Embed Size (px)
DESCRIPTION
Perioperative Care of Elderly Patients with Hip Fracture. J Rush Pierce Jr, MD, MPH Hospitalist Best Practices Conference May 5, 2009. - PowerPoint PPT Presentation
Citation preview

Perioperative Care of Elderly Patients with Hip Fracture
J Rush Pierce Jr, MD, MPH
Hospitalist Best Practices Conference
May 5, 2009

A 78 year old woman fell at church. She complained of left hip pain and was unable to arise. EMS was activated and transported her to the ED where x-rays disclose a hip fracture.
She has a history of hypertension, hyperlipidemia, and coronary artery disease. She suffered a myocardial infraction seven years ago. She has not had any chest pain or symptoms of CHF. Her medicines are lisinopril, atenolol, aspirin, and atorvastatin. She lives with her husband who reports that she is active, does housework and walks everyday. She has had some memory difficulty and has poor vision.
On examination she complains of pain, The left leg is external rotated. Heart and lung exam is normal. She has no edema. Her Folstein MMSE is 23 and Mini COG is 2.
Her laboratory reveals a normal CBC and electrolytes. BUN is 25 and creatinine is 1.0. CXR is normal. EKG shows Q waves in limb leads 2, 3 , and AVF.

Hip fracture in the elderly
How will this likely affect her life? What evaluation does she need before
surgery? What is the best evidence based care?
Preoperative Operative Postoperative
What can we do to prevent another hip fracture in the future?

Hip Fracture – epidemiology & natural history 350,000 hip fxs yearly in USA Lifetime risk for hip fx = 17.5% ♀, 6.0% ♂ Mortality:
5% during index hospitalization 13% @ 3 mos 24% @ one year
50% require assistance device @ one year 25% in LTC @ one year

What type of pre-operative evaluation does she need?

Assessing the cause of the fall Did she have syncope?
Most falling in the elderly not due to syncope Syncope suggest possibility of cardiac
arrhythmias
Has she fallen before (6 months)? Suggest frailty and poorer prognosis Medication review especially important

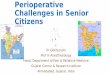
Causes of syncope in the elderly
Ungar A, et al. J Amer Geriatrics Soc 2006;54:1531-6
“In contrast with previous reports, prodromic symptoms were remarkably frequent in this older population but proved to be poorly specific and, hence, of limited utility in orienting the diagnosis toward neurally mediated syncope.”

“She needs Clearance”

“We need clearance!”

Preoperative Risk Assessment






Preoperative management
Traction – no benefit with regard to pain or ease of fracture reduction
Pressure sore prevention Foam mattress (RR = 0.34) Alternating pressure mattress (RR=0.20)
Beta blockers – recent meta-analysis showed no benefit for non-cardiac surgery (Lancet. 2008 Dec 6;372:1962-76)

Meta-analysis of peri-operative beta blockers 33 trials included 12,306 patients. β blockers were not associated
with any significant reduction in the risk of all-cause mortality, cardiovascular mortality, or heart failure, but were associated with a decrease (odds ratio [OR] 0·65, 95% CI 0·54–0·79) in non-fatal myocardial infarction (number needed to treat [NNT] 63) and decrease (OR 0·36, 0·26–0·50) in myocardial ischaemia (NNT 16) at the expense of an increase (OR 2·01, 1·27–3·68) in non-fatal strokes (number needed to harm [NNH] 293). The beneficial effects were driven mainly by trials with high risk of bias. For the safety outcomes, β blockers were associated with a high risk of perioperative bradycardia requiring treatment (NNH 22), and perioperative hypotension requiring treatment (NNH 17). We recorded no increased risk of bronchospasm.
(Lancet. 2008 Dec 6;372:1962-76)

Her children are coming from out of state and ask that surgery be delayed for two days until they arrive.
What is the best timing of surgery in this woman?

Timing of Surgery Early repair (24 – 48 hrs) [Evidence based,
mostly level 2] ↓ one-year mortality ↓ pressure sores (RR= 0.46) ↓ major medical complication (RR=0.26) Reduced LOS by 1.94 days
Reasons to delay surgery [Opinion] Acute coronary syndrome Acute CVA Sepsis Severe hypoxemia

Hip fracture in the elderly - anatomy Femoral neck (1/3)
Non displaced– usually internal fixation with nail/pin
Displaced - hemiarthroplasty
Intertrochanteric (2/3) Open reduction with
internal fixation (ORIF)
Zuckerman. N Engl J Med 1996;23:1519-1525

Intertrochanteric fracture
Zuckerman. N Engl J Med 1996;23:1519-1525

Zuckerman. N Engl J Med 1996;23:1519-1525
Non-displaced femoral neck fracture

Displaced femoral neck fracture
Zuckerman. N Engl J Med 1996;23:1519-1525

Parker and Gurusamy. Disability and Rehab 2005; 27:1045 – 1051.

Operative management Type of surgery - arthroplasty for displaced
femoral neck fxs Pre-operative antibiotics (1 or 2 doses of long-
acting cephalosporin) Decreased post-op wound infection (RR=0.36) Decreased post-op UTI (RR=0.66)
Regional anesthesia Decreased 30 day mortality (RR=0.69) Decreased proximal DVT (RR=0.64) Decreased post-op pneumonia (RR=0.61)

Post-operative management Pain management
Decreased cardiac complications with epidural (1 study); better pain management with epidural
Expert opinion: avoid meperidine & propoxyphene Urinary catheter
UTI occurs in 25% Little evidence about catheter type and UTI Post-op urinary retention – normal voiding returns
4.3 days sooner with intermittent vs. indwelling catheter (1 study)

Thromboembolic prophylaxis Prevalence: DVT = 48%; fatal PTE = 4 -14% Benefit to all modalities (RR~0.6); no one
clearly preferred, most use an anticoagulant Heparin, LMWH, low dose coumadin, ASA + SCD
Begin preoperatively Heparin, coumadin - day before LMWH – not before 12 hrs preoperatively
Duration – not well studied; suggest need for 6 weeks

Post-operative management (cont) Nutrition
Oral supplements reduced LOS (one study) Multidisciplinary team
No level 1 benefit shown but difficult to study

Rehab and Recovery Early mobilization important – 24 hours
[evidence based] Earlier discharge ↓ costs ↑ functional status
Gait training and occupational therapy decrease risk of recurrence [evidence based]
Organized rehab assoc with 10% ↓ in death and institutionalization - pts with mild dementia most likely to benefit [evidence-based]

Is post-operative delerium likely in this woman?

Postoperative delerium
Common 3.8% low risk (0 risk factors) 11% middle risk (1 - 2 risk factors) 37% high risk (3 – 4 risk factors)
Risk factors: Visual impairment (>20/70) MMSE < 24 pre-op APACHE II >16 BUN/creat ratio >= 18
Kalisvarrt et al: JAGS 2006; 54:817-822.

Postoperative delerium
Pre-existing dementia very common, but often not diagnosed
Pre-operative Mini-Cog (0-2 + abnormal Clock drawing test) five times as likely to develop

Postoperative delerium – assessment and treatment Look for treatable causes
Hypoxemia Electrolyte abnormalities Hypotension
Avoid sedative/hypnotics, drugs with anticholinergic properties, narcotics
Reassurance, reorientation, geriatric nursing care
Huddleston & Whitford: Mayo Clin Proc 2001; 76:295-298.

How do we prevent this from happening again?

Hip fracture – prevention of recurrence Almost all accompanied by osteopenia or
osteoporosis Calcium and Vit D in hospital Consider bisphosphonates Hold estrogens (thromboembolic potential)
Fall prevention

Falls in the Elderly - Epidemiology 30% community dwelling adults over 65
years old fall at least once each year Over 50% nursing home residents fall yearly Over 10% of falls result in serious injury About 5 – 6 % of Medicare expenditures
result of falls

Medications associated with hip fractures in epidemiologic studies
Benzodiazepines Antidepressants Antipsychotics

Fall prevention – evidence of benefit Education – not helpful Exercise programs (balance training >
strength or endurance) – benefit only for targeted community dwelling adults
Environmental assessment – benefit outside home as well as in home
Withdrawal of psychotropic drugs – but studies show that most patients resume withdrawn medications within one year

Fall prevention – extent of benefit Most studies show modest (10 -15%
reduction in falls) Best multi-component intervention programs
show 35% reduction (30% - 20%) Repeated falling in the elderly often predicts
general physical and cognitive decline – review living situation and driving

Clinical Bottom Line Telemetry for syncope [opinion] “Clear” almost all patients Push for early surgery (24-48 hrs) and regional
anesthesia Pre-operatively order a mattress, peri-operative
antibiotics , DVT prophylaxis Post-operatively get Foley out; ambulate early;
order PT/OT; avoid meperidine & propoxyphene; anticipate delerium; order Ca and Vit D; consider bisphosphonates; rehab