Embed Size (px)
Citation preview
Personality Disordersin the Primary Care Setting
Presented by: Jonathan Betlinski, MDDate: 02/05/2015
Disclosures and Learning Objectives
Learning Objectives:•Know what percentage of Primary Care Patients have a Personality Disorder•Be familiar with the common diagnostic features of Personality Disorders•Know the names and clusters of all ten Personality Disorders•Be able to name at least three strategies for success with each Disorder Cluster
Disclosures: Dr. Jonathan Betlinski has nothing to disclose.
Personality Disorders in Primary Care
• Review the epidemiology of Personality Disorders
• Review the diagnostic criteria for Personality Disorders
• Discuss the impact of Personality Disorders in Primary Care
• Discuss strategies for working with those who have Personality Disorders
Personality Disorders: Epidemiology
Personality Disorders are quite common• 9% currently have a Personality Disorder• 10-13% lifetime prevalence• Up to 30% of Primary Care patients
Individuals with Personality Disorders have• Poorer health status• Poorer treatment outcomes• Higher rates of healthcare use• Higher overall healthcare costs
http://apt.rcpsych.org/content/8/1/1.full.pdf+html; http://www.aafp.org/afp/2004/1015/p1505.pdf
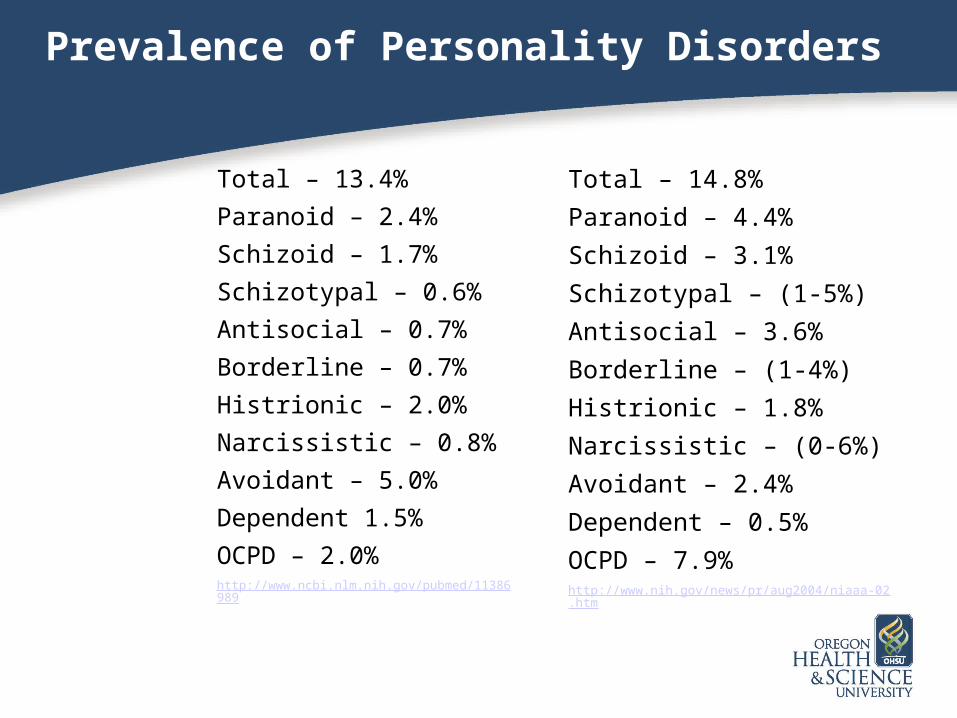
Prevalence of Personality Disorders
Total – 13.4%
Paranoid – 2.4%
Schizoid – 1.7%
Schizotypal – 0.6%
Antisocial – 0.7%
Borderline – 0.7%
Histrionic – 2.0%
Narcissistic – 0.8%
Avoidant – 5.0%
Dependent 1.5%
OCPD – 2.0%http://www.ncbi.nlm.nih.gov/pubmed/11386989
Total – 14.8%
Paranoid – 4.4%
Schizoid – 3.1%
Schizotypal – (1-5%)
Antisocial – 3.6%
Borderline – (1-4%)
Histrionic – 1.8%
Narcissistic – (0-6%)
Avoidant – 2.4%
Dependent – 0.5%
OCPD – 7.9%http://www.nih.gov/news/pr/aug2004/niaaa-02.htm
Personality Disorders: Diagnosis
A. An enduring pattern of inner experience and behavior that deviates markedly from the expectations of an individual’s culture. The pattern is manifested in two (or more) of the following ways
• Cognition
• Affectivity
• Interpersonal Function
• Impulse Control
http://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
http://www.dsm5.org/Documents/Personality%20Disorders%20Fact%20Sheet.pdf
Personality Disorders: Diagnosis
B. The enduring pattern is inflexible and pervasive across a broad range of personal and social situations
C. The enduring pattern leads to clinically significant distress or impairment in social, occupational or other important areas of functioning
D. The pattern is stable and of long duration, and its onset can be traced back at least to adolescence or early adulthood
http://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Personality Disorders: Diagnosis
Problematic Personality Patterns
PervasivePersistent
Present early
Cluster A: Odd or Eccentric Behaviors
Cluster A Personality DisordersParanoid
Schizoid
Schizotypal
Management strategies• Adopt a respectful, professional stance
• Provide clear expectations
• Avoid over-involvement in personal and social issues https://www.harvardpilgrim.org/portal/page?_pageid=253,840018&_dad=portal&_schema=PORTAL
Paranoid Personality Disorder
Mistrust and Suspiciousness of others (4/7)
• Suspects, without sufficient basis, that others are exploiting, harming or deceiving him or her
• Is preoccupied with unjustified doubts about the loyalty or trustworthiness of friends or associates
• Is reluctant to confide in others because of unwarranted fear that the information will be used maliciously against him or her
• Reads hidden demeaning or threatening meanings into benign remarks or events
• Persistently bears grudges, i.e. is unforgiving of insults, injuries or slights
• Perceives attacks on his or her character or reputation that are not apparent to others and is quick to react angrily or to counterattack
• Has recurrent suspicions, without justification, regarding fidelity of spouse or sexual partner
http://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Paranoid Personality Disorder: Management
Challenges• Fear physician may harm• Arguments and other conflict
Strategies for Success• Adopt a professional stance• Provide clear explanations• Be empathetic to fears• Avoid directly challenging paranoid ideation
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Schizoid Personality Disorder
Restricted Range of Emotional Expression &
Detachment from Social Relationships (4/7)• Neither desires nor enjoys close relationships, including being part of a
family
• Almost always chooses solitary activities
• Has little, if any, interest in having sexual experiences with another person
• Takes pleasure in few, if any, activities
• Lacks close friends or confidants other than first-degree relatives
• Appears indifferent to the praise or criticism of others
• Shows emotional coldness, detachment, or flattened affectivityhttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Schizoid Personality Disorder: Management
Challenges• Delay in seeking care• Appear unappreciative
Strategies for Success• Adopt a professional stance• Provide clear explanations• Avoid over-involvement in personal and social
issueshttp://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Schizotypal Personality Disorder
Cognitive, Behavioral, Perceptual Oddities &
Discomfort with Close Relationships (4/8)• Ideas of reference
• Odd beliefs or magical thinking that influences behavior and is inconsistent with subcultural norms
• Unusual perceptual experiences, including bodily illusions
• Odd thinking and speech (vague, circumstantial, metaphorical, etc)
• Suspiciousness or Paranoid Ideation
• Inappropriate or constricted affect
• Behavior or appearance that is odd, eccentric, or peculiar
• Lack of close friends or confidants other than first-degree relativeshttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Paranoid Personality Disorder: Management
Challenges• Delay in seeking care• Odd beliefs and behaviors
•Strategies for Success• Adopt a professional stance• Provide clear explanations• Tolerate odd beliefs and behaviors• Avoid directly challenging paranoid ideation
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Cluster B: Dramatic or Erratic Behaviors
Cluster B Personality DisordersAntisocial
Borderline
Histrionic
Narcissistic
Management Strategies• Set Clear Limits
• Avoid Excessive Familiarity
• Provide clear, non-technical explanationshttps://www.harvardpilgrim.org/portal/page?_pageid=253,840018&_dad=portal&_schema=PORTAL
http://www.nimh.nih.gov/news/science-news/2007/national-survey-tracks-prevalence-of-personality-disorders-in-us-population.shtml
Antisocial Personality Disorder
Disregard for and Violation of Others’ Rights by age 15 (3/7)
• Failure to conform to social norms with respect to lawful behaviors as indicated by repeatedly performing acts that are grounds for arrest
• Deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure
• Impulsivity or failure to plan ahead
• Irritability and aggressiveness, as indicated by repeated physical fights or assaults
• Reckless disregard for safety of self and others
• Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations
• Lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated or stolen from another
http://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Antisocial Personality Disorder: Management
Challenging Behaviors• Anger• Deceit• Impulsive or manipulative behavior
Strategies• Carefully investigate concerns and motives• Communicate clearly and non-punitively• Set clear limits
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Borderline Personality Disorder
Instability of Interpersonal Relationships, Self-Image and Affects (5/9)
• Frantic efforts to avoid real or imagined abandonment
• A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation
• Identity disturbance: markedly and persistently unstable self-image or sense of self
• Impulsivity in at least two areas that are potentially self-damaging
• Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior
• Affective instability due to a marked reactivity of mood
• Chronic feelings of emptiness
• Inappropriate, intense anger or difficulty controlling anger
• Transient, stress-related paranoid ideation or severe dissociative symptomshttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Borderline Personality Disorder: Management
Challenging Behaviors• Fear of rejection and abandonment• Self-destructive acts• Idealization and devaluation of PCP
Strategies• Avoid excessive familiarity• Use Relationship Management Techniques• Refer for Dialectic Behavioral Therapy
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2379842/pdf/canfamphys00110-0101.pdf
Histrionic Personality Disorder
Excessive Emotion & Attention-Seeking (5/8)• Is uncomfortable in situations in which he or she is not the center of attention
• Interaction with others is often characterized by inappropriate sexually seductive or provocative behavior
• Displays rapidly shifting and shallow expression of emotions
• Consistently uses physical appearance ot draw attention to self
• Has a style of speech that is excessively impressionistic and lacking in detail
• Shows self-dramatization, theatricality, and exaggerated expression of emotion
• Is suggestible, i.e., easily influenced by others or circumstances
• Considers relationships to be more intimate than they actually arehttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Histrionic Personality Disorder: Management
Challenging Behaviors• Overly dramatic, attention-seeking behavior• Inability to focus on facts and details• Somatization
Strategies• Avoid excessive familiarity• Show professional concern for feelings• Emphasize objective issues
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Narcissistic Personality Disorder
Grandiosity, Need for Admiration, and Lack of Empathy (5/9)
• Has a grandiose sense of self importance
• Is preoccupied with fantasies of unlimited success, power, brilliance, beauty or ideal love
• Believes that he or she is “special” and unique and can only be understood by, or should associate with, other special or high-status people
• Requires excessive admiration
• Has a sense of entitlement (expects especially favorable treatment)
• Is interpersonally exploitative (takes advantage of others for own ends)
• Lacks empathy (unwilling to recognize feelings and needs of others)
• Is often envious of others or believes that others are envious
• Shows arrogant, haughty behaviors or attitudeshttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Narcissistic Personality Disorder: Management
Challenging Behaviors• Frequently demanding• Denial of illness• Alternating praise and devaluation of PCP
Strategies for Success• Validate concerns• Give attentive and factual responses• Channel patient’s skills into dealing with illness
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Cluster C: Anxious or Fearful Behaviors
Cluster C Personality DisordersAvoidant
Dependent
Obsessive-Compulsive
Management Strategies• Provide reassurance
• Provide thorough explanations
• Encourage patient participation in treatmenthttps://www.harvardpilgrim.org/portal/page?_pageid=253,840018&_dad=portal&_schema=PORTAL
Avoidant Personality Disorder
Social Inhibition, Feelings of Inadequacy, Hypersensitivity to Negative Eval (4/7)
• Avoids occupational activities that involve significant interpersonal contact, because of fears of criticism, disapproval or rejection
• Is unwilling to get involved with people unless certain of being liked
• Shows restraint within intimate relationships because of the fear of being shamed or ridiculed
• Is preoccupied with being criticized or rejected in social situations
• Is inhibited in new interpersonal situations because of feelings of inadequacy
• Views self as socially inept, personally unappealing or inferior to others
• Is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing
http://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Avoidant Personality Disorder: Management
Challenging Behaviors• Withholds information• Avoids questioning providers• Avoids disagreeing with providers
Strategies for Success• Provide reassurance and validate concerns• Consider referral for Behavioral Therapy• Encourage reporting of symptoms and concerns
http://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Dependent Personality Disorder
Excessive need to be taken care of, Submissive/Clinging Behaviors (5/8)
• Has difficulty making everyday decisions without an excessive amount of advice and reassurance from others
• Needs others to assume responsibility for most major areas of his or her life
• Has difficulty expressing disagreement with others because of fear of loss of support or approval
• Has difficulty initiating projects or doing things on his or her own
• Goes to excessive lengths to obtain nurturance and support from others
• Feels uncomfortable or helpless when alone because of exaggerated fears of being unable to care for himself or herself
• Urgently seeks another relationship as a source of care and support when a close relationship ends
• Is unrealistically preoccupied with fears of being left to take care of himself or herselfhttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Dependent Personality Disorder: Management
Challenging Behaviors• Urgent demands for attention• Prolongation of illness to obtain care and other
attention
Strategies for Success• Provide reassurance; avoid rejection• Schedule regular check-ups• Set realistic limits on availability• Enlist others to support patient http://www.aafp.org/afp/2004/1015/p1505.pdf;
http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Obsessive-Compulsive Personality Disorder
Need for Orderliness, Perfection, Control (4/8)• Is preoccupied with details, rules, lists, order, organization or schedules to the extent
that the major point of the activity is lost
• Shows perfectionism that interferes with task completion
• Is excessively devoted to work and productivity to the exclusion of leisure activities and friendships
• Is overconscientious, scrupulous, and inflexible about matters of morality, ethics or values
• Is unable to discard worn-out or worthless objects even when they have no sentimental value
• Is reluctant to delegate tasks or to work with others unless they submit to exactly his or her way of doing things
• Adopts a miserly spending style toward both self and others
• Shows rigidity and stubbornnesshttp://www.psi.uba.ar/academica/carrerasdegrado/psicologia/sitios_catedras/practicas_profesionales/820_clinica_tr_personalidad_psicosis/material/dsm.pdf
Obsessive-Compulsive Personality Disorder: Management
Challenging Behaviors• Fear of relinquishing control• Excessive questions and attention to details• Anger about disruption of routines
Strategies for Success• Thorough histories, exams and explanations• Encourage patient participation in treatment• Do not overemphasize uncertaintyhttp://www.aafp.org/afp/2004/1015/p1505.pdf; http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
Personality Disorders: Pharmacology
• Lithium may be helpful for aggression• AEDs may help mood instability, irritability
and impulsivity• Antipsychotics may help psychotic symptoms,
especially in Schizotypal PD• SSRIs may help BPD• SSRIs may help with Cluster C anxiety
http://apt.rcpsych.org/content/8/1/1.full.pdf+html
Summary
• Personality Disorders are very common in Primary Care settings
• Remembering the basic features of each cluster (and disorder) will help you remember the best style of interaction
• Pharmacology is less likely to be helpful for Personality Disorders
• When in doubt, refer for an assessment and therapy
http://cdn.hivguidelines.org/wp-content/uploads/2009/06/m-personality.pdf
The End!
Obsessive-Compulsive
Disorder
02/12/15
http://proof.nationalgeographic.com/2014/12/08/photo-of-the-day-best-of-november-2/?source=photosite