Embed Size (px)
Citation preview

PERIPARTUM CARDIOMYOPATHY
CA N D I CE S I LV E RS I D ES , M D
M I LES N A DA L CH A I R I N P R EG N A N CY A N D HEA RT
D I S EA S E
U N I V E RS I T Y OF TORON TO P REGNA NC Y A ND H EA RT
D I S EA S E P ROG RA M

Case
• 40-year-old G3P1 at 36 weeks gestation
• African American
• No medical history
• Sister with “heart problems” after a pregnancy who was told never to get pregnant
• Gestational diabetes

Case
• Presented with shortness of breath
• On exam: BP 120/85 mmHg, HR 120-130 bpm, clinical heart failure
• Echo: Moderate to severe LV systolic dysfunction

Case
Is this PPCM?
1. Yes
2. No
3. Maybe

Case
Is this PPCM?
1. Yes
2. No
3. Maybe

OBJECTIVES
Overview of PPCM
Clinical presentation
Treatment options
Prognosis

OBJECTIVES
Overview of PPCM
Clinical presentation
Treatment options
Prognosis

DEFINITION OF PPCM
Davis and Elkayam JACC 2020

DIFFERENTIAL DIAGNOSIS
Blauwet and Cooper heart 2011

INCIDENCE OF PPCM
Blauwet and Cooper Heart 2011
1 in 100 in Nigeria1 in 1,000-4,000 in US1 in 200,000 in Japan

OVERVIEW
Davis and Elkayam JACC 2020

Blauwet and Cooper Heart 2011

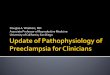
VASCULOTOXIC HYPOTHESIS

Vasculotoxic hormones are released from the placenta and pituitary during late gestation and early postpartum periods
Damage the Cardiac Microvasculature
Cardiomyocyte Dysfunction
Contractile Failure
• One of these potentially toxic hormones is prolactin
• Prolactin can be cleaved by extracellular proteases to yield a 16-kDa peptide that is profoundly vasculotoxic

PATHOGENESIS
Arany and Elkayam Circ 2016

VASCULOTOXIC HYPOTHESIS
Arany and Elkayam Circ 2016
Cleaved 16-kDa prolactin molecule triggers endothelial and cardiomyocyte damage
Soluble Fms-like tyrosine kinase 1 (sFlt1) inhibits the VGEF pathway and triggering PPCM

GENETICS: TTN GENE
Ware et al NEJM
• 172 women with PPCM underwent targeted sequencing of DCM genes
• 15% prevalence of high impact variants
• Majority of variants were in the TTN gene, a critical structural component of sarcomeres in cardiac and skeletal muscle

OBJECTIVES
Overview of PPCM
Clinical presentation
Treatment options
Prognosis

CLINICAL PRESENTATION
Asymptomatic
Pulmonary edema
Cardiogenic shock
Cardiac arrest
Thromboembolic complications
Death

CLINICAL PRESENTATION
Asymptomatic
Pulmonary edema
Cardiogenic shock
Cardiac arrest
Thromboembolic complications
• LV thrombus on echo reported in 10-17% of pregnancies
Death

Elkayam JACC 2011
TIMING OF PRESENTATION

Bauersach et al EJHF 2019

Outcomes of Women with PPCM in the US
Author (year) NMean Follow up Period
Mortality Heart Transplant
Witlin 1997 28 FU not reported 18% 11%
Felker 2000 42 FU 8.6 years 7% 7%
Chapa 2005 32 FU not reported 9.6% 6.5%
Amos 2006 55 43 +/- 43 months 0 10%
Mielniczuk 2006 16,296 FU No reported In hospital 2.5 % NA
Brar 2007 60 4.7 years 3.2% NA
Goland 2009 182 19 months 7% 6%
Modi 2009 40 54 months 15.9% 0
Elkayam JACC 2011

Prospective cohort study of 100 women with PPCM followed for 1 year
4 deaths over the course of a year
6 women had died, undergone transplant or were on an LVAD
6 had severe (LVEF < 35%) chronic cardiomyopathy

Timing of Mortality After Diagnosis in PPCM
Elkayam JACC 2011

OBJECTIVES
Overview of PPCM
Clinical presentation
Treatment options
Prognosis

Case
• PPCM, heart failure and moderate to severe LV systolic dysfunction
• Which medications would you consider for therapy in this patient?
1. Lasix
2. ACEI
3. Beta-blocker
4. Brompcriptine

Case
• Started on Lasix
• Oxygen 2L by nasal prongs

Bauersach et al EJHF 2019

Regitz-Zagrosek et al EHJ 2018
It is recommended to treat women with HF during pregnancy according to current guidelines for non-pregnant patients, respecting contraindications for some drugs in pregnancy
I B

Medications
Heart Failure Medications Potential Adverse Effects
Βeta-blockers IUGR; fetal bradycardia and hypoglycemia
Lasix Caution for hypovolemia or hypotension that may lead to decreased placental perfusion
Hydralazine + Nitrates Caution with hypotension
Digoxin No associated congenital defects
ACEI or ARB Anuria, oligohydramnios, fetal limb contractures, craniofacial deformation, pulmonary atresia, fetal hypocalvaria, intra uterine growth restriction, prematurity, patent ductus arteriosus, stillbirth, neonatal hypotension and death
Sacubitril-valsartan Same as ACE-I/ARB
Spironolactone Spironolactone has been associated with antiadrenergic activity, feminization of male rat fetuses and permanent changes in reproductive tract in both sexes
Ivabradine Scant data in humans, animal data suggest risk
Modified from Davis and Elkayam JACC 2020

PEACE REGISTRY(PEripArtum Cardiomyopathy in NigEria)

PPCM PROFILES IN DIFFERENT STUDIES

Koczo et al JACC 2019

Koczo et al JACC 2019
Stop BreastfeedingBromocriptine

Bromocriptine
Proof of concept; 10 women in each arm Sliwa et al Circ 2010
8 weeks bromocriptine
treatment

Bromocriptine
• 96 women in Burkina Faso
• Women were on HF therapy with ACEI/Lasix
• Randomized to 4 weeks of bromocriptine
• LVEF higher in women receiving bromocriptine at 2 weeks, 3/6/12 months
• Mortality lower in women receiving bromocriptine (17% vs 29%, p=0.0001)
Yameogo et al J Cardiol Clin Res 2017

Bromocriptine
• Multicentre trial of 63 women with PPCM + LVEF ≤ 35% + standard heart failure therapy: • Short-term (1week: bromocriptine 2.5mg) • Long-term (8 week: 5 mg for 2 weeks followed by 2.5mg for 6weeks)
• Bromocriptine started 1.6 +/- 1.6 months after delivery
• Left ventricular ejection fraction • 1 week: 28% to 49% - ΔLVEF 21% • 8 weeks: 27% to 51% - ΔLVEF 24% Delta-LVEF: P = 0.381
Hilfiker-Kleiner et al EHJ 2017

Bromocriptine
Hilfiker-Kleiner et al EHJ 2017
Full-recovery (LVEF ≥ 50%) was present in 52% of the 1W- and in 68% of the 8W-group

Bromocriptine
Hilfiker-Kleiner et al EHJ 2017
• No differences in secondary end points between groups • 3/62 had thromboembolic complications (2 venous embolism,1 peripheral
artery embolus) – all women had prophylactic anticoagulation

Regitz-Zagrosek et al EHJ 2018
In patients with PPCM, bromocriptine treatment may be considered to stop lactation and enhance recovery
IIb B

Regitz-Zagrosek et al EHJ 2018
Bromocriptine treatment should be accompanied by prophylactic (or therapeutic) anticoagulation
IIa C

PREGNANCY MANAGEMENT
Davis and Elkayam JACC 2020

DELIVERY
Davis and Elkayam JACC 2020

Case
• Presented at 36 weeks gestation with PPCM and moderate to severe LV systolic dysfunction
• What is your recommendation for the mode of delivery?
1. Vaginal delivery
2. Cesarean delivery

Case
• Presented at 36 weeks gestation with PPCM and moderate to severe LV systolic dysfunction
• What is your recommendation for the mode of delivery?
1. Vaginal delivery
2. Cesarean delivery

Regitz-Zagrosek et al EHJ 2018
Vaginal delivery is recommended as the first choice in most patients
I C
Cesarean delivery should be considered for obstetrical indications or for patients with ….. severe heart failure
IIa C

Case
• Induced at 37 weeks
• Arterial line
• Epidural
• Assisted vaginal delivery
• Oxytocin

Case
• Is it safe to breastfeed?
1. Yes
2. No
3. Unknown

Case
• Is it safe to breastfeed?
1. Yes
2. No
3. Unknown

Regitz-Zagrosek et al EHJ 2018
Due to the high metabolic demands of lactation and breastfeeding, preventing lactation may be considered in patients with severe heart failure
IIb B
In patients with PPCM, bromocriptine treatment may be considered to stop lactation and enhance recover
IIb B



Breastfeeding
Decisions on whether to inhibit lactation and terminate breastfeeding should be decided jointly with the patient on a case-by-case basis factoring in the health of the mother and the benefit of breastfeeding for the infant

Case
• Any other postpartum recommendations?

Regitz-Zagrosek et al EHJ 2018
It is recommended to treat women with HF during pregnancy according to current guidelines for non-pregnant patients, respecting contraindications for some drugs in pregnancy
I B

Medications during Breastfeeding
Heart Failure Medications
Lactation
Βeta-blockers Yes
Lasix Yes, but over-diuresis can lead to decreased milk production.
Hydralazine + Nitrates Yes, but ACE-I/ARB typically chosen post-partum
Digoxin Yes
ACEI or ARB Enalapril and captopril can be used
Spironolactone Spironolactone can be used
Sacubitril-valsartan No information in human, present in rat milk
Ivabradine No information in human, present in rat milk
Modified from Davis and Elkayam JACC 2020

ANTICOAGULATION
• Therapeutic anticoagulation is recommended in women with intracardiac thrombus or atrial fibrillation
• ESC Guidelines on the Management of Cardiovascular Disease in Pregnancy do not provide recommendations about prophylactic anticoagulation
• ESC Position Statement on PPCM recommended prophylactic anticoagulation because of the high rate of peripheral arterial and venous embolism Bauersachs et al EHJ 2019
Regitz-Zagrosek et al EHJ 2018

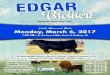
www.researchgate.net/figure/The-wearable-cardioverter-defibrillator
• 12 women with PPCM• 7 with an LVEF < 35% agreed to a use a
wearable cardioverter defibrillator (WCD)
• 2 women refused• During a medial of 81 days, there were
episodes of 4 ventricular fibrillation with appropriate and successful WCD shock in 3 women
• No deaths in the women not using a WCD
Duncker et al Eur J Heart Fail 2014

• Retrospective study in 107 women with PPC and a wearable cardioverter/defibrillator (WCD)
• Average follow up 4 months
•No shocks were delivered
•No deaths when using the WCD; 3 deaths after it was removed
Saltzberg et al J Card Fail 2012

POSTPARTUM CONSIDERATIONS
Davis and Elkayam JACC 2020

Objectives
Overview of PPCM
Clinical presentation
Treatment options
Prognosis

RECOVERY OF LEFT VENTRICULAR SYSTOLIC FUNCTION
Elkayam JACC 2011

LVEF AT PRESENTATION
AND LATE OUTCOMES
McNamara et at (IPAC) JACC 2015

OUTCOMES ACCORDING
TO LV SIZE AND
FUNCTION
•No subjects with both a baseline LVEF <30% and an LVEDD ≥6.0 cm recovered by 1 year postpartum
• 91% of subjects with a baseline LVEF ≥30% and an LVEDD <6.0 cm recovered by 1 year postpartum
McNamara et at (IPAC) JACC 2015

Poor PrognosisLower LVEF
Dilated LV
LV thrombus
Obesity
African American race
Concomitant pre-eclampsia
Biomarkers: NTBNP, troponin, sFlt1
Delayed diagnosis

Case
• PPCM and moderate to severe LV systolic dysfunction
• How long does she need to stay on her heart failure medications?
1. Indefinite
2. 1 year
3. 3 years
4. Until the LV systolic function recovers
5. Depends

Case
• PPCM and moderate to severe LV systolic dysfunction
• How long does she need to stay on her heart failure medications?
1. Indefinite
2. 1 year
3. 3 years
4. Until the LV systolic function recovers
5. Depends

Withdrawal of Medication
Women should remain on combined drug therapy for heart failure until they experience complete myocardial recovery and for at least 12–24 months after full recovery of LV function
Bauersachs et al EHJ 2019

Withdrawal of Medication
For women with full recovery of LVEF:
•Some experts recommend that all women with PPCM remain on long-term therapy
•Some experts recommend gradual withdrawn under careful surveillance with serial cardiac imaging and biomarker measurement
•A discussion between patient, family and clinicians is necessary where the pros and cons of stopping or continuing therapy are carefully considered

Case
• Full recovery of LV systolic function
• Can she have another pregnancy?
1. Yes
2. No
3. Maybe

Case
• Full recovery of LV systolic function
• Can she have another pregnancy?
1. Yes
2. No
3. Maybe

Maternal Complications with Subsequent Pregnancies
HF >20% drop Persistent Mortality
LVEF Dysfunction
Elkayam et al NEJM 2011
Red = LV recoveryGreen = persistent LV dysfunction

Regitz-Zagrosek et al EHJ 2018
In patients with PPCM and DCM, counselling for recurrence risk during subsequent pregnancy is recommended in all cases, even after recovery of LV function
I C
In patients with PPCM, subsequent pregnancy is not recommended if LVEF does not normalize.
III C

SUMMARY: DEFINITION
Davis and Elkayam JACC 2020

SUMMARY: MANAGEMENT
Davis and Elkayam JACC 2020

SUMMARY: POSTPARTUM
Davis and Elkayam JACC 2020

SUMMARY: LONGTERM OUTCOMES
Davis and Elkayam JACC 2020

Thank you