Embed Size (px)
Citation preview

ภญ.ณัฎฐณิชา ศภุลกัษณ์บนัลือPediatric Clinical Pharmacists
Ramathibodi Hospital
1
pH & Osmolarityof Solutions

Outline
Extravasation
– Chemotherapy
– Vascular regulators
– Hyperosmolar
– Acid & Alkaline agents
Compatibility
ตวัอย่างสารนํ�าและการผสมยาที�สั �งใช้บอ่ยในเดก็
Case Study2
TOPICs

3
Extravasation Drugs
Chemotherapy
HyperosmolarAcid & Alkaline agents
Acid & Alkaline agents
Vascular Regulators Vascular
Regulators

4
Vascular regulators
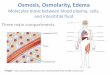
กลไกในการเกิด extravasation
Richard E. Klabunde.Cardiovascular Physiology Concepts. 2011

ยาที�ใช้แล้วส่งผลให้เกิด Extravasation ได้บอ่ย ได้แก่ Adrenaline, Dobutamine, Dopamine, Noradrenaline, Vasopressin
5
Vascular regulators

6
Vascular regulators

7
Vascular regulators
ถ้าผูป้ฏิบติังานพบว่าผูป่้วยเกิดอาการดงักล่าวขึ�น ควรหยดุให้ยาในทนัที พยายามดึงยาที�เหลือออกมาจากเส้นให้ได้มากที�สดุ และประเมินว่าผูป่้วยมีอาการมากน้อยเพียงใด แล้วประคบอุ่นให้กบัผูป่้วยเพื�อช่วยขยายหลอดเลือดในส่วนนั�น โดยยาที�ใช้ในการรกัษาอาการ ได้แก่
Phentolamine 5 – 10 mg in 10 – 20 ml (hypodermic)
Terbutaline 1 mg in 10 ml (SC) 2% Topical nitroglycerin
การรกัษาโดยทั �วไป

8
Vascular regulators
Norepinephrine
12/10/2017 01/11/2017

9
Hyperosmolar
Osmolarity คือ ความเข้มข้นของสารที�อยู่ในสารละลาย วดัเป็นออสโมลของตวัถกูละลายต่อลิตรของสารละลายPlasma osmolarity (Posm) เป็นตวักาํหนดที�สาํคญัของปริมาณนํ�าในเซลลต่์างๆ ของร่างกาย เนื�องจากค่า osmolarity จะเท่ากนัทั �งร่างกาย ทั �งใน ICF และ ECF ดงันั�น ถ้ามีการเปลี�ยนแปลงของ plasma osmolarity จะทาํให้มีการซึมของนํ�าเข้า หรือออกจากเซลล์มากขึ�นเพื�อปรบัให้ osmolarity เท่ากนั
Posm = 2(PNa) + Glucose + BUN 18 2.8
ค่าปกติของ plasma osmolarity = 275-290 mosmol/kg

10
Hyperosmolar
https://oli.cmu.edu/jcourse/workbook/activity/page?context=434a5e0380020ca601cb36072cd41718
กลไกในการเกิด extravasation

11
Hyperosmolar
• 10% Calcium chloride, 10% Calcium gluconate
• Hypertonic glucose (>10%)
• 20% Magnesium sulfate
• Mannitol (10-20%)
• Parenteral nutrition
• Potassium chloride (>40 mEq/L)
• Sodium bicarbonate

12
Hyperosmolar
669 mOsm/L Dilute in NSS, D5W Maximum conc. 20 mg/ml Maximum rate : 200 mg/min
10% Calcium gluconate

13
Hyperosmolar
4000 mOsm/L Dilute in NSS, D5W Peripheral infusion :
Maximum conc. = 100 mEq/L Maximum rate = 10 mEq/hr
Central infusion : Maximum conc. = 200-400 mEq/L Maximum rate = 40 mEq/hr
Potassium chloride

14
Hyperosmolar
7400 mOsm/L Dilute in NSS, D5W Peripheral line :
Maximum conc. = 67 mmol K2HPO4/L(100 mEq of potassium/L)
Maximum rate = 10 mEq of potassium/hr
Central line administration: Maximum conc. = 268 mmol K2HPO4/L
(40 mEq potassium/L) Maximum rate = 40 mEq of potassium/hr
Dipotassium phosphate

15
Hyperosmolar
4060 mOsm/L Dilute in NSS, D5W Maximum conc. 200 mg/ml Maximum rate
I.V. infusion : 2 - 4 g/hr I.V. push : 150 mg/min
50% Magnesium sulfate

16
HyperosmolarPeripheral Parenteral Nutrition (PPN) การให้โภชนบาํบดัทางหลอดเลือดดาํส่วนปลาย
• คาดว่าทาํการรกัษาในระยะเวลาสั �น (10-14 วนั)• ความต้องการพลงังานและโปรตีนอยู่ในระดบั
ปานกลาง• Osmolarity 600 - 900 mOsm/L • ไม่จาํกดัสารนํ�า

17
HyperosmolarTotal Parenteral Nutrition (TPN) การให้โภชนบาํบดัทางหลอดเลือดดาํส่วนกลาง
• มีความต้องการพลงังานและโปรตีนแบบครบถ้วน
• ไม่จาํกดั Osmolarity• จาํกดัสารนํ�า

18
Hyperosmolar
1) ควรหยดุให้ยาในทนัที 2) ดึงยาออกจากเส้นให้มากที�สดุ 3) ประเมินว่าผูป่้วยมีอาการมากน้อยเพียงใด 4) ประคบเยน็เพื�อป้องกนัไม่ให้ยาออกไปทาํลายเส้นเลือดมาก
กว่าเดิม และใช้ antidote ได้แก่ Hyaluronidase* ซึ�งเป็นเอนไซน์ที�ช่วยให้ตวัยากระจายเข้าสู่ผิวหนังได้ดีขึ�น
5) ติดตามการให้ยาทุก 30 นาที
การรกัษาโดยทั �วไป
* หากไม่มีอาจใช้เป็น moderate topical steroid แทน

19
acid & alkaline agents
https://vimeo.com/93586253https://www.phreshproducts.com/

20
acid & alkaline agents
ลกัษณะการทาํลายเส้นเลือดมี 2 แบบ คือ การทาํลายแบบกรด : กรดจะดึงนํ�าออกจากเซลล ์ทาํให้เกิด
การทาํลายของเนื�อเยื�อที�สมัผสัแบบ Coagulation necrosis มีผลทาํให้เนื�อเยื�อแขง็หนา (Eschar formation) ซึ�งเป็นการจาํกดัขอบเขตของการได้รบัอนัตรายด้วยตนเอง
การทาํลายแบบด่าง : ด่างจะทาํให้เกิดการทาํลายของเนื�อเยื�อแบบ Liquefaction necrosis ซึ�งมีผลทาํให้เนื�อเยื�อเปื� อยเหลว ทาํให้สารด่างสามารถทะลุผา่นและทาํลายเนื�อเยื�อชั �นลึกลงไปก่อให้เกิดการทาํลายเนื�อเยื�อบริเวณใกล้เคียงร่วมด้วย
กลไกในการเกิด extravasation

21
acid & alkaline agents
MEDICATION DILUENT STANDARD DILUTIONS PH MISCELLANEOUS
AMIODARONE D5W [150 mg / 100 ml] [10 min] 4.1Recommended: 1-6 mg/ml(Central line is required for concentrations > 2 mg/ml)
AMPHOTERICIN B D5W [1 mg / 10 ml ] [4 - 6 hours] 5-6Central line: 0.25 mg/ml Peripheral line: 0.1 mg/ml
CIPROFLOXACIN D5W [200 mg / 100 ml] [1 hour] 3.3 - 4.6 Max conc. : 2 mg/ml
CLOXACILLIN
NS (preferred),
D5W
[1000 mg / 100 ml] [1 hour][500 mg / 50 ml] [1 hour]
2.5 -5.5 Max conc. : 10 mg/ml
Acid agents
https://www.pedagogy-inc.com/Home/Resources/IV/Phlebogenic-Medications.aspx

22
acid & alkaline agents
MEDICATION DILUENT STANDARD DILUTIONS PH MISCELLANEOUS
LEVOFLOXACIN NS, D5W- Up to 250 mg/50 ml [60 min]- Up to 500 mg/100 ml [60 min]- Up to 750 mg/150 ml [90 min]
3.8 - 5.8 Max conc. : 5 mg/ml
PENTAMIDINE D5W [350 mg/250 ml] [60 min] 4 - 4.4 Max conc. : 6 mg/ml
VANCOMYCIN NS, D5W
Concentration < 5 mg/mlIV drip > 1 hoursConcentration < 10 mg/mlIV drip > 2 hours
2.5 -4.5 Max conc. : 10 mg/ml
Acid agents
https://www.pedagogy-inc.com/Home/Resources/IV/Phlebogenic-Medications.aspx

23
acid & alkaline agents
MEDICATION DILUENT STANDARD DILUTIONS PH MISCELLANEOUS
ACYCLOVIR NS, D5W[0-350 mg / 50 ml] [1 hour][351-700 mg / 100 ml] [1 hour]
10.5 - 11.6 Max conc. 7 mg/ml
AMPICILLIN/SULBACTAM
NS[0 - 1.5 g / 50 ml] [30 min][Over 1.5 g / 100 ml] [30 min]
8 - 10 Max conc. 30 mg of ampicillin/ml
GANCICLOVIR NS, D5W [5-6 mg/kg / 100 ml] [60 min] 11 Max conc. 10 mg/ml
PHENYTOIN NS
Loading Dose: Not exceed 1-3 mg/kg/min (or 50 mg/min whichever is slower) Infusion: The final conc. of phenytoin sodium in the solution not less than 5 mg/ml
12
- Max conc. 10 mg/ml- Administration should commence immediately after the mixture has been prepared and must be completed within 1-4 hr
SULFAMETHOXAZOLE/TRIMETHOPRIM
D5W
[0-80 mg / 100 ml] [60 min][81-120 mg / 150-250 ml] [90 min][121-240 mg / 250 ml] [90 min][241-450 mg / 500 ml] [90 min]
10Minimum dilution:
80 mg TMP/ 75 ml
Alkaline agents
https://www.pedagogy-inc.com/Home/Resources/IV/Phlebogenic-Medications.aspx

24
acid & alkaline agents
การรกัษาโดยทั �วไป
1) ควรหยดุให้ยาในทนัที 2) ดึงยาออกจากเส้นให้มากที�สดุ 3) ประเมินว่าผูป่้วยมีอาการมากน้อยเพียงใด 4) ประคบอุ่นเพื�อกระจายตวัยาไม่ให้อยู่ที�เดิม เพื�อให้เนื�อเยื�อ
ต่างๆ ช่วยดดูซึมและห้าม neutralization โดยเดด็ขาด เพราะอาจจะทาํให้เกิดผิวหนังแยกชั �นมากขึ�นกว่าเดิม
5) ติดตามการให้ยาทุก 30 นาที

25
Compatibility
Compatible – สารละลายทั �งสองชนิดสามารถเข้ากนัได้Incompatible – สารละลายทั �งสองชนิดไม่สามารถเข้ากนัได้Variable – ความเข้ากนัได้ของสารละลายทั �งสองชนิด
ขึ�นกบัความเข้มข้นของสารละลาย

26

27

28
Compatibility
ผสมใน D5W เท่านั�น ผสมใน NSS เท่านั�นAmphotericin B Phenytoin (Dilantin)
Amphocil (Collodal dispersion) Ampicillin
Ambisome (Liposome) Amoxicillin + Clavulanic (Augmentin)
Filgrastim (Neutromax, Neupogen) **Ampicillin+Salbactam (Unasyn)
**Lenograstim (Granocyte) Ertapenem (Invanz)
Oxaliplatin (Eloxatin) Meropenem (Meronem)
**Sulfamethoxazole/Trimethoprim (bactrim) Doripenem (Doribax)
Norepinephrine (Levophed) Daptomycin (Cubicin)
Amiodarone (Cordarone) Caspofungin (Cancidas)
Desmopressin (DDAVP) (Minirin)

29
Compatibility

Aminoglycoside VS Beta lactam Penicillins
Chemical Incompatibility

จากการศึกษาในหลอดทดลองพบว่า ยาในกลุ่ม aminoglycosides จะมีฤทธิ� ต้านเชื�อ
แบคทีเรียลดลงเมื�อมียาในกลุ่ม -lactams อยู่ด้วย เนื�องจากยามีปฏิกิริยาต่อกนัทาํให้วง
แหวน -lactams แตกออก และเกิดกระบวนการ acylation ของ amino groups ของยากลุ่ม aminoglycosides ทาํให้ยาเสียคณุสมบติัในการฆ่าเชื�อ
ไม่ควรผสมยาทั �ง 2กลุ่มเข้าด้วยกนัก่อนนําไปให้แก่ผูป่้วย
Compatibility
https://www.slideshare.net/AliAlSamawy1/incompatibilities-of-drug-admixtures-64834073

32
ตวัอย่างสารนํ�าและการผสมยาที�สั �งใช้บ่อยในเดก็
Medication Diluent Max conc. Administration
Acyclovir* NS , D5W 7 mg/ml IV infusion over 60 min
Amikacin* NS , D5W 5 mg/ml IV infusion over 30-60 min
Ambisome D5W 2 mg/ml IV infusion over 2 hr
Amphotericin B* D5W0.4 mg/ml (central)
0.1 mg/ml (peripheral)IV infusion over 4 hr
Ampicillin/Sulbactam* NS45 mg/ml (Unasyn)
30 mg/ml (ampicillin)IV infusion over 30 min
Azithromycin* NS , D5W 2 mg/ml IV infusion over 60 min
Caspofungin* NS 0.5 mg/ml IV infusion over 60 min
Cefazolin NS , D5W 20 mg/ml IV infusion over 10-60 min
Cefepime* NS , D5W 40 mg/ml IV infusion over 30 min

33
Medication Diluent Max conc. Administration
Cefoperazone/Sulbactam NS , D5W 25 mg/ml IV infusion over 15-30 min
Cefotaxime* NS , D5W 40 mg/ml IV infusion over 30 min
Cefoxitin* NS , D5W 40 mg/ml IV infusion over 30 min
Ceftriaxone* NS , D5W 40 mg/ml IV infusion over 30-60 min
Cefuroxime* NS , D5W 30 mg/ml IV infusion over 30 min
Cetazidime* NS , D5W 40 mg/ml IV infusion over 30 min
Ciprofloxacin* D5W 2 mg/ml IV infusion over 60 min
Clindamycin NS , D5W 18 mg/ml IV infusion over 30 mg/min
Cloxacillin* NS 10 mg/ml IV infusion over 60 min
Colistin NS , D5W 3 mg/ml IV infusion over 30 min
Co-trimoxazole* D5W 1 mg of TMP/ml IV infusion over 60-90 min
Cyclosporin A NS , D5W 2.5 mg/ml IV infusion over 2-6 hr
ตวัอย่างสารนํ�าและการผสมยาที�สั �งใช้บ่อยในเดก็

34
Medication Diluent Max conc. Administration
Doxycycline* NS , D5W 1 mg/ml IV infusion over 60 min
Ertapenem NS 20 mg/ml IV infusion over 30 min
Fluconazole NS , D5W 2 mg/ml IV infusion over 1-2 hr
Ganciclovir* NS , D5W , LR 10 mg/ml IV infusion over 60 min
Gentamicin NS , D5W 10 mg/ml IV infusion over 30-60 min
Imipenem* NS 5 mg/ml IV infusion over 60 min
Levetiracetam NS , D5W , LR 15 mg/ml IV infusion over 15 min
Levofloxacin* NS , D5W 5 mg/ml IV infusion over 60-90 min
Meropenem* NS 20 mg/ml IV infusion over 60 min
Micafungin NS , D5W 4 mg/ml IV infusion over 60 min
ตวัอย่างสารนํ�าและการผสมยาที�สั �งใช้บ่อยในเดก็

35
Medication Diluent Max conc. Administration
NTG NS , D5W 400 mcg/ml IV continuous drip
Pentamidine* D5W 6 mg/ml IV infusion over 60 min
Phenobarbital NS N/A IV infusion over 30 mg/min
Phenytoin* NS 5-10 mg/ml IV infusion over 50 mg/min
Piperacillin/Tazobactam NS , D5W 80 mg/ml of piperacillin IV infusion over 30 min
Tigecycline NS , D5W , LR 1 mg/ml IV infusion over 30-60 min
Valproic acid NS , D5W 1 mg/ml IV infusion over 20 min
Vancomycin* NS , D5W5 mg/ml
10 mg/ml
IV infusion over 60 min
IV infusion over 120 min
Voriconazole NS , D5W , LR 5 mg/ml IV infusion over 2 hr
ตวัอย่างสารนํ�าและการผสมยาที�สั �งใช้บ่อยในเดก็

36

37
Q & A
Question?

ข้อมลูผูป่้วย ผูป้ว่ยเพศชาย อาย ุ14 ปี นํ�าหนกั 34 kg สว่นสงู 158 cm
CC: ชกัเกรง็กระตุกมากขึ�น 7 hr PTA
HPI: 9 days PTA หลงัจากปรบัยา VPA เป็น TPM มอีาการชกัมาก
ขึ�น เกรง็กระตุกทั �งตวั ตามองเหลอืก ประมาณ 10-20 วนิาท/ีครั �ง มีอาการวนัละ 20-30 ครั �ง/วนั โดยไมไ่ดข้าดยา ไมม่ไีข ้
3 days PTA อาการชกัเป็นมากขึ�น ลกัษณะเดมิ ระยะเวลาพอเดมิ กนิขา้วไดน้้อยลง ปสัสาวะน้อยสเีขม้ขึ�น 7 hr PTA ชกัมากขึ�น ถี�ขึ�น ระหวา่งทางมารพ. มชีกัเกรง็ตาเหลอืกครั �งละ 20 วนิาท ีประมาณ 10-20 ครั �ง
Case Study

ข้อมลูผูป่้วย PMH: ไดร้บัการวนิิจฉยัเป็น epilepsy ตั �งแต่อาย ุ2 ปี เคย on phenytoin
(50) 3x3 ไมไ่ดต้ดิตามการรกัษามา 5 ปี (ซื�อยาจากรา้นยา)10/2/59 มา neuro clinic ตรวจพบ nystagmus
[phenytoin level = 96.27 mcg/ml] เลย off phenytoin 14/2/59 phenytoin level = 58.45 mcg/ml start
topiramate (50) 0.5x2 นาน 1 wk then 1x2
Case Study

การรกัษาในโรงพยาบาล
24/2/59: Admit ที� ER มอีาการชกัเกรง็แขนขา 2 ขา้ง ตาเหลอืกขึ�นบน Diazepam 10 mg IV stat (2 doses) Load phenytoin 600 mg + NSS up to 80 ml IV drip in 10 min stat
(20 mg/kg/dose)• หลงัจากนั �น 1 hr เริ�มมอีาการแดงบรเิวณแขนขา้งที�ใหย้า ปลายมอื
ของผูป้ว่ยเปลี�ยนเป็นสมีว่งคลํ�า บวม
Case Study

41SCOTT KIRSCH, MAX BAYARD, KATIE DARRAJ. Distal Upper Extremity Edema and Discoloration. Am Fam Physician. 2007
Case Study

42
อาการดงักล่าวเรียกว่าอะไร?A. Anaphylaxis reactionB. Purple glove syndromeC. Histamine releasedD. Redman syndrome
Case Study

43SCOTT KIRSCH, MAX BAYARD, KATIE DARRAJ. Distal Upper Extremity Edema and Discoloration. Am Fam Physician. 2007
Phenytoin-induced Purple Glove Syndrome
Case Study

44
MEDICATION DILUENT STANDARD DILUTIONS PH MISCELLANEOUS
PHENYTOIN NS
Loading Dose: Not exceed 1-3 mg/kg/min(or 50 mg/min whichever is slower) Infusion: The final conc. of phenytoin sodium in the solution not less than 5 mg/ml
12
Administration should commence immediately after the mixture has been prepared and must be completed within 1-4 hr
Rate 20 mg/kg/dose/10 min = 2 mg/kg/dose/min x 600 mg/10 min = 60 mg/min
Case Study
Phenytoin 600 mg + NSS up to 80 ml IV drip in 10 min
Concentration Phenytoin 600 mg + NSS up to 80 ml = 7.5 mg/ml