Embed Size (px)
Citation preview

Marit Silén is interested in nursing ethics, especially in how social and organizational contexts shape and influence nurses’ encountering of ethical issues. She has a Masters in Nursing Science from Örebro University and is a Registered Nurse. This book is her PhD thesis in Nursing.
This thesis explores and describes what nurses find ethically problematic and morally distressing in their work, the factors contributing to there being ethically problematic situations and the actions reported taken in order to handle them, thus creating an ethical climate. The analyses are based on interviews with as well as questionnaire data from nurses working at somatic acute care wards at Swedish hospitals. The findings demonstrate that the nurses experienced ethical problems and moral distress when they could not provide good care, and thereby could not fulfill the goal of nursing. In understanding why problematic situations turn into ethical problems, factors associated with the professional role of being a nurse seem to be of significance. The nurses described several actions that were used when handling ethical problems. Some were explicitly described as promoting a positive ethical climate, i.e. a perception of the ethical problems being handled well. Several of the approaches were actions that in their essence strived to bridge the gap between employees from the same as well as different professions.
ISSN 1654-3602 ISBN 978-91-85835-19-5 HHJ
School of Health Sciences Jönköping University
Dissertation Series No. 20, 2011
Encountering ethical problems and moral distress as a nurse
Experiences, contributing factors and handling
Dissertation Series N
o. 20, 2011E
ncountering ethical problems and m
oral distress as a nurse E
xperiences, contributing factors and handlingM
ar
It SIléN
DS
MarIt SIléN
MarIt SIléN
DS
Hälsohögskolan, Högskolan i Jönköping
Encountering ethical problems and
moral distress as a nurse
Experiences, contributing factors and handling
Marit Silén
DISSERTATION SERIES NO. 20, 2011
JÖNKÖPING 2011

© Marit Silén, 2011 Publisher: School of Health Sciences Print: Intellecta Infolog ISSN 1654-3602 ISBN 978-91-85835-19-5

“Experience: that most brutal of teachers. But you learn, my God do you learn.”
C.S. Lewis


Abstract
The aim of this thesis was to explore and describe what nurses find ethically problematic and morally distressing in their work, the factors contributing to the arising of ethically problematic situations and the actions reported taken in order to handle them, thus creating an ethical climate.
Descriptive as well as correlational and exploratory designs were employed in the four papers on which this thesis is based. A total of 283 nurses from 21 acute care wards at four Swedish hospitals participated. Interviews were analyzed using qualitative content analysis and the critical incident technique, and questionnaires were analyzed using descriptive and non-parametric statistics.
The nurses described ethical problems and moral distress related to decision making about life-sustaining treatment, but also when they experienced difficulties in preserving a patient’s integrity and when they could not give care that was necessary and safe. Inadequate communication between healthcare staff, the physicians’ ways of handling potentially ethically problematic situations and patients’ poor state of health, which hindered their participation in decisions concerning them, were some of the factors that could contribute to the rise of an ethically problematic situation. Among the actions described as being used to handle ethical problems and moral distress, some were explicitly stated to promote a positive ethical climate, i.e. a perceived positive handling of ethical issues. These were supporting each other in the working group, using policies and routines as help, giving care based on the needs of patients and their next of kin and daring to speak out, thus contributing to setting a standard for behavior. Having the need for explanations and information satisfied and working as a team also promoted a positive ethical climate.
In conclusion, the professional role of being a nurse seems to be of importance not only when it comes to what situations are experienced as ethically problematic and morally distressing, but also concerning what factors may contribute to the rise of them. Perceiving a positive ethical climate may mediate these experiences.

Original papers
The thesis is based on the following papers, which are referred to in the text by their Roman numerals:
Paper I Silén, M., Tang, P.F., Wadensten, B., & Ahlström, G. (2008). Workplace distress and ethical dilemmas in neuroscience nursing. Journal of Neuroscience Nursing, 40(4), 222-231.
Paper II Silén, M., Svantesson, M., & Ahlström, G. (2008). Nurses’ conceptions of decision making concerning life-sustaining treatment. Nursing Ethics, 15(2) 160–173.
Paper III Silén, M., Svantesson, M., Kjellström, S., Sidenvall, B., & Christensson, L. Moral distress and ethical climate in a Swedish nursing context: perceptions and instrument usability. Journal of Clinical Nursing. Epub ahead of print 2 September, 2011, doi: 10.1111/j.1365-2702.2011.03753.x.
Paper IV Silén, M., Kjellström, S., Christensson, L., Sidenvall, B., & Svantesson, M. What actions promote a positive ethical climate? A critical incident study of nurses’ perceptions. Submitted. The articles have been reprinted with the kind permission of the respective journals.

Contents
Acknowledgements .............................................................................. 10 Introduction ....................................................................................... 12 Background ........................................................................................ 12
Ethical problems ........................................................................................ 12
Ethical problems in nursing care ............................................................ 13 Factors affecting the handling of ethical problems.................................. 15
Moral distress ............................................................................................ 17
Definition ............................................................................................. 17 The process that results in moral distress ............................................... 17 Research on moral distress within healthcare ......................................... 18 Criticism of the concept of moral distress .............................................. 19 Similar concepts .................................................................................... 19
Ethical climate ........................................................................................... 20
Original definition ................................................................................. 20 Ethical climate and organizational research ............................................ 21 Criticism of the original definition ........................................................ 21 Ethical climate in healthcare .................................................................. 22
Overview of the relation between the concepts .......................................... 23
Rationale for the thesis ........................................................................ 24 Aim of the thesis ................................................................................. 26 Method .............................................................................................. 26
Design ....................................................................................................... 26
Participants and settings ............................................................................ 28
Qualitative methods .................................................................................. 29
Data collection ...................................................................................... 29 Data analyses ......................................................................................... 31 Trustworthiness ..................................................................................... 32
Quantitative method ................................................................................. 33
Data collection ...................................................................................... 33 Data analyses ......................................................................................... 34
Validity and reliability ........................................................................... 34
Ethical considerations ................................................................................ 35
Results ................................................................................................ 36 Situations that are experienced as ethically problematic and morally distressing .................................................................................................. 36
Factors that contribute to the arising of ethically problematic situations .... 38
Actions reported taken in order to handle ethically problematic and morally distressing situations, thus creating an ethical climate ................................ 39
Discussion .......................................................................................... 42 Reflections on the results ........................................................................... 42
Ethical problems and moral distress – the importance of the professional role ........................................................................................................ 42 Positive ethical climate – a mediating factor when encountering ethical problems and moral distress ................................................................... 45
Methodological considerations................................................................... 49
Participants ............................................................................................ 50 Data collection ...................................................................................... 50 Data analysis .......................................................................................... 51 Trustworthiness ..................................................................................... 52
Conclusions and implications .................................................................... 53
Svensk sammanfattning ....................................................................... 54 Att möta etiska problem och moralisk stress som sjuksköterska – Upplevelser, bidragande faktorer och hanterande ........................................................... 54
References ........................................................................................... 57
10
Acknowledgements
This work has been carried out at the Research School of Health and Welfare at School of Health Sciences, Jönköping University. I am grateful to the following sources of financial support for my projects: School of Health Sciences at Jönköping University, Swedish Society of Nursing, and Futurum – the Health Care Academy in Jönköping County Council. For five years I have worked with this thesis, and there are many who have helped me make it possible and to whom I want to express my sincere gratitude. My supervisors. Thank you for never letting me doubt that I had the ability to actually write this thesis. I have felt secure having you on my “team”, at the same time as you have allowed me to continuously grow as a researcher. Lennart Christensson, my main supervisor. You have been a supervisor beyond the call of duty, not least during the final hectic months. Your calmness during this time has been invaluable. Birgitta Sidenvall, Mia Svantesson and Sofia Kjellström, my co-supervisors. Thank you for being so dedicated to your roles as co-supervisors and for sharing all your knowledge without prestige. My co-authors on Papers I and II, for a successful collaboration. I would especially like to thank Gerd Ahlström for introducing me to the world of nursing research. All of you, past and present, at the Research School of Health and Welfare, for making it a dynamic and fun place to work at. There are a few of you who deserve extra thanks:
11
My “sisters” in Pro colloquio for all the fruitful and fun discussions on research in general, methods specifically and life after these years as a doctoral student. I will keep on dreaming about that university of our own! Linda Johansson and Marie Golsäter, you have been great companions during these years. Thank you for sharing the good days and the not so good ones, knowledge, ideas and hotel rooms. You make my life richer! My family. Grandmother, for keeping your fingers crossed for me whenever needed. Juliana and Andreas, for really trying to understand this research field of mine, not least the strange (or so I think you consider them to be?) research methods. Thank you for letting me take part in the student life in Uppsala when I have had an aching need for traditions! Father, for reading manuscripts and helping me make my lines of argument clearer. Mother and Father, for your help and support in all possible ways. You encouraged me to begin this work and without you it would not have been finished. Jönköping, September 2011 Marit Silén
12
Introduction
The goal of nursing is to work for the good of the patient. Nursing can therefore be regarded as an ethical practice (Gastmans, Dierckx de Casterle & Schotsmans, 1998). This means that the ethical dimension of nursing care is not restricted to specific situations but is rather an integral part of all nursing care (Bishop & Scudder, 1990). Ever since the beginning of modern nursing, starting with the Nightingale era, ethics has been regarded as a vital part of nursing. In her Notes on Nursing, Nightingale points to the importance of listening to patients, putting their needs first and upholding confidentiality (Nightingale, 2010). Today we would describe these as ethical actions. They were in some sense formalized in 1953, when the International Council of Nurses (ICN) launched its first code of ethics (ICN, 1953). But laws and other regulations on a national level, such as the Swedish Health and Medical Service Act (Ministry of Health and Social Affairs, 1982:763), also regulate how nurses and other healthcare staff should act. This means that nurses have to navigate among the ethical values of different stakeholders: patient, organization, profession and society. When these values are threatened or clash, nurses have to take a stand on how to deal with this. The aim of this thesis is to explore and describe what nurses find ethically problematic and morally distressing in their work, the factors contributing to the arising of ethically problematic situations and the actions reported taken in order to handle them, thus creating an ethical climate.
Background
Ethical problems
This thesis takes its starting point in nurses’ experiences of situations they consider ethically problematic and morally distressing. A number of different
13
concepts are used in the literature to describe situations that are in one way or another ethically problematic. Some of these concepts are ethical problems, ethical dilemmas, ethical conflicts, ethical concerns and ethical issues. However, although these situations are labeled differently their core seems to entail a person encountering situations in which values, norms or principles are threatened or in conflict and a decision has to be made on how to act. In the literature, such as in Thompson, Melia, Boyd and Hornsburgh (2006), differences between concepts are described. However, in research studies motivation is seldom given for the use of a specific concept, and they seem to be used quite interchangeably. Due to an apparent lack of consensus on what concept to use when for ethical problems, and as a consequence of taking as a starting point the nurses’ experiences and thereby relying on an inductive perspective, the nurses were given the preferential right to define what situations they considered ethically problematic. In this thesis no distinction is made between the two terms “ethics” and “morals”. They can be regarded as overlapping, and distinctions are mostly made when they are used in a more formal way (Thompson et al., 2006). With regard to the aim of this thesis, a distinction was not considered necessary.
Ethical problems in nursing care
Ethical problems for nurses can arise in situations such as when decisions are to be made on life-sustaining treatment, but also in other situations when there is a question of what is in the patient’s best interest. Sometimes it is difficult to decide how much information should be given to patients and next of kin, leading to ethical problems concerning informed consent. Policies intended to facilitate can sometimes give rise to ethical problems if different policies apply, supporting different actions. Factors that can contribute to the arising of ethical problems are, among others, hierarchical structures and a lack of different kinds of resources. The area of decision making regarding life-sustaining treatment is one where nurses experience ethical problems. This mainly concerns how long futile treatment should be continued (Bunch, 2001; Çobanoglu & Algier, 2004) and

14
what ethical criteria can be used to terminate life-sustaining treatment (Hermsen & van der Donk, 2009). In a setting like intensive care there can be tension between nurses’ personal values regarding what constitutes a good death and the purpose of intensive care, i.e. saving life (Cronqvist, Theorell, Burns & Lützén, 2004). The decision on the course of treatment is experienced as being further complicated when the patient whom the decision concerns is decision-incompetent (Enes & de Vries, 2004). Ethical problems involving the withholding or withdrawal of treatment also can give rise to conflict between nurses and physicians, according to nurses. Nurses have advocated withdrawal of treatment sooner than physicians (Torjuul & Sörlie, 2006). This has been explained by differences of perspective, whereby physicians are the ones who make the decisions while nurses are the ones who carry out these decisions (Oberle & Hughes, 2001). However, other studies (Eliasson, Howard, Torrington, Dillard & Phillips, 1997; Svantesson, Sjökvist, Thorsén & Ahlström, 2006) have shown contradictory results, with high agreement between nurses and physicians regarding aggressiveness of treatment for the patients they care for. Ethical problems in the form of divergent opinions also arise in other situations, for example when patients refuse the care offered (Karlsson, Roxberg, da Silva & Berggren, 2010) or make, from a professional perspective, irrational decisions (Hermsen & van der Donk, 2009; Sandman & Nordmark, 2006). It can also happen that nurses and next of kin have different opinions on what is in the best interest of the patient, or that different family members disagree on the patient’s best interest (Sandman & Nordmark, 2006). Nurses have also told about ethical problems related to giving information and informed decision (Killen, 2002; Ulrich et al., 2010). This comprises difficulties involving how much information a patient or next of kin should be given (Torjuul & Sörlie, 2006) or having to get a patient sign agreement for treatment although it is uncertain if the patient understands what this means (Shapira-Lishchinsky, 2009). Information can also be withheld from a next of kin at the request of the patient (Torjuul & Sörlie, 2006). Although policies can be a guide in decision making when facing an ethical problem, they can sometimes be perceived as constraining and as giving rise to

15
ethical problems (Oberle & Tenove, 2000). An ethical problem can consist of a conflict between different policies or between a policy and a judgment about what should be in the patient’s best interest (Sandman & Nordmark, 2006). As there is a considerable amount of research on what situations nurses find ethically problematic, what may contribute to the rise of an ethically problematic situation is more sparsely discussed here. However, some of the factors that have been pointed out are nurses’ position in the hierarchical structure of professions (Oberle & Hughes, 2001) and physicians’ way of handling situations involving decision making concerning life-sustaining treatment (Cronqvist et al., 2004). Lack of resources, such as equipment, finances (Gaudine, LeFort, Lamb & Thorne, 2011) time, staffing and private rooms (Torjuul & Sörlie, 2006) might also contribute to there being ethical problems regarding prioritization.
Factors affecting the handling of ethical problems
When confronted with an ethical problem, nurses have to decide what actions to take in order to handle it. In a review, Goethals, Gastmans and de Casterlé (2010) have described this as two interrelated processes, beginning with reasoning about how to deal with the ethical problem. In this process the nurses observe, analyze and judge the problem, which results in a decision. Thereafter, a process of implementing this decision in clinical practice follows. During both these processes there are several factors that affect the nurses, some personal and others contextual. Among the personal factors are nurses’ values, convictions, experiences and skills. Examples of contextual factors include opinions and expectations of others, rules, routines, procedures and guidelines (Goethals et al., 2010). The process of reasoning cannot be reduced to a cognitive activity as it is contextually embedded, and it is the personal relationship between nurses and patients that forms this context. Factors that facilitate this process include education, guidelines and standards, supportive colleagues and experience at the same workplace. However, if the nurses experience a stressful working environment with complex patient situations, insufficient resources such as
16
time, and dominance within the medical profession, this hinders the process of reasoning (Goethals et al., 2010). A personal factor that is believed to affect the reasoning process is moral sensitivity (Lützén, Dahlqvist, Eriksson & Norberg, 2006). This has been described as a personal capacity that is the result of personal experience. Moral sensitivity involves more than relying on one’s emotions when identifying the moral values in a conflict situation. It means having an attention to moral values and an awareness of one’s own role and responsibility in the situation (Lützén, 1993). In the process of implementing a decision into clinical practice, it has been shown that this can prove to be difficult due to contextual factors that limit nurses’ ability to act in the desired way. These include hierarchical relationships, traditional structures of power, not being involved in decision making, poor cooperation with physicians and feelings of not being respected as a professional. However, if the nurses are involved in ethical decision making with a mandate in ethics deliberations and have a positive collaboration with physicians this facilitates the implementation process. Besides these contextual factors, personal factors such as knowledge, experience, risk taking and boldness facilitate this process (Goethals et al., 2010). To summarize, research on nurses’ conceptions of ethical problems has shown that these are experienced in a number of situations, those regarding life-sustaining treatment among the most prominent. However, it is less well described what factors are perceived as contributing to the rise of an ethical problem, which is important when it comes to how a certain ethical problem should be dealt with, and what actions are taken in order to handle the situation. All situations of ethical difficulty are not experienced as ethical problems, however; at times it might be difficult to know how to act, but there is at least acting space. If this acting space is lacking, a situation might be experienced as morally distressing.
17
Moral distress
Definition
The term moral distress was coined in 1984 by Jameton, who viewed it as one of three categories into which ethical problems arising in a hospital context could be sorted. The first of these categories was moral uncertainty, which he described as “when one is unsure what moral principles or values apply, or even what the moral problem is” (1984, p.6). The next category of ethical problems was, according to Jameton, moral dilemmas that “arise when two (or more) clear moral principles apply, but they support mutually inconsistent courses of action” (1984, p.6). Moral distress, finally, “arises when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action” (1984, p.6). Jameton later (1993) made a distinction between two forms of distress, namely that of initial and reactive distress. Initial distress is felt in the form of frustration, anger and anxiety when confronted with institutional obstacles, while reactive distress is the result of not acting upon the initial distress (Jameton, 1993).
The process that results in moral distress
Kälvemark Sporrong (2007) has described the process that could have moral distress as a possible reaction as starting with a moral stressor. She suggests that in order to be a moral stressor, in the case of healthcare services, “it has something to do with the professional role as care-giver for someone, of not being able to fulfill obligations towards the patient” (2007, p.26). The experience of a moral stressor, according to Kälvemark Sporrong (2007), forces the individual to deal with it, i.e. ethical decision making. Possible outcomes include the situation involving the moral stressor not being solved; it being solved but the individual not being satisfied with the outcome; or it being solved and the individual being satisfied with the outcome. A possible reaction to the first two outcomes can be moral distress (Kälvemark Sporrong, 2007). This model resembles the one described by Wilkinson (1987/1988). In this model, the phenomenon of moral distress includes both the experience of a situation in which a moral decision not being followed through gives rise to

18
painful feelings and disequilibrium, and effects such as coping behaviors (successful or unsuccessful) and immediate and long-term effects on the care of the patient (Wilkinson, 1987/1988).
Research on moral distress within healthcare
Although the definition of moral distress is profession neutral, it has been researched mostly among nurses but also among physicians (e.g. Førde & Aasland, 2008), social workers (Brazil, Kassalainen, Ploeg & Marshall, 2010) and auxiliary nurses (Kälvemark, Höglund, Hansson, Westerholm & Arnetz, 2004). The predominant method of data collection has been the questionnaire, with the Moral Distress Scale (Corley, Elswick, Gorman & Clor, 2001; Corley, Minick, Elswick & Jacobs, 2005), based on Jameton’s conceptualization of moral distress, being the most used. Situations in which moral distress has been shown to arise are, among others, those when the level of staff is considered unsafe (Corley et al., 2005), when a lack of staff forces the personnel to prioritize between equally important tasks (Kälvemark et al., 2004) and when there is disagreement regarding the appropriate level of treatment (Hamric & Blackhall, 2007). Corley et al. (2005) found that higher age was associated with lower levels of moral distress, but Mobley, Rady, Verheijde, Patel and Larson (2007) and Pauly, Varcoe, Storch and Newton (2009) found no statistically significant associations between moral distress and demographic variables. Frequency of moral distress has been shown to be negatively correlated to perceptions of ethical climate (Corley et al., 2005) and positively correlated to emotional exhaustion (Meltzer & Huckabay, 2004). Feelings associated with the experience of moral distress include anger and guilt (Deady & McCarthy, 2010) as well as helplessness (Harrowing & Mill, 2010) and self-blame (Kelly, 1998). Avoiding patient interaction (Deady & McCarty, 2010; Kelly, 1998), working fewer hours or leaving the unit (Kelly, 1998) or even leaving nursing (Corley et al., 2005; Kelly, 1998) are strategies nurses have used in order to cope with moral distress. One study (Kälvemark Sporrong, Arnetz, Hansson, Westerholm & Höglund, 2007) reports on the use of a structured education and training program in ethics, which aimed at decreasing the moral distress of

19
healthcare sector professionals, but moral distress did not change significantly after the training program. The research on moral distress has largely been concerned with the negative experiences of moral distress, but according to Hanna (2004) moral distress can involve aspects such as development of moral character if it is handled well.
Criticism of the concept of moral distress
During recent years the concept of moral distress has been criticized from different points of view. Based on empirical work, Kälvemark et al. (2004) have proposed a revision of Jameton’s definition of moral distress, in which moral distress is not separated from moral dilemmas or moral uncertainty. Jameton’s definition has been viewed as unclear and incomplete (Hanna, 2004), and the research based on this definition as being too focused on the distress reaction while the ethical principles at stake in a certain situation and the external factors preventing a desired action are not sufficiently articulated. The term moral stress has therefore been proposed in order to capture these aspects (Lützén, Cronqvist, Magnusson & Andersson, 2003). A critical overhaul of the concept of moral distress has been advocated, focusing on what the concept might add to our understanding of situations experienced as ethically difficult and of what it is that properly qualifies as moral distress and not as individuals’ dissatisfaction with decisions that are made (McCarty & Deady, 2008; Repenshek, 2009).
Similar concepts
As mentioned above, concepts similar to that of moral distress have been proposed, e.g. moral stress (Lützén et al., 2003). The term ethics stress has also been used (Ulrich et al., 2007). Another closely related concept is that of stress of conscience. Stress of conscience has its theoretical roots in the philosophy, theology and psychology literature on the concept of conscience. In this literature, conscience is described as the voice of moral responsibility – a moral responsibility we have towards both ourselves and others (Juthberg, 2008). A study of staff within psychiatric care showed that conscience was perceived as an

20
authority, a warning signal and a burden, but that it was also a resource. Conscience is something that requires sensitivity as it must be interpreted and is culturally sensitive (Dahlqvist et al., 2007). If the conscience is perceived as a burden and a person feels the need to deaden it, (s)he runs a higher risk of emotional exhaustion (Dahlqvist, 2008; Juthberg, Eriksson, Norberg & Sundin, 2008). A troubled conscience alerts a person who is morally sensitive that ethical values or principles are at stake and can guide the action. If, however, the person is unable to act in accordance with his/her conscience (s)he experiences an inner conflict, labeled stress of conscience (Glasberg et al., 2006). Stress of conscience refers not only to stress that can be a result of institutional obstacles but also to stress that arises due to self-selected actions or neglect (Glasberg, 2007). The concept of stress of conscience therefore differs from that of moral distress in that it does not solely focus on institutional obstacles for ethical actions but rather widens the perspective to also include the actor’s responsibility. To summarize, moral distress has been studied for nearly three decades and, despite the fact that the original definition by Jameton (1984) has been criticized, it is still the definition used as a starting point for most moral distress studies. Although moral distress could be regarded as arising due to organizational shortcomings, there is a limited amount of research on the relation between moral distress and organizational aspects, such as ethical climate.
Ethical climate
Original definition
During the late 1980s a new concept within the field of business ethics research was described, namely that of ethical climate. Its first definition described it as “the shared perception of what is ethically correct behavior and how ethical issues should be handled” (Victor & Cullen, 1988 p.77-78).
21
Ethical climate and organizational research
Ethical climate has often been considered to belong to the research field of organizational climate (Mayer, Kuenzi, & Greenbaum, 2009), i.e. the psychological life of organizations (Schneider, Ehrhart, & Macey, 2011). In the early organizational climate surveys, the focus of study was individuals’ perceptions of climate in relation to the individual behavior of the respondent, and not in relation to organizational effectiveness. This was later considered a weakness since both the variable climate and the outcome should be on a unit level of analysis in order for research to be regarded as organizational climate research. A distinction was therefore suggested between psychological climate and organizational climate. The former refers to studies in which both the unit of data collection and the unit of analysis was the individual. The latter requires the individual data to be aggregated to reflect the organizational attribute of climate (Schneider et al., 2011) as well as high within-group agreement, reflecting that the perceptions are shared and therefore comprise an organizational variable (James et al. 2008). Ethical climate could therefore be regarded as part of the tradition of research on organizations. However, it should not be viewed as a certain form of organizational climate unless data are aggregated and there is high within-group agreement. If this is not the case, it should be regarded as a variable on the psychological climate level (Mayer et al., 2009). This does not mean that ethical climate and psychological climate are the same; only that they can be measured on the same level. Ethical climate refers to perceptions of how situations involving ethical problems or other ethical dimensions are or should be handled in an organizational context (cf. Olson, 1995; Victor & Cullen, 1988). Psychological climate, however, refers to employees’ perceptions and interpretations of psychological climate dimensions such as role clarity, job importance, leader support and work-group cooperation (Baltes, 2001).
Criticism of the original definition
Victor and Cullen’s definition of ethical climate, which is the basis for the majority of research on ethical climate, is regarded by Mayer at al. (2009) as insufficient as it is unclear what “correct behavior” refers to; it could be either

22
what is considered correct behavior specific to a particular organization or behaviors that are in concordance with general societal norms. The fact that the definition says nothing about policies, practices or procedures is also considered a weakness, since all of these are regarded as key components of climate. The “shared” perceptions are emphasized in the definition, but studies using this definition seldom mention the use of appropriate measures to study within-group agreement (Mayer et al., 2009). Alternative definitions have been proposed, e.g. by Olson (1995), that overcome these shortcomings.
Ethical climate in healthcare
Nearly a decade after the introduction of the term ethical climate in business ethics research, the term was introduced in the field of healthcare organizations. Olson (1995) then described ethical climate for nurses specifically as “nurses’ perceptions of how such issues [ethical issues] are handled” (p. 90). Since then, ethical climate has been studied within healthcare contexts, predominantly hospitals, with mainly nurses as respondents. The studies have used different theoretical starting points, such as the ethical climate framework developed by Victor and Cullen (e.g. Filipova, 2009; Tsai & Huang, 2008) or Olson’s work on ethical climate in hospitals (e.g. Lützén, Blom, Ewalds-Kvist & Winch, 2010; Pauly et al., 2009). The knowledge generated from these studies includes the discovery of a relationship between type of ethical climate perceived and intent-to-leave (Filipova, 2009) as well as between type of ethical climate perceived and job satisfaction (Tsai & Huang, 2008). It has also been reported that the more positive the ethical climate is perceived to be, the less the intent to leave is and the higher the job satisfaction is (Ulrich et al., 2007). A negative association has been found between ethical climate and moral distress, implying that the more positive the ethical climate is perceived to be, the less moral distress is reported (Corley et al., 2005). To summarize, in the planning and initiation of the present research process only one study was found that had shown results pointing to the importance of experiencing a positive ethical climate. However, there was a lack of studies that could contribute to the knowledge about what actions promote a positive
23
ethical climate, i.e. what actions are considered to promote the handling of situations of moral distress and ethical problems.
Overview of the relation between the concepts
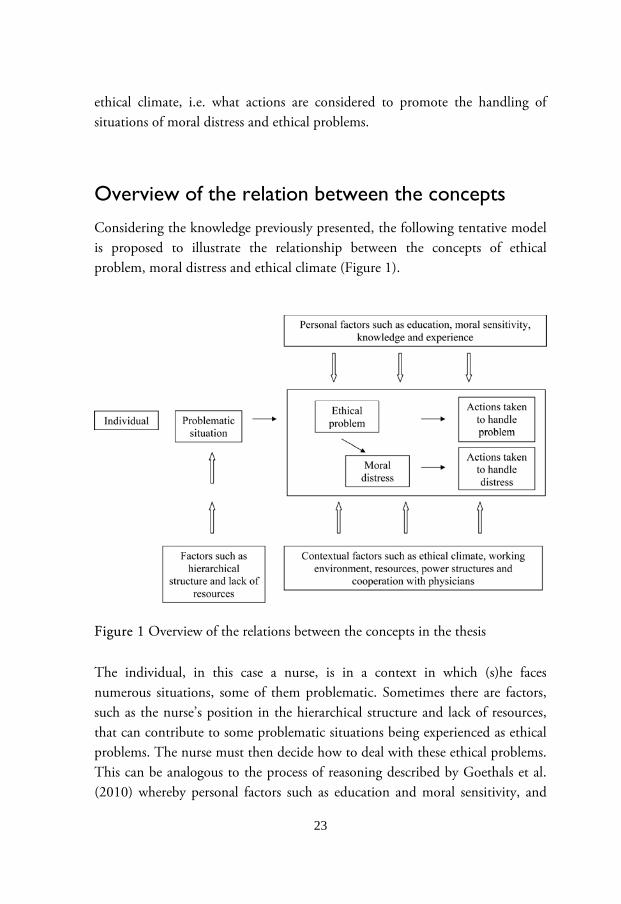
Considering the knowledge previously presented, the following tentative model is proposed to illustrate the relationship between the concepts of ethical problem, moral distress and ethical climate (Figure 1).
Figure 1 Overview of the relations between the concepts in the thesis The individual, in this case a nurse, is in a context in which (s)he faces numerous situations, some of them problematic. Sometimes there are factors, such as the nurse’s position in the hierarchical structure and lack of resources, that can contribute to some problematic situations being experienced as ethical problems. The nurse must then decide how to deal with these ethical problems. This can be analogous to the process of reasoning described by Goethals et al. (2010) whereby personal factors such as education and moral sensitivity, and

24
contextual factors such as a stressful working environment and insufficient resources, play important roles. When the nurse has decided what to do, actions are taken to handle the ethical problem. As described by Goethals et al. (2010), factors like knowledge and experience might facilitate this process whereas there are a number of contextual factors that might limit one’s ability to act as desired, such as poor cooperation with physicians and traditional power structures. If there is no acting space, the ethical problem might grow into experiences of moral distress. In this case, actions cannot be directed at handling the ethical problem but are instead focused on dealing with the feelings of moral distress (Goethals et al., 2010). It might be hypothesized that a perceived positive ethical climate, which can be regarded as a contextual factor, might facilitate this process with less moral distress as a result.
Rationale for the thesis
Previous research has shown that nurses experience ethical problems and moral distress in their work. There is considerable research on what ethical problems nurses experience, but there are settings in which this has not been investigated and where it would be of value to study it. Knowledge of the factors that can contribute to the arising of ethically problematic situations is important, since without such knowledge it is difficult to deal with the ethical problems appropriately. However, research on this aspect seems sparse. In cases of moral distress, organizational shortcomings are regarded as the reason for these experiences. Despite this, there is a limited amount of research on the relationship between moral distress and organizational aspects, for example ethical climate. Ethics is an integral part of healthcare and situations involving ethical problems and moral distress will always arise. Therefore, more knowledge is needed about what actions are reported to be taken in order to handle ethical problems and

25
moral distress, and especially what actions are considered to contribute to these situations being handled well. At the beginning of this research project, little was known about the connection between moral distress and ethical climate and even less about what contributes to a positive ethical climate. This pointed to a need to explore the actions that promote a perceived positive ethical climate.

26
Aim of the thesis
The aim of the thesis was to explore and describe the encountering of ethical problems and moral distress by nurses. The research questions were: What situations are experienced as ethically problematic and morally distressing? (I, II, III) What factors contribute to the arising of ethically problematic situations? (I, II) What actions do nurses report are taken in ethically problematic and morally distressing situations in order to handle them, thus creating an ethical climate? (I, II, III, IV)
Method
Design
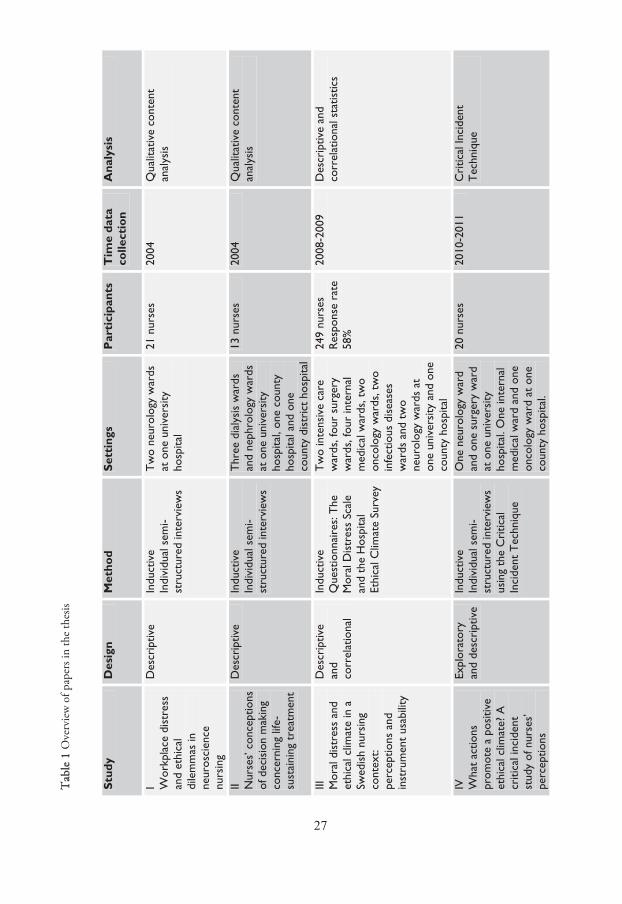
Different kinds of designs have been used in this thesis (Table 1). Descriptive design was used in Papers I and II since what was desired were straight descriptions of the phenomena studied and low-inference interpretations of data (Sandelowski, 2000). The focus on individuals’ experiences called for a qualitative approach (Patton, 2002). From Papers I and II, results emerged that called for being studied in a larger sample in Paper III. Paper III aimed at describing perceptions of phenomena and investigating the relationship between them. This required descriptive and correlational designs (Brink & Wood, 1998), and consequently a quantitative approach. In Paper IV, a closer examination of results from Paper III was carried out. Since the problem area had not previously been studied in any depth in a sample with personal experiences of the phenomenon an exploratory design, together with a descriptive one (Brink & Wood, 1998), with a qualitative approach was chosen.
27
TABELL 1
Tab
le 1
Ove
rvie
w o
f pap
ers i
n th
e th
esis
Stud
y D
esig
n M
etho
d Se
ttin
gs
Par
tici
pant
s
Tim
e da
ta
colle
ctio
n A
naly
sis
I Wor
kpla
ce d
istr
ess
and
ethi
cal
dile
mm
as in
ne
uros
cien
ce
nurs
ing
Des
crip
tive
Indu
ctiv
e In
divi
dual
sem
i-st
ruct
ured
inte
rvie
ws
Tw
o ne
urol
ogy
war
ds
at o
ne u
nive
rsity
ho
spita
l
21 n
urse
s 20
04
Qua
litat
ive
cont
ent
anal
ysis
II Nur
ses’
con
cept
ions
of
dec
isio
n m
akin
g co
ncer
ning
life
-su
stai
ning
tre
atm
ent
Des
crip
tive
Indu
ctiv
e In
divi
dual
sem
i-st
ruct
ured
inte
rvie
ws
Thr
ee d
ialy
sis
war
ds
and
neph
rolo
gy w
ards
at
one
uni
vers
ity
hosp
ital,
one
coun
ty
hosp
ital a
nd o
ne
coun
ty d
istr
ict
hosp
ital
13 n
urse
s 20
04
Qua
litat
ive
cont
ent
anal
ysis
III
Mor
al d
istr
ess
and
ethi
cal c
limat
e in
a
Swed
ish
nurs
ing
cont
ext:
perc
eptio
ns a
nd
inst
rum
ent
usab
ility
Des
crip
tive
and
corr
elat
iona
l
Indu
ctiv
e Q
uest
ionn
aire
s: T
he
Mor
al D
istr
ess
Scal
e an
d th
e H
ospi
tal
Ethi
cal C
limat
e Su
rvey
Tw
o in
tens
ive
care
w
ards
, fou
r su
rger
y w
ards
, fou
r in
tern
al
med
ical
war
ds, t
wo
onco
logy
war
ds, t
wo
infe
ctio
us d
isea
ses
war
ds a
nd t
wo
neur
olog
y w
ards
at
one
univ
ersi
ty a
nd o
ne
coun
ty h
ospi
tal
249
nurs
es
Res
pons
e ra
te
58%
2008
-200
9 D
escr
iptiv
e an
d co
rrel
atio
nal s
tatis
tics
IV
Wha
t ac
tions
pr
omot
e a
posi
tive
ethi
cal c
limat
e? A
cr
itica
l inc
iden
t st
udy
of n
urse
s’
perc
eptio
ns
Expl
orat
ory
and
desc
ript
ive
Indu
ctiv
e In
divi
dual
sem
i-st
ruct
ured
inte
rvie
ws
usin
g th
e C
ritic
al
Inci
dent
Tec
hniq
ue
One
neu
rolo
gy w
ard
and
one
surg
ery
war
d at
one
uni
vers
ity
hosp
ital.
One
inte
rnal
m
edic
al w
ard
and
one
onco
logy
war
d at
one
co
unty
hos
pita
l.
20 n
urse
s 20
10-2
011
Cri
tical
Inci
dent
T
echn
ique

28
Participants and settings
All participants were recruited from acute care wards that treated adults only at one university hospital, two county hospitals and one county district hospital in Sweden (Table 1). They were selected using different purposeful sampling strategies (Patton, 2002). In Paper I, 21 nurses from two neurology wards at one university hospital participated. The setting of neurology wards was chosen because there was scant research on ethical problems in this setting, in which nurses care for patients with varying severity of conditions. The participants were selected through criterion sampling (Patton, 2002) whereby all nurses who met the criterion of working dayshifts were invited to participate. All but one gave consent to participate. In Paper II, 13 nurses working at dialysis and/or nephrology wards at one university hospital, one county hospital and one county district hospital participated. Staff at these wards was involved in a research project on ethics rounds directed at investigating a professional perspective on the boundaries of life-sustaining treatment (Svantesson, Anderzén-Carlsson, Thorsén, Kallenberg & Ahlström, 2008a; Svantesson, Löfmark, Thorsén, Kallenberg & Ahlström, 2008b). The setting of dialysis and nephrology wards was motivated by the fact that previous studies concerning nurses’ conceptions of life-sustaining treatment had been conducted in settings where the patients are mostly decision-incompetent. The opposite is often the case with patients undergoing dialysis. The participants were selected through criterion sampling, used in two ways (Patton, 2002). First, all the nurses at these wards were invited to participate, but only ten volunteered and six met the inclusion criterion of having participated in the first ethics round. Thereafter, participants known for a willingness to verbalize opinions in general (not necessarily ethical issues) were approached. All these seven gave consent to participate. In Paper III, 249 nurses (response rate 58%) from 16 wards at one university hospital and one county hospital participated. The wards included intensive care, surgery, internal medical, oncology, infectious diseases and neurology

29
wards. Intensity sampling (Patton, 2002) was used to select the wards and criterion sampling (Patton, 2002) to select participants. First, the wards were chosen on the basis that the nurses on these wards might have experience of the situations described in the Moral Distress Scale (MDS). Thereafter, all nurses who met the criterion of working dayshifts at these wards were invited to participate. In Paper IV, 20 of the participants in Paper III participated. These participants worked at one neurology ward, one surgery ward, one internal medical ward and one oncology ward at one university hospital and one county hospital. Intensity sampling (Patton, 2002) was used to select wards that were perceived as having a positive ethical climate. Thereafter, criterion sampling was used whereby nurses who were judged to be able to provide rich descriptions of the phenomenon under study were asked to participate. Of the 28 nurses who were given information on the study, 20 were interviewed.
Qualitative methods
Data collection
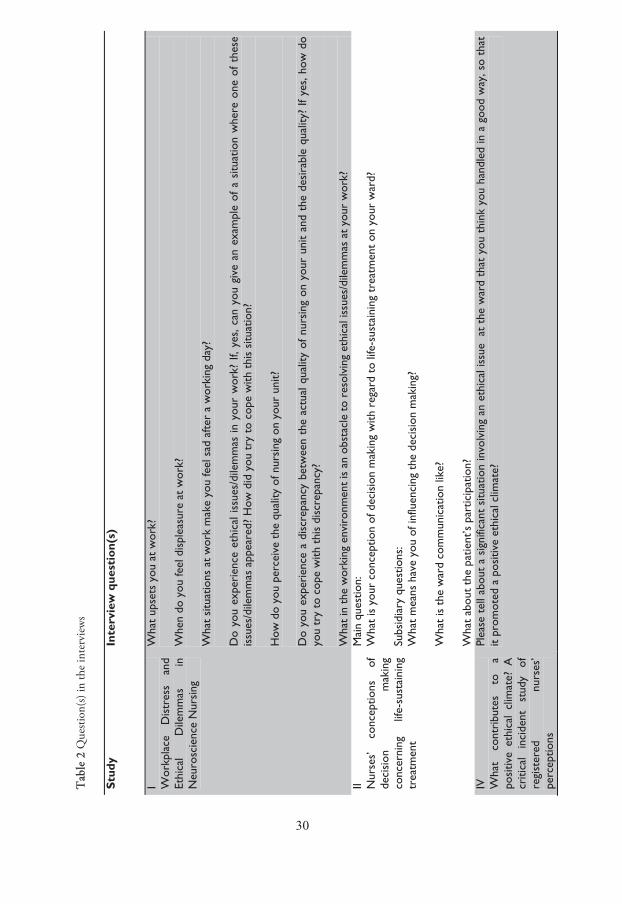
The method of data collection in Papers I, II and IV was the individual semi-structured interview, meaning that a guide with suggested questions was used but that these were not necessarily asked in a predetermined order (Kvale & Brinkman, 2009). In Paper I an interview guide with several questions was used, whereas a main question was asked in Papers II and IV (Table 2). When the answers were unclear to the interviewer, subsidiary questions were asked in order to clarify. The questions in Paper I were based on the project leader’s (fourth author of the paper) knowledge of the research area. In Paper II the questions were formulated by the second author against the background of previous studies (Breen, Abernethy, Abbott & Tulsky, 2001; Reckling, 1997; Viney, 1996; Svantesson, Sjökvist & Thorsén, 2003), which had identified shortcomings in the areas in question. In Paper IV, the question was formulated by the first author in accordance with Flanagan’s Critical Incident Technique (CIT) (1954).
Tab
le 2
Que
stion
(s) i
n th
e in
terv
iew
s
Stud
y In
terv
iew
que
stio
n(s)
I Wor
kpla
ce
Dis
tres
s an
d Et
hica
l D
ilem
mas
in
N
euro
scie
nce
Nur
sing
Wha
t up
sets
you
at
wor
k?
Whe
n do
you
feel
dis
plea
sure
at
wor
k?
Wha
t si
tuat
ions
at
wor
k m
ake
you
feel
sad
afte
r a
wor
king
day
? D
o yo
u ex
peri
ence
eth
ical
issu
es/d
ilem
mas
in y
our
wor
k? I
f, ye
s, c
an y
ou g
ive
an e
xam
ple
of a
situ
atio
n w
here
one
of
thes
e is
sues
/dile
mm
as a
ppea
red?
How
did
you
try
to
cope
with
thi
s si
tuat
ion?
H
ow d
o yo
u pe
rcei
ve t
he q
ualit
y of
nur
sing
on
your
uni
t?
Do
you
expe
rien
ce a
dis
crep
ancy
bet
wee
n th
e ac
tual
qua
lity
of n
ursi
ng o
n yo
ur u
nit
and
the
desi
rabl
e qu
ality
? If
yes,
how
do
you
try
to c
ope
with
thi
s di
scre
panc
y?
Wha
t in
the
wor
king
env
iron
men
t is
an
obst
acle
to r
esol
ving
eth
ical
issu
es/d
ilem
mas
at
your
wor
k?
II Nur
ses’
co
ncep
tions
of
de
cisi
on
mak
ing
conc
erni
ng
life-
sust
aini
ng
trea
tmen
t
Mai
n qu
estio
n:
Wha
t is
you
r co
ncep
tion
of d
ecis
ion
mak
ing
with
reg
ard
to li
fe-s
usta
inin
g tr
eatm
ent
on y
our
war
d?
Subs
idia
ry q
uest
ions
: W
hat
mea
ns h
ave
you
of in
fluen
cing
the
dec
isio
n m
akin
g?
Wha
t is
the
war
d co
mm
unic
atio
n lik
e?
Wha
t ab
out
the
patie
nt’s
par
ticip
atio
n?
IV
Wha
t co
ntri
bute
s to
a
posi
tive
ethi
cal
clim
ate?
A
criti
cal
inci
dent
st
udy
of
regi
ster
ed
nurs
es’
perc
eptio
ns
Plea
se t
ell a
bout
a s
igni
fican
t si
tuat
ion
invo
lvin
g an
eth
ical
issu
e a
t th
e w
ard
that
you
thi
nk y
ou h
andl
ed in
a g
ood
way
, so
that
it
prom
oted
a p
ositi
ve e
thic
al c
limat
e?
30
Insert Table 2 here

31
All the interviews were tape-recorded and transcribed verbatim by an experienced secretary, but did not include non-verbal information.
Data analyses
Interview data were analyzed using qualitative content analysis (Papers I and II) and the procedures of the CIT (Paper IV). Comments regarding the MDS (Paper III) were read through and then sorted into categories based on similarities in the situations described. Content analysis has been described as a research technique for making inferences from texts (Krippendorff, 2004) whereby both the manifest content, i.e. the visible and obvious, and the latent content, i.e. the underlying meaning, of the text can be described (Downe-Wamboldt, 1992). Both the manifest and the latent content involve interpretation, but this varies in depth and level of abstraction (Graneheim & Lundman, 2004). The decision to use qualitative content analysis for analyzing data in Papers I and II was based on the fact that there were no methodological or theoretical assumptions that had guided the data collection. The analyses were therefore also inductive, and followed the models for analysis described by Graneheim and Lundman (2004). The initial step of the analyses was reading through the interview texts several times. Thereafter sentences and paragraphs containing the same meaning, i.e. meaning units, were marked. These were condensed so that the text was shortened but the core meaning was preserved. Thereafter, each condensed meaning unit was assigned a code. In Study I the following steps involved the generation of subthemes and preliminary themes based on the codes. Thereafter, a sorting of meaning units with appropriate codes, subthemes and preliminary themes was done using the framework of content areas. These had been developed on the basis of the interview questions. Within each of the content areas, themes were formulated that captured the latent content of the data. In Study II the codes were compared with each other and similar codes were combined to form a subcategory. The different subcategories were then compared and abstracted into five categories. The final step involved the

32
formulation of a theme that captured the central latent content of all the categories. The Critical Incident Technique (CIT) consists of procedures for both the collection of observations of human behaviour and the analysis of these observations (Flanagan, 1954). The CIT was chosen because it focuses on solving practical problems (Flanagan, 1954). In the analysis, significant situations were identified together with the actions the nurses considered had led to a given situation being handled in a good way, i.e. actions that had contributed to a positive ethical climate. Each action was assigned a code that captured the essential part of the action in a few words. The codes were then compared and similar codes were assembled into a subcategory. Thereafter, the subcategories were grouped into categories, which in the final step were brought together into main areas.
Trustworthiness
In qualitative research quality is often assessed using the criteria of credibility, dependability, confirmability and transferability, which together establish the trustworthiness of the research (Lincoln & Guba, 1985). During the analysis for Papers I, II and IV the resulting material was discussed and reflected on among the co-authors, who had previous experience of qualitative research. They critically examined the analyses performed by the first author, and these were modified until there was consensus among the authors. This way of working reinforced the credibility and the confirmability of the results. To facilitate the judgements of others concerning transferability, descriptions are given on the settings and the characteristics of participants together with rich presentations of the study findings.

33
Quantitative method
Data collection
In Paper III the Moral Distress Scale and the Hospital Ethical Climate Survey were used. The Moral Distress Scale (MDS) is an instrument for measuring the extent to which moral distress is a part of nurses’ professional experience. It is based on Jameton’s concept of moral distress, House and Rizzo’s role conflict theory and Rokeach’s theory on values and value systems (Corley et al., 2001). The revised MDS consists of 38 items describing situations that might give rise to moral distress. For each situation participants are asked to indicate the level of moral distress perceived and how often they encounter the situation. Responses are given on a seven-point Likert-type scale, ranging from “none”/”never” (0) to “a great extent”/”very frequently” (6). The MDS should therefore be considered an ordinal scale (Svensson, 2005). Cronbach’s alpha is 0.98 for the revised MDS level dimension and 0.90 for the frequency dimension (Corley et al., 2005). For the purpose of Paper III, the revised MDS with 38 items was translated into Swedish by three independent authorized translators. The translations were critically discussed by the doctoral student and a senior researcher with experience in the development and translation of instruments. Six items were excluded as they were considered irrelevant in a Swedish context. The Swedish MDS therefore consists of 32 items. Thereafter, the Swedish MDS was pilot tested by seven nurses working at different wards, resulting in clarifications regarding the completion of the instrument. In the data collection proper, the participants were also invited to suggest other situations that give rise to moral distress that they considered should be included in a moral distress questionnaire. These comments were analyzed using a qualitative method. Participants were also asked to indicate how often they had considered leaving a position due to moral distress (“never”, “seldom”, “sometimes”, “often”) and whether they had ever done so (“yes”/ “no”). The Hospital Ethical Climate Survey (HECS) is an instrument for measuring the ethical climate at hospital wards as perceived by nurses. The HECS is based on a concept analysis of the concept of ethical climate in healthcare organizations,
34
an integrative review of the literature in business and nursing ethics and on the developer’s experience in nursing practice and administration. The instrument development was guided by Schneider’s concept of types of organizational climate and Brown’s conditions for ethical reflection in organizations. It consists of 26 items describing different practices in a nurse’s work setting. Scores are given on a five-point Likert-scale ranging from “Almost Never True” (1) to “Almost Always True” (5) (Olson, 1998); thus the HECS is an ordinal scale (Svensson, 2005). Reliability Cronbach’s alpha is 0.91 for the whole scale, with a range of 0.68 to 0.92 for its five different dimensions (nurses’ relationships with peers, patients, managers, the hospital and physicians) (Olson, 1998). The translation and pilot test procedures were in accordance with those used for the MDS, but no further adaptations to a Swedish context were judged to be necessary.
Data analyses
Data from the instruments used in Paper III were ordinal. This type of data demands non-parametric statistical methods (Svensson, 2005). When investigating relationships between moral distress and ethical climate, Spearman’s rho was calculated. Significant levels were set at a two-tailed p<0.05.
Validity and reliability
In order to quantify validity, instruments were chosen that had taken different steps in order to support validity. The validity methods used when developing the instruments were content validity (MDS and HECS) (Corley et al., 2001; Olson, 1998) and construct validity (HECS) (Olson, 1998). When selecting an instrument, a decision needs to be made regarding which of the aspects of reliability are most relevant. Equivalence is most appropriate in observational studies (Polit & Beck, 2011) and was therefore not relevant for Paper III. Stability refers to the stability of the results when using the same
35
instrument on different occasions (Polit & Beck, 2011). Ethical climate is considered relatively enduring but not static (Olson, 1995), and it could therefore be regarded as relevant to assess the stability of the HECS. However, it is unsure whether perceptions of moral distress as a phenomenon are stable over time. Based on this, it was deemed that it was most relevant to calculate the internal consistency (Polit & Beck, 2011) of both instruments.
Ethical considerations
Regional Ethical Review Boards approved Papers II-IV (dnr Ö3266 040818 Paper II; dnrs 18-08 and 18-08 T Paper III; dnr 2010/289-32 Paper IV). For Paper I no formal approval from a Regional Ethical Review Board was needed, in accordance with the then-present Swedish act (Ministry of Eduation and Cultural Affairs, 2003:460) concerning the ethical review of research involving humans. Supported by the principle of autonomy, participation was based upon informed consent (Council for International Organizations of Medical Sciences [CIOMS], 2002). Participants were given both oral and written information about the studies, in which it was clearly stated that participation was voluntary and that they could withdraw at any time. Completion of an interview or of the questionnaires was viewed as consent to participate. In Paper IV the participants also gave a written consent to participate. Participants were guaranteed confidentiality. This implied not only that data were safely stored so that the participants’ identities were protected, but also that information that could identify a certain participant, colleague or patient was left out when reporting data. This was done with support from the principle of beneficence (CIOMS, 2002). The principle of justice demands an equitable selection of participants and equality in the distribution of benefits and burdens among the population group likely to benefit from the research (CIOMS, 2002). In this case the population was nurses, who, as a group, are not considered vulnerable. The burden of participation can be divided into the time required for the

36
completion of an interview or of questionnaires on the one hand and the possible psychological burden of participation, i.e. the possible distress that can result from discussing ethical issues on the other. However, the time required for participation was between 15 minutes and one and a half hours, and there has been no indication that participation has caused the participants emotional distress. The burden of participation could therefore been regarded as relatively limited. The direct gain the participants received from participation is probably small, in that working conditions or practices considered negative probably did not change as a result of their participation. However, participation was an opportunity to share experiences, which could be considered meaningful for the participants. Although the participants probably received little direct gain from participating, the rationale for the papers could be motivated from a wider perspective. The participation involved little risk to the participants, and the new and valuable knowledge generated from the papers could be considered to weigh heavier than these risks.
Results
Situations that are experienced as ethically problematic and morally distressing
Decision making regarding life-sustaining treatment could be experienced as ethically problematic and morally distressing: when no decision was made, when there were incomprehensible shifts between treatment and no treatment, and when the nurse did not agree with the decision. Difficulties in maintaining a patient’s integrity or in giving the necessary care could also be experienced as ethical problems and moral distress. Not being competent enough or working with colleagues lacking competence was morally distressing, and the same applied when the level of nursing staff was considered inadequate.
37
The ethical problems associated with decision making concerning life-sustaining treatment regarded the initiation of treatment, as well as its continuation or withdrawal. The ethical question was whether the treatment would benefit the patient or cause suffering (I, II). Just because it was possible to initiate or continue life-sustaining treatment, this did not mean it was the right thing to do; the patient’s quality of life had to be taken into consideration. The nurses found these situations difficult, and experienced powerlessness and moral distress (I). Sometimes no decision was made, or there could be shifts between life-sustaining treatment and the withdrawal of such treatment, which the nurses considered incomprehensible. These situations were emotionally difficult to bear (I, II). But it could also be ethically problematic to care for a patient for whom a decision to withdraw treatment had been made but the patient continued to live (I). At other times the nurses felt powerless when having to withhold treatment from a patient and when trying to explain this to next of kin (I). When a nurse had to initiate life-sustaining treatment although (s)he felt that this only prolonged death, (s)he could experience moral distress (III). Moral distress, frustration and anger also arose when the nurses had to carry out physicians’ orders for tests and treatment although a patient was terminally ill (I, III). Not being included in the decision making process contributed to the difficulty of the situation (I, II). Sometimes the nurses felt that the life-sustaining treatment was continued too long (II), but there were also situations when they felt that the decision to withdraw treatment was too rash (I). Another aspect of the ethical problems associated with the decision making about life-sustaining treatment was that the nurses and the patient’s next of kin could hold different opinions on what the level of treatment should be, thereby giving rise to conflict (I). Difficulties in maintaining a patient’s integrity, such as being able to talk privately to the patient or being in a situation in which the nurse had to persuade the patient to accept a certain situation, for example new living arrangements, could be experienced as ethically problematic (I). Not being able to give the necessary care and situations in which the complexity of the nurses’ working situation was obvious were also considered morally distressing. Actions taken (or not taken) that meant that the patient might suffer were also experienced as morally distressing. This could involve having to carry out unnecessary tests and treatments, or not being able to alleviate a patient’s pain
38
with the prescribed medications (III). Not feeling that one’s own competence, or the competence of other healthcare professionals, was satisfactory was experienced as morally distressing, and the same applied to cases in which the level of nursing staff was considered unsafe (III).
Factors that contribute to the arising of ethically problematic situations
Several factors could contribute to the rise of an ethically problematic situation. Some of these were inadequate communication between healthcare staff, the physicians’ ways of handling potentially ethically problematic situations and patients’ poor state of health, which hindered their participation in the planning of their own care. Institutional obstacles could also contribute to the rise of an ethical problem. One factor that was considered to contribute to the arising of ethically problematic situations was inadequate communication with other healthcare staff, mainly with physicians (I, II). This lack of communication was thought to be a result of hierarchical structures, according to which physicians have more power than nurses. Inadequate communication also meant that nurses did not always have the information they needed (I) and felt there was a lack of explanation. Not knowing why a physician had made a certain decision regarding the aggressiveness of treatment for a patient made it difficult for them to accept the decision (II). They also felt that physicians did not listen to them; the physicians seldom asked their opinion before decisions were made, and the nurses did not feel that their knowledge about the patient was considered valuable. In short, they did not feel respected as professionals (I, II). The physicians’ ways of handling potentially ethically problematic situations also contributed to the rise of ethical problems. The nurses experienced that physicians were afraid of making end-of-life decisions and shied away from them. This manifested itself in a perceived hesitation to talk to patients about their future treatment. This was attributed to prestige; the physicians had to know what the right decision was and were not willing to give up treatment too
39
soon (II). The nurses also felt there was a lack of consensus among the physicians as a group, resulting in a lack of a clear strategy concerning the patient’s treatment (II). Sometimes the patient’s poor health contributed to the arising of an ethically problematic situation. This could be the case both when a decision had to be made concerning life-sustaining treatment (II) and at care-planning meetings together with a social welfare case officer (I). When a patient was too ill to be involved in the decision regarding the future direction of treatment, this could result in the patient being given treatment although (s)he did not want it but was too ill to be able to express this (II). A patient in a poor state of health was not always able to take part in decisions during care-planning meetings, and it was therefore unsure what the patient’s opinion was about what kind of help (s)he thought was needed (I). Due to institutional obstacles, a patient’s integrity could not always be maintained. One of these obstacles was the physical environment at the wards, which did not have enough single rooms, meaning that patients often had to share rooms and making it difficult to talk privately with them (I). Another obstacle was the municipality’s inability to provide for patients’ needs. Sometimes there were no suitable living arrangements available to a patient, which meant that aftercare was not always in accordance with the patient’s needs (I).
Actions reported taken in order to handle ethically problematic and morally distressing situations, thus creating an ethical climate
Some of the actions reported to be used in order to handle ethically problematic and morally distressing situations, thus creating an ethical climate, were getting and using support in different ways. One type of support was offered by policies and routines, and another type was offered by colleagues. It was important that explanations and information be given by physicians and managers in order for the nurses to know why a certain decision had been made or what was going

40
on. Working as a team, not least as an interprofessional team, was considered important for the handling of ethically problematic situations. This did not mean that there always had to be agreement on what to do and how to act, although this was required in certain situations. The nurses tried to do all they could for patients so that they could later feel that they had done their best. The nurses’ relationships with peers, physicians, managers, patients and the hospital were made up of different actions. When these actions promoted relationships that led to a perceived positive handling of ethically problematic situations, this meant that the ethical climate was considered positive and moral distress occurred less frequently (III). The use of policies and routines was regarded as one type of support when it was difficult to decide how to act or when motivating one’s actions (IV). Being able to turn to colleagues when situations were found to be ethically problematic was regarded as a valuable form of support (I, IV). This kind of support was considered reciprocal, as the nurses both received and gave support (IV). Discussions about ethically problematic situations were often informal, but there could sometimes be a more formal meeting for the whole staff at which a future decision regarding a patient’s treatment was discussed in order to shed light on as many aspects as possible. Another aim of the meeting could be for the physicians explain why a certain decision had been made (I). It was considered important to receive information and explanations in order to understand the reasons for decisions regarding a patient’s treatment, especially if the decision concerned life-sustaining treatment. In these cases the nurses could sometimes accept the decision even if they held a different opinion (IV). Information and explanations given by the nurse’s immediate manager were also helpful, as was the manager attending to the staff’s working situation by, for example, arranging the working schedule in a way that distributed the burden of caring for certain patients (IV). Working as a team was regarded as helpful when handling ethically problematic situations. One aspect of teamwork was interprofessional collaboration, which was especially helpful in complex patient care or emergency situations. This collaboration meant that not only did everyone do their part of the work, they also referred issues outside their sphere of responsibility to other professionals.

41
A precondition for this interprofessional collaboration was an experience of fewer professional hierarchies (IV). There also had to be a standard for behaviour within the team that the team members could refer to when they felt another team member was not behaving appropriately. This required that team members dared to speak out (IV). It was not considered that there always had to be agreement among the staff in all situations regarding what should be done, but in certain cases this was regarded as important. This was especially the case when a patient or next of kin behaved in a way that was difficult to handle and the staff therefore had to reach consensus on how to relate to this (IV). If the nurse did not agree with a physician’s decision (s)he could question this, based on what (s)he considered to be in the best interest of the patient. Physicians could sometimes, according to the nurses, show a certain irritation, but at other times they felt they were listened to and could reach a decision together. They acknowledged that the physicians had to make hard decisions and therefore offered their support and tried to make it easier by passing information among patient, next of kin and physician. But although they felt involved in decision making at times, they considered themselves to be the ones who rather carried out the decisions (II). One type of action reported taken in order to handle ethical problems and moral distress was doing all that could be done for a patient, so that the nurse could be satisfied with his/her own work even if the outcome was not the desired one (I). Attending to the psychosocial needs of the patients was one type of action reported taken when handling ethically problematic situations. This meant putting the patient’s needs first and could involve quite simple actions, but at other times it was more complex. It could involve complying with a patient’s wishes, and compromises sometimes having to be sought (IV). The nurses also took actions directed at the needs of next of kin when handling ethical problems (IV). When they knew they had done all they could, they could accept their own limitations (I). On the one hand the nurses felt it was important not to think about work when they were off duty, but on the other hand family and friends could offer support by listening to them tell about ethical problems at work. Leaving thoughts about work at work had become easier with increased working
42
experience, which had also increased the nurses’ ability to reflect upon ethically problematic situations from different perspectives (I).
Discussion
Reflections on the results
Ethical problems and moral distress – the importance of the professional role
The nurses described ethical problems and moral distress related to decision making concerning life-sustaining treatment (I, II, III), but also when they experienced difficulties in preserving a patient’s integrity (I) and when they could not give care that was necessary and safe (III). These results mainly confirm those of previous studies. The ethical problems and moral distress concerned with decision making regarding life-sustaining treatment mainly parallel those described by Bunch (2001) and Torjuul and Sörlie (2006). The inability to give safe care directed at the needs of the patient has also previously been reported to cause moral distress to varying degrees (Pauly et al., 2009; Zuzelo, 2007). Although these results are not new, they are nevertheless of value since they are partly derived from settings, such as neurology (I) and renal care (II), in which the phenomenon under study had not been investigated to any depth at the time of the respective studies. This is interesting because it raises the question of whether the specific setting matters when it comes to ethical problems and moral distress, or whether there are other factors that might be of greater importance. Chambliss (1996) has argued that the ethical problems nurses experience are systematic. By this he means that the same problems occur over and over again in various settings. The implication of this is that “the problem is not of the person but of the system” (Chambliss, 1996 p.91). It may be tempting to agree
43
with this line of reasoning, but that would mean that the individual and all the personal factors (cf. Figure 1) would be more or less ruled out and that the only thing that matters is the system, with the contextual factors (cf. Figure 1) as one aspect of it. Although it is beyond the aim of this thesis to clarify the balance between personal and contextual factors in the case of ethical problems, Chambliss’ (1996) questioning of the role of setting is worth bearing in mind in the following discussion. Several factors were described as contributing to the arising of an ethical problem (see Figure 1), such as institutional obstacles (I) and the poor health of patients (I, II). However, the dominant factor concerned the nurses’ relationships with other healthcare professionals, mainly physicians. Inadequate communication whereby the nurses did not feel listened to or respected as professionals (I, II), together with the physicians’ ways of handling situations (II), were stressed as contributing to many of the ethical problems. These factors are similar to those previously described by, for example, Cronqvist et al. (2004) and Oberle and Hughes (2001). Goethals et al. (2010) do not describe factors contributing to the rise of an ethical problem, but instead those that hinder ethical reasoning and the implementation of a decision in clinical practice. However, there are striking similarities between these and the ones described in the present studies: not being involved in decision making, poor cooperation with physicians, feelings of not being respected as a professional and hierarchical relationships (Goethals et al., 2010). Therefore, it seems that the same factors that might contribute to an ethical problem can also be active during the stages of ethical reasoning and implementation of a decision on how to act in clinical practice. What all the factors appear to have in common is that they concern the professional role of nurses, especially in relation to physicians. One of the most prominent factors contributing to the rise of an ethical problem mentioned by nurses was inadequate communication with physicians, mainly regarding decision making concerning life-sustaining treatment (I, II). Previous research regarding communication among physicians and nurses about decisions on life-sustaining treatment has shown that physicians consider nurses to be involved in the decision making to a higher degree than nurses do (Ferrand et al., 2003). This further emphasizes nurses’ perceptions of not being listened to or involved, and raises the question of why this might be. The nurses
44
interviewed (I, II) seldom used theoretical ethical concepts when describing ethical problems, and sometimes found it hard to express what it was they considered to be the problem. This has also been reported in previous studies (Bunch, 2001; Cronqvist et al. 2004; Gold, Chambers & Dvorak, 1995; Svantesson et al., 2008a). This difficulty expressing what they consider to be the ethical problem might be one constraint when trying to discuss their opinions with physicians. The consequence should not be a conclusion that the nurses were not aware of the specific ethical dimensions of the situation, but only that they were not used to putting them into words. In line with the suggestions by Rodney et al. (2002), nurses should be encouraged to frame what they perceive to be ethical problems in ethical terms, and might therefore be in need of informal as well as formal forums and education where they can gain this ability. As for the finding that the nurses considered that the physicians’ ways of handling decision making regarding life-sustaining treatment contributed to an ethical problem (II), it might be worth considering that nurses and physicians by regulation have different roles when it comes to these kinds of decisions. It is the physician who makes the decisions regarding life-sustaining treatment, but (s)he is advised to discuss these with the other staff responsible for the care of the patient (National Board of Health and Welfare, 2011:7). The nurses in Paper II acknowledged that it must be hard for a physician to make a decision whose outcome concerns another person’s life and death. However, they were critical of how the physicians handled the decision making and it was implicit that if they had been the ones who had to decide they would have acted differently. Since nurses are not in a position to make these kinds of decisions it is impossible to say if this would prove true, but it can be discussed whether this approach is a way forward if the wish is to improve practices of decision making concerning life-sustaining treatment. Chambliss (1996) warns that there is a risk that ethical difficulties may be labeled as such when they are in fact fundamental conflicts between professional groups, with their ground in significantly different goals of nurses and physicians, respectively (Chambliss, 1996). Therefore, it might be more purposive for nurses to clearly articulate their opinions on why they find a situation ethically difficult than to blame physicians for making the wrong decisions.
45
If, as argued here, there is a commonality in the factors of importance in the rise of ethically difficult situations and how they are handled – which is an aspect of nurses’ professional role – it might be asked whether there is a commonality in the situations experienced as ethically difficult. What seems to be the core of the ethical problems related to decision making regarding life-sustaining treatment (I, II, III), difficulties in preserving the patient’s integrity (I) and an inability to give necessary and safe care (III) is the inability to provide good care and thereby also fulfill the goal of nursing (cf. Gastmans et al., 1998). Rodney et al. (2002) have used the metaphor of moral horizon to describe the good that nurses strive for. Their description of the features of the moral horizon resembles in many ways what the nurses in the papers (I, III) considered to be good nursing care. Features of the moral horizon, according to Rodney et al. (2002), include relieving suffering, preserving human dignity, offering physical and psychological safety to patients and promoting the wellbeing of patients and their next of kin. But the moral horizon was not always reached due to different kind of constraints, resulting in feelings of powerlessness for the nurses (Rodney et al., 2002); this is also evident in the present findings (I, III). In a way this resembles the feelings of inadequacy described by psychiatric healthcare staff when experiencing a troubled conscience when not able to give the care that was deemed good (Dahlqvist, Söderberg & Norberg, 2009). Nurses’ professional role and the responsibility inherent in this role seem to be of importance when discussing not only what contributes to the arising of ethical problems but also what the core of these problems are. The attention might then be turned to the implications this has for how these kinds of situations can be handled and what actions are reported to be taken in order to deal with them.
Positive ethical climate – a mediating factor when encountering ethical problems and moral distress
Ethical problems often seem to arise because there are factors that contribute to a situation turning into an ethical problem. Successful handling of an ethical problem might involve dealing not only with the specific ethically problematic
46
situation but also with the factors that might have contributed to the rise of an ethical problem. This can prevent the problem from occurring over and over again. Thompson et al. (2006) state that there has traditionally been a focus on the individual’s responsibility for the handling of an ethical problem, but they advocate a different approach that considers the interconnections between individual, team and organization. This means that an individual does not work in isolation or in a vacuum but rather in an organization that is structured in a complex way and has connections with other organizations and society at large. The implication of this perspective is that depending on what kind of ethical problem is in focus and what factors might contribute to its rise, it is most properly dealt with at a certain level in the organization. In the case of inadequate communication (I, II) it might be most appropriately handled on what Thompson et al. (2006) call the macho (sic.) level, which concerns interdisciplinary cooperation and teamwork. Thompson et al. (2006) state that this is a task for team leaders, but it might be argued that this responsibility belongs to all the members of a team. If there are factors in the character of institutional obstacles (I) this might be dealt with on a meso or macro level, which concerns financial resources as well as inter-agency relations (Thompson et al., 2006). This is purely theoretical reasoning, but points to a need to consider the importance of actions emanating from different levels of an organization when handling ethical problems instead of leaving it up to the individual to deal with. The focus will now turn to the actions nurses report are actually taken in order to handle ethical problems, and which of these are regarded as promoting the handling of the problems. Perceptions of how ethical problems are handled might be summarized with the concept of ethical climate (Olson, 1995). This concept was explicitly used in Papers III and IV. In Papers I and II nurses told about how situations involving ethical problems were handled, but the concept of ethical climate was not used. Henceforth, however, the term ethical climate will be used for all the findings regarding the nurses’ perceptions of how ethical problems were handled. In Paper III it was shown that the more positive the ethical climate was perceived to be, i.e. the more positive perceptions the nurses had of how the
47
ethical problems were handled, the less frequently they reported that moral distress occurred. It must be taken into account, however, that ethical climate only explained some of the variation regarding frequency of moral distress. However, the most likely interpretation of this finding is that ethical climate is the independent variable that causes change in the dependent variable, i.e. moral distress. Based on this, the following hypothesis might be stated regarding the role of ethical climate in situations of moral distress and ethical problems: If the ethical climate is perceived as positive, nurses have experiences of ethical problems having been handled well in the past. When encountering an ethical problem they may draw on these previous experiences and feel that there is acting space and that possible actions can be taken to deal with the ethical problem. In these cases, the ethical problem is more seldom experienced as moral distress than as an ethical problem (cf. Figure 1). The nurses described several actions they took when handling ethical problems, some of which were explicitly stated to promote a positive ethical climate. These included supporting each other in the working group (IV), using policies and routines as help (IV), the giving of care based on the needs of patients and next of kin (IV) and daring to speak out, thus contributing to setting a standard for behavior (IV). A satisfaction of the need for explanations and information (IV) and working as a team (IV) also promoted a positive ethical climate. Previous research regarding what actions promote a positive ethical climate is scant. The present findings do, however, partly parallel those reported by Rodney et al. (2002) as facilitating a navigation towards the moral horizon. Supportive colleagues and the use of professional guidelines were mentioned as some of the facilitating currents (Rodney et al., 2002). A positive collaboration with physicians, described by Goethals et al. (2010) as facilitating the implementation of ethical decisions, is also reflected in the present findings. The present findings, however, deepen the existing knowledge and contribute new knowledge about what is considered to promote a positive ethical climate. Several of the actions considered to promote a positive ethical climate were those that in their essence strived to bridge the gap between employees from the same as well as different professions. Being provided with explanations and information (IV) could mean that there was no reason to question decisions (II) because there was an understanding of the grounds on which the decision has

48
been made, or this might be the starting point for a dialogue on the possibility to make a different decision. Interprofessional teamwork (IV) meant that different professions were seen as complimentary rather than competing. This reasoning does not imply that trying to bring different professionals closer to each other means that ethical problems and moral distress will no longer occur, but they may occur more seldom, as indicated by the results in Paper III. Supporting each other in the working group and daring to speak out (IV) may also be considered to more firmly establish a common ground for a working group when it comes to taking actions to handle ethical problems and thus improve the ethical climate. In order to strengthen healthcare staff’s ability to handle ethically difficult situations, the ethics rounds method has been used. This method takes its starting point in staff’s experiences of a troubling patient case, which is then discussed in the working group under the leadership of an ethicist (Kälvemark Sporrong, 2007). When the effects of ethics rounds and closely related methods have been evaluated, no expected changes have been shown with regard to decreased moral distress (Kälvemark Sporrong et al., 2007), increased job satisfaction, decreased burnout (Forsgärde, Westman & Nygren, 2000) or stimulated ethical reflection (Svantesson et al., 2008a). However, ethics rounds have been shown to increase mutual understanding (Molewijk, Verkerk, Milius & Widdershoven, 2008; Svantesson et al., 2008b) and decrease professional hierarchies (Svantesson et al., 2008b). Since lack of communication and cooperation (I, II) between mainly nurses and physicians were cited as factors contributing to ethical problems, ethics rounds may be one way to improve these aspects and perhaps also the ethical climate. However, less formal ways of discussing and dealing with situations experienced as ethically problematic were also desired (I); it might be a task for both staff and managers to encourage these discussions on a daily basis. Besides the above-mentioned actions that were considered to promote a positive ethical climate, other actions taken to handle ethical problems were described. These included using support in private life (I), doing all that could be done and thereafter accepting the situation (I), passing on information among those concerned (II) and carrying out decisions that had been made (II). The nurses were not asked whether they considered that these actions promoted or
49
constrained a positive ethical climate. It might be easy to view the actions as more passive than those previously mentioned, and therefore as less effective in handling the ethical problem. The implication should therefore be that they did not promote a positive ethical climate. However, as Lazarus and Folkman (1984) point out, no action or strategy taken in order to handle a situation can be labeled as inherently good or bad since it must be seen in relation to the context (Lazarus & Folkman, 1984). These actions may therefore have been appropriate and effective in the situations in which they were taken. It is worth noting, however, that none of them were described in Paper IV as actions that promoted a positive ethical climate.
Methodological considerations
This thesis collected data on what nurses found to be ethically problematic and morally distressing in their work, the factors contributing to the rise of ethically problematic situations, and actions reported taken in order to handle them, thus creating an ethical climate. In Papers I and IV, participants were given the preferential right to define what they regarded as ethical problems. This decision was made because there seems to be debate regarding what counts as ethical problems. A large number of the experiences concerning ethical problems and moral distress concerned situations of decision making concerning life-sustaining treatment. This may partly be attributed to the aims of the original papers and the methods of data collection. In Paper II the aim was to collect perceptions of decision making regarding life-sustaining treatment, and in the MDS used in Paper III a considerable number of the items describe situations involving life-sustaining actions. Therefore Papers II and III already from the beginning had, to varying degrees, a focus on life-sustaining treatment issues, which should be considered when discussing the results. However, decision making concerning life-sustaining treatment has previously been reported as commonly involving ethical problems (Førde & Vandvik, 2005); therefore, the results in this thesis are likely not only a result of the aims of the original papers and methods of data collection.

50
Participants
The selection of participants in the different papers can be discussed from different points of view. In Papers I and III the inclusion criterion was that the nurses worked during the day. In Paper III this was based on the judgment that the items in the MDS largely described situations and procedures that occurred during the day. As a great majority of the nurses on the selected wards had working schedules that included all kinds of shifts, few were excluded as a consequence of this criterion. In Paper I it might have been of value to have also included nurses working night shifts, as these nurses work partly under different conditions than nurses working day shifts. In Paper IV one of the inclusion criteria was that the nurses had completed the HECS in Paper III. This was motivated by the fact that they therefore had some previous knowledge of ethical climate and thus had the potential of being information-rich cases (Patton, 2002). Here, information-rich cases would be those with experience of significant situations involving an ethical issue that were handled in a good way, i.e. those with experiences of positive ethical climate. Due to ethical considerations it was not possible to contact potential participants with high scores, i.e. positive perceptions of ethical climate. The best way to get into contact with potential participants was therefore judged to be with the help of the nurse manager at the respective ward, who was considered to be able to give advice about nurses who had the ability to provide rich descriptions of the phenomenon under study. To decide on the sample size for Paper III, a power analysis was conducted based on the results of previous studies. However, since a power analysis requires interval data and the data in Paper III were treated as ordinal data, the power analysis served as a guide in the decision on sample size.
Data collection
In the translation of instruments there are different steps that need to be taken in order to achieve equivalence between the original instrument and the translated one. Regarding conceptual equivalence (Streiner & Norman, 2008), before the instruments in Paper III were translated they were discussed by the
51
first author and a senior researcher, both nurses, who determined that it would be possible to use translated versions of the instruments in a Swedish context. The instruments were then translated by three independent translators, who translated into their native tongues, which is in line with the recommendations by Streiner and Norman (2008). However, no back-translations were done, which is recommended (Streiner & Norman, 2008). There were two reasons for this. First, it proved difficult to find another team of translators with the necessary skills to perform the back-translations. Secondly, since the translation of the MDS required adaptations due to its being used in a new cultural context, it was determined that this made back-translation difficult. All the adaptations were discussed with the creator of the instrument in order to ensure that the translations captured the intended meanings. At the time when Paper III was planned and initiated, the MDS was considered the most widely used and well-founded instrument available for measuring moral distress. However, the results of Paper III indicate that the MDS has several shortcomings that should be seriously considered when deciding on which instrument to use. In recent years a new instrument (Eizenberg, Desivilya & Hirschfeld, 2009) that overcomes some of these shortcomings has been developed, which might offer an alternative to the MDS.
Data analysis
In Papers I and II the first author, who was responsible for the analysis of the data, did not formulate the interview questions or perform the interviews. This can be discussed from several points of view. It can be regarded as a weakness that the researcher has not been involved in the whole research process. The interview situation is sometimes regarded as the starting point of the analysis, and this in turn affects what follow-up questions are asked. On the other hand, it might be a benefit that the actual analysis phase is not influenced by preconceptions from the interview situations. The researchers who conducted the interviews scrutinized and discussed the analyses, and could therefore add any knowledge from the interview situations that would benefit the analyses. All the interviews in Papers I, II and IV have been transcribed by the same secretary, who has a great deal of transcription experience. The benefits of the

52
researcher transcribing the interviews are sometimes discussed, such as learning about one’s own interview style and starting the analysis process already in the transcription phase (Kvale & Brinkmann, 2009). All the interviews were transcribed verbatim but did not include overlaps, pauses or intonations of speech, since the focus of the analyses was not on linguistic style or social interaction in interviews. The first author, performing all the analyses, listened to the interviews for Papers I and IV and compared the recordings with the transcriptions, thereby minimizing the risk of material being lost or misinterpreted. This could also be regarded as the beginning of the analysis process, equivalent to an analysis process starting during transcription. The method chosen for Paper IV was CIT, which involves steps for both collecting and analyzing data, with a focus on providing solutions to practical problems (Flanagan, 1954). As this method aims at “pinpointing facts and reducing personal opinions, judgments and generalizations” (Kemppainen, 2000, p.1265), it could be regarded as involving a lesser degree of interpretations of data than some other qualitative methods. Although the interview questions are formulated to meet this aim, it is possible that the interviews generate data whose full potential in the form of depth is not taken advantage of due to the method of analysis.
Trustworthiness
In order to increase the dependability and confirmability of qualitative studies, different kinds of auditing are suggested (Lincoln & Guba, 1985). In the present studies no such processes have taken place, but the co-authors have scrutinized the analyses and been active during the whole research process. The papers have also been discussed at research seminars, where other researchers have critically read and commented on them. The use of outside experts to increase the trustworthiness of qualitative studies, as suggested by Lincoln and Guba (1985), has been criticized as these experts do not have the same knowledge about the data as the principle investigator(s) do (Sandelowski, 1998). However, in Paper IV an expert on the method of CIT served as an advisor both in the formulation of interview questions and in the initial phase of the analysis.
53
Conclusions and implications
The results of this thesis show that nurses experience ethical problems and moral distress in a number of situations, the core of them being the inability to provide good care, which has been stated to be the goal of nursing. Factors associated with the professional role of being a nurse seem to be of significance in understanding why problematic situations turn into ethical problems. This thesis has contributed knowledge about the importance of perceiving the ethical climate as positive when it comes to moral distress. It has also deepened the understanding of what actions can contribute to a perceived positive ethical climate. Several of these were actions that in their essence strived to bridge the gap between employees from the same as well as different professions. Future research should study the ways working conditions, such as lack of resources and workplace stress, may affect the perceived ethical climate. It would also be of interest to investigate whether there are similarities or differences in how different professional groups at the same workplace perceive the ethical climate, as well as how perceptions of ethical climate at a workplace can be improved.

54
Svensk sammanfattning
Att möta etiska problem och moralisk stress som sjuksköterska – Upplevelser, bidragande faktorer och hanterande
Målet med omvårdnad har beskrivits vara att arbeta för patienters bästa. Omvårdnad kan därför ses som en etisk verksamhet. När sjuksköterskor ska förverkliga detta mål har de dock att ta hänsyn till en rad olika etiska värden: den egna professionens värden, patienters värden, värden som lyfts fram av den organisation som sjuksköterskan arbetar i samt samhälleliga värden som uttrycks i bl.a. lagstiftning. Tidigare forskning har visat att sjuksköterskor upplever etiska problem i samband med beslutsfattande om livsuppehållande behandling, i situationer när problematiken gällde vad som var i patientens bästa samt relaterat till informationsgivning och informerat samtycke. Alla situationer som upplevs som etiskt svåra behöver dock inte ha karaktären av ett etiskt problem, där det kan vara svårt att veta vilken den rätta handlingen är men där det ändå finns handlingsutrymme. Om detta handlingsutrymme saknas kan situationen istället upplevas som moraliskt stressande. Sådan stress har bl.a. visat sig förekomma när brist på personal tvingar fram prioriteringar mellan uppgifter som upplevs som lika viktiga och när det inte finns tillräckligt med personal för att kunna ge en god vård. Trots att moralisk stress per definition innebär stress som är ett resultat av att en person vet hur han/hon önskar handla men inte kan göra så p.g.a. organisatoriska hinder finns det begränsat med forskning om hur moralisk stress förhåller sig till organisationsvariabler. En sådan organisationsvariabel är etiskt klimat som innebär uppfattningar om hur etiska problem hanteras på en arbetsplats. Syftet med denna avhandling är att beskriva och utforska vad sjuksköterskor tycker är etiskt problematiskt och moraliskt stressande i sitt arbete, vilka faktorer som bidrar till uppkomsten av etiskt problematiska situationer samt vilka handlingar som uppges vidtas för att hantera dessa situationer, genom vilka ett etiskt klimat skapas.
55
För att besvara syftet genomfördes intervjuer med 54 sjuksköterskor och 249 sjuksköterskor besvarade enkäter. De arbetade på någon av 21 akutvårdsavdelningar på fyra svenska sjukhus. Intervjuerna analyserades med hjälp av innehållsanalys respektive critical incident-metoden, medan enkäterna analyserades med deskriptiva och icke-parametriska statistiska metoder. Resultaten visade att beslutsfattande om livsuppehållande behandling kunde uppfattas som etiskt problematiskt och moraliskt stressande. Det gällde främst när det inte fattades något beslut, när aktiv behandling avslutades utan information eller förklaringar samt när sjuksköterskan inte ansåg att rätt beslut hade fattats. Svårigheter i att bibehålla patientens integritet eller i att kunna ge nödvändig vård kunde uppfattas som etiskt problematiskt och moraliskt stressande. Moralisk stress upplevdes också när sjusköterskan själv eller arbetskamrater inte hade den nödvändiga kompetensen och när nivån på sjuksköterskebemanningen var för låg. Det fanns flera faktorer som bidrog till uppkomsten av etiskt problematiska situationer. Bristande kommunikation med annan personal, främst läkare, läkares sätt att hantera potentiellt etiskt problematiska situationer och patienters bristande hälsa, vilken hindrade deras deltagande i beslut som rörde dem själva, var några av de främsta, men även institutionella hinder kunde bidra. Några av de handlingar som sjuksköterskorna uppgav att de vidtog för att hantera situationer som upplevdes som etiskt problematiska och moraliskt stressade var att göra sitt bästa och därefter försöka att acceptera situationen, vidarebefordra information mellan berörda parter, utföra det beslut som fattats samt att söka stöd bland familj och vänner. Att uppfatta att de etiska problemen på arbetsplatsen hanterades på ett bra sätt, d.v.s. att uppfatta det etiska klimatet som positivt, visade sig ha samband med lägre frekvens av moralisk stress. Ett närmare studerande av de handlingar som resulterade i att det etiska klimatet uppfattades som positivt visade att dessa bl.a. var att arbeta som ett team, att använda policies och rutiner som hjälp vid beslutsfattande och att ge vård utifrån patienters och anhörigas behov. Men också att kunna få stöd av arbetskamrater, att våga säga ifrån för att visa vad som var acceptabelt beteende och att få behov av information och förklaringar tillfredsställda var viktigt för att det etiska klimatet skulle uppfattas som positivt.

56
Sammanfattningsvis kan det konstateras att sjuksköterskor erfar etiska problem och moralisk stress i en rad situationer vilka förenas av att sjuksköterskorna i dem upplever en oförmåga i att ge god vård och därmed också uppfylla vad som uppgetts som målet med omvårdnad. Faktorer som bidrog till uppkomsten av etiska problem tycks förenas av att de har med den professionella rollen som sjuksköterska att göra. Denna avhandling har bidragit med kunskap om betydelsen av ett uppfattat positivt etiskt klimat när det gäller moralisk stress. Den har också fördjupat förståelsen för vilka handlingar som kan bidra till ett uppfattat positivt etiskt klimat. I vidare forskning bör det studeras på vilket sätt arbetsförhållanden såsom brist på resurser och arbetsrelaterad stress kan påverka det uppfattade etiska klimatet. Det är också av intresse att undersöka om det finns likheter eller skillnader i hur olika professionella grupper på samma arbetsplatser uppfattar det etiska klimatet, liksom vilka insatser som kan förändra uppfattningar om etiskt klimat på arbetsplatsen i en positiv riktning.

57
References
Baltes, B. B. (2001). Psychological climate in the work setting. In N. J. Smelser & P. B. Baltes (Eds.), International encyclopedia of the social & behavioral sciences, 18 (pp. 12355-12359). New York: Elsevier/Pergamon.
Bishop, A.H., & Scudder, J. J. (1990). The practical, moral and personal sense of nursing: a phenomenological philosophy of practice. Albany: State University of New York Press.
Brazil, K., Kassalainen, S., Ploeg, J., & Marshall, D. (2010). Moral distress experienced by health care professionals who provide home-based palliative care. Social Science and Medicine, 71(9), 1687-1691.
Breen, C. M., Abernethy, A. P., Abbott, K. H., & Tulsky, J. A. (2001). Conflict associated with decisions to limit life-sustaining treatment in intensive care units. Journal of General Internal Medicine, 16(5), 283-289.
Brink, P. J., & Wood, M. J. (1998). Advanced design in nursing research (2nd ed.). London: SAGE Publications.
Bunch, E. H. (2001). Hidden and emerging drama in a Norwegian critical care unit: ethical dilemmas in the context of ambiguity. Nursing Ethics, 8(1), 57-67.
Chambliss, D. F. (1996). Beyond caring: hospitals, nurses, and the social organization of ethics. Chicago: The University of Chicago Press.
Çobanoglu, N., & Algier, L. (2004). A qualitative analysis of ethical problems experienced by physicians and nurses in intensive care units in Turkey. Nursing Ethics, 11(5), 444-458.
Corley, M. C., Elswick, R. K., Gorman, M., & Clor, T. (2001). Development and evaluation of a moral distress scale. Journal of Advanced Nursing, 33(2), 250-256.
Corley, M. C., Minick, P., Elswick, R. K., & Jacobs, M. (2005). Nurse moral distress and ethical work environment. Nursing Ethics, 12(4), 381-390.
Council for International Organizations of Medical Sciences (CIOMS) (2002). International ethical guidelines for biomedicial research involving human subjects. Available at: http://www.cioms.ch/publications/layout_guide2002.pdf (accessed 16 August 2011)

58
Cronqvist, A., Theorell, T., Burns, T., & Lützén, K. (2004). Caring about - caring for: moral obligations and work responsibilities in intensive care nursing. Nursing Ethics, 11(1), 63-76.
Dahlqvist, V. (2008). Samvete i vården: att möta det moraliska ansvarets röster (Conscience in care: facing the voices of moral responsibility). Avhandling. Umeå universitet, Umeå.
Dahlqvist, V., Eriksson, S., Glasberg, A.-L., Lindahl, E., Lützén, K., Strandberg, G., et al. (2007). Development of the perceptions of conscience questionnaire. Nursing Ethics, 14(2), 181-193.
Dahlqvist, V., Söderberg, A., & Norberg, A. (2009). Facing inadequacy and being good enough: psychiatric care providers' narratives about experiencing and coping with troubled conscience. Journal of Psychiatric and Mental Health Nursing, 16(3), 242-247.
Deady, R., & McCarthy, J. (2010). A study of the situations, features, and coping mechanisms experienced by Irish psychiatric nurses experiencing moral distress. Perspectives in Psychiatric Care, 46(3), 209-220.
Downe-Wamboldt, B. (1992). Content analysis: method, applications, and issues. Health Care for Women International, 13(3), 313-321.
Eizenberg, M. M., Desivilya, H. S., & Hirschfeld, M. J. (2009). Moral distress questionnaire for clinical nurses: instrument development. Journal of Advanced Nursing, 65(4), 885-892.
Eliasson, A. H., Howard, R. S., Torrington, K. G., Dillard, T. A., & Phillips, Y. Y. (1997). Do-not-resuscitate decisions in the medical ICU: comparing physician and nurse opinions. Chest, 111(4), 1106-1111.
Enes, S. P. D., & de Vries, K. (2004). A survey of ethical issues experienced by nurses caring for terminally ill elderly people. Nursing Ethics, 11(2), 150-164.
Ferrand, E., Lemaire, F., Regnier, B., Kuteifan, K., Badet, M., Asfar, P., et al. (2003). Discrepancies between perceptions by physicians and nursing staff of intensive care unit end-of-life decisions. American Journal of Respiratory and Critical Care Medicine, 167(10), 1310-1315.
Filipova, A. A. (2009). Licensed nurses' perceptions of ethical climates in skilled nursing facilities. Nursing Ethics, 16(5), 574-588.
Flanagan, J. C. (1954). The critical incident technique. Psychological Bulletin, 51(4), 327-358.
Forsgärde, M., Westman, B., & Nygren, L. (2000). Ethical discussion groups as an intervention to improve the climate in interprofessional work with

59
the elderly and disabled. Journal of Interprofessional Care, 14(4), 351-361.
Førde, R., & Aasland, O. G. (2008). Moral distress among Norwegian doctors. Journal of Medical Ethics, 34(7), 521-525.
Førde, R., & Vandvik, I. H. (2005). Clinical ethics, information, and communication: review of 31 cases from a clinical ethics committee. Journal of Medical Ethics, 31(2), 73-77.
Gastmans, C., Dierckx de Casterle, B., & Schotsmans, P. (1998). Nursing considered as moral practice: a philosophical-ethical interpretation of nursing. Kennedy Institute of Ethics Journal, 8(1), 43-69.
Gaudine, A., LeFort, S. M., Lamb, M., & Thorne, L. (2011). Clinical ethical conflicts of nurses and physicians. Nursing Ethics, 18(1), 9-19.
Glasberg, A.-L. (2007). Stress of conscience and burnout in healthcare: the danger of deadening one's conscience. Dissertation. Umeå University, Umeå.
Glasberg, A.-L., Eriksson, S., Dahlqvist, V., Lindahl, E., Strandberg, G., Söderberg, A., et al. (2006). Development and initial validation of the Stress of Conscience Questionnaire. Nursing Ethics, 13(6), 633-648.
Goethals, S., Gastmans, C., & de Casterlé, B. D. (2010). Nurses' ethical reasoning and behaviour: a literature review. International Journal of Nursing Studies, 47(5), 635-650.
Gold, C., Chambers, J., & Dvorak, E. M. (1995). Ethical dilemmas in the lived experience of nursing practice. Nursing Ethics, 2(2), 131-142.
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105-112.
Hamric, A. B., & Blackhall, L. J. (2007). Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Critical Care Medicine, 35(2), 422-429.
Hanna, D. R. (2004). Moral distress: the state of the science. Research and Theory for Nursing Practice: An International Journal, 18(1), 73-93.
Harrowing, J. N., & Mill, J. (2010). Moral distress among Ugandan nurses providing HIV care: a critical ethnography. International Journal of Nursing Studies, 47(6), 723-731.
Hermsen, M., & van der Donk, M. (2009). Nurses' moral problems in dialysis. Nursing Ethics, 16(2), 184-191.
International Council of Nurses (ICN) (1953). Code of Ethics. James, L. R., Choi, C. C., Ko, C.-H. E., McNeil, P. K., Minton, M. K.,
Wright, M. A., et al. (2008). Organizational and psychological climate:
60
a review of theory and research. European Journal of Work and Orgnizational Psychology, 17(1), 5-32.
Jameton, A. (1984). Nursing practice: the ethical issues. Englewood Cliffs, NJ: Prentice-Hall.
Jameton, A. (1993). Dilemmas of moral distress: moral responsibility and nursing practice. AWHONN's Clinical Issues in Perinatal Women's Health Nursing, 4(4), 542-551.
Juthberg, C. (2008). Samvetsstress hos vårdpersonal i den kommunala äldreomsorgens särskilda boenden (Stress of conscience among care-providers in municipal residential care of older people). Avhandling. Umeå universitet, Umeå.
Juthberg, C., Eriksson, S., Norberg, A., & Sundin, K. (2008). Stress of conscience and perceptions of conscience in relation to burnout among care-providers in older people. Journal of Clinical Nursing, 17(14), 1897-1906.
Karlsson, M., Roxberg, Å., da Silva, A. B., & Berggren, I. (2010). Community nurses' experiences of ethical dilemmas in palliative care: a Swedish study. International Journal of Palliative Nursing, 16(5), 224-231.
Kelly, B. (1998). Preserving moral integrity: a follow-up study with new graduate nurses. Journal of Advanced Nursing, 28(5), 1134-1145.
Kemppainen, J. K. (2000). The critical incident technique and nursing care quality research. Journal of Advanced Nursing, 32(5), 1264-1271.
Killen, A. R. (2002). Stories from the operating room: moral dilemmas for nurses. Nursing Ethics, 9(4), 405-415.
Krippendorff, K. (2004). Content analysis: an introduction to its methodology (2nd ed.). Thousand Oaks, CA: Sage.
Kvale, S., & Brinkmann, S. (2009). InterViews: learning the craft of qualitative research interviewing. Los Angeles: Sage Publications.
Kälvemark Sporrong, S. (2007). Ethical competence and moral distress in the health care sector: a prospective evaluation of ethics rounds. Dissertation. Uppsala University, Uppsala.
Kälvemark Sporrong, S., Arnetz, B., Hansson, M. G., Westerholm, P., & Höglund, A. T. (2007). Developing ethical competence in health care organizations. Nursing Ethics, 14(6), 825-837.
Kälvemark, S., Höglund, A. T., Hansson, M. G., Westerholm, P., & Arnetz, B. (2004). Living with conflicts-ethical dilemmas and moral distress in the health care system. Social Science and Medicine, 58(6), 1075-1084.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer Publishing Company.
61
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Newbury Park, CA.: Sage Publications.
Lützén, K. (1993). Moral sensitivity: a study of subjective aspects of the process of moral decision making in psychiatric nursing. Dissertation. Karolinska Institutet, Stockholm.
Lützén, K., Blom, T., Ewalds-Kvist, B., & Winch, S. (2010). Moral stress, moral climate and moral sensitivity among psychiatric professionals. Nursing Ethics, 17(2), 213-224.
Lützén, K., Cronqvist, A., Magnusson, A., & Andersson, L. (2003). Moral stress: synthesis of a concept. Nursing Ethics, 10(3), 312-322.
Lützén, K., Dahlqvist, V., Eriksson, S., & Norberg, A. (2006). Developing the concept of moral sensitivity in health care practice. Nursing Ethics, 13(2), 187-196.
Mayer, D. M., Kuenzi, M., & Greenbaum, R. L. (2009). Making ethical climate a mainstream management topic: a review, critique, and prescription for the empirical research on ethical climate. In D. De Cremer (Ed.), Psychological perspectives on ethical behavior and decision making (pp. 181-213). Charlotte, NC: Information Age Publishing.
McCarthy, J., & Deady, R. (2008). Moral distress reconsidered. Nursing Ethics, 15(2), 254-262.
Meltzer, L. S., & Huckabay, L. M. (2004). Critical care nurses' perceptions of futile care and its effect on burnout. American Journal of Critical Care, 13(3), 202-208.
Ministry of Eduation and Cultural Affairs (2003:460). The act concerning the ethical review of research involving humans.
Ministry of Health and Social Affairs (1982:763). The health and medical service act.
Mobley, M. J., Rady, M. Y., Verheijde, J. L., Patel, B., & Larson, J. S. (2007). The relationship between moral distress and perception of futile care in the critical care unit. Intensive and Critical Care Nursing, 23(5), 256-263.
Molewijk, B., Verkerk, M., Milius, H., & Widdershoven, G. (2008). Implementing moral case deliberation in a psychiatric hospital: process and outcome. Medicine, Health Care, and Philosophy, 11(1), 43-56.
National Board of Health and Welfare. Socialstyrelsens föreskrifter och allmänna råd om livsuppehållande behandling (Mandatory rules and general advice on life-sustaining treatment from the National Board of Health and Welfare). SOSFS 2011:7.
62
Nightingale, F. (2010). Notes on nursing: what it is, and what it is not. In V. Skretkowicz (Ed.), Florence Nightingale's Notes on nursing: what it is and what it is not & Notes on nursing for the labouring class (pp. 45-284). New York: Springer.
Oberle, K., & Hughes, D. (2001). Doctors' and nurses' perceptions of ethical problems in end-of-life decisions. Journal of Advanced Nursing, 33(6), 707-715.
Oberle, K., & Tenove, S. (2000). Ethical issues in public health nursing. Nursing Ethics, 7(5), 425-438.
Olson, L. (1995). Ethical climate in health care organizations. International Nursing Review, 42(3), 85-95.
Olson, L. L. (1998). Hospital nurses' perceptions of the ethical climate of their work setting. Image: The Journal of Nursing Scholarship, 30(4), 345-349.
Patton, M. Q. (2002). Qualitative research & evaluation methods (3rd ed.). Thousand Oaks, CA: Sage.
Pauly, B., Varcoe, C., Storch, J., & Newton, L. (2009). Registered nurses' perceptions of moral distress and ethical climate. Nursing Ethics, 16(5), 561-573.
Polit, D. F., & Beck, C. T. (2011). Nursing research: generating and assessing evidence for nursing practice (9th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Reckling, J. B. (1997). Who plays what role in decisions about withholding and withdrawing life-sustaining treatment? Journal of Clinical Ethics, 8(1), 39-45.
Repenshek, M. (2009). Moral distress: Inability to act or discomfort with moral subjectivity? Nursing Ethics, 16(6), 734-742.
Rodney, P., Varcoe, C., Storch, J. L., McPherson, G., Mahoney, K., Brown, H., et al. (2002). Navigating towards a moral horizon: a multisite qualitative study of ethical practice in nursing. Canadian Journal of Nursing Research, 34(3), 75-102.
Sandelowski, M. (1998). The call to experts in qualitative research. Research in Nursing and Health, 21(5), 467-471.
Sandelowski, M. (2000). Whatever happened to qualitative description? Research in Nursing and Health, 23(4), 334-340.
Sandman, L., & Nordmark, A. (2006). Ethical conflicts in prehospital emergency care. Nursing Ethics, 13(6), 592-607.
Schneider, B., Ehrhart, M. G., & Macey, W. H. (2011). Perspectives on organizational climate and culture. In S. Zedeck (Ed.), APA handbook

63
of industrial and organizational psychology. Volume 1: building and developing the organization (pp. 373-414). Washington, DC: American Psychological Association.
Shapira-Lishchinsky, O. (2009). Ethical dilemmas: the experiences of Israeli nurses. Qualitative Health Research, 19(11), 1602-1611.
Streiner, D. L., & Norman, G. R. (2008). Health measurement scales: a practical guide to their development and use. (4th ed.). Oxford: Oxford University Press.
Svantesson, M., Anderzén-Carlsson, A., Thorsén, H., Kallenberg, K., & Ahlström, G. (2008a). Interprofessional ethics rounds concerning dialysis patients: staff's ethical reflections before and after rounds. Journal of Medical Ethics, 34(5), 407-413.
Svantesson, M., Löfmark, R., Thorsén, H., Kallenberg, K., & Ahlström, G. (2008b). Learning a way through ethical problems: Swedish nurses' and doctors' experiences from one model of ethics rounds. Journal of Medical Ethics, 34(5), 399-406.
Svantesson, M., Sjökvist, P., & Thorsén, H. (2003). End-of-life decisions in Swedish ICUs. How do physicians from the admitting department reason? Intensive & Critical Care Nursing, 19(4), 241-251.
Svantesson, M., Sjökvist, P., Thorsén, H., & Ahlström, G. (2006). Nurses' and physicians' opinions on aggressiveness of treatment for general ward patients. Nursing Ethics, 13(2), 147-162.
Svensson, E. (2005). Val och konsekvens: mätnivån avgör den statistiska verktygslåda (Choice and consequence: the measurement level determines the statistical toolbox). Läkartidningen 102(17): 1331-1337.
Thompson, I. E., Melia, K. M., Boyd, K. M., & Hornsburgh, D. (2006). Nursing Ethics (5th ed.). Edinburgh: Churchill Livingstone.
Torjuul, K., & Sörlie, V. (2006). Nursing is different than medicine: ethical difficulties in the process of care in surgical units. Journal of Advanced Nursing, 56(4), 404-413.
Tsai, M.-T., & Huang, C.-C. (2008). The relationship among ethical climate types, facets of job satisfaction, and the three components of organizational commitment: a study of nurses in Taiwan. Journal of Business Ethics, 80, 565-581.
Ulrich, C., O'Donnell, P., Taylor, C., Farrar, A., Danis, M., & Grady, C. (2007). Ethical climate, ethics stress, and the job satisfaction of nurses and social workers in the United States. Social Science and Medicine, 65(8), 1708-1719.

64
Ulrich, C. M., Taylor, C., Soeken, K., O'Donnell, P., Farrar, A., Danis, M., et al. (2010). Everyday ethics: ethical issues and stress in nursing practice. Journal of Advanced Nursing, 66(11), 2510-2519.
Victor, B., & Cullen, J. B. (1988). The organizational bases of ethical work climates. Administrative Science Quarterly, 33, 101-125.
Viney, C. (1996). A phenomenological study of ethical decision-making experiences among senior intensive care nurses and doctors concerning withdrawal of treatment. Nursing in Critical Care, 1(4), 182-187.
Wilkinson, J. M. (1987/1988). Moral distress in nursing practice: experience and effect. Nursing Forum, 23(1), 16-29.
Zuzelo, P. R. (2007). Exploring the moral distress of registered nurses. Nursing Ethics, 14(3), 344-359.
School of Health Sciences Dissertation Series
1. Linddahl, Iréne. (2007). Validity and Reliability of the Instrument DOA; A Dialogue about Working Ability. Licentiate Thesis. School of Health Sciences Dissertation Series No 1. ISBN 978-91-85835-00-3
2. Widäng, Ingrid. (2007). Patients’ Conceptions of Integrity within Health Care Illuminated from a Gender and a Personal Space BoundaryPerspective. Licentiate Thesis. School of Health Sciences Dissertation Series No 2. ISBN 978-91-85835-01-0
3. Ernsth Bravell, Marie. (2007). Care Trajectories in the oldest old. Doctoral Thesis.School of Health Sciences Dissertation Series No 3. ISBN 978-91-85835-02-7
4. Almborg, Ann-Helene. (2008). Perceived Participation in Discharge Planning and Health Related Quality of Life after Stroke. Doctoral Thesis. School of Health Sciences Dissertation Series No 4. ISBN 978-91-85835-03-4
5. Rosengren, Kristina. (2008). En hälso- och sjukvårdsorganisation i förändring – från distanserat till delat ledarskap. Doctoral Thesis.School of Health Sciences Dissertation Series No 5. ISBN 978-91-85835-04-1
6. Wallin, Anne-Marie. (2009). Living with diabetes within the framework of Swedish primary health care: Somalian and professional perspectives. Doctoral Thesis.School of Health Sciences Dissertation Series No 6. ISBN 978-91-85835-05-8
7. Dahl, Anna. (2009). Body Mass Index, Cognitive Ability, and Dementia: Prospective Associations and Methodological Issues in Late Life. Doctoral Thesis. School of Health Sciences Dissertation Series No 7. ISBN 978-91-85835-06-5
8. Einarson, Susanne. (2009). Oral health-related quality of life in an adult population. Licentiate Thesis.School of Health Sciences Dissertation Series No 8. ISBN 978-91-85835-07-2
9. Harnett, Tove. (2010). The Trivial Matters. Everyday power in Swedish elder care. Doctoral Thesis. School of Health Sciences Dissertation Series No 9. ISBN 978-91-85835-08-9
10. Josefsson, Eva. (2010). Immigrant background and orthodontic treatment need - Quantitative and qualitative studies in Swedish adolescents. Doctoral Thesis. School of Health Sciences Dissertation Series No 10. ISBN 978-91-85835-09-6
11. Lindmark, Ulrika. (2010). Oral Health and Sense of Coherence - Health Behaviours, Knowledge, Attitudes and Clinical Status. Doctoral Thesis. School of Health Sciences Dissertation Series No 11. ISBN 978-91-85835-10-2
12. Pihl, Emma. (2010). The Couples’ Experiences of Patients’ Physical Limitation in Daily Life Activities and Effects of Physical Exercise in Primary Care when having Chronic Heart Failure. Doctoral Thesis. School of Health Sciences Dissertation Series No 12. ISBN 978-91-85835-11-9
13. Nilsson, Stefan. (2010). Procedural and postoperative pain management in children - experiences, assessments and possibilities to reduce pain, distress and anxiety. Doctoral Thesis. School of Health Sciences Dissertation Series No 13. ISBN 978-91-85835-12-6
14. Algurén, Beatrix. (2010). Functioning after stroke - An application of the International Classification of Functioning, Disability and Health (ICF). Doctoral Thesis.School of Health Sciences Dissertation Series No 14. ISBN 978-91-85835-13-3
15. Kvarnström, Susanne. (2011). Collaboration in Health and Social Care - Service User Participation and Teamwork in Interprofessional Clinical Microsystems. Doctoral Thesis. School of Health Sciences Dissertation Series No 15. ISBN 978-91-85835-14-0
16. Ljusegren, Gunilla. (2011). Nurses’ competence in pain management in children. Licentiate Thesis. School of Health Sciences Dissertation Series No 16. ISBN 978-91-85835-15-7
17. Arvidsson, Susann. (2011). Health promoting factors in people with chronic musculoskeletal pain or with rheumatic diseases: a descriptive and interventional study. Doctoral Thesis. School of Health Sciences Dissertation Series No 17. ISBN 978-91-85835-16-4
18. Berggren, Elisabeth. (2011) Identity construction and memory after Subarachnoid Haemorrhage - Patients’ accounts and relatives’ and patients’ statements in relation to memory tests. Licentiate Thesis. School of Health Sciences Dissertation Series No 18. ISBN 978-91-85835-17-1
19. Ericsson, Iréne. (2011) Välbefinnande och demens - Aspekter på välbefinnande hos äldre personer med måttlig till svår demenssjukdom. Doctoral Thesis. School of Health Sciences Dissertation Series No 19. ISBN 978-91-85835-18-8
20. Silén, Marit. (2011) Encountering ethical problems and moral distress as a nurse - Experiences, contributing factors and handling. Doctoral Thesis. School of Health Sciences Dissertation Series No 20. ISBN 978-91-85835-19-5