Embed Size (px)
Citation preview

2/18/20
1
Peripheral Nerves
South Carolina Occupational Therapy Association
February 29, 2020
Tambra Marik, OTR/L, OTD, CHTMedical University of South Carolina
Marc Bartholdi, OTR/L, OTD, CHTSelect Medical
1
Peripheral Nerve Injuries
South Carolina Occupational Therapy Association Annual Conference 2020
Tambra Marik, OTD, OTR/L, CHTAssistant Professor Medical University of South Carolina
Marc Bartholdi, OTR/L, OTD, CHTSelect Medical
2/28/20
2
Objectives
• Discuss the basic anatomy and physiology of the nervous system• Identify varying surgical techniques for common nerve compression injuries• Apply assessment tools to evaluate peripheral nerve compression• Apply evidence-based intervention to treatment of common nerve
compression conditions• Identify common brachial plexus injuries• Analyze proximal nerve symptoms to guide with treatment• Demonstrate cervical screening to rule in/out spinal nerve root injury• Implement treatment strategies for cervical nerve root compression• Evaluate and implement therapeutic techniques for Thoracic Outlet (TOS)
3

2/18/20
2
Structurally
• Central Nervous System (CNS)• Brain and spinal cord
• Peripheral Nervous System (PNS)• Nerve fibers and cell bodies
Functionally• Somatic Nervous System
• Voluntary: Sensory carries sensations and position sense from skin and joints. Motor carries impulses to muscles
• Autonomic Nervous System• Involuntary/visceral: walls of
blood vessels, sweat glands, viscera (internal organs), body cavities (heart, stomach, bladder, etc)
The Nervous System
By Own work, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=10187018 By OpenStax College - Anatomy & Physiology, Connexions Web site.
http://cnx.org/content/col11496/1.6/,Jun 19, 2013., CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=301480084
4
Peripheral Nervous System
(PNS)
Central Nervous System (CNS)
Structure: Brain & Spinal Cord
Function: Control Center & Integrative
Structure: Cranial & Spinal Nerves
Function: Communicates between CNS and the rest of the body
Sensory
Structure: Somatic & visceral fiber
Function: Connects impulses from receptors to the CNS
Motor
Structure: Motor nerve fibers
Function: Conducts impulses from CNS to muscles & glands
AutonomicInvoluntary/Visceral
Sympathetic: Fight or flight
Parasympathetic: Conserves Energy
5
By OpenStax College - Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013., CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=30148131
https://upload.wikimedia.org/wikipedia/commons/f/f3/Sobo_1909_615.png
Spinal cord relays information to and from the brain through the spinal tracts through the thalamus and finally to the cortex.
Dorsal HornSensory
Ventral HornMotor
6
6
2/18/20
3
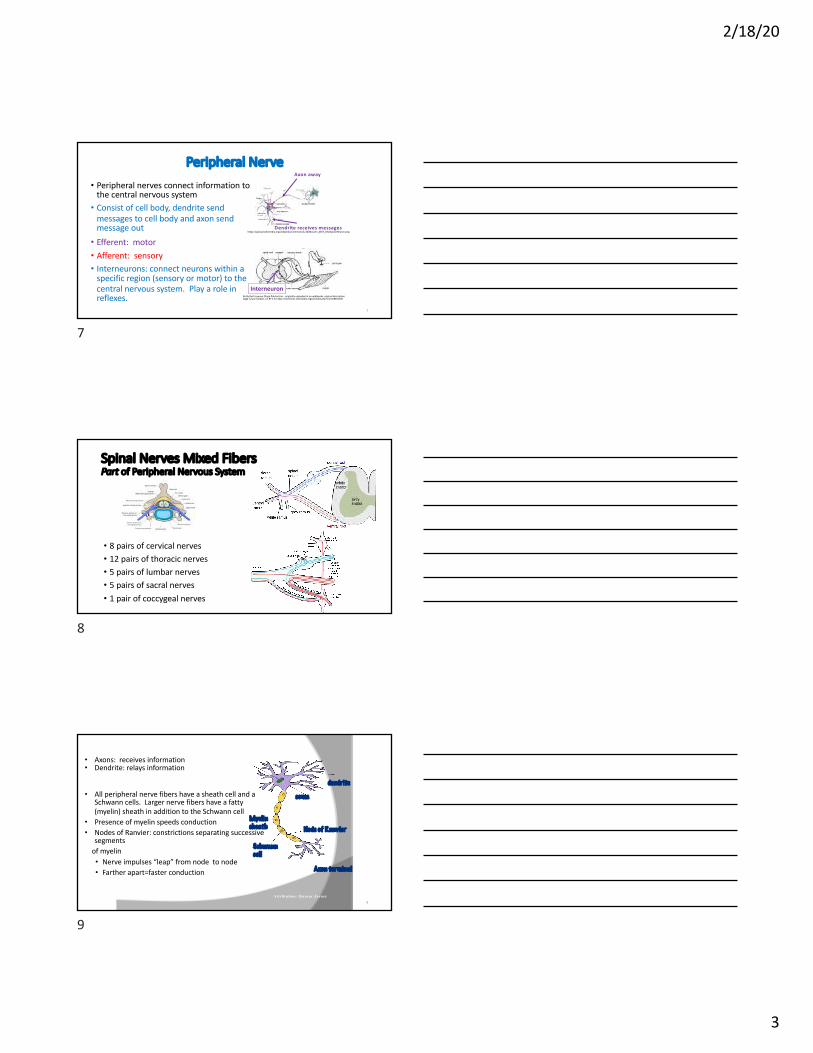
Peripheral Nerve
• Peripheral nerves connect information to the central nervous system• Consist of cell body, dendrite send
messages to cell body and axon send message out• Efferent: motor• Afferent: sensory• Interneurons: connect neurons within a
specific region (sensory or motor) to the central nervous system. Play a role in reflexes.
https://upload.wikimedia.org/wikipedia/commons/1/10/Blausen_0657_MultipolarNeuron.png
By By Ruth Lawson Otago Polytechnic - originally uploaded at en.wikibooks. original description page is/was here[1], CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=8831185
Axon away
Dendrite receives messages
7
Interneuron
7
Spinal Nerves Mixed FibersPart of Peripheral Nervous System
• 8 pairs of cervical nerves• 12 pairs of thoracic nerves• 5 pairs of lumbar nerves• 5 pairs of sacral nerves• 1 pair of coccygeal nerves
8
• Axons: receives information• Dendrite: relays information
• All peripheral nerve fibers have a sheath cell and a Schwann cells. Larger nerve fibers have a fatty (myelin) sheath in addition to the Schwann cell
• Presence of myelin speeds conduction• Nodes of Ranvier: constrictions separating successive
segments of myelin • Nerve impulses “leap” from node to node• Farther apart=faster conduction
dendrite
soma
Schwann cell
Node of RanvierMyelin sheath
Axon terminal
Attribution: Quasar Jarosz 9
9

2/18/20
4
Peripheral Nerve Communication
• Nerves have three connective tissue layers to protect• Endoneurium: inner most nerve fiber or axons; protects
against transmission of substances across the membrane• Perineurium: surrounds fasicles of nerve axons controls
substances bi-directionally, diffusion barrier• Epinueurium: outer most connective tissue that is highly
vascularized 10
10
Sensory Receptors
• Mechanoreceptors/Pressure, Proprioception• Meissner corpuscles: light touch• Merkel cells: light touch (abundant in fingertips)• Ruffini (Bulbous Corpuscle): skin stretch, temperature, contribute to proprioception• Pacinian corpuscle: vibrations• Free nerve endings: pain
fast adapting (A delta II)slow adapting (A delta I and C fibers)
http://www.bayareapainmedical.com/nerve.html
11
Sensory Receptors of Muscle & Tendon
• Muscle Spindles : detect changes in length, protects muscle length with the stretch reflex. • Golgi tendon reflex (inhibitory): detects muscle tension changes,
protects muscle force to help maintain steady levels of tension and stable joints to counteract effects that reduce muscle force such as fatigue
12
2/18/20
5
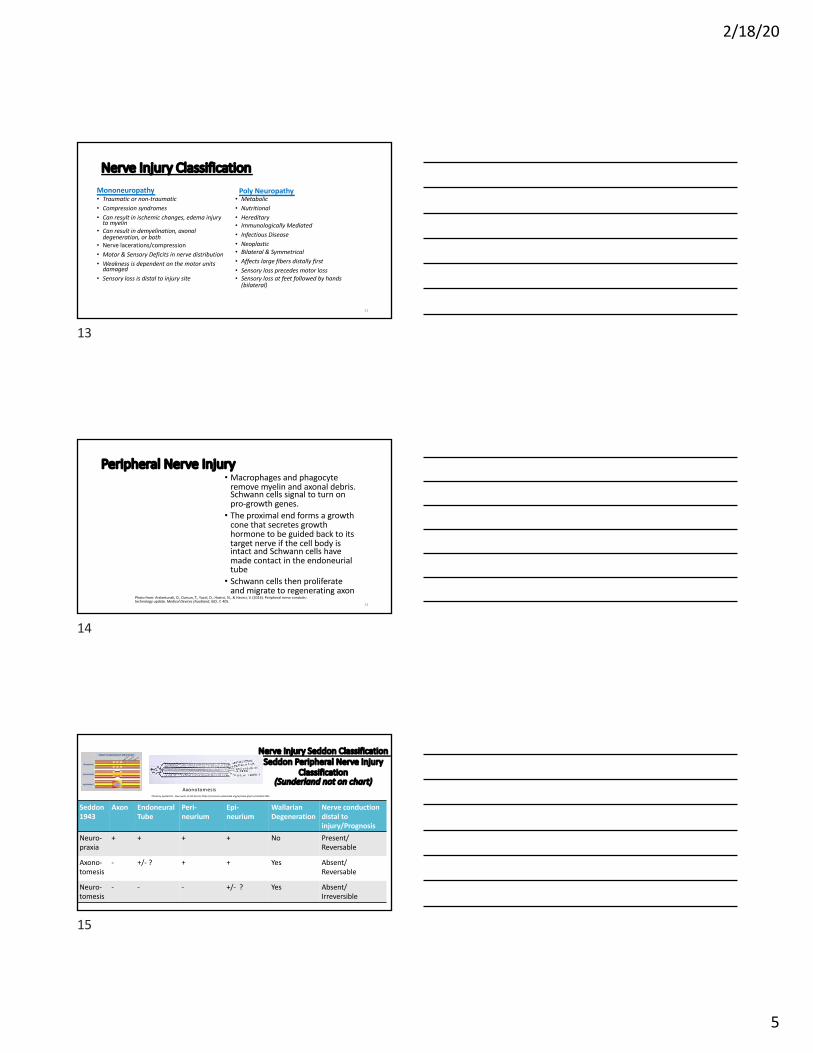
Nerve Injury ClassificationMononeuropathy• Traumatic or non-traumatic• Compression syndromes• Can result in ischemic changes, edema injury
to myelin• Can result in demyelination, axonal
degeneration, or both• Nerve lacerations/compression• Motor & Sensory Deficits in nerve distribution• Weakness is dependent on the motor units
damaged• Sensory loss is distal to injury site
Poly Neuropathy• Metabolic• Nutritional • Hereditary• Immunologically Mediated• Infectious Disease• Neoplastic• Bilateral & Symmetrical• Affects large fibers distally first• Sensory loss precedes motor loss• Sensory loss at feet followed by hands
(bilateral)
13
13
Peripheral Nerve Injury• Macrophages and phagocyte
remove myelin and axonal debris. Schwann cells signal to turn on pro-growth genes.• The proximal end forms a growth
cone that secretes growth hormone to be guided back to its target nerve if the cell body is intact and Schwann cells have made contact in the endoneurial tube• Schwann cells then proliferate
and migrate to regenerating axon 14
Photo from: Arslantunali, D., Dursun, T., Yucel, D., Hasirci, N., & Hasirci, V. (2014). Peripheral nerve conduits: technology update. Medical Devices (Auckland, NZ), 7, 405.
14
Nerve Injury Seddon Classification Seddon Peripheral Nerve Injury
Classification(Sunderland not on chart)
Seddon1943
Axon Endoneural Tube
Peri-neurium
Epi-neurium
Wallarian Degeneration
Nerve conduction distal to injury/Prognosis
Neuro-praxia
+ + + + No Present/Reversable
Axono-tomesis
- +/- ? + + Yes Absent/Reversable
Neuro-tomesis
- - - +/- ? Yes Absent/Irreversible
Photo by Syedm191 - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=58517905
Axonotomesis
15

2/18/20
6
Nerve Injury Classification Sunderland
16
Medical Treatment
• Neurapraxia - Observation
• Axonotmesis - Surgical intervention may be required
• Neurotmesis - Loss of nerve trunk, surgical intervention necessary.
17
Nerve Mechano-sensitivity Proximal Injuries Referring Distally
Sensitivity of Regenerating Axon Sprouts
• Micro-neuromas (sprouting nerve cells) form around the damage nerve
• New cells fire causing severe electrical burning and shooting pain
http://www.bayareapainmedical.com/nrvpain2.html
18

2/18/20
7
Nerve Mechano-sensitivity Proximal Injuries Referring Distally
Nervi Nervorum (unmyelinated or poorly myelinated fibers in peripheral
nerve sheaths)
• Participate in the transmission of evoked sensory information• Neuropeptide release leading to edema
due to poor lymphatic drainage. Distorts the endoneurom and epineurom due to pressure.• Inflammatory mediators spread distal
likely related to poor lymphatic drainage • Nerve becomes more sensitive
Image from: Lam, K. H. S., Hung, C. Y., Chiang, Y. P., Onishi, K., Clark, T. B., Reeves, D. K., & Daniel, S. (2020). Ultrasound-Guided Nerve Hydrodissection for Pain Management: An Updated Review of Anatomy and Techniques.
19
Histopathology of Chronic Nerve Compression
20
Double Crush SyndromeAxioplasmatic Flow Disruption
Alterations of Axoplasmic Flow
• Possible alterations with a proximal lesion affecting distal compression sites• Possible alterations with a distal lesion affecting
proximal lesion sites
• Alterations to neural transmission (axoplasmic flow), but each site in isolation may not reproduce patient symptoms when tested
(Hurst, Weissberg & Carroll, 1985)
21

2/18/20
8
Double Crush Syndrome Possible Posture Contribution (cont.)
• Movement patterns and posture can be effected with a nerve compression• Muscle imbalances can occur
↓ Muscle LengthSternocleidomastoid
Serratus anterior
Pronator teres
Scalenes
Pectoralis minor↑ Nerve Tension/Compres-
sionCarpal tunnel
Cubital tunnel
Median nerve forearm
Radial sensory
Brachial plexus
Muscle Weakness
Middle trapeziusLower trapezius
Serratus anterior
Muscle OveruseUpper trapeziusLevator scapulae
↑ Muscle Length
Middle traps.Lower traps.
Novak & Mackinnon, 2005
22
Thoracic Outlet (TOS)
Potential Compression Sites• Interscalene triangle
Anterior and middle scalenes• Costoclavicular space
Between clavicle and 1st rib• Thoraco-coraco-pectoral space
Pectoralis minor
23
neural, arterial and/or venous
Photo from: Jones, M. R., Prabhakar, A., Viswanath, O., Urits, I., Green, J. B., Kendrick, J. B., ... & Kaye, A. D. (2019). Thoracic outlet syndrome: a comprehensive review of pathophysiology, diagnosis, and treatment. Pain and therapy, 8(1), 5-18.
23
Compartment of Potential Compression
Borders Contents
Interscalene triangle
Anterior: anterior scalenePosterior: middle scaleneInferior: 1st rib
• Brachial plexus
• Subclavian artery
Costoclavicular space
Anterior: subclaviusInferoposterior: 1st rib and anterior scaleneSuperior: clavicle
• Brachial plexus
• Subclavian artery
• Subclavian vein
Sub-coracoid space
Anterior: pectoralis minorPosterior: ribs 2-4Superior: coracoid
• Brachial plexus
• Axillary artery• Axillary vein
Photo from: Jones, M. R., Prabhakar, A., Viswanath, O., Urits, I., Green, J. B., Kendrick, J. B., ... & Kaye, A. D. (2019). Thoracic outlet syndrome: a comprehensive review of pathophysiology, diagnosis, and treatment. Pain and therapy, 8(1), 5-18.
24

2/18/20
9
Double Crush
“Local damage to a nerve at one site along its course may sufficiently impair the overall functioning of the nerve cells that they become more susceptible than would normally be the case to trauma at other sites.”(Upton and McComas, 1973)
• 53 cases of ulnar nerve anterior subcutaneous transposition, 7 had TOS. 44/50 had resolved symptoms at 12-74 months post-op. 5/7 had persistent subjective symptoms and objective motor dysfunction. (Lascar & Laulan, 2000)
25
True
•Paresthesia am & pm
•Compressors day pain > night pain
•Confirmation with neurophysiological tests
Disputed
• Paresthesia awaken often pm
• Releasers pm pain > day pain
• No confirmation with neurophysiological test
• Estimated to be 95-99% of all neurogenic types and is bilateral (Stewman, Vitanzo & Harwood, 2014)
Neurogenic TOS Estimated 95% of Cases (Freischlag & Orion, 2014)
26
ReleasorCompressor
26
27
Test Sensitivity Specificity LR+ LR-
Supraclavicular Pressure (Nord et al
2008)
NT 85-98 NA NA
Cervical Rotation Lateral Flexion (Gilbert et al 2004)
0.42-1.0 100 NT NA
Cyriax Release (Brisme et al 2004)NT 77-97 NA NA
Upper limb tension (Bertilson, Grunnesio &
Strender, 2003)
90 38 1.5 0.3
Roos Elevated Arm Stress (Rayan &
Jensen 1995)
52-84 30-100 1.2 0.4-0.53
Costoclavicular Maneuver (Nord et
al 2008)
NT 53-100 NA NA
Wright’s (Gillard et al 2001)70-90 29-53 1.27-1.49 0.34-0.57
27

2/18/20
10
Clinical Tests: Cervical Rotation Lateral Flexion Client must have at least 20% of lateral flexion to perform test
Patient is seated and the examiner is behind the patient. The examiner blocks the side being tested with their forearm. The examiner rotates the head away from the tested side and gently flexes the neck. Is lateral flexion limited? Bony end block?Positive Test: Notably decreased forward flexion and a hard end feel. Compare sides.
Testing right side
28
Lindgren, Leino & Manninen, 1992)
28
Clinical Tests: Upper Limb Tension Test (ULLT) or Elvey Test Suspected positive test for Neurogenic TOS
• #1: Arms abduction to 90°
• #2: Extend wrists
• #3: Tilt head to side
Positive Test: pain and/or paresthesia in the hand or around the elbow
Position 1
Position 2
Position 3
+ test which position provoked symptoms29
29
Clinical Tests for Thoracic Outlet• Rule Out Negative Tests: Highest Sensitivity (2 negative tests)
• Cervical Rotation Lateral Flexion• Roo’s Elevated Stress Test• Upper limb tension testing• Wrights
• Rule In Positive Tests: Highest Specificity (5 positive tests)
• Supraclavicular pressure• Cervical Flexion Lateral Rotation• Cyriax Release Test• Roo’s Elevated Stress Test• Costoclavicular Manuever• Wright’s Test
30

2/18/20
11
Suspected Compression Site
Clinical Reasoning
Restriction Treatment Strategy
Anterior & Middle Scalenes
• Supraclavicular Pressure test +
• Cervical lateral flexion test +
• Elvey test +
• Soft tissue shortness
• Elevated 1st rib
• Hypomobility of 1st rib
• Scalenes mobilization & stretching
• Neuromuscular re-education
• Diaphragmatic breathing
• 1st rib mobilization
Posture: Scalenes Length & 1st Rib Mobility
31
Teach Diaphragmatic Breathing• Teach diaphragmatic
breathing• Scalenes release• Stretch scalenes• 1st rib mobility
(Hooper, Denton, McGalliard, Brismee & Sizer, 2010)
32
32
Soft Tissue Mobilization Technique #1: Scalenes Soft Tissue Release
• Teach diaphragmatic breathing• Scalenes release• Stretch scalenes• 1st rib mobility
(Hooper, Denton, McGalliard, Brismee & Sizer, 2010)
Client is sitting with therapist standing behind client. Therapist places index and/or long digits on anterior scalenes with moderate caudal pressure. Client movesslowly towards slight lateral flexion to uninvolved side and rotation to involved side. Perform 5 to 10 reps.
33
33

2/18/20
12
Promote 1st Rib Mobility
(Hooper, Denton, McGalliard, Brismee & Sizer, 2010)
• Clinician places radial hand on the 1st rib while using the other hand to stabilize the shoulder.• The patient turns their head towards the
treatment side.• Clinician provides a glide to the 1st rib towards
the opposite hip and slightly anterior.
34
• Teach diaphragmatic breathing• Scalenes release• Stretch scalenes• 1st rib mobility
34
Promote 1st Rib Mobility Home Program
Self 1st Rib MobilityThe patient is in sitting with cervical spine retracted. The client sits on a sheet/towel and places the sheet 1 inch lateral to the transverse process of T1. The patient uses their own hand to pull on the sheet in a contralateral caudal (opposite hip) direction. Adding a head rotation will stretch the scalenes (H o o p e r, D e n to n , M cG alliard , B rism e e & S ize r, 2 0 1 0 )
35
35
Suspected Compres-sion Site
Clinical Reasoning
Restriction at Scapula Treatment Strategy
Costoclavicular between clavicle and 1st
rib
• Poor posture• Depressed
and/or downwardly rotated scapula observed
• Scapular Correction Test +
• Depression: poor muscular recruitment to achieve scapular upward rotation and/or muscular tightness at shoulder depressors (latissimus dorsi, pectoralis major/minor)
• Downward Rotation: same as above except muscle tightness possibly at scapular downward rotators (levator scapulae and rhomboids)
• Poor movement patterns between scapula and humerus
• Diaphragmatic breathingDepression• Stretch tight muscles
(latissimus and pectoralis)
• Neuromuscular retraining (taping) scapula upward rotators
• Strengthening scapula upward rotators (lower trapezius and serratus anterior)
• Scapula mobilization• Disassociate scapula and
humerus motion
36

2/18/20
13
Suspected Compres-sion Site
Clinical Reasoning
Restriction Scapula or Glenohumeral Joint
Treatment Strategy
Costoclavicular space and/or beneath pectoralis minor
• Palpation• Observations
of poor posture
• Scapula correction test +
• Anterior tilted scapula
• Short pectoralis minor muscle
• Joint specific test + for humerus
• Poor scapula posture and recruitment: Anterior tilted and/or downward rotation due to muscular shortness or poor muscular recruitment patterns
• Poor glenohumeral motion:posterior capsule tightness; unable to dissociate scapular from glenohumeral motions
• Diaphragmatic breathingDepression• Stretch tight muscles
(latissimus and pectoralis)
• Neuromuscular retraining (taping) scapula upward rotators
• Strengthening scapula upward rotators (lower trapezius and serratus anterior)
• Scapula mobilization• Disassociate scapula and
humerus motion
37
Suspected Compres-sion Site
Clinical Reasoning
Restriction Treatment Strategy
Costo-clavicular space between clavicle and 1st rib
• Cervical lateral flexion test +
• Soft tissue shortness scalenes• Elevated 1st rib• Hypomobility of 1st rib
• Scalenes mobilization & stretching
• Neuromuscular re-education• Diaphragmatic breathing• 1st rib mobilization
Costo-clavicular space between clavicle and 1st rib
• Joint specific test suggest poor clavicle mobility
• Hypo-mobility of clavicle acromioclavicular (AC) and/or sternoclavicular (SC) joints
• AC and SC mobilizations
38
Lab/Treatment Strategies for:Depressed Scapula Effecting Costoclavicular Space AC & SC Mobility
• Mobilize clavicle• Correct scapular restrictions• Disassociate glenohumeral from scapula
motions• Correct glenohumeral capsular
restrictions• Thoracic mobility• Progress to strengthening
(H o o p e r, D e n to n , M cG alliard , B rism e e & S ize r, 2 0 1 0 )
Image from Watson, Pizzari & Baister, 2010)
39

2/18/20
14
Downward Rotation• Inferior border of
scapula is closer to the spine as compared to superior border
Anterior Tilt• Inferior border
protrudes from thorax
Depressed scapula• Superior border is lower that T2• One arm longer than the other
Assessing Scapula by Observation Static
40
41
Test: Muscle length of latissimus dorsi, pectoralis clavicular and sternal fibers
• Shortness exists when the patient is unable to reach arms overhead to the mat.
Kendall, F.(2005). MUSCLES TESTING AND FUNCTION WITH POSTURE AND PAIN. Baltimore, MD: Lippincott Williams & Wilkins.
Marik, T. Latissimus Dorsi assessment, December 2009. Courtesy Tambra Marik
• Short clavicular fibers exist when the arm can not abduct/drop down to the mat at 90°abduction
Marik, T. Assess pectoralis major clavicular fibers,December, 2009. Courtesy Tambra Marik
Marik, T. Assess pectoralis major clavicular fibers,December, 2009. Courtesy Tambra Marik
• Short muscle fiber exists when horizontally abduction at 120° to 140° does not drop down to the mat.
Latissimus dorsiP. major sternal fibers
P. major clavicular fibers
41
Testing: Posture Observations and Muscle Length
• Perform muscle length test for pectoralis minor.• Client lies supine with external rotation (palms up). • Check for asymmetry. Is the posterior acromion higher off the mat on one
side.• Tightness at pectoralis minor will contribute to scapular anterior tilt
causing the acromion to be higher on the tight side.42
Inferior angle protrudes R acromion higher
42

2/18/20
15
Treatment: Pectoralis Muscles
Stretching pectoralis minor with client on a foam roller and therapist manually stretching. Therapist’s hands are on the coracoid process stretching dorsal and lateral.
Stretching pectoralis minor and major with client on a foam roller. Therapist’s as one hand on unilateral coracoid process stretching dorsal and lateral. The other hand supports the arm.
43
Treatment Strategies: Scapular Restrictions
• Mobilize clavicle• Correct scapular restrictions• Lengthen short muscles• Scapula Mobilizations• Neuromuscular Re-education
• Correct glenohumeral capsular restrictions• Disassociate glenohumeral capsular restrictions from scapula• Thoracic mobility• Progress to strengthening
44
Treatment Strategies: Stabilize scapula with pectoralis minor in a lengthened position
The client is supine. Client is instructed to flex at knees and hips. A roller or towel is placed lengthwise down spine. Humerus supported. The client stabilizes scapula while performing external rotation exercises. Perform 5 to 10 reps 45
45

2/18/20
16
Treatment: Mobilize Clavicle
• One hand on the scapula• Thenar eminence of the
other hand on the medial clavicle providing a inferior and posterior glide.
• One hand stabilizes the AC joint• The thumb of the other
hand is placed on the posterior acromion• Provide a anterior glide to
the posterior acromion while stabilizing with the other hand
SC Glide
AC Glide
Marik 2018 Nerve Compression and Injuries 46
46
Treatment: Neuromuscular Re-educationScapula Downward Rotation/Depression/Anterior Tilt
• Wall slides for upward rotation. Ulnar forearm on wall. Slide towards a teardrop position. 5 to 10 reps. Progress to resisted scaption exercises.
• Exercises to promote scapular upward rotation
• Taping to promote upward rotation
(Hooper, Denton, McGalliard, Brismee & Sizer, 2010)
47As symptoms improve exercises can progress. Position #1
47
EVALUATION PERIPHERAL
NERVE COMPRESSION
• OBSERVATIONS• MOTOR• SENSORY• LIGHT MOVING TOUCH• VIBRATION THRESHOLDS• CUTANEOUS PRESSURE THRESHOLDS• 2 POINT DISCRMINATION
• PAIN EVALUATION• PALPATION, POTENTIAL COMPRESSION
SITES & CLINICAL PROVOCATIVE TESTS• EVAULATING CERVICAL
48

2/18/20
17
Observations (distal) Early LateVasomotor (temp., color, edema , cold tolerance)
Skin rosy Skin mottled
Skin warm Skin coldSudomotor(sweat patterns)
Dry skin Dry or overly moist skin
Pilomotor (“goose flesh”) Absent AbsentTropic (skin texture, atrophy to digit pulps, nail changes, hair growth changes, slow skin healing)
Fingernails blemish Curved
Longer & fine hair growth Longer & fine hair growth
Skin soft & smooth Skin smooth/non-elastic
Slight atrophy Atrophy at finger pulps
SOURCE: Callahan, Anne D. : SensibilityTesting: Clinical Methods Rehab of the Hand , ed2, 1984 The CV Mosby Co.49
49
Evaluation: Differentiating Nerve Lesions
• Combine clinical findings of reflex, sensory and strength testing• Motor
• Nerve Root: Myotome• Peripheral: Peripheral Nerve Innervation
• Sensory• Nerve Root: Dermatomes• Peripheral: Peripheral Nerve Cutaneous Distribution
• Deep Tendon Reflexes • Interpreted with sensory and strength findings to determine nerve root versus peripheral
nerve lesion:• Hypotonia involving lower motor neurons (nerve root, neuromuscular junction or muscle)• Hypertonia involving upper motor neurons
50
MOTOR EVALUATION: Manaul Muscle Testing
Nerve Root Myotome Associations• C5- shoulder abduction • C6– Elbow flexion, Wrist extension • C7 – Elbow extension, Wrist flexion• C8 – Finger flexion• T1 – Finger abduction
Peripheral Nerve Associations• Muscles innervated by each
nerve• Median• Ulnar• Radial• Musculocutaneous• Axillary
Clinical Hints: T1 intrinsicsC6 supinatorC5 shoulder abduction, extension and external rotationC7 & 8 almost all others
51

2/18/20
18
SENSORY EVALUATION: Patient Subjective Symptoms
Peripheral Nerve• Decreased sensation and
strength in the peripheral distribution pattern
Nerve Root• Spinal segment representation of
dermatome (sensory) and myotome (motor) patterns
52
By Grant, John Charles Boileau - An atlas of anatomy, / by regions 1962, Public Domain, https://commons.wikimedia.org/w/index.php?curid=30017222
By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" section below)Bartleby.com: Gray's Anatomy, Plate 812File:Gray812.png andFile:Gray814.png, Public Domain, https://commons.wikimedia.org/w/index.php?curid=3460423
52
Quick Scan of Motor Scan for Peripheral Nerve
• Resist palmar abduction for median nerve
– Resist index finger abduction and palpate 1st dorsal interossei for ulnar nerve
53
– Resist thumb dorsal retropulsion for radial nerve
Median
Radial
Ulnar
53
SENSORY EVALUATION: Moving Light Touch
Ten Test is a screen for large A-Beta fibers (testing moving fibers Meissner and Pacini quick adapting receptors)• Moving touch contra-lateral unaffected digit identifying normal sensation at
10/10.• Touch the same area on the involved side and patient rates the normal
sensation compared to the contra-lateral side. (Strauch et. al, 1997)
54

2/18/20
19
Muscle ReflexesGrade Response Interpretation Clinical Reasoning
0 No response Always abnormal Lower neuron
1+ Slight, muscle contraction but there is no joint movement
May or may not be normal
Lower neuron
2+ Brisk response Normal Normal
3+ Very brisk response May or may not be normal
Upper motor neuron
4+ Clonus Always abnormal Upper motor neuron
55
Deep Tendon ReflexesSpinal Level Reflex Peripheral
NerveC6 Biceps Musculocutaneous
C5-6 Brachioradialis Radial Nerve
C7 Triceps Radial Nerve
Hypotonic reflex: suspect lower motor neurons/cervical radiculopathy; individuals with carpal tunnel likely will not cause changes with reflexes due to a distal compression.
56
SENSORY EVALUATION: Vibration Thresholds
Testing sensory return: 30 cps vibration to affected area (testing Merkel & Ruffini low frequency quick adapting receptors)
Testing for early neural changes: 256 cps to digit pulp of involved followed by a comparison of sensation intensity to the uninvolved (testing Pacini and Meissner high frequency quickly adapting receptors)
High adapting fibers are thought to be affected first in chronic nerve compression (Novak & Mackinnon. 2005)
256 cps best for testing in chronic injury because they are the first affected
57

2/18/20
20
SENSORY EVALUATION: Cutaneous Pressure Thresholds
Testing sensory return of fine tactile & discriminative location: Semmes Weinstein testing screens for threshold (testing slow adapting Merkel receptors)
58
SENSORY EVALUATION: Two Point Discrimination (pd)
Testing quantity of innervated sensory receptor
Static Two-Point Discrimination (Table modified from Klein, 2014)
1-5 mm Normal6-10 mm Fair11-15 mm PoorOnly one point perceived
Protective sensation only
No point perceived Anesthetic
59
Pain Evaluation
• Pain during varying activities (work, home, sleep, etc.)• Pain scales (visual analog scale)• Pain descriptors• Body diagram chart• How is client coping with pain? Mechanisms such as medications• Would the client benefit from psychological counseling? Will pain
hinder the progress in therapy?
60

2/18/20
21
Visceral Referral Pain Patterns
By OpenStax College - Autonomic Reflexes and Homeostasis http://cnx.org/content/m46579/1.2/, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=30017359
61
General characteristics of pain due to visceral pathology
1. Is poorly localized with referral to somatic structures2. Produces nonspecific regional or whole-body motor responses3. Produces strong autonomic responses4. Leads to sensitization of somatic tissues5. Produces strong affective responses(Sikandar & Dickenson, 2012)
61
Palpation, Potential Compression Sites & Clinical Tests
• Creates nerve tension and compression at nerve sites• Assist with determining compression site• Helpful identifying area of compression in the early stages when there
may not be symptoms of sensory changes• Tinels and provocative tests performed from proximal to distal for
clinical signs of double crush syndrome. (Novak & Mackinnon, 2005)
62
Nerve Pathways & Palpation:Median Nerve Path Proximally C5,6,7,8,T1
• Lateral root arises from lateral cord; medial root arises from medial cord
• Follows the brachial artery; medial at elbow• Passes through two heads of
pronator; deep to bicep aponeurosis
• Passes b/w FDS and FCR• Emerges distally b/w FPL & FDS
• Enters carpal tunnel
https://upload.wikimedia.org/wikipedia/commons/d/de/Gray812and814.PNG
ForearmInnervations
By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" section below)Bartleby.com: Gray's Anatomy, Plate 816, Public Domain, https://commons.wikimedia.org/w/index.php?curid=328869
63
63

2/18/20
22
Median Nerve Possible Compression SitesCarpal Tunnel
Pronator Syndrome (PS) Anterior Interosseus Nerve (AIN) Syndrome
Carpal tunnel Supracondylar process (spurs)? Edge of deep pronator
Ligament of Struthers FDS arch
Bicipital aponeurosis Accessory head FPL Gantzers
B/w ulnar and humeral heads of pronator teres
Accessory muscle from FDS to FDP
FDS arch
64
65
Carpal Tunnel Cervical Radiculopathy
Paresthesia in digits #1-2 & radial side #3
Sensory deficit at lateral arm and digits #1-3
Waking due to night pain
Hand weakness, clumsy Arm and hand weakness
Upper extremity pain Pain at neck, scapula and upper extremity
Waier et al 2000
Carpal Tunnel vs. Cervical Radiculopathy Symptoms
65
CLINICAL TESTSCarpal compression testPhalensTinelsMedian nerve tension test
Provocative Tests:
Carpal Tunnel Testing
66
66

2/18/20
23
Pronator Teres Syndrome AIN Syndrome
Resisted pronation with elbow extended (pronator teres)
Weak pronation tested with elbow flexed?Weakness of thumb IP and IF DIP.Weak grip/pinchUnable to make OK sign
Resisted contraction to long finger FDS (FDS compression)
67
Clinical Tests Pronator Syndrome versus Anterior Interossei Nerve Compression tests
67
Clinical Tests Pronator Syndrome• Pronator Compression Tests: Pressure
for 30 seconds at PT (1.5 in distal flexion crease) muscle belly recreates symptoms.(PT compression)• + Tinels at proximal forearm; pronator
compression• Symptoms reproduced with resisted
pronation (wrist neutral) passively extending elbow.(PT compression)• Resist elbow flexion between 120-130
degrees with supination recreates symptoms. (Bicipital aponeurosis compression)
68
68
Nerve Pathways & Palpation:Radial Nerve Path Proximally C6,7,8,T1
• Exits triangular interval• Posterior between long head
of triceps and humerus• Through spiral groove• Lateral intermuscular septa
(b/w brachialis and brachioradialis anterior to lateral epicondyle)
By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" section below)Bartleby.com: Gray's Anatomy, Plate 818, Public Domain, https://commons.wikimedia.org/w/index.php?curid=541674
Proximal InnervationsTricepsAnconeusECRLECRBBrachioradialis
By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" section below)Bartleby.com: Gray's Anatomy, Plate 818, Public Domain, https://commons.wikimedia.org/w/index.php?curid=541674 69
69

2/18/20
24
Compression Sites Proximal to the Elbow: TRIANGULAR INTERVAL (TI) & SPIRAL GROOVE
Triangular Interval (TI)• TI contains radial nerve and profunda artery• TI compressions can occur from:
• Posture humeral add/ir and scapular protraction• Hypertrophy of teres major • Adaptive shortening of internal rotators• Fibrous arch at the long head of triceps
http://upload.wikimedia.org/wikipedia/commons/1/16/Gray412-spaces.png
70
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-008-9781455726721.jpg
Spiral Groove• Compression
distal triceps
70
Mechanism of InjuryTriangular Interval Spiral Groove
Hypertrophy at teres major and medial triceps
Compression from leaning on a hard surface “Saturday Night Palsy”
Fibrous bands at teres major and medial triceps
Radial shaft fractures
Shortened teres majorSports with forceful shoulder extensionSymptoms reproduced with external rotation combined abduction
71
71
Triangular Interval Spiral Groove
MotorPresen-tation
Weakness in all muscles innervated by radial nerve
Triceps spared.Weakness at all muscles innervated by radial nerve distal to triceps
SensoryPresen-tation
• Posterior cutaneousnerve of arm
• Lower lateral cutaneous nerve of arm
• Posterior cutaneous nerve of forearm
• Superficial radial nerve
Superficial radial nerve
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg
Adapted from Haymaker, W., Woodhall, B., 1953. Peripheral nerve injuries. WB Saunders, Philadelphia.)
72
Presentation Sites Radial
Nerve
72

2/18/20
25
Compression Sites Radial Nerve Distal to ElbowTwo conditions; Same compression sites
Posterior Interossei Nerve (PIN)
Radial Tunnel
Fibrous bands at radiocapitellar jointLeash of HenryMedial edge of ECRBProximal edge of supinator (Arcade of Frohse)Distal edge of the supinator
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg (Roles & Maudsley, 1972)
73
73
Clinical Presentation: Radial NervePIN Radial TunnelWeakness and/or paralysis to: ECRB, supinator, ECU, EDC, EDM, APL, EPL, EPB, EI
Lateral proximal forearm pain, tenderness at supinator muscle, pain with supination with extended elbow, pain with resisted long finger. • No motor weakness
Awakens nocturnally due to forearm pain
Pronation, elbow ext and wrist flex ↑ symptoms
Rule out tennis elbow, may have lateral elbow tenderness
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg 74
74
Posterior Interossei Radial TunnelResisted supination recreates pain. Tenderness 3-5 cm distal lateral
epicondyleTest for weakness of MP extension and wrist weakness.Observe wrist extension for a bias towards radial deviation.
Resisted supination with the elbow and wrist extended reproduces pain.
Positive pain with long finger extension test.Passive pronation with wrist flexion reproduces pain 75
Provocative Tests Radial NervePosterior Interossei versus Radial Tunnel
75

2/18/20
26
Nerve Pathways & Palpation: Ulnar Nerve Path C8, T1
• Arises from the medial cord• Descends distally and medially at the arm• 1/3 distal arm pierces intermuscular septum
traveling posterior• Crosses elbow posterior in supracondylar
area• Enters forearm b/w medial epicondyle and
olecranon• Deep to FCU in forearm • In hand, lateral to pisiform and hook of
hamate• Ulnar nerve superficial branch (cutaneous)
and deep (motor) within Guyon’s canal76
76
Compression Sites Ulnar Nerve
High Lesions Low LesionsCubital Tunnel Distal to FCU and FDP
motor branchesMedial Intermuscular Septum
Guyon’s canal
Arcade of StruthersFlexor carpi ulnaris (FCU)
77
77
Ulnar Nerve Clinical PresentationHigh Lesions• All extrinsics and intrinsics affected (weak
wrist flexors)• Sensory loss over palmar and dorsal aspect
of small digit and ulnar half of ring digitLow Lesions• Deep intrinsics affected (wrist flexors intact)• No sensory loss over proximal and middle
phalanx of dorsal small and ring digits due to dorsal cutaneous nerve branch being spared
https://www.google.com/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&cad=rja&uact=8&ved=2ahUKEwierPXpmavaAhVo94MKHQRmBCIQjRx6BAgAEAU&url=http%3A%2F%2Fteachmeanatomy.info%2Fupper-limb%2Fnerves%2Fthe-ulnar-nerve%2F&psig=AOvVaw16f9ivvlLRnTQg53iMtSzi&ust=1523294471613937 78
78

2/18/20
27
Clinical Tests Cubital TunnelTinels at cubital tunnel and Guyon’s canal
Modified Shoulder Internal Rotation Test
Elbow Flexion TestScratch CollapseClinical Test for Guyons CanalSensory testing at dorsal ulnar digits normal but, volar ulnar digits impaired 79
Provocative Tests for Unar NerveGuyons Canal versus Cubital Tunnel
79
Clinical Tests:Cubital Tunnel Syndrome
TinelsSensitivity:54% to 70%
Modified Shoulder Internal Rotation TestSensitivity: 87% (5 second)Specificity: 97% O c h i e t a l 2 0 1 2
Elbow Flexion TestSensitivity: 46% to 75% (1 to 3 min.)
( H u t c h i n s o n e t a l 2 0 1 1 )
80
80
CERVICAL SCREENING
• Retrieved on 12/10/12 from:• http://upload.wikimedia.org/wikipedia/commons/thumb/5/54/Cervical_vertebrae_lateral2.png/600px-Cervical_vertebrae_lateral2.png
81
81

2/18/20
28
Cervical Spondylosis: Non-specific termCervical RadiculopathyType I
Cervical nerve roots compression and inflammation of the nerve root or roots at or near the cervical foramen. Symptoms are pain radiating into the arm corresponding to the dermatome of the involved cervical nerve root
Cervical MyelopathyType II
Compression of the cervical spinal cord related to degeneration of discs and bone spurs. Symptoms can include: weakness and numbness, loss of balance and coordination and neck pain. Rheumatoid arthritis can cause myelopathy due to synovium swelling destructing facet joints.
Axial Joint PainType III
Neck pain with pain radiation to one or more of the following: medial scapula, chest wall, shoulder area and head. Symptoms stem from the joints. Correlation between activity and pain. Pain is expected to improve with rest.
https://www.coloradospineinstitute.com/files/3614/5121/6098/13_vert_body.jpg
https://upload.wikimedia.org/wikipedia/commons/c/cb/Doberman_C6-C7_and_C5-C6_traction_responsive_myelopathy_A.jpg
82
EXAMINATION1. History2. Pain Patterns & Scales3. Inspection4. AROM/PROM of upper limb & cervical5. Palpation6. Myotome scan7. Dermatome scan8. Vertebral Artery test9. Provocative tests 10. Upper limb neural tension testing (median, ulnar,
and radial nerves)83
Adapted from McClure 2004
83
History
• Current condition and past condition• Age• Past medical information/surgeries• Onset/history of current condition• Medications• Social history (past & present)• Occupations and functional status• Past location• Pain Characteristics: patterns (dermatomal, mechanical, segmental
distribution pattern, trigger point), aggravating activity, intensity, duration, location
84
2/18/20
29
Pain: Classification Central SensitizationCentral nervous system centralization. Dominance of allodynia and hyperalgesia
Administer Laniss Pain scalehttp://www.bayareapainmedical.com/chrnanm.html
DenervationSignificant axonal compromise but no central nervous system changes. Loss of nerve supply. Can be from injury, disorders or surgery.
Peripheral Nerve SensitizationInflammation arising from nerve trunk or peripheral nerve without clinical evidence of significant denervation. Injury to the area produces a flare.
Musculoskeletal PainPain is referred from non-neural structures.
85
Posture
• Patient attempts to shorten anatomical distance over the course of the sensitized nerve when experiencing central sensitization• Elevated scapula, ipsilateral
side cervical flexion and elbow flexed
• Patient may attempt to increase the available space surrounding the nerve roots when experiencing neuropathic pain related to denervation from compressed, stenotic nerve root
86
Inspection/PostureForward head posture, rounded shoulders, kyphosis• Scapula protracted & internally rotated (IR) and
glenohumeral IR or flat cervical spine• Associated with headaches and interscapular
pain (Griegel-Morris, Larson, Mueller-Klaus & Oatis, 1992)
• Interscapular pain (G rie g e l-M o rris, Larso n , M u e lle r-K lau s & O atis, 1 9 9 2 )
• Overly extended cervical spine can cause overstretching and friction on nerve roots
• Asymmetry? Alignment of scapula? Scoliosis?
• Guarding
87
Figure from: Donatelli, R. A., & Wooden, M. J. (2009).
87

2/18/20
30
Inspection: (cont.)
Forward Head Posture
Forward Head Posture Joint Mechanical Changes• Excessive forces at mid cervical spine• Increased forces on intervertebral disc &
neural arches• Degeneration of disc
• Osteophytic spurs a posterior facet joints• Friction at cervical vertebrae due to
repetitive extension & rotation causing friction on the nerve roots at the transverse processes
88
Vertebral Artery TestingPatient can be supine or sitting.• Extend, rotate and flex the cervical spine to the
right when testing the left side (vice versa for testing the right side). Hold the position for approximately 30 seconds and ask the patient to count back from 20.• Signs of a positive test are:
• Dizziness• Diplopia (double vision)• Dysarthria (poor motor speech)• Dysphagia (difficulty swallowing)• Drop attacks (short loss of consciousness• Nausea and vomiting• Sensory changes• Nystagmus
89
Cervical AROMCheck for quality of movement, burning, sharp pain, numbnessis there a correlation of adverse responses?
• Client actively flexes cervical spine• Followed by active cervical extension with the mouth open to
avoid tension of suprahyoid and infrahyoid muscles
90
Clinical Reasoning: Muscular, Ligament Strain/Sprain or Nerve RootManeuver Pain (soft tissue) Pain (nerve root)AROM Yes Yes
PROM Yes Yes
Provocative of ligament or muscle or ligament
Yes Yes
Provocation of neural tissue
No (paresthesia) Yes (paresthesia)
90

2/18/20
31
Cervical ROM (cont.)
Active motion first, followed by overpressure, if there was no pain actively.
• Flexion
• Extension
• Side-bending
• Rotation
91
91
Provocative Tests: Testing Recreation of Symptoms• AROM, if no pain
• Over pressure at end range, if no pain
• Compression/Distraction, if no pain
• Spurlings• Arm squeeze test (Gumina, Carbone, Albino, Gurzi &
Postacchini, 2013)
• Determine cluster signs
92
Palpation• Start with uninvolved side• Palpation should be mild (blanch the nailbed of the palpating finger)• Supra and infra-clavicular fossa associated with TOS involvement• Distal nerve palpation to rule out peripheral nerve involvement
Upper and Middle Trunks • Posterior to sternocleidomastoid (STM) • Between the anterior and middle scalenes
93
2/18/20
32
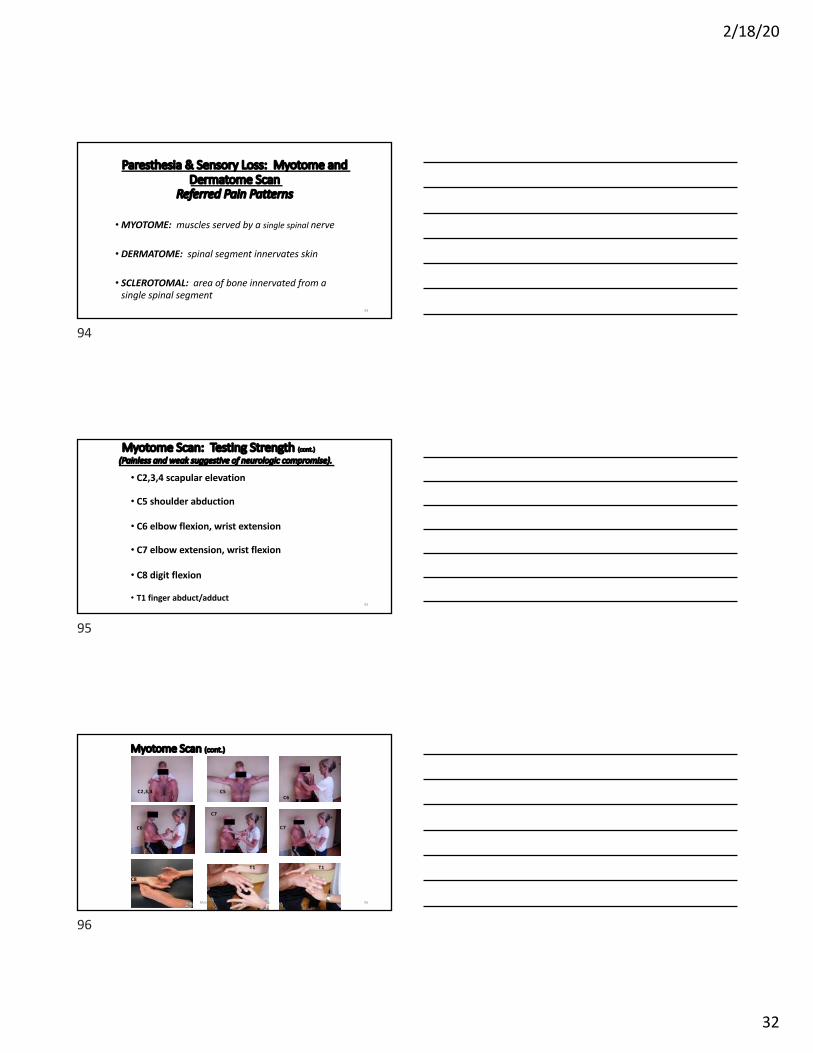
Paresthesia & Sensory Loss: Myotome and Dermatome Scan
Referred Pain Patterns
•MYOTOME: muscles served by a single spinal nerve
• DERMATOME: spinal segment innervates skin
• SCLEROTOMAL: area of bone innervated from a single spinal segment
94
94
Myotome Scan: Testing Strength (cont.)
(Painless and weak suggestive of neurologic compromise).
• C2,3,4 scapular elevation
• C5 shoulder abduction
• C6 elbow flexion, wrist extension
• C7 elbow extension, wrist flexion
• C8 digit flexion
• T1 finger abduct/adduct95
95
Myotome Scan (cont.)
Marik 2018 Nerve Compression and Injuries 96
C2,3,4 C5C6
C7
C6 C7
T1 T1
C8
96

2/18/20
33
Dermatome Pain: Testing sensory (cont.)
• C4 supraclavicular area• C5 lateral arm• C6 dorsal lateral thumb• C7 long finger• C8 ulnar hand• T1 medial forearm• T2 apex axilla
Marik 2018 Nerve Compression and Injuries 97
Retrieved on 07/05/09 from:http://en.wikipedia.org/wiki/File:Dermatoms.svg
97
Peripheral Nerve Management
98
PERIPHERAL NERVE MANAGEMENT
Post-op:• Good MD Communication• Protect surgical structures• Manage edema and pain• Sensory Re-training techniques• Cortical Retraining activities can be
helpful• Maintain Mobility of uninvolved
joints• Orthosis as indicated
Non-Op Management:• Improve Tissue mobility• Activity Modification• Improve nerve mobility• Orthosis as needed• Space, motion, and slack
99

2/18/20
34
Post-Surgical management
• Good Communication with MD is key• Type of repair?• Tension?• Nerve Graft and nerve conduits?• Nerve Transfer?
100
Sensory Re-education & Cortical Re-mapping
101
Sensory Re-education:• Localization and Discrimination• 4 to 6 months after repair
Cortical Re-mapping :• Cortical Silent period• Application EMLA cream• Cutaneous anesthesia significantly
improved distal sensation after 6 weeks• Protect surgical structures
Lundborg, G., Björkman, A., & Rosén, B. (2007). Enhanced sensory relearning after nerve repair by using repeated forearm anaesthesia: aspects on time dynamics of treatment. In How to Improve the Results of Peripheral Nerve Surgery (pp. 121-126). Springer, Vienna.
101
• Walbruch and Kalliainen retrospective study
• Established post-op standardization protocol• Result suggest cortical reorganization improve sensory outcomes.
Procedure• 2 weeks post repair forearm rubbed with anesthesia. Denervated
area rubbed with varying textures (2x wk/1 mo followed by 1xwk/4 mo).
• Visual and auditory feedback
• Imagery activities: client described how things feel.• Laminated cards with 15 action verbs read throughout the day and
client visualized doing the activity• Mirror therapy 1 to 2x daily using varying textures(Walbruch & Kallianinen, 2015)
Sensory Re-Education and Cortical Re-mapping
102
102

2/18/20
35
Sensory Re-Education: Patient is able to identify vibration 30cpsPhase II
• Nerve is beginning to innervate• Introduce traditional sensory training• Rice bins• Textures• Shapes• Tracing items with digits
103
103
Proprioceptive Activities
Marik 2018 Nerve Compression and Injuries 104
Gentle Oscillations
Light Ball Toss
Scarf Juggling
104
Non-operative Peripheral Nerve Management
• Goal is to create space, slack, and glide around the nerve• Soft tissue mobilization• Neuro mobilization/Nerve Glides (mobilize/glide)• Orthosis (create slack)• Taping (create space)• Cupping? (create space)
M. Butler (2019, May). Scrape, Cup & Glide: Neuro Mobilization for the UE. Presented at Select Physical Therapy Charlotte, NC
105

2/18/20
36
Cupping Principles
• Primary objective to provide space along the nerve bed• Compressive forces around the rim and distraction at center cup• Combine with distraction to maximize tensile and distractive forces• Static- sustained pressure/tissue distraction• Evidence?• Contraindications:
• Can produce erythema and ecchymosis• Avoid DVT• Compromised skin
M. Butler (2019, May). Scrape, Cup & Glide: Neuro Mobilization for the UE. Presented at Select Physical Therapy Charlotte, NC
106
Median Nerve
107
Pronator Syndrome AIN Syndrome
Rest; orthosis to avoid rotation
Rest; orthosis with elbow flexion at 90 degrees (8-12 wks)
Nerve glides? Nerve glides?Taping? Taping?Soft Tissue Mobilization?
Soft Tissue Mobilization?
Decompression surgery is indicated if symptoms remain.
108
108

2/18/20
37
Carpal Tunnel vs. Cervical Radiculopathy: Symptoms
109
Carpal Tunnel Cervical Radiculopathy
Paresthesia in digits #1-2 & radial side #3
Sensory deficit at lateral arm and digits #1-3
Waking due to night pain
Hand weakness, clumsy Arm and hand weakness
Upper extremity pain Pain at neck, scapula and upper extremity
Waier et al 2000
109
Interventions
Nocturnal wrist orthosis
Carpal mobilization techniques
Nerve gliding
Tendon gliding
Carpal tunnel Interventions
Marik 2018 Nerve Compression and Injuries 110
110
Carpal Tunnel Treatment
Symptoms improved with wear of nocturnal and day wrist orthosis.
Walker, Metzler, Cifu, Swartz, 2000
111
• 12 week follow-up supports full-time wear of orthosis for median motor distal latency deduction and improvement with median motor compound muscle action potential
111

2/18/20
38
Carpal & Nerve Mobilization
• Mobilization group compared to controls• Therapy 3 days a week for 4 weeks• Carpal mobilizations performed 3x for 30 seconds• Neural mobilizations performed 15 reps/3x with oscillatory elbow
flexion and extension• Mobilization group improved with function status scale and improved
motor latency
(Oskouei et. al, 2015)
112
112
Carpal Tunnel Gliding: adding digit abd/add• Traditional nerve gliding
exercises resulted in minimal gliding at the carpal tunnel.
• Adding digit abduction increased median nerve glide at carpal tunnel.• Positive numbers represent
proximal gliding
• Negative numbers represent distal gliding
(Meng et. al, 2015)
113
Median Nerve Gliding Occurs during Tendon Gliding Exercises
• Significant changes from hook to fist position• Significant changes from straight to hook position• Increased compression in controls and experimental group in
fist positionEchigo, Aoki, Ishiai, Yamaguchi, Nakamura & Sawada, 2008)
114
114

2/18/20
39
Carpal Tunnel Management
• Daily Orthosis Wear• Carpal Mobilization techniques can be helpful• Neuro mobilization with Finger Abduction• Avoid Forceful Gripping
115
115
Ulnar Nerve
116
Compression Sites Ulnar Nerve
High Lesions Low LesionsArcade of Struthers Distal to FCU and FDP
motor branchesMedial Intermuscular Septum
Guyon’s canal
Cubital TunnelFlexor carpi ulnaris (FCU)
117
117

2/18/20
40
Interventions for Ulnar NerveInterventions for CubitalTunnel
Interventions for Guyon’s Canal
Rest/Orthosis: elbow flexion block nocturnally; heelbo during waking hours
Wrist orthosis?
Patient Education Patient Education
Activity Modification: Avoid elbow flexion end range, leaning on elbow or any repetitive elbow activity.
Activity Modification: Avoid palmar compression and/or trial wear padded protective gloves
Nerve Glides Nerve Glides: Is this effective distally?
118
Interventions for Ulnar NerveCubital Tunnel Syndrome
Acute phase GOAL: Decrease pain/paresthesia• Patient education: Avoid elbow flexion and
leaning on cubital tunnel.• Activity modification: Avoid repetitive
elbow motion, elbow flexion• Orthosis (elbow at 45 degrees flexion,
wrist neutral, forearm slight supination)4-6 wks• Modalities with caution(
119
119
Conservative GuidelinesUlnar Cubital Tunnel Syndrome
Phase II GOAL: Decrease pain/paresthesia
• Orthosis wear as needed• Nerve gliding? Use with caution• Progress to strengthening as symptoms
resolve with emphasis on proximal strengthening.
Retrived on 3/31/11 from:J Hand Ther, 2006;19:170-9.
Retrieved on 3/31/11 from:http://3.bp.blogspot.com/_P0F5l7HTnDU/S4YRUUOVt4I/AAAAAAAAAJY/6vi_43V7skA/s1600/Butler.jpg.gif
Butler Tech.
120
120
2/18/20
41
Radial Nerve
121
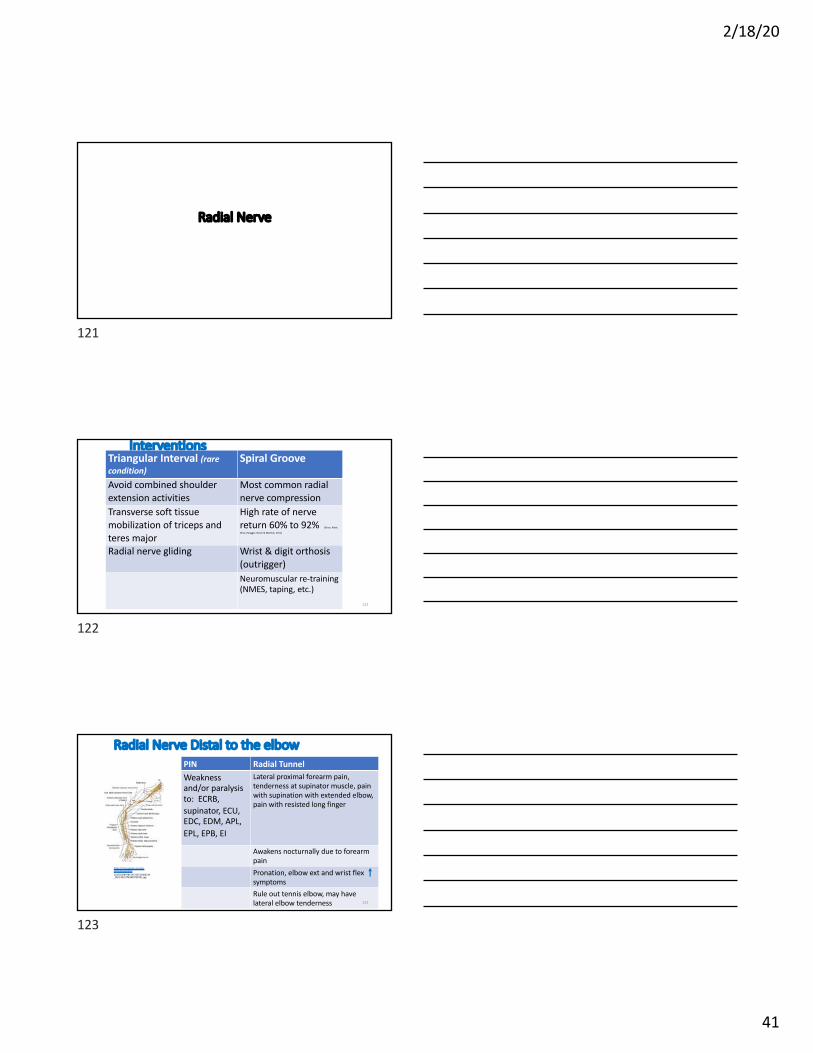
InterventionsTriangular Interval (rare condition)
Spiral Groove
Avoid combined shoulder extension activities
Most common radial nerve compression
Transverse soft tissue mobilization of triceps and teres major
High rate of nerve return 60% to 92% (Grass, Kabir,
Ohse, Rangger, Besch & Mathiak, 2011)
Radial nerve gliding Wrist & digit orthosis (outrigger)Neuromuscular re-training(NMES, taping, etc.)
122
122
Radial Nerve Distal to the elbowPIN Radial TunnelWeakness and/or paralysis to: ECRB, supinator, ECU, EDC, EDM, APL, EPL, EPB, EI
Lateral proximal forearm pain, tenderness at supinator muscle, pain with supination with extended elbow, pain with resisted long finger
Awakens nocturnally due to forearm painPronation, elbow ext and wrist flex symptomsRule out tennis elbow, may have lateral elbow tenderness
https://clinicalgate.com/wp-content/uploads/2015/03/B9781455726721000210_f021-002-9781455726721.jpg
123
123

2/18/20
42
Posterior Interossei Nerve (PIN)
Radial Tunnel
Maintain PROM
Orthosis to unload tension
Orthosis for positioningand function
Nerve gliding
Stretching wrist extensors and supinator?
Limit activities limiting pronation and elbow extension. Limit prolonged activities with wrist ext and pronation
Non-operative Management
Marik 2018 Nerve Compression and Injuries 124
124
PERIPHERAL NERVE MANAGEMENT
Post-op:• Good MD Communication• Protect surgical structures• Manage edema and pain• Sensory Re-training techniques• Cortical Retraining activities can be
helpful• Maintain Mobility of uninvolved
joints• Orthosis as indicated
Non-Op Management:• Improve Tissue mobility• Activity Modification• Improve nerve mobility• Orthosis as needed• Find a way to create Space,
motion, and slack
125
Lab: Nerve Tension Testing
and Gliding
• Slider: Tension off nerve• Tensioner: Tension on nerve
Theraband demonstration: median, ulnar, radial nerves
Abnormal responses to gliding and/or tension of a nerve can result in:• Impaired nerve mobility• Decreased nerve conduction velocity• Nerve damage• Loss of functionGoal of nerve gliding: healthy blood profusion, axonal conduction and target tissue innervations
126

2/18/20
43
Upper Limb Tension Testing SittingMedian Nerve
• Place involved side in following position:• Abduction and external rotation with slight extension• Elbow extension with forearm supination• Wrist extension• Cervical side bending to uninvolved side
Marik 2018 Nerve Compression and Injuries 127
127
Brachial Plexus Neurodynamic Test (BPNT): Grading Scale 0-5Median Nerve Bias
0/5 Supine, shoulders level with arm with arm resting on abdomen; shoulder IR and adducted and elbow at 90°n flexion; wrist and fingers in neutral
1/5 Externally rotate shoulder to neutral; keep elbow at 90° flexion; the wrist and fingers remain neutral
2/5 The wrist and fingers remain in neutral, elbow 90° flexion; radial abduct the thumb; abduct shoulder to 110° in coronal plane while blocking scapula elevation; maintain forearm neutral rotation
3/5 Externally rotate the shoulder to 90° with the elbow remaining at 90° flexion; follow with supination while keeping the digits and wrist in neutral with thumb radial abducted
4/5 Keep the above position, but slowly extend the elbow
5/5 Same as above with elbow extended, slowly extend the wrist and digits(Butler, Karagiannopoulos & Galantino, 2019)
128
+/-+ Beyond the grade but,
< half-way to the next grade
- > half-way to the next level
0/5 1/5
2/5Forearm neutral
4/5Wrist & digits
neutral
3/5Forearm supination
Established Reliability and Accuracy
(Butler, Karagiannopoulos & Galantino, 2019)
Left side testing pictured
5/5Wrist & digits
extended
129

2/18/20
44
Peripheral Nerve Glide Lab
~ 5' yellow Theratube with loop for neck and finger
• Median Nerve Glide• Neck to long finger
• Ulnar Nerve Glide• Neck, cubital tunnel, small finger
• Radial Nerve Glide• Neck, under axilla, spiral groove to index finger
130
Median Nerve:
Tension: • Shoulder abduction• Wrist/finger extension• Shoulder external rotation• Elbow extension• Cervical side-bending
Thera-tube around long fingerhttps://www.youtube.com/watch?v=Fv_EJV8q2E0
Median Nerve:Slider distally at wrist. Side bend neck to other side while flexing and extending the wrist.
Median Nerve:Slider proximally at the neck. Extend the wrist while moving the neck from side flexion to neutral or ipsilateral side flexion.
Median Nerve Gliding
131
Upper Limb Tension Testing Sitting Radial Nerve
• Place involved side in following position:• Abduction and internal rotation with slight extension• Elbow extension with forearm pronation• Wrist flexion• Add cervical side bending to uninvolved side clinical clues
Marik 2018 Nerve Compression and Injuries 132
132

2/18/20
45
Upper Limb Tension Testing Radial Nerve
Patient is supine while the examiner and fixates the scapula with body weight.Position 1: Shoulder girdle depressionPosition 2: Shoulder internal rotation & forearm pronationPosition 3: Wrist & finger flexionPosition 4: Shoulder abductionPosition 5: Cervical side-bendingPositive Tests: Symptoms with tensioning of the nerve
(Schmid et al 2009)
Differentiate• Release cervical side-
bending• Release shoulder
depression• Release wrist flexionMarik 2018 Nerve Compression and Injuries 133
133
Upper Limb Tension Testing Sitting Ulnar Nerve
• Place involved side in following position:• Abduction and external rotation• Elbow flexion with forearm pronation• Wrist flexion• Add cervical side bending to uninvolved side for clinical
cluesMarik 2018 Nerve Compression and Injuries 134
134
Upper Limb Tension Test Ulnar Nerve
Patient is supine while the examiner and fixates the scapula with body weight.Position 1: Wrist/finger extensionPosition 2: Forearm pronationPosition 3: Elbow flexionPosition 4: Shoulder external rotationPosition 5: Shoulder girdle depressionPosition 6: Shoulder abductionPositive Tests: Symptoms with tensioning of the nerve
(Schmid et al 2009)
Differentiate• Release cervical side-
bending• Release shoulder
depression• Release wrist
extension
Marik 2018 Nerve Compression and Injuries 135
135

2/18/20
46
Ulnar Nerve:Tensioner tube behind medial epicondyle:
• Wrist/finger extension• Forearm pronation• Elbow flexion• Shoulder external rotation• Shoulder girdle depression• Shoulder abduction• Cervical side bending
Thera-tube around small finger
Ulnar Nerve:Slider at the elbow. Side bend neck to opposite side. Flex and extend elbow.
Ulnar Nerve:Slider proximally. Flex elbow and side bend neck to neutral or opposite side. May need to modify elbow extension.
Ulnar Nerve Gliding
136
Radial Nerve:
Tensioner wrap the tube around the humerus.
• Shoulder girdle depression• Shoulder internal rotation &
forearm pronation• Wrist & finger flexion• Shoulder abduction 40° & ext 20°• Cervical side-bending
Thera-tube around index finger.
Radial Nerve:Slider at the wrist. Side bend neck to opposite side while flex/extend wrist to tolerance.
Radial Nerve:Slider proximally. Move neck to opposite side and back to neutral with the wrist extended.
Radial Nerve Gliding
137
Novel Median Nerve Gliding Techniques
• Exercise 1: ER & Abd. at shoulder, elbow extension, supination, wrist and digit extension while performing digit abd./add.
https://www.youtube.com/watch?v=Hl0CIg8QwY4
• Exercise 2: ER & Abd. at shoulder, elbow extension, supination, wrist and digit extension while performing forearm supination and pronation
138

2/18/20
47
Novel Median Nerve Gliding Techniques
• Exercise 3: ER & Abd. at shoulder, elbow extension, supination, wrist and digit extension while performing elbow flexion and extension
Modify with sliding at cervical (side bend when elbow is extended)
139
Novel Median Nerve Gliding Techniques
• Exercise 4: ER & Abd. at shoulder, elbow extension, supination, wrist and digit extension while performing shoulder circumduction
• Exercise 5: ER & Abd. at shoulder, elbow extension, supination, wrist and digit extension while performing shoulder distraction with side cervical bending
140
References• Apelby-Albrecht, M., Andersson, L., Kleiva, I. W., Kvåle, K., Skillgate, E., & Josephson, A. (2013). Concordance of upper limb neurodynamic tests with medical
examination and magnetic resonance imaging in patients with cervical radiculopathy: a diagnostic cohort study. Journal of manipulative and physiological therapeutics, 36(9), 626-632.
• Arslantunali, D., Dursun, T., Yucel, D., Hasirci, N., & Hasirci, V. (2014). Peripheral nerve conduits: technology update. Medical Devices (Auckland, NZ), 7, 405.
• Ballestero-Pérez, R., Plaza-Manzano, G., Urraca-Gesto, A., Romo-Romo, F., de los Ángeles Atín-Arratibel, M., Pecos-Martín, D., ... & Romero-Franco, N. (2017). Effectiveness of nerve gliding exercises on carpal tunnel syndrome: a systematic review. Journal of manipulative and physiological therapeutics, 40(1), 50-59.
• Brismée, J. M., Gilbert, K., Isom, K., Hall, R., Leathers, B., Sheppard, N., ... & Sizer, P. (2004). Rate of false positive using the cyriax release test for thoracic outlet syndrome in an asymptomatic population. Journal of Manual & Manipulative Therapy, 12(2), 73-81.
• Butler, M. W., Karagiannopoulos, C., Galantino, M. L., & Mastrangelo, M. A. (2019). Reliability and accuracy of the brachial plexus neurodynamic test. Journal of Hand Therapy, 32(4), 483-488.
• Butler D (2000) The sensitive nervous system. Adelaide: Noigroup Publications
• DeFrancesco, C. J., Shah, D. K., Rogers, B. H., & Shah, A. S. (2019). The epidemiology of brachial plexus birth palsy in the United States: declining incidence and evolving risk factors. Journal of Pediatric Orthopaedics, 39(2), e134-e140.
• Donatelli, R. A., & Wooden, M. J. (2009). Orthopaedic Physical Therapy-E-Book. Elsevier health sciences.
• Fejer, R., Kyvik, K. O., & Hartvigsen, J. (2006). The prevalence of neck pain in the world population: a systematic critical review of the literature. European spine journal, 15(6), 834-848.
• Grubb S, Kelly C. & Bogduk N. (2000). Cervical discography: clinical implications from 12 years of experience.Spine, 25:1382-9
• Griegel-Morris, P., Larson, K., Mueller-Klaus, K., & Oatis, C. A. (1992). Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Physical therapy, 72(6), 425-431.
• Gumina, S., Carbone, S., Albino, P., Gurzi, M., & Postacchini, F. (2013). Arm Squeeze Test: a new clinical test to distinguish neck from shoulder pain. European Spine Journal, 22(7), 1558-1563.
141

2/18/20
48
• Hurst, L. C., Weissberg, D., & Carroll, R. E. (1985). The relationship of the double crush to carpal tunnel syndrome (an analysis of 1,000 cases of carpal tunnel syndrome). The Journal of Hand Surgery: British & European Volume, 10(2), 202-204.
• Jones, M. R., Prabhakar, A., Viswanath, O., Urits, I., Green, J. B., Kendrick, J. B., ... & Kaye, A. D. (2019). Thoracic outlet syndrome: a comprehensive review of pathophysiology, diagnosis, and treatment. Pain and therapy, 8(1), 5-18.
• Klein, L. J. (2014). Evaluation of the hand and upper extremity. Fundamentals of hand therapy-e-book: clinical reasoning and treatment guidelines for common diagnoses of the upper extremity. Elsevier, St. Louis, 67-86.
• Kleinrensink, G. J., Stoeckart, R., Mulder, P. G. H., Hoek, G. V. D., Broek, T. H., Vleeming, A., & Snijders, C. J. (2000). Upper limb tension tests as tools in the diagnosis of nerve and plexus lesions: anatomical and biomechanical aspects. Clinical Biomechanics, 15(1), 9-14
• Kurumadani, H., Yoshimura, M., Fukae, A., Onishi, K., Hayashi, J., Shinomiya, R., & Sunagawa, T. (2019). Long-term disuse of the hand affects motor imagery ability in patients with complete brachial plexus palsy. NeuroReport, 30(6), 452-456.
• Lascar, T., & Laulan, J. (2000). Cubital tunnel syndrome: a retrospective review of 53 anterior subcutaneous transpositions. Journal of Hand Surgery, 25(5), 453-456.
• Lee, A., & Lee-Robinson, A. (2010). Evaluating concomitant lateral epicondylitis and cervical radiculopathy: a correlation was found, suggesting comanagement of the disorders. The Journal of Musculoskeletal Medicine, 27(3), 111-111.
• Lindgren, K. A., Leino, E., & Manninen, H. (1992). Cervical rotation lateral flexion test in brachialgia. Archives of physical medicine and rehabilitation, 73(8), 735-737.
• Lemeunier, N., da Silva-Oolup, S., Chow, N., Southerst, D., Carroll, L., Wong, J. J., ... & Murnaghan, K. (2017). Reliability and validity of clinical tests to assess the anatomical integrity of the cervical spine in adults with neck pain and its associated disorders: Part 1—A systematic review from the Cervical Assessment and Diagnosis Research Evaluation (CADRE) Collaboration. European Spine Journal, 26(9), 2225-2241.
•Manvell, N., Manvell, J. J., Snodgrass, S. J., & Reid, S. A. (2015). Tension of the ulnar, median, and radial nerves during ulnar nerve neurodynamic testing: observational cadaveric study. Physical therapy, 95(6), 891-900.
• Novak, C. B., & Mackinnon, S. E. (2005). Evaluation of nerve injury and nerve compression in the upper quadrant. Journal of Hand Therapy, 18(2), 230-240.
• Rodrıguez-Sanz, D., Calvo-Lobo,C., Francisco Unda-Solano, F., Sanz-Corbalan, I., Romero-Morales, C., & Lopez-Lopez, D. (2017). Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical Trial. Pain Medicine; 18: 2492–2503. doi: 10.1093/pm/pnx011
142
• Sikandar, S., & Dickenson, A. H. (2012). Visceral pain–the ins and outs, the ups and downs. Current opinion in supportive and palliative care, 6(1), 17. •Meng, S., Reissig, L. F., Beikircher, R., Tzou, C. H. J., Grisold, W., & Weninger, W. J. (2015). Longitudinal gliding of the median nerve in the carpal tunnel: Ultrasound cadaveric evaluation of conventional and novel concepts of nerve mobilization. Archives of physical medicine and rehabilitation, 96(12), 2207-2213.• Saavedra-Hernández, M., Castro-Sánchez, A. M., Arroyo-Morales, M., Cleland, J. A., Lara-Palomo, I. C., & Fernandez-De-Las-Penas, C. (2012). Short-term effects of kinesiotaping versus cervical thrust manipulation in patients with mechanical neck pain: a randomized clinical trial. journal of orthopaedic & sports physical therapy, 42(8), 724-730.• Smith, T. M., Sawyer, S. F., Sizer, P. S., & Brismée, J. M. (2008). The double crush syndrome: a common occurrence in cyclists with ulnar nerve neuropathy-a case-control study. Clinical Journal of Sport Medicine, 18(1), 55-61.• Strauch, B., Lang, A., Ferder, M., Keyes-Ford, M., Freeman, K., & Newstein, D. (1997). The ten test. Plastic and reconstructive surgery, 99(4), 1074-1078.• Stewman C, Vitanzo PC, Harwood MI. (2014). Neurologic thoracic outlet syndrome: summarizing a complex history and evolution. Curr Sports Med Rep.;13(2):100–6.• Upton AR, McComas AJ (1973). The double crush in nerve entrapment syndromes. Lancet, 7825:359–362
• Urschel, J. D., Hameed, S. M., & Grewal, R. P. (1994). Neurogenic thoracic outlet syndromes. Postgraduate medical journal, 70(829), 785
• Van Blommestein, A. S., MaCrae, S., Lewis, J. S., & Morrissey, M. C. (2012). Reliability of measuring thoracic kyphosis angle, lumbar lordosis angle and straight leg raise with an inclinometer. Open Spine Journal.
• Voorhies, R. M. (2001). Cervical spondylosis: recognition, differential diagnosis, and management. Ochsner Journal, 3(2), 78-84.
•Wainner, R. S., Fritz, J. M., Irrgang, J. J., Boninger, M. L., Delitto, A., & Allison, S. (2003). Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine, 28(1), 52-62.
•Wazir, N. N., & Kareem, B. A. (2011). New clinical sign of cervical myelopathy: Wazir hand myelopathy sign. Singapore medical journal, 52(1), 47-49.
• Yukawa, Y., Nakashima, H., Ito, K., Machino, M., Kanbara, S., & Kato, F. (2013). Quantifiable tests for cervical myelopathy; 10-s grip and release test and 10-s step test: standard values and aging variation from 1230 healthy volunteers. Journal of Orthopaedic Science, 18(4), 509-513.
143
Website References
• https://www.orthobullets.com/spine/2031/cervical-myelopathy
144