Embed Size (px)
Citation preview

Primary And Secondary Tumors Of Neck
Dr Tridip Dutta BaruahAsst Prof, Dept Of Surgery
MGMCRI

What are Primary Neck Tumors?
Primary tumors originate in the head or neck itself, including the thyroid, throat, larynx, salivary gland or other locations.
Primary tumors of the head and neck typically spread to the lymph nodes in the neck.

Common Sites Of Neck Primary
1. OralCavity, Toungue and Tonsils2. Salivary Glands3. Pharyx and Nasopharynx4. Larynx5. Oesophagus6. Thyroid

What are secondary tumors ? Secondary cancers are tumors that have spread
from primary tumors in other parts of the body to the head or neck.
Most often, secondary tumors of the neck originate in the lung, breast, kidney, or from melanomas in the skin.
Cancers in the nasal and sinus passages may spread to the brain through nerves in the skull.

Histological Types Of Secondaries
1. Squamous cell carcinoma(Mainly from oral cavity and pharynx)
2. Adenocarcinoma(From GIT and usually involves left supraclavicular lymph nodes)
3. Rarely Melanoma

Risk Factors Tobacco and heavy alcohol use are the most
common risk factors for head and neck cancer. This includes all tobacco products including
cigarettes, cigars and chewing tobacco. Cigarette smokers have a lifetime increased risk
for head and neck cancers 5-25 times over the general population
Ex-smokers risk for head and neck cancer begins to approach the general population 20 years after quitting tobacco

Additional Risk Factors
Leukoplakia (1/3 develop oral cancer
M > F (2-3 times risk) Age > 40 Betel nut chewing
Occupational inhalant exposures including nickel refining, textile fibers and woodworking dust

Clinical Presentation
Patients generally present with a painless, solitary neck mass, most often discovered by the patient.
Masses are usually at least 2-3 cm Patients have usually gone through at least
one course of antibiotics Benign masses are also often solitary and
painless

Features Of Secondaries Of Neck1. Age: Elderly male. Commonly presents with rapidly
growing painless swelling in the neck.2. Swelling has nodular surface, hard in consistency and
often fixed.3. Secondaries can infiltrate muscles, post vertebral
muscles, nerves such as spinal acessory and hypoglossal and sometimes cervical sympathetic chain.
4. It can spread to surrounding soft tissue causing fungation and ulceration.
5. In advanced cases can infiltrate major blood vessel such as carotid or one of its branches causing torrential haemorrahge.

Symptoms Of Secondaries Of NeckPatient May present with1. Horseness: carcinoma Larynx or Thyroid2. Dysphagia: Carcinoma post 1/3 of toungue,
Pharynx and esophagus3. Haemoptysis, cough and dypsnoea: Carcinoma
Lung4. Ear pain and deafness: Nasopharyngeal carcinoma.5. Involvent of 7/11/12 Cranial nerves and
Sympathetic chain.

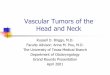
Levels of the Neck

Relationship of Node Location to Likely Disease
Nodes at certain levels more likely certain primaries
Upper neck nodes are the most likely to be head and neck cancera) Subdigastric node may be virtually any head and neck primary, or a non-Hodgkin’s lymphomab) Submandibular node suggests oral cavity, lip, nasal vestibule or salivary gland primaryc) Submental nodes are uncommon

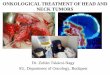
Relationship of Node Location to Likely Disease
Mid NeckLikely primaries include larynx, hypopharynx, and less commonly esophagus, disease below clavicles or lymphoma Lower Neck and Supraclavicular Nodesa) Most often metastatic from chest or abdomen, possible esophagus or lymphoma. A primary head and neck node is uncommon at this levelb)Parotid lymph nodes are more likely skin cancer than from a primary parotid tumorc)Benign neck masses are most common except in supraclavicular lymph nodes

Head and Neck Cancer- Squamous Cell.Carcinoma
6th most common cancer worldwide. HNSCC ~ 5% all cancers S.C.C most common upper aero digestive tract
malignancy Smoking and 50% HNSCC occur in oral cavity Management presents considerable functional
and aesthetic problems Multidisciplinary approach imperative

Treatment of Head and Neck - Squamous Cell Carcinoma
Removal of Primary tumor + cervical nodes Surgery / Radiation / Chemotherapy Sometimes palliation Cervical neck disease reduces survival by 50%

Lymphomas
Lymphomas are malignant cell infiltrations of the lymphatic system.
Once a malignancy begins in one part of the lymph system, it often spreads throughout the rest of the system before it is detected.
Lymphomas share similar symptoms such as painless swelling of the lymph nodes, fever and fatigue.
Broadly, they are classified as either non-Hodgkin's and Hodgkin's.

Types Of Neck Secondaries
I. Seconadaries with known PrimaryII. Secondaries with clinically unknown PrimaryIII. Secondaries with Occult Primary

I. Secondaries With Known Primary
Here secondary are present and primary identified in oral cavity, pharynx, larynx and other areas.
Biopsy of primary and FNAC of secondary are done.
Primary treated accordingly by surgery or radiotherapy.
Secondaries when mobile are treated by Radical lymph node block dissection.

II. Secondary With Clinically Unidentified Primary
FNAC of the secondary done and primary searched by investigations.
Investigations done are-a. Laryngo-pharyngoscopyb. Oesophagoscopyc. Bronchoscopyd. Blind biopsy from lat wall of pharynx, Fossa of
Rosenmuller,Pyriform Fossa,Tonsil and larynxe. FNAC of thyroid.f. CT Scan

III. Secondaries Of Neck With Occult Primary
Here secondary in the neck lymph node confirmed by FNAC but primary not revealed by any available investigations.
Initially secondaries if mobile treated with radical lyph node dissection and regular follow up done at three monthly interval till primary is revealed.
If lymph node when fixed is inoperable then external radiotherapy given to palliate pain and to prevent anticipated bleeding and sometimes it downstages the sewlling which can be delt with block dissection later.
Primary when revealed is treated accordingly.