Embed Size (px)
Citation preview

Pediatric and Neonatal Critical Care Neurology
Child Neurology MGH CME CourseOctober 2015
Patricia L Musolino MD, PhDCritical Care and Vascular Neurology
I have no financial disclosures

Critical Care Neurology in Neonates and Children
® Acute insults to the brain can be group into the same categories in Newborns, young children and teenagers
® Presentations and symptoms differs depending the stage of development of the brain and associated co morbidities ® myelination, established vs developing networks, synaptic plasticity,
susceptibility to metabolic disturbances)® A systems-symptoms based diagnostic approach can be used
at all ages® Therapeutic approach differs greatly depending on
® Nature of the Disorders® Age® Duration of symptoms® Degree of systemic diseases associated with neurological injury® Parents/family level of understanding ® Expected degree of neurological sequela

Disease Categories
® Brain Perfusion Disorders® Increase Intracranial Pressure ® Infections: encephalitis, meningitis, abscess ® Metabolic-Genetic Encephalopathies: MELAS, Inborn
Errors of Metabolism® Epilepsy-Status Epilepticus® Malignancies ® Traumatic Brain Injury


Pediatric Neurocritical Care® More children are surviving critical illness
® Overall PICU mortality decreased from 11% to 4.8% between 1982 and 2005
® Increased incidence of moderate to severe disability following ICU admission (8.4% in 1982 to 17.9% in 2005–2006 (p < .001)
® Brain injury is the most common proximate cause of death in the Pediatric ICU (mortality 65.4%)

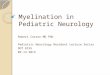
TemporalCascadeofEventsà Post-anoxia

Lo. Nat Rev Neurosci. 2003;4:399
MolecularPathwaysofCellDeath• Excitotoxicity
and ionic imbalance
• Oxidative and nitrosative stress
• Apoptotic mechanisms
• Necrosis

Neuroprotection-SandwichModel
Glutamate
Mitochondria
Proteolysis
Oxidative Stress
ER Stress
Inflammation
Surv
ival
Dea
th
GlutamateMitochondriaProteolysis
Oxidative StressER Stress
Inflammation

Pediatric Code Blue
in the ED

Preventing Secondary Insults changes Outcome
McHugh G, Doortje CE, et al. J Neurotrauma 2007Kokoska et al. (1998), Journal of Pediatric Surgery, 33(2);
Number of Hypotensive Episodes
in the first 24 hours after TBI

Pediatric Neurology Handbook. Lippicontt. 2013
Normal Paremeter by Age: BP, MAP, ICP, CPP

Pediatric Neurology Handbook. Lippicontt. 2013
General Principles: Neuro Assessments

General Principles: Airway and Breathing
® Hypoxemia is a profound insult® Pediatric patients have both:
® Higher CMR O2 extraction (outside of newborn period)® Lower reserve oxygen supply (FRC)
® Indications for intubation® Impending or Acute Respiratory Failure® Inability to protect airway® Decrease work load of CV system
Adapted from Chugani, et al, Ann Neurol 1987

O2: too little is bad ... too much can be worse!
® Oxidative stress injury® Animal models suggest hyperoxia is harmful
® inflammation, neuronal death® Exacerbates neurologic dysfunction in several models® In newborns resuscitated with 21% vs 100% FiO2 meta-
analysis of RCT shows reduced risk of mortality, trend toward reduced risk of severe HIE

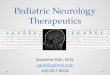
CBF
MAP(mmHg)
Normal 50 - 100 ml / min
Normal 60 - 150 mmHg
Cerebral Blood FlowRegulation of Cerebral Vascular Resistance
PaCo2 (mmHg)
Normal 30 - 50 mmHg
Adapted from: Rogers (1996) Textbook of Pediatric Intensive Care pp. 648 - 651

CBF-Ventilation
CBF pre- hyperventilation CBF post-hyperventilation
Adapted from research by Skippen et al. (1997)

Musts in the Care of Acute Neurological Insult in Children
® Serial neurologic assessments and physical examination
® Continuous cardio-respiratory, ICP, and CPP monitoring, +/- cerebral metabolism monitoring adjuncts
® Continuous EEG monitoring (seizures, ischemia, encephalopahty)
® Optimize Physiology:® Oxygenation and Ventilation® Perfusion® Cerebral metabolic rate® Address metabolic-electrolyte disturbances (see appendix for Hyponatremia)

® Normalize or Reduce Cerebral Metabolic Rate® Monitor for and prevent seizures (see appendix for Status Epilepticus algorithm)
® Reserve pentobarbital for refractory conditions® Avoid hyperthermia, +/- hypothermia® Avoid hyperglycemia (early) or hypoglycemia
Musts in the Care of Acute Neurological Insult in Children

® Avoid Increases in ICP® Prevent airway obstruction ® Treat pain and agitation - consider pre-medication for
nursing activities, +/- neuromuscular blockade (only when needed)
® Careful monitoring of ICP during nursing care, cluster nursing activities and limit handling when possible
® Suction only as needed, limit passes, pre-oxygenate / +/- pre-hyperventilate (PaCo2 not < 30) / use lidocaine IV or IT when possible
® After careful preparation of visitors, allow calm contact® Do not constrain venous return (tight neck collar)
Musts in the Care of Acute Neurological Insult in Children

® Normalize intracranial pressure ® Evacuate mass occupying lesions (tumor, hemorrhages) ® Consider draining CSF with ventriculostomy when
possible to prevent decrease CPP® Hyperosmolar therapy, +/- diuresis (cautious use to
avoid hypovolemia and decreased BP)® Mid-line neck, elevated head of bead (some research
supports elevation not > 30 degrees)
Musts in the Care of Acute Neurological Insult in Children

Management of Increase ICP in Children


Pathophysiology of increase ICP
Rosner, M. J Neurosurg 83:949–962, 1995

Signs and Symptoms of Increase ICP
Early® Headache® Emesis® Altered MS® Decrease GCS® Irritability® Sunsetting® Decrease eye contact® CN Dysfunction® Seizures
Late® Further Decrease in GCS® Bulging fontanel® Decrease Spontaneous
Movements® Posturing® Papilledema® Pupil dilatation® Increase BP, Irregular
Respirations ® Chushig’s triad

Exam and Respiratory Patterns Rostro-caudal Progression in Herniation Syndromes

Management of Increase ICP Algorithm


Pediatric Neurology Handbook. Lippicontt. 2013

Metabolic Emergencies
® Although individually rare, altogether they are 1:800-5000 incidence.
® Broadly Defined: An inherent deficiency in a key metabolic pathway resulting in® Cellular Intoxication® Energy deprivation® Combination of the two

Suspect IEM when
® Rapid deterioration in an otherwise well infant® Septic appearing infant ® History of Failure to thrive® Regression in milestones® Recurrent emesis or feeding difficulty, alterations
in respirations, abnl urine/body smell, changing MS/lethargy, jaundice, sz, intractable hiccups.
® Can masquerade like pyloric stenosis.® Dietary aversion-proteins, carbs.

Emergency Management:® ABC’s® Laboratory Investigation: ABG-acidosis, NH4, Lactate,
Pyruvate® NPO, reverse catabolism with D5-D10 1-1.5 x maint.® Correct hypoglycemia® Correct metabolic acidosis® Dialysis, lactulose if High/toxic NH4 (>100µmol/L)® Search for and treat precipitants; ie: Infection, dehydration ® Low threshold for Sepsis w/u + ABx if uncertain ® Pyridoxine for neonatal sz. if AED no-response® Ativan, Versed, Pentobarb coma, AEDs for status
epilepticus.® Carnitine for elimination of Organic Acid through creation
of carnitine esters® Sodium Benzoate, Phenylacetate for Hyper NH4

Without Focal Neurological Sx
With Neurological Sx
Cerebral Edema Extrapyramidal signsHemiplegiaHemianopia
MSUD, OTC MSUD, OTC, MMA, PA, PGK
MMA, GA I, Wilson dz,
Homocystinuria
Stroke-like episodes
UCD, MMA, RCD (MELAS), Fabry dz, PA, IVA, HMG-coA,
Homocystinuria, Thiamine-responsive megaloblastic anemia, Protein S or C Def, CDG, SCD,
PGK
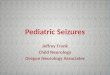
Metabolic AcidosispH <7.2, CO3H <10,
PCO2 <25
HyperammonemiaNH3 >100, pH >7.45,
PCO2 <25
Hypoglycemia<20
Lactic AcidemiaLac >4
Ketosis +PCD, MDD, RCD, MMA, PA, IVA, GA I, MSUD, FDP, G6P
Ketosis –PDD, HMG-coA,
FAOD, FDP
Euglycemia UCD (OTC, CPS, ASS, AS)
HHH, LPI, AGS
HypoglycemiaFAOD, HMG-coA
Acidosis +Neoglucogenesis def
MSUD, HMG CoA
Acidosis -FAOD, HMG-CoA
EuglycemiaPC, MCD, RCD, Krebs & Mito DNA mut, PDH
HypoglycemiaFDP, G6P, PC,
FAOD
Metabolic Coma
Pediatric Neurology Handbook. Lippicontt. 2013

Neonatal Hyperammonemia
OTC DefCPS Def
No Acidosis
Sx < 24 hours of life Sx > 24 hours of life
Premature Full term
Transient Hyperammonemia of the neonate
IEM-Organic Acidemia-Pyruvate Carboxyl Deficiency
Acidosis
Organic Acidemias
Urea Cycle DefectsPlasma Amino Acids
Absent Citrulline Moderately elevated Citrulline, ASA present
Markedly elevated Citrulline, no ASA
CitrullinemiaArgininosuccinic aciduriaUrine Orotic Acid
Low High
HypoglycemiaHypoketosis
-Resp Chain Dz
Normoglycemia
Pediatric Neurology Handbook. Lippicontt. 2013

Normal Lactate Elevated Lactate
Abnormal Organic Acids
ORGANIC ACIDEMIA
MMA, PA, MDD
Dicarboxylic Aciduria
Hypoglycemia
Elevated Pyruvate, normal
L:P ratio
RCD, PCD
Abnormal Organic Acids
Normal Organic Acids
Anion Gap Metabolic Acidosis
Fatty Acid Oxidation Def
Normal-low Pyruvate,
elevated L:P ratio
No Hypoglycemia
PHD, PCD GSD I, Fructose 6-DP Def, PEP Carboxykinase
Def.
Pediatric Neurology Handbook. Lippicontt. 2013

ThankYou.AnyQuestions?
35

Appendix

Hyponatremia


Clinical Manifestations• Serum [Na] > 130 mmol/l
– Usually asymptomatic
• Serum [Na] 125-130 mmol/l– Predominantly GI symptoms (nausea,
vomiting)
• Serum [Na] < 125 mmol/l– Lethargy, headache, ataxia, psychosis,
weakness
– Severe cerebra edema-seizures, coma, brain-stem herniation, respiratory depression/arrest

Complications
• Complications of Hyponatremia– Rhabdomyolysis
– Seizures
– Permanent neurologic sequelae (from seizures or cerebral edema)
– Death
• Complications of Treatment– Fluid Overload
– Central Pontine Myelinolysis: ODS

Central Pontine Myelinolysis
• Focal demyelination of pontine and extrapontine areas
• Symptoms 1-3 days after rapid correction of Na– Dysarthria/dysphagia– Altered mental status, seizures
– Quadriparesis– Hypotension
• Often Irreversible
• Possible Therapy: relowering of Na with hypotonic fluids and desmopressin
Soupart A, Ngassa M: therapeutic lowering of the serum sodium in a patient after excessive correction of hyponatremia. Clin Nephrol. 1999 51 (6) 383-6

Whatkind?
Pediatric Neurology Handbook. Lippicontt. 2013

TreatmentofHyponatremiaSIADH:waterrestrictionandnormaltohypertonicsaline.CSW:saltloading,volumereplacementandfludrocortisone.
ACUTEHYPONATREMIA:IfNahasfallenrapidly(<48h),therearesymptoms,orNais
• <110mEq/L,thenitshouldbecorrectedrapidly.– Thegoaloftreatmentistoincreasetheserumsodiumlevelby1.5to2mEq/L/huntil
symptomssubsideoruntilthesodiumconcentrationis>118to120mEq/L,withtheprimaryfocustominimizetheriskofseizure.
– Eveninsymptomaticpatients,thesodiumlevelshouldnotbeincreasedby>12mEq/Linthefirst24h,orby>18mEq/Linthefirst48h,toavoidosmoticdemyelinationsyndrome.
• Whenpatientsbecomeasymptomaticandsodium levelsriseabove118mEq/L,correctionshouldbeslowedtono>8mEq/Lin24htoachievethetargetsodiumconcentration.
CHORNICHYPONATREMIAshouldbecorrectedataslowerrate,• Notexceeding0.5mmol/L/hor10to12mEq/Loverthefirst24h.• Useofhypertonic23%Nasolution iscontroversialinthePICUandreservedonlyfor
acutemanagementwhenimminentherniationorseizuresarepresent.

Status Epilepticus in Children

Management
Pediatric Neurology Handbook. Lippicontt. 2013

Neuroassessments

Reilly P.L., Simpson D.A, et al Child Nerv Sys 1998

Reilly P.L., Simpson D.A, et al Child Nerv Sys 1998

Kirkham, Newton et al 2008 Dev Med and Child Neurology

Infant Face Scale (IFS)
Durham et al, J Neurotrauma 2000

Pediatric Neurology Handbook. Lippicontt. 2013

TargetedTemperatureManagementinPediatricNeurocriticalCare:Clinical
Update
SarahMurphy,MDPediatricCriticalCare/PediatricNeurocriticalCareMassGeneralHospitalforChildren

Ihavenorelevantfinancialrelationships todisclose

Hypothermia
TherapeuticHypothermia
TargetedTemperatureManagement
InducedHypothermia

Pubmed KeywordSEARCHdp 2013-2015
• “Hypothermia”2385• “Hypothermia”and“TBI”96• “Hypothermia”and“CardiacArrest”608• “TargetedTemperatureManagement”66

Neuroprotection:
Thiopental
Corticosteroids
Mannitol Magnesium
Barbiturates Nimodipine
ICPMonitoringHypothermia

Neuroprotection:trials
Thiopental
Corticosteroids
Mannitol Magnesium
Barbiturates Nimodipine
ICPMonitoring

Neuroprotection:
Thiopental
Corticosteroids
Mannitol Magnesium
Barbiturates Nimodipine
ICPMonitoring
HYPOTHERMIA

• Therearebothimmediateanddelayedprocessesof“secondary”injury

Pathophysiology ofglobalischemicevent
• Cascadeofbraininjurybeginswithinminutes• Oxygenstoresdepletedwithin20seconds• GlucoseandATPdepletedwithin5minofischemia
• AfterROSCinsufficientperfusionofthebrainpersists– “Nore-flow”(microvasculardysfunction)– Failureofcerebralautoregulation

IschemicCascade
• DepleteATP• Na+andK+transmembranegradientsarelost• Depolarizationofcellmembrane• IncreaseinintracellularCa• Releaseofglutamate• Activationofenzymesystems

ReperfusionInjury
• Oxygenfree-radicalspeciesinducedamage• Lipidperoxidation• Continuedactivationofglutamate• Enhancedactivityofinflammatorycells

• Increasestissuetolerancetoischemia– Decreasingcerebralmetabolicrate• Mitigatesdamage– Quietstheinflammatorycascadeandproductionofreactiveoxygenspecies
Hypothermia


Dell’anna et al Curr Opin Critical Care 2014

??

TargetedTemperatureManagement• Clinicalindication:globalhypoxic-ischemicinjuries
– Post-cardiacarrestsyndrome– NeonatalHypoxic-IschemicEncephalopathy

NielsenandTTMTrialInvestigators2013,NEJM369:2197
THAPCA

Whatwasthebackground?



Bernard HACA
n 77 275
temp 33 32-34
duration 12h 24h
rapidity 2 hrs, met goal 4 hrs, median 8
incl/excl vfib witnessed vfib/vtach

BERNARD:AdjustedforageandtimetoROSC,oddsratioofgoodoutcomeinHTgroup5.25(1.47-18.76,P=.011)49%vs26%(p=.046)
HACA:55%vs39%“good”outcomeRRofgoodoutcome1.4(1.08-1.81)Mortality41%vs55%


Sterz,CurrentOpinioninCriticalCare2003

How Ice Can Save Your Life'Therapeutic Hypothermia' Can Protect the Brain in the Aftermath of Cardiac Arrest
By RON WINSLOWUpdated Oct. 6, 2009 12:01 a.m. ET
The Wall Street Journal, 2009

‘‘A healthy brain and functional patient are the primary goal of cardiopulmonary-cerebral resuscita-tion. Brain-oriented intensive care is essential.’’—American Heart Association

Though benefit was demonstrated in specific population: adults with out of hosp vfib/vtach witnessed arrest, the use of TH was extended to other, scenarios in advance of clinical trials that might prove benefit, including patients presenting with non-shockable rhythms, patients who had an in-hospital arrest, and pediatric patients.


Nielsenreview
• Included 5 RCTs (478) patients
• The majority of hypothermia trials compare hypothermia with no temperature control
– Hypothermia should not be recommended without a trial comparing a “fever control” control group with “hypothermia” treatment group
• Prognostication and the problem of re-direction of care
– Most common cause of death in studies is withdrawal of life-support
– None of the studies specified how a decision about withdrawal of intensive care was made, whether assessor of prognostication was blinded
IntJournalCardiology2011

2001
OR of poor outcome: 2.26 (1.24–4.12) for every degree higher than 37 °C
2002
OR of survival 2.7 (1.2-6.2) for temp < 37.8

• RCT,randomizedtoTTMof33or36• Conductedat36centersinEuropeandAustralia• Inclusion:Adults,OOHCA,GCS<8onarrivaltohospital,ROSC
for20min,• Exclusion:unwitnessed asystolic arrest,>4hrsfromROSCto
randomization,ICHorstroke,temp<30• TTMfor28hrs,bothgroupssedated,aggressivecontrolof
tempincontrolandinterventiongroup• Intentionfornormothermia for72hrs
NielsenandTTMTrialInvestigators2013,NEJM369:2197



Intervention
• Interventionperiodwas36hrsfromrandomization
• Allpatientssedated,continuoustemperaturemanagement,maintainedatgoaltemperature(methodnotspecified)
• At28hrsbegangradualrewarmingto37by0.5deg/hr
• Intentionwastomaintain<37.5for72hrs• After36hrsnomandatorysedation,atdiscretionofsites

• 950patientsenrolled• Primaryoutcome:mortality– Followedfor180d• Secondaryoutcome:poorneurologicfunctionordeath(CPC3-4,MRS4-6)

P<.001forseparationoftemperaturecurves


• Mortality50%inhypothermiagroupand48%inthenormothermiagroup[hazardratio1.06;0.89-1.28,p=0.51]
• RiskratioofaCPCof3-5fornormothermia1.02[0.88-1.16,p=0.78]
• RiskratioofMRSof4-61.01[0.89-1.14,p=0.87]


Withdrawalofcarein247(26%)patients





??

2015Ahapost-cardiacarrestguidelines

• Windowof4hrstoolong?Another4hrstocooling?
• Intra-arrest/Intra-cprcooling?• Hemodynamicoptimization?• Higherproportionofdeathsbeforeprognosticationin33deggroup?
• Effectsofsedation?• Toorapidre-warming?

• However, this finding was not borne out in a randomised controlled trial that included 1359 patients with out-of-hospital cardiac arrest due to both shock- able and non-shockable rhythms and found similar rates of sur- vival to discharge or neurological outcome.
22 Moreover, a higher incidence of hypoxia and pulmonary oedema after cold saline infusion was noted in the
prehospital cooling arm. It remains unclear whether the use of a surface cooling method, as used in the other hypothermia trials instead of cold saline infu- sion, would have altered the study’s outcome.
1. Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. JAMA 2014;311:45–52.


PediatricCardiacArrest
• EpidemiologyofpediatricCA:10,000children/yr
• Highmorbidityandmortality• Usuallyduetoasphyxiaandshockasopposedtoadults
• MostcommonlyPEAandasystole(rhythmsexcludedfromRCTs)
• Betteroutcomesthanadults




Circulation,2009
AdjustedfordurationofCA,propensityscores,ECMORetrospective,included79patientsfrom5CanadiancentersHypothermiausedmoreoftenafterprolongedarrestorwithECMOMostlycardiacpatients,neonatalDidtreat/aimedtopreventfever

• AlsocomparedtargetedNormothermia(36.8)toHypothermia(33)
THAPCA

• Conductedat38PICUsinUSandCanada• Children>48hrsand<18yo• OOHcardiacarrest• Exclusion:unabletoberandomizedby6hrs,majortrauma,
electnottopursueaggressivetreatment,mGCSof5or6
THAPCA- OutofHospitalCardiacArrestTrial

• Randomized1:1bypermutedblocks• TTMwasactivelymaintainedfor120hrsinbothgroups
• BlanketrolIIIforcoretemptargetfor48hrs• Rewarmedover16hrsto36.8• Maintainedat36.8x120hrs
THAPCA- OutofHospitalCardiacArrestTrial


• Primaryoutcomesurvivalwithgoodneurobehavioraloutcomeat12months
• “goodoutcome”standardscoreof70orhigheronVinelandAdaptiveBehaviorScalre








TargetedTemperatureManagement
• TBI(adultandpediatric)• Stroke• Spinalcordinjury

• Primarybraininjuryfromdirecttrauma– Macroscopic:
• Shearingofwhitemattertracts• Focalcontusions• Hematoma• Edema
– Cellular:• Microperforationofmembranes• Leakingionchannels• Microhemorrhage• Conformationalchangesinproteins
TBI

• Secondaryinjury(Acute/Subacute/Chronic)– Neurotransmitterrelease– Freeradicalformation/oxidativestress– Ca-mediateddamage– Geneactivation– Mitochondrialdysfunction– Inflammatoryresponse
– Seizures– ICH
TBI

TBItrials
NABIS:HI

TBItrials
NABIS:HI
NABIS:HII

TBItrials
NABIS:HI
NABIS:HII

TBItrials
NABIS:HI
NABIS:HII

TBItrials
NABIS:HI
NABIS:HII
EUROTHERM

Stroketrials
• Systematicreviewandmeta-analysisforevidenceofefficacyinanimalmodelsofAIS

• 86publicationsincluded,15abstracts• Mediantempofcooling33(24-35)• Overalldecreaseininfarctsizeby43.5%(95%CI:40.1-47.0%)
• Overallimprovementinneurobehavioralscores45.7%(95%CI:36.5-54.5%)

Stroketrials• Hypothermiaimprovedoutcome– histologicalandfunctionaloutcome• Efficacywasgreatest:– atlowertemperatures– whentreatmentwasstartedbeforeoratonsetofischemia– intemporaryischemiamodels

IntravascularCoolingintheTreatmentofStroke(ICTuS)trial,awakestrokepatientsweresuccessfullycooledusinganendovascularcoolingcatheter
IntheICTuS-Lstudy,thecombinationofendovascularhypothermiaandthrombolysiswasshowntobefeasibleandhypothermiahadnoincreasedriskofbleeding
ICTuS2/3designedtostudysafetyofcombinedthrombolysisandendovascularhypothermiaandtodetermineifthecombinationshowssuperioritycomparedwiththrombolysisalone.
ICTuSTrials

FeverPOOR Outcome

ClinicalAssociations
• Feverinallbraininjurytypesisassociatedwithmorbidityandmortality(GreerStroke2008)
• FeverintheacutestageofSAHindependentlypredictsmorbidityandmortality(FernandezNeurology2007)
• FeverearlyafterTBIisassociatedwithincreasedICP,worseneurologicoutcome(BohmanCurrOpinCriticalCare2014)
• Degreeanddurationoffevercorrelatedwithoutcome(LiJNeurotrauma2012)

AnimalEvidence
• Elevationsintemperatureincreasepro-inflammatorycytokines
• Increaseaccumulationofneutrophilsininjuredtissue
• Increaseneuronalexcitotoxicity• Increaseneurotransmitterrelease• Acceleratefree-radicalproduction• Increaseintracellularacidosis

Fever
• Elevationofcorebodytemp>37• Commoninpatientswithbraininjury(Badjatia2009,
Thompson2003)
• 7-13%increaseincerebralmetabolismforeach1%increaseincorebodytemp
• Thoughhealthyhumanbrainsareabletotolerateincreasesinmetabolism,injuredbrainmaynot
• Lowerthresholdforischemia,at-riskofmismatchbetweenimpairedflowandincreaseddemand

Conclusions:

CardiacArrest

TBIStrokeOtherNeurologicInjury?