Embed Size (px)
Citation preview

3/21/2012
1
Rita Shugart, RN, RVT, FSVUShugart Consulting
March 21, 2012
1. LCD’s2. Ordering and signature requirements3. CPT and ICD-9 coding 4. Reports5. Risky practices6. Case Studies
Patient populationPrivate insurance applicabilityTransparency
LCD’s -Medicare payer policies that identify circumstances under which services will be (or will not be) considered covered, correctly coded, and possibly reimbursed
•Technical Staff Credentialing•Facility Accreditation•Physician Qualifications•Diagnosis codes considered medically necessary
•Types of exams covered•Types of exams not covered•Frequency of repeat exams•Documentation requirements
LCD’s typically include:
Palmetto GBA NIVT LCD - Parts A and B
Contractor�NamePalmetto GBAopens in new window
Contractor�Number11502
Contractor�TypeMAC ‐ Part B
Back to TopLCD�Information
Document�Information�
LCD�ID�NumberPrimary�Geographic�Jurisdiction��opens�in�new�window�
L31712
LCD�TitleNoninvasive Vascular Testing (NIVT)
Contractor's�Determination�NumberL6607
AMA�CPT/ADA�CDT�Copyright�StatementCPT codes, descriptions and other data only are copyright 2011 American MedicalAssociation (or such other date of publication of CPT). All Rights Reserved.Applicable FARS/DFARS Clauses Apply. Current Dental Terminology, (CDT)(including procedure codes, nomenclature, descriptors and other data containedtherein) is copyright by the American Dental Association. © 2002, 2004 AmericanDental Association. All rights reserved. Applicable FARS/DFARS apply.
p
North Carolina
Oversight�RegionRegion IV
Original�Determination�Effective�DateFor services performed on or after 03/19/2011
Original�Determination�Ending�Date
Revision�Effective�DateFor services performed on or after 02/15/2012
Revision�Ending�Date
Vascular studies must be: 1. performed by or under direct supervision of credentialed persons OR2. performed in accredited lab
Examples of appropriate certification/accreditation:ARDMS RVT ARRT(VS)ICAVL ACRICAVL ACR
“All credentialed laboratories extending their noninvasive vascular testing to include additional CPT codes have 12 months to become accredited for the new CPT codes. It is expected that all labs, after receiving accreditation, maintain credentialed personnel on staff to performand supervise these procedures. Laboratory accreditation should be specific to the testing being performed.”

3/21/2012
2
1. Evaluation of patients with hemispheric neurologic symptoms, including stroke, transient ischemic attack, and amaurosis fugax.2. Evaluation of patients with a cervical bruit.3. Evaluation of pulsatile neck masses.4 E l ti f bl t k t4. Evaluation of blunt neck trauma.5. Evaluation of postoperative patients following carotid surgery.6. Evaluation of suspected subclavian steal syndrome.7. Preoperative evaluation in patients scheduled for major cardiovascular surgical procedures.8. Intraoperative monitoring of vascular surgery.
For a patient with stenosis of 81 - 99 %, surgery is commonly performed
If not performed further surveillance is not usually If not performed, further surveillance is not usually necessary, unless symptoms are progressive
1. The evaluation of hemodynamic effects of severe stenosis or occlusion of the extracranial arteries greater than or equal to 60% diameter reduction or major basal intracranial artery stenosis greater than or equal to 50% diameter reduction.2. Detection and serial evaluation of cerebral vasospasm due
b h id h h ( i )to subarachnoid hemorrhage (spontaneous or traumatic).3. Evaluation of cerebral arteriovenous malformations when surgical intervention is an option.4. Intraoperative and perioperative monitoring of intracranial hemodynamics during carotid endarterectomy.5. Evaluation of cerebral embolism.6. Evaluation of hemodynamics in suspected brain death.
Dizziness, not associated with localizing symptomsHeadachesBrain tumorsFamilial and degenerative disease of the central nervous systemP hi t i di dPsychiatric disordersEpilepsyMigraineIntraoperative monitoring during major surgery other than intra or extracranial cerebrovascular surgeryAssessment of physiologic and pharmacologic responses of cerebral arteries
1. For a patient with stenosis of 20 - 49%, annual follow-up may be necessary
2. For a patient with stenosis of 50 - 80%, repeat studies no more than every 6 months
3. For a patient with stenosis of 81 - 99 %, surgery is commonly performed If not performed, further surveillance is not usually necessary, unless symptoms are progressive
Post Endarterectomy Surveillance:6 weeks, 6 months and Annually thereafterAnnually thereafterRecurrent or new neurological events

3/21/2012
3
1. Clinical instability of patients with intracranial hemorrhage or intracranial vascular surgeryvascular surgery
2. Inconclusive study for brain death
Part B, Outpatients Part A, Inpatients
• All states except: • 30 states +jurisdictions: AR CO CT DE FL IL IN
AZ, AK, MT, ND, OR, SD, UT, WA, WY(Noridian)
MA, ME, NH, RI, VT (NHIC)
AR, CO, CT, DE, FL, IL, IN, IA, KS, KY, LA, MD, MI, MS, MO, MN, NC, NE, NJ, NM, NV, NY, OH, OK, PA, SC, TX, VA, WV, WI; DC, PR, VI
• Plus some providers in all states except NY where WPS is the FI
http://www.cms.hhs.gov/mcd/index_lmrp_bystate_criteria.asp?from2=index_lmrp_bystate_criteria.asp&
Before you start, determine your MAC, Carrier, FISelect state nameSelect Part A (inpatient) or Part B (outpatient)( p ) ( p )Accept License AgreementLook in alphabetical list of “Active” Policies for vascular testing (may be under several different letters)Also check “Draft” and “Future Effective Policies”Check frequently for updates, changes
Local – not used in every state Not applied to all providers within some statesFrequent changes due to Medicare contractor reformSmall specialties have little representation on CAC’sPoorly written – incomplete, contradictory, inaccurate, non-sensical, exhibit poor understanding of “real” practiceConstant vigilance required
Carotid Duplex
TCD

3/21/2012
4
• Diagnostic tests must have orders from “Treating Physician/Practitioner”
• ALL orders should include type of exam and diagnosis/indication/reason for testg
• Referring physician must document intent to order and reason for exam in his/her office notes
• Maintain copies of orders in case of audit• Follow regulations for additional/un-ordered
tests
• A physician /practitioner as defined under the SS Act ANDWho treats for a specific medical problem• Who treats for a specific medical problemOR
• Who furnishes a consultation AND
• Who uses the results of the diagnostic test in the management of the specific medical problem
Medicare Benefit Policy Manual , Chapter 15, 80.6
• Provide space for some, but not all, demographics• Have clearly defined space for type of test,
indication• Have space for referring extra info, notes,
instructions• If ICD-9 codes are listed, avoid steering to only
those codes that meet “medical necessity”• Distribute to referring MD’s offices as referral and
marketing tool
• Provider clearly identified• Legible first and last names, credentials
recommended• Can be handwritten or• Electronic
• Digitized• Electronic• Digital
• Not acceptable:• Signature stamps• “Signed but not read”• “Signature on File”

3/21/2012
5
Effective January 1, 2011
Clarification, more specific wording of d fi iti f CPT d 93922 93923 d definitions of CPT codes 93922, 93923, and 93924
Instructions can be found in the Introduction to “Noninvasive Vascular Diagnostic Studies” in the CPT Code Book
CPT definition :LOWER Extremities ONLYTREADMILL stress testing ONLYMOTORIZED treadmillBilateralMust include:
At rest, immediately after, and at timed intervals after standardized protocolTime of onset of sx, max walking time, time to recovery
One deletion: 93875 - cerebrovascular physiologic studies (OPG, periorbital, spectral analysis)
One addition93998 – Unlisted noninvasive vascular diagnostic study
• Read the CPT book• Be sure that:
The coder understands how to code vascularexamsThe exam performed fulfills the requirements of the billed CPT code
• Remember – you may know more about the patient, vascular testing. and vascular diagnoses than the “official” coder
“The use of a simple handheld or other Doppler device that does not produce hard copy output, or that produces a record that does not permit analysis of bidirectional vascular flow, is considered to be part of the physical examination of the vascular system and is not separately reported. “p y p
“Noninvasive physiologic studies are performed using equipment separate and distinct from the duplex scanner.”
“Photoplethysmography is NOT a covered service”
CPT 2012, AMA

3/21/2012
6
“A complete transcranial Doppler (TCD) study (93886) includes ultrasound evaluation of the right and left anterior circulation territories and the posterior circulation territory (to include vertebral arteries and basilar artery).”
“I li it d TCD t d (93888) th i lt d “In a limited TCD study (93888) there is ultrasound evaluation of two or fewer of these territories.”
“To report common carotid intima-media thickness (IMT) study for the evaluation of atherosclerotic burden or coronary heart disease risk factor assessment, use Category III code 0126T.
CPT 2012, AMA
Know the definition of the CPT Code; allcomponents of the procedure as defined by the CPT Code must be included in the exam
If the exam does not meet the definition of the CPT Code, another CPT Code or a modifier must be used
The documentation (Report) must fully support the CPT Code on the claim
Example 1:Billing CPT Code 93924 (Exercise Exam) for TOS exam or LE Exercise exam with “toe-ups” or exam or LE Exercise exam with toe ups or walking in hallway
Example 2:Billing CPT Code 93990 (Duplex Access) for evaluation of access site only
Example 1:Billing CPT Code 93922 (LE Arterial Physiologic Ltd) for someone with an AKA. If l t it i i d i l d If only one extremity is examined, include Modifier -52 to indicate “Reduced Service”or “less than”service
Example 2:Billing CPT Code 93882 (EC Car Dup, limited) for IMT. IMT is billed as Code G0126
Example 1:Billing CPT Code 93930 (UE Arterial Duplex complete) and report reads “antegrade flow in complete) and report reads antegrade flow in vertebral arteries”
Example 2:Billing CPT Code 93886 (TCD complete) and report reads “no evidence of intracranial ICA dissection”

3/21/2012
7
• International Classification of Diseases • Published by WHO• MD’s required to use for MCR reimbursement
since 4-1-89• Purposes:
• Describe medical necessity of a procedure• Facilitate payment of health services• Evaluate utilization patterns• Permit study of appropriateness of health care costs• Serve as basis for epidemiological studies• Serve as basis for research into health care quality
Code the diagnosis, symptoms, conditions or reasons responsible for the service being providedCode a confirmed or definitive diagnoses documented by the diagnostic testDo not use the initial “referral” indication if it is inaccurateChoose the ICD-9 code that provides the highest degree of accuracy and completenessCan not use “rule out”, “suspected”, “probable”, or “questionable” on outpatients
Know the definition of the ICD-9 Code
The patient’s clinical condition history or the The patient’s clinical condition, history, or the test results must meet the definition of the ICD-9 Code (Diagnosis Code) on the claim
The exam documentation (Report) must fully support the ICD-9 Code on the claim
440.22 Rest Pain440.22 Atherosclerosis with Rest pain
440.30 Atherosclerosis of BPG of extremities, unspecified graft
440.31 Atherosclerosis of autologous vein bypass graft440.32 Atherosclerosis of synthetic graft
Example 1:Pt has Family history, but no personal history, of AAAAAA
Billing with ICD-9 Code 441.4, Aneurysm Abdominal Aorta, not ruptured and report reads “ no evidence of AAA”
Example 1:Billing with ICD-9 Code 440.21 atherosclerosis with intermittent claudication, and report pdescribes “burning, stinging in toes and feet”
Example 2:Billing with ICD-9 Code 435.9, TIA and report shows indication as “headache”

3/21/2012
8
It Depends ……Which examsReasons for exams (indications)DocumentationHow claim is filed
NCCIMUE’sUse of modifier
• Which exams• Must not be “bundled” codes
• Reasons for exams• Both exams must be medically necessary • Both exams must be medically necessary
• Documentation• Both exams must meet LCD requirements• Both exams must meet definition of billed CPT codes• Separate ICD-9 codes not required, but good to use, if
appropriate• Report each exam separately to reflect the separate
amount of work associated with each exam
Modifier Not Allowed (cannot be billed together):
93880 - 93882
93888 - 93886
REPORTS
Review your Report Forms!Be sure that:• Final Reports are complete, easy to understand • CMS Ordering and Signature requirements are
fulfilled• Records are maintained as required by LCD,
state law, other policiesReport should “stand alone” (all necessary documentation included)
Report should include space for required components of CPT code(i.e. 93886 include space for all relevant intracranial arteries)
D ’ L b ifi f RDon’t use Lab-specific names for ReportsDon’t combine documentation for two or more
CPT codes on one Report form(i.e. Extracranial Carotid Duplex + TCD + IMT combined on one “Comprehensive Cerebrovascular Evaluation” Report)

3/21/2012
9
“Medical Necessity” is established through Indications & Impression sections of the Report
Indications: Use narrative/words, not only numerical ICD-9 codeBe specific to that patient for that exam on that dayInclude relevant associated medical historyInclude relevant associated medical history
Impression:• Distinguish between ultrasound “findings” and
Impressions/Conclusions (example: velocities and plaque morphology vs. % stenosis)
• Be as specific as possible, especially if results may change the ICD-9 coding on the claim (to make the ICD-9 more specific)Include important negative conclusions as well as positive conclusions

3/21/2012
10
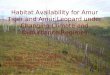
Cerebrovascular�Duplex�Scan�Patient:�� Account�#:��DOB:�� Study�Quality:��Study�Date:�� Room:�Room�3�Referring�Physician:��Ordering�Physician:��CC:����Indications:�Follow�up�of�60�‐�79%�right�ICA�stenosis��with�maximum�velocities�of�273�PSV/67��EDV��on�last�exam�of�X/XX/11.�The�left�ICA�has�known�occlusion.��No�recent�related�symptoms.��������������Results�
Right� � � Left� �PSV�
(cm/s)�EDV�(cm/s)�
Stenosis� Plaque� � PSV�(cm/s)�
EDV�(cm/s)�
Stenosis� Plaque�
140� 18.1� � � Prox�CCA� 115� 13.4� � �112� 28.3� � � Dist�CCA� 101� 17.3� � �341� 67.3� 60‐79%� � Prox�ICA� � � Occluded� �367� 73.3� 60‐79%� � Mid�ICA� � � Occluded� �251� 61 7� 60‐79%� � Dist�ICA� � � Occluded� �251� 61.7� 60 79%� � Dist�ICA� � � Occluded� �316� 33.7� � � ECA� 424� 55� � �132� 32.2� � � Vertebral� 79.2� 5.3� � �
�
�� Patent�Endarterectomy� ���
Antegrade� Vertebral�Flow� Retrograde�
Findings�Right:��Moderate�focal�increase�in�ICA�velocities.�
�Left:��Significant�plaque�and�no�audible�flow�in�the�ICA�.�Conclusions��
1. Moderate�right�ICA�stenosis,�60‐79%.�2. ICA�occlusion�on�the�left.�3. Compared�to�previous�exam,�these�results�remain�essentially�unchanged.�
��Sonographer:���Reading�Physician:���Electronically�signed�on�X/XX/2012�10:47:33�AM.����

3/21/2012
11
• False statement or misrepresentation made or caused to be made that is material to entitlement or payment
• Incorrect reporting of diagnoses or procedures to maximize payments
• Billing for services not furnished Alt i l i f l t i l i d di l • Altering claim forms, electronic claim records, medical documentation, etc., to obtain a higher payment amount.
• Misrepresentations of dates and descriptions of services furnished or the identity of the beneficiary or the individual who furnished the services.
• Billing non-covered or non-chargeable services as covered items.
Poor documentation of medical necessity through vague, inadequate, or incorrect IndicationsAmbiguous or lab-specific exam name –unclear Ambiguous or lab specific exam name unclear if it matches the billed CPT codeExam performed differs from orderDocumentation doesn’t support billed CPT codeDocumentation doesn’t support billed ICD-9 code
Multiple tests on same date of serviceContinuing to bill for services or combinations of services that are usually deniedRoutine use of modifiers to bypass CCI and MUE editsAlways billing complete examsBilling structural and vascular codes from the same body parts together
• Claims review• something that stands out• statistical outlier• random sampling
• Pattern recognition• Claim differences Part A versus Part B• Diagnosis Coding• Qui Tam suits• RAC Target
Signed Order from referring MDReferring MD’s documentation of intent to order and reason for examExam performed by qualified technologist technologist Final Report signed by qualified interpreting physicianFinal Report that documents allcomponents of billed CPT codeFinal Report that supports all billed ICD 9 codes

3/21/2012
12
Scenario: Cardiology office labSurveillance of CEA pts:
Exam performed w/no MD appt; If all is OK, RVT writes down time for
next appt on bottom of encounter form; US appt made, still w/no MD appt
Discovered during consultation
Potential Issues:•No order
•No documentation that MD is fulfilling resp as treating physician (“uses the results of the diagnostic test in the management of the specific medical problem”)
•Potential charge of medical negligence (“If a doctor fails to give a patient the proper tests, performs unneeded procedures, or fails to check progress after a procedure, he is committing medical negligence.” 2012 MedicalMalpracticeHelp.com)
Outcome: Next appointment no longer made at Check OutMD completes Order Form as he/she reads each examMD sends fu letter to patient regarding results of exam and time of next follow up apptPatients scheduled for appt with MD or PA at least every two years
Scenario: IDTF located in state identified by OIG as having “excessive” us utilizationOrder by neurologists for Carotid dup + TCD Indications: dizziness vertebral insufficiencyIndications: dizziness, vertebral insufficiencyBilled as 5 complete exams: Car dup, TCD, Car physiologic, UE Art Dup, UE art physiologic
Found by Medicare contractor audit to be statistical outlier with > 800% higher billing
than comparable provider
Potential Issues:• Multiple studies (5) on same patient, same DOS• Performing unordered exams• No medical necessity for unordered exams• Following internal protocols• All requirements of billed CPT codes not met• Located in high-utilization state

3/21/2012
13
Outcome: One audit becomes multiple auditsMultiple personal and telephone meetings with MACRepayment of $$$ $$$Repayment of $$$,$$$Placed on Pre-Payment AuditLab income decreased by 90%, consultant calledOutcome: Testing Protocols, billing practices changedOff Pre-Payment Audit after 1 yearLab survived
Scenario:Office-based vascular lab, owned by large hospital
Orders for Bilateral UE Vein mapping prior to dialysis access placement
Coded as CPT 93970, Venous Duplex Complete (x 2 years)
Audit performed by Coding Consultant hired as result of complaint from vascular lab staff member
Potential Issues:• Exams were of bilateral cephalic veins only
• All requirements of billed CPT code were not metAll requirements of billed CPT code were not met(bilateral exam, but limited (not complete) exam was performed)
Outcome:Termination of Technical DirectorVoluntary re-payment of $$,$$$ to MedicareThreatened shut-down of facility by ownerComplete audit of all lab coding/billing/exam protocolsSome testing Protocols, billing practices changedContinuing compliance scrutiny of practice by hospital corporate owner No subsequent scrutiny by MAC (? Yet)
Scenario:Order reads “Carotid duplex exam for rule out CVA”
Billed as Carotid duplex exam - CPT 93880/dx CVA + TCD Complete - CPT 93886/dx CVA + Carotid Duplex Limited – CPT 93882/dx CVA
93886 included only intracranial carotid arteries93882 was actually for an IMT examDiscovered incidental to consultation for separate matter
Potential Issues:•Performing unordered exams•No medical necessity for unordered exams•Following internal protocol•All requirements of billed CPT code 93886 not met•Billing IMT exam (Cat III Code) as reimbursable 93882 code•Billing “rule out” diagnoses as true diagnoses on clam

3/21/2012
14
Outcome:
Testing Protocols, billing practices changed