Embed Size (px)
Citation preview
| 1
Phase I in clinical drug development
Philippe Grosjean Sanofi R&DClinical Sciences and Operations
M2 Pharmacocinétique31 janvier 2013

| 2
New drug investigations in human
● Objectives of the clinical investigations of drugs or devices in human ● Therapeutic (efficacy and adverse events)● Pharmacodynamic (including the mechanism of action)● Pharmacokinetics (ADME)

| 3
The Drug Development Process
LIFE
PREPA- RATION
and
SUBMISSION
of a
NEW DRUG
APPLICATION
DOSSIER
MARKETING CLINICAL EVALUATION IN MAN
PHASE I PHASE II PHASE III
Tolerance and
pharmaco-kinetics
Biological activity and
research of a therapeutic
effect
Determination of the optimal
dose
Confirmation of the
therapeutic effect and tolerance
1
RESEARCH DEVELOPMENT BIRTH2 years 1 to 2 years 1 year Contin. 6 to 8 years
LCM
LIFE
CYCLE
MANAGEMENT
30 3 10 50,000 to 500,000 molecules
RESEARCH INTO
CHEMICAL STARTING
POINTS
OPTIMIZATION PRECLINICAL EVALUATION
IN VITRO AND IN ANIMAL
• Conception • Target selection • Test Development • Synthesis
SCREENING (+ High Throughput
Screening) Active Molecules (lead compounds)
• Intrinsic activity • Selectivity • Oral absorption • Duration of action • Efficacy in relevant animal models
1 to 2 years P
R
O
D
U
C
T
I
O
N
• Chemical Development • General Pharmacology • Analytical Methods • Stability • Safety • Toxicity • Metabolism and Pharmacokinetics • Formulation
P H A R M A C O V I G I L A N C E
| 4
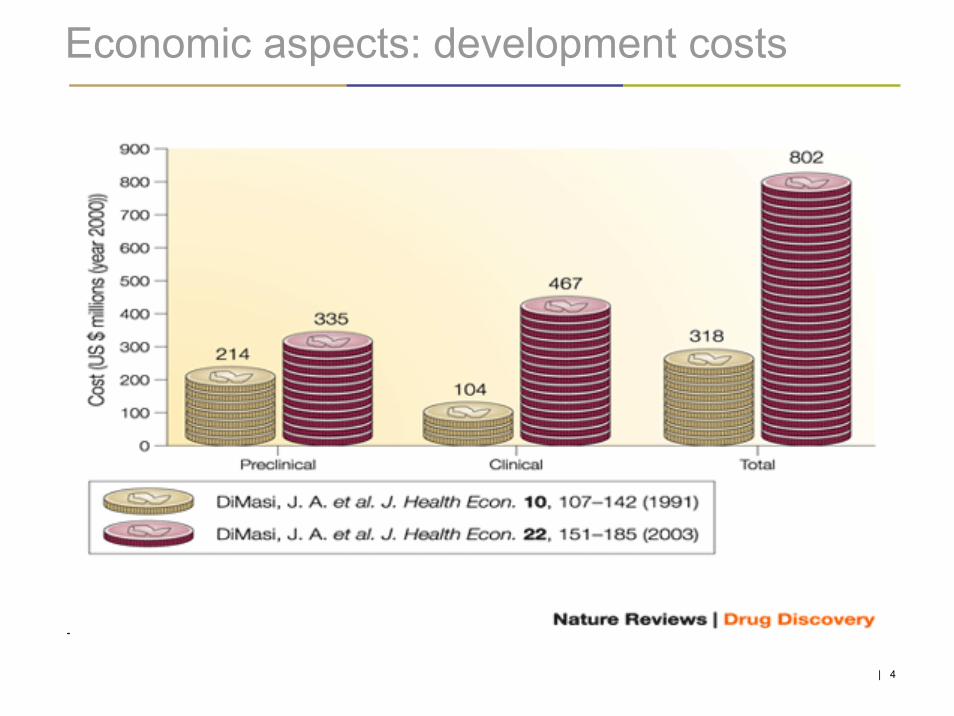
Economic aspects: development costs

| 5
Reason for development discontinuation
| 6
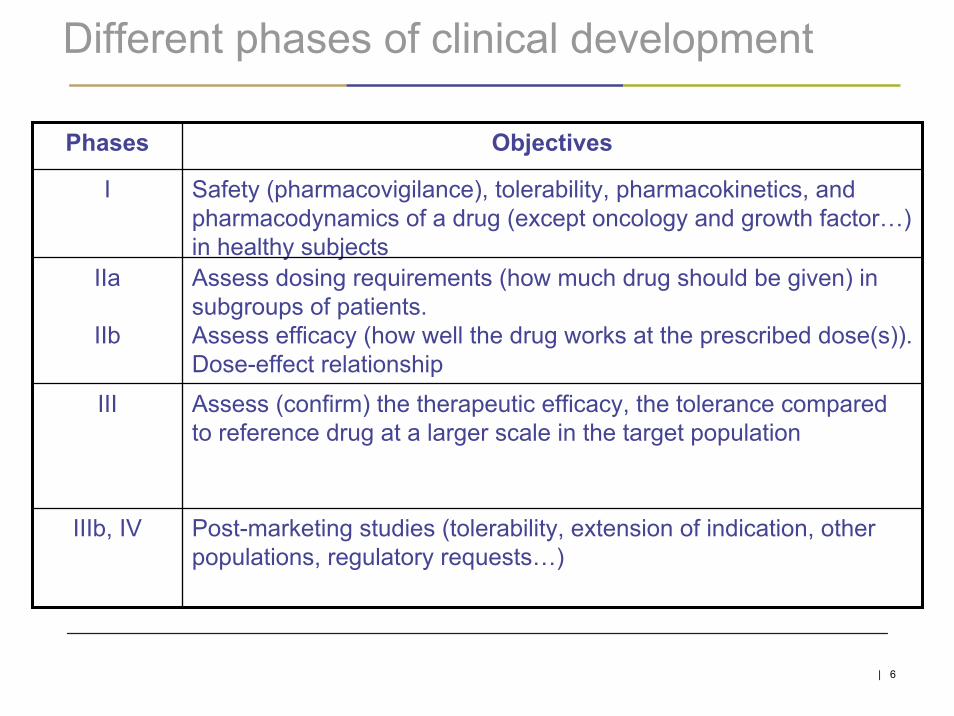
Different phases of clinical development
Post-marketing studies (tolerability, extension of indication, otherpopulations, regulatory requests…)
IIIb, IV
Assess (confirm) the therapeutic efficacy, the tolerance comparedto reference drug at a larger scale in the target population
III
Assess dosing requirements (how much drug should be given) in subgroups of patients. Assess efficacy (how well the drug works at the prescribed dose(s)). Dose-effect relationship
IIa
IIb
Safety (pharmacovigilance), tolerability, pharmacokinetics, and pharmacodynamics of a drug (except oncology and growth factor…) in healthy subjects
I
ObjectivesPhases
| 7
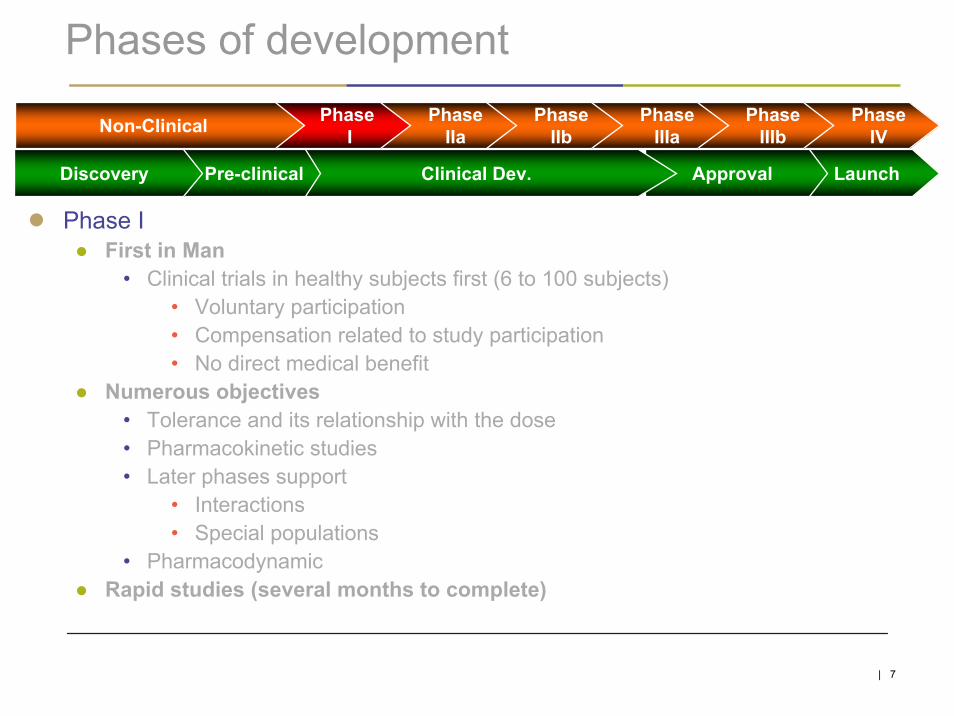
Phases of development
● Phase I● First in Man
• Clinical trials in healthy subjects first (6 to 100 subjects)• Voluntary participation• Compensation related to study participation• No direct medical benefit
● Numerous objectives• Tolerance and its relationship with the dose• Pharmacokinetic studies• Later phases support
• Interactions • Special populations
• Pharmacodynamic● Rapid studies (several months to complete)
PhaseIV
PhaseIIIb
PhaseIIIa
PhaseIIb
PhaseIIa
PhaseINon-Clinical
LaunchApprovalClinical Dev.Pre-clinicalDiscovery
| 8
Clinical development plan
● Summarizes the rationale, the objectives, the strategy of investigational product development● Study needs● Study links – relationship - chronology● Go/no go criteria
● Plan discussed with the Health Authorities at the beginningof development● Regular meetings during the course of development● At specific times (e.g. end of phase II…)● Specific guidelines (ICH, FDA, EMA…)

| 9
Schematic presentation of a clinical plan
FIM RD
InteractionPK 1
MetabolismNew
formulation
Foodeffect
Efficacy 1
Dose findingendpoint y
. . .
Efficacy 2
Tox 1 Tox 3 Tox 6
Dose findingendpoint x
InteractionPK 2
Registrationsupport
Carcinogenicity
PDyn
Y1 Y2 Y3

| 10
Regulatory environment (1/2)● Strict international regulatory environment
● Declaration of Helsinki and its revisions (1964)● ICH recommendations● Good Clinical Practices
● Country-dependent regulations (e. g. Ethics committees, IRB…) ● USA : Code of Federal Regulation of the FDA (Food and Drug
Administration) ● Europe : European directive (2001, France 2004)● France : Loi « Huriet » (modifiée à la suite de la Directive Européenne sur
les Essais cliniques) : autorisation des lieux de recherches, consentement, Comités de Protection des Personnes, fichier national des volontaires sains...
• La loi distingue deux grandes catégories de recherches biomédicales • Celles dont on attend un bénéfice individuel direct et immédiat, pour la
personne (malade) qui s’y prête ou une partie des personnes concernées.
• Celles dénommées sans bénéfice individuel direct où aucune des personnes ne peut tirer un bénéfice personnel et immédiat pour sa santé

| 11
● The clinical development is conditioned by a scientific and technicaldossier including animal experimental data within a precise regulatory and legal framework
● Before FIM: toxicology pre-requisites, characterization of the compound (part of the investigator’s brochure…)
● Trials conduct: protection of the subjets, choice of clinical centers, methodology (statistics, reference, placebo, design…)
● Number of trials and number of subjects needed
● Information presented in a standard dossier (CTA clinical trial application / investigational medicinal product dossier EUR in force in France sinceAugust 2006) or IND investigational new drug (US)
Regulatory environment (2/2)

| 12
Toxicology pre-requisites : phases I, II (Europe)
Study Type Parameters assessed
Pharmacology Vital functions (respiratory system, cardiovascular system, CNS…)
Toxicokinetic and pharmacokinétic
Absorption,distribution, metabolism, excretion
Acute and chronic toxicity 2 species (rodent, non-rodent)
Genotoxicity Mutations, chromosomal aberrations
Reproduction Male fertility (not required for healthy male subjects inclusion), female fertility, embryogenesis, post and peri-natal abnormalities
Local tolerance If needed (eg : topic, IV…)

| 13
Toxicology pre-requisites: phases I ,II (US, EU)
Planned duration of clinical trial Minimum duration of toxicity studiesRodent Non-rodent
Single doseUp to 2 weeksUp to 1 monthUp to 3 monthsMore than 3 months
2-4 weeks 2 weeks2-4 weeks 2 weeks3 months 3 months6 months 3 months6 months chronic
| 14
Choice of dose in First-in-Man
● FDA approach● Maximum recommended starting dose (MRSD)
• Example
● Allometric scaling● Predicted human clearance
• Example
● MABEL● Pharmacology rather than toxicology
| 15
Take into account animal toxicity findings
● Monitorability animal findings● Laboratory● ECG● Exploratory parameters● Histopathology
● Severity of findings
● Reversibility
● Type of findings● Body systems● Death
● Differences between species / gender
● Knowledge of the therapeutic class
● Definition of the No Observable Adverse Effect Level (NOAEL)
| 16
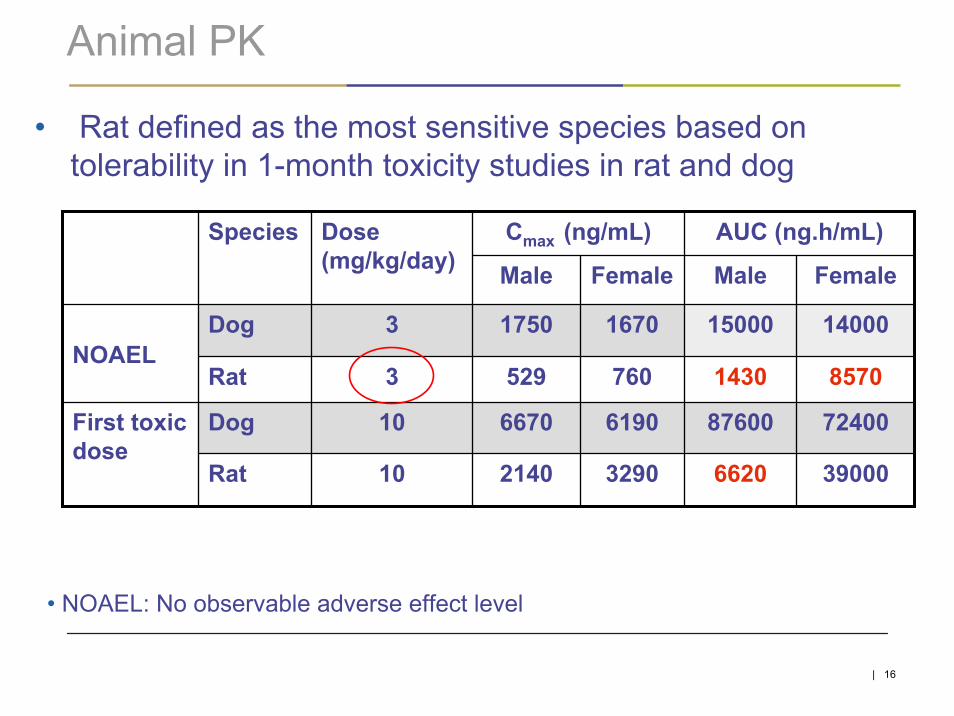
Animal PK
• Rat defined as the most sensitive species based on tolerability in 1-month toxicity studies in rat and dog
• NOAEL: No observable adverse effect level
Cmax (ng/mL) AUC (ng.h/mL)
Male Female Male Female
Dog 10 6670 6190 87600 72400
Rat 10 2140 3290 6620 39000
First toxic dose
Dog 3 1750 1670 15000 14000
760 8570Rat 3 529 1430NOAEL
Species Dose (mg/kg/day)

| 17
First dose proposal for FIMToxicology data: FDA approach
● Maximum Recommended Starting Dose (MRSD)● Human Equivalent Dose: HED= NOAEL x BSA-CF
• NOAELRAT and DOG: 3 mg/kg/day (or most sensitive species)• BSA-CF: body surface area converting factor: 0.162 for rat, 0.541 for dog
• HEDdog = 1.62 mg/kg• HEDrat = 0.49 mg/kg = lowest HED
● MRSD (mg) = HEDrat x HBW x SF-1 Safety factor (SF)• SF = 10 (default)• HBW: human body weight = 60 kg (default)
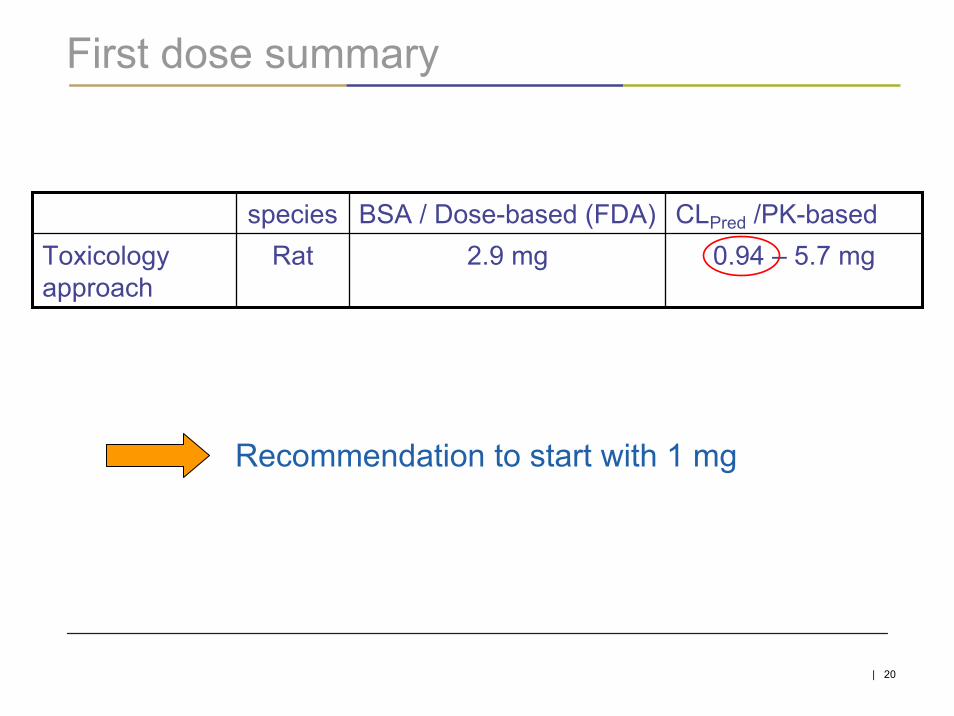
MRSD is (3 x 0.162 x 60)/10 = 2.9 mg

| 18
Prediction of Human ClearanceAllometric Scaling (Mahmood and Balian Method)
• Predicted CLhuman = 6.6 L/h
• Exponent of simple allometric equation (b=0.515) not included in 0.55 to 0.70 (no other correction needed e.g. brain weight…)
Simple allometric approach could lead to underestimation
Cl = a*(W)b
Rat
Rabbit Dog
Human Clpred

| 19
First dose proposal for FIMToxicology data: allometric approach
● PK based approach● FIM Dose (mg) = Clhuman x AUC NOAELrat / F x SF
● Clhuman , lowest predicted clearance, 6.6 L/h● AUCNOAEL, male rat, 1.43 mg.h/L● AUCNOAEL, female rat, 8.57 mg.h/L● Safety factor (SF) = 10 (default)● Bioavailability F = 1 (default)
Proposed First-in-man dose : (6.6 x 1.43) / (1 x 10) = 0.94 mg
based on male rat (based on female rat = 5.7 mg)
| 20
First dose summary
Recommendation to start with 1 mg
species BSA / Dose-based (FDA) CLPred /PK-basedToxicology approach
Rat 2.9 mg 0.94 – 5.7 mg

| 21
Considerations of the choice of the top dose
● Dose range should not significantly exceed the exposure at FTD in F rat (6.6 mg.h/mL)
● Dose/BSA approach● Human Equivalent Dose (mg) = FTD (mg/kg) x BSA-CF ● In rat, FTD is 10 mg/kg, HED = 10 x 0.162 = 1.62 mg/kg
• total dose = 97.2 mg (hbw 60 kg)● In dog, FTD is 10 mg/kg, HED = 10 x 0.541 = 5.41 mg/kg
• total dose = 324.6 mg (hbw 60 kg)
HED: lowest corresponding HED is 97.2 mg

| 22
Considerations of the choice of the top dose● PK-based approach
● Human Equivalent Dose(mg) = Clhuman (L/h) x AUCFirst toxic dose(mg.h/L)● Clhuman, lowest predicted clearance = 6.6 L/h● AUCFirst toxic dose
• In male rat, FTD is 10 mg/kg, corresponding AUC is 6.6 mg.h/L• 6.6 x 6.6L/h = 43.6 mg
• In female rat, FTD is 10 mg/kg, corresponding AUC is 39 mg.h/L• 39 x 6.6 = 257.4 mg
• In dog, FTD is 10 mg/kg, corresponding AUC is 72.4 mg.h/L• 72.4 x 6.6L/h = 477.8 mg
HED: lowest corresponding HED is 43.6 mg
Top dose capped by exposure < 6.6 mg.h/mLConsider Cmax when intravenous route

| 23
Dose proposal for FIMFirst and top doses proposal
BSA / Dose-based CLPred /PK-based Proposal
Starting Dose
Top Dose
2.9 mg 0.94 mg 1 mg
97.2 mg 80 mg43.6 mg
Human equivalent dose
Top dose 80 mg if exposure < 6.6 mg.h/mL

| 24
Dose proposal for FIM: doses range proposalDose Dose (mg)
Escalation rateratio
1 -
2.5
2
2
2
2
2
2.5
5
10
20
40
80 *
HED
1 Starting dose NOAEL/10 Male (M) rat (3 mg/kg) (PredCL)
6 < FTD M rat (10 mg/kg) (PredCL)
2
3
4 ≈ NOAEL M rat (3 mg/kg) (PredCL)
5 < FTD/2 M rat (10 mg/kg) (PredCL)
7 Top dose If AUC<FTD M rat (10mg/kg/day) and < NOAEL Female (F) rat (3mg/kg/day)
* 80 mg or earlier with exposure <6.6 mg.h/mL
| 25
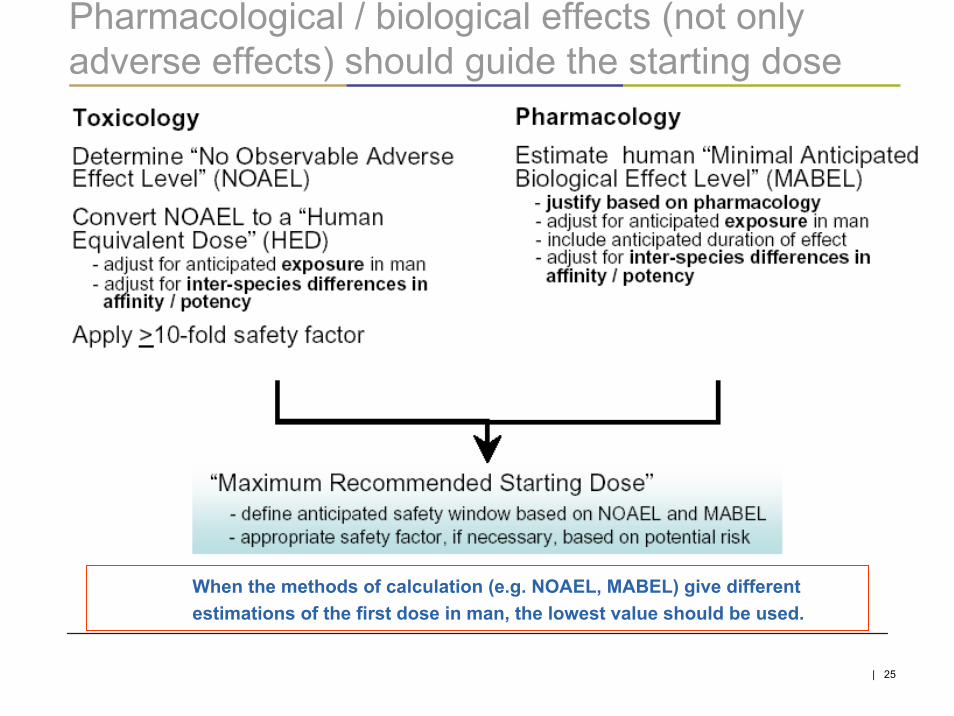
Pharmacological / biological effects (not only adverse effects) should guide the starting dose
When the methods of calculation (e.g. NOAEL, MABEL) give different estimations of the first dose in man, the lowest value should be used.

| 26
The main challenge… selection of a pertinent biological parameter for calculating the MABEL
● Preclinical efficacy or activity parameter in vivo● Lowest dose showing a significant shift in efficacy or activity● Then calculate the HED
● Receptor binding on human cells● Concentration - percent occupancy
• For agonists, choose the concentration with low percent occupancy (10%)
• For antagonists, higher percent occupancy may be reasonable● Use animal PK data to project concentrations in humans
● In vitro human cell responses● Concentration – response● Use animal PK data to project concentrations in humans
● … apply a safety factor (currently not specified)
| 27
Methodology of clinical trials
● Placebo● Neutral substance that substitutes a drug in order to control or
suscitate the psychologic effects linked to drug intake● Essential for the use of blinding procedures● Allows to answer the question, is the new treatment efficacious?
● Blinding● Indicate that the nature of treatment is not known● Allows to reduce the bias in clinical trials, in particular to
evidence the placebo effect● Single blind: only the subjects ignore the treatment received● Double-blind: both the subjects and the investigator(s) ignore
the treatment received… and actually the sponsor as well

| 28
W5W4W3
R
RED
n=4
n=4
R
ED decision of dose escalation based on tolerability profile of dose n-1 and PK dose n-2
Randomization
R
R
ED
Dose 2
+ PK Dose 1
R
R
Dose 3
+ PK Dose 2
R
R
ED
Dose 4
+ PK Dose 3
R
R
ED
Dose 5
+ PK Dose 4
R
R
ED
Dose 6
+ PK Dose 5
R
R
Dose 7 optional
Dose 1 (8 subjects : 6V + 2 P)
D1 D2dosing
dosing
D7
Week1 W2 W6 W7 Follow-upW8
ScreeningW-3
ED
Parallel groups

| 29
●Pros● Simple protocol● Limits the study duration for a subject● No carry-over effect, no period effect
●Cons● Increases the number of subjects● No assessments of the intra-individual variability
Parallel groups

| 30
Product B
Product A
Wash out
Cross-over
Sequences
A-B
B-A
SequencesA-E-D-CB-A-E-DC-B-A-ED-C-B-AE-D-C-B
Period 1 Period 2
Period 1 Period 2 Period 3 Period 4
ABCDE
Incomplete sequences
Sequence BA 1-sequence

| 31
●Pros ● Decreases the number of subjects● Assess the intra-individual variability
●Cons● Increases the duration of study (per subject)● Period effect● Carry-over effect
Cross-over

| 32
First in Man – Single dose● Objectives
● Assess the tolerability and safety after single dose● Define a maximum tolerated dose (MTD) or maximum adminsitered
dose (MAD)● Define the PK profile
● Design● Double-blind, placebo controlled, parallel groups● single dose● 8 subjects per group (dose) with 2 placebo and 6 verum● Usually, 5 to 7 ascending doses tested
● Assessments● Adverse events, clinical laboratory, ECG, vital signs, other safety
parameters, PD, biomarkers● PK

| 33
First in Man – Repeated dose
● Objectives● Assess the tolerability and safety after repeated doses● Define a MTD or MAD● Define the PK profile
• Rac● Design
● Double-blind, placebo controlled, parallel groups● 7 to 14 days of administration (QD, or BID)● 12 subjects per group (dose) with 3 placebo and 9 verum● Usually, 2 to 4 ascending doses tested
● Assessments● Adverse events, clinical laboratory, ECG, vital signs, other
safety parameters, PD, biomarkers● PK

| 34
Other phase I studies with safety/PD objective(s)
● DALA (Drug of abuse liability assessment)● Part of the Registration Dossier for CNS acting drugs (primary or
secondary effects)• Based on behavioral effects in animals• Dependence, overdose, and drug abuse liability potential
● TQT (Thorough QT study )● Assess effect of the investigational product on cardiac
repolarization● Pharmacodynamic
● Mechanism of action, biomarker● Safety parameters● Challenge tests● Other
● Other, product-dependent

| 35
PK studies● Numerous studies with a PK objective can be conducted during an investigational product
(IP) development● They occur at different stages of the drug development
● Type of studies include● Drug-drug interactions
• Based on in vitro metabolic profile (CYP, transporters…), physico-chemical properties• IP on other drugs’ PK profile• Other drugs on the IP’s PK profile• Food (includes alcohol, fruit juices, high-fat meals, high-carbohydrate meals…)
● Metabolism● Bioavailability
• Bioequivalence• Absolute• Relative
• Formulation comparisons● Specific populations
• Hepatic impairment• Renal impairment• Elderly• Children
| 36
PK to support development (1/5)● Excretion balance and metabolism study
● Further development of drugs requires greater knowledge of the metabolism and excretion in human.
• To determine the excretion balance and systemic exposure of radioactivity after oral administration of [14C]-drug;
• To determine the PK of the drug and its contribution to overall exposure of radioactivity;
• To determine the metabolic pathways of the drug and identify the chemical structures of the main metabolites
● Based upon the results, PK studies in patients with renal and/or hepatic impairments will be performed subsequently
● Identification of major metabolites● N = 4 to 6● Collection of blood, urine, feces, expired 14CO2● Usually long collections periods >8 days (t1/2z)

| 37
PK to support development (2/5)● Interaction with CYP3A4 substrate (midazolam)
● Effect of the IP on a drug’s PK which is a substrate of CYP3A4● Depends on in vitro in human liver microsomes investigations● Midazolam is exclusively metabolized by CYP3A4/3A5; after oral
administration, its clearance reflects combined intestinal and hepatic CYP3A activity.
● The aim of this study is to assess the effect of a repeated administration of the IP on the pharmacokinetic profile of a single dose of midazolam, in healthy male and female subjects
● Classification of CYP3A inhibitors• a single oral dose of midazolam allows discrimination between strong (≥ 5-
fold increase in midazolam plasma AUC values), moderate (2 to 5-fold increase) and weak inhibitors (1.25 to 2-fold increase)
● Cross-over● N = 12

| 38
PK to support development (3/5)● Interaction with CYP3A inhibitor (ketoconazole)
● Effect of a potent CYP3A inhibitor on the PK of the IP● Based on invitro studies that showed that the IP is metabolized
by cytochrome P450 3A (CYP3A) isoenzyme● Ketoconazole is a well-known potent CYP3A4 inhibitor
• Widely used as a reference inhibitor to test in vivo the potential effect of CYP3A inhibition on drugs being a substrate for thisenzyme
● The aim of this study is to assess the effect of a repeatedketoconazole administration on the pharmacokinetic profile of a single oral dose of the IP, in healthy male subjects
• Cross-over• N = 12
| 39
PK to support development (4/5)● Cocktail interaction study
● When preclinical data suggest that an IP could have an impact on several subtypes of the cytochrome P450, potential drug-drug interactions, using a CYP probe cocktail (1A2, 2C9, 2C19, 2D6 and 3A4) can be investigated
• Probes showed identical PK when administered separately or when combined together (cocktail)
• Bioequivalence (cocktail versus each probe drug alone) was demonstrated for both Cmax and AUClast
• Combined administration of the five probes proved to be well tolerated● Global approach enables the testing of several hypotheses in the same study, in a
limited number of healthy subjects● Assess the effect of the IP on the pharmacokinetics of each cocktail probe
• CYP2C9, 2C19 and 2D6 poor metabolizers (PM) will be excluded from this study• 2C9 : warfarin: 10 mg single dose• 1A2 : caffeine: 100 mg single dose• 2C19 : omeprazole: 20 mg single-dose• 2D6 : metoprolol: 100 mg single dose• 3A4 : midazolam: 0.03 mg/kg single dose, leading to a 2 mg dose in this study
population● Cross-over● N = 20

| 40
PK to support development (5/5)● Interaction with food – case study
● Safety Results: IP at 200 mg single dose was well tolerated in healthy subjects whatever the condition of administration (fasted or fed[standardized high-fat breakfast])
● As compared to fasted administration, after a single oral dose of 200 mg administered following a high-fat food intake, Cmax and AUC strongly increase by 73.8-fold and 41.5-fold, respectively.

| 41
Transition to phase II● Early phase I studies provided
● Safety and tolerability data• Wide dose range (SD, RD)
● Pharmacokinetic data• Drug-drug interactions (assess most co-prescribed drugs)• Special populations
● Pharmacodynamic data● Bridging studies
• Match safety/PD in target population● Based on these data
● Phase II doses are selected• Safety ratio• Activity or efficacy / exposure ratio
● Treatment duration is defined according to the disease● Phase I continues to support registration
Early Phase I data

| 42
Merci de votre attention !









![Drug Development - clinical trials phase I: 25-45 healthy volunteers [safety evaluation] phase II: 20-150 diseased individuals [safety and efficacy] phase](https://img.pdfslide.net/doc/110x75/56649e9d5503460f94b9d8af/drug-development-clinical-trials-phase-i-25-45-healthy-volunteers-safety.jpg)



















