Embed Size (px)
Citation preview

Peter T. Buser Klinik Kardiologie
Unviersitätsspital Basel
Antithrombotic Summit Basel 2012 Basel, 26. April 2012

Background
stroke = third-leading cause of death among adults
1/5 of stroke survivors require institutional care > 3 months
USA: of 780‘000/a strokes 180‘000 are recurrent events
90 day risk of stroke after TIA estimated at 3-17%
25-40% of all strokes are designated cryptogenic (CS)
prevalence of PFO/ASA higher in CS as compared to stroke
with known cause or general population
optimal treatment of cryptogenic stroke??

Closure or Medical Therapy for Cryptogenic Stroke with PFO
Furlan AJ et al. N Engl J Med 2012; 366: 991.
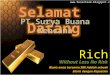
909 pat (18-60 yo) with TIA/ischemic stroke within 6 months, PFO exclusion: CA stenosis, complex aortic arch atheroma, significant LV dysfunction or LV aneurysm, AF

Agenda
morphology and diagnosis of PFO/ASA
PFO/ASA as a risk factor for cryptogenic stroke
medical therapy for stroke prevention in the presence of PFO
PFO closure vs medical therapy for stroke prevention
guidelines 2012 for stroke prevention with PFO
summary

Prevalence, Morphology and Diagnosis of PFO/ASA
PFO at autopsy: 17-27% PFO with TEE (stroke free): 14-24% ASA with TEE (stroke free): 1.9-2.5% diameter PFO: 4.9 (1-19)mm length of PFO: 9.4 (2.4-19.5)mm
Hagen PT et al. Mayo Clin Proc 1984;59:17. Di Tullio MR et al. JACC 2007;49:797. Meissner I et al. JACC 2006;47:440.

Handke M et al. N Engl J Med 2007; 357:2262.
503 pat with stroke (20-84 yo)
26% < 55 yo 45% cryptogenic:
63% of pat <55 yo 39% of pat >55 yo

PFO and the Risk of Ischemic Stroke in a Multiethnic Population (NOMAS)
Di Tullio MR et al. J Am Coll Cardiol 2007; 49:797.
1148 stroke free subjects (58% female, 68±10 yo), TTE with saline injection

Patent Foramen Ovale: Innocent or Guilty? Evidence from a Prospective Population-Based Study
(Olmsted County, MA)
91% vs 93% 81% vs 93%
Meissner I et al. J Am Coll Cardiol 2006; 47:440.
585 subjects (50% male, 67±13 yo), TEE to identify PFO/ASA PFO in 140/577 (24%), ASA in 11/577, 6/11 ASA with PFO FU 5 years, EP: CV events (TIA, stroke, death due to TIA/stroke))

Mas JL et al. N Engl J Med 2001; 345:1740.
1340 consecutive stroke pat (18-55 yo) 51% with known cause of stroke 22% excluded
598 (27%) included, TTE and TEE 304 without atrial septal anomalies 216 with PFO 10 with ASA alone 51 with PFO+ASA FU 5.1 years

Secondary Prevention of Cerebral Ischemia in PFO: Systematic Review and Meta-Analysis
Orgera MA et al. South Med J 2001; 94:699.
aspirin vs warfarin warfarin vs surgical closure

Effect of Medical Treatment in Stroke Patients with PFO: The PICS Study
Homma S et al. Circulation 2002; 105:2625.
Substudy of WARSS: 2206 stroke pat randomized to aspirin vs warfarin. FU 24 months. EP: recurrent ischemic stroke or death. 630 CS pat (WARSS) underwent TEE for identifiaction of PFO/ASA PFO in 203/630 (33.8%), ASA in 11.5%

Clinically Used Closure Devices for PFO
Meier B et al. Eur Heart J 2012; 32: 705.

Incidence and Clinical Course of Thrombus Formation on ASD and PFO Closure Devices in 1000 Consecutive
Patients
Krumsdorf U et al. J Am Coll Cardiol 2004; 43:302.

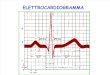
Comparison of Medical Treatment with Percutaneous Closure of PFO in Patients with Cryptogenic Stroke
Windecker S et al. J Am Coll Cardiol 2004; 44:750.
308 pat with CS and PFO (TEE). 150 underwent PFO closure, 158 were treated medically (aspirin or VKA).Death, stroke, TIA.
death, stroke, TIA stroke, TIA

Wahl A et al. Circulation 2012; 125: 803.
Long-Term Propensity Score-Matched Comparison of Percutaneous Closure of PFO with Medical Treatment
after Paradoxical Embolism

Wahl A et al. Circulation 2012; 125: 803.
Long-Term Propensity Score-Matched Comparison of Percutaneous Closure of PFO with Medical Treatment
after Paradoxical Embolism

Closure or Medical Therapy for Cryptogenic Stroke with PFO
Furlan AJ et al. N Engl J Med 2012; 366: 991.

Limitations of the Study by Furlan et al
patient selection bias: > 5 years 909 pat included, > 80‘000
devices implanted
lacunar strokes included: no benefit of PFO closure expected
selection of closure device: highest rate of thrombosis
statistical power: sample size reduced, 2pat/center,
reduction of 10 EP by 55% with PFO
closure

Recommendations for Antithrombotic Therapy: PFO and ASA
asymtpomatic PFO/ASA: no antithrombotic TX
cryptog. stroke with PFO/ASA: aspirin 50-100 mg/d
recurrent events despite aspirin: VKA (INR 2.0-3.0)
consideration of device closure
cryptog. stroke, DVT and PFO/ASA: VKA > 3 months (INR 2.0-3.0)
consideration of device closure
Whitlock RP et al. ACCP Evidence-based Practice Guidelines. Chest 2012;141:e576S.

Summary
correlation between occurence of cryptogenic stroke and finding of
PFO/ASA
however, causative prove only in single cases
primary prevention with PFO not recommended
for secondary prevention of cryptogenic stroke with PFO,
observational and comparative data seem to favour closure vs
medical therapy
however: one randomized study did not show significant benefit of
closure vs medical therapy and further hard evidence is lacking