Embed Size (px)
Citation preview

Radiología. 2014;56(5):400---412
www.elsevier.es/rx
UPDATE IN RADIOLOGY
Perineural spread in head and neck tumors�
B. Brea Álvarez ∗, M. Tunón Gómez
Radiodiagnóstico. Hospital Universitario Puerta de Hierro-Majadahonda, Majadahonda, Madrid, Spain
Received 30 November 2013; accepted 13 April 2014Available online 8 November 2014
KEYWORDSMeSh terms;Neoplasm metastasis;Cranial nerveneoplasms/diagnosis;Cranial nerveneoplasms/secondary;Head and neckneoplasms/diagnosis;Head and neckneoplasms/secondary;Magnetic resonanceimaging;Computedtomography;X-Ray;Multimodal imaging;Neoplasminvasiveness
Abstract Perineural spread is the dissemination of some types of head and neck tumorsalong nervous structures. Perineural spread has negative repercussions on treatment because itrequires more extensive resection and larger fields of irradiation. Moreover, perineural spreadis associated with increased local recurrence, and it is considered an independent indicator ofpoor prognosis in the TNM classification for tumor staging. However, perineural spread often goesundetected on imaging studies. In this update, we review the concept of perineural spread, itspathogenesis, and the main pathways and connections among the facial nerves, which are essen-tial to understand this process. Furthermore, we discuss the appropriate techniques for imagingstudies, and we describe and illustrate the typical imaging signs that help identify perineuralspread on CT and MRI. Finally, we discuss the differential diagnosis with other entities.© 2013 SERAM. Published by Elsevier España, S.L.U. All rights reserved.
PALABRAS CLAVEMeSh Terms;Metástasis;Tumores NerviosCraneales/Diagnóstico;
Diseminación perineural en tumores de cabeza y cuello
Resumen La diseminación perineural corresponde a una forma de extensión de algunostipos de tumores de cabeza y cuello por las estructuras nerviosas. Su existencia reper-cute negativamente en el tratamiento porque requiere resecciones quirúrgicas más extensasy campos de irradiación mayores, está asociada con un incremento en las recurrencias
� Please cite this article as: Brea Álvarez B, Tunón Gómez M. Diseminación perineural en tumores de cabeza y cuello. Radiología.2014;56:400---412.
∗ Corresponding author.E-mail address: [email protected] (B. Brea Álvarez).
2173-5107/© 2013 SERAM. Published by Elsevier España, S.L.U. All rights reserved.
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 401
Tumores NerviosCraneales/Secundarios;Neoplasias Cabezay Cuello/Diagnóstico;RM;TC;Imagen Multimodal
locales y se considera un indicador pronóstico independiente en la clasificación TNM para estadi-ficar el tumor. Sin embargo con frecuencia pasa desapercibida en los estudios de imagen. En estaactualización revisaremos el concepto, la patogenia y las principales vías y conexiones entrelos nervios faciales, que son esenciales para comprender este proceso. Además, valoraremos latécnica apropiada para realizar un estudio correcto, presentaremos los signos de imagen típicospara reconocer esta entidad en la TC y RM y abordaremos los diagnósticos diferenciales.© 2013 SERAM. Publicado por Elsevier España, S.L.U. Todos los derechos reservados.
Introduction
Perineural spread is how some types of tumors spread fromhead to neck through nerve sheaths. Jean Cruveilheir wasthe first to talk about this way of tumor spread in 1835,1 soit is not a new way of neoplasm spread due to changes inbehavior thanks to the advances of medical care. Howeverit often goes unnoticed in such a way that it does not usuallyshow up in radiological reports.2
Perineural spread, perineural spread, perineural macro-scopic invasion, perineural affectation, small or big nerveaffectation are terms that can be used indiscriminately inliterature yet they show very different processes. Perineu-ral invasion (PNI) or small-caliber nerve invasion (SCNI) is themacroscopic affectation of nerve fascicula that can be seenanatomopathologically and found where the main tumorrests. Perineural spread (PNS) or large-caliber nerve inva-sion (LCNI) is the macroscopic shape that can be seen inimage studies or found clinically and is located beyond themain tumor lesion.3---5
The goal of this article is get to know this kind of tumorspread, its meaning, its spread patterns and its radiologicalfeatures in order to understand the condition and avoid falsenegatives in radiological reports.
Basic anatomical concepts
Peripheral nerves are made up of three layers called fromthe inside out epineurium, perineurium, and endoneurium(Fig. 1). In the epineurium both the most external com-ponent of the vasa nervorum and lymphatic channels canbe found. Perineurium is the intermediate layer---one con-centrically arranged multilayered structure of endothelialcells.6 Endoneurium is not a layer per se rather the laxusvascular connective tissue surrounding the Schwann cell-axon-complex making up the nerve fiber or small nerve.Various nerve fibers and the adjacent endoneurium gatheraround by the perineurium creating nerve fascicula. Thecluster of several fascicula surrounded by the epineuriumis what makes up the peripheral nerve or large nerve.Endoneurium is isolated from the extracellular compartmentby the perineurium and from blood flow by the strong linksof endothelial cells of endoneurial capillary. This is whatis called hematoneural barrier. Its disruption allows the out-flow of perineural contrast that in PNS patients is responsiblefor nerve pathological enhancement in image modalities.
Controversy on perineural affectation
There are several controversies in the actual literature onthis type of tumor spread due to several reasons:
A. There is not a standard use of different terms. In mostcases each publication uses a different term and doesnot specify on what grounds.
B. Not even among anatomopathologists there is a clearconsensus on what PNI really means. Some authors definePNI as the malignant cells located in the perineural spacewith total or almost total affectation of nerve circum-ference in the tangential anatomopathological cutting.7
Others like tumor affectation of one third of nerve cir-cumference or tumor cells in any of the componentlayers.4
C. According to the American College of Pathologists PNIneeds to be present in the reports filled out byanatomopathologists8 (present, absent or undetermined)and is conditioned by sampling methods, staining andimmunohystochemical processing of tumor.
Studies show variable and contradictory results depend-ing on the anatomopathological features and anatomicallocation of primary tumor:
--- PNI has been reported in many tumor lineages butis more common in the cystic adenoid carcinoma(CAC) (20---80%)9---11 and in the squamous carcinoma (SC)(27---82%).12,13
--- PNS is rare in SC at the level of the mouth floor, tonsillarfossa, larynx, pharynx and in the presence of PNI in theprimary tumor recurrence is also rare according to someauthors.5,14 However, other authors claim that survival isworse when PNI is found in tongue tumors.15,16 It seemsthat in the CAC there are no differences in the incidenceof PNS among those located in the major salivary glands orother regions. Also its repercussion on overall survival, orthe very capacity of tumor to invade adjacent structuresis not clear.11,14,17---20
--- Prognosis of PNI in mucoepidermoid carcinoma is pooreven though it is not characteristically associated withthis type of tumor.11,21,22
Despite contradictions, it seems evident that PNS hasa negative impact in treatment (more extensive surgical
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

402 B. Brea Álvarez, M. Tunón Gómez
Perineurium
Axon + schwann
Epineurium
Perineurium
Never fibers and endoneurium
A
B
Endoneurium
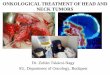
Figure 1 (A) Anatomopathological cut. Nerve fasciculus made up of several nerve fibers and the endoneurium surrounded by theperineurium. In this case there was perineural affectation due to tumor cells (arrow points) that completely surrounded the nervecircumference. (B) Diagram of peripheral nerve.
resection and larger field irradiation), yet the risk of localrecurrence is higher and in the last TNM classification, it isa prognostic marker of malignant tumors of the nasal cavityand paranasal sinuses, nasopharinx, major salivary glands,mucosal melanoma and cutaneous SC.23
Pathogenesis
The biological mechanism of pathogenesis is not fully under-stood. Former theories claim that the tumor spreads throughendoneurial lymphatic channels while the lymphatic onescan be found in the outer layer of epineurium since they donot penetrate any further. Considering that certain types oftumors are associated with PNS while others---more aggres-sive are not even in advanced stages the most widespreadaccepted theory is that of the reciprocal signals betweenthe nerve and tumor cells that activate the signalingpathways.14 These pathways include trophic and chemotac-tic factors and adhesion proteins to the extracellular matrix.Several growth factors and adhesion proteins have beenfound.18,24---29 At the CAC-level the p75 neurotrophin receptorhas been reported.24 During the development of the nervoussystem this receptor can be seen in the Schwann cells and itsinteraction with growth factor is capable of stimulating themigration of Schwann cells across the nerve. There might bea similar mechanism in PNI. In the PNI-related oropharyngalSC there is overexpression of the nerve growth factor andits receptor---tyrosine kinase A that can potentially be usedas a marker to predict tumor progression.25 Between theadhesion molecules at CAC both the N-CAM---in 93% of PNIpatients18 and ICAM-5 (telencephaline)26 are expressed. InSC of head and neck the N-CAM is expressed in between 50%and 93% of all cases.30,31
The activation of these pathways can draw tumor cells,stimulate its growth across the nerves and promote migra-tion and invasion.14 Recently it has been confirmed thatit can also stimulate axonogenesis or nerve enlargement,increase axons and neurogenesis or the number of neuronswhich would in turn increase the density of nerves in andaround neurotrophic tumors.32
Anatomy of nerves of the facial regionand patterns of spread
To be able to understand and define the PNS patterns weneed to take into consideration facial nerves and regionalclassification.33---37 The nerves frequently associated withPNS are the cranial nerves V and VII since they havethe largest regional spread and a closer relationship tothose anatomical regions where tumors grow whose anato-mopathological type is most commonly associated with PNS(Fig. 2). Yet in the facial skeleton there is a rich network ofanastomosis between cranial nerves and the cervical plexusso all nerves can potentially be affected (Tables 1 and 2).
Trigeminal nerve
In all cranial nerves there are five (5) different anatom-ical regions: nuclear, fascicular, cisternal, the skull baseand the peripheral one. Even though spread can affect allsegments the most commonly affected ones are the periph-eral and the skull base segments.
In the cranial nerve V the region of skull base reachesout from Meckel’s cave where the Gasser ganglion islocated towards the exit foramina of its three (3) peripheralbranches---ophthalmic, maxillary and mandibular nerves.
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 403
P
P
SM
L
SMP
P
NLATN
CTN
GSPN
LDPN
Vidian
nerve
SPN
Palatine nerve
Anterior trunk
Inferior alveolar nerve
Lingual nerve
Facial nerve
V1
V2
V3
Lacrimal
nervel
Glossopharyngeal nerve
IDPN
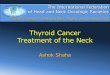
Figure 2 Scheme of the main branches of pairs V and VII. Anastomoses between both pairs are represented in red---the color ofthis figure can be seen in the electronic version of this article only. GSPN: greater superficial petrosal nerve. LDPN: large deeppetrosal nerve. lDPN: lesser deep petrosal nerve. AUN: Auriculotemporal nerve. CTN: chorda tympani nerve. PP: pterygopalatineganglion. SPN: Sphenopalatine nerve. Anastomosis (triple line) between the SPN and the lacrimal branch of V1.
Figure 3 Anatomy of cranial pair V. (A) T2-weighted axial MRI. Nuclear region of cranial pair V in the protuberance. In frontof it at the prepontine cistern-level the cisternal segment can be found (long white arrow). (B) T1-weighted coronal MRI aftergadolinium injection. (C) T1-weighted coronal MRI with fat saturation after gadolinium injection. (D) T1-weighted axial MRI aftergadolinium injection. (E) T1-weighted axial MRI with fat saturation after gadolinium injection. The V1 branch can be seen (B) inthe superior orbitary fissure (white silhouette), lateral to the anterior clinoid apophysss (*); V2, (B) and (D), in the larger roundbayonette-shaped foramen (white arrow point) to reach into the infraorbitary nerve canal (white line); V3, (C) and (E), in the ovalforamen (white triple arrow) and descending to innervate the muscles of the chewing space (triple line).
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

404 B. Brea Álvarez, M. Tunón Gómez
Figure 4 Perineural spread in the three (3) branches of pair V. (A) and (B) CT in axial and sagittal planes. Spread through the leftV1 branch (black arrow) in one patient with cutaneous epidermoid carcinoma. (C) and (D) T1-weighted axial and coronal MRI aftergadolinium injection in one patient with perineural spread along the right V2 branch (white double arrows) due to nasal melanoma.Nerve is thickened and contrast-enhanced, yet it is never as hyperintense as the normal fat of the normal pterygopalatina fossa(‘‘evil gray’’) (white arrow points). Compare it to the normal V2 left branch in the infraorbitary canal (discontinuous arrow).(E) and (F) T1-weighted axial and coronal MRI after gadolinium injection without (E) and with fat saturation (F) in one patient withcavum carcinoma. The left V3 branch is augmented and completely contrast-enhanced (white double arrow). It is evident whenwe compare it to the normal right nerve that only shows the peripheral enhancement of venous plexus (round white arrow). PNSreached Meckel’s cavum and consequently zone 2 (white asterisk) and also spread along the V2 branch (open white arrow points)and the vidian nerve (white arrow point).
Beyond the orifices the peripheral region can be found(Figs. 3 and 4).
The ophthalmic nerve (V1) arises from the Gasser gan-glion anterior and medial region continuing through thelateral wall of cavernous sinus towards the superior orbitalfissure. Just before penetrating in the fissure it is dividedinto three (3) terminal branches: lacrimal, frontal, andnasal.
The maxillary nerve (V2) reaches out from Meckel’scave onwards crossing the major round foramen towardsthe pterygopalatine fissure. Then it reaches to the outsideand looking down, this double angulation has a bayonette-shaped axial cutting to get into the infraorbital nerve canal.
Table 1 Connection of the V cranial pair.
Cranial pairs V Pair
V Pair Sphenopalatine nerve (V2)Lacrimal nerve (V1)
VII Pair Auriculotemporal nerve (V3)Parotid branchesSphenopalatine nerve (V2)Greater superficial petrosalnerve-vidianLingual nerve (V3)Chorda tympani nerve
Ocularmotor NN Cavernous sinusIII, IV, and VI
IX Pair and sympatheticplexus
Sphenopalatine nerve (V2)
Eventually at the end of the canal it emerges through theinfraorbital hollow dividing into three (3) terminal branches.All along its itinerary it sprouts collateral branches of whichtwo (2) are worth mentioning here: sphenopalatine andpalatine nerves. The sphenopalatine nerve sprouts from theV2 in the pterygopalatina fossa. Right there it contacts thepterygopalatine ganglion located in front of the vidian nervecanal to which it is also connected (Figs. 5 and 6). It hassympathetic branches to innervate the bucco-pharingeal
Table 2 Connection of the VII cranial pair.
Cranial pairs VII Pair
X Pair Mastoideus segmentArnold nerve
V Pair Parotid branchesAuriculotemporal nerve(V3)Greater superficialpetrosal nerve-vidianSphenopalatine nerve(V2)Chorda tympani nerveLingual nerve (V3)
Cervical plexus Cervical branchesGreater auricular nerve
IX Pair and carotidsympathetic plexus
Greater superficialpetrosal nerveLarge deep petrosalnerve-Vidian nerve
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 405
Figure 5 Obliteration of fat pads. (A) and (B) CT and (C) T1-weighted axial MRI. Obliteration of fat from left pterygopalatinefossa (long black arrows) in one patient with cavum carcinoma (compare it to the healthy right side; discontinuous black arrow).Invasion of the vidian nerve canal (black arrow point) too. Even though the obliteration of fat seen is that of the pterygopalatinefossa it can also be seen in other locations like in the patient of the inferior line. (D) and (E) CT with perineural spread through theleft inferior alveolar nerve (white long arrow) secondary to one cystic adenoid carcinoma of left submandibular gland. Compare itto the normal fat of the right side (discontinuous white arrow).
Figure 6 Patient underwent surgery due to cystic adenoid carcinoma of right maxillary sinus. T1-weighted axial MRI with gadolin-ium without (B) and with fat suppression (A), (C), (D) and (E) and T1-weighted coronal MRI with gadolinium without fat suppression,(F). Perineural spread along the right V1, bilateral V2, and right V3 branches of the right inferior alveolar nerve (discontinuousblack arrow), palatine nerves bilateral in the palate (black arrow points) and palatine foramina (white arrow points) of the rightauriculotemporal nerve (discontinuous white arrow), right greater superficial petrosal nerve (white long arrow) and vidian nerve(white double arrow). Affectation of Jacobson’s nerve IX pair (black curved arrow) probably from the vidian nerve and of the largedeep petrosal nerve of the right carotid sympathetic plexus (white discontinuous circle). Affectation of the III pair (white curvedarrow) due to connection with V1 branch in the cavernous sinus.
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

406 B. Brea Álvarez, M. Tunón Gómez
Figure 7 (A) Axial CT. (C) and (D) Oblique sagittal CT. (B) T1-weighted axial MR after gadolinium injection. Patient with cysticadenoid carcinoma at the palate and perineural spread along the right greater superficial petrosal nerve (discontinuous whitearrows/white bar). This nerve sprouts from the geniculate ganglion (G) and anastomoses with the V2 branch. In this patient thereis affectation of the V pair in the oval foramen (discontinuous circle). Perineural spread disseminated across all segments of the VIIpair: canalicular C, labrynthic L, transtympanic TT y mastoideus M. Compare bone widening and intense asymmetric enhancementof the geniculate ganglion and the various segments of facial nerve with perineural spread in the right side and compare it to thehealthy left side (*).
mucosa and the lacrimal gland---this last one anastomoseswith the lacrimal nerve of V1. The palatine nerve isalso born inside the pterygopalatine fossa and movingthrough the palatine canal towards the palate. When itreaches the palate it divides itself into greater and lesserpalatine nerves reaching through the mucosa through thegreater and lesser palatine foramina (Fig. 6).
The mandibular nerve (V3) passes under the Gasser gan-glion coming out of the skull through the oval foramen.Then it gives rise to one motor-wise small anterior trunkand another sensitive-wise posterior trunk. The motor trunkinnervates the chewing muscles. The posterior trunk dividesinto three (3) branches: auriculotemporal, lingual, and alve-olar inferior nerves (Figs. 5 and 6). The auriculotemporalnerve38 passes through the parotid gland located behind themandibular condyle. At the parotid gland it anastomoseswith branches from the facial nerve (Figs. 2 and 6). The lin-gual nerve runs under the lingual espace. It connects to thechorda tympani---one facial nerve branch with parasympa-thic innervation of the submandibular and sublingual glands(Fig. 2).
Facial nerve
In this cranial pair the skull base region is structuredinto four (4) segments. The canicular segment runs fromthe acoustic porous through the anterosuperior compart-ment of the internal auditory canal (IAC) and towards the
fundus: the labryrinthic segment that runs between thefundus and the geniculate ganglion; the tympanic segmentrunning---in a bony canal at the medial wall of the tympanicbox from the geniculate ganglion to the second elbow; thelast segment or mastoideus running from the second elbowtowards the stylomastoid orifice. The peripheral regionstarts at the cranial exit through the stylomastoid orifice.From this location it runs through the parotid gland divid-ing into five (5) terminal branches responsible for the motorinnervation of facial muscles.
All along its itinerary the facial nerve produces two (2)important branches: the greater superficial petrosal nerve(GSPN) (Fig. 7) and the chorda tympani. The GSPN39 emergesfrom the geniculate ganglion, moves forward and thenanastomoses with the large deep petrosal nerve (LDPN) tomake up the vidian nerve that reaches into the sphenopala-tine ganglion to then make contact with the sphenopalatinenerve (Figs. 5 and 6). The chorda tympani sprouts from theVII cranial pair before it exists the stylomastoid orifice tothen make contact with the lingual nerve.
Other cranial pairs and cervical plexus
The cervical plexus is a structure made up of the afore-mentioned division for the four (4) first cervical nerves.40
It innervates the postarticluar region (greater auricularnerve)41 and the anterosuperior region of the neck giving
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 407
Table 3 Zone classification.
V1 V2 V3 VII
Zone 1 Up to the superiororbitary fissure
Up to the externalopening of the largeround foramen
Up to the externalopening of the ovalforamen
Up to the externalopening of thestylomastoid foramen
Zone 2 From zone 1 toGasser’s ganglion
From zone 1 to thelateral end of the IAC
From zone 1 to thelateral end of IACD
Zone 3 The whole nerve fromGasser’s ganglion orIAC to the cisterns orthe encephalic trunk
IAC, internal auditory canal.
rise to numerous branches for the deep muscular structureslike the cervical loop and the phrenic nerve.
A branch sprouts from the glossopharyngeal nerve---thetympanic nerve (nerve of Jacobson). Through the tympaniccanaliculus it enters the tympanic box forming a plexuxover the cochlear promontory (Fig. 6). It receives branchesfrom the carotid sympathic plexus making up the LDPNand the lesser deep petrosal nerve (lDPN). In the lDPNit anastomoses with the LDPN making up the vidiannerve (Figs. 2---5 and 7). The lDPN connects to the ATN(aruculotemporal nerve).
The vagus nerve gives rise to one branch---Arnold’s nervelocated in a separate canal that anastomoses with the mas-toid segment of facial nerve.
The hypoglossal nerve in its cisternal segment establishesconnections with cranial pairs IX and X.
Regional classification
It allows us to describe the anatomical spread of PNSon the MRI by segments of affectation. This system deter-mines the spread of surgical, subcranial or skull baseresection,42 and has proven to be a predictor of overallsurvival.43 It is all about three (3) regions whose limits aredefined by the affected cranial pair (V or VII) and by thedifferent branches of cranial pair V (V1, V2, or V3) (Table 3).
Clinical manifestations
Up to 45% of the patients with PNS are asymptomatic evenwith extensive affectation. And there are patients with clin-ical data suggestive of PNS showing no alterations in imagemodalities.44,45
Overall the clinical manifestations of PNS are late andpresent subtle and unspecifically.46 We must be suspiciousin the presence of an insidious affectation of cranial pairsslowly progressive and not coming back to normal functionafter six (6) months of therapy or if several cranial nervesare affected on one side only---Garcin’s syndrome.46
Image modalities
The image modalities used to diagnose this entity are MRI,CT and PET-CT. The MRI is the chosen one because of
its greater contrast resolution and sensibility to discard‘‘segmental’’ nerve affectation. Despite its use being stillnot widespread, recent literature claims that the PET-MRcan even be more accurate to diagnose PNS.47
Magnetic resonance
Use T1-weighted high-resolution spatially isotropic volumet-ric sequences with or without fat saturation.48 Modalitieswith fat saturation allow us to define enhanced lesions thatare close to espaces with fat like the orbits, the ptery-gopalatine fissure and neurovascular foramina.33,36 However,other authors prefer sequences without fat saturation49,50
because they think they can see very well those fatpads that are adjacent to foramina and distinguish themfrom those that obliterate pathologically due to tumor infil-tration and because even after injecting gadolinium, thetumor never shows the same hyperintensity as fat does---theso-called ‘‘evil gray’’ (Fig. 4). Also not saturating fat avoidsthe susceptibility artifacts frequently observed in saturationsequences. In our institution the protocol consists of T1-weighted sequences without fat saturation before injectingthe contrast and then T1-weighted sequences with fat sat-uration after injecting gadolinium. T2-weighted sequencesare necessary for the study of cisternal, fascicular andnuclear segments of cranial pairs, when region 3 is affected.Also fat saturation can be useful to assess the inflamma-tory component associated with this entity above all wherenerves are associated with fat pads.
Computed tomography
CT does a real good evaluation of both the shape and size offoramina and bone canals at the skull base-level. It allows usto distinguish between a rapidly destructive process usuallyassociated with a speckled permeative pattern and anotherprocess with a slower and indolent course prone to remod-eling and expansion.
PET-CT
It is very useful to diagnose head and neck cancers where itis superior to CT and MRI in the study ganglionar affectation
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

408 B. Brea Álvarez, M. Tunón Gómez
Figure 8 Secondary findings. (A) T2-weighted coronal MR and (B) T1-weighted coronal MR with fat saturation and gadolinium.Patient with perineural spread across the V3 branch and acute muscular denervation. T2 hyperintensity and T1-weighted enhance-ment with volume preservation of left side pterygoid (black arrow point), temporal (white arrow point), and masseter muscles(white arrow). Check out the difference with the healthy side (*). T1-weighted coronal (C) and axial (D) MR of another patient withatrophy due to chronic denervation. Hyperintensity and loss of volume of the right chewing space muscles due to fat substitution.
and to find residual or recurrent tumors.51 However, when itcomes to PNS there are no accepted data on its sensibilityand specificity. Nevertheless any linear or curvilinear foci ofabnormal FDG-uptake in the anatomical territories of cranialpairs must lead us to suspect PNS and correlate them withsigns of MR to confirm diagnosis.52
Radiological findings
1. Primary. They are associated with the direct affectationof the nerve by the tumor.--- Complete enhancement or complete uptake of
the whole nerve circumference in T1-weightedgadolinium-enhanced sequences (due to rupture ofhematoneural barrier) and thickening or enlargementof the nerve normal caliber.36,53 We must distinguishbetween the complete enhancement of the patholog-ical nerve and the peripheral symmetric enhancementand variable thickness of the normal nerve (targetappearance) (Figs. 3 and 4). Peripheral enhance-ment is due to the perineural venous plexus and itcan be frequently seen in the foramina segments ofthe three (3) branches of the trigeminal nerve, inthe geniculate ganglion, at the LDPN level and inthe proximal part of the labyrinth segment of facialnerve.35,54
--- Deletion or obliteration of juxtaforaminal fat pads55
due to tumor growth and the associated inflammatorycomponent (Fig. 5).
--- Size increase of foramina and bone canals(Figs. 5 and 7).
--- Spread of intracranial compartment. It is associatedwith the infiltration of cavernous sinus, lateral walldilating, dural thickening adjacent to the affectednerve segments and thickening or enhancement of cis-ternal and fascicular segments of the affected cranialpairs (Figs. 4E and 6C).
2. Secondary. Neural affectation causes atrophia due todenervation. This finding is more frequent in boththe chewing muscles (due to the affectation of V3)and the tongue (due to affectation of the hypoglos-sal muscle) and less common in the muscles of facialexpression.56 The process of denervation has three (3)stages with different muscular signal patterns on the MRI.In the acute stage (1st month) the muscles are hyper-intense in T2-weighted sequences and increase theirsize and enhancement in contrast-enhanced T1-weightedsequences. Hyperintensity is due to the increase ofextracellular water volume and the reduction of theintracellular water one; the T2 of extracellular water islonger than the intracellular one. Enhancement is dueto an increase in perfusion and accumulation of contrastin the extracellular espace. In the subacute stage (up to20 months) hyperintensity can still exist in T2 sequenceswhile the signal in non-contrast-enhanced T1 sequencesincreases due to fat deposits; muscles keep their normalsize though. In the chronic stage atrophy is general, themuscular volume diminishes and the signal increases innon-contrast-enhanced T1 sequences (Fig. 8).
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 409
Figure 9 Zone classification 3. T1-weighted MR after gadolinium injection. (A) Axial image with fat saturation, (B) Axial imagewithout fat saturation, and (C) coronal image without fat saturation. Patient with a history of right frontal cutaneous epidermoidcarcinoma resection 7 years ago. He presented some time later with Tolosa-Hunt syndrome. (A) Inflammatory abnormalities inthe orbitary vertex (white arrow point) and the cavernous sinus (white arrows). Corticoids were administered due to suspicion ofinflammatory pseudotumor that resolved the clinical presentation partially. However in the control MR (not shown) abnormalitiesin the cavernous sinus persisted. Two (2) years later the patient presented with left Garcin syndrome. (B) and (C) The affectationof left cavernous sinus and Meckel’s cavum is now more significant (asterisk) as well as the spread of the process towards the basalcisterns (discontinuous white arrows) and even towards the protuberance (black arrow). The biopsy of the affected ophthalmicnerve (not shown) was also positive for epidermoid carcinoma.
We must not forget that the signs of PNS can persist indef-initely yet despite clinical improvement. This is why we mustbe suspicious about relapse when the lesion deterioratesor symptoms grow worse.50 When a head and neck malig-nant tumor is stratified---especially those associated with PNSwe must fully study the course of all cranial nerves. Dueto the extensive network of connections all nerves can bepotentially affected (Fig. 6). Nerve alteration can look dis-continuous in the image (‘‘‘‘skip’’ metstasis’’) though atthe anatomopathological level it is continuous.3,57---59 Dis-crepancy is due to the fact that tumor load is variable allalong the nerve and also to the fact that where discrepancyis lesser it might not be seen in radiological studies.5
Differential diagnosis
The differential diagnosis of this entity is established withlesions of tumor, inflammatory and infectious origin.50
The affectation of zone 1 (Fig. 4A---D)---peripheral usuallyis due to benign tumors of the nerve sheath like schwanomesand neurofibromes. In these lesions the tumor mass islocated focally surrounding the nerve and even though itssize is variable it is usually highly segmented not affectingall of its trajectory. Schwanomes are more common and usu-ally originated in the junction between Schwann cells andglial cells and this is the reason why the usual location iszone 2. Even though it can be associated with any cranial
pairs the VIII and V are the most common ones. Neurofi-bromes are usually peripheral and can be found isolated orin neurofibromatosis Type 1.
The affectation of zone 2 (Figs. 4E and 9) is mainly rep-resented by the affectation of cavernous sinus.60 Amongtumors meningiomas, schwanomes of pair V and metas-tasis are the most frequent lesions of all. Inflammatorypseudotumors,61 granulomatose conditions,62 and infectionsare among non-tumor lesions. The clinical presentation ofmost of these processed has to do with the affectation ofoculomotor pairs---above all the VI cranial pair. However, inthe PNS the affectation of V pair is very common. Also in theimage there are useful data like hyperostosis and the ero-sion of the adjacent bone that can lead us to meningiomasor metastasic processes, respectively. The dural tail that ismore characteristic of meningiomas and inflammatory pro-cesses and one inflammatory process in the orbitary vertexis very suggestive both of inflammatory pseudotumors andthe spread of an infectious sinusal process63---65 needs to becautiously considered and followed for proper management(Fig. 9).
When the lesion is not continuous---though of variable sizefrom zone 1 to zone 3 there are few processes that canbe included. In these situations malignant lineage neuraltumors,66 meningiomas and obviously PNS must be sus-pected.
The exclusive affectation of zone 3 is not a charac-teristic finding of PNS. It is now when we should think of
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

410 B. Brea Álvarez, M. Tunón Gómez
granulomatose inflammations like sarcoidosis,62 infec-tions like neuritis of viral origin33,67,68 and tumors likeleptomenyngeal spread of extracerebral lymphoma.
Conclusion
Perineural spread is a type of metastasic spread moreprevalent in certain types of tumors usually occurring inhead and neck tumors. It is often misdiagnosed in imagestudies and yet it modifies the protocols of treatment andis associated with a higher rate of local recurrence and isalso an independent prognostic factor of TNM classificationof malignant tumors. Getting to know this association, theanatomical distribution of cranial pairs V and VII and theirrich neural connection is essential. MRIs allow us to studythe neural trajectory from the peripheral to the nuclearregion in order to find thickness increases, completeenhancements and the obliteration of fat planes---which areall primary findings of this type of tumor spread.
Authors
1. Manager of the integrity of the study: BBA2. Original Idea of the Study: BBA3. Study Design: BBA, MTG4. Data Mining: BBA, MTG5. Data Analysis and Interpretation: BBA, MTG6. Statistical Analysis: BBA7. Reference Search: BBA, MTG8. Writing: BBA, MTG9. Manuscript critical review with intellectually relevant
contributions: BBA10. Final Version Approval: BBA, MTG
Ethical responsibilities
Protection of people and animals. Authors confirm that noexperiments have been performed on human beings or ani-mals.
Data confidentiality. Authors confirm that in this reportthere are no personal data from patients.
Conflict of interests
Authors reported no conflicts of interests.
References
1. Cruveilhier J. Anatomie pathologique du corp humain. BrainBooks; 1835.
2. Ginsberg LE. Reinterpretation of head and neck scans: mas-sive can of worms or call to action? Am J Neuroradiol.2002;23:1617---8.
3. Nemzek WR, Hecht S, Gandour-Edwards R, Donald P, McKennanK. Perineural spread of head and neck tumors: how accurate isMR imaging? Am J Neuroradiol. 1998;19:701---6.
4. Liebig C, Ayala G, Wilks JA, Berger DH, Albo D. Perineu-ral invasion in cancer: a review of the literature. Cancer.2009;115:3379---91.
5. Johnston M, Yu E, Kim J. Perineural invasion and spread in headand neck cancer. Expert Rev Anticancer Ther. 2012;12:359---71.
6. Akert K, Sandri C, Weibel ER, Peper K, Moor H. The finestructure of the perineural endothelium. Cell Tissue Res.1976;165:281---95.
7. Dunn M, Morgan MB, Beer TW. Perineural invasion: identifica-tion, significance, and a standardized definition. Dermatol Surg.2009;35:214---21.
8. Cancer Protocols and Checklists. College of American Patholo-gists; 2012.
9. Hutcheson JA, Vural E, Korourian S, Hanna E. Neural cell adhe-sion molecule expression in adenoid cystic carcinoma of thehead and neck. Laryngoscope. 2000;110:946---8.
10. Shimamoto H, Chindasombatjaroen J, Kakimoto N, Kishino M,Murakami S, Furukawa S. Perineural spread of adenoid cys-tic carcinoma in the oral and maxillofacial regions: evaluationwith contrast-enhanced CT and MRI. Dentomaxillofac Radiol.2012;41:143---51.
11. Van Weert S, Bloemena E, van der Waal I, de Bree R, RietveldDH, Kuik JD, et al. Adenoid cystic carcinoma of the head andneck: a single-center analysis of 105 consecutive cases over a30-year period. Oral Oncol. 2013;49:824---9.
12. Kurtz KA, Hoffman HT, Zimmerman MB, Robinson RA. Perineu-ral and vascular invasion in oral cavity squamous carcinoma:increased incidence on re-review of slides and by usingimmunohistochemical enhancement. Arch Pathol Lab Med.2005;129:354---9.
13. Fagan JJ, Collins B, Barnes L, D’Amico F, Myers EN, Johnson JT.Perineural invasion in squamous cell carcinoma of the head andneck. Arch Otolaryngol Head Neck Surg. 1998;124:637---40.
14. Gil Z, Carlson DL, Gupta A, Lee N, Hoppe B, Shah JP, et al.Patterns and incidence of neural invasion in patients with can-cers of the paranasal sinuses. Arch Otolaryngol Head Neck Surg.2009;135:173---9.
15. Brown B, Barnes L, Mazariegos J, Taylor F, Johnson J, Wag-ner RL. Prognostic factors in mobile tongue and floor of mouthcarcinoma. Cancer. 1989;64:1195---202.
16. Soo KC, Carter RL, O’Brien CJ, Barr L, Bliss JM, Shaw HJ. Progno-stic implications of perineural spread in squamous carcinomasof the head and neck. Laryngoscope. 1986;96:1145---8.
17. Hanna E, Vural E, Prokopakis E, Carrau R, Snyderman C,Weissman J. The sensitivity and specificity of high-resolutionimaging in evaluating perineural spread of adenoid cystic car-cinoma to the skull base. Arch Otolaryngol Head Neck Surg.2007;133:541---5.
18. Gandour-Edwards R, Kapadia SB, Barnes L, Donald PJ, JaneckaIP. Neural cell adhesion molecule in adenoid cystic carci-noma invading the skull base. Otolaryngol Head Neck Surg.1997;117:453---8.
19. Choi Y, Kim S-B, Yoon DH, Kim JY, Lee S, Cho KJ. Clini-cal characteristics and prognostic factors of adenoid cysticcarcinoma of the head and neck. Laryngoscope. 2013;123:1430---8.
20. Barrett AW, Speight PM. Perineural invasion in adenoid cysticcarcinoma of the salivary glands: a valid prognostic indicator?Oral Oncol. 2009;45:936---40.
21. Spiro RH, Thaler HT, Hicks WF, Kher UA, Huvos AH, Strong EW.The importance of clinical staging of minor salivary gland car-cinoma. Am J Surg. 1991;162:330---6.
22. McHugh CH, Roberts DB, El-Naggar AK, Hanna EY, Garden AS,Kies MS, et al. Prognostic factors in mucoepidermoid carcinomaof the salivary glands. Cancer. 2012;118:3928---36.
23. Sobin LH, Compton CC. TNM seventh edition: what’s new, what’schanged: communication from the International Union AgainstCancer and the American Joint Committee on Cancer. Cancer.2010;116:5336---9.
24. Fanburg-Smith JC, Miettinen M. Low-affinity nerve growth fac-tor receptor (p75) in dermatofibrosarcoma protuberans and
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Perineural spread in head and neck tumors 411
other nonneural tumors: a study of 1,150 tumors and fetal andadult normal tissues. Hum Pathol. 2001;32:976---83.
25. Kolokythas A, Cox DP, Dekker N, Schmidt BL. Nerve growthfactor and tyrosine kinase A receptor in oral squamous cell car-cinoma: is there an association with perineural invasion? J OralMaxillofac Surg. 2010;68:1290---5.
26. Maruya S, Kim HW, Weber RS, Lee JJ, Kies M, Luna MA, et al.Gene expression screening of salivary gland neoplasms: molec-ular markers of potential histogenetic and clinical significance.J Mol Diagn. 2004;6:180---90.
27. Iwamoto S, Odland PB, Piepkorn M, Bothwell M. Evidencethat the p75 neurotrophin receptor mediates perineural spreadof desmoplastic melanoma. J Am Acad Dermatol. 1996;35:725---31.
28. Dos Reis PP, Bharadwaj RR, Machado J, Macmillan C, Pin-tilie M, Sukhai MA, et al. Claudin 1 overexpression increasesinvasion and is associated with aggressive histological fea-tures in oral squamous cell carcinoma. Cancer. 2008;113:3169---80.
29. Ayala GE, Dai H, Powell M, Li R, Ding Y, Wheeler TM, et al.Cancer-related axonogenesis and neurogenesis in prostate can-cer. Clin Cancer Res. 2008;14:7593---603.
30. Vural E, Hutcheson J, Korourian S, Kechelava S, Hanna E. Corre-lation of neural cell adhesion molecules with perineural spreadof squamous cell carcinoma of the head and neck. OtolaryngolHead Neck Surg. 2000;122:717---20.
31. McLaughlin Jr RB, Montone KT, Wall SJ, Chalian AA, WeinsteinGS, Roberts SA, et al. Nerve cell adhesion molecule expressionin squamous cell carcinoma of the head and neck: a pre-dictor of propensity toward perineural spread. Laryngoscope.1999;109:821---6.
32. Binmadi NO, Basile JR. Perineural invasion in oral squamouscell carcinoma: a discussion of significance and review of theliterature. Oral Oncol. 2011;47:1005---10.
33. Borges A, Casselman J. Imaging the trigeminal nerve. Eur JRadiol. 2010;74:323---40.
34. Alves P. Imaging the hypoglossal nerve. Eur J Radiol.2010;74:368---77.
35. Yousry I, Moriggl B, Schmid UD, Naidich TP, Yousry TA.Trigeminal ganglion and its divisions: detailed anatomic MRimaging with contrast-enhanced 3 D constructive interferencein the steady state sequences. Am J Neuroradiol. 2005;26:1128---35.
36. Maroldi R, Farina D, Borghesi A, Marconi A, Gatti E. Per-ineural tumor spread. Neuroimaging Clin N Am. 2008;18:413---29.
37. Rouvière H, Delmas A. Nervios de la cabeza y del cuello.Anatomía humana: descriptiva, topográfica y funcional. 9.a edBarcelona-Méjico: Masson; 1998. p. 257---316.
38. Schmalfuss IM, Tart RP, Mukherji S, Mancuso AA. Perineuraltumor spread along the auriculotemporal nerve. Am J Neuro-radiol. 2002;23:303---11.
39. Ginsberg LE, De Monte F, Gillenwater AM. Greater superficialpetrosal nerve: anatomy and MR findings in perineural tumorspread. Am J Neuroradiol. 1996;17:389---93.
40. Kozic D, Njagulj V, Gacesa JP, Semnic R, Prvulovic N. Perineu-ral tumor spread -Interconnection between spinal and cranialnerves. J Neurol Sci. 2012;323:254---6.
41. Ginsberg LE, Eicher SA. Great auricular nerve: anatomy andimaging in a case of perineural tumor spread. Am J Neuroradiol.2000;21:568---71.
42. Williams LS, Mancuso AA, Mendenhall WM. Perineural spreadof cutaneous squamous and basal cell carcinoma: CTand MR detection and its impact on patient manage-ment and prognosis. Int J Radiat Oncol Biol Phys. 2001;49:1061---9.
43. Solares CA, Lee K, Parmar P, O’Rourke P, Panizza B. Epidemiol-ogy of clinical perineural invasion in cutaneous squamous cell
carcinoma of the head and neck. Otolaryngol Head Neck Surg.2012;146:746---51.
44. Gulya AJ, Scher R, Schwartz A, Wilson WR. Facial and trigemi-nal neural dysfunction by a primary cutaneous squamous cellcarcinoma: MRI and clinicopathologic correlates. Am J Otol.1992;13:587---90.
45. Veness MJ. Treatment recommendations in patients diagnosedwith high-risk cutaneous squamous cell carcinoma. AustralasRadiol. 2005;49:365---76.
46. Alapatt JP, Premkumar S, Vasudevan RC. Garcin’s syndrome----a case report. Surg Neurol. 2007;67:184---5.
47. Kuhn FP, Hüllner M, Mader CE, Kastrinidis N, Huber GF, vonSchulthess GK, et al. Contrast-enhanced PET/MR imaging ver-sus contrast-enhanced PET/CT in head and neck cancer:how much MR information is needed? J Nucl Med. 2014;55:551---8.
48. Ong CK, Chong VF. Imaging of perineural spread in head andneck tumours. Cancer Imaging. 2010;10:S92---8. Spec no A.
49. Curtin HD. Detection of perineural spread: fat suppression ver-sus no fat suppression. Am J Neuroradiol. 2004;25:1---3.
50. Moonis G, Cunnane MB, Emerick K, Curtin H. Patterns of perineu-ral tumor spread in head and neck cancer. Magn Reson ImagingClin N Am. 2012;20:435---46.
51. Sadick M, Schoenberg SO, Hoermann K, Sadick H. Current onco-logic concepts and emerging techniques for imaging of head andneck squamous cell cancer. GMS Curr Top Otorhinolaryngol HeadNeck Surg. 2012;11:Doc08.
52. Paes FM, Singer AD, Checkver AN, Palmquist RA, de La VegaG, Sidani C. Perineural spread in head and neck malignan-cies: clinical significance and evaluation with 18F-FDG PET/CT.Radiographics. 2013;33:1717---36.
53. Carter RL, Foster CS, Dinsdale EA, Pittam MR. Perineural spreadby squamous carcinomas of the head and neck: a morphologicalstudy using antiaxonal and antimyelin monoclonal antibodies.J Clin Pathol. 1983;36:269---75.
54. Hong HS, Yi BH, Cha JG, Park SJ, Kim DH, Lee HK, et al. Enhance-ment pattern of the normal facial nerve at 3.0 T temporal MRI.Br J Radiol. 2010;83:118---21.
55. Yamamoto M, Curtin HD, Suwansa-ard P, Sakai O, Sano T, OkanoT. Identification of juxtaforaminal fat pads of the second divi-sion of the trigeminal pathway on MRI and CT. Am J Roentgenol.2004;182:385---92.
56. Fischbein NJ, Kaplan MJ, Jackler RK, Dillon WP. MR imaging intwo cases of subacute denervation change in the muscles offacial expression. Am J Neuroradiol. 2001;22:880---4.
57. Parker GD, Harnsberger HR. Clinical-radiologic issues in per-ineural tumor spread of malignant diseases of the extracranialhead and neck. Radiographics. 1991;11:383---99.
58. Nemec SF, Herneth AM, Czerny C. Perineural tumor spread inmalignant head and neck tumors. Top Magn Reson Imaging.2007;18:467---71.
59. Caldemeyer KS, Mathews VP, Righi PD, Smith RR. Imaging fea-tures and clinical significance of perineural spread or extensionof head and neck tumors. Radiographics. 1998;18:97---110.
60. Razek AA, Castillo M. Imaging lesions of the cavernous sinus. AmJ Neuroradiol. 2009;30:444---52.
61. Lu C-H, Yang C-Y, Wang C-P, Yang C-C, Liu H-M, Chen Y-F. Imagingof nasopharyngeal inflammatory pseudotumours: differentialfrom nasopharyngeal carcinoma. Br J Radiol. 2010;83:8---16.
62. Amin A, Balderacchi JL. Trigeminal neurosarcoidosis: casereport and literature review. Ear Nose Throat J. 2010;89:320---2.
63. McLean FM, Ginsberg LE, Stanton CA. Perineural spreadof rhinocerebral mucormycosis. Am J Neuroradiol. 1996;17:114---6.
64. Frater JL, Hall GS, Procop GW. Histologic features of zygomy-cosis: emphasis on perineural invasion and fungal morphology.Arch Pathol Lab Med. 2001;125:375---8.
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

412 B. Brea Álvarez, M. Tunón Gómez
65. Mayayo E, Landeyro J, Stchigel AM, Gazzoni A, Capilla J. Per-ineural spread by fungal cells. Case report and literature review.Rev Iberoam Micol. 2010;27:94---7.
66. Bowers CA, Taussky P, Duhon BS, Chin SS, Couldwell WT.Malignant peripheral nerve sheath tumour of the trigeminalnerve: case report and literature review. Br J Neurosurg.2011;25:750---3.
67. Bathla G, Hegde AN. The trigeminal nerve: an illustratedreview of its imaging anatomy and pathology. Clin Radiol.2013;68:203---13.
68. Karlberg M, Annertz M, Magnusson M. Acute vestibular neu-ritis visualized by 3-T magnetic resonance imaging withhigh-dose gadolinium. Arch Otolaryngol Head Neck Surg.2004;130:229---32.
Documento descargado de http://www.elsevier.es el 10/11/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.