-
8/20/2019 Perioperative Fluid Therapy.ppt
1/36
Perioperative Fluid Management
Oleh
Hasanuddin
Pembimbing
Dr. Abd. Wahab, SpAn
-
8/20/2019 Perioperative Fluid Therapy.ppt
2/36
The principle of uid therapy is tomaintain tissue
perfusion
How much should we inuse!
What luids should we use!
How should we monitor luid replacement!
So…
-
8/20/2019 Perioperative Fluid Therapy.ppt
3/36
Total Body Water
• Total body water varies between 55-70% of BW
• Depend on : - age
- se
!ale " fe!ale #!ore fat$
• TBW approi!ately 0% of BW
• & person of 0 'gs (as 0 0% ) * +
-
8/20/2019 Perioperative Fluid Therapy.ppt
4/36
"ntra #ellular Space
# e l l m e
m b r a n e
" n
t r a v a s c u l a r S p a c e
RBC
# a p i l l a r $ m e m b r a n e
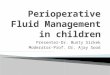
Distribution o bod$ luids
total bod$ water %&' (W
)*'
*' +&'
a - )+& me/l
0 -
+
me/l , a - ) + & m e . / l
0 - + m e . / l
"nterstitial
Space
#olloid cr$stalloids
1lucose solution
a - 2 me/l
0 - )*)
me/l
-
8/20/2019 Perioperative Fluid Therapy.ppt
5/36
,o!position of flid
.o!part!ents
plasma interstitial intracellular
CationsNa 140 146 12K 4 4 150Ca 5 3 10Mg 2 1 7
Anions
Cl 103 104 3HCO 24 27 10O4 1 1 !H"O4 2 2 116"rotein 16 5 40
-
8/20/2019 Perioperative Fluid Therapy.ppt
6/36
3$pe o Fluid 4oss in Perioperative Periode
5 (asal luid reuirements
5 Fluid loses on drainage, istel, maagslang6
5 7edistributive and evaporativesurgical losses
5 Fluid shits 83hird space losses65 (leeding
How much should we inused !
-
8/20/2019 Perioperative Fluid Therapy.ppt
7/36
10 #g $ 4 %lg ' 40 %l
10 #g $ 2 %lg ' 20 %l
50 #g $ 1 %lg ' 50 %l
110 %ls & (r )ggest to *reo*erati+e re(idrate ,it(
gl)#osa t(at -an .
1/ de-rease sel)ler ins)lin resistan-e *ost o*erati
2/ n-rease %)s-le ton)s *ost o*erati
/ole of -1-2
/e3ire!ents for 70'g !an
-
8/20/2019 Perioperative Fluid Therapy.ppt
8/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
9/36
7edistributive and evaporative surgical luid
losses
Degree o tissue trauma Additional luidreuirement
Minimal 8 herniorrhaph$6 & 9 : cc/ ;g/hour
Moderate8 cholec$stectom$6
: 9 + cc/;g/ hour
Severe 8 bowel resection6 + 9 2 cc/;g/hour
-
8/20/2019 Perioperative Fluid Therapy.ppt
10/36
#lass " #lass "" #lass """ #lass "<
(lood loss =p to >*& >*&?)*&&
)*&&?:&&& @:&&&
(lood loss
8 '(
-
8/20/2019 Perioperative Fluid Therapy.ppt
11/36
#ourse o h$povolaemic shoc; in absence otherap$
De.o!pen-sation
,o!pen-sation
Bleeding
Heart rate%in
(lood pressure mmHg
9rreversi-bility
3hree Shoc; phases
Bloodpressre
0
*&
)&&
)*&
-
8/20/2019 Perioperative Fluid Therapy.ppt
12/36
Problems with Perioperative Fluid
7eplacement
• We canEt accuratel$ evaluate blood volume
• We canEt accuratel$ identi$ luid overload
• We canEt accuratel$ identi$ h$povolemia
•
We canEt accuratel$ evaluate tissue perusion
-
8/20/2019 Perioperative Fluid Therapy.ppt
13/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
14/36
#omplication
• 7is;s o inadeuate resuscitation
4ie?threatening G lactic acidosis, A7F, MOF
on?atal G thirst$, drows$ness, di$, nausea I
-
8/20/2019 Perioperative Fluid Therapy.ppt
15/36
/estri.tive vs +iberal
-
8/20/2019 Perioperative Fluid Therapy.ppt
16/36
}
-
8/20/2019 Perioperative Fluid Therapy.ppt
17/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
18/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
19/36
Starling #apillar$ Forces
5 3wo orces regulate bul; low across capillariesG
9 H$drostatic 8HP6 and osmotic pressure 8OP6
5 3hese orces eist in two luid compartmentsG
9 (lood 8(6 and interstitial luid 8"F6
Arterial nd
-
8/20/2019 Perioperative Fluid Therapy.ppt
20/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
21/36
W(at flid s(old we se >
5 #r$stalloid solutions 9 "sotonic
9 H$potonic 9 h$pertonic
5 #olloid solutions 9 Semi?s$nthetic
colloids 9 aturall$ occurring human
plasma derivatives
-
8/20/2019 Perioperative Fluid Therapy.ppt
22/36
Crystalliod Colloid"ntravascular persistance Poor 1ood
Haemod$namicstabilisation
3ransient Prolonged
7euired inusion volume 4arge Moderate
7is; o tissue oedema Obvious "nsigniicant
nhancement o capillar$ perusion
Poor 1ood
7is; o anaph$lais il 4ow to moderate
Plasma colloid osmotic pressure
7educed Maintained
#ost "nepensive pensive
#r$stalloids and colloids
-
8/20/2019 Perioperative Fluid Therapy.ppt
23/36
T(e CrystalloidsCrystalloids are a gro)* o intra+eno)s l)id in
,(i-( %ay e.
9oni. soltion
? /inger la.tate4 a.etate
? @a,l p(ysiologi. #0A% saline$
? 6art!anCs soltion
? t.
• ostly iso-os!olar ) isotoni.
• ,(eap easy to !anfa.tre
• 6as no i!!nologi. rea.tion
• ainly .onfined to t(e etra.elllar flid
@on ioni.
? Detrose 5%
? altose 20%
? t.
• Distribted to intra.elllar spa.e
-
8/20/2019 Perioperative Fluid Therapy.ppt
24/36
le-trolyte Co%*arison
Bet,een NaCl 0/8
Na9
K9
Ca9
Cl!
a-tate Os%/=las!a 20 5 20* - *00
/inger +a.tate 2*0 * 20 18 17*
@a,l 25 - - 25 - *08
-
8/20/2019 Perioperative Fluid Therapy.ppt
25/36
=ra.ti.al .rystalloid t(erapy
• yo) in)se NaCl 0/8 1000%l: all t(e Na9 ,ill
re%ain in t(e C;
• As NaCl is isotoni- t(ere is no -(ange in C;os%olality and no
,ater e$-(ange o--)rs
a-ross t(e -ell %e%rane
• NaCl e$*ands C; only
• ntra+as-)lar +ol)%e ,ill e in-reased y 250%l
-
8/20/2019 Perioperative Fluid Therapy.ppt
26/36
=ra.ti.al .rystalloid t(erapy .ont…
• yo) in)se gl)-ose 58 1000%l: t(e gl)-ose
,ill enter t(e -ell and e %etaolised
• T(e ,ater e$*ands ot( C; and C; in
*ro*ortion to t(eir +ol)%es
• T(e C; +ol)%e ,ill in-rease y 333%l
• ntra+as-)lar +ol)%e ,ill only in-rease y
a**ro$i%ately 100%l
-
8/20/2019 Perioperative Fluid Therapy.ppt
27/36
T(e ,olloids
,olloids are flids w(i.( .ontain on.oti.
parti.les t(erefore eert an on.oti. pressre
• Blood
• =las!a• &lb!in
• &rtifi.ial .olloids ) plas!a epander
?
? H #6ydroyet(yl star.($ e/g/ (e%o(es 68 &
108
-
8/20/2019 Perioperative Fluid Therapy.ppt
28/36
#olloids luid loading leads to greater increase in
preload recruit table 4
-
8/20/2019 Perioperative Fluid Therapy.ppt
29/36
5 Saline or colloids do not aect permeabilit$
5 HS decrease permeabilit$ due to endothelial protections
5 4"S 8 lung "nKur$ Score 6 ma$ slightl$ increase in colloid
estimated b$ L respirator$ compliance caused b$
increase"3(< which "< volume was included 8 increased volume
dueto increased #OP 6
-
8/20/2019 Perioperative Fluid Therapy.ppt
30/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
31/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
32/36
How should we monitor luid replacement!
• (P, H7, =O
• Filling pressures
• 1astric pHi
• 3ransthoracic or transeophageal
echo
• 1oal?directed 7
-
8/20/2019 Perioperative Fluid Therapy.ppt
33/36
-
8/20/2019 Perioperative Fluid Therapy.ppt
34/36
• C(e-# @ regi%e ordered in o* or%
• Assess or dei-its y -(e-#ing &O -(art and +ital
signs
• Cal-)late %aintenan-e re)ire%ents
• s)ally K9 not started in irst 24 (rs
• Monitor -are)lly +ital signs and )rine o)t*)t
• Cardia-: renal and li+er ail)re still %)stres)s-itate/ nd*oint
are less *redi-tale: %onitor
%ore intensi+ely =C n+asi+e %onitoring>
=ostoperative flid t(erapy
# l i
-
8/20/2019 Perioperative Fluid Therapy.ppt
35/36
#onclusions G
3arget o Fluid 3herap$ Perioperative
5 Hemod$namic Optimalisation 9 "n acute emergenc$
resuscitation irst priorit$ J restoration
o an adeuate circulating volume adeuate
intravascular volume, DO:, blood pressure, adeuate
Microcirculation 9 Over h$dration adverse
outcome
5 Optimal volume distribution
5 Speciic losses should be replaced with appropriate
luid
cr$stalloid 9 colloid, consider both solute, dissolve
solute,electrol$te content, total osmolalit$, saet$, and side
eect
-
8/20/2019 Perioperative Fluid Therapy.ppt
36/36