28:41 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1499
m Nuclei of residual normal or atrophic parathy-roidglandtypicallysmallerthanthenucleioftheadenoma.
• Growthpatternsincludesolid(diffuse)sheets,cords,nests,acini,follicles,andmicrocysts:m Follicle formation may contain eosinophilic
“colloid-like”material.m Distincttrabecularpatternisuncommon.
• Predominantlycomposedofchiefcells:m Nucleiroundandregularwithcentraltoslightly
basal location within the cell and have incon-spicuous nucleoli; usually lack significantpleomorphism:– Cells with hyperchromatic enlarged nuclei as
well as multinucleated cells are common andcanbe found scattered throughout the tumoror may be clustered in small foci; these scat-tered atypical nuclei are not an indicator ofmalignancy in the absence of other evidenceof a malignancy (see section on parathyroidcarcinoma).
m Cytoplasmvaries,includingslightlyeosinophilic,amphophilic,clear,oroxyphilic.
m Chiefcellsofanadenomafrequentlylargerthanthe non-neoplastic chief cells in the uninvolvedrimofparathyroidtissue,ifoneispresent
m Oncocyticcellsmaybeseeninvariablenumbers,focally admixed with chief cells or as nodularaggregates.
• Mitotic figures are identifiable in many adenomas,butusuallynumberfewerthan1per10high-powerfields;mitoticratesashighas4mitosesper10high-powerfieldshavebeendescribedinoccasionalcases.
• Delicate vascular network composed of thin fibro-vascularstroma,sinusoid-likebloodvesselsorcapil-lariestraversetheneoplasm.
Fig. 33-6.Parathyroid adenoma.
Parathyroidadenomaappearingasanodularfocuswithcysticchangeandassociatedcalcification.
Fig. 33-7.Parathyroid adenoma, fine-needle aspiration.
A,Cellularsmearwithcohesivegroupsofsmallepithelialcellsandfragmentsofpinkcolloid-likematerialmaysuggestafollicularneoplasmofthyroidorigin;thecolloid-likematerial,however,issomewhatsparse(Diff-Quickstain).B,Thecellsarefragile,yieldingsmearswithnumerousnakednuclei,someofwhicharelargeandhyperchromatic;scatteredlargeatypicalnucleiarecommoninparathyroidadenomas(Diff-Quick).C,Papanicolaou-stainedsmearshowsscatteredcompactclustersofsmallepithelialcellswithdistinctcellbordersandarimofclearcytoplasm;thenucleiaresmallandhyperchromatic.
A
B
C
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0035 f0040
u0290
u0295
u0300
u0305u0310u0315
u0320
u0325
u0330
u0335
u0340
u0345
Wenig_Chapter 33_main.indd 1499 4/29/2015 5:28:43 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1500 SECTION 9 ParathyroidGlands
Fig. 33-8.Parathyroid adenoma.
A,Parathyroidadenomacharacterizedbyhypercellularproliferationdevoidofintraparenchymalfat,whichinthelowerportionoftheillustrationhasawell-definedcapsuleseparatingthecellularproliferationfromathinrimofcompressednormalparathyroidglandparenchyma.B,Athighermagnification,thecellsandnucleioftheadenoma(bottom)arelargerthanthoseoftheresidualnon-neoplasticparathyroidglandparenchyma(top).
A
B
Fig. 33-9.Parathyroid adenoma.
A,Diffuseproliferationofchiefcellswithscatteredadmixedoncocyticcells.B,Tumoristraversedbydelicatefibrovascularstroma.
A
B
• Intraparenchymalfatcellsabsentbutmayfocallybeseenassinglecellsorgroupsintheperipheralaspectoftheneoplasm:m Neoplasticcellsusuallyhavelessintracellularfat
thandothecellsintheuninvolved(orsuppressed)parathyroidtissue,eitherinotherglandsorinarim of non-neoplastic parathyroid tissue in anadenomatousgland.
• Cells with markedly enlarged and hyperchromaticpleomorphic or bizarre-appearing nuclei may bepresentandwhenpresent:m Appearadmixedwithbland-appearingnuclei.m Tendtobefocallyandnotdiffuselyidentified.m Occurintheabsenceofincreasedmitoticactivity
and/orotherfeaturesthatmaybeassociatedwithparathyroidcarcinoma.
• Reactiveanddegenerativechangesmaybepresent,including cyst formation, edema, fibrosis, hemor-rhage (freshor in the formofhemosiderindeposi-tion),orinfarction:m Mayoccurspontaneouslyormayoccurfollowing
a traumatic event such as prior surgery to theneckorfine-needleaspirationbiopsy
m Presence of reactive and degenerative changes,especiallyfibrosis,maycauseadherencetoadja-centstructures,suggestinginvasivegrowthandapossiblediagnosisofparathyroidcarcinoma.
m Infarctedtumormayretainantigenicityforpara-thyroidhormone.
• Rarely,anassociatedmature lymphocyticcell infil-tratemaybepresent.
• Uninvolvedparathyroidparenchymalcellsinpatientswithadenomasaretypicallysmallerandoftenhavemore stromal fat cells than the glands in patients
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0045
f0050
u0350
u0355
u0360
u0365u0370u0375
u0380
u0385
u0390
u0395
u0400
u0405
Wenig_Chapter 33_main.indd 1500 4/29/2015 5:28:45 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1501
Fig. 33-10.Parathyroid adenoma.
Parathyroidadenomasmaybecomposedofanadmixtureof(A)chiefcells,(B)oncocyticcells,and/or(C)clearcells.Inanygiventumortwoorallofthecelltypesmaybepresent,creatingamosaicpattern.
A
B
C
Fig. 33-11.IHC staining in parathyroid adenoma.
Lesionalcellsofparathyroidadenomasareimmunoreactivefor(A)parathyroidhormoneand(B)parafibromin(diffusenuclearstaining).
A
B
Fig. 33-12.Parathyroid adenoma.
Parathyroidadenomashowingcord-likeortrabeculargrowthcomposedofcellswithclear-appearingcytoplasm.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0055 f0060
f0065
Wenig_Chapter 33_main.indd 1501 4/29/2015 5:28:49 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1502 SECTION 9 ParathyroidGlands
A
B
C
Fig. 33-13.Parathyroid adenoma.
A,Parathyroidadenomashowingafollicularpatternofgrowth(so-calledfollicularvariant)thatmaycauseconfusionwiththyroidfollicularneoplasms;immunoreactivityfor(B)parathyroidhormoneand(C)parafibromin(nuclear),coupledtotheabsenceofthyroglobulinandTTF1(notshown)allowfordifferentiatingparathyroidadenomafromathyroidfollicularlesion.
Fig. 33-14.
A,Parathyroidadenomacomposedofuniformandbland-appearingnucleiinlowerportionofimageaswellasnumerouslargecellswithhyperchromaticnuclei;intralesionalfibrosisisalsopresent.B,Bizarre-appearingpleomorphicandhyperchromaticnucleiadmixedwithbland-appearingnuclei.Suchfindingsintheabsenceofincreasedmitoticactivityand/orotherfeaturesassociatedwithparathyroidcarcinomacanbeseeninparathyroidadenomas.
A
B
without hyperparathyroidism; they also have morecytoplasmicfat,oftenfoundaslargedroplets,thannormallyfunctioningparathyroidglands.
• Histochemicalstains:m Colloid-like material in follicular structures are
PASpositive.m Considerablevariationintheliteratureregarding
theutilityof fat stains in thediagnosisofpara-thyroidproliferativediseases
m Generally, hyperfunctioning cells have a signifi-cantly decreased amount of intracellular fat(usingSudanblackoroilredO)comparedwith
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0070
f0075
u0410u0415
u0420
u0425
Wenig_Chapter 33_main.indd 1502 4/29/2015 5:28:52 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1503
normalorsuppressedparenchymalcells;thereis,however,variabilityinthisfinding.
m Fat stains, when used with adequate clinicalinformation, intraoperative findings, and histo-logicexamination,areuseful if their limitationsarekeptinmind.
• Immunohistochemistry:m Positiveforparathyroidhormoneandparafibro-
min(nuclearstaining):– Majority of parathyroid adenomas express
parafibromin– Loss of parafibromin expression may be
seeninpatientswithhyperparathyroidism-jawtumorsyndromeindicativeofgeneinactivationthroughmutationoftheHRPT-2gene.
m Cytokeratin,chromograninApositivem Calcitonin and synaptophysin typicallynegative
but in smallpercentageof casesmaybe focallypositive
m PAX8 (nuclear) reactivity present in approxi-mately40%ofadenomasandhyperplasia
m Galectin3rarelypositive(<5%).m Ki67(MIB1)proliferativeindexislow:
– Anindexgreaterthan5%shouldraisesuspi-cionforcarcinoma,butthediagnosisofcarci-noma requires confirmatory diagnosticfindings.
– Proliferativeindicesindifferentiatingadenomafrom carcinoma are of limited utility givenoverlappingfindingsintheselesions.
Fig. 33-15.Parathyroid adenoma.
Parathyroidadenomawithassociatedreactiveanddegenerativechanges,includingfibrosisandhemorrhagemayresultinadherencetosurroundingstructures,clinicallysuggestingapossiblediagnosisofparathyroidcarcinoma.Suchchangesmayoccurspontaneouslyormayoccurfollowingatraumaticeventsuchaspriorsurgerytotheneckorfine-needleaspirationbiopsy.
Fig. 33-16.Parathyroid adenoma.
A,Parathyroidadenomawithinfarctionbutretentionofghostoutlinesoftheneoplasm.Notetheresidualnoninfarctedandnon-neoplasticparathyroidparenchyma,includingmaturefat(upper right).B,Parathyroidhormoneimmunoreactivityispresentintheinfarctedtumorandintheresidualnon-neoplasticparathyroidparenchyma(upper right).
A
B
m CyclinD1stainingin39%ofcasesm NegativeforthyroglobulinandTTF-1
• Electronmicroscopy:m Adenomas associated with very high serum
calciumlevelsmayhavealargenumberofmicro-villi,whicharethoughttoreflectahigherlevelofendocrineactivity
m Adenomas often have more abundant roughendoplasmic reticulum and more prominentGolgiapparatusthannon-neoplasticcells.
m Annulatelamellaemaybeseen.• Cytogeneticandmolecularfindings:
m Approximately5%showpericentricinversionofchromosome11,causing translocationofcyclin
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0080 f0085
u0430
u0435u0440
u0445
u0450
u0455u9160
u9165
u0460u0465u0470
u0475
u0480u0485u0490u0495
u0500
u0505u0510u0515
Wenig_Chapter 33_main.indd 1503 4/29/2015 5:28:53 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1504 SECTION 9 ParathyroidGlands
m Distinction between hyperplasia and adenomamay be extremely difficult and requires thepathologic examination of more than a singlegland.
• Diagnosticcriteriafordoubleadenomasinclude:m 2enlarged,hypercellularparathyroidglandsm Intraoperativeconfirmationthatremainingpara-
thyroidglandsarenormaland/orbiopsyprovenhistologicallynormalparathyroidglands
m Absence of family history of MEN or familialhyperparathyroidism
m Permanentcureofhypercalcemiafollowingexci-sionofenlargedglands:– Arguablythemostdefinitivecriterion– Requires years of follow-up to include moni-
toring of serum calcium and parathyroidhormonelevels
D1 (CCND-1/PRAD-1) gene with parathyroidhormone gene, resulting in overexpression ofcyclinD1.
m Somatic mutation in MEN-1 gene at 11q13 in40%ofcases
m AbsenceofRETmutationm 5% have somatic mutation in CDKN1B gene
(p27Kip1)
Double Parathyroid Adenomas• Most“multipleadenomas”representcasesofasym-
metricornodularhyperplasia:
Fig. 33-17.Intrathyroidal parathyroid adenoma.
A,Intrathyroidalparathyroidadenoma(lower)predomi-nantlycomposedofchiefcellsaswellasoncocyticcells(arrow)andclearcells(arrowhead)surroundedbythyroidfollicularepithelialcellsandanadenomatoidnodule(upper right).B,Histologically,theintrathyroidalparathyroidadenomashowstypicalmorphologicfindingspredominantlycomposedofchiefcellsandsharplyseparatedfromthecolloid-filledthyroidfollicles(left side).
A
BFig. 33-18.Oncocytic parathyroid adenoma.
A,Thetumorisencapsulatedand(B)exclusivelycomposedofcellswithgranulareosinophilic-appearingcytoplasm.
A
B
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0090
f0095
u0520
u0525u0530
s0050
p0570
u0540
u0545u0550u0555
u0560
u0565
u0570u0575
Wenig_Chapter 33_main.indd 1504 4/29/2015 5:28:56 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1505
Fig. 33-19.Parathyroid lipoadenoma.
Lipoadenomasformcords,islands,andfolliclesadmixedwithstromalfatcellswithmatureadipocytes,thelattermakingupfrom20%to90%oftheneoplasm.Lipoadenomasareencapsulatedandmaybeassociatedwitharimof“normal”gland(notshown)andcanbedifficulttodistinguishfromnormalparathyroidglandinsmallbiopsies.
Fig. 33-20.Parathyroid adenoma associated with osteitis fibrosa cystica.
Left panel,Theadenomaistypicalwithadistinctcapsuleandarimofnormalparathyroidparenchymaincludingmaturefat(lower);right panel,thetumoriscomposedofchiefcells.Thepatienthadapathologicfractureofthehumerusaswellasgeneralizedosteopeniawithmultiplelyticskeletallesions.Atthetimeofpresentationhehadhypercalcemia.Theinitialclinicalimpressionwasmetastaticcarcinomawithsecondaryhypercalcemia.
Fig. 33-21.Brown tumor of hyperparathyroidism.
ThehumerallesionfromthepatientinFig.33-20.Left panel,Dissectingosteitis,withresorptionoftrabecularboneandreplacementbyfibroustissue;thepresenceofhemosiderinindicateshemorrhagesecondarytomicrofracturesintheweakenedbone.Right panel,Browntumorofhyperparathyroidismdevelopsafterrepeatedcyclesofboneresorption,microfractures,andhemorrhage,leadingtolargeareasofcysticdegenerationwithaggregatesofosteoclastsandforeignbodygiantcellsinafibroblasticstromacontaininghemosiderin.
• Iftheabovecriteriaarefulfilled,thenadiagnosisofdoubleadenomascanbeconfirmed.
• Truedoubleparathyroidadenomasarerare:m Majority(greaterthan70%)arebilateralm Predilectstosuperiorglands
Histologic Variants of Parathyroid Adenoma• Oncocytic(oxyphilic)adenoma(seeFig.33-18):
m Exclusively composed of oncocytic cells withprominenteosinophilicgranularcytoplasm
m Demographicfeaturesaresimilartothoseofthemorecommonadenomascomposedofchiefcells
m Thoughttobenonfunctional;usuallyassociatedwith lesser degree of hypercalcemia; however,several reports document an association withprimaryhyperparathyroidism
m Composed of large cells with abundant eosino-philic granular cytoplasm and hyperchromaticnuclei:– Scattered large atypical nuclei or multinucle-
atedcellsmaybeseen.– Cytoplasm is stuffed with mitochondria on
electronmicroscopy.m Animportantdifferentialconsiderationisthefre-
quentpresenceofnodularoncocyticcellchangeseeninnormalglandswithincreasingage.
m Intrathyroidallocalizationmaysuggestadiagno-sis of an oncocytic thyroid follicular (so-calledHürthlecell)neoplasm:– Parathyroid oncocytic adenomas have more
distinctcellmembranes.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0100
f0105
f0110
u0580
u0585u0590u0595
s0055
p0640u0605
u0610
u0615
u0620
u0625
u0630
u0635
u0640
u0645
Wenig_Chapter 33_main.indd 1505 4/29/2015 5:28:57 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1506 SECTION 9 ParathyroidGlands
m Circumscriptionand/orencapsulationaswellaslarge size (1 to 15cm) support adenomatousnature:– May be associated with a compressed rim of
“normal”glandm May be difficult to recognize as “abnormal”
parathyroid tissue in small biopsies, when theyareeasilymistakenfornormalparathyroidtissuebecauseoftheabundanceofstromalfat
m Stromal fat often contains areas of fibrosis ormyxoidalteration.
m Mostareassociatedwithhyperparathyroidism.• Otherrarevariantsofparathyroidadenomainclude:
m Papillary variant characterized by prominentpapillaryarchitecture:– May not be a “true” variant but papillary
architecture, especially in association withfibrosis and hemorrhage (recent and remote),likelyisareactive/degenerativephenomenon
m Follicular variant characterized by prominentfollicular(acinar)architecture
m Water-clearvariantcharacterizedbypresenceofpolygonalcellswithclearcytoplasmanddistinctcellmembranes.
• Atypicalparathyroidadenoma:m Definition: parathyroid tumor showing features
worrisomeforparathyroidcarcinomabutlackingabsolute diagnostic features for parathyroidcarcinoma
m Synonymsincludeatypicalparathyroidneoplasm,parathyroidneoplasmof uncertain biologic sig-nificance, or parathyroid neoplasm inconclusiveformalignancy
m Atypicalhistologicfeaturessuggestingcarcinomabutfallingshortforthisdiagnosismayinclude:– Capsular irregularities or invasion without
infiltrationintoadjacentsofttissues– Increased mitotic activity (>5 per 10 high-
powerfields)– Intralesional fibrosis characterized by broad
fibrousbandscoursingthroughthelesion– Coagulativenecrosis– Diffusecellularatypia– Diffuse sheet-like growth of monotonous
cells with increased nuclear-to-cytoplasmicratio
– Macronucleoliinmanycellsm Atypical parathyroid adenomas lack conclusive
featuresdiagnosticforcarcinomaincluding:– Invasionofsurroundingsofttissues– Invasion of surrounding structures including
thyroidgland,larynx,trachea,pharynx,esoph-agus,carotidartery,recurrentlaryngealnerves
– Angioinvasion– Perineuralinvasion– Metastasis
– Presence of thyroglobulin and TTF1 supportlesionofthyroidorigin.
• Lipoadenoma(seeFig.33-19)m Alsoreferredtoasparathyroidhamartomam Rarebenignneoplasmcharacterizedbyprolifera-
tion of chief and oxyphilic cells forming cords,islands, and follicles admixed with matureadipocytes:– Matureadipocytesmakeupfrom20%to90%
oftheneoplasm.
Fig. 33-22.Brown tumor of hyperparathyroidism.
Browntumorofhyperparathyroidismcharacterizedby(A)proliferationofnumerousmultinucleatedgiantcellsandmononuclearcells,aswellasfociofhemorrhage;thegiantcellstendtobeclusteredratherthandiffuselydistributed.B,Thenucleiofthemultinucleatedgiantcellsareratherblandandaresimilartothoseofthesurroundingmononuclearcells.Amitoticfigure(arrow)ispresent.Thebrowntumorofhyperparathyroidismishistologicallysimilartogiantcell(reparative)granuloma,therebyrequiringclinicalandlaboratorycorrelationtodifferentiatetheselesions.
A
B
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0115
u0650
u0655u0660u0665
u0670
u0675
u0680
u0685
u0690
u0695u0700u0705
u0710
u0715
u0720
u0725u0730
u0735
u0740
u0745
u0750
u0755
u0760u0765u0770
u0775u0780
u0785u0790
u0795u0800u0805
Wenig_Chapter 33_main.indd 1506 4/29/2015 5:28:58 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1507
TABLE 33-1 Comparative Features of Parathyroid Proliferative Diseases
Hyperplasia Adenoma Carcinoma
Gender; age Slight female predilection; most common in 5th-6th decades
More common in women; most common in 4th decade
Equal gender predilection; wide age range
Clinical Asymptomatic or complaints of lethargy, weakness, polyuria, polydipsia, arthralgia, constipation, and depression
Similar to hyperplasia Similar to hyperparathyroidism of benign cause but more severe due to the higher serum calcium levels; higher proportion of renal disease (nephrolithiasis) and bone disease; peptic ulcer disease; palpable neck mass more common than in adenoma
Serum calcium 11.7 mg/dl (average) 12.5-13.5 mg/dl Often >14 mg/dl
Intraoperative findings
2 or more glands enlarged, easily dissected; enlargement may be very asymmetric
1 gland enlarged; easily dissected; more frequent in lower glands or ectopic sites
1 gland enlarged; often adherent to surrounding tissues
Weight Total gland weight usually <1 g, but may be up to 5 g
0.3-1.0 g commonly, but may weigh several grams in patients with bone disease
>1.5 g (often much larger)
Capsule Circumscribed by capsule of parathyroid gland, may be incomplete. No compressed rim of atrophic or normal parathyroid tissue
Thin tumor capsule, often surrounded by rim of uninvolved parathyroid, which may appear atrophic
Thickened capsule; rim of normal parathyroid rarely seen
Gross appearance Gray-brown, soft. Cut surface may be homogeneous or nodular. Lacks fibrous bands
Red-brown, firm. Usually homogeneous, lacks fibrous bands
Gray-white, firm, often lobulated or irregular. Fibrous bands often produce coarse nodularity
Histologic pattern Diffuse or nodular, sometimes pseudofollicular or acinar
Diffuse or nodular, frequently pseudofollicular or acinar
Diffuse, nodular, pseudofollicular, or acinar; often trabecular pattern with distinctive nuclear palisading predominates
Cytologic features Chief cells predominate; transitional and oncocytic cells often present
Chief cells predominate, but mixture of chief, transitional, and oncocytic cells may be seen; rarely, purely oncocytic
Cells usually resemble chief cells, but variable cytoplasmic oncocytic change may be seen; cell borders often indistinct
Intracytoplasmic lipid
Decreased Decreased in tumor; abundant in atrophic rim of parathyroid
Usually absent
Stromal fat cells Scanty to absent Usually absent in tumor; present rim of atrophic parathyroid
Absent
Nuclear morphology Normal to slightly increased N-to-C ratio; usually without nuclear pleomorphism
Nuclei enlarged, with variability in size; scattered groups of large pleomorphic, hyperchromatic nuclei, or multinucleated cells
Increased N-to-C ratio; enlarged atypical nuclei; often with monotonous (bland appearing) nuclei
Nucleoli Inconspicuous to small Inconspicuous to small Frequently prominent and enlarged
Mitoses Common (60% of cases; most with <1 mitotic figure/10 HPF)
Common (70% of cases; most with <1 mitotic figure/10 HPF)
Common (80% of cases), may include atypical mitoses; may be numerous
Continued
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
t0010
Wenig_Chapter 33_main.indd 1507 4/29/2015 5:28:58 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1508 SECTION 9 ParathyroidGlands
Hyperplasia Adenoma Carcinoma
Capsular and vascular invasion
Absent Absent; entrapment of tumor cells may occur in capsule if degenerative changes present
Capsular invasion present in two thirds; may involve only capsule or extend into adjacent tissues
Vascular invasion present in up to 15%; usually in capsular vessels
Remainder of gland Entire gland is abnormal Normal or atrophic Normal
Degenerative changes
May be seen in very large glands
Includes hemorrhage, areas of fibrosis, and cystic change
Common, especially in larger adenomas; includes hemorrhage, fibrosis, and cystic change, sometimes calcification
Tumor cell necrosis; calcification and cystic changes may be present
Treatment Subtotal parathyroidectomy with surgical removal of three glands, leaving a remnant of the 4th or total parathyroidectomy* with autotransplantation of parathyroid tissue in forearm
Surgical removal of the enlarged gland
En bloc resection, including ipsilateral thyroid lobe and adjacent soft tissues
Prognosis Excellent Excellent Up to 50% of patients are cured by en bloc resection; considered an indolent malignancy even in presence of recurrence or metastasis with long survival even after recognition of tumor recurrence; morbidity and mortality correlate to complications of severe hypercalcemia
Recurrence and metastasis
Recurrence in approximately 16% of cases due to inadequate neck exploration and may not be evident for years
Absent Recurrence in two thirds of patients usually within 3 years of the first surgery; metastasis is 35%, is a late event usually preceded by local recurrence; most commonly to lung, cervical lymph nodes, and liver
Familial and/or MEN association
Yes, in approximately 20% of cases
Uncommon Rare
TABLE 33-1 Comparative Features of Parathyroid Proliferative Diseases—cont’d
g, Grams; HPF, high power fields; MEN, multiple endocrine neoplasia syndrome; N-to-C, nuclear-to-cytoplasmic.*Particularly in cases of familial hyperparathyroidism.
m Mostatypicalparathyroidadenomasprovetobebenigninlong-termfollow-up,butowingtotheuncertainty in their malignant potential, theyhavebeentermedatypical.
m Treatment is similar to a typical parathyroidadenoma, but patients should be followed forpotential recurrent hyperparathyroidism, localrecurrence of tumor, and/or evidence of aggres-sivebehavior(e.g.,metastasis).
Differential Diagnosis• Primarychiefcellhyperplasia(seeTable33-1)• Parathyroidcarcinoma(seeTable33-1)• Follicularneoplasmofthyroidgland
Treatment and Prognosis• Mostwidelyacceptedtherapyisexcisionoftheade-
nomatous gland with biopsy of at least one addi-tionalglandthatis“normal”insize
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
u0810
u0815
s0060
p0865u0825u0830
s0065
p0885
Wenig_Chapter 33_main.indd 1508 4/29/2015 5:28:58 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1509
• Some favor a full bilateral neck exploration withsubtotal parathyroidectomy and have reported alower incidence of recurrent hypercalcemia thatrequiredreoperation:m There isanincreasedincidenceofpostoperative
hypoparathyroidismwiththisprocedure.• Recurrence rates vary significantly and may reflect
problems in classification, particularly in cases ofhyperplasiawithnodules,whichmayerroneouslybedesignatedasadenomas.
• Although generalized osteopenia is now morecommon, osteitis fibrosa cystica, also known asbrowntumorofhyperparathyroidismisoccasionallyseen(seeFigs.33-20to33-22):m Mayoccurinhyperparathyroidismofanycause
but is related to degree and duration of serumcalciumelevation
m Lesionsarecharacterizedbyresorptionofbone,whichisreplacedbyfibroustissue,probablyasareparativeresponsetomicrofractures
m Hemorrhagewithinthefibroustissueleadstotheaccumulationofhemosiderinandaproliferationof multinucleated giant cells in addition to theosteoclasts
m With timedegenerative changes lead to the for-mationofcysticspaces
m Osteitis fibrosa cystica cannot be distinguishedhistologically from the giant cell (reparative)granuloma of the jaw; clinical information isessential.
• Recurrent hyperparathyroidism following surgeryfor an adenoma may also result from incompleteexcision,ruptureofthetumorcapsulewithspillageinto the operative field, or from hyperfunction ofautografted parathyroid tissue following subtotalparathyroidectomy.
PARATHYROID CARCINOMA (Figs. 33-23 through 33-38, see Table 33-1)
Definition:Malignantneoplasmofparathyroidparen-chymalcells.
Clinical• Rare neoplasm; responsible for approximately 2%
ofcasesofhyperparathyroidism• Nogenderpredilection;most common infifthand
sixthdecades:m Affectpatientsapproximatelyadecadeyounger
thanthosewithadenomasm Rarecasesreportedinchildren
• Clinicalfindings associatedwithparathyroid carci-nomaarelistedinBox33-2.
• Most patients have severe hypercalcemia andhypophosphatemia:m Mean serum calcium 14.0mg/dl, in contrast to
mean serum calcium of 12.0mg/dl in benignhyperparathyroidism
• Occasionalnormocalcemicpatientsmayoccur.• Symptomsareduetoexcessiveparathyroidhormone
secretion and are similar to those in patients withhyperparathyroidismofbenigncausebuttendtobemoresevereduetothehigherserumcalciumlevels:m Presenting symptoms include polyuria, polydip-
sia,fatigueandweakness,depression,bonepainand fracture (high incidence in earlier series),renalcolicandnephrolithiasis(uptotwothirdsofpatientsinearlierstudies,butprobablydecreas-ingwithroutinebiochemicalscreeningandearlierdetection), peptic ulcer disease, and recurrentpancreatitis.
• Palpableneckmassesmorecommonthaninhyper-plasiaoradenoma.
• Etiologyisunknown:m Mostcasesaresporadic.m Lossoftheretinoblastoma(Rb)tumor-suppressor
genemayplayanimportantroleinthedevelop-mentofparathyroidcarcinoma,and itsabsencemay be helpful in distinguishing parathyroidadenomafromcarcinoma.
m Some cases occur in hyperparathyroidism-jawtumor syndrome, MEN, or familial isolatedhyperparathyroidism.
m Externalbeamirradiationtotheneckmaybeapossibleriskfactor.
m Rare cases occur in patients with secondaryhyperparathyroidism,possiblylinkingthedevel-opmentofparathyroidcarcinomafromparathy-roidadenomaorhyperplasia.
• May be associated with hyperparathyroidism-jawtumorsyndrome(HPT-JT):m Autosomal-dominant disorder with germline
mutation in HRPT-2 gene on chromosome1q25-31
m Characterizedby:– Parathyroidadenomaorcarcinoma– Fibro-osseouslesionsofthejaw(e.g.,ossifying
fibromaofmandibleormaxilla):30%ofcases
BOX 33-2 Clinical Features Associated with Malignancy in Parathyroid Neoplasms
• Serum calcium level >14 mg/dl• Serum parathormone levels 2 to 3 times normal• Severe metabolic manifestations: nephrolithiasis, bone
disease, etc.• Palpable neck mass• Difficulty in surgical dissection owing to adherence to
surrounding structures
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
b0015
p0980u0920u0925
u0930u0935
u0840
u0845
u0850
u0855
u0860
u0865
u0870
u0875
u0880
u0885
s0070
p0945
s0080
p0950
u0895
u0900
u0905u0910
u0940
u0945
u0950u0955
u0960
u0965
u0970u0975u0980
u0985
u0990
u0995
u1000
u1005
u1010u1015u1020
Wenig_Chapter 33_main.indd 1509 4/29/2015 5:28:58 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1510 SECTION 9 ParathyroidGlands
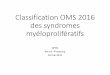
Fig. 33-23.Parathyroid carcinoma in a patient with severe hyperparathyroidism.
A,AxialT2-weightedMRimageshowsademarcated2.5-cmmediastinalmass(*)thatrepresentsaparathyroidcarcinoma.B,AxialT2-weightedMRimageofanotherpatientwithhypercalcemiashowsanonhomogeneousmassintherighttracheoesophagealgroove.Themarginsareslightlyunsharp.Thisisaparathyroidcarcinoma.C,AxialT2-weightedMRimageshowsalargemassintherighttracheoesophagealgrooveinthispatientwithseverehypercalcemia.Atsurgery,thiswasaparathyroidcarcinoma.(From Som PM, Curtin HD: Head and neck imaging, ed 5, Philadelphia, 2011, Elsevier, Fig. 41-110, p 2674.)
A
*
B
C
– Renal cyst, hamartoma, carcinoma: 20% ofcases
– Approximately 80% of patients develophyperparathyroidism.
– Usuallypresentslateinadolescence– Hypercalcemiatendstobesevere.
m Higher incidence of parathyroid carcinoma incomparison with patients with MEN-1 andMEN-2A
m Renallesionsmayinclude:– Renal cysts, polycystic renal disease, renal
hamartoma– Papillary renal cell carcinoma, renal cortical
adenomas,Wilmstumor
Radiology• Imagingproceduresareofsimilarutilityasinpara-
thyroidadenomas.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0120
u1025
u1030
u1035u1040u1045
u1050u1055
u1060
s0085
p1135
Wenig_Chapter 33_main.indd 1510 4/29/2015 5:28:59 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1511
Pathology• Pathologicfindingspotentiallyassociatedwithpara-
thyroidcarcinomaarelistedinTable33-2.
Gross• Average size is larger than parathyroid adenomas:
mean weight 6.7g (range 1.5 to 27g), althoughsmaller tumors are being identified more often inrecentyears.
• Maybeencapsulatedorinfiltrative
Fig. 33-24.Parathyroid carcinoma.
Parathyroidcarcinomaappearingasalargetumorwithareasofcysticdegenerationassociatedwithlargenodulesofviabletumor;thecapsuleisgrosslythickened.
Fig. 33-25.Parathyroid carcinoma.
Parathyroidcarcinomaappearingasanirregular,infiltrative,indurated,whiteneoplasmadherenttotheadjacentthyroidlobe(on the left).Difficultiesindissectionaparathyroidlesionfromadjacentstructuresissuggestive,althoughnotdefinitivelydiagnostic,forcarcinoma.Histologicconfirmationisalwaysrequiredforadiagnosisofparathyroidcarcinoma.
Fig. 33-26.Parathyroid carcinoma.
Someparathyroidcarcinomaslikethisonearemoreadvancedatpresentationwithextensiveinvasionofsurroundingtissues.Casessuchasthisoneareraretodayasaresultofroutinebiochemicalscreeningofmostpopulationsindevelopedcountries.
Fig. 33-27.Parathyroid carcinoma.
Parathyroidcarcinomacharacterizedbyathickenedcapsule,andfibrousbandsdissectingthroughthetumordividingthetumorintoseparatenodules;thetumorwasadherenttoandinvadedintothethyroidgland(right).
• Browntogray-white,carcinomasmayhaveasmooth,firmcutsurfaceindistinguishablefromanadenomaormaybedistinctlyindurated
• Difficulty indissectionofthetumorandadherenceto the thyroid gland are common intraoperativeobservations.
Histology• Histologic criteria in diagnosing parathyroid carci-
nomaaredetailedinTable33-2.• Manyparathyroidcarcinomasareencapsulated,and
usually the capsule of a carcinoma is thicker thanthatseeninmostadenomas:m Some adenomas with reactive and degenerative
changeshavethickandunevencapsules.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0125
f0130
f0135
f0140
s0090
p1145
s0095
p1255
u1180
u1185
u1190
s0100
p1280
u1200
u1205
Wenig_Chapter 33_main.indd 1511 4/29/2015 5:29:00 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1512 SECTION 9 ParathyroidGlands
Fig. 33-28.Parathyroid carcinoma.
Parathyroidcarcinomawithacellularfibrousbandscoursingthroughtheneoplasmdividingthetumorintomultiplenodules.
Fig. 33-29.Parathyroid carcinoma.
Parathyroidcarcinomashowingvascularinvasionwithinanendothelial-linedbloodvessel.
Fig. 33-30.Parathyroid carcinoma.
Parathyroidcarcinoma(P)withperineuralinvasion(arrows).Theneoplasticproliferationincludesratherbland-appearinganduniformnuclei,butthepresenceofneurotropismrepresentsinvasivegrowthdiagnosticforcarcinoma.
P
Fig. 33-31.Parathyroid carcinoma.
Parathyroidcarcinomacharacterizedbyhypercellularityandtrabeculargrowth.
TABLE 33-2 Pathologic Features Associated with Malignancy in Parathyroid Neoplasms
Features Definitively Diagnostic for MalignancyFeatures Worrisome for But Not Definitively Diagnostic for Malignancy
• Invasive growth including into:Surrounding soft tissuesSurrounding viscera or vital structures (thyroid gland,
larynx, trachea, esophagus, pharynx, carotid artery, recurrent laryngeal nerve)
• Vascular invasion• Perineural invasion• Metastatic disease:
Regional lymph nodesDistant sites
• Large size (mean weight 6.7 g)• Adherence to surrounding structures (e.g., thyroid tissue, others)• Irregular contour; lack of distinct encapsulation• Thick capsule• Intralesional fibrous bands• Mitotic activity (especially >5 per 10 HPF)• Coagulative tumor necrosis• Diffuse cellular atypia• Diffuse sheet-like monotonous small cells with increased N : C• Macronucleoli in many tumor cells• Trabecular growth• Spindling of tumor cells
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0145
f0150
f0155
f0160
t0015
u1075u1080u1085
u1090u1095u1100u1105u1110
u1130u1135
u1165u1170
Wenig_Chapter 33_main.indd 1512 4/29/2015 5:29:02 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1513
evenfocally,shouldraisesuspicionforthediag-nosisofcarcinoma.
m Nuclearpalisadingmaybeprominentintrabecu-larareas.
m Spindlingofcellsisalsoafeaturemoreoftenseenincarcinomasthaninbenignproliferations.
m Trabecular pattern and spindle-shaped cells,although worrisome for a possible diagnosis ofcarcinoma,arenotdefinitivediagnostic featuresforcarcinoma.
• Growthpatternsalsovaryandincludesolidsheets,acinarformation,cords,rosettes,and,ofparticulardifferential diagnostic significance, trabecularpattern:m Trabecularpatternisafindingmoreoftenidenti-
fied in association with parathyroid carcinomathaninadenomaorhyperplasia,anditspresence,
Fig. 33-33.Parathyroid carcinoma.
Acomparisonofthenucleiinparathyroidcarcinoma(left)withparathyroidadenoma(right)showsthecellsofthecarcinomatohaveahighernuclear-to-cytoplasmicratiothanthoseoftheadenoma.Suchafeatureisworrisomebutintheabsenceofotherfindingsisnotdiagnosticforcarcinoma.
Fig. 33-34.Parathyroid carcinoma.
Parathyroidcarcinomawithspindle-shapedtumorcells.
Fig. 33-35.Parathyroid carcinoma with mitotic figure (arrow).
Mitosesarenot,bythemselves,accuratepredictorsofmalignancy,becausetheymaybeseeninparathyroidhyperplasiaandadenomas.
Fig. 33-32.Parathyroid carcinoma.
Highermagnificationofthepreviousillustrationshowsthetrabecularpatternofgrowthcomposedoffairlyuniform,monotonous-appearingnuclei,althoughscatteredenlarged(pleomorphic)nucleiarepresent.Suchenlargedatypicalnucleicanbeseeninadenomas,andbyitselfisnotadefinitivediagnosticfeatureforcarcinoma.Suchenlargedatypicalnucleiareconsideredtobeanuncommonfeatureinparathyroidhyperplasia.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0165
f0170
f0175
f0180
u1210
u1215
u1220
u1225
u1230
Wenig_Chapter 33_main.indd 1513 4/29/2015 5:29:04 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1514 SECTION 9 ParathyroidGlands
• Nuclearpleomorphismislesscommonthaninade-nomas, which often contain scattered foci withenlargedatypicalnuclei:m Monotonyofnuclearsizeandshapeisfrequently
presentincarcinomas.m Pleomorphism, when present, is usually more
diffusethaninadenomas.• Mitotic activity is identified in most, but not all,
parathyroidcarcinomas:m Presenceofatypicalmitosesisvirtuallydiagnostic
ofmalignancym Althoughahighmitoticrateisahelpfulfeature,
the presence of mitotic activity exceeding 1 per10high-powerfieldsinaminorityofparathyroidadenomasandinparathyroidhyperplasiamaybeseen.
m Overlap inmitoticactivitybetweenallparathy-roidproliferativediseases (i.e.,adenoma,hyper-plasia, and carcinoma) makes mitotic activity ausefulfindingonlywhencoupledwithotherfea-turesofmalignancy.
• Capsularinvasionmaybeobviousinsomecases,ormay be represented only by irregular tongues orislands of parathyroid tissue protruding into thecapsule;invasionbeyondthecapsuleisindicativeofmalignancy:m Entrapped islands of parathyroid parenchymal
cells in benign disease should be distinguishedfrom these invasive foci by their rounded con-toursandlackofdesmoplasticreaction.
• Follicularpatternofgrowthnotoftenifeverseeninparathyroidcarcinomas
• Tumorcellsmayhavevariablemorphology:m Someareasmayshowsimilarfeaturesasbenign
chief cells with slightly eosinophilic to clearcytoplasm.
m Otherareasmaycontainenlargedcellswithmoredistinctly eosinophilic cytoplasm, large nucleiwithprominentnucleoli.
m Rareoncocyticcellvariantidentified.
Fig. 33-36.Parathyroid carcinoma with necrosis.
Fig. 33-37.Parathyroid carcinoma.
Parathyroidcarcinomashowingmarkedlyenlargedandhyperchromaticnuclei;althoughsimilarnuclearatypiacanbeseeninadenomas,thefactthatthesechangeswerediffuselypresentratherthanfocallypresent(assingleatypicalnucleiand/orinsmallclusterswithinthetumor)supportsadiagnosisofparathyroidcarcinomaandnotparathyroidadenomaorhyperplasia.Amonotonousnuclearpatternis,surprisingly,moreoftenseenincarcinomasthaninadenomas.
Fig. 33-38.Parathyroid carcinoma.
Parathyroidcarcinomacharacterizedbyamonotonousbutcrowdedproliferationofcellswithlargenucleiandverylargeeosinophilicnucleoli(macronucleoli);thesefindingsseeninsomeparathyroidcarcinomasarenottypicallypresentinbenignparathyroidlesions(i.e.,adenoma,hyperplasia);mitoticfigurescanbeseen(middle upper, upper right).
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0185
f0190
f0195
u1235
u1240u1245
u1250
u1325
u1255
u1260
u1265
u1270
u1275
u1280
u1285
u1290
u1295
Wenig_Chapter 33_main.indd 1514 4/29/2015 5:29:05 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1515
• Fibrous bands extending from a thickened capsulefrequentlydividethetumorintoirregularcompart-mentsand/ornodules.
• Angioinvasion is diagnostic of carcinoma but ispresentinaminorityofcases:m Usually foundwithinvessels in the thick tumor
capsulem Artifactually displaced clumpsof tumor cells in
vascularspacesshouldbedistinguishedfromtrueinvasionbytheirfrequentlydegeneratedappear-ance and by their lack of attachment to thevesselwall.
• Perineuralinvasion,althoughrarelyseen,isalsovir-tuallydiagnosticofmalignancy.
• Immunohistochemistry:m Positive for cytokeratins, chromogranin as well
asforparathyroidhormonem Loss of (nuclear) parafibromin staining is com-
monlybutnotinvariablyidentified:– Onlyabout50%ofcarcinomaslackparafibro-
minstaining– Somecarcinomasmayshowpositiveparafibro-
minstaining– Lossofparafibrominreportedinsporadicade-
nomas(unassociatedwithhyperparathyroidism-jawtumorsyndrome)
m HighfrequencyofcyclinD1expression(reportedinmorethan90%ofcases):– May result from loss of parafibromin ex-
pression– Mayreflectincreasedcellularproliferation– Highlevelsofexpressionalsopresentinhyper-
plasia (approximately 61%) and adenomas(approximately39%)sonotuniquely seen incarcinoma.
m Galectin-3reactivityfrequentlyseen:– Morethan90%ofcasesreportedpositive– Seen in less than 5% of parathyroid ade-
nomasm Diffusestrongstainingforproteingeneproduct
9.5(PGP9.5)frequentlyfoundm Ki67(MIB1)proliferativeindexmaybeincreased:
– Anindexgreaterthan5%shouldraisesuspi-cionforcarcinomabutthediagnosisofcarci-nomarequiresconfirmatorydiagnosticfindings.
– Proliferativeindicesindifferentiatingadenomafrom carcinoma are of limited utility givenoverlappingfindingsintheselesions.
m Loss of immunoreactivity for retinoblastoma(Rb)protein
m NegativeforthyroglobulinandTTF-1• Cytogeneticandmolecularbiology:
m Mutations of tumor suppressor gene HRPT-2maybeimportantinthepathogenesisofparathy-roidcarcinoma:
– InactivationofgermlinemutationsinHRPT-2believedtoplayasignificantroleinthedevel-opmentofparathyroidcarcinoma■ Locatedon1q25■ Encodesparafibrominknowntofunctionin
thesuppressionofcyclinD1■ Implicated in the hyperparathyroidism-jaw
tumorsyndrome■ Identifiedintwothirdsofcasesofsporadic
occurringparathyroidcarcinoma■ Practically never found in parathyroid
adenomasm Allelic loss of the retinoblastoma (Rb) tumor-
suppressorgeneiscommon:– Mayplayanimportantroleinthedevelopment
ofparathyroidcarcinoma– Loss of immunoreactivity for Rb protein
reported in 20% to 100% of parathyroidcarcinomas
– Absencemaybehelpfulindistinguishingpara-thyroid adenomas from carcinomas but notconsidered sufficiently reliable in differentiat-ingadenomafromcarcinoma
m SomaticmutationinMEN-1gene:– Foundin13%ofcarcinomas– Suggests a role in the development of
carcinomam Alleliclossofthep53m Reduced expression of cyclin-dependent kinase
inhibitorproteinp27commonlyidentified:– In contrast, adenomas show higher labeling
index.
Differential Diagnosis• Parathyroidadenoma(seeTable33-1)• Parathyroidhyperplasia(seeTable33-1)• Parathyromatosis:
m Represents microscopic foci of hyperplasticparathyroid tissue in the soft tissues of theneck in association with primary chief cellhyperplasia
m May be the cause of recurrent disease after anapparently complete resection of the grosslyevidenthyperplasticglands
m Should not be mistaken for invasion as seen inparathyroid carcinoma; differentiating featuresmayinclude:– Absence of associated fibroblastic reaction or
infiltrativecontour– Absence of an intravascular location of these
nests– Absence of other histologic features of carci-
nomashouldhelpexcludemalignancy.• Metastaticcarcinomafromanothersite
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
u1300
u1305
u1310
u1315
u1320
u1330u1335
u1340
u1345
u1350
u1355
u1360
u1365
u1370u1375
u1380u1385u1390
u1395
u1400u1405
u1410
u1415
u1420u1425u1430
u1435
u1440u1445
u1450
u1455
u1460
u1465
u1470
u1475
u1480
u1485u1490u1495
u1500u1505
u1510
s0105
p1605u1520u1525u1530
u1535
u1540
u1545
u1550
u1555
u1560
Wenig_Chapter 33_main.indd 1515 4/29/2015 5:29:05 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1516 SECTION 9 ParathyroidGlands
m StageI:invasionofsurroundingsofttissues;90%disease-freesurvival
m Stage II: vascular invasion; 46% disease-freesurvival
m Stage III: invasion of vital organs or regionallymphnodemetastasis;50%disease-freesurvival
m Stage IV: distant metastases; no disease-freesurvival
SECONDARY NEOPLASMS (Fig. 33-39)
Definition: Contiguous involvement from tumors inadjacentstructuresormetastaticneoplasmsfromdistantsitesinvolvingtheparathyroidgland.
Clinical• Usually asymptomatic; may present with a neck
mass;othersymptomsmayincludehoarseness,dys-phagia,andneckpain;rarecaseshavebeenassoci-atedwithclinicalhypoparathyroidismduetomassivereplacementofmultipleglands
• May result from direct extension, especially fromthyroid or laryngeal tumors, or from metastaticspread
• Metastasis to parathyroid glands is rare; amongthe more common primary malignancies that maymetastasizetotheparathyroidglandsinclude:m Breastcarcinoma(mostcommon)m Hematologicmalignancies
Treatment and Prognosis• Surgeryistheprimarytreatmentmodalitywithrec-
ommendedtreatmentincludingenblocresection,toinclude the ipsilateral thyroid lobe, strap muscles,recurrent laryngeal nerve, trachea, or esophagus ifinvolved:m Offersthebestchanceforcurem Up to 50% of patients are cured by en bloc
resection.• Prophylactic lymphadenectomy not recommended
duetothelowrateofnodaldisease(reportedtobe6%):m Neckdissectionwarrantedifthereisclinicalevi-
denceofneck(nodal)disease• Adjuvant radiotherapy may improve local control
andlimit theoccurrenceof localrelapse,especiallywhen the carcinoma is incompletely excised withinvolvementofresectionmargins.
• Efficacyofchemotherapynotproven• In general, parathyroid carcinomas are generally
indolentbehaving:m 5-yearsurvivalfrom60%to85%m 10-yearsurvivalfrom40%to79%
• Recurrencesgenerallymanifestwithin3yearsofthefirstsurgerywithlocallyrecurrentdisease:m Recurrenceratesrangefromapproximately33%
to50%m Lowerratesofrecurrencereported(8%)withen
blocresectionm Higher recurrence rates reported (51%) when
treatedbyparathyroidglandexcision• Metastaticdiseaseoccursratherlateinthecourseof
disease:m Foundinapproximatelyonethirdofpatientsm Usually occurs several years after primary
diagnosism Sitesofmetastasesincluderegionallymphnodes,
mediastinum,lungs,liver,andbones.• Surgical resectionofmetastaticor locallyrecurrent
diseaseisfrequentlyhelpfulduetotheratherindo-lentnatureofparathyroidcarcinoma:m Patients usually survive for several years after
recognitionoftumorrecurrence.• Recurrenceand/ormetastaticdiseaseoftenmanifest
withrecurrenthypercalcemia:m Lifelong monitoring for recurrent and/or meta-
staticdiseasemosteffectivelyaccomplishedwithserumcalciumlevels.
• Majordifficultyinmanagementofrecurrentdiseaseisseverehypercalcemiaanditscomplications.
• Death is related to excessive hormonal productionwithsubsequenthypercalcemiarather thandirectlytotumorburden.
• Prognosis has been shown to be related to tumorstage:
Fig. 33-39.Metastatic breast carcinoma.
Metastaticbreastcarcinomatotheparathyroidgland.Residualparathyroidparenchymaispresentinthecenteroftheimagesurroundedbyamalignantglandularlesion.Thepatienthadaknownhistoryofbreastcarcinomathatwaswidelymetastatic,includingtheparathyroidgland.Immunohistochemicalstaining(notshown)includedreactivityformammaglobin,BRST-2,andGATA-3.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
f0200
s0110
p1660
u1570u1575
u1580
u1585
u1590
u1595u1600
u1605u1610u1615
u1620
u1625
u1630
u1635
u1640u1645
u1650
u1655
u1660
u1665
u1670
u1675
u1680
u1685
u1690
u1695
u1700
u1705
s0115
p1810
s0125
p1815
u1715
u1720
u1725u1730
Wenig_Chapter 33_main.indd 1516 4/29/2015 5:29:05 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1517
– Malignantmelanoma:S100protein,HMB45,melanA,tyrosinase,MITF1,Sox10,vimentin
– Lungcarcinoma:NapsinA,TTF1– Renal cell carcinoma: RCC antibody, CD10,
PAX2,PAX8,CAIX– Prostatecarcinoma:PSA,PAP,prostein
Differential Diagnosis• Parathyroidcarcinoma:
m Reactivity for parathyroid hormone, chromo-granin
Treatment and Prognosis• Treatmentbasedonprimarysiteoforigin• Prognosispoor,relatedtodisseminationofprimary
disease
FURTHER READING
ReferencesmaybeaccessedonlineatExpertConsult.
m Malignantmelanomam Lungcarcinomam Renalcellcarcinomam Sarcomas
Pathology• Foundin11.9%ofcancerpatientsinautopsystudies• Mayinvolveoneormultipleglands• Immunohistochemistry:
m Avarietyoforgan-specificmarkersmaybehelpfulin the diagnosis of a metastatic tumor to theparathyroidgland
m Presence of specific immunomarkers helpful indistinguishing between primary and secondaryneoplasms:– Breast carcinoma: mammaglobin, BRST2,
GATA-3– Hematologic malignancies: CD45 (leukocyte
commonantigen),B-cell(CD20,others),T-cell(CD3,others)
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
u1735u1740u1745u1750
s0130
p1865u1760u1765u1770
u1775
u1780
u1785
u1790
u1795u1800
u1805
s0135
p1925u1815
s0140
p1940u1825
s0145
p1955
Wenig_Chapter 33_main.indd 1517 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1517.e1
FURTHER READING
Parathyroid AdenomaAbdul-HajSK,ConklinH,HewittWC:Functioninglipoadenomaof
the parathyroid gland: report of a unique case, N Engl J Med266:121–132,1962.
Bai S, LiVolsi VA, Fraker DL, Bing Z: Water-clear parathyroidadenoma:reportoftwocasesandliteraturereview,Endocr Pathol23(3):196–200,2012.
Baloch ZW, LiVolsi VA: Oncocytic lesions of the neuroendocrinesystem,Semin Diagn Pathol16(2):190,1999.
BedettiCD,DekkerA,WatsonCG:Functioningoxyphilcelladenomaoftheparathyroidgland.Aclinicopathologicstudyoftenpatientswithhyperparathyroidism,Hum Pathol15:1121–1126,1984.
BettsG,BeckettE,NonakaD:GATA3showsdifferential immuno-histochemicalexpressionacross thyroidandparathyroid lesions,Histopathology2014.
BleiweissIJ,HarpazN,StrauchenJA,etal:Functioninglipoadenomaof theparathyroid: case report and literature review,Mt Sinai J Med56(2):114–117,Review,1989.
BombiJA,NadalA,MunozJ,CardesaA:Ultrastructuralpathologyof parathyroid glands in hyperparathyroidism: a report of 69cases,Ultrastruct Pathol17:567–582,1993.
BondesonA-G,BondesonL,LjungbergO,etal:Fatstaininginpara-thyroiddisease—diagnosticvalueandimpactonsurgicalstrategy,Hum Pathol16:1255–1263,1985.
BricaireL,OdouMF,Cardot-BautersC,etal;GTEGroup:FrequentlargegermlineHRPT2deletions in aFrenchNational cohortofpatients with primary hyperparathyroidism, J Clin Endocrinol Metab98(2):E403–E408,2013.
Carlson D: Parathyroid pathology: hyperparathyroidism andparathyroid tumors,Arch Pathol Lab Med 134(11):1639–1644,2010.
Carpten JD, Robbins CM, Villablanca A, etal: HRPT2, encodingparafibromin,ismutatedinhyperparathyroidism-jawtumorsyn-drome,Nat Genet32(4):676–680,2002.
ChanJKC:Doubleadenomas. InFletcherCDM,editor:Diagnostic histopathology of tumors,ed4,Philadelphia,2013,ElsevierSaun-ders,pp1275–1276.
ChowLS,EricksonLA,Abu-LebdehHS,WermersRA:Parathyroidlipoadenomas: a rare cause of primary hyperparathyroidism,Endocr Pract12(2):131–136,2006.
Cinti S,ColussiG,MinolaE,DickersinGR:Parathyroid glands inprimaryhyperparathyroidism:anultrastructuralstudyof50cases,Hum Pathol17:1036–1046,1986.
Clark O, Duh Q-Y: Primary hyperparathyroidism. A surgicalperspective, Endocrinol Metabol Clin North Am 18:701–714,1989.
Costa-GudaJ,ArnoldA:Geneticandepigeneticchangesinsporadicendocrinetumors:parathyroidtumors,Mol Cell Endocrinol2013.pii:S0303-7207(13)00367-5.
Costa-Guda J, Soong CP, Parekh VI, etal: Germline and somaticmutations in cyclin-dependent kinase inhibitor genes CDKN1A,CDKN2B, and CDKN2C in sporadic parathyroid adenomas,Horm Cancer4(5):301–307,2013.
DeLellisRA:Parathyroidtumorsandrelateddisorders,Mod Pathol24(Suppl2):S78–S93,2011.
DeLellisRA,MazzagliaP,MangrayS:Primaryhyperparathyroidism:a currentperspective,Arch Pathol Lab Med 132(8):1251–1262,2008.
DewandaNK,ChumberS,TandonN,KarakAK:Functioningoxyphiladenomaofparathyroid,J Postgrad Med46(3):215–216,2000.
Ducatman BS, Wilkerson SY, Brown JA: Functioning parathyroidlipoadenoma.Reportofacasediagnosedbyintraoperativetouchpreparations,Arch Pathol Lab Med110:645–647,1986.
EzzatT,MacleanGM,ParameswaranR,etal:Primaryhyperparathy-roidismwithwater clear cell content: the impact of histologicaldiagnosisonclinicalmanagementandoutcome,Ann R Coll Surg Engl95(3):e60–e62,2013.
Fleischer J, Becker C, Hamele-Bena D, etal: Oxyphil parathyroidadenoma: a malignant presentation of a benign disease, J Clin Endocrinol Metab89(12):5948–5951,2004.
GeelhoedGW:Parathyroidadenolipoma:clinicalandmorphologicalfeatures,Surgery92:806–810,1982.
Ghandur-Mnaymneh L, Kimura N: The parathyroid adenoma. Ahistopathologic definition with a study of 172 cases of primaryhyperparathyroidism,Am J Pathol115:70–83,1984.
Gill AJ, Clarkson A, Gimm O, etal: Loss of nuclear expressionof parafibromin distinguishes parathyroid carcinomas andhyperparathyroidism-jawtumor (HPT-JT)syndrome-relatedade-nomasfromsporadicparathyroidadenomasandhyperplasias,Am J Surg Pathol30(9):1140–1149,2006.
GiorgadzeT,StrattonB,BalochZW,LivolsiVA:Oncocyticparathy-roid adenoma: problem in cytological diagnosis, Diagn Cytopa-thol31(4):276–280,2004.
GrimeliusL,DeLellisRA,BondesonL,etal:Parathyroidadenoma.InDeLellisRA,LloydRV,HeitzPU,EngC,editors:World Health Organization classification of tumours. Pathology and genetics: tumours of the endocrine organs, Lyon, 2004, IARC Press, pp128–132.
JuhlinC,LarssonC,YakolevaT,etal:Lossofparafibrominexpres-sion ina subsetofparathyroidadenomas,Endocr Relat Cancer13(2):509–523,2006.
KhanA,TischlerAS,PatwardhanNA,DeLellisRA:Calcitoninimmu-noreactivityinneoplasticandhyperplasticparathyroidglands:animmunohistochemicalstudy,Endocr Pathol14:249–255,2003.
LeeAY,WangBY,HellerKS:Importanceof intraoperativeparathy-roidhormonemeasurementinthediagnosisofparathyroidlipo-adenoma,Head Neck33(6):917–919,2011.
NatsuiK,TanakaK, SudaM, etal:Oxyphil parathyroid adenomaassociated with primary hyperparathyroidism and marked post-operative hungry bone syndrome, Intern Med 35:545–549,1996.
Obara T, Fujimoto Y, Ito Y, etal: Functioning parathyroidlipoadenoma–reportof fourcases: clinicopathologicalandultra-sonographicfeatures,Endocrinol Jpn36:135–145,1989.
OrdóñezNG:ValueofPAX8immunostainingintumordiagnosis:areviewandupdate,Adv Anat Pathol19:140–151,2012.
OzcanA,ShenSS,HamiltonC,etal:PAX8expressioninnon-neo-plastictissues,primarytumors,andmetastatictumors:acompre-hensive immunohistochemical study, Mod Pathol 24:751–764,2011.
PakerI,YilmazerD,YandakciK,etal:Intrathyroidaloncocyticpara-thyroid adenoma: a diagnostic pitfall on fine-needle aspiration,Diagn Cytopathol38(11):833–836,2010.
Palmer M, Ljunghall S, Akerstrom G, etal: Patients with primaryhyperparathyroidismoperatedonovera24-yearperiod:temporaltrends of clinical and laboratory findings, J Chron Dis 40:121–130,1987.
PiggottRP,WatersPS,AshrafJ,etal:Water-clearcelladenoma:arareformofhyperparathyroidism,Int J Surg Case Rep4(10):911–913,2013.
RastogiA,JainM,AgarawalT,etal:Parathyroidlipoadenoma:casereport and review of the literature, Indian J Pathol Microbiol49(3):404–406,2006.
RichTA,HuMI,Martin JW,etal:CDC73-relateddisorders.2008Dec31 [updated2012May24]. InPagonRA,AdamMP,BirdTD,etal,editors:GeneReviews™ [Internet],Seattle(WA),1993-2013, University of Washington, Seattle. Available from: http://www.ncbi.nlm.nih.gov/books/NBK3789/.
RosaiJ,DeLellisRA,CarcanguiML,etal:Parathyroidadenomaandvariants. In Silverberg SG, editor: Tumors of the thyroid and
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
Wenig_Chapter 33_main.indd 1 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
1517.e2 SECTION 9 ParathyroidGlands
parathyroid glands. Fourth series, Fascicle21,Washington,DC,2014,ArmedForcesInstituteofPathology,pp513–542.
RothSI:Water-clearcell“adenoma.”Anewentityinthepathologyof primary hyperparathyroidism, Arch Pathol Lab Med119(11):996–997,1995.
SasanoH,GeelhoedGW,SilverbergSG:Intraoperativeevaluationoflipidinthediagnosisofparathyroidadenoma,Am J Surg Pathol12:282–286,1988.
SeethalaRR,YimJH,Hunt JL:Pathologyquiz case2.Parathyroidlipoadenoma,Arch Otolaryngol Head Neck Surg132(12):1391–1393,2006.
SharrettsJM,SimondsWF:Clinicalandmoleculargeneticsofpara-thyroid neoplasms, Best Pract Res Clin Endocrinol Metab24(3):491–502,2010.
SnoverDC,FoucarK:Mitoticactivityinbenignparathyroiddisease,Am J Clin Pathol75:345–347,1981.
TehBT,SweetKM,MorrisonCD:Hyperparathyroidism-jawtumoursyndrome. InDeLellisRA,LloydRV,HeitzPU,EngC, editors:World Health Organization classification of tumours. Pathology & genetics tumours of the endocrine organs,Lyon,2004, IARCPress,pp228–229.
TurnerWJ,BaergenRN,PellitteriPK,etal:Parathyroidlipoadenoma:casereportandreviewoftheliterature,Otolaryngol Head Neck Surg114:313–316,1996.
WolpertHR,VickeryALJr,WangCA:Functioningoxyphilcellade-nomasoftheparathyroidgland.Astudyof15cases,Am J Surg Pathol13:500–504,1989.
YoonV,TreatK,MaaloufNM:Ectopicatypicalparathyroidlipoad-enoma: a rare cause of severe primary hyperparathyroidism,J Bone Miner Metab31(5):595–600,2013.
ZhouW,KatzMH,DeftosLJ,etal:Metachronousdoubleparathy-roid adenomas involving two different cell types: chief cell andoxyphilcell,Endocr Pract9(6):522–525,2003.
Parathyroid CarcinomaBombiJA,NadalA,MunozJ,CardesaA:Ultrastructuralpathology
of parathyroid glands in hyperparathyroidism: a report of 69cases,Ultrastruct Pathol17:567–582,1993.
BondesonL,GrimeliusL,DeLellisRA,etal:Parathyroidcarcinoma.InDeLellisRA,LloydRV,HeitzPU,EngC,editors:World Health Organization classification of tumours. Pathology & genetics tumours of the endocrine organs, Lyon, 2004, IARC Press, pp124–127.
BricaireL,OdouMF,Cardot-BautersC,etal;GTEGroup:FrequentlargegermlineHRPT2deletions in aFrenchNational cohortofpatients with primary hyperparathyroidism, J Clin Endocrinol Metab98(2):E403–E408,2013.
BusaidyNL,JimenezC,HabraMA,etal:Parathyroidcarcinoma:a22-yearexperience,Head Neck26:716–726,2004.
CarlsonD:Parathyroidpathology:hyperparathyroidismandparathy-roid tumors, Arch Pathol Lab Med 134(11):1639–1644,2010.
CavacoBM,SantosR,FélixA,etal:Identificationofdenovogerm-line mutations in the HRPT2 gene in two apparently sporadiccases with challenging parathyroid tumor diagnoses, Endocr Pathol22(1):44–52,2011.
Cetani F, Pardi E, Viacava P, etal: A reappraisal of the Rb1 geneabnormalities inthediagnosisofparathyroidcancer,Clin Endo-crinol (Oxf)60(1):99–106,2004.
CohnK, SilvermanM,Corrado J, SedgewickC:Parathyroid carci-noma: the Lahey Clinic experience, Surgery 98:1095–1100,1985.
Costa-GudaJ,ArnoldA:Geneticandepigeneticchangesinsporadicendocrinetumors:parathyroidtumors,Mol Cell Endocrinol2013.pii:S0303-7207(13)00367-5.
CrynsVL,ThorA,XuHJ,etal:Lossoftheretinoblastomatumor-suppressor gene in parathyroid carcinoma, N Engl J Med330(11):757–761,1994.
DeLellisRA:Parathyroidcarcinoma:anoverview,Adv Anat Pathol12(2):53–61,Review,2005.
DeLellisRA:Challenginglesionsinthedifferentialdiagnosisofendo-crine tumors:parathyroidcarcinoma,Endocr Pathol19(4):221–225,2008.
DeLellisRA:Parathyroidtumorsandrelateddisorders,Mod Pathol24(Suppl2):S78–S93,2011.
DeLellisRA,MazzagliaP,MangrayS:Primaryhyperparathyroidism:a currentperspective,Arch Pathol Lab Med 132(8):1251–1262,2008.
DotzenrathC,TehBT,FarneboF,etal:Alleliclossoftheretinoblas-tomatumorsuppressorgene:amarkerforaggressiveparathyroidtumors?,J Clin Endocrinol Metab81(9):3194–3196,1996.
EricksonLA,JinL,PapottiM,etal:Oxyphilparathyroidcarcinomas:aclinicopathologicand immunohistochemical studyof10cases,Am J Surg Pathol26:344–349,2002.
FitkoR,RothSI,HinesJR,etal:Parathyromatosisinhyperparathy-roidism,Hum Pathol21:234–237,1990.
Gill AJ: Understanding the genetic basis of parathyroid carcinoma,Endocr Pathol2014.[Epubaheadofprint].
Gill AJ, Clarkson A, Gimm O, etal: Loss of nuclear expressionof parafibromin distinguishes parathyroid carcinomas andhyperparathyroidism-jawtumor (HPT-JT)syndrome-relatedade-nomasfromsporadicparathyroidadenomasandhyperplasias,Am J Surg Pathol30(9):1140–1149,2006.
Haven CJ, Howell VM, Eilers PH: Gene expression of parathyroidtumors:molecularsubclassificationandidentificationofthepoten-tialmalignantphenotype,Cancer Res64:7405–7411,2004.
KutcherMR,RigbyMH,BullockM,etal:Hyperparathyroidism-jawtumorsyndrome,Head Neck35(6):E175–E177,2013.
LevinKE,GalanteM,ClarkOH:Parathyroidcarcinomaversuspara-thyroidadenomainpatientswithprofoundhypercalcemia,Surgery101:649–660,1987.
Munson ND, Foote RL, Northcutt RC: Parathyroid carcinoma: isthere a role for adjuvant radiation therapy?, Cancer 98:2378–2384,2003.
Rosai J,DeLellisRA,CarcanguiML, etal: Parathyroid carcinoma.InSilverbergSG,editor:Tumors of the thyroid and parathyroid glands.Fourthseries,Fascicle21,Washington,DC,2014,ArmedForcesInstituteofPathology,pp543–560.
SchantzA,CastlemanB:Parathyroidcarcinoma.Astudyof70cases,Cancer31:600–605,1973.
Sharretts JM, Kebebew E, Simonds WF: Parathyroid cancer, Semin Oncol37(6):580–590,2010.
SharrettsJM,SimondsWF:Clinicalandmoleculargeneticsofpara-thyroid neoplasms, Best Pract Res Clin Endocrinol Metab24(3):491–502,2010.
ShattuckTM,ValimakiS,ObaraT:Somaticandgerm-linemutationsoftheHRPT2geneinsporadicparathyroidcarcinoma,N Engl J Med349:1722–1729,2003.
SnoverDC,FoucarK:Mitoticactivityinbenignparathyroiddisease,Am J Clin Pathol775:345–347,1981.
TanMH,MorrisonC,WangP,etal:Lossofparafibrominimmuno-reactivity is a distinguishing feature of parathyroid carcinoma,Clin Cancer Res10(19):6629–6637,2004.
TehBT,SweetKM,MorrisonCD:Hyperparathyroidism-jawtumoursyndrome. InDeLellisRA,LloydRV,HeitzPU,EngC, editors:World Health Organization classification of tumours. Pathology & genetics tumours of the endocrine organs,Lyon,2004, IARCPress,pp228–229.
WangC,GazRD:Naturalhistoryofparathyroidcarcinoma:diagno-sis,treatment,results,Am J Surg149:522–527,1985.
WeiCH,HarariA:Parathyroidcarcinoma:updateandguidelinesformanagement,Curr Treat Options Oncol13(1):11–23,2012.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
Wenig_Chapter 33_main.indd 2 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

C
CHAPTER 33 NeoplasmsoftheParathyroidGlands 1517.e3
Secondary NeoplasmsDeLellisRA:Secondarytumours.InDeLellisRA,LloydRV,HeitzPU,
Eng C, editors: World Health Organization classification of tumours. Pathology & genetics tumours of the endocrine organs,Lyon,2004,IARCPress,p133.
HorwitzCA,MyersWP,FooteFWJr:Secondarymalignanttumorsof the parathyroid glands: report of two cases with associatedhypoparathyroidism,Am J Med52:797–808,1972.
Rosai J, DeLellis RA, Carcangui ML, etal: Secondary tumors. InSilverberg SG, editor: Tumors of the thyroid and parathyroid glands.Fourthseries,Fascicle21,Washington,DC,2014,ArmedForcesInstituteofPathology,pp585–587.
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
Wenig_Chapter 33_main.indd 3 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

Codes Change ListThe following codes have been either added or deleted since the first proof.
Add Removeu1130p0010u9160u9165
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
Wenig_Chapter 33_main.indd 4 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.

Codes Change List
The following codes have been either added or deleted since the first proof.
Add Removeu1130p0010u9160u9165
ISBN:978-1-4557-3382-8;PII:B978-1-4557-3382-8.00034-7;Author:Wenig;00034
Wenig_Chapter 33_main.indd 5 4/29/2015 5:29:06 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication.