Embed Size (px)
Citation preview


THE HEALTH of the periodontium is important to the proper function of a tooth.
The periodontium includes the gingiva, cementum, periodontal ligament (PDL), and alveolar bone.
Disease that affects the periodontium usually is a result of the direct extension of pulpal disease or due to apical progression of periodontal disease.

When the pulp becomes infected, the disease can progress beyond the apical foramen and inflame the PDL.
The inflammatory process results in replacement of the periodontal ligament by inflammatory tissue.
Without proper treatment, the inflammatory response can cause resorption of the alveolar bone, cementum, and dentin.

Besides going through the apical foramen, pulpal disease can progress through lateral canals.
Lateral canals are seen mostly in the apical third of the root and in the furcation area of molars.
Pulp disease may cause an inflammatory response of the PDL at the opening of lateral canals, resulting in a lateral radiolucency on the root.

The inflammatory response at the lateral canals may extend crestally along the lateral aspects of the root and ultimately involve the furcation or crestal area of the attachment apparatus.
The effect of periodontal disease on the pulp is not as clear-cut as the effect of pulpal disease on the periodontium.
Periodontal inflammation may exert a direct effect on the pulp through the same lateral canal or apical foramen pathways.

The normal pathways of communication between the endodontium and the periodontium (1 -the apical foramen, 2, 3 - lateral and accessory canals)

The endodontium and periodontium are closely related and diseases of one tissue may lead to secondary diseases in the other.
The differential diagnosis of endodontic and periodontal diseases can sometimes be difficult but it is of vital importance to make a correct diagnosis so that the appropriate treatment can be provided.

Pulpal infection can drain through the periodontal ligament space and give an appearance of periodontal destruction, termed retrograde periodontitis.
Both pulpal and periodontal infections can coexist in the same tooth, termed combined lesions, where the treatment depends on the degree of involvement of the tissues.
Both endodontic and periodontal diseases are caused by a mixed anaerobic infection.

X-ray image of an endodontic-periodontal lesion caused by an internal root resorbtion.
Pre-operatory image of the same lesion while measuring the initial pocket depth.

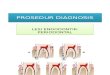
a) Primary endodontic lesion with drainage through
the periodontal ligament.
b) Primary endodontic lesion with secondary periodontal
involvement.
c) Primary periodontal lesion.
d) Primary periodontal lesion with secondary endodontic
involvement.
e) Combined endodontic-periodontal lesion.


An acute exacerbation of a chronic apical lesion on a tooth with a necrotic pulp may drain coronally through the periodontal ligament into the gingival sulcus.
This condition may mimic, clinically, the presence of a periodontal abscess.
a deep narrow probing defect is noted on just one aspect of the tooth root .

For diagnosis purposes, it is imperative for the clinician to insert a gutta-percha cone into the sinus tract and to take one or more radiographs to determine the origin of the lesion.
When the pocket is probed, it is narrow and lacks width.
Primary endodontic diseases usually heal following root canal treatment.

The root canal system primarily becomes infected as a result of dental caries, traumatic injuries and coronal microleakage.
Pulp inflammation or necrosis may lead to an inflammatory response in the periodontal ligament at the apical foramen or foramina or at the site of a lateral or accessory canal.

Such a lesion may result in a localized or diffuse swelling that may occasionally involve the gingival attachment.
Long-term existence of the defect has resulted in deposits of plaque and calculus in the pocket with subsequent advancement of the periodontal disease.
After adequate root canal treatment, lesions resulting from pulpal necrosis resolve an exceptionally high percentage of the time.

The integrity of the periodontium will be reestablished if root canal treatment is done well.
If a draining sinus tract through the periodontal ligament is present before root canal treatment, resolution of the defect that can be probed is expected

Endodontic-periodontal lesion with primary endodontic lesions and secondary periodontal involvement of 16

These lesions are primarily caused by periodontal pathogens. In this process, chronic periodontitis progresses apically along the root surface. In most cases, pulp tests indicate a clinically normal pulpal reaction. There is frequently an accumulation of plaque and calculus and the pockets are wider. The prognosis depends on the stage of periodontal disease and the efficacy of periodontal treatment. The pulp may remain vital but may show some degenerative changes over time.

The apical progression of a periodontal pocket may continue until the apical tissues are involved.
In this case, the pulp may become necrotic as a result of infection entering via lateral canals or the apical foramen.
In single-rooted teeth, the prognosis is usually poor.
In molar teeth, the prognosis may be better.

The pulp response to cementum and dentin removal and exposure of patent dentinal tubules by periodontal root planning will vary with the remaining dentin thickness.
Unless dentin removal is excessive, pulp response will be negligible.
Although the pulp is exposed to a bacterial challenge through patent dentinal tubules, it is quite capable of repair and healing.
Production of reparative dentin and reduced canal diameter may result, but pulp tissue remains relatively unaffected.

Primary periodontal lesions with secondary endodontic involvement lesion

These lesions occur when an endodontically induced periapical lesion exists at a tooth that is also affected by marginal periodontitis.
The tooth has a pulpless, infected root canal system and a co-existing periodontal defect.
This is particularly true in single-rooted teeth. In molar teeth, root resection can be considered as a treatment alternative if not all roots are severely involved

Endodontic and periodontal diseases are occurring independently of each other.

Endodontic disease is occurring secondarily to a periodontal condition due to bacterial retrograde from distal root

Periodontal disease at the furcation is occurring secondarily to a pinpoint perforation at the furcation floor.

5 mm interproximal periodontal pocket on teeth #16 and 17 and inadequate endodontic treatment on tooth #17.

Pulpal necrosis subsequent to periodontal treatment and significant osseous loss. No other aetiology could be shown.

The major connections between periodontal and pulpal tissues are the apical foramina.
In addition to the apical foramina and accessory canals, there is a third possible route for bacteria and their products, the dentinal tubules.


They are serious complications during dental treatment and have a rather poor prognosis. Perforations may be produced by powered rotary instruments during the attempt to gain access to the pulp or during preparation for a post. Improper manipulation of endodontic instruments can also lead to a perforation of the root.

The second group of artificial pathways between periodontal and pulpal tissues are vertical root fractures. Vertical root fractures are caused by trauma and have been reported to occur in both vital and non-vital teeth. In vital teeth, vertical fractures can be continuations of coronal fractures in the "cracked tooth syndrome," or can occur solely on root surfaces.

A thorough visual examination of the lips,
cheeks, oral mucosa, tongue, palate and
muscles should be carried out .
The alveolar mucosa and the attached gingiva
are examined for the presence of
inflammation,ulcerations or sinus tracts.
Frequently, the presence of a sinus tract is
associated with a necrotic pulp.

Palpation is performed by applying firm digital
pressure to the mucosa covering the roots and
apices .
With the index finger the mucosa is pressed
against the underlying cortical bone .
This will detect the presence of periradicular
abnormalities or ''hot'' zones that produce painful
response to digital pressure .

Although this test does not disclose the condition
of the pulp, it indicates the presence of a
periradicular inflammation.
An abnormal positive response indicates
inflammation of the periodontal ligament that
may be either from pulpal or periodontal origin .
The sensitivity of the proprioceptive fibers in an
inflamed periodontal ligament will help identify
the location of the pain .
This test should be performed gently, especially
in highly sensitive teeth .

Tooth mobility is directly proportional to the integrity of the attachment apparatus or to the extent of inflammation in the periodontal ligament. Hypermobility is quite common in cases of
primary endodontic involvement and should not be confused with true mobility caused by periodontal destruction. In cases of primary endodontic pathology, the
mobility resolves within a week of initiating endodontic therapy.

Interpretation of discrete periapical or lateral lesions and discrete periodontal lesions is of clinical importance in suggesting the cause of the lesion and the proper diagnostic procedures to follow to confirm the cause.
Often, the initial phases of periradicular bone resorption from
endodontic origin are confined only to cancellous bone. Therefore, it cannot be detected unless the cortical bone is
also affected. However, when there is radiographic evidence that bone loss
extends from the level of crestal bone to or near the apex of the tooth, the radiograph is of little value in determining the cause.

Endodontic or periodontal disease may
sometimes develop a fistulous sinus track.
Inflammatory exudates may often travel through
tissues and structures of minor resistance and
open anywhere on the oral mucosa or facial skin.
Intraorally, the opening is usually visible on the
attached buccal gingiva or in the vestibule.

Fistula tracking is done by inserting a semirigid
radiopaque material into the sinus track until
resistance is met.
Commonly used materials include gutta-percha
cones or pre-softened silver cones.
A radiograph is then taken, which reveals the
course of the sinus tract and the origin of the
inflammatory process .

The most commonly used pulp vitality tests
are cold test, electric test, blood flow tests
and cavity test.
The presence or absence of vital tissue in a
tooth with a single canal can be determined
with confidence with the current pulp-testing
procedures.
The same degree of confidence cannot be
ascribed to positive pulp test responses in a
tooth with multiple canals.

In general, when primary disease of one tissue, i.e. pulp or periodontium, is present and secondary disease is just starting, treat the primary disease. When secondary disease is established and chronic, both primary and secondary diseases must be treated. By and large, endodontic therapy precedes periodontal therapy. Periodontal therapy may or may not be required, depending on disease status. The complete healing of destroyed periodontal support can be expected following the treatment of pulpal pathology.

It is important to realize that it is clinically not possible to determine the extent to which one or the other of the two disorders (endodontic or periodontal) has affected the supporting tissues.
Therefore, the treatment strategy must be first to focus on the pulpal infection and to perform debridement and disinfection of the root canal system.

The second phase includes a period of observation, whereby the extent of periodontal healing resulting from the endodontic treatment is followed.
Reduced probing depth can usually be expected within a couple of weeks while bone regeneration may require several months before it can be radiographically detected.
Thus, periodontal therapy, including deep scaling with and without periodontal surgery, should be postponed until the result of the endodontic treatment can be properly evaluated.


It is a known fact that root canal infection significantly affects periodontal healing.
Pocket depth reduction is significantly lesser in the presence of canal infection.
Removal of cementum will expose dentinal tubules, which means that if there are bacteria in the canal, it could promote inflammatory resorption.
It may also expose periodontal tissues to toxic medicaments if used in canal.
This is not so critical in areas with recession.

Early initiation of endodontic treatment ensures that the cementum layer is kept intact until root canal infection is eliminated. Because there would be no exposed dentine on the root surface, there is reduced chance of root resorption and improved periodontal healing. On the other hand, if the root canal filling does not have a good seal then the filled canals may be reinfected from periodontal bacteria.

The risk of infection is heightened if periodontal treatment is delayed, especially when a "combined lesion with communication" exists between the two sites.
Sterility is more likely while there is a medicated dressing like calcium hydroxide in the canal.
Hence, in some cases, it might be prudent to delay the root filling until the periodontal infection has been eliminated.

This would be required when:
both endodontic and periodontal infection are present simultaneously.
The true combined endodontic and periodontic lesion requires an accurate diagnosis.
This is often a difficult diagnosis and therefore requires reevaluation after either the periodontal or endodontic problems are treated.
In such cases, if there is no communication, then complete the endodontic therapy first and initiate periodontal treatment soon after.
When lesions communicate, it makes sense to commence endodontic treatment first and medicate canals until prognosis is known.