-
EDUCATIONAL OBJECTIVES
66. Appropriate knowledge of theimmediate management of the
in-fant with hypertonic dehydration(81/82).67. Appropriate
knowledge of theimmediate management of hypo-natremic dehydration
(81/82).68. Appropriate familiarity withmanagement of maintenance
fluidand electrolyte administration forthe pediatric patient
(81/82).
#{149}Montefiore Hospital and Medical Center,Bronx, New
York.
pediatrics in review vol. 3 no. 4 october 1981 PIR 113
Treatment of Dehydration in InfancyLaurence Finberg, MD*
NORMAL CHEMICAL ANATOMYAND PHYSIOLOGY
Before discussing dehydration itis worthwhile to review the
normalfeatures of an infant with respect tocontent and distribution
of water andmineral. Approximately 70% of thelean body mass is
water. The distri-bution of this water is shown in Fig1 . The
plasma volume owes its integ-rity to its protein content, which is
arelatively impermeable species ofmolecule. The extracellular
fluidcomposition differs strikingly fromthe intracellular fluid
despite themovement of most ions across cellmembranes because of an
activetransport system (N&, K, ATPase)in the membrane that
extrudes so-dium. The compositional differencesare diagrammed in
Fig 2.
The second consideration neces-sary to handle any problem is
that ofobligatory water requirements to re-place losses. Table 1
gives the re-lationship between caloric expendi-ture and water loss
with the basalstate as the point of reference. Forordinary clinical
circumstances re-quirements are about 11/2 timesbasal state.
Electrolyte requirementshave a wide range. Practical
consid-erations make it necessary to pro-vide solute in an
intravenous solu-tion, when one is needed, to preventhemolysis. All
conditions may be metby allowing 2 to 3 mEq/kg/day ofboth sodium
and potassium. Chlo-ride and bicarbonate (or other base)ions for
the healthy infant awaitingsurgery, for example, should be di-vided
about 3:1. In disease statesappropriate modification may
bemade.
In this brief presentation the treat-ment plans are developed
aroundparenteral therapy. In many situa-tions, eg, diarrheal
disease, oralfluid will be equally satisfactory if thepatient is
able to drink. The readershould be able to adapt the princi-ples to
an oral route of administra-tion whenever it is appropriate.
Here
we have assumed severe dehydra-tion that requires at least
initial par-enteral repair.
CLINICAL EVALUATION OFDEHYDRATION
Dehydration regardless of the eti-ologic factors that produce it
is aphysiologic disturbance of clinicalimportance. Proper
assessment willlead to appropriate therapy whentreatment is
required. In any clinicalevaluation, the tools are the
clinicalhistory, the examination of the pa-tient, and a review of
laboratorydata. Then should come a sys-tematic analysis of the
problem thatresults in a diagnosis of the physio-logic disturbance
and suggests thenature of therapeutic intervention, ifany.
In obtaining the history, a numberof points need special
stress.Clearly, these are the things thatbear upon the intake of
fluid andmineral and on unusual losses ofthese. When it is possible
to obtainfrom the history a recent weight ofthe patient, this
information mayprove useful as a benchmark. Thepresence of fever,
level and durationif possible, is clearly important. Adescription
of the patients environ-ment in regard to temperature andhumidity
should be at least approxi-mated. Any evidence of infection,local
or systemic, is also of impor-tance because of the influence
ofinfection on catabolism as well asthe implications of an
infection forphysiologic change.
Intensive questioning should becentered on the site of fluid
loss andon the type and amount of loss.Since most fluid losses are
from thegastrointestinal tract, this is usuallythe focus but it
should be pointedout that fluid loss can occur into atissue or
through the urine as well.
The symptoms of anorexia andvomiting are of special importancein
infancy because a high oral intakeof liquid is essential to life
proc-esses, especially during a catabolicstate. Indeed, the advent
of vomitingin an infant with diarrhea is whatusually precipitates
admission to the
hospital since under most circum-stances this symptom ends the
abil-ity of the family to care for the baby.
In examining an infant for dehy-dration, the most important
singledetermination is the patients weight.This measurement should
always beobtained with great care and preci-sion. If the patient is
lethargic, it isimportant also to determine whetherirritability is
present both withoutstimulus and when such stimuli assound, light,
and touch are applied.Unusual body movements or convul-sive
twitchings should be noted, andone should ascertain whether
thereare tears.
The skin provides many clues tothe state of hydration. This is
partic-ularly true in infancy up to the ages1 to 2 years. In older
children, ex-amination of the skin is less usefulin determining the
state of hydration.Two signs of special importance arechanges in
elasticity and in turgor.When the abdominal skin in normalinfants
is pinched, it will snap backpromptly on release. When dehydra-tion
has progressed to a seriouspoint, pinched skin will remainstanding
in folds because elasticityhas been lost. This sign may also
beseen, however, in serious under-nu-trition without dehydration.
The na-ture of the subcutaneous tissue isdifferent in older
children and adults,and this loss of elasticity will not beelicited
when they are dehydrated.The presence of turgor is a sign
ofcirculatory adequacy. One exam-
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
mOsm/Kg ECF I ICF
HC0328
t:I3 - PLASMA6%LBM LUNGS-ECF----1----- IKIDNEY
INTERSTITIALFLUID19%LBM SKI
11
ICE45% LBM
TRANSCELLULAR*ATER I%LBM
NON-AQUEOUSTISSUE 28% LBM :
LEANBODYMASS(FATFREE)OFINFANT
+
47
CLIT
F-.-- No-
Na-KATPase
-.- KK kA)
(54 PROTEIN
AINTRACELLULARFLUID - MUSCLE
PLASMA
K 4 ._j_. H2P04Co 3 4 S04Mg __i__ R
INTERSTITIALFLUID
Fig 2. Ionic profiles of body fluids. Composition of the three
physiologically importantcompartments is shown with separating
barrier indicated. Concentrations (mEq/liter) areshown and left
hand scale (mOsm/kg) emphasizes nonidentity of these measures
except forunivalent unbound ions. Shaded areas indicate low or
absent osmotic activity because of largemolecule size or because of
binding of ion to large molecule. Protein and amino acids
haveimportant osmolal contribution, even in low concentration
because of relative impermeability.ECF, Extracellular fluid; ICF,
intracellular fluid.
TABLE 1 . Basal Caloric Expenditure for Infants and Children
A geWeight
(kg)Surface Area
(sq m)Calories
(/kg)Newborn 2.5-4 0.2-0.23 501 wk to 6 mo 3-8 0.2-0.35
65-706tol2mo 8-12 0.35-0.45 50-6012 to 24 mo 10-15 0.45-0.55 45-502
to 5 yr 1 5-20 0.6-0.7 456toloyr 20-35 0.7-1.1 40-4511 to 15 yr
35-60 1.5-1.7 25-40Adult 70 1 .75 15-20
* Water expenditure equals 1 mI/calorie.
Fluids and Electrolytes
PIR 1 1 4 pediatrics in review #{149} vol. 3 no. 4 october
1981
-ALIMENTARYTRACTTC*#{149}l%LBM
I
Fig 1. Diagram of normal distribution ofbody water in lean body
mass (LBM). Adiposetissue is not associated with significant
water.Arrows indicate flows of water and ions.Transcellular water
(TCW) includes waterwithin intestines (out of scale on diagram,
butpotentially much greater than normal). OtherTcw is water
sequestered tightly in tissuesand not rapidly involved in acute
bodychanges. ECF, Extracellular fluid; ICF, intra-cellular
fluid.
ines for it by pinching the skin andsqueezing out the blood from
thepinched area and thereby causing acolor change. In the healthy
patient,the color returns almost instantane-ously upon release.
Slowness in thereturn of color denotes a loss ofturgor. Very slow
return in the ab-sence of a local skin problem (oredema) indicates
shock.
Pulse rate and pressure are mostimportant determinations
sincetachycardia is the first manifestation
of dehydration. The examination ofthe muscle tone including
checkingfor nuchal rigidity and testing thedeep tendon reflexes is
a helpfulassessment as will be discussed be-low. Auscultation of
the heart andlungs gives information on the qual-ity of the heart
sounds and confirmsobservations with respect to the rateand depth
of breathing.
Routine laboratory studies in de-hydration should include a
hemato-crit and a urinalysis. In addition to
these routine studies, in a dehy-drated patient blood should
bedrawn for analysis (as a minimum) ofthe urea nitrogen level and
the elec-trolytes (sodium, potassium, chlo-ride, and bicarbonate).
If a more ex-tensive analysis is desired, bloodgases plus calcium,
phosphorus,magnesium, glucose, and albuminshould be measured. Most
patientsdo not require such an extensivework-up. For complicated or
unusualcases, however, such studies canbe quite valuable.
Having obtained the data basefrom history, examination, and
pre-liminary laboratory data, the nextstep is a systematic analysis
of fivecardinal clinical points. Each shouldbe reviewed in
assessing the pa-tients status although in the mostseverely ill
patients, one may initiallyhave to forgo laboratory
informationaltogether because of the urgencyof the patients
condition. The fiveclinical points are: (1) volume, (2)osmolality,
(3) hydrogen ion status,(4) intracellular ions, and (5)
skeletal
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
DEHYDRATION
pediatrics in review vol. 3 no. 4 october 1981 PLR 115
ions. Each of these will be discussedin detail enabling the
physician todefine the degree of dehydration,the distortion of body
water distri-bution, and the metabolic disturb-ances arising from
effects upon hy-drogen, potassium, and calciumions. The first two
points of assess-ment are more important than thelast three if the
patient has poten-tially adequate renal and pulmonaryfunction. The
homeostatic mecha-nisms of kidneys and lungs will cor-rect the
metabolic disturbances ifthe volume and space disturbancesare
quickly and appropriately cor-rected. Patients with impaired
renalor pulmonary function will requirecareful attention to all
five points ofassessment.
When going through these as-sessments, one should
determinewhether an emergency state exists.The dehydration may be
classifiedinto hypernatremic, isonatremic, orhyponatremic states.
Finally, themetabolic disturbances includingthose of hydrogen ion
should beevaluated.
1. Volume
The therapist has three consider-ations with respect to volume.
Thefirst of these is to assess the degreeof deficit. This, of
course, is achange in composition and can beexpressed as in
milliliters per kilo-gram of body weight or as a per-centage of
weight loss. In jargon,this is often designated as 5% or10%
dehydration, by which ismeant 5% or 10% body weight loss.The least
objectively detectable def-icit is approximately 50 mI/kg (5%acute
weight loss). Elevated pulserate and diminished pulse
pressure,diminution of output of tears andurine, may be the only
manifesta-tions. When a deficit of approxi-mately 100 mI/kg exists,
a constel-lation of clinical signs is usually pres-ent. These
include depressed fon-tanelle in infants and sunken eye-balls in
patients at any age, loss ofelasticity and of turgor of the
skin,and other evidences of circulatorydeficit which include
coolness andacrocyanosis or mottling of the skinof the extremities,
feeble hearttones, and a weak, rapid pulse. The
brachial blood pressure is usuallymaintained. At this point the
patientis in medical shock from the loss ofextracellular fluid.
Between theabove two landmarks, one can inter-polate-but not with
precision-in-termediate degrees of deficit. Whenthe deficit over a
short period of timeapproaches 1 5% of the body weight,blood
pressure drops and a mori-bund state ensues.
The basis for estimating the vol-ume of deficit has been the
dehy-drated weight rather than calculatingthe hydrated weight and
using it.This error is compensated for inthe clinical calculations
by also ig-noring the water of oxidation pro-duced by the patient
in each timeperiod, an error in the opposite di-rection. The net
result of these twoomissions is that they cancel oneanother for
most patients when ther-apy is for a short time period-a dayor
two.
The volume of fluid estimated asthe deficit should be thought of
asprimarily deficit from extracellularfluid. Therefore, it is a
fluid with asodium concentration of about 150mEq/liter, chloride 1
1 5-1 20 mEq/liter, and bicarbonate or other baseof 25 to 30
mEq/liter. After consid-ering the next several analysispoints,
these estimates may be mod-ified.
While assessing the deficit it isalso appropriate to consider
the vol-ume needs of the patient to replaceongoing obligatory
losses. This fluidvolume assessment is sometimes re-ferred to as
maintenance fluid. Oneassesses the metabolic state of thepatient to
estimate these ongoinglosses. At basal conditions there isan age-
or size-dependent caloricexpenditure which in turn deter-mines
water expenditure. Deviationsfrom the basal state include
bodytemperature changes, ventilationchanges, and changes from
muscu-lar movement. At average clinicalconditions of normal body
tempera-ture ( 1 C) a slight increase in ven-tilation and with
normal movement inbed, the caloric and water expendi-ture are about
1#{189}times the basalamount. On an experimental basisrather
precise increments for any ofthe abnormalities described can
bedefined, but this is not practical din-
ically nor does it prove to be evenadvisable to attempt such
detailedcalculation. A margin of safety of10% has proven clinically
safe;this makes meticulous precision un-necessary. A marked
increase inany one of the three important van-ables will move the
ongoing obliga-tony losses to approximately doublebasal state.
Should all three be in-creased, that is, high fever,
hypen-ventilation , and continued convul-sive movements, the effect
would beto triple the basal expenditure. Fromthese guideposts,
reasonable esti-mates may be readily made by theclinician. The
water estimates hereare free of electrolyte. Table 1 givesbasal
energy expenditure data forinfants.
A final concern with respect tovolume is related to continued
ab-normal losses. In a few diseases,such as Asiatic cholera, these
canbe estimated from empirical data,but for most of the etiologies
causingdiannheal disease on other problems,the abnormal losses will
have to beascertained by continuing direct ob-servation of the
patient.
2. Osmolality
The term as used here is a one-word shorthand way of saying
thatwhats being assessed is a disturb-ance of the distribution of
water inthe body spaces. The principal em-phasis at this point in
the analysis isto determine whether the patient is:hyponatnemic,
with a relative pre-pondenance of water in the cells atthe expense
of extracellular fluid;isonatnemic with a proportionateconstriction
of body fluids; on hypen-natremic, with relative cellular
des-sication, the displaced water beingfound in the extracellular
space.
The history is helpful in makingthese distinctions. If purging
hasprogressed for a number of days,sodium losses will be high,
particu-larly if no sodium intake has oc-curred during this period.
In fact, ifrelatively mineral-free water hasbeen offered by any
route, a hypo-natnemic state will result. If the pa-tient has
maifltained regular food in-take followed by an abrupt cessationof
intake with on without vomiting,then water losses will tend to
pre-
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
* Associated history and signs encountered with differing
physiologic disturbances when 100 mI/kg rapid weight losthas
occurred secondary to diarrheal disease. These cumulative
descriptions are clinically probable stereotypes;exceptions may be
seen though usually a cluster of these findings will prove an
accurate predictor. No one attribute orsign is specific; moreover,
the disease process may change the disturbance from one part of the
illness to another asmay partial therapy. The manifestations listed
may be either the cause of or the result of the physiologic
disturbance.
Fluids and Electrolytes
PIR 1 1 6 pediatrics in review #{149} vol. 3 no. 4 october
1981
TABLE 2. Clinical P rofiles of Physiologic Distu rbances in
Dehydration*
CharacteristicsOsmolal State
Isonatremic Hyponatremic HypernatremicAge Any Any Often under 1
yr of age (any pos-
sible)Time of year Any Any, more in summer Most in winter
months, especially
when humidity is very low insideFever and other Variable
Variable, minimal nespina- High grade fever common; respi-
evidences of in- tory involvement usual ratory symptoms common
withfectious etiology increased ventilatory rate
Anorexia Late in course of ill-ness
Minimal, good oral intakeof wated maintained
Marked early in illness
Vomiting Late manifestation Late or absent Early, may be coffee
groundDiarrhea Moderate through-
outLong duration (3 or more
days)Variable
State of con- Normal May be obtunded Disturbedsciousness
Lethargy Variable Common Usual and markedHypenirnitability
Unusual Unusual Marked to tactile, sound, and light
stimuliMuscle tone Normal Normal or weak Increased; nuchal
stiffness some-
times present; muscle twitch-occasionally seen
Skin elasticity Poor Very poor Normal; skin may have a velvetyor
uncommonly a doughyfeel
Skin turgor Diminished Poor GoodPulse rate Increased beyond
that caused byfever
Markedly increased Lroportionate to fever
Blood pressure Maintained orslightly low
Reduced, borderline ofcirculatory failure
Normal
Hyperpnea Variable Often, but variable Variable, sometimes
marked andcontributory to water loss
dominate and hypennatnemia will ne-suIt. The presence of any
factor thatpredisposes to insensible waterloss, high ambient
temperature, lowhumidity, fever-especially high fe-yen, and
hyperventilation all predis-pose to hypernatremia.
On examination deficient circula-tion points to loss of
extracellularfluid. If the circulation is not severelyimpaired but
there are signs refera-ble to the nervous system, particu-larly the
identifiable combination oflethargy unstimulated and
hypenirnit-ability to virtually any stimulus, a hy-pernatremic
state should be sus-pected. Hypernatremic patients, in-stead of
losing dermal elasticity inthe usual fashion, often have adoughy
feel to their abdominal skin.
Even more commonly the skin willhave a somewhat velvety feel
whichwe have found more reliable as anindicator of hypernatremia
than themore traditionally described doughyfeeling. In
hypernatremic states,there will be increased muscle toneoften
including mild nuchal rigiditywhich is occasionally mistaken forthe
nuchal rigidity of meningitis.
The definitive measurement forthis assessment is the level of
so-dium in the serum. This is a bettermeasurement than the
osmolalityper se because some substancesthat affect osmolality, eg,
urea, donot influence body water distribu-tion.
This assessment point permits as-signment of a sodium
concentration
to the deficit portion of the repairsolution. For most patients,
thosewith isonatnemic dehydration, thiswill be 1 40 to 1 55
mEq/Iiter. Moresodium should be given if hyponatre-mia is diagnosed
and less if hyper-natremia is present. Table 2 listsclinical
associations frequentlylinked to different osmolan disturb-ances,
whether as a cause, or aresult or even both.
3. Hydrogen Ion Disturbance
The history is helpful in detectinghydrogen ion disturbance. In
infancyunless there has been vomiting withhigh obstruction, almost
all disturb-ances produce acidosis and thenacidemia. Diarrhea is
particularly
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
DEHYDRATION
pediatrics in review vol. 3 no. 4 october 1981 PIR 117
prone to cause this type of disturb-ance. The degree of acidosis
or aci-demia is not easily gauged withoutlaboratory data. Hyperpnea
is evi-dence of a compensatory phenom-ena and suggests acidosis.
Thepresence of ketones in the urine issimilarly helpful. It should
be remem-bered, however, that this latter lab-oratory change does
not appear ininfants less than the age of 5 monthsfrom either
starvation, or dehydra-tion, or both. Ketonunia in infantsless than
5 months old usually is asign of metabolic disease such asdiabetes
or one of the aminoacido-pathies.
Measurement of the bicarbonateion or the complete blood gas
bat-tery gives quantitative dimensions tothis disturbance. Although
therapycould and sometimes should takehydrogen ion disturbance into
ad-count, it should be remembered thatadequate attention to volume
andcorrection of maldistnibution of waterwill usually enable the
kidney andlung to do this task quite satisfacto-rily. During
therapy the ions selectedshould either be chosen to be
slowlycorrective or at least not to worsenthe disturbance. Remember
the nor-mal pH of plasma and extracellularfluid is alkaline not
neutral; there-fore, some base is usually properlyincluded even in
maintenance so-lution.
4. Intracellular Ion Losses
Whereas intracellular ion lossesinclude potassium, magnesium,
andphosphate, from a clearly clinicalpoint of view it is usually
only thepotassium loss that is important.Whenever there are losses
of gas-trointestinal secretions, significantpotassium losses are
likely to occur.The extent of these losses is knownfrom empirical
data rather than fromany easy method of either estimatingor
measuring with the current clini-cal laboratory. When the patient
hashad longstanding diarrhea or vomit-ing, the potassium losses
will belarge. If there has been polyunia, po-tassium losses will be
predictablylarge as well. Measurement of potas-sium level in the
serum may be de-ceptive because any diminution inthe glomerular
filtration will cause
the potassium level to rise evenwhen the total body potassium
islow. A high bicarbonate and a lowchloride level in serum suggest
po-tassium deficit. This is true in relativeas well as absolute
terms so that theexperienced clinician is occasionallygiven a clue
by what seems an in-appropriate ratio of bicarbonate tochloride.
The electrocardiogram un-fortunately reflects only the
extra-cellular value of potassium and soadds no quantitative
information.Phosphate and magnesium levelsare only occasionally of
clinical im-portance in states of dehydration.
The important clinical principle isthat potassium must be
provided toreplace tissue losses from diseaseand losses produced by
the antici-pated high urine output during then-apy.
5. Skeletal Ions
Although phosphate and magne-sium may be included here as
well,it is really the calcium ion that is ofimportance. Infants in
the first weekor two of life frequently have im-paired calcium
homeostasis so thatsuperimposed dehydration may tipthem to
hypocalcemia. Hyperna-tremic states frequently producemild
hypocalcemia; uncommonlythey may produce significant hypo-calcemia.
Other factors that may dothis include high phosphate levels(often
because of renal insuffi-ciency) and alkalemia, which is un-usual.
Relative alkalemia, however,can be produced by treatment ofacidemia
or acidosis, and rapid hy-dration may also produce a
dilutionalstate. Either of these may predis-pose to hypocalcemia
though notcommonly. In summary, the neonatalperiod and
hypernatremic states arethe factors of most importance
indisturbances of calcium ion duringdehydration.
IMPLEMENTATION INISONATREMIC ANDHYPONATREMIC DEHYDRATION
The clinical analyses just reviewedenables one to know both
qualita-tively and quantitatively the amountof fluid required for
repair and forother needs during an ensuing time
which will arbitrarily be one day. Be-fore implementation this
informationmust be translated into a plan for therate of
administration and for decid-ing whether each of the componentsis
to be spread over the day orwhether there are times for
specialemphasis for a given element of then-apy. Therapy in the
first 24 hours inpatients with either isotonic constnic-tion of
body fluids (isonatremia) orthose requiring slight
modificationbecause of a hyponatremic state willbe considered
here.
It is useful to divide therapy intophases, each with its own
time seg-ment within the 24 hours. The daymay be divided into three
segments:emergency, repletion, and early re-covery. When water is
lost from thebody through the gastrointestinaltract, the loss
ultimately involves allof the body compartments to somedegree. It
follows then that watergiven during treatment must wind upin the
various body compartmentsas well.
The emergency phase, then, hasas its emphasis replacement
ofplasma volume. Most of the waterloss in isonatremic dehydration
isfrom the extracellular fluid. Asidefrom the plasma, the other
compo-nent of this water is the interstitialfluid which serves as
the transportmedium for virtually all substancesactive in bodily
functions. This spaceneeds early repletion, the secondphase, so
that metabolic processesmay proceed normally. Finally, wa-ten and
salts from cells, intracellularfluid, will need replacement to
en-sure proper cellular function. Thethree body spaces indicated
thenroughly correspond to the emphasisplaced during each of the
threephases of therapy.
First, from the clinical assessmentscheme, the volume of fluid
neededto repair the deficit may be estimatedas the amount required
to recoverobligatory ongoing losses. Empiricaldata have indicated
that it is appro-priate to give this combined volumeof fluid to the
usual dehydrated pa-tient within the first 24 hours. Thusthere is a
tentative volume to use inplanning therapy to which may beadded any
continuing abnormallosses. From the earlier considera-tion of the
pathogenesis of dehydna-
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
Fluids and Electrolytes
PIR 118 pediatrics in review #{149} vol. 3 no. 4 october
1981
tion it is also known how much so-dium to give during the first
day anda qualitative concept of the amountof base and of potassium
and cal-cium. It remains now to quantitatespecifically each ofthe
elements andto divide up the administration in theseveral
phases.
Emergency
An emergency phase is to be im-plemented only if there is
significantcirculatory deficit. If such is not pres-ent, the
emergency phase is repne-sented only by a more rapid rate ofinitial
infusion during the repletionphase on it may even be omittedwhen no
circulatory manifestationsof any sort are detectable; eg,
notachycardia. The emphasis for theemergency phase is restoration
ofthe plasma volume. The simplestway to do this is to infuse a
fluid thatcontains either protein on other sub-stances that will
have the same on-cotic properties as plasma albumin.Thus, single
donor plasma on a so-lution of 5% albumin or any otheranalogous
fluid is ideal. The volumeof water in this infusion will, at
leastfor an appreciable ieniod of time,remain intravascular and
accom-plish the intended goal. Empirically,it was learned long ago
that one caninfuse 20 mI/kg of plasma on 5%albumin to a dehydrated
patientwithout risk of clinical consequencefrom overexpansion of
the plasmavolume. This then has become onestandard way to implement
theemergency phase. Subsequently, itwas learned that one may also
useaqueous solutions for this purposeand avoid the expense and
hazardsof protein solutions, yet accomplish-ing the desired goal.
In neonates andmalnourished infants, the albuminsolutions are
preferred for the emer-gency phase as well as for hypen-natremic
patients in shock.
In other patients aqueous solu-tions prove to be equally
satisfactoryduring the emergency phase, but thevolume given must be
greater toachieve a similar effect on plasmavolume-theoretically
four times asmuch. When an aqueous solution isto be used, different
authorities haverecommended various solutions. Iprefer the use of
solutions contain-
ing glucose to Ringers lactate so-lution though both have been
usedsuccessfully. In fact, even when us-ing albumin solutions I
immediatelyfollow administration of that solutionwith 10% glucose
in water, 20 ml/kg, also very rapidly. These two in-fusions
together can usually be ad-complished within one hour, a totalof 40
mI/kg, a volume which is thensubtracted from the proposed totaldays
volume to ascertain how muchmore is needed. If an aqueous solu-tion
alone is to be given initially, a10% glucose solution to which
isadded 75 mEq/Iiter of sodium, 55mEq/Iiten of chloride, and 20
mEq/liter of bicarbonate (on other base) isrecommended. This
solution, 40 mI/kg, is administered over approxi-mately the same
one-hour interval.Either of these alternatives consti-tutes the
emergency phase.
Those who use Ringers lactate or0.9% sodium chloride (so-called
normal on physiologic saline)recommend 40 to 50 mI/kg again
inapproximately one hour. I prefer hy-pentonic glucose to be used
becausethis substance not only providessubstrate for the nutrition
of starvingcells but also temporarily pulls ad-ditional water to
the extracellulanfluid, even into the vascular fluid,and thus
initiates urine formation abit more rapidly.
In assigning the emergency fluid,either to the deficit or
maintenanceportion of the allotment, the task isobvious. Simple
plasma on albuminsolutions contain sodium and there-fore should be
assigned to the deficitfraction. Glucose water without so-dium
belongs to the estimated main-tenance portion. A solution with
75mEq/Iiten of sodium is half deficitand half maintenance. If one
were touse Ringers lactate on 0.9% salineall of it should be
assigned to thedeficit fraction.
Repletion
The duration of the repletionphase, together with the
emergencyphase if any, should be one third ofa day on eight hours.
The emphasisfor this phase is restoration of theinterstitial fluid.
The volume to begiven is such that 50% of the tenta-tively assigned
days volume will be
administered within eight hours.During this phase there is no
pointin using 1 0% glucose, but rather 5%glucose which serves well
as thestock solution. The sodium contentis adjusted according to
the esti-mated sodium need and can rangein concentration from 40 to
80 mEq/liter. Assuming that urine formationhas become clinically
visible it istime to add panenteral potassium. Asafe concentration
that will preventthe clinical effects of potassium de-pletion is 20
mEq/Iiten. Chloride ionand base may be distributed accord-ing to
the clinical assessment of thehydrogen ion status of the
patient.
Early Recovery
The emphasis in this phase is re-placement of the intracellular
fluid.The rate can be slowed and thephase lasts for the remaining
twothirds of the day or 1 6 hours. Thecomposition fluid is similar
to onidentical with that of the precedingphase. Table 3 shows the
foregoingtherapeutic implementation for a pa-tient who is presumed
to have a def-icit of 1 00 mI/kg (1 0% of bodyweight) with an
isotonic dehydrationand who requires an emergencyphase. An oral
glucose-electrolytesolution may be substituted at thispoint for any
patient who can acceptit.
THERAPEUTIC MANAGEMENTFOR HYPERNATREMICDEHYDRATION
Because the pathophysiology ofhypennatnemia has distinct
featuresseparating this form of dehydrationfrom the more common
varieties, theprinciples of therapy must accom-modate the
differences. Mild hypo-calcemia occurs in approximately20% of
patients. Hyperglycemia, oc-casionally severe, also occurs
inperhaps one third of patients. Theplan of therapy must consider
thesedisturbances.
Restoration of hydration follows adifferent path when moderate
hyper-natremia is present. The objective oftreatment is to replace
fluid volume,to restore water distribution, and toconnect the
complicating disturb-ances. At first glance therapy seems
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
TABLE 3. Scheme for First 24 Hours of Rehydration for Isotonic
Dehydration of an lnfant*Period 1 Period 2 Period 3 Total
Phase Emergency Repletion Early RecoveryDuration #{189}-ihr 6-7
hr 16 to 18 hours 24 hoursEmphasis for res- Plasma volume
Extracellulan fluid Intracellular fluid All compartments
tonationFluid composi- A. Plasma or 5% albu- 5% glucose with Na
5% glucose with Na Na 9 mEq/kg, K 3
tiont mm + 10% glu-cose
B. 1 0% glucose withNa 75, C1 55,HCO3 20 mEq/li-ten
40, K 20, C1 40,and base 20mEq/liter
40, K 20, C1 40to 45, and base1 5 to 20 mEq/Iiter
mEq/kg, Cl 8.5mEq/kg
Amount (mI/kg A. 20 mI/kg of each 60 mI/kg 1 00 mI/kg plus any
200 mI/kgof body solution totaling 40 additional abnormalweight)f
mI/kg
B. 40 mI/kglosses
* Estimated deficit = 1 0% of weight(i 00 mI/kg). Estimated
ongoing losses = 1 00 mI/kg.t Use either plan A or B in period
1.
mm H2O
150
140
130
#{149}120
20 mI/kg
90 Ijb 2OI J I I I I J
40 60 80 100 120TIME IN MINUTES
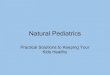
:1_g 3 Effect on CSFpressure ofarapid intravenous infusion of 5%
glucose in water, 20 ml!
kg. Same pressure increase will occur at any base line
CSFpressure. This phenomenon, whensymptomatic, is called water
intoxication.
DEHYDRATION
pediatrics in review vol. 3 no. 4 october 1 981 PIR 119
to be the simple replacement of wa-ten. In fact, careful
attention to thecontent of solution used and to therate of
administration reveal that im-portant special measures must
betaken. Two other circumstances alsorequire comment: the presence
ofoligunia influences decision making,and finally, salt poisoning
should beconsidered as a separate entity.
Most patients with hypennatnemicdehydration are not severely
oligunicowing to the relatively expandedplasma volume. This group
may thenbe considered first. If one were toinfuse plain 5% glucose
water intothese patients, the risk would becerebral
swelling-actually waterintoxication. This results from thepresence
of endothelial cell tightjunctions in the CNS. Just as
rapidinfusion of hypertonic salt results inbrain shrinkage, so does
rapid infu-sion of isotonic glucose water causebrain swelling.
Glucose rapidlycrosses the blood-CNS barrier byactive transport so
that unlike thered cell, the brain does not necog-nize glucose as
an osmol, at least atphysiologic levels of glucose, butdoes react
to sodium and chlorideions as relatively impermeable be-cause of
the tight junctions.
When 5% glucose water is infusedrapidly intravenously the CSF
pres-sure rises (Fig 3). The increase inmillimeters of water is the
same fora given infused volume and rate ne-gardless of the initial
pressure. The
increase in pressure is from swellingof the brain cells, not an
increase ininterstitial fluid, ie, not edema. Brainswelling affects
a number of nervoussystem functions frequently result-ing in
convulsions. For some yearsafter hypernatremic dehydrationwas
described and recognized din-
ically, convulsions were commonlyseen during therapy, because
rapidwater replacement was attempted.
This circumstance led many cen-tens to suggest adding 75
mEq/literor more of sodium salts to initialtherapy. This will
reduce risk of con-vulsions but adds to the sodium bun-
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
Considerations(in Order)
TABLE 4. Regimen for Therapy of Hypernatremic Dehydration
1. Volume
Action
2. Glucose content
3. Sodium content
4. Potassium con-tent
5. Anion content
a Estimate the patients deficit by clinical meansfirst (mI/kg)
and multiply by weight (kg) for to-tal sum.
b. Estimate 48 hr worth of maintenance waterfollowing usual
clinical rules.
c. Add a + b for tentative volume of solution for2 days.
Use 2#{189}(2%-3%) to obviate later possible prob-lems with
hyperglycemia.
Allow 80-1 00 mEq/liter for deficit fraction of fluidand none
for maintenance portion. Resultantconcentration is usually 20-35
mEq/Iiter. Usethis concentration of sodium or simply estimateat 25
mEq/Iiten.
Generally, maximum safe amount for IV infusionon about 40
mEq/Iiter.
Sodium plus potassium advised equals 60-75mEq/liter of cation.
Distribute anions betweenchloride and base in accordance with
clinicaljudgment. Ifdesired, start with more base andchange to more
chloride after 6-12 hr. Do notuse HCO3 as base because of calcium
to beadded. Use acetate on lactate along with chlo-
6. Calcium content
7. Rate of adminis-tration
ride.One amplue of 10% calcium gluconate for every
500 ml of infusate.1/48 of volume/hr for 48 hr. In infant, usual
volume
will be 275-350 ml/kg/48 hr or 6-7 mI/kg/hr.
Fluids and Electrolytes
PIR 120 pediatrics in review #{149} vol. 3 no. 4 october
1981
den, frequently while excessive in-sensible water losses are in
prog-ness, thus aggravating hypennatne-mia. Such therapy also
frequentlyproduces visible edema in patients,leading to
prolongation of the recov-ery period. An alternative to increas-ing
concentration is to slow the rateof infusion which will also avoid
con-vulsions, but at risk of being too slowin repairing
dehydration, again withsuboptimal outcome.
A compromise resolution to theseproblems can be found, in part,
byconsidering that a high potassiumintake would offset cerebral
swellingand some of the potassium wouldenter depleted cells (mostly
musclecells) carrying water into them. Atthe same time water is
delivered tothe patient at a slow even rate. Thisregimen is
appropriate provided thepatient has no initial serious circu-latory
deficiency. The repair solution
is constructed with consideration ofvolume to be administered
for 48hours and of glucose content, so-dium content, potassium
content,anion distribution, calcium additive,and rate of
administration. Table 4demonstrates a method for analysisof each of
these points for use in apatient with hypernatnemic dehydra-tion,
but not in shock, and who pro-duces visible urine. Shock,
oligunia,and salt poisoning are consideredseparately.
Shock
If the patient has circulatory im-pairment (shock), first infuse
20 mI/kg of 5% albumin solution (singledonor plasma, plasma without
im-munoglobulin, on whole blood are allsatisfactory). Sodium
content inthese fluids up to 140 mEq/liten isnot important since
nearly the whole
volume will remain intravascular. Ifthe patient is producing
urine, pro-ceed as in the general manner givenabove.
Anuria
If the patient, even though not inhypotensive shock, has no
apparenturine, try a rapid infusion of 5% al-bumin. If urine then
enters the blad-den, proceed as before. If no urineenters the
bladder, give furosemide,1 mg/kg. If urine flow occurs, pro-ceed as
above; if not treat the patientwithout potassium in the
infusion.Increase the sodium concentrationto 50 mEq/Iiten, slow the
rate byreducing the volume to be adminis-tered, subtracting half
the mainte-nance allowance from the 48-hourtotal.
Salt Poisoning
In the event of massive salt poi-soning (plasma concentration of
so-dium >200 mEq/liten) use penito-neal dialysis to remove
excess so-dium chloride. For the dialyzing so-lution use 8% glucose
with no elec-trolyte, 1 00 mI/kg, two on threetimes at
approximately one-hour in-tervals. Simultaneously be sure
tomaintain an intravenous solution todeliver a volume of repair and
main-tenance solution as above. The hy-penglycemia induced by this
methodoffsets the removal of sodium andprevents water intoxication.
As theglucose is metabolized, water slowlyenters cells.
Insulin is not advisable for any hy-pennatnemic patients with
hypergly-cemia because rapid removal of glu-cose by metabolism is
the physio-logic equivalent of rapid water infu-sion.
In summary, the best treatmentseems to be a slow infusion
relativelylow in both glucose and sodium andhigh in potassium with
added cal-cium. For the past 12 years this reg-imen has been highly
successful andhas not produced complicating con-vulsions.
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
DOI: 10.1542/pir.3-4-1131981;3;113Pediatrics in Review
Laurence FinbergTreatment of Dehydration in Infancy
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/3/4/113including
high resolution figures, can be found at:
Permissions & Licensing
http://pedsinreview.aappublications.org/site/misc/Permissions.xhtmlentirety
can be found online at: Information about reproducing this article
in parts (figures, tables) or in its
Reprintshttp://pedsinreview.aappublications.org/site/misc/reprints.xhtmlInformation
about ordering reprints can be found online:
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from
-
DOI: 10.1542/pir.3-4-1131981;3;113Pediatrics in Review
Laurence FinbergTreatment of Dehydration in Infancy
http://pedsinreview.aappublications.org/content/3/4/113the World
Wide Web at:
The online version of this article, along with updated
information and services, is located on
Print ISSN: 0191-9601. Village, Illinois, 60007. Copyright 1981
by the American Academy of Pediatrics. All rights
reserved.trademarked by the American Academy of Pediatrics, 141
Northwest Point Boulevard, Elk Grove
andpublication, it has been published continuously since 1979.
Pediatrics in Review is owned, published, Pediatrics in Review is
the official journal of the American Academy of Pediatrics. A
monthly
by Desiree 'Desi' Rivera-Nieves on March 22,
2015http://pedsinreview.aappublications.org/Downloaded from