Embed Size (px)
Citation preview
Pediatric RadiologyCase Presentation
Ed. John Lilly, MD
Christopher Sears MSIV10/19/2018

▪ Baby girl born precipitously at 25+5 in OSH ED▪ APGARs 3/5/7 at 1/5/10 minutes
▪ Intubated at 8 minutes of life
▪ No antenatal steroids▪ 1 dose surfactant given atOSH▪ At UNC the UVC was replaced and a UAC wasplaced
▪ X-Ray was obtained to evaluate line placement

ETT at thoracic inlet
UAC atT9-T10
UVC at mid/upper RA
Diffuse, hazy opacities central > peripheral
UACCheckDOL 0

▪ s/p OGT placement on DOL #4; “was hard to pass” per NICUprovider note
▪ Physical exam reveals protuberant abdomen and absentbowel sounds
▪ Differential included sepsis vs obstruction vs NEC
▪ Abdominal X-Ray with subsequent LLD

Interval UVC retraction Interval UAC removal Enteric tube in place
No pneumatosisNo pneumoperitoneum
No portal venous gas
Triangular lucency/edge
Rounded lucency
Protuberant abdomen, diminished bowel sounds
DOL 5

Triangular and round lucencies in thoraxEnteric tube retroperitoneal?
Protuberant abdomen, diminished bowel sounds
DOL 5

▪ NICU team was concerned with enteric tube location and replaced it
▪ Abdominal X-Ray was obtained

Diffuse hazy right lung
Irregular lucencies
Triangular lucency
Obscured hemidiaphragm
New enteric tube
ReplacedOGTDOL 5
Replaced OGT
DOL 5

▪ Working differential: diaphragmatic hernia vs esophageal perforation
▪ Pediatric surgery was consulted
▪ Recommendations:
▪ Remove OGT
▪ Keep NPO
▪ Obtain UGI series to evaluate for perforation
▪ Patient was intubated in preparation for UGI series
▪ Chest/abdomen X-ray was obtained

Resolved medial lucency
Enteric tube
Lucency
IntubationDOL 6

Fluoroscopic Post-Procedure Overhead
Barium Swallow
DOL 7

Post-Barium Swallow
DOL 7

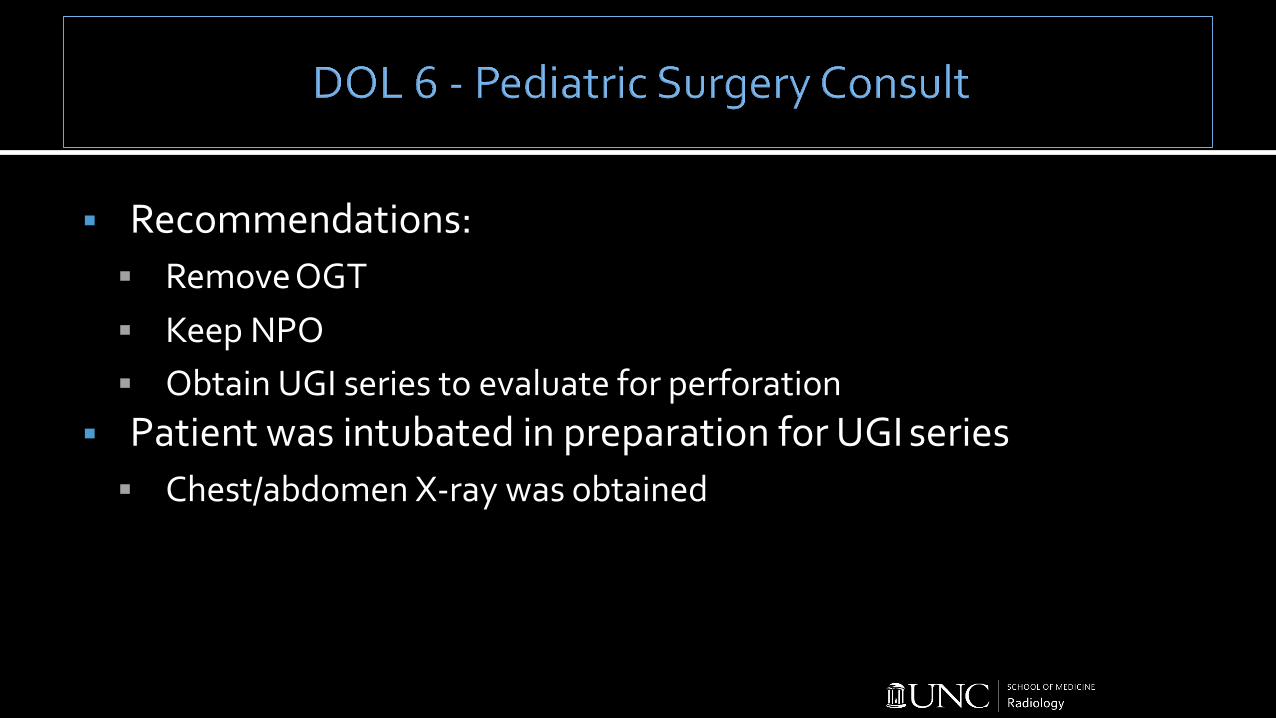
▪ NICU team places inferior PICC forTPN
▪ Chest/abdominal X-Ray was obtained
Malpositionedinferior PICC
Improved lucencies
PICC Placement
DOL 8

PICC
PICC Reposition
DOL 8

▪ “Difficult to pass” enteric tube with subsequent pneumothorax and apparent malposition of tube▪ Supports loculated pneumothorax due to esophageal/pharyngeal▪ perforation
▪ RDS patient on mechanical ventilation▪ Supports pneumothorax due to barotrauma

▪ Prevalence of misplaced enteric tubes reported 21-43.5% 1,2
▪ Perforation is a more rare, but serious complication
▪ Can perforate esophagus, stomach, bronchi
▪ Usually at pharyngoesophageal junction;
▪ lumen is narrowed by cricopharyngeus muscle3
▪ Can cause aspiration pneumonia, tension pneumothorax,▪ tension pneumoperitoneum
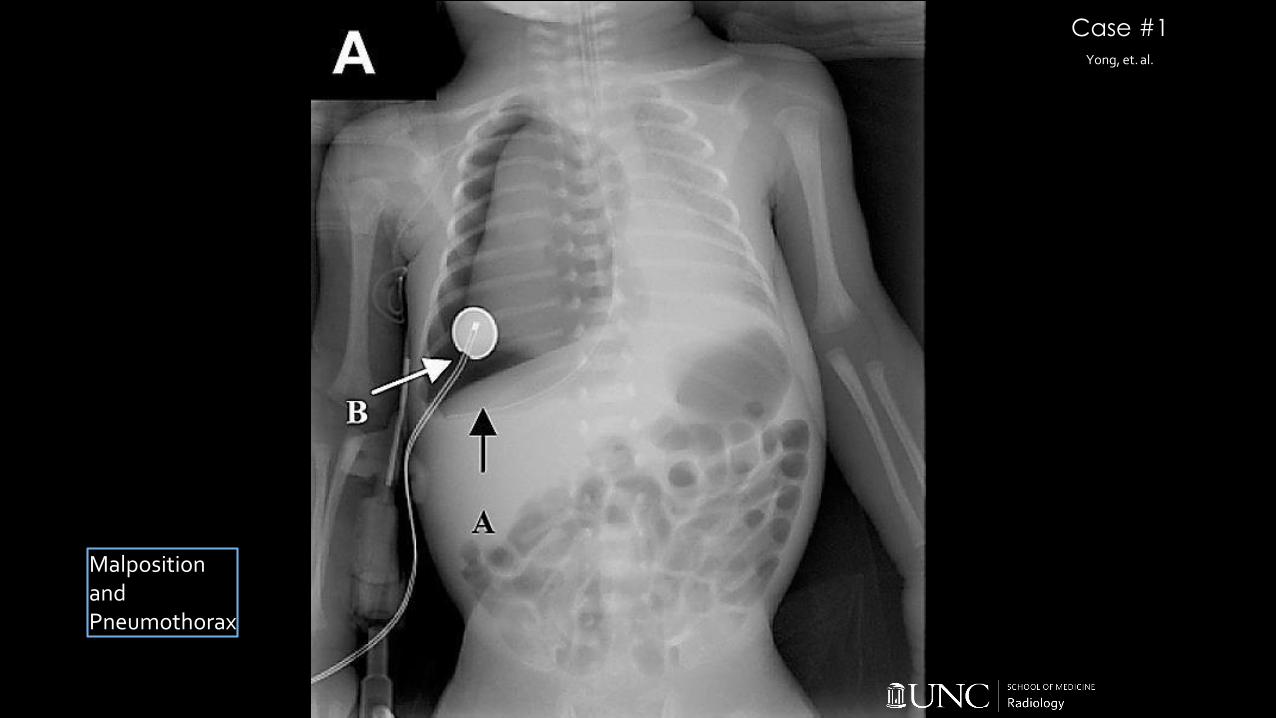
Yong, et. al.
Case #1
Malposition and Pneumothorax

Case #2Hosheh, et. al.
Malposition

Hosheh, et. al.
Case #2
Reposition
and Pneumothorax

Hosheh, et. al.
Case #2
Respiratory Distress hours later due to Pneumothorax

Case #3Lawther, et. al.
Gastric Perforation

▪ Have a low threshold to obtain imaging after placing any newtube or line, especially if clinical status deteriorates or clinicalassessment is equivocal

1. M. Farrington, S. Lang, L. Cullen, S. Stewart. Nasogastric tube placement verification in pediatric and neonatal patients. Pediatric Nursing 2009; 35:17-24.
2. N.A. Metheny, K.L. Meert, R.E. Clouse. Complications related to feeding tube placement. Current Opinions in Gastroenterology 2007; 23:178-182.
3. S.G. Emil. Neonatal esophageal perforation. Journal of Pediatric Surgery 2004; 39:1296-1298.4. Yong SB, Ma JS, Chen FS, Chung MY, Yang KD. Nasogastric tube placement and esophageal perforation
in extremely low birth weight infants. Pediatrics & Neonatology 2016; 57:427-430.5. Hosheh O, Mckechnie L. Rare and unexpected complications after a malpositioned nasogastric tube in
a neonate. BMJ Case Reports 2018.6. Lawther S, Patel R, Lall A. Neonatal gastric perforation with tension pneumo-peritoneum. Journal of
Pediatric Surgery Case Reports 2013; 1:14-16

▪ Respiratory Distress Syndrome
▪ Caused by surfactant deficiency
▪ Inversely correlated with gestational age
▪ 93% incidence in infants born <28 weeks7
▪ 0.3% incidence in infants born >38 weeks8
▪ Antenatal steroids, exogenous surfactant, and CPAP have improved disease course9
▪ Progressive respiratory failure shortly after birth in combination with▪ characteristic chest radiograph

Diffuse reticulogranular appearance
Low lung volumes(look for ETT)
Air bronchograms

▪ Caused by rupture of overdistended alveoli, most often in mechanically ventilated infants with lung disease
▪ Air is trapped in perivascular space
▪ Transient finding that often precedes pneumothorax unless▪ ventilator settings are changed
▪ High-frequency oscillation ventilation (HFOV)10
▪ Diagnosed via chest radiograph - can be unilateral or bilateral
▪ Ipsilateral bronchial occlusion11

Seen peripherally AND
centrally
Hyperinflation
Mediastinal Shift
Coarsenon-branching linear
ORcystic lucencies

▪ Air in the space between the parietal and visceral pleura
▪ High level of suspicion in mechanically ventilated infant withworsening cardiopulmonary function
▪ Can be asymptomatic if small
▪ Large pneumothoraces are easily seen on supine chest radiograph
▪ Smaller pneumothoraces benefit from lateral decubitus imaging

Atelectasis and flattening of the diaphragmMediastinal shift Air between visceral and parietal pleura

7. Stoll BJ, Hansen NI, Bell EF, et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 2010; 126:443.
8. Consortium on Safe Labor, Hibbard JU,Wilkins I, et al. Respiratory morbidity in late preterm births. JAMA 2010;304:419.
9. Sakonidou S, Dhaliwal J. The management of neonatal respiratory distress syndrome in preterm infants (European Consensus Guidelines--2013 update). Arch Dis Child Educ Pract Ed 2015; 100:257.
10. Gaylord MS, Quissell BJ, Lair ME. High-frequency ventilation in the treatment of infants weighing less than 1,500 grams with pulmonary interstitial emphysema: a pilot study. Pediatrics 1987; 79:915.
11. Rastogi S, Gupta A, Wung JT, Berdon WE. Treatment of giant pulmonary interstitial emphysema by ipsilateral bronchial occlusion with a Swan-Ganz catheter. Pediatr Radiol 2007; 37:1130.