-
18.ThefundamentalsofpediatricradiologyAuthor:vaKis
SemmelweisUniversity1stDepartmentofPediatrics,Budapest
18.1.Differencesbetweenpediatricandadultradiology
Thechildisnotasmalladultitmightseemasaclich,butinfactitisthebasictruth.Childrenandadolescentsufferfromdifferentdiseasesthanadultsandrequiredifferenttherapiesaswellasalteredimagingapproaches.Thestrategiesfordiagnosticimagingaredifferent,althoughthemodalitiesarethesameorsimilartothoseusedinadultradiology.Thesequenceofmodalitychoice,someofthetechnicalparametersandthefollowupprotocolsaredifferentinpediatricradiology.Thenumberonedifferenceisradiationsafety.Childrenareespeciallysensitivetoionizingradiation.Immaturetissuesareextremelysensitivetoradiationandthereisnominimalsafetydosagethatisconsideredabsolutelyharmless.Tissuesingrowthandtheredbonemarrowthattakesupmostofthebonemarrowtissueatthisagegroupareespeciallysensitivetoradiation.Becauseofthesmallerbodysize,thegonadsareclosertotheirradiatedzones.Moreover,becauseofthelongerlifeexpectancyinchildren,thecumulativedoseofnaturalandartificialradiationmeanhigherriskforthedevelopmentofmalignantdiseases.Thebestprotectionistominimizeortocompletelyavoidtheuseofionizingradiationinchildren.This,ononehandmeansstrictcontrolandsupervisionoftheindicationsofXrayandCTexaminations,ontheotherhand,whenpossible,theuseofnonionizingexaminationssuchasultrasoundorMRIarepreferred.TheotherperspectiveofradiationsafetyistodecreasethenumberofXrayexpositionstothebareminimum,meaningthatunnecessaryrepetitions,comparativeormultiangularexaminationsshouldbeavoided.CTexaminationsshouldonlybeperformediftheyareabsolutelynecessaryandifsowiththeuseofspecial,lowdoseprotocols.ThesocalledALARAacronymstandsforAsLowAsReasonablyAchievable,thereforeitmeansthatoneshouldusethelowestdosageofradiationpossible.Thispointofviewcanneverbeneglectedinpediatricradiology.Thischapterismeanttointroducethemostimportantradiologicmodalitiesinchildrenandadolescentcaredifferingfromtheadultradiology,aswellastogiveanoverviewofthemostcommondiseasesinashortandbasicmanner.
18.2.Radiologicdiagnosticsofthechest18.2.1.Thenormalnewbornchest
Normalnewbornlungs:anewbornschestgoesthroughsomefundamentalchangesduringthefirstdaysofextrauterinelife.Theheartisrelativelyrounded,characterizedbythedominanceoftherightside.Thecardiothoracicindextakeninamidinspiratorystateisbetween0.550.62.Expiratorystatecanleadtodiagnosticmistakes.Thymus:isusuallymadeupoftwoasymmetricallobes,situatedintheanteriorsuperiormediastinumandshowsagreatvariabilityofbothsizeandshape.Itdoesnotcauseanycompressionontheneighboringorgans.Onultrasoundexaminationitappearsasahomogenoussolidtissue,relativelymorehypoechoicthanthethyroidgland.Thediaphragmisabitmoreelevatedinmidinspiratorystateitsarchisbetweenthe89thribonthebackandatthe6thribinthefront.Bonythorax:theribsarehorizontalandthesagittalandhorizontaldiametersofthechestareveryclosetoeachother.
1.a.Expiratorystate:thetransparencyofthelungisdiffuselydecreased.
1.b.Inspiratorystate,thelungistransparent,theheartisnormalsized.Ribsrunhorizontallyininfants.
2.Thymushasacontouronbothsides.Healthynewborn.
18.2.2.Afewdiseasesofthenewborns
Wetlung,transitoricustachypnoe.Fetalliquidsinthelungarenotproperlydrainedbythevenousandlymphaticvessels;thenewbornwillshowsignsofdyspneaandtachypnea.OnXray,thechestappearshyperinflated,withdecreasedtransparencyandwitharelativecardiomegaly.Thesesignsusuallydisappearwithin72hours.IRDS(Idiopathicrespiratorydistresssyndrome).Preterminfants,youngerthan34weeks,haveimmaturelungswithsurfactantshortagethatleadstoalveolarinsufficiency.Thebreathingdisorderprogresseswithtimeastachypnea,dyspnea,cyanosisandgruntingoccur.OnXrayimagestherespiratoryvolumewillregressandadiffusereticularnodularpatterncanbeobserved,alsowideairbronchogramswillappearrunningtotheperipheries.Thecontoursoftheheartwillbeblurredorevenacompletelossoftransparencyisvisible(stagesIIV).Surfactantadministeredintimewillresultinimprovedradiologicpicture.Meconiumaspirationsyndrome(MAS).Itisfrequentlythediseaseoftermandposttermnewborns.Thefetusdefecatesmeconiumtotheamnioticfluidthatis
-
aspiratedatbirth,anditcauseschemicalpneumonitis.Ontheradiographthisisdepictedwithcoarsepatchyandstreakyalveolarshadows.Bronchopulmonarydysplasia(BPD).Itisthepulmonarydamagethatoccursinimmaturenewbornsduetoprolongedperspiration.Itsradiologicpicturedependsonthestageofthedisease,earlysignsofBPDareundistinguishableformIRDS.Inlaterstages,thelungishyperexpandedwithpronouncedcentralreticularpattern.Atelectasisisafrequentcomplicationthatpromotestheappearanceofinfectiousdiseases.
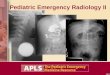
3.Whitelung.IRDS.IV.
4.Asnowstormlikenodularpatchyinfiltrateonbothsidedofthelung.
Meconiumaspiration.
5.Thebasallobesofthelungareinflated,onbothsidesthereisanirregularreticularpattern.BPD.
6.Intestinalshadowsintheleftsideofthechest,themidlineisdislocatedtotheright.Leftsideddiaphragm
hernia.
Congenitaldiaphragmhernias.Itistheresultofabnormaldiaphragmdevelopment.Itsradiologicpictureisinfluencedbyitsseverity,localization,andtimeofduration.Leftsidedherniasaremorefrequent(alsocalledBochdalekhernias).Thenewbornsuffersfromrespiratoryinsufficiency,intestinalanddislocatedheartsoundscanbeheardabovethechest,theabdomeniscollapsed.TherightsideddiaphragmherniaisalsocalledtheherniaofMorgagniandcausesalesssevereclinicalpicture,manytimesdiscoveredaccidentallyontheXray.Onultrasoundthemissingdiaphragmandaherniatedportionoftheliverisseen.
18.2.3.Pneumonia.
Incaseofcharacteristicclinical,auditoryandpercussionexaminationresults(crepitation,bronchialbreathingsounds,dullnessatpercussion)aradiologicexaminationisnotevennecessary.Radiography:forthemajorityofpneumoniasasinglePAchestXrayisenoughforthediagnosis.Theinitialexaminationwithinthefirst24hoursofonsetisgenerallynegative,ifitsclinicallynecessary,controlexamistobeperformed.However,ifthetreatmentforbronchopneumoniaimprovestheclinicalsymptomsXraycanbeneglected.Thefinalconfirmationthattheinfiltratehasbeenresolvedisalwaysdocumentedonaradiograph.Incaseofpleuropneumoniasultrasonographyiscapabletocontrol,toanalyzeandtofollowthecourseofthepleuraleffusion.Therefore,manycontrolXrayexamscanbesubstitutedwithUS.Xrayingeneralisnotappropriatetofullydeterminetheetiologyofpneumonia,butcanbeindicativeinsomecases.StreptococcusBpneumonia:.isanacquiredinfectionafterbirthofmaturenewbornsanditcanmimicIRDS.ThedifferencetoIRDSisthecoarserreticularnodularappearanceaccompaniedbypleuraleffusionatmanytimes.Sometimesscatteredorconfluentperihilarpatterncanberecognized.Staphylococcusaureuspneumonia:isacommonbacterialpneumoniainsmallbabies.ItsclinicalpictureonXrayisaccompaniedbycoarsenodularorconfluentinfiltrations,withfrequentpleuraleffusions.Thepneumonicnodulesconsolidatefastandformpneumatocelesthatcangrowfurtherandpersistforalongertime.Healingusuallylastsformonths.Roundpneumonia:isacharacteristicpediatricdisease.TheroundshapedinfiltrationmimicsatumorontheXrayimage(neuroblastoma,bronchogeniccyst).Acutedevelopment,afeverishstate,andairbronchogramappearancewithintheinfiltratehelpwiththedifferentiation,aswellastheregressionoftheinfiltratebytheendofthetherapy.ThemostcommonbacteriumisStreptococcuspneumoniae.Furtherimaging(CT)israrelynecessary.
7.Pneumatocelesintherightupperlobe.
8.Almostcompleteresolutionwithinonemonth.
9.aAtexpirationtherightsideisexpanded.
9.b.Atinspirationthemidlineisshiftedtotheright.Holzknechtsign:foreignbodyin
therightbronchus
18.2.4.Airwayforeignbody
-
Childrenputanythingintheirmouthand,thereforefromtimetotimeaccidentalaspirationstendtooccur.Thesymptomsofacuteaspirationareveryapparent.Apneumoniarecurringatcertainlocalizationishighlysuggestiveofchronicaspirationofaforeignbody.Hence,theroleofradiologyismoreimportantinchroniccasesofaspiration,wherepatienthistorydoesnotnecessarilyindicateforeignbodyaspiration.Xrayexamination:aspiratedforeignbodiesarerarelyXrayabsorbing,andthereforerarelyappearontheradiographs.AnegativeinspiratorychestXraydoesnotexcludethepossibilityofaFBaspiration.MostFBscauseocclusiononthelevelofthebronchi,whichmeansthatininspirationaircangetfurtherthantheFBbutatexpirationitwillblocktheairway.Thus,onexpiratorychestXray,theaffectedlungsegmentwillbepneumatic;thediaphragmwillbepushedlowerontheipsilateralside,whileatinhalationthemidlinewillbeshiftedtowardstheaffectedside(Holzknechtsign).InsuspicionofFBaspiration(evenifchestradiographisnegative)bronchoscopyiscompulsory.
18.3.Gastrointestinal(GI)tract18.3.1.Examinationmethods:
Preparation:Whenperformingapassageexaminationinnewbornsorsmallinfantsthelastfeedingisskipped.Astartingabdominalplainfilmradiographismandatorybeforeeachpassageexamination(toidentifythedistributionofintestinalgas,toruleoutfreeabdominalair,orintestinalwallpneumatizationandtolocatethelevelofobstruction.)Plainabdominalxrayisinmanycasesinformative,whethercontrastadministrationisreallynecessary,andifanimmediatesurgeryisunavoidable(e.g.:freeabdominalair,orincaseofaproximalatresiainnewborns).Incasesofcontrastexaminations(passageexamorcolonenema)thepreferredcontrasagenthasalowosmolalityandisabsorbable.
18.3.2.Afewimportantdiseases
Esophagealatresia:iscommonlylocatedattheleveloftheupper/middleesophagealborderandissometimesassociatedwithtracheoesophagealfistulas.Newbornsareunabletoswallowtheirsalivaandthediagnostictubegetsstuckintheesophagus.Themostcommonformisatresiawithalowerfistula.In50%ofthecasesotherabnormalitiesarepresent;aspartofthesocalledVACTERLsyndrome(vertebral,anal,cardiac,tracheoesophagealfistula,renalandlimb)variousadditionalabnormalitiescanbeobserved.Xrayexamination:anXrayabsorbenttubeisvisibleintheobstructeddiverticulaoftheesophagus.Incasesofalowerfistula,theintestinesareaerated,theaccompanyingcostalandvertebralabnormalitiescanalsobeobserved.Hypertrophicpyloricstenosis(HPS).Asaresultofthehypertrophyandhyperplasiaofthepyloricmusculatureasecondarystenosiscanoccur,thatusuallyleadstosymptomaticstatesin36weeksoldinfants.Itprimarilyoccursinboysasfrequent,progressive,nonbilious,projectilevomiting.Onultrasonographyanenlarged(15mmormore),thickwalled(3mmormore)pyloruscanbeseeninbothlongitudinalandinaxialcrosssection.
10.Thetubeinsertedintheesophagusturnsbackintheheightofthe4thThoracic
vertebra,theintestinesarefilled
withgas.Esophagusatresiawithlowerfistula.
11Thetubeinsertedintheesophagusturnsbackintheheight
ofthe2ndThoracicvertebra.Theabdomenis
gasless.Esophageal
atresiawithoutfistula.
12a:AbdominalUS:thepyloriccanalisextended,itswallisthickened.Pylorus
stenosis,longitudinalview.
12.b.Axialcrosssection.
Duodenalobstruction.Thecauseofproximalobstructionisprimarilyduodenalatresiaorstenosis.UsuallyUSisabletodepictthedistendedstomachandduodenumduringintrauterineUSexaminationasacysticmass,whileotherintestinesarecompletelyfreeoffluids.Vomitingoccursinthefirsthoursofextrauterinelife.Plainabdominalradiographincasesofatresiawillrevealthesocalleddoublebubblesign,wherethestomachandtheduodenumaredistendedbutondistalsegments,theintestinesaregasfree.Incasesofstenosis,thedistalintestinalloopswillalsoshowsomeaircontent.Otherexaminationsareunnecessaryandaircanbeusedasanegativecontrastmaterial.Malrotationvolvulus.Duringthenormaldevelopmentoftheintestinaltract,theintestinalloopsmakethree90degreeclockwiserotationsaroundthemesentericsuperiorartery(MSA.)Ifthisrotationonlypartiallyoccursduringtheembryonicdevelopmenttheintestinesremaininanonrotationalormalrotationalposition,themesentericrootwillbeshorterandthececumwillbeweaklyattached.Thisanatomicpositioningcanbesymptomfreethroughoutalifetime,butitpredisposesforvolvulus.Volvuluscanoccuratanyage,butitismostfrequentinthefirstmonthsoflife,whenitabruptlyoccurswithacutebiliousvomiting.Inthisstatetheintestinesaroundthemesentericroottwist,endupinacompleteobstructionthatcanleadtoarapiddeathoftheintestines.Ultrasonographycandepictthemesentericsuperiorvein(MSV)coileduparoundtheMSA,socalledwhirlpoolsign.DuringXrayexaminationthecontrastmaterialdoesnotprogresstothejejunalloopsoritshowsacorkscrewsignontherightsideofthevertebraeasitpilesupin
-
thetwistedintestinalloops.
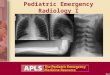
13.Distendedstomachandduodenalbulbus,Doublebubblesign.Duodenal
atresia.
14.WhirlpoolsignThemesenteryandthesuperiormesentericvein,asitcoilsaroundthesuperior
mesentericartery.Volvulus.USexam.
15.Contrastmaterialemptiesthestomachslowly,smallintestinesarefoundontherightsideoftheabdomen.Malrotationvolvulus.
16.Nonused,narrowcolon.Newborn,meconium
ileus
Meconiumileusoccursin10%ofchildrenwithcysticfibrosis(CF),andalmostallofmeconiumileuscasesarearesultofCFdisease.Itischaracterizedbyvomitingandabdominaldistention,asthemeconiumcannotbedefecated.Onplainabdominalradiographtheintestinesaredistendedwithoutanyairfluidlevelsduetotheadhesivenatureofmeconium.Colonenemaexaminationwithwatersolublecontrastmaterialwillshowamicrocoloninwhichthemeconiumwillcausecontrastfillingdefectsresemblingsmallpearls.Contrastmaterialthatreachestheterminalileum,andtherepetitionoftheenemascansometimessolvetheileus.Invagination.Adistalintestinalloopinvaginatingtoaproximalintestinalloopcanresultinamechanicalintestinalobstruction,andcauseischemicdamage.Itmostfrequentlyoccursininfants(324months)withrecurring,coliclikecomplaints,distendedintestines,apalpablemassandwithfrequentvomitingandbloodystool.Invaginationrequiresimmediatediagnosisanddesinvagination.USexamrevealstheinvaginatedintestinesasatargetsigninaxialcrosssectionandlookslikeapseudokidneyinlongitudinalcrosssection.Thetherapyishydrostaticorpneumaticdesinvagination.Perforationand/orperitonitisareabsolutecontraindicationstotheseprocedures.HydrostaticdesinvaginationcanbeperformedunderfluoroscopyorwithUSguidanceandisconsideredsuccessfulifairorthecontrastmaterialappearsintheterminalileumandtheinvaginatedloopdisappears.Iftheseeffortsdonotsucceed,surgicaldesinvaginationisneeded.
17.Targetsign.Invagination.. 18.abcDesinvaginationwithair.
18.b.Arrow:invaginatedsegment.
18.c.Successfuldesinvagination
Necrotizingenterocolitis(NEC).Itisasevereintestinalnecrotizingdiseaseofthenewborns.Itusuallyoccursasearlyasthefirst10daysoflife,butcanhappeninthefirstfewmonthsafterbirth.Vomiting,distendedintestines,bloodystool,acidosis,peritonitisandperforationarefrequentfindings.PlainabdominalXraycanbenoninformativeintheearlystagesofthedisease;laterdistensionindicatestheseparationofloopsduetowallthickening.Often,airbubblesappearintheintestinalsubserosalorsubmocosallayers,ascharacteristicsignsofintestinalpneumatosis.Theintramuralaircandiffusetothemesentericveinsandappearintheportalcirculationintheprojectionoftheliver.Freeabdominalairisindicativeofperforationandrequiressurgicalintervention.USexaminationcanrevealthesecharacteristicsofthediseasebeforeXrayisindicative.UScandepictthickenedintestinalwall,portalandintramuralair,abdominalfreefluidorabscesses.Hirschsprungdisease.Inthisdiseasetheganglionsofthedistalcolonaremissing.Thelackofinnervationofthecolonicsmoothmuscleresultsinspasticfunctionalobstruction.Thesymptomscanappearrightafterbirthwiththelackofmeconiumdefecationandsignsofobstruction.OnplainabdominalXraytheproximalintestinesaredistendedwithorwithoutairfluidlevels,thedistalloopsaregasfree.Withcontrastenemathedistal,irregular,spastic,noninnervatedsegmentsandtheproximalprestenoticdilatationofthecoloncanbevisualized.
-
19.Distendedbowelloops.Airisseenintheintestinalwall,
intestinalpneumatosis.Necrotizingenterocolitis.
20.NEC,USexamination.Freeabdominalfluid,withdense
innerechos.Airbullblesintheintestinalwall:zebrasign
(arrow).
21.Thedistalsegmentofthecolonisnarrow,irregular
(aganglionarsegment).Transitionalzone(arrow)
andcompensatoryprestenoticdilatation.Hirschsprungdisease.
18.4.Urogenitalsystem18.4.1.Diagnosticmethods
Ultrasoundisthemethodofchoice,providesdetailedinformationofthemorphologyofthekidneysandtheurinarytract.Prenatalexaminationscanreadilydiagnosemostofthelesionsattheintrauterineage.Mictioncystourethrography(MCU).Isthegoldstandardfortheimagingofthebladderandthedistalurinarytractsaswellastheinvestigationofvesicouretralreflux.Aurinarycatheterisinsertedandcontrastagentisadministeredwithfluoroscopiccontrol.Sonocystography.Ultrasonographiccontrastmaterialisadministeredtothebladderthroughacatheter.Thecontrastmaterialincreasestheechogenityoftheurine(fluid)andincasesofrefluxthischangecanbedetectedintheureterandthepyelon.ThismethodinmostcasescansubstituteMCU,however,theurinarycatheterstillremainsaninvasivestepoftheexamination.Nuclearmedicineexaminations(seethere)MRurography(seethere)
18.4.2.Someimportantdiseases
Congenitalobstructiveuropathies.Congenitalabnormalitiesofkidneydevelopmentcanoccuratanyleveloftheurinarytract.Itsmostcommonsingisurinarytractdilatation.Theroleofimagingisin:diagnosingthecause,thelevelandthestageofdilatationanddifferentiatingtheobstructivecasesformnonobstructiveones.Uretropelvicobstruction(UPO).Uretropelvicjunctionstenosiscanbeanacquiredoraninnatestate,withdifferentdegreesthatleadtothedysfunctionofexcretionofurinefromthepyelontotheproximalureter.Itisthemostfrequentformofobstructiveuropathy.USexaminationevenatprenatalstatescandiagnosetheurinarytractdilatationthatcanbeuniorbilateral,alwayswithoutureterdilatation.Isotopeexamination:theisotope(Tc99mMAG3)injectedwithdiureticscanbeusedtoanalyzerenalfunction.Distalurethralvalve(subvesicalobstruction).Itisthemostsevereformofobstructiveuropathy.Innewbornboysthevalvedysfunctioncanleadtobilateralobstructionwithhydronephrosisandhydroureter.Urinationcanonlyoccurintermittently.Thebladderwallisthickened,trabecularandrefluxisfrequent.Theproximalurethraisdistendedaswell.
22.Thecalicesandthepyelonofthekidneyaremarkedlydilated,theparenchymais
thinner.Severehydronephrosis.Theureterisnotvisible.Pyelouretralstenosis.
23.Mictioncystourethrography.Asmalldiverticulaisseenontherightside,theproximalurethraisdilated,beneathisafilling
defect.Subvesicalobstruction,dorsalurethral
valve.
Vesicouretral(VU)reflux.Refluxstandsforthereentryofurinefromthebladdertotheureterandthecollectingsystemofthekidneysduetotheinsufficiencyoftheuretrovesicalvalve.Thiscanleadtoatransientorapermanentdilatationoftheurinarytracts.UScanonlyraisesuspicionforUVrefluxthroughindirectsignssuchasthickenedpyelonwall,smallkidney,thinnerandblurrycorticomedullaryjunction,unevenparenchyma,thickenedbladderwall.RefluxcanbedepictedwithMCUorsonocystogrphy.Refluxisinternationallycategorizedin5levels(IV).Itsspecialformistheintrarenalrefluxthatappearsintheupperorlowerpoleofthekidney.
-
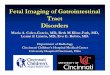
24.a. 24.b. 24.c. 24.d. 24.e.
Mictioncystourethrography.a.Refluxintheleftnormaldiameterureter.VURl.s.Gr.I.b.Bothuretershaveanormaldiameterastheyrefillwiththecontrastmaterialrefluxingfromthebladder.VURl.u.Gr.II.c.Thereisaslightlydilatedrightureterandcollectingsystemintherightkidney,thecalicesarewidened.VURl.s.Gr.III.d.Dilatedureterandcollectingsystemcanbeseenontheleftside.VURl.s.Gr.IV.e.Therightureterismarkedlydilatedandelongatedthepelvicalycealsystemisalsomarkedlydilated,thecalicesarerounded,contrastmaterialappearsinthetubulesaswell.VURl.d.Gr.5.withintrarenalreflux.
18.5.Abdominalmasses
Neuroblastoma.isatumorthatdevelopsatanypartofthesympatheticnervoussystem.Therefore,inover90%ofthecasestheurinarycatecholaminelevelsareelevated.Itisthemostfrequentextracranial,solidtumorinchildrenandhasitshighestmalignancyratewithinthefirstyear.Itismostcommoninchildrenaged15years,appearsasapalpableabdominalmass,withfever,hypertension,andanemia;incasesofbonemetastases,bonepainandlimpingarecommon.USexaminationrevealsawellcircumscribed,echogenicmassusuallycrossingthemidline,dislocatingthekidney;itisfrequentlycalcified,highlyvascular,surroundingandcompressingtheabdominalvessels.Inprogressivecasesliverandnodalmetastasescanbefound.Thetumorcanalsobesolid,homogenousandwithasmoothmargin.TheadrenalregioninnewbornsiswellvisualizeablewithUS,butatolderagesonlymajorlesionscanbedepicted.CT/MRIexamination:candepictalargesized,irregularshaped,extrarenalmass,withfrequentnecrosis,hemorrhageandcalcifications.Thelesionsshowaheterogeneouscontrastenhancement.Nuclearmedicineexamination:MIBGscintigraphyisbasicallya100%specificbutitssensitivityislower,becausenonMIBGuptakingtumorsexistaswell.
25.USexamination,longitudinalview.Abovetherightkidney,intheadrenalregionasolid,slightlyinhomogeneousmasscanbeseen.
Neuroblastoma.
26.MRIexamination,axialT2weightedimage.Irregular,largesolid,inhomogeneousretroperitonealtumorisseen.Neuroblastoma.(withthe
courtesyofDr.GborRudas)
Wilmstumor.Itisthemostcommonkidneytumorinchildhoodthatappearsbetween25yearsofage.Itisusuallyonlynotedwhenthetumorispalpableasanabdominalmass.Hematuria,hypertension,vomitingandabdominalpainarealsopartoftheclinicalpicture.USexaminationisabasicmethodinboththediagnosticsandthefollowupofthetumor.Thetumorisnormallyseenasahomogenousoraninhomogeneousmass,dislocatingthepyelonandthesurroundingretroperitonealbloodvessels.Itisimportanttoruleoutanylesionintheotherkidney.MRIexamination:givesapictureoftheentireabdomen,kidneysincluded.Nodalmetastases,tumorthrombusarewelldepictable.CTexamination:istobechosenifMRIisnotavailable.Thetumorshowsaninhomogeneouscontrastenhancementandpulmonarymetastases(invisibletoxrayexamination)arealsodepictable.
27.Asolid,echogenicmassarisingfromtherightkidney.Wilmstumor.AbdominalUS.
28.MRIexaminationaxial,T2weightedsequence.Asolidmassarisingfromtherightkidneyandfillingouttheright
29.CTexaminationafteriv.contrastadministration.Mostlyhypodensemassarisingfromtheleftkidney.
-
sideoftheabdomen,withperipheralfollicularcysticcomponents.Wilmstumor.(withthecourtesyofDr.
GborRudas)
Wilmstumor.(withthecourtesyofDr.Z.Kardi)
18.6.Centralnervoussystem(CNS)
Duetothevastnessofthisfield,inthissegmentwecanonlyconsidersomefundamentallydifferentdiagnosticmethodsandafewCNSdiseasestypicaltonewbornsandinfants.ThemostimportantdiagnosticmethodoftheCNSofinfantsandchildrenisMRI.(seethere)
18.6.1.Specialimagingmethodsofnewbornsandinfants
Cranialultrasonography:isthefirstmethodofchoiceinbrainparenchymaexaminations.Itcanonlybeperformeduntiltheclosureofthefontanelles(810months)(anteriorandposteriorfonatnelles,mastoidalandtemporalregion).Examinationsrequireahighfrequencyconvextransduceraswellasalinearone.Vertebralultrasound:canonlybeperformedinthefirst23monthsoflifeuntiltheclosureofthevertebralarch,withalineartransducer.
30.a. 30.b. 30.c. 30.d.
30.ad)Cranialultrasound.Normalnewbornbrain.ab.Coronal,cd.Sagittalviews.
USexaminationisalsocapableofdiagnosingandfollowingupcerebralcomplicationsofprematureinfantse.g.:germinalmatrixhemorrhage,periventricularleukomalacia(PVL),hydrocephalusandforthescreeningofcertaindevelopmentaldisorders(corpuscallosumagenesis,Galeniveinaneurysm,DandyWalkersyndrome).However,wehavetorememberthatUSisnotsensitivetoallabnormalitiesormoresophisticatedlesions.Metabolicdiseasesandsomehemorrhagesetc.arenotalwaysdetectablewithUS.ItisaveryusefulmethodbutitslimitationshavetobekeptinmindandwhennecessaryMRIistobeused.
31.NormalspinalUS,longitudinalview(longarrow:medullarcone,smallarrowvertebralbody.)Newborn.
32.USexamination,sagittalview.Radialpatternofthegyri.Corpuscallosumagenesis
33.a.USexamination,coronalview.Ontherighttemporallobeasmallechogenicarea
canbeseen.
33.b.MRI,axialview,diffusionsequence.Rightsided,3.5cmarea
withrestricteddiffusion.Acuteinfarctintheparietotemporalregion.(SE,
MRKK,withthecourtesyofdr.GyrgyVrallyai).
-
33ab.Cerebralinfarct,newborn.
18.6.2.Somediseasesofpreterminfants
Germinalmatrixhemorrhage.Itisahemorrhagetypicallyoccurringinprematureinfants.Thereare4stagesdistinguished(subependymalbleeding,ventricularhemorrhage,ventricularbleedingwithhydrocephalus,andthelatter+parenchymableeding).Hydrocephaluscanbeafrequentcomplicationaftergerminalmatrixhemorrhage,butatabouthalfofthecasesitresolvesspontaneously.USexaminationisamethodforitsdiagnosticsandalsoforitsfollowup.Periventricularleukomalacia(PVL).Itisusuallyabilateralporenchephaliccysticdiseaseintheperiventricularwhitematterthatdevelopsduetoischemicdamageinpreterminfants.
34.CranialUS,coronalview.Moderateventriculardilatationwithinhomogeneous
bleedingintheventralhornoftherightlateralventricle.GradeIII.hemorrhage.
35.CranialUS,coronalview.Theposteriorhornsaredilated,hemorrhageispresentinall
ventricles.Leftsidedperiventricularparenchymableeding.GradeIV.hemorrhage.
36.CranialUS,sagittalview.Dilatedventricle,periventricularcysts.PVI.
18.6.3.Maturenewborns
Hypoxicischemicencephalopathy(HIE).Hypoxicischemia,orperinatalasphyxiaisthemostcommoncauseforsevereneurologicabnormalitiesofthenewborns.Theroleofimagingistodeterminethegradeandextentofthedamageandtomonitorthedamagedlesionasearlyaspossible.Ultrasonography:insomecasesintheacutestagesofthediseasecanvisualizefocalordiffusehyperechogenicperiventricularorbasalganglialesions.Inchronicstagesperiventricularcysts,encephalopathy,hydrocephalusandwidenedsubarachnoidspacecanbedetected.MRIexaminationisthemostsensitivemethod,asitcandepictchangesundetectablebyUS.IntheacutestageMRspectroscopyisverysensitivetothedamagethatisindicatedbylactatepeakandadecreaseinothermetabolites.Diffusionweighedimagingisthemostsensitivewaytodetectcytotoxicedemarightaftertheischemicinsult.
18.6.4.DevelopmentaldisordersoftheCNS
Theyareamongstthemostcommondevelopmentaldisorders(1:100births).Thespectrumisbroad,coveringsmall,focalcorticaldysplasiaaswellascomplexsyndromes.Theearlydetectionofthesedevelopmentaldiseaseshelpsindeterminingthedegreeofthelesionandmighthelpinthetherapy,aswellasintheprognostics.Itplaysafundamentalroleintheplanningoffuturepregnancies.USexaminationisonlygoodforpartialdiagnostics;MRIisthebestchoiceforthedetectionofcorticalmalformations,migrationalanomaliesandmyelinationdisorders.
18.6.5.Supraandinfratentorialbraintumorsinchildren
Brainneoplasmsarethesecondmostcommontumorsinchildren,afterleukemia.Theirsymptomsdifferfromtheonesofadulthood,ononehandbecauseweencounterdifferenttypesoftumorsinchildrenandontheotherbecausethebonysuturesarestillnotclosedinthisagegroup.Braintumorsbelowtheageof2tendtobeprimarilysupratentorialinlocalization,whileinagesbetween2and10yearstheyaremostlyinfratentorial.Above10yearsofagethesupraandinfratentorialtumorratioisbasicallythesame.BeforebrainsurgeryMRIexaminationisperformedwithvarioussequencesandiv.contrastadministration,moreoverfunctionalMRIexamsmightbeusedascomplementarytechniquestohelpthecorrectdiagnosisandsurgicaldecisionmaking.Earlyphase(24hours)postoperativeMRIiscapabletoshowresidualtumors.USexaminationisoflimitedvalue,itcanbeusedinthefollowupofconsequentialhydrocephalus.
18.7.Musculoskeletalsystem
18.7.1.Diagnosticmethods(seethere)
18.7.2.Someimportantdisorders.
-
Osteomyelitis.Osteomyelitisstandsfortheinflammationoftheboneandthebonemarrow.Itsmostimportantsymptomsarefever,pain,erythema,swellingandelevatedinflammatorylabparameters.Innewbornsandpreterminfantsitisoftensymptomfreeandmultifocal.Earlydiagnosticsandtherapyareextremelycrucial,sincethedevelopingbonesmightsufferapermanentdamage.Under1yearofagetheepiandmetaphysisarerichinbloodvesselanastomosesthatprovideaspreadingroutefortheinflammationtowardstheepiphysisoreventothejointsortheadjacentbone.After1yearofagetheanastomoticconnectionsdisappearandthediseaseischaracteristicallymetaphyseal.Rarely,butprimarydiaphysealandepiphysealosteomyelitiscanalsooccur.Xray:doesnotshowanychangeswithinthefirst714days.Thefirstsignisfocal,unevenporosis.Infurtherstagessofttissueswelling,bonydestruction,osteolysis,bonenecrosiscanoccurandevenlater,sequestrationandperiostealreactiontakesplace.Radiologichealingtakesmonths.Ultrahasonography:detectsearlysignsbeforeXrayexaminationdoes.Itcanquicklydepictsofttissueedema,periostealreactionandsubperiostealfluids.Nuclearmedicine:offersamethodwitha90%andupsensitivityandspecificitytoosteomyelitis,howeverwithinthefirst6monthsoflifeisonlypartiallyreliableinthediagnostics.Itshowsacharacteristicactivityincreaseinall3stagesoftheexamination.MRI:candetectosteomyelitisinearlystages,andwithgreatreliability.Itsrateforidentificationandthedetectionoftheextentofthediseaseisbetween88100%.MRIisabletoprovideagoodpictureofthephysis,epiphysisandtherelationoftheinflammationtothejointaswell(edema,exudates,abscess).
37.a. 37.b. 37.c. 37.d.
37.ad)Xrayoftherighthumerus.a.Rarefactionintheproximalmedialpartofmetaphysisoftherighthumerusearlyosteomyelitis.b.Twoweeksafterthelyticareahasgrown.c.1monthlaterscleroticregenerationhasbegun.d.4monthsafteralmostcompletehealing.Osteomyelitis,infant.
38.US,longitudinal.Ontheproximalpartoftherightfemur,theperiostealsofttissueis
hypoechoic,theflowisincreased.Osteomyelitis
39.a. 39.b.
39.ab.MRI,T2weightedandT1weighted,postcontrastaxialimages.Signalintensityincreaseandincreasedcontrastenhancementinthebonemarrowoftheleftfemoralneck,.2yearsoldchild,osteomyelitis.(withthecourtesyofdr.GborRudas).
Transitorycoxitis.Itisatransitionalinflammatorydiseaseofthehipjointthatcausespainandlimping.Thepainismanytimeslocalizedelsewhere;onthelimbortheknee,leavinglimpingasanonlysymptom.USexamination:candepictsmallamountsoffluid.Eithera4mmwidefluidcollectionor2mmdifferencecomparedtotheotherlegareindicativeofinflammation.Thesynoviumisoftenthickened.
-
Rachitis.RachitiscanbecausedbyinsufficientvitaminDalimentation,adecreaseinmineraluptake(e.g.:prematureinfants)andvitaminDshortageduetomalabsorption(coeliakia,cysticfibrosis)oradisorderinvitaminDproductionprocess.Itsclinicalsymptomsareverycharacteristic:thewristisswollen,apalpablemassorstrainisoftenfoundontheanteriorachoftheribs,theskulliscompressiblelikeapingpongball.Xrayexamination:thetypicalsignsofrachitiscanalwaysbefoundinthetransitionalossificationzone.Onwristradiographthedistalmetaphysisoftheulnaandtheradiushaveanirregularcontour,theyarehollowed,thedistancebetweentheboneandtheepiphysealcoreiswidened.Rntgenfelvtel:acsipdysplasiaacsontosfemurfejmagjnakmegjelensigcsakindirektjelekbldiagnosztizlhat.
40.WristXray.Thedistanceofthewrist
bonesandradial/ulnarepiphysisiswidened,unevenandhollowed,atpartsthebone
densityisdecreased.Rachitis
41.USexamination,hip,longitudinalview.Thelefthipsarticularspaceiswidened,withecho
freefluidinit.Transitorycoxitis.
42.USexamination.Normalnewbornhip(arrow:hipbone.)
Hipdysplasia.Congenitalhipdysplasiaisamultifactorialdiseasethatoccursmoreingirls(1:9)andcausesthedislocationoftheheadofthefemur.Acetabularrimdevelopmentandconfigurationabnormalities,ligamentlooseness,musclecontracture,familyhistoryofhipdysplasia,orintrauterinebreechpositionhaveallbeenmentionedaspossiblefactorscausinghipdysplasia.USexaminationiscapabletodiagnoseinfanthipdysplasia.Itisindicatediftheclinicalexaminationraisessuspicionorifriskfactors(breechposition,twinpregnancy,familyhistory,oligohydramnion,deformedlimb,neuromusculardisease)persist.UScanbeusedasascreeningtool.Duetothephysiologicloosenessoftheligamentsbefore4weeksofagethehipisimmature,thereforescreeningexamshouldtakeplaceafter4weeksandcanbeperformeduntil46months.Xrayexam:canonlydetectindirectsignsofhipdysplasiauntiltheappearanceoftheossificationcentersofthefemoralhead.Batteredchild,childabuse,shakenbabysyndrome,nonaccidentalinjury.Theseareallsynonymsdescribingthesyndromeofchildabuse(usuallyofnewbornsandinfants).Atmanytimesonlytheradiologistcanidentifythesecases.Therearesomecharacteristicinjuriesthatarenotinrelationwiththestorytheparentstell.Fracturesofmultiplenumbers,orinvarioushealingstagesareindicativeofchildabuse.Complexskullfracturesarerareinsimplecasesoffalling.Themostcharacteristicsingsaremetaphysealorcornerfracturesonthemetaphisesofthetubularbones.Violentshakingcausesribfracturesandthetoandfromotionoftheheadleadstosubduralhematomas,hypoxiedematouscontusion.Xrayexamination:chest,bidirectionalskull,vertebralandlimbradiographsarenecessary.USexamination:bothcranialandabdominalUSareperformedininfants.CTexaminationcanberequirediftheabdominalorthevertebralinjuriesaresevere.MRIisunavoidableifneurologicsymptomspersist.
43.ComparisonRadiographoftheknees.Onthedistallateralepiphysisoftherightfemurcornerfractureisseen,lyticarea,periostealreaction.Bothproximaltibia,
onthevisiblepartofthepictureshowperiostealreaction.Batteredchild.
Summary
1.ALARAAsLowAsReasonablyAchievable,atermfortheuseofaslowradiationdoseaspossible.Itisafundamentalandprimarypointofviewinpediatric
-
radiology.2.DiseasesofthechestcanmostcommonlybediagnosedwithXray,andcomplementaryUSexaminations.CT/MRIisrarelynecessary.3.Airintheimagingofgastrointestinaldevelopmentaldiseasecanoftenbeusedasanegativecontrastmaterialonplainabdominalxrays,andissufficientfordiagnosis.4.TheinvestigationoftheGItractofthenewbornsiscarriedoutbylowosmolality,absorbablecontrastmaterials.USexaminationsareimportantpartofthediagnostictoolkit.5.US,mictioncystourethrography,nuclearmedicineandrarelyMRIareneededinthediagnosticsofurinarytractdisorders.6.CranialandvertebralUSexaminationshavesomelimitations,butareusefuldiagnosticmethodswhilethefontanellasandthevertebralarchareopen.IftheUSexaminationisnotsatisfactorytheCNSshouldbeexaminedwithMRI.