Embed Size (px)
Citation preview

Phage therapy
Mario Vaneechoutte
Novel compounds and strategies to combat pathogenic microorganisms
Brussels, 24 November 2006

Phage therapy: History
Frederick Twort1915
Félix d'Hérelle George Eliava 1917

Phage therapy: history
The first evidence for a viral-like agent with antibacterial properties was reported by M. E. Hankin in 1896.
Found in the Ganges river in India, it was temperature sensitive, capable of passing through a porcelain filter, and could reduce titres of the bacterium Vibrio cholerae in laboratory culture.
Hankin suggested that it might help to decrease the incidence of cholera in people using water from the Ganges.
Adhya S and C. Merril. 2006. The road to phage therapy. Nature 443: 754-755
Phage therapy: history
d’Herelle’s first clinical experiences in 1920’sd'Herelle F. (1917). Sur un microbe invisible antagoniste des bacilles dysentériques.
Acad. Sci. Ser. D 165:373d’Herelle F. (1925) Essai de traitement de la peste bubonique par le bactériophage.
La Presse Med. 33: 1393-94.George Eliava starts the microbiology institute in Tbilisi (1923) and d'Hérelle is invited by Stalin to the Eliava Institute (1936).
Commercialization of phages in France and USA in 1930’sL’Oréal: Bacté-intesti-phage, Bacté-pyo-phage, Bacté-staphylo-phageEli Lilly: Colo-lysate, Entero-lysate, Staphylo-lysate
Phage therapy was abandoned in the West, because oflack of understanding of the high specificity and mode of action of phages
exaggerated claims of effectiveness: urticaria, herpes, eczemathe rise of broad-spectrum antibiotics
but phage therapy research continued in Eastern Europe ...

Was d'Hérelle a renown scientist at his time?In 1925, d'Hérelle received the honorary doctorate of the University of Leiden,
as well as the Leeuwenhoek medal, which is only awarded once every ten years. The latter was especially important to him,
as his idol Louis Pasteur received the same medal in 1895.
The next years, he was nominated eight times for the Nobel prize, though he was never awarded one.
Phage therapy: history
d'Hérelle worked at the Tbilisi Institute and even dedicated one of his books, published in Tbilisi in 1935, to Comrade Stalin.
He had already started to build a cottage on the grounds of the Institute.
But just then, his friend Eliava fell in love with the Georgian woman (or the other way round?) with whom the head of the secret police (BERIA!) also happened to be in love. Eliava's fate was sealed. He was executed and denounced as an enemy of the people. d'Hérelle ran for his life and never returned to Tbilisi.

Phages: sizes and genome sizes
MS2: 3.6 kbpPhiX174: 5.4 kbp Poliovirus: 7.4 kbp
Lambda bacteriophage: 48 kbp
Mycoplasma genitalium: 580 kbp
Largest viral genome: bacteriophage G (Giant), Bacillus megaterium: 670 kbp
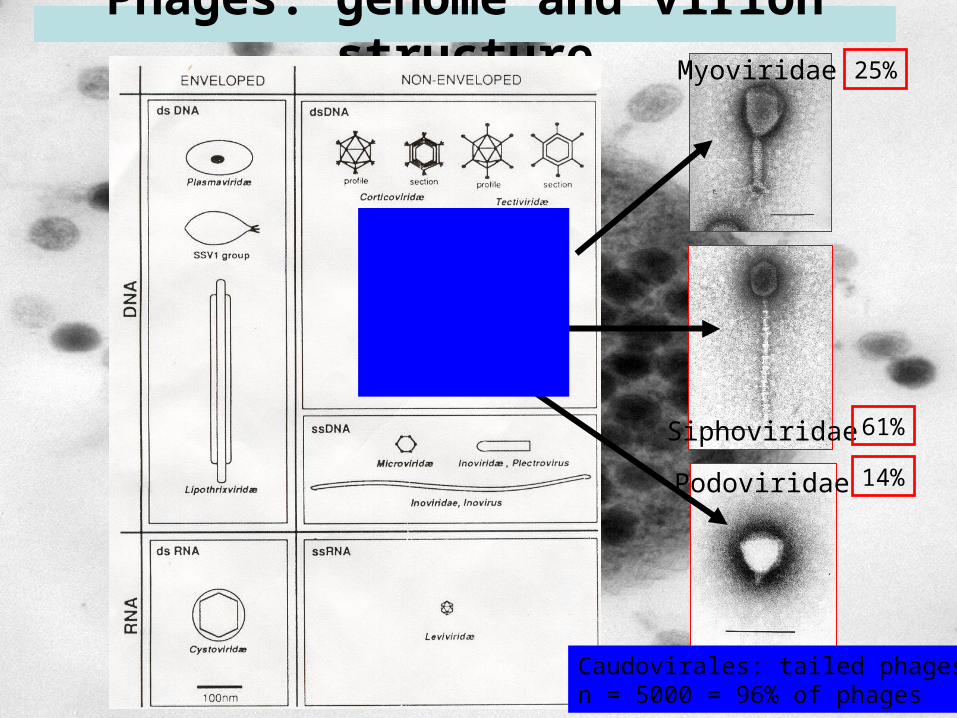
Phages: genome and virion structure
Caudovirales: tailed phagesn = 5000 = 96% of phages
Myoviridae
Siphoviridae
Podoviridae
61%
25%
14%

Phages: Caudovirales: Myoviridae virion structure
Head
Tail
Fibers
Endplate

E. coli phage T4 (Myoviridae)

P. aeruginosa phage PT-1 (Myoviridae)

Phages: Infection by Myoviridae

Phages: Infection by E. coli T4-bacteriophage

Phages: Infection by E. coli T4-bacteriophage

Chronic phages (e.g. E. coli phage M13):after injection phage particles are formed immediately.These leave the host cell without lysis
Lytic phages (e.g. E. coli phage T4):after injection phage particles are formed immediately and thebacterial cell is lysed before duplication: virulent phages
Lysogenic phages (e.g. E. coli phage Lambda): after injection the phage genome is incorporated into the bacterial genome as a prophage and duplicated together with the bacterial genome: lysogenic phase later the prophage can be activated and enter a lytic cycle: lytic phase
temperate phages
Therapeutic phages
Phages: Life cycles. Chronic, lytic, lysogenic

Chronically infecting phages: E. coli M13

Time course of lytic infection cycle

Lytic vs lysogenic phages
Lytic Lysogenic

Lytic phages Lysogenic phagesvirulent temperate
clear plaques opaque plaques all cells lysed not all cells lysed

Titration of lysogenic phage D3112
20 plaques in 100 µlof a 10-10 dilution = 200 x 1010 = 2 x 1012 phages/ml pfu/ml
Phage Dilution 10-6
Dilution 10-9
Dilution 10-8 Dilution 10-10

Phage therapy: opportunitiescurrent problems in infectious diseases
Antibiotic resistance is increasing
Limited number of antibiotics in the pipeline
Chronic recurrent infections are due to biofilm: intrinsic poor efficacy of antibiotics due to altered metabolism:
infection of URT in CF-patients: Pseudomonas aeruginosachronic otitis media: Haemophilus influenzae, Alloiococcus otitidis?recurrent UTI: uropathogenic Escherichia colibacterial vaginosis: Gardnerella vaginalis, Atopobium vaginaeburn wounds: Pseudomonas aeruginosa, Staphylococcus aureusforeign object infections: catheters, valves, ...: Staphylococcus spp.
!!! chronic infection: time to select the best phages.
Phage therapy: advantages
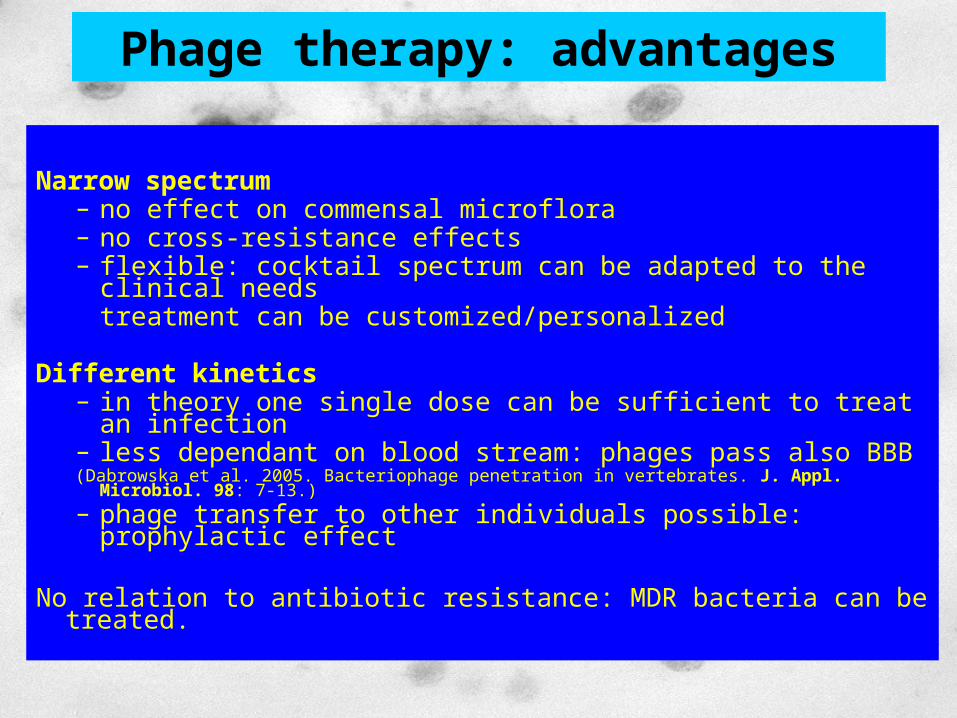
Narrow spectrum– no effect on commensal microflora – no cross-resistance effects– flexible: cocktail spectrum can be adapted to the clinical needs
treatment can be customized/personalized
Different kinetics– in theory one single dose can be sufficient to treat an infection– less dependant on blood stream: phages pass also BBB(Dabrowska et al. 2005. Bacteriophage penetration in vertebrates. J. Appl. Microbiol. 98: 7-13.)
– phage transfer to other individuals possible: prophylactic effect
No relation to antibiotic resistance: MDR bacteria can be treated.

Phage therapy: strategies1. Classic: use of cocktails of lytic virulent phagesMerril et al. 2003. The prospect for bacteriophage therapy in Western medicine. Nature Reviews/Drug Discovery 2: 489-497.
2. Use of phage-derived antibacterial products:T4-lysozyme, lysines, capsule polysaccharide depolymerases, ...Loeffler et al. 2001. (group of Fischetti, also KULeuven: Volckaert, Lavigne)Rapid killing of Streptococcus pneumoniae with a bacteriophage cell wall hydrolase. Science 294: 2170-2172.
Two different lines of reasoning lead to the estimate that 2 billion phage genes are present, i.e. that only 0.0002% of the global phage genome – comprised in 100 million phage species has been sampled.Rohwer, F. 2003. Global phage diversity. Cell 113: 171-182.
3. Genetically manipulated lysogenic phages for in situ gene delivery: --> in situ delivery to bacterial cells of
* killing genes (doc)* antisense RNA to block translation
Westwater et al. 2003. Use of a genetically engineered phage to deliver antimicrobial agents to bacteria: an alternative therapy for treatment of bacterial infections. Antimicrob. Agents Chemother. 47: 1301-1307.
4. Phages as probiotics with immunomodulatory effects?Phages inhibit human T-cell activation and proliferationPhages diminish cellular infiltration into allogeneic skin allografts
Gorski et al. 2006. Bacteriophages and transplantation tolerance. Transplant. Proc. 38: 31-333.

Fishing for phages
Phage therapy: strategiesLytic phages

Phage therapy: StrategySelection of active phages
P. aeruginosa Phages
PT-01 PT-02 PT-04 PT-05 PT-08B025 - - + - -B026 + - + + +B027 + + + + +B028 + - + - +B029 + + + + +B030 + - + - +B031 - - - - -B032 + - + - +B033 + + + + +B034 + + + + +
Valentie 8 4 9 5 8
Phage selection for the composition of a cocktail:
1. Phages PT6, PT8, PNM, 14/1, 9/3, F77 and PL togetherlyse 97% of all P. aeruginosa-isolates.
2. 90% of the isolates are lysed by 2 or more phages

Selection of phages for S. aureus: several phages lyse 95-100% of S. aureus strains
very efficiently, including all MRSA
Phage therapy: StrategySelection of active phages

Phages are safe by definition: viruses which infect bacteria only
1. Bacteriophages infect specifically bacteriasince they need to recognize bacterial cell wall structures: peptidoglycane, LPS.
2. Bacteriophages that were manipulated genetically to infect mammalian cells were not able to multiply inside the mammalian cells after infection. Di Giovine et al. 2001. Binding properties, cell delivery, and gene transfer of adenoviral penton based displaying bacteriophage. Virology 282: 102-112.
3. No bacteriophage genes can be found in the human genome, whereas retro-viruses have left hundreds of genes integrated into the human genome.
In summary, bacteriophages have no tropism towards mammalian cells and cannot multiply in them.
Phages: safety. Theoretical considerations 1

Phages: safety. Theoretical considerations 2
Bacteriophages are numerous and ubiquitous:
NumerousEstimate of total number of tailed phage particles on Earth: 4-6 x 1031 = 10-fold of number of prokaryotes. Bergh. 1989. Nature 340: 467-468 Whitamn et al. 1998. PNAS 95: 6578-6583
Ubiquitous Up to log9 phages per ml of surface waters In animal sera, in vaccines, in food E. coli phages in 11% of faeces of healthy persons B. fragilis phages in 68% of faeces of healthy persons
"We live in a sea of phages" still no infections with phages have been reported

Phage therapy: safety. Lytic vs lysogenicUse of lytic (= virulent) phages and not lysogenic ( = temperate) phages:
1. Lysogenic phages can carry virulence factors
Prophage DNA accounts for half of the 1.3 Mb of additional DNA found in the food pathogen E. coli O157, but absent in the reference strain K12.
Ohnishi et al. 2001. Diversification of Escherichia coli genomes: are bacteriophages the major contributors?Trends Microbiol. 10:481-485.
Hendrix et al. 1999. Evolutionary relationships among diverse bacteriophages
and prophages: all the world's a phage. PNAS 96: 2192-2197.

Phage therapy: safety. Lytic vs lysogenicUse of lytic phages and not lysogenic phages:2. Lysogenic are responsible for lateral gene transfer (specialized transduction
Lytic phages: generalized transduction Lysogenic phages: specialized transduction

1. Bacteriophages and bacteria occur and interact in a multitude of natural environments,including our body (even at the highest concentrations), whereby gene exchange is often a natural and unavoidable phenomenon.
2. Problem of increased lateral gene transfer due to antibiotics has been overlooked?:Treatment with aminoglycoside and quinolone antibiotics induces hyper-transformability of Streptococcus pneumoniae, leading to increased uptake of foreign DNA by the bacterial cells which might include incorporation of virulence and antibiotic resistance genes:
Prudhomme et al. 2006. Antibiotic stress induces genetic transformability in the human pathogen Streptococcus pneumoniae. Science 313: 89-92.
Summary:Mass antibiotic treatment of the past decades may have caused gene exchange (transformation, transconjugation) at much higher rates than will be possibly caused by the use of lytic bacteriophages (transduction).
Use of lytic phages and not lysogenic phages:2. Lysogenic are responsible for lateral gene transfer (specialized transduction)
Phage therapy: safety. Lytic vs lysogenic
Phage therapy: (safety). Lytic vs lysogenic
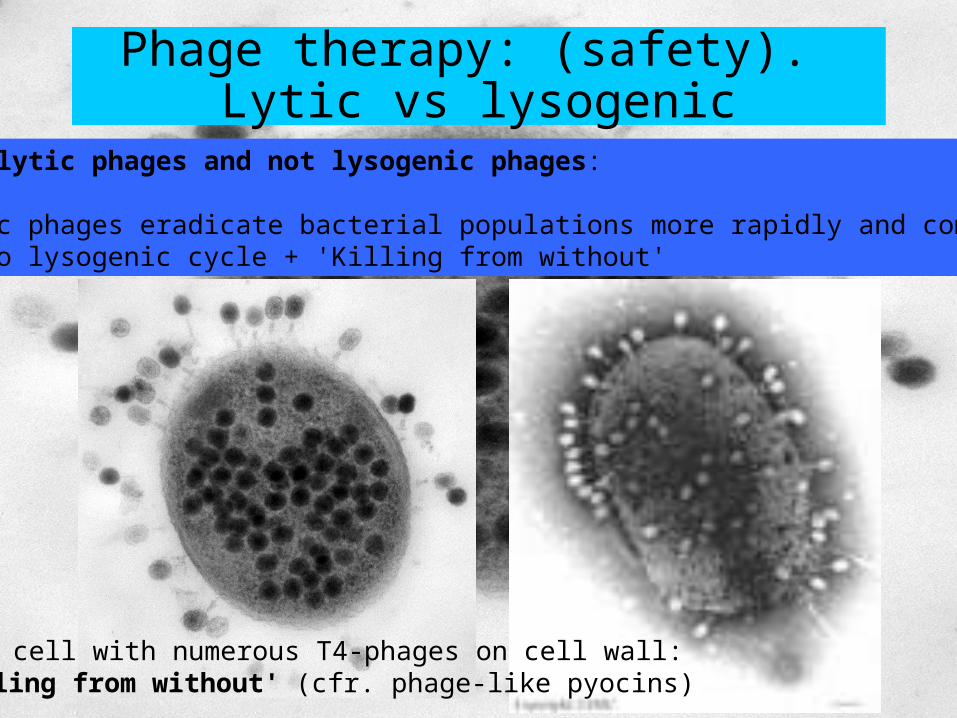
Use of lytic phages and not lysogenic phages:
3. Lytic phages eradicate bacterial populations more rapidly and completely:No lysogenic cycle + 'Killing from without'
E. coli cell with numerous T4-phages on cell wall:'Killing from without' (cfr. phage-like pyocins)
Numerous animal experiments (see efficacy), without adverse effects.
Merril et al. (1996) and Capparelli et al. (2005)selected bacteriophages for persistence in the mouse circulatory system, indicating that their persistent systemic presence does not pose a problem to mammals.
Merril et al. 1996. Long-circulating bacteriophage as antibacterial agents. Proc Natl Acad Sci USA 93: 3188-3192. Capparelli et al. 2005. Selection of an Escherichia coli O157:H7 bacteriophage for persistence in the circulatory system of mice infected experimentally. Clin. Microbiol. Infection 12: 248-253.
Phage therapy: safety in practiceAnimal studies

During the long history of using bacteriophages as therapeutic agents bacteriophages have been administered to thousands of humans
(i) orally, in tablet or liquid formulations (log5 to log11 bacteriophages/dose), (ii) rectally, (iii) locally: skin, eye, ear, nasal mucosa, burn wounds, rinses and creams (iv) as aerosols or intrapleural injections, and (v) intravenously, albeit to a lesser extent than the first four methods.
Sulakvelidze et al. 2001. Bacteriophage therapy. Antimicrob. Agents Chemother. 45: 649-659.
Only one group, from the Hirszfeld Insitute, Wroclaw, Poland, renown for its clinical application of bacteriophagesreported a few minor side effects (e.g. nausea, fever). Weber-Dabrowska et al., 2000. Bacteriophage therapy of bacterial infections: an update of our institute’s experience. Arch. Immunol. Therap. Experiment. 48: 547-551.
These effects may have been due to the liberation of endotoxins from lysed bacteria, a phenomenon that can also be observed when antibiotics are usedand therefore cannot be considered as specifically bacteriophage related.
Phage therapy: safety in practiceHuman studies 1

"Vaccination" study in Tbilisi, Georgia (1965)
30.769 children aging 6 months to 7 years old.
17.044 children ingested bacteriophages against Shigella dysenteriae.13.725 children, living at the opposite side of the streets, served as a control group.
Babalova et al. 1968. Preventive value of dried dysentery bacteriophage. Zh. Mikrobiol. Epidemiol. Immunobiol. 2: 143-145.
Phage therapy: safety in practiceHuman studies 2

Log 5 E. coli T4-bacteriophages/ml raw preparations (incl. 2 µg endotoxin/ml)were administered in drinking water to 15 healthy adult volunteers.
One day after a single dose exposure, bacteriophages could be recovered in the faeces of the volunteers.
No adverse effects were observed and no IgA, IgM or IgG antibodies against T4-bacteriophage were detected one month after administration.
Bruttin, A., and H. Brussow. 2005. Human volunteers receiving Escherichia coli phage T4 orally: a safety test of phage therapy. Antimicrob. Agents Chemother. 49: 2874-2878.
Phage therapy: safety in practiceHuman studies 3

E. coli bacteriophage phiX174 is IV injected since decades to test the influence on the immune response of different medicines.
E.g. IV injection of log9 phiX174 bacteriophages/kg body weight, twice, in 18 patients with chronic renal failure.Bearden et al. 2005. Rituximab inhibits the in vivo primary and secondary antibody response to a neoantigen, bacteriophage phiX174. Am. J. Transplant. 5: 50-57.
This research group uses this approach since the early 70s without reporting any adverse effects.
Ochs et al. 1971. Immunologic responses to bacteriophage phiX174 in immunodeficiency diseases. J. Clin. Investigation 50: 2550-2558.
Wedgwood et al. 1975. The recognition and classification of immunodeficiency diseases with bacteriophage phiChi 174. Birth Defects Orig. Artic. Ser. 11: 331-338.
Phage therapy: safety in practiceHuman studies 4

Phage therapy: efficacy, animal studies 1
Biswas et al. 2002. Bacteriophage therapy rescues mice bacteremic from a clinical isolate of vancomycin-resistant Enterococcus faecium.Infect Immun 70: 204-210.
Cheng et al. 2005. Removal of group B streptococci colonizing the vagina and oropharynx of mice with a bacteriophage lytic enzyme. Antimicrob. Agents Chemother. 49: 111-117.
Wagenaar et al. 2005. Phage therapy reduces Campylobacter jejuni colonization in broiler chickens. Vet. Microbiol. 19: 275-283.

Institute for Animal Disease Research in Houghton, Cambridgeshire, UK
Diarrhoea causing E. coli in mice, calves, lambs and piglets, Treatment with bacteriophages
reduces the number of bacteria from log7 to log2 in 2 hours, andstops the associated fluid loss.
--> survival of all treated animals, compared to the placebo group
Smith WH and Huggins MB. 1983. Effectiveness of phages in treating experimental Escherichia coli diarrhoea in calves, piglets and lambs. J. Gen. Microbiol. 129: 2659-2675.
Smith, et al. 1987. The control of experimental Escherichia coli diarrhoea in calves by means of bacteriophages. J. Gen. Microbiol. 133: 1111-1126.
Phage therapy: efficacy, animal studies 2

Intramuscular injection (single) in one leg with bacteriophage MW to treat intramuscular E. coli infection in the other leg in mice.
is more effective than multiple IM administration of antibiotics
Smith WH and Huggins MB. 1982. Succesful treatment of experimental Escherichia coli infections in mice using phage: its general superiority over antibiotics. J. Gen. Microbiol. 128: 307-318.
Phage therapy: efficacy, animal studies 3

14 guinea pigs with excised burn wounds to which 6 x log5 cfu/ml of P. aeruginosa and 1.2 x log7 BS24 bacteriophages
were applied simultaneously (MOI = 10) and upon which the excised tissue was replaced:
1 of 7 bacteriophage treated grafts was rejected, whereas
7 of 7 of non bacteriophage treated grafts failed.
Soothill, J.S. 1994. Bacteriophage prevents destruction of skin grafts by Pseudomonas aeruginosa. Burns 20: 209-211.
Phage therapy: efficacy, animal studies 4
Series of 5 mice intraperitoneally infected with 5 times the LD50 dosis of A. baumannii (log8 cfu/ml), or of P. aeruginosa (log8 cfu/ml), or of S. aureus (log10 cfu/ml)
Treatment with different doses of bacteriophages. log8 pfu of bacteriophage BS46 for A. baumannii : 4/5 mice survivedlog7 pfu of bacteriophage BS24 for P. aeruginosa : 4/5 mice survivedlower doses or no bacteriophage: 0/5 mice survived
The S. aureus bacteriophage had no effect.The A. baumannii phage titer had increased 100-fold.
Soothill JS. 1992. Treatment of experimental infections of mice with bacteriophages. J. Med. Microbiol. 37: 258-261.
Phage therapy: efficacy, animal studies 5

"Vaccination" study in Tbilisi, Georgia (1965)
30.769 children aging 6 months to 7 years old
17.044 children ingested bacteriophages against Shigella dysenteriae 13.725 children, living at the opposite side of the streets, served as a control group.
[Dysentery incidence in control group is 2.6 fold higher than phage treated group]
Babalova et al. 1968. Preventive value of dried dysentery bacteriophage. Zh. Mikrobiol. Epidemiol. Immunobiol. 2: 143-145.
Phage therapy efficacy: applications in humans 1

Weber-Dabrowska et al., 2000. Bacteriophage therapy of bacterial infections: an update of our institute’s experience. Arch. Immunol. Therap. Experiment. 48: 547-551.
Phage therapy efficacy: applications in humans 2

Belgium, two case reports (end of last century)
1. Young female with post-measles subacute sclerosing panencephalitis (SSPE)One year long relapsing infections and debilitating fevers up to 41°C. Numerous antibiotics administered. Cultures of S. aureus and E. faecalis sent to Tbilisi, Georgia.Bacteriophage cocktail against both species was administered intravenously. One week later: free of fever. No further relapse.
2. Female with chronic pansinusitisNo cure after several operations and antibiotic treatmentsUniversity ENT-professor imported the bacteriophages from Georgia.Local application into the sinus cavities.No cure.
Phage therapy efficacy: applications in humans 3

Phage therapy: Problem 1Narrow spectrum
Advantage: commensal microflora not affectedDisadvantage: species and clone need to be identified before application.
Solutions:1. Use of phage mixtures (cocktails)2. Application in chronic infections: time to select appropriate phages3. Broad spectrum phages (e.g. all S. aureus) exist. (4. Add phages to antibiotics)

Phage therapy: Problem 2Bacterial resistence
Mutant bacteria can become susceptible for other phages.
Mutant bacteria can loose virulence.E. coli K1-phages induce phage-resistant E. coli but these are K1 negative: reduced virulence (Smith & Huggins 1982).
Phages can co-evolve (they do since 4 billion years).
Phages can be propagated in vivo to adapt to resistant hosts.
New phages can be found: fishing for phages.
Most important strategies of bacteria for developing phage resistance:
1. Mutation of cell wall receptors which are used by phages as adherence ligand2. DNA restriction/modification systems: nonmodified (phage) DNA is restricted.
Hanlon et al. 2001. Reduction in exopolysaccharide viscosity as an aid to bacteriophage penetration through Pseudomonas aeruginosa biofilms. Appl. Environ. Microbiol. 67: 2746-2753.
Sillankorva et al. 2004. Pseudomonas fluorescens infection by bacteriophage PhiS1: the influence of temperature, host growth phase and media. FEMS Microbiol. Lett. 241: 13-20.
85% biomass reduction in planktonic as well as biofilm growth.
Hughes et al. 1998. Biofilm susceptibility to bacteriophage attack: the role of phage-borne polysaccharide depolymerase. Microbiology 144: 3039-3047.
Phage therapy: Problem 3 Can phages penetrate biofilms?

Phage therapy: Problem 3 Can phages penetrate biofilms?

Current phage research Belgium
1. Laboratorium voor Gentechnologie, KULeuven. Guido Volckaert, Rob LavigneConstruction of phage and fasmidevectors for E. coli and P. aeruginosaSequence analysis of P. aeruginosa phagesRecombinant expression of phage genes in E. coli:
lysozymes, holines, polymerases, capside proteins
2. Laboratorium Microbiologie, KULeuven. Jozef AnnéLegionella phages
3. SCMBB, ULB, Ariane Toussaint: Aclame Database: A CLAssification of genetic Mobile Elements
4. Laboratory Food Microbiology and Food Preservation, UGent. Frank DevlieghereListeria phages for food decontamination

Phages are everywhere:The world is a phage. We live in a sea of phages.
Different strategies are possible: lytic phageslytic phage productsmodified lysogenic phages for gene deliveryphages as probiotics?
Phages are safe
Phages are efficient, also against antibiotic resistant bacteria and against bacteria in biofilm
Several Belgian laboratories are already involved in phage research
Clinical trials are held back because of 'safety' considerations and lack of appropriate regulatory framework
Phage therapy: Summary

Phage therapy: lack of regulatory framework make the final step
towards application too steep(See Poster: Verbeken et al.)

Crossing the RubiconBelgian burn wound trial to be expected soon???
[email protected] Bacteriologie, UZ Gent
In collaboration withMaia Merabishvili, Nino Chanishvili, Marina Tediashvili
George Eliava Institute, Tbilisi, Georgia
Victor Krylov, State Institute Genetics, Moscow, Russia
Jean-Paul Pirnay, Daniël De Vos, Gilbert Verbeken, Kenneth CoenyeQueen Astrid Military Hospital, Nederoverheembeek, Belgium
Thierry De Baere, Leen Van Simaey, Catharine De GanckGhent University Hospital, Belgium
Slides downloadable athttp://users.ugent.be/~mvaneech/LBR.htm

Declaration of Helsinkihttp://www.wma.net/e/policy/b3.htm
In the treatment of a patient, where proven prophylactic, diagnostic and therapeutic methods do not exist or have been ineffective, the physician, with informed consent from the patient, must be free to use unproven or new prophylactic, diagnostic and therapeutic measures, if in the physician's judgement it offers hope of saving life, re-establishing health or alleviating suffering.
Where possible, these measures should be made the object of research, designed to evaluate their safety and efficacy. In all cases, new information should be recorded and, where appropriate, published.
The other relevant guidelines of this Declaration should be followed.

Can bacteriophages be used against intracellular bacteria?
A Survey of the Bacteriophage WO in the Endosymbiotic Bacteria Wolbachia.Gavotte L, Henri H, Stouthamer R, Charif D, Charlat S, Bouletreau M, Vavre F. Mol Biol Evol. 2006 Nov 9; [Epub ahead of print]
The particular lifestyle of obligatory intracellular bacteria usually protects them from phage infection. However, Wolbachia, an intracellular alpha-proteobacterium, infecting diverse arthropod and nematode species and best known for the reproductive alterations it induces, harbours a phage named WO, which has recently been proven to be lytic.
Broxmeyer et al. 2002. J. Infect. Dis. 186:1155-1160.Killing of Mycobacterium avium and Mycobacterium tuberculosis by a mycobacteriophage delivered by a nonvirulent mycobacterium: a model for phage therapy of intracellular bacterial pathogens.























![Lamda phage[1]](https://img.pdfslide.net/doc/110x75/58cedaba1a28abd4098b6283/lamda-phage1.jpg)



