Embed Size (px)
Citation preview
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 1/9
Perio-endo lesions
- As usual this script includes the slides, sentences that are written in Arial fon t are thing
that the Dr said, the rest are the same as the slides
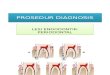
Anatomic consideration
There is an intimate relationship between the periodontium and pulpal tissues, as the
tooth develops and the root is formed, 3 main ways for communication are created:
1-Apical Foramen: It is the principal and the most direct route, bacterial and
inflammatory byproducts may exit/inter from/ to the root canal system, when theabscess is formed from it it's called periapical abscess or periodontal apicalabscess, which results from the infection of the pulp, and later on may result in
infection and resorption of the bone, and as you know the bone is considered as apart of the periodontal system.
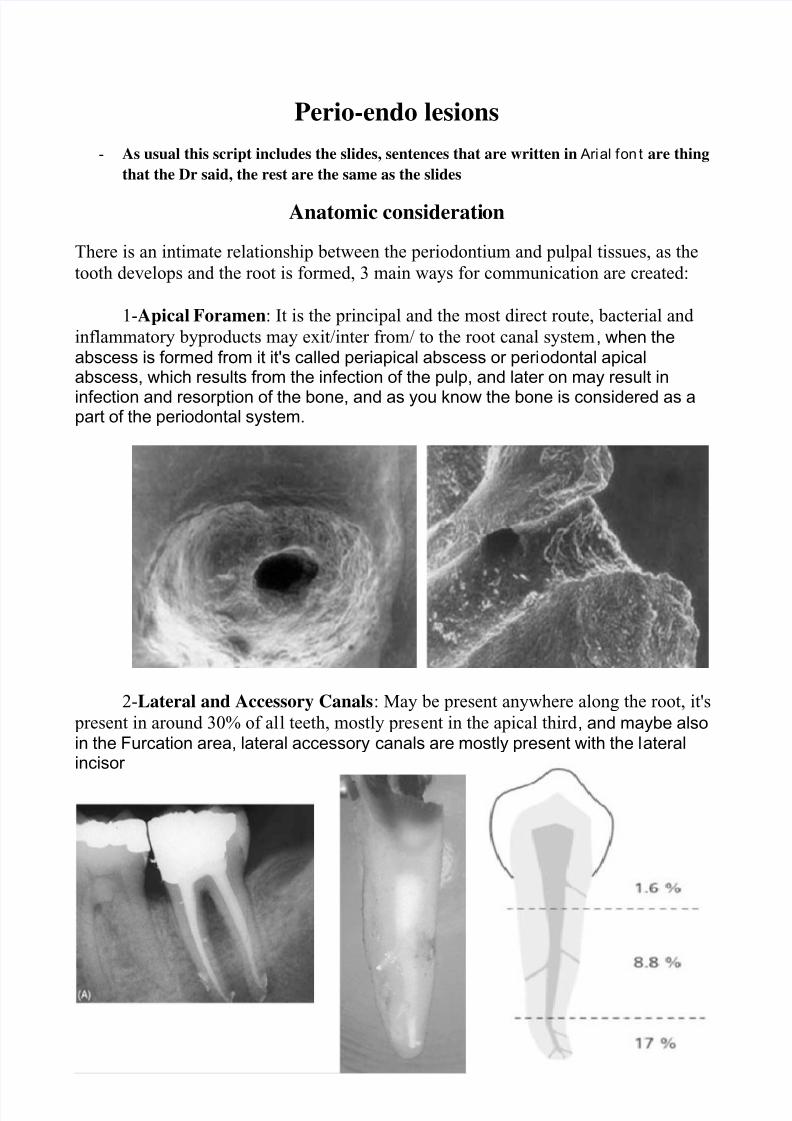
2-Lateral and Accessory Canals: May be present anywhere along the root, it's
present in around 30% of all teeth, mostly present in the apical third , and maybe alsoin the Furcation area, lateral accessory canals are mostly present with the lateralincisor
.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 2/9
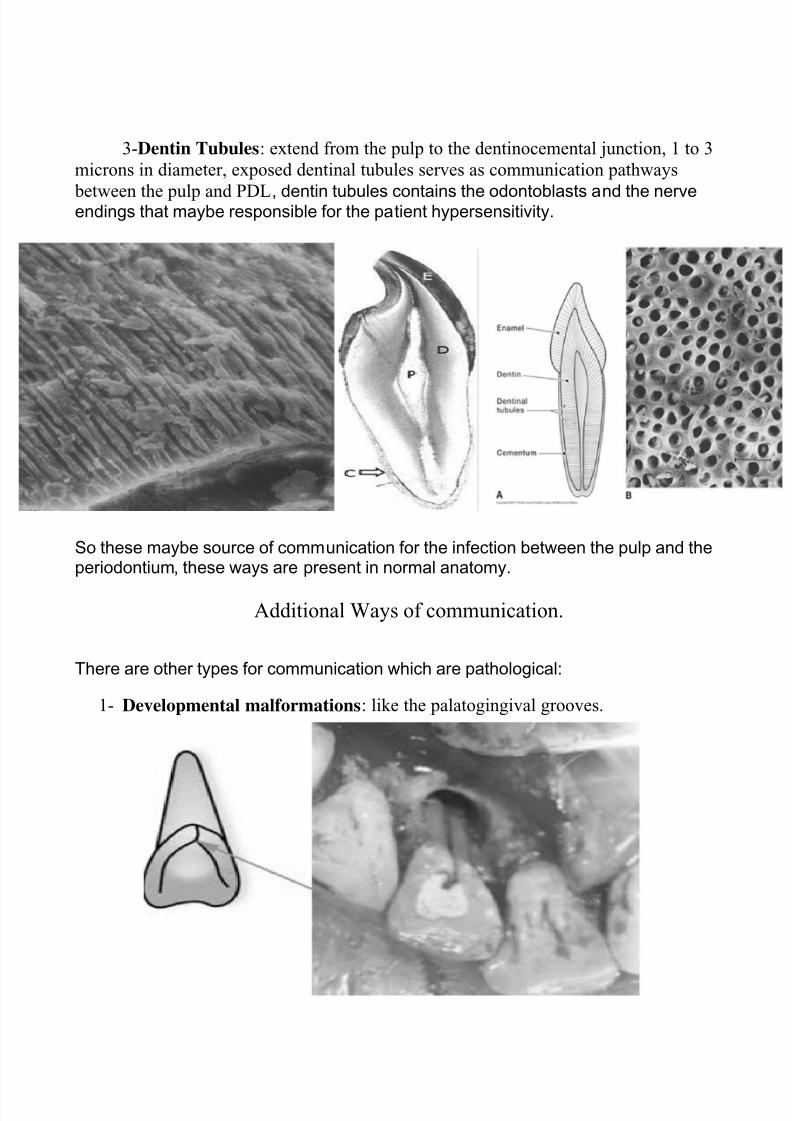
3-Dentin Tubules: extend from the pulp to the dentinocemental junction, 1 to 3
microns in diameter, exposed dentinal tubules serves as communication pathways
between the pulp and PDL, dentin tubules contains the odontoblasts and the nerveendings that maybe responsible for the patient hypersensitivity.
So these maybe source of communication for the infection between the pulp and theperiodontium, these ways are present in normal anatomy.
Additional Ways of communication.
There are other types for communication which are pathological:
1- Developmental malformations: like the palatogingival grooves.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 3/9
2- Perforations: these are either iatrogenic, because of carious lesions, resorption.
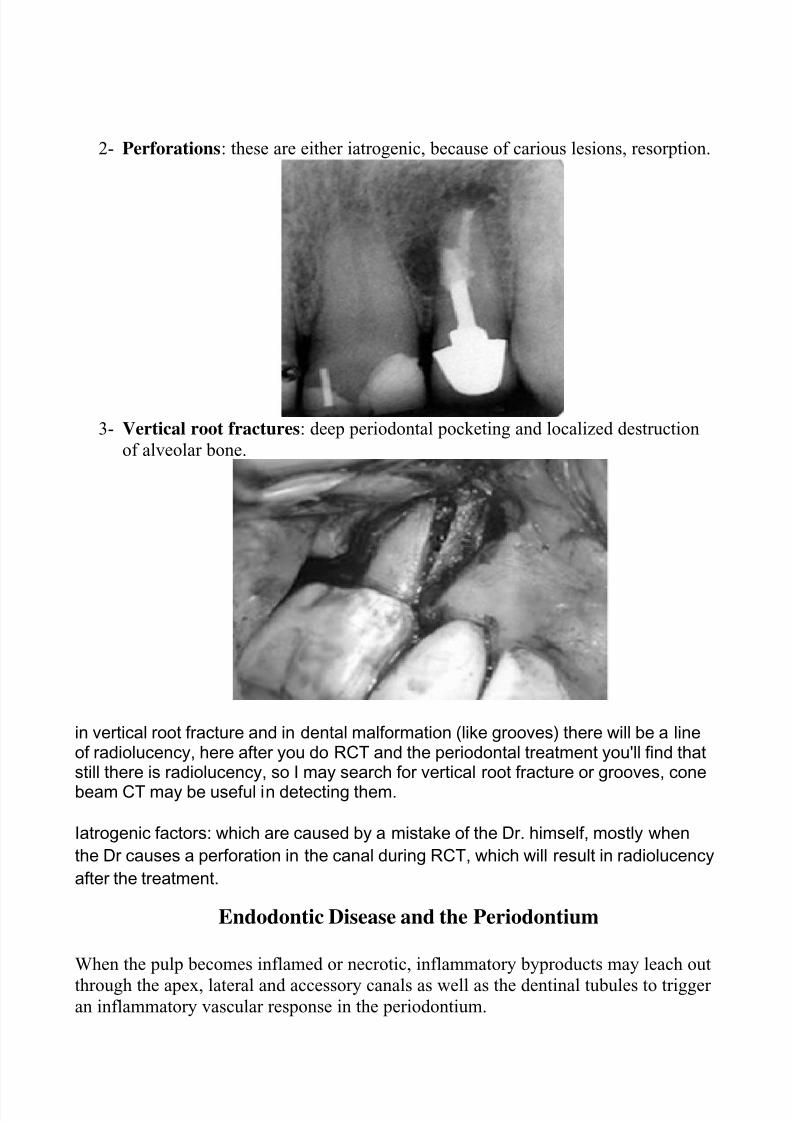
3- Vertical root fractures: deep periodontal pocketing and localized destruction
of alveolar bone.
in vertical root fracture and in dental malformation (like grooves) there will be a lineof radiolucency, here after you do RCT and the periodontal treatment you'll find thatstill there is radiolucency, so I may search for vertical root fracture or grooves, cone
beam CT may be useful in detecting them.
Iatrogenic factors: which are caused by a mistake of the Dr. himself, mostly when
the Dr causes a perforation in the canal during RCT, which will result in radiolucency
after the treatment.
Endodontic Disease and the Periodontium
When the pulp becomes inflamed or necrotic, inflammatory byproducts may leach out
through the apex, lateral and accessory canals as well as the dentinal tubules to trigger an inflammatory vascular response in the periodontium.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 4/9
Periodontal Disease and the Pulp:
The effect of periodontal inflammation on the pulp is controversial and conflicting
studies exist, It has been suggested that periodontal disease has no effect on the pulp,at least until it involves the apex, also, It has been reported that pulpal changes
resulting from periodontal disease are more likely to occur when the apical foramen is
involved
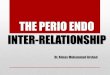
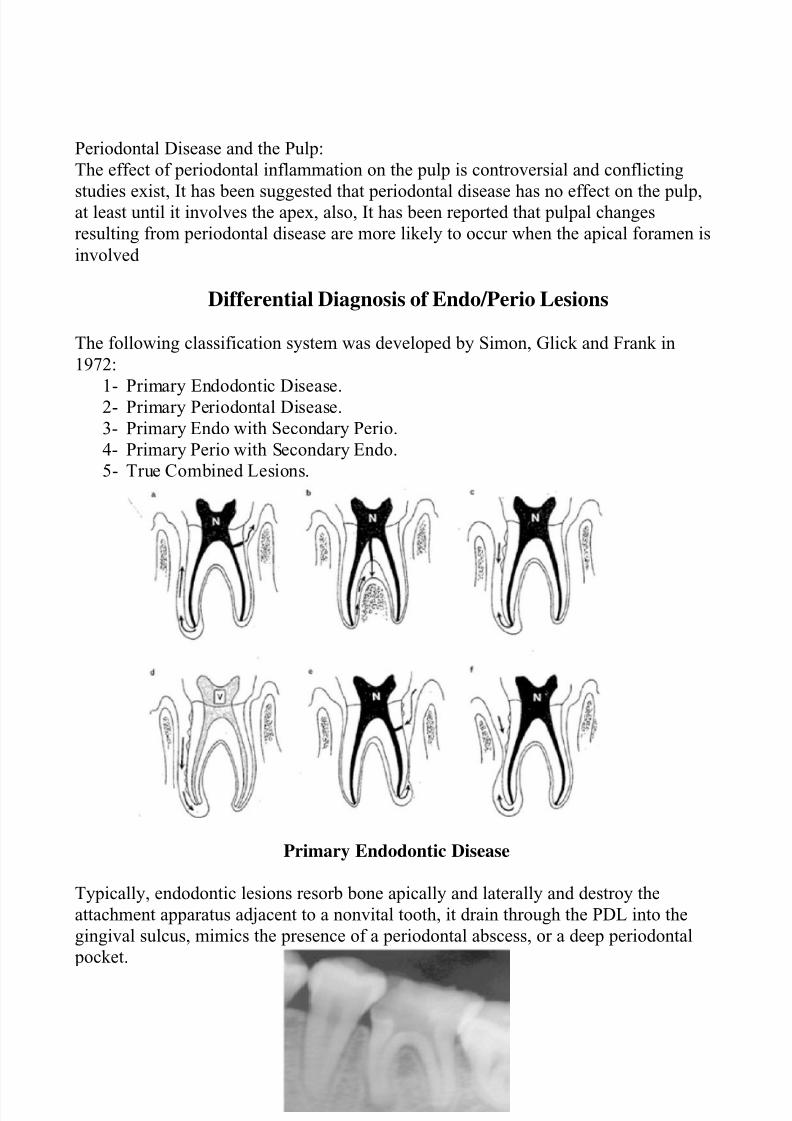
Differential Diagnosis of Endo/Perio Lesions
The following classification system was developed by Simon, Glick and Frank in
1972:
1- Primary Endodontic Disease.2- Primary Periodontal Disease.
3- Primary Endo with Secondary Perio.
4- Primary Perio with Secondary Endo.
5- True Combined Lesions.
Primary Endodontic Disease
Typically, endodontic lesions resorb bone apically and laterally and destroy the
attachment apparatus adjacent to a nonvital tooth, it drain through the PDL into the
gingival sulcus, mimics the presence of a periodontal abscess, or a deep periodontal
pocket.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 5/9
Periapical abscess:
Sinus tract.
Periodontal pocket (deep pocket). Furcation area (furcation defect).
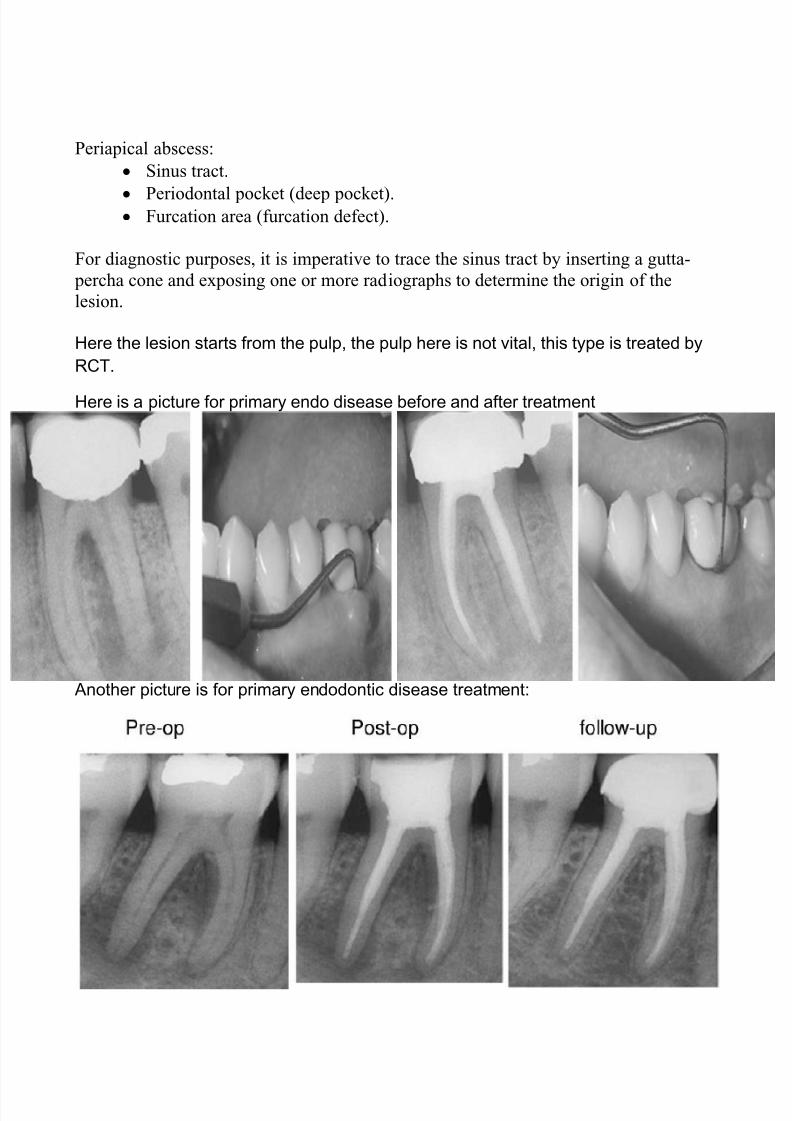
For diagnostic purposes, it is imperative to trace the sinus tract by inserting a gutta-
percha cone and exposing one or more radiographs to determine the origin of the
lesion.
Here the lesion starts from the pulp, the pulp here is not vital, this type is treated by
RCT.
Here is a picture for primary endo disease before and after treatment
Another picture is for primary endodontic disease treatment:
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 6/9
Primary Periodontal Disease
- Dental plaque.
- Pulp tests (vital tooth).- Periodontal pockets are wider, and are generalized.
When it starts from the periodontium (like if we have deep pocket and attachment
loss), the pulp here is mostly vital, this type is treated by scaling and root planing.
In these 2 types we have problem in 1 of them only.
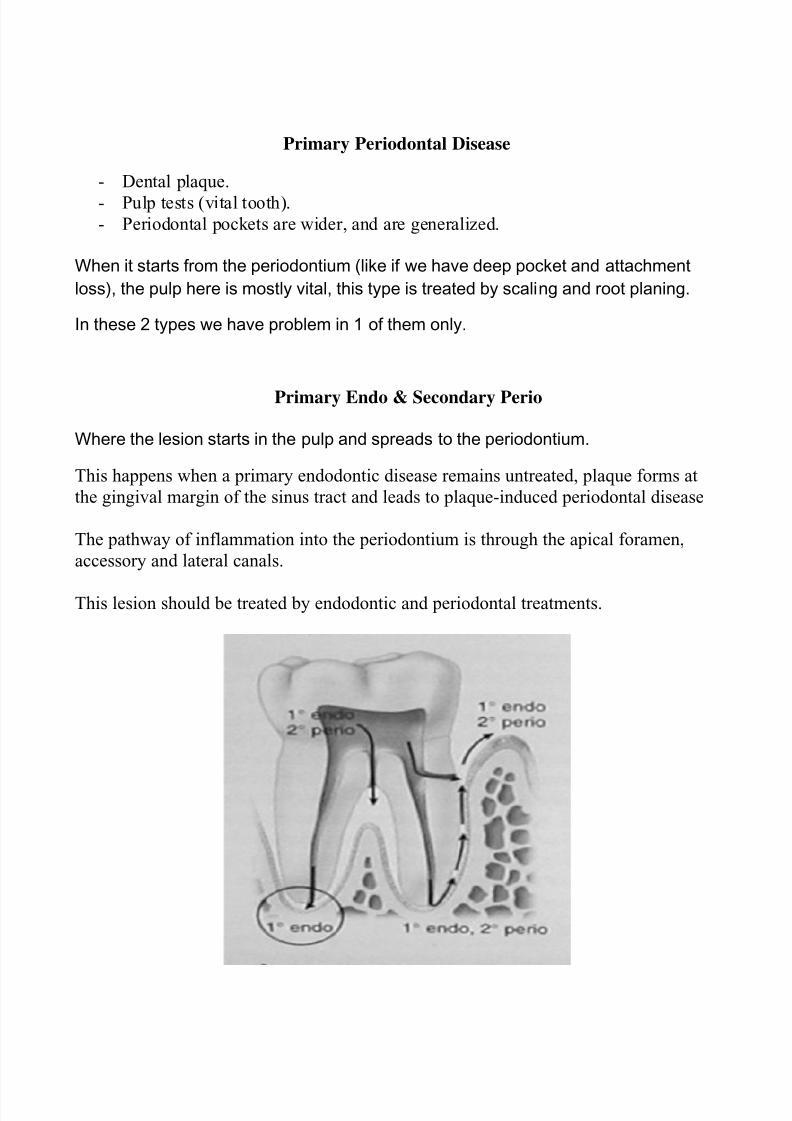
Primary Endo & Secondary Perio
Where the lesion starts in the pulp and spreads to the periodontium.
This happens when a primary endodontic disease remains untreated, plaque forms at
the gingival margin of the sinus tract and leads to plaque-induced periodontal disease
The pathway of inflammation into the periodontium is through the apical foramen,
accessory and lateral canals.
This lesion should be treated by endodontic and periodontal treatments.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 7/9
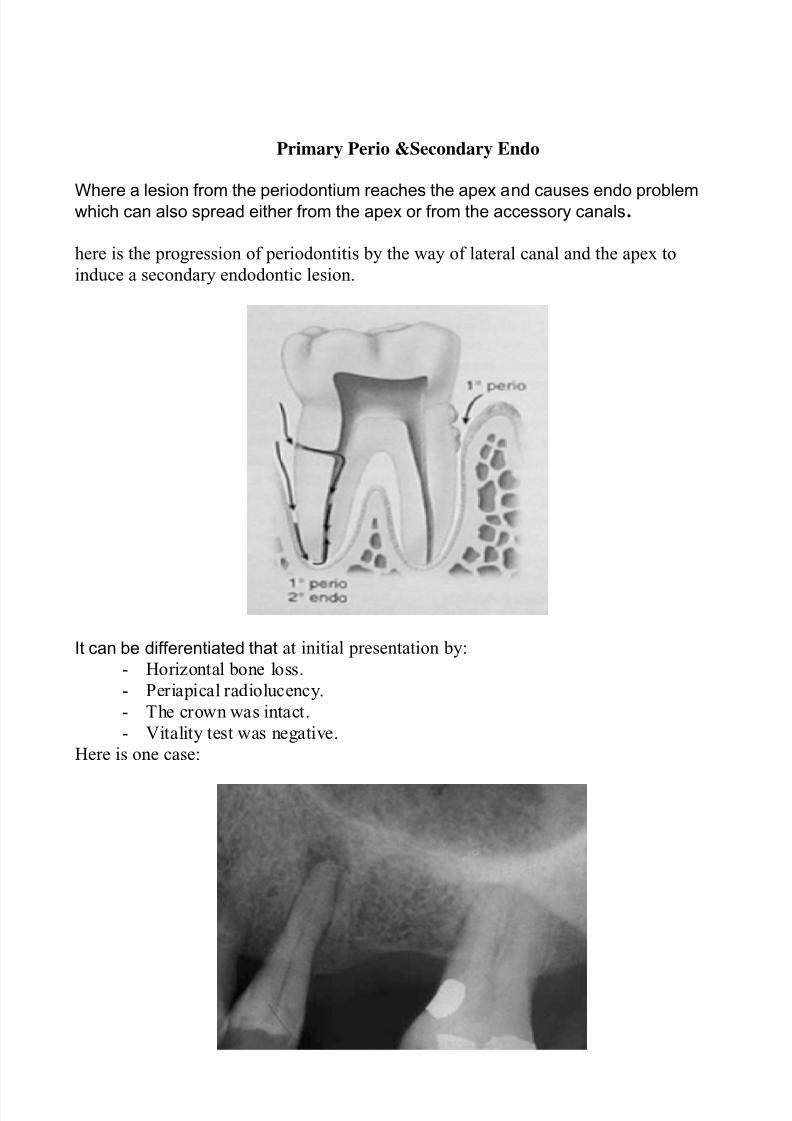
Primary Perio &Secondary Endo
Where a lesion from the periodontium reaches the apex and causes endo problemwhich can also spread either from the apex or from the accessory canals.
here is the progression of periodontitis by the way of lateral canal and the apex to
induce a secondary endodontic lesion.
It can be differentiated that at initial presentation by:
- Horizontal bone loss.
- Periapical radiolucency.
- The crown was intact.
- Vitality test was negative.
Here is one case:
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 8/9
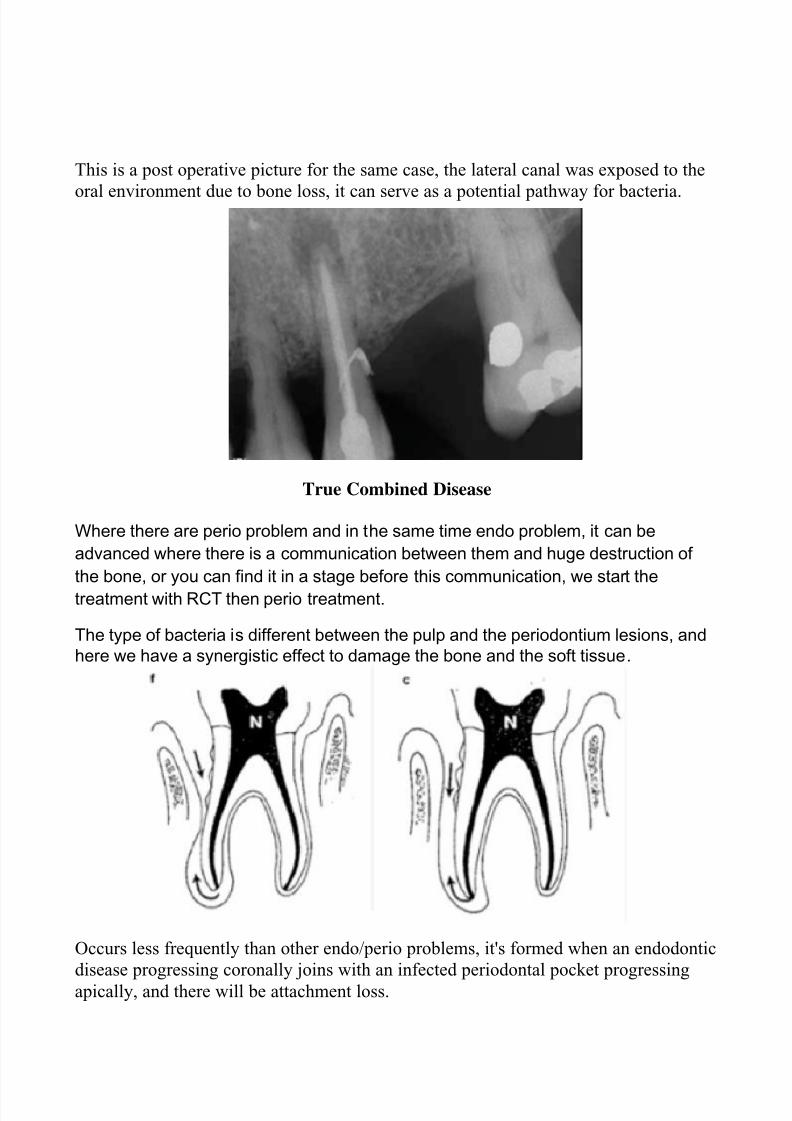
This is a post operative picture for the same case, the lateral canal was exposed to the
oral environment due to bone loss, it can serve as a potential pathway for bacteria.
True Combined Disease
Where there are perio problem and in the same time endo problem, it can be
advanced where there is a communication between them and huge destruction of
the bone, or you can find it in a stage before this communication, we start the
treatment with RCT then perio treatment.
The type of bacteria is different between the pulp and the periodontium lesions, and
here we have a synergistic effect to damage the bone and the soft tissue.
Occurs less frequently than other endo/perio problems, it's formed when an endodontic
disease progressing coronally joins with an infected periodontal pocket progressing
apically, and there will be attachment loss.
8/13/2019 Perio Endo Lesions3
http://slidepdf.com/reader/full/perio-endo-lesions3 9/9
Clinical exam revealed coronal color change and pus exuding from the gingival
sulcus. Pulp vitality tests were negative.
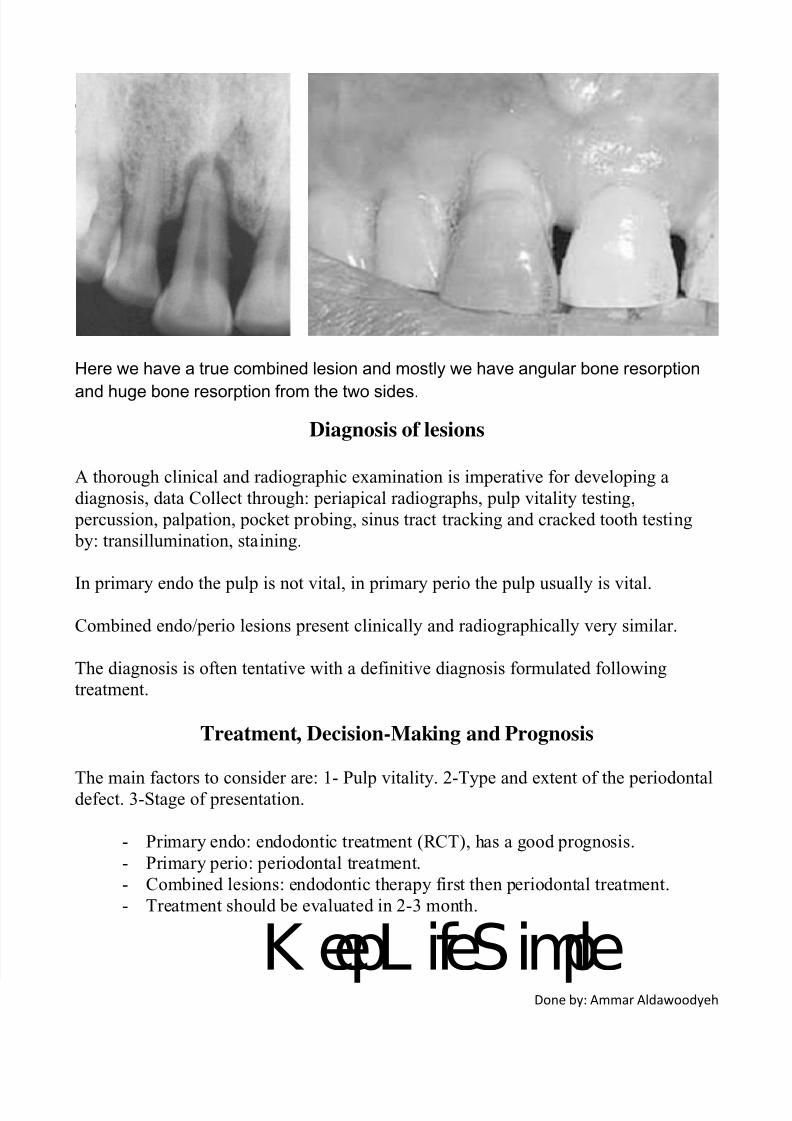
Here we have a true combined lesion and mostly we have angular bone resorption
and huge bone resorption from the two sides.
Diagnosis of lesions
A thorough clinical and radiographic examination is imperative for developing a
diagnosis, data Collect through: periapical radiographs, pulp vitality testing,
percussion, palpation, pocket probing, sinus tract tracking and cracked tooth testing
by: transillumination, staining.
In primary endo the pulp is not vital, in primary perio the pulp usually is vital.
Combined endo/perio lesions present clinically and radiographically very similar.
The diagnosis is often tentative with a definitive diagnosis formulated following
treatment.
Treatment, Decision-Making and Prognosis
The main factors to consider are: 1- Pulp vitality. 2-Type and extent of the periodontaldefect. 3-Stage of presentation.
- Primary endo: endodontic treatment (RCT), has a good prognosis.
- Primary perio: periodontal treatment.
- Combined lesions: endodontic therapy first then periodontal treatment.
- Treatment should be evaluated in 2-3 month.
K eepL ifeSimpleDone by: Ammar Aldawoodyeh