Embed Size (px)
Citation preview

Philippine College of Chest Physician (PCCP): Consensus Statement on the Performance
and Reporting of Spirometry Testing Executive Summary

i
Report of the Council on Diagnostics and Therapeutics Philippine College of Chest Physicians
Primary Investigator: Tim S. Trinidad, MD, FPCCP Secondary Investigators: Ma. Janeth T. Samson, MD, FPCCP
Celeste Mae L. Campomanes, MD, FPCCP
Marites A. Tan- Ang, MD,FPCCP
Geraldine C. Garcia, MD, FPCCP
Maria Peachy Lara L. Villanueva,MD,FPCCP
Lolita Brigida V. Micu, MD, FPCP
Rachel M. Lee-Chua,MD, FPCP
Maria Piedad R. Natividad, MD, FPCCP
PROPONENTS: Chair: Ma. Janeth T. Samson, MD, FPCCP Advisers: Camilo C. Roa, MD,FPCCP
Tomas M. Realiza, MD, FPCCP
Vincent M. Balanag Jr.,MD, FPCCP
Benilda B. Galvez, MD, FPCCP
Jennifer Ann M. Wi, MD, FPCCP
Ricardo C. Zotomayor, MD, FPCCP
Consultative Groups: All hospitals and individuals who have participated in the meetings and voting forms and have commented in one way or another. Chinese General Hospital: Eden D. Chua, MD, FPCCP Shirley Jane Chua-Panganiban, MD, FPCCP Lung Center of the Philippines: Luisito F. Idolor, MD, FPCCP Augusto S. Sablan, Jr. MD, FPCP Araceli Pascual, RT Manila Doctors Hospital: Dennis C. Teo, MD, FPCCP Aileen M. David-Wang, MD, FPCCP Philippine Heart Center: Rodolfo E. Tamse, MD, FPCCP Irenee Faustina J. Casiño, MD, FPCP

ii
St. Luke’s Medical Center: Myrna N. Bañares,MD, FPCCP Raphael Ryan R. Zantua, MD, FPCCP Ma. Janeth T. Samson, MD, FPCCP University of Perpetual Help Medical Center: Ricardo M. Salonga, MD, FPCCP Jose Edzel V. Tamayo, MD, FPCCP Mary Leslee Tabi,RT Niño Jessielito N. Doydora, MD University of the Philippines – Philippine General Hospital: Ma. Bella R. Siasoco, MD, FPCCP Jubert P. Benedicto, MD, FPCCP University of Sto. Tomas Hospital: Tim S.Trinidad, MD, FPCCP Celeste Mae L. Campomanes, MD, FPCCP Apolonio G. Javier, JR., MD, FPCCP Veterans Memorial Medical Center: Eloisa S. De Guia, MD, FPCCP PCCP- Central and North Luzon Chapter: Ruel G. Rivera, MD, FPCCP PCCP-Cebu Chapter: Evan N. Mendoza,MD, FPCCP PCCP-Iloilo Chapter: Malbar G. Ferrer, MD, FPCCP PCCP-Negros Chapter: Ethel Marie B. Tangarorang-Lacson, MD, FPCCP PCCP – Northern Mindanao Chapter: Eileen G. Aniceto, MD, FPCCP PCCP-Southern Mindanao Chapter: Romulo T. Uy, MD, FPCCP PCCP- Southern Tagalog Chapter: Violeta C. Reyes, MD, FPCCP Key Opinion Leaders
Camilo C. Roa, MD,FPCCP Joven Q. Tanchuco, MD, FPCCP Abundio A. Balgos, MD, FPCCP Jennifer Ann M. Wi, MD, FPCCP Ricardo C. Zotomayor, MD, FPCCP
Council of Diagnostics and Therapeutics Members
Caburnay, Eloise Arabelle, MD, FPCCP
Campomanes, Celeste Mae L.,MD, FPCCP
Chavez, Christine L., MD, FPCP
Chua-Panganiban, Shirley Jane, MD, FPCCP
Claveria, Angelica, MD, FPCCP
Cristobal- Aquino, Ma. Flordeliza, MD, FPCCP
FPCP

iii
Dalupang, Julius, MD, FPCCP
Divinagracia, Charissa, MD, FPCCP
Elisterio, Helarose M., MD, FPCCP
Garcia, Geraldine, MD, FPCCP
Germar, Arnold G., MD, FPCCP
Gonzales, Andrew S.A., MD, FPCCP
Lee-Chua, Rachel, MD, FPCP
Llanes-Gracia, Liza, MD, FPCCP
Mapanao, Daisy, MD, FPCCP
Micu, Lolita Brigida, MD,FPCP
Mora, Czarina J., MD, FPCCP
Natividad, Ma. Piedad R., MD, FPCCP
Ogbac, William George, MD,FPCP
Peñafiel, Alvin, MD, FPCCP
Reside, Evelyn Victoria E., MD, FPCCP
Reyes, Mary Jane, MD, FPCCP
Santos, Alfredo Romeo Q., MD, FPCCP
Tan, Marites, MD, FPCCP
Tan, Florita, MD, FPCCP
Samson, Lyndon H., MD, FPCCP
Trinidad, Tim S., MD, FPCCP
Valenzuela, Rosauro Vicente H. Jr.,MD, FPCCP
Villanueva, Anna Tessa, MD. FPCCP
Villanueva, Ma. Peachy Lara, MD, FPCCP
Villasanta, Edwin I.,MD,FPCCP
Zantua, Raphael Ryan R., MD, FPCCP

iv
Message from the PCCP President
Greetings from the Philippine College of Chest Physicians (PCCP) !
Spirometry is a useful tool in the assessment of lung function. National and international guidelines like the Global Initiative for Chronic Obstructive Lung Disease guidelines, recommend spirometry as the gold standard for accurate measurement of lung function.
Spirometry has many clinical applications in assessing and managing respiratory disease such as: detecting the presence of obstructive and restrictive lung defects, determining the severity of lung disease, evaluation of patients with unexplained respiratory symptoms, assessment of preoperative pulmonary risk, disability testing, and screening people at risk in certain occupational environments. However, despite the known usefulness of spirometry, it has remained underutilized in clinical practice. No uniform way of reporting the interpretation of spirometry results is also available in our country.
This spirometry manual was prepared by the PCCP Council on Diagnostics and Therapeutics with the aim of providing standards on the performance and reporting/interpretation of spirometry testing. It is meant to be a working reference for chest specialists, internists, general practitioners, primary care physicians, medical trainees and paramedical personnel.
On behalf of the PCCP Executive Board of Directors, I commend the Council on Diagnostics and Therapeutics under the leadership of Dr. Ma. Janeth T. Samson, for their hard work and dedication in preparing this manual.
I hope that all users of this manual will benefit greatly from it and promote the use of spirometry more extensively. BENILDA B. GALVEZ, MD, FPCCP President (2012-2013) Philippines College of Chest Physicians

v
Message from the Council Chair
Greetings! The Council of Diagnostics and Therapeutics of the Philippine College of Chest Physicians aims to promote awareness of the use of spirometry in the diagnosis of pulmonary diseases as well as to measure lung wellness. The under utilization of this diagnostic tool may be because of its unavailability in the rural areas as well as the lack of understanding of the spirometry report among non-pulmonologist. This lack of understanding may stem from differences in the interpretation of the values in the report or in the manner of reporting these interpretations. It is our objective that by promoting uniformity in the conduct and reporting of simple spirometry we will be able to create more understanding of the report eventually increasing its use to improve the quality of patient care.
This project would not have been possible if not for the cooperation and support of executive board, resource persons from training institutions, chapters and key opinion leaders. Likewise, special thanks to the members of the council who painstakingly contributed their efforts and support , spearheaded by Dr. Tim Trinidad, in making this manuscript a reality.
Ma. Janeth T. Samson, MD, FPCCP Council Chair
PCCP Council of Diagnostics and Therapeutics

vi
Table of Contents
Introduction -------------------------------------------------------------------------------- 1
Methodology ------------------------------------------------------------------------------- 1
Statements
Performance of the Test ------------------------------------------------------------- 2
Quality Control ------------------------------------------------------------------------- 3
Parameters Measured --------------------------------------------------------------- 3
Test Result Selection ---------------------------------------------------------------- 3
Parts of the Report ------------------------------------------------------------------- 3
General Data -------------------------------------------------------------------------- 4
Technician’s Comment -------------------------------------------------------------- 4
Semantics in Interpretation --------------------------------------------------------- 5
Interpretation Algorithm -------------------------------------------------------------- 5
Use of other Parameters Not in Algorithm -------------------------------------- 5
Grading of Severity ------------------------------------------------------------------- 7
Lower Limit of Normality ------------------------------------------------------------ 7
Response to Bronchodilator -------------------------------------------------------- 8
Statement on Need for Additional Test ------------------------------------------ 9
Reference Equations ----------------------------------------------------------------- 9
Comments on the Quality of the Test -------------------------------------------- 10
Graphical Representation ----------------------------------------------------------- 11
Results in Tabular Graph ------------------------------------------------------------ 11
Interpreter’s Comments -------------------------------------------------------------- 12
Final Interpretation -------------------------------------------------------------------- 13
References ---------------------------------------------------------------------------------- 13
Appendix ------------------------------------------------------------------------------------- 14

1
Philippine College of Chest Physician (PCCP): Consensus Statement on the Performance and
Reporting of Spirometry Testing Introduction
Spirometry testing is an underutilized ancillary procedure. There are numerous reasons for this observation. Perhaps one of the reasons is the non-uniformity and complexity of the reports generated. It is for reason the Philippine College of Chest Physician (PCCP) Council of Diagnostics and Therapeutics (DATS) came out with this consensus document. It is envisioned that with these recommendations, PCCP Pulmonary Fellowship Training Institutions (PFTI) will be able to come up with a recommended generic spirometry report that is of good quality and simple enough for both the pulmonary and non-pulmonary specialist (general practitioner) to use. (Kindly see appendix A). Methodology & Results Generation of the List of Statements for Voting
From September till December of 2011, the PCCP PFTI pulmonary function lab directors or resource persons were requested to answer a survey questionnaire on performance and reporting of spirometry testing in their respective institutions. They were likewise requested to submit a sample of their reports that shows the following results: normal, obstructive, possible restrictive and possible combined defect. The composition of the PCCP-PFTI and their corresponding pulmonary function lab director/resource persons can be seen in appendix B.
On January 9, 2012 and February 20, 2012, the collected survey forms were tallied and analyzed by DATS. Specifically, DATS evaluated the uniformity of the performance and reporting of spirometry testing. From the results and statements of American Thoracic Society and European Respiratory Society Task Force on Standardization of Lung Function Testing (ATS-ERS-TFLFT), DATS came out with a list of proposed recommendations for the different PCCP-PFTI in the performance and reporting of spirometry testing.
The initial list of statements was presented and deliberated upon by the representatives of PCCP-PFTI on March 2, 2012. A revised list was presented to the members of the PCCP during its annual convention on March 14 & 16, 2012. The statements were further modified based on the suggestions during the annual convention. Method Used in Voting and Grading of Consensus Statements
On April 2, 2012, DATS deliberated on the penultimate statements. Thereafter the penultimate document was distributed to the different 11 PCCP PFTI, 4 PCCP Chapters and 3 key opinion leaders for voting. The form used for voting and the list of those who voted can be seen in appendix K & L respectively.
After the votes were tallied (this can be seen in appendix M), the statements were classified according to the following level of consensus:

2
Perfect consensus is defined as 100% of the voters agreeing with the statement and none of the voters chose option D.
Very good consensus is defined as 80 to 99% of the voters agreeing with the statement and there are less than 20% of the voters who chose option D.
Good consensus is defined as either 80 to 99% of the voters agreeing with the statement with more than 20% of
the voters choosing option D 60 to 79% of the voters agreeing with the statement with less than 20% of the
voters choosing option D Some consensus is defined as 51 to 59% of the voters agreeing with the statement No consensus is defined as less than 50% of voters agreeing with the statement
The computation of the parameters needed for the level of consensus classification can
be seen in appendix N.
Based on the level of consensus, the statements were modified based on the modal auxiliary verbs: must, should and may. Statements classified as having either a perfect or a very good consensus used the modal auxiliary verb “must”. Must is used in the context that personnel involved in spirometry testing has a responsibility or an obligation to follow the statement. Statements classified as having a good consensus used the modal auxiliary verb “should”. Should is used in the context that personnel involved in spirometry testing are advised to follow the statement.
There are 22, 25 & 4 statements with perfect, very good and good consensus
respectively. None of the statements were classified as some or no consensus.
Spirometry Testing Consensus Statements
Performance of the Test Statements:
(S1-1) Spirometry testing using the closed circuit technique must be performed based on the standards set by the ATS-ERS-TFLFT1. Part of the procedure includes the answering of the “PCCP DATS Spirometry Testing Information Sheet”. Kindly see appendix I & J (very good consensus).
(S1-2) A referring physician must either request any of the following types of spirometry testing (perfect consensus):
Simple spirometry Spirometry with post bronchodilator study Simple spirometry study with possible post bronchodilator study if initial result is abnormal.
(S1-3) In a situation where in the referring physician requested only a simple spirometry
and it showed abnormal results, the technician in coordination with the doctor (interpreter of the results) must try to seek permission from the referring physician to proceed in performing a post bronchodilator study while the patient is still in the test site (very good consensus) or may suggest Postbronchodilator study in the results.

3
Quality Control
Statements: (S2-1) Daily instrument calibration must be done (very good consensus). (S2-2) The interpreter (lab medical director or pulmonary consultant on deck) must
give a feedback to the technician with regards to the quality of the test (perfect consensus).
(S2-3) A log book must be maintained. It must contain the following (very good consensus): 1. Daily calibration results 2. Anomalous events or problems encountered with the system 3.Feedback of the interpreter to the technician
Parameters Measured
Statements: (S3-1) The following must be measured and reported: FEV1/ FVC, FVC and FEV1 (perfect consensus).
(S3-2) If the spirometry machine is capable, the following should be measured and reported (in order of decreasing importance) (very good consensus):
A. PEFR B. FEF 25-75 C. FEF 75 D. MIF50/ MEF50 E. FEV1/FV6 F. MVV G. MIF 50 H. MEF 50 I. FEV6 J. FEF 25 K. FEF 50
Test Result Selection
Statement: (S4-1) Test result selection must be based on the recommendations set by the ATS-ERS-TFLFT1 (perfect consensus).
1. Report the highest FVC and FEV1 obtained. 2. The spirogram with the highest sum of FEV1 & FVC is chosen as the best trial. 3. The other parameters reported are obtained from the best trial.
Parts of the Report Statements: (S5-1) In the spirometry report, there must be 3 sections for the interpretation of the results (perfect consensus):
A. Technician’s Comments

4
B. Interpreter’s comments C. Final Interpretation
(S5-2) Clinical correlation should not be incorporated in the final interpretation (good consensus).
General Data
Statement: (S6-1) The spirometry report must contain a section on general data which contains the following information (very good consensus):
A. Name of patient B. Age of patient C. Gender of patient D. Measured height E. Measured weight F. Race of patient G. Date of procedure H. Time of procedure I. Room temperature at time of testing J. Room atmospheric pressure at time of testing K. Name of referring physician L. Name of the laboratory M. Phone number of laboratory
Components of the Report Technician’s Comment
Statements: (S7-1) The report must contain a section for the technician’s comments. It should state the indication for doing the test and the information about previous spirometry testing (very good consensus).
(S7-2) The technician’s comments must state if the test done satisfies the ATS-ERS- TFLFT1 reproducibility criteria. If not, it must state which of the criteria was not satisfied (perfect consensus).
(S7-3) The technician’s comments must state if conditions that may alter the results are present or not (perfect consensus).
(S7-4) The technician’s comments must state if the patient is on respiratory drug and if so, when was the last intake (perfect consensus).
(S7-5) The technician’s comments must state the patient’s smoking history particularly the pack years and the last time the patient smoked cigarettes (perfect consensus).

5
For example: Technician’s Comments:
A spirometry test was done to confirm the diagnosis of COPD. Patient has no history of previous spirometry testing. The patient is a previous smoker who has a 20-pack year of smoking history.
His last intake of cigarette smoke was 10 years ago. There were no conditions present in the check list which may alter the results
of this study. The patient took his Indacaterol 16 hours prior to test The test done satisfied the reproducibility criteria set by the ATS-ERS.
Semantics in Interpretation Statement: (S8-1) In the interpretation of the results, the report must use the phrase “ventilatory defect” (not lung defect or ventilatory pattern) (very good consensus).
Interpretation Algorithm
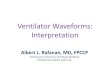
Statement: (S9-1) Spirometry results must be interpreted based on the ATS-ERS-TFLFT2
suggested algorithm.
Fig. 1 Interpretative strategies for lung function tests: R. Pellegrino, G. Viegi, V. Brusasco, et al. Eur Respi Respi J 2005; 26: 948-968.
Use of other Parameters Not in the ATS-ERS-TFLFT Interpretation Algorithm Statements: (S10-1) The best trial flow volume (pre and post-bronchodilator if done) must be part of the spirometry report (perfect consensus).
(S10-2) In cases of possible upper airway obstruction interpretation, all of the trial flow volume loops must be reported. If the spirometry software is not capable, reproducibility

6
of the flow volume loop must be mentioned in the interpreter’s comments (very good consensus). Example: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. The FEV1/FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
4. Flow volume shows a plateau shape of the expiratory limb which is reproducible in 3 acceptable trials. The MIF50/MEF50 is greater than one. These are suggestive of a variable intra thoracic upper airway obstruction.
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation: Probable variable intra-thoracic upper airway obstruction Please correlate results with patient’s clinical data.
(S10-3) Slowing down of the terminal portion of spirogram must be described as “exaggerated concavity in the distal portion of the expiratory limb of the flow volume loop”. Use of the term “scooping” is discouraged (perfect consensus).
(S10-4) In cases where in the interpretation uses any of the following: flow volume loop’s configuration, FEF25-75 and “other spirometry parameters”, it must be stated that these parameters are suggestive but not definitive. Use of the term “compatible” is discouraged (very good consensus). Example: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. The FEV1/FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
4. There is (exaggerated) concavity of the flow volume loop. The FEF 25-75 and FEF 75 are low (using 65% of the predicted as the lower limit of normality). These are suggestive of obstructive (small airways disease) ventilatory defect.
5. The severity of the probable obstructive ventilatory defect is mild, based on the post bronchodilator FEV1 % predicted of 80.
6. There is no significant response to bronchodilator. 7. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation: Probable mild obstructive ventilatory defect Please correlate results with patient’s clinical data.

7
Grading of Severity Statements: (S11-1) Grading of severity must be based on the criteria set by ATS-ERS-TFLFT2 (perfect consensus).
(S11-2) FEV1% predicted (post bronchodilator value if available) must be used both for obstructive and restrictive ventilatory defect (perfect consensus). Table 1: Grading of Severity of Ventilatory Defect
Degree of Severity FEV1 % Predicted (post bronchodilator if available)
Mild 70 & above
Moderate 60-69
Moderately Severe 50-59
Severe 35-49
Very Severe <35
Lower Limit of Normality Statements:
(S12-1) In the spirometry report, all parameters must have corresponding (perfect consensus):
Actual value (in BTPS) Predicted value % Predicted
(S12-2) If the spirometer software is capable (optional), the value corresponding to the 95% CI of the predicted value must be written in the report (very good consensus). (S12-3) If the spirometer software is capable (optional), values < 5th percentile of the predicted should be flagged down (either a change of color or marked). If the spirometer software is not capable, the technician or interpreter should derive this value by manual computation or uses an online calculator at http://www.dynamicmt.com/dataform3.html (good consensus).
(S12-4) The cut-off value for the FEV1/FVC ratio should be <5th percentile of predicted value. If not available, it should be stated in the interpreter’s comments what cut off value was used for the lower limit of normality (good consensus).
(S12-5) Cut off value for the lower limit of normality must be stated in the interpreter’s comments (very good consensus).

8
Example 1: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower limit of normality), there is an obstructive ventilatory defect.
3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
4. The severity of the obstructive ventilatory defect is moderately severe, based on the post bronchodilator FEV1 % predicted of 50.
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation: Moderately severe obstructive ventilatory defect with no significant response to Bronchodilator Please correlate results with patient’s clinical data. Example 2: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS- ERS. 2. The FEV1/FVC is normal (using a fixed cut-off value of 0.70 as the lower limit of normality). 3. The FVC is low (using the 80% of the predicted as the lower limit of normality) which is probably due to a restrictive ventilatory defect or obstructive ventilatory defect (with residual volume hyperinflation). 4. The severity of the restrictive ventilatory defect is mild, based on the post bronchodilator FEV1 % predicted of 70. 5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation:
Probable mild restrictive ventilatory defect with no significant response to bronchodilator.
We suggest requesting for a lung volume study to confirm presence of a restrictive ventilatory defect and rule out obstructive ventilatory defect.
Please correlate results with patient’s clinical data. Response to Bronchodilator Statements: (S13-1) Performance of a post-bronchodilator study must be done based on the recommendations of ATS-ERS-TFLFT2 (perfect consensus).
Procedure for Performance of Post-bronchodilator Study
1. Assess lung function at baseline 2. Administer salbutamol in four separate doses of 100 mg through a spacer 3. Re-assess lung function after 15 minutes. If you want to assess the
potential benefits of a different bronchodilator, use the same dose and the

9
same route as used in clinical practice. The wait time may be increased for some bronchodilators
(S13-2) Interpretation of response to bronchodilator must be based on the criteria set by the ATS-ERS-TFLFT2 (perfect consensus). Criteria for Significant Response to Bronchodilator:
An increase in FEV1 or FVC > 12% of control and > 200 mL. (S13-3) FEF 25-75 must not be used in the interpretation of the post bronchodilator response (perfect consensus). (S13-4) To standardize the semantics, response to bronchodilator must be labeled as “significant or no significant response to bronchodilator”. The use of other terms such as “poor or good response to bronchodilator” are discouraged (perfect consensus).
Statement on Need for Additional Test Statement: (S14-1) Interpretation must include suggestion/s on need for an additional test if warranted (very good consensus).
Reference Equations Statements: (S15-1) In the section on “Interpreter’s Comments” the report must state what reference equation was used in the interpretation of the results. Statement on the need to correlate clinically should be written in the section on “Final Interpretation” (very good consensus). Example: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower limit of normality), there is an obstructive ventilatory defect.
3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
4. The severity of the obstructive ventilatory defect is moderately severe, based on the post bronchodilator FEV1 % predicted of 50.
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation
Moderately severe obstructive ventilatory defect with no significant response to bronchodilator Please correlate results with patient’s clinical data.
(S15-2) A research study must be conducted by the Council of Diagnostics & Therapeutics to determine which reference equation is best fitted for the local Filipino population (very good consensus).

10
Comments on the Quality of the Test Statements: (S16-1) In the reports section on “Interpreter’s Comments”, it must be stated if the test satisfies the reproducibility criteria set by the ATS-ERS-TFLFT1 or not (very good consensus). (S16-2) If the test does not satisfy one of the acceptability or reproducibility criteria, it must state the consequences of this deficiency in the parameters (very good consensus). Example1. Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower limit of normality), there is an obstructive ventilatory defect.
3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality).
4. The severity of the obstructive ventilatory defect is moderately severe, based on the post bronchodilator FEV1 % predicted of 50.
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Example 2: Interpreter’s Comments:
1. Despite several attempts, the end of test criteria was not met. This may underestimate the “true FVC” of the patient. The FEV1 is however reproducible and therefore the patient’s FEV1/FVC may overestimate the patient’s “real FEV1/FVC”
2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower limit of normality), there is an obstructive ventilatory defect.
3. The FVC is low (using the 5th percentile of the predicted as the lower limit of normality). This may be due to poor effort of the patient, obstructive ventilatory (with residual volume hyperinflation) or a concomitant restrictive ventilatory defect.
4. The severity of the obstructive ventilatory defect is moderately severe, based on the post bronchodilator FEV1 % predicted of 50.
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation:
Moderately severe obstructive ventilatory defect with no significant response to bronchodilator
Please correlate results with patient’s clinical data.

11
Components of the Report: Graphical Representation Statements:
(S17-1) The spirometry report must contain at least, the pre (and post-bronchodilator if done) best trial flow volume loop/s (perfect consensus). (S17-2) The spirometry report must contain the flow volume loops of all trials if an interpretation of central airway obstruction (CAO) or upper airway obstruction (UAO) is made. If the spirometry software is not capable, the reproducibility of the flow volume loop must be stated in the section on “Interpreter’s Comments” (very good consensus).
Example: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS- ERS. 2. The FEV1/FVC is normal (using the 5th percentile of the predicted as the lower limit of normality). 3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of normality). 4. Flow volume shows a plateau shape of the expiratory limb which is reproducible in 3 acceptable trials. The MIF50/MEF50 is greater than one. These are suggestive of a variable intra thoracic upper airway obstruction. 5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation:
Probable variable intra-thoracic upper airway obstruction Please correlate results with patient’s clinical data.
Components of the Report: Results in Tabular Graph Statements:
(S18-1) The spirometry report must contain the measured parameters tabular graph (very good consensus).
(S18-2) The first 3 rows of the tabular graph must be allotted for the most reliable spirometry parameter (MRSP) in the following order: {This order will facilitate the interpretation of the results based on the proposed algorithm of ATS-ERS-TFLFT2} (very good consensus).
FEV1/FVC FVC FEV1
(S18-3) The succeeding rows maybe be allotted for the “other parameters” in the following order of priority (very good consensus):
A. PEFR B. FEF 25-75

12
C. FEF 75 D. MIF50/ MEF50 E. FEV1/FV6 F. MVV G. MIF 50 H. MEF 50 I. FEV6 J. FEF 25 K. FEF 50
(S18-4) In the tabular graph, each parameter must have its corresponding (perfect consensus):
A. Actual Values (pre & post if done) B. Predicted C. 95% Confidence Interval Limit (if the spirometry software is capable) D. % Predicted (pre & post if done) E. % Change from baseline of post-bronchodilator measurement (if the spirometry software is capable)
(S18-5) In the tabular graph (if the spirometry software is capable), each parameter below the 5th percentile should be flagged down (good consensus).
Components of the Report: Interpreter’s Comments Statements: (S19-1) The report must contain a section for the interpreter’s comments (IC) of the results (perfect consensus).
(S19-2) The IC section must state if the test satisfied the ATS-ERS-TFLFT1 reproducibility criteria. If the test did not satisfy the criteria, the interpreter must state the consequences of this deficiency (very good consensus).
(S19-3) The IC section must also contain the basis for the interpretation. Specifically it must apply, the ATS-ERS-TFLFT2 (very good consensus):
A. Interpretation algorithm B. Criteria for Severity C. Response to Bronchodilator
Example: Interpreter’s Comments:
1. The spirometry test is of good quality based on standards set by the ATS-ERS.
2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower limit of normality), there is an
obstructive ventilatory defect. 3. The FVC is normal (using the 5th percentile of the predicted
as the lower limit of normality). 4. The severity of the obstructive ventilatory defect is moderately severe, based on the post bronchodilator FEV1 % predicted of 50.

13
5. There is no significant response to bronchodilator. 6. The normality of the parameters is based on the Morris Polgar equation
Components of the Report: Final Interpretation Statements: (S20-1) The spirometry report must contain a section for the final interpretation (FI) of the results (perfect consensus).
(S20-2) The FI must contain the following information (very good consensus):
Presence or absence of Obstructive Ventilatory Defect and severity if present Presence or absence of probable Restrictive Ventilatory Defect and severity if present Significant or No Significant Response to Bronchodilator if done Suggestion for specific additional test if indicated A generic sentence “Please correlate results with patient’s clinical data.” Printed Name and Signature of the Interpreter/s
Example Final Interpretation:
Probable mild restrictive ventilatory defect with no significant response to bronchodilator.
We suggest requesting for a lung volume study to confirm presence of a restrictive ventilatory defect and rule out obstructive ventilatory defect.
Please correlate results with patient’s clinical data. NB: Full document and Executive Summary of the PCCP: Consensus Statement of Spirometry Testing can be down loaded at the PCCP website http://www.philchest.org/ References:
1. American Thoracic Society/ European Respiratory Society. Stardization of Spirometry: M.R. Miller, J. Hankinson, V. Brusasco, F. et al. Eur Respi Resepi J 2005; 26: 319-338.
2. American Thoracic Society/ European Respiratory Society. Interpretative
strategies for lung function tests: R. Pellegrino, G. Viegi, V. Brusasco, et al. Eur Respi Respi J 2005; 26: 948-968.

14
Appendices

APPENDIX A
Name: Juan Cruz
Age: 55
Gender: Male
Height (inch): 64
Weight (lbs): 135
Race: Asian
Date: 11/20/09
Time of procedure: 10:00 AM
Room temperature: 30
Room atmospheric: 760
Referring physician: Dr. Pedro Andres
Name of the laboratory: PCCP PFT Lab
Phone number of laboratory: 723-30-80
Technician’s Comments:
1. A spirometry test was done to confirm the diagnosis of COPD. 2. Patient has no history to previous spirometry testing. 3. The patient is a previous smoker who has a 20-pack year of smoking history. His
last intake of cigarette smoke was 10 years ago. 4. There were no conditions present in the check list which may alter the results of
this study. 5. The patient took his Indacaterol, 16 hours prior to test. 6. The test done satisfied the reproducibility criteria set by the ATS-ERS.
SGD Charlie Go, RT
Interpreter’s Comments: 1. The spirometry test is of good quality based on standards set by the ATS-ERS. 2. Based on a low FEV1/FVC (using the 5th percentile of the predicted as the lower
limit of normality), there is an obstructive ventilatory defect. 3. The FVC is normal (using the 5th percentile of the predicted as the lower limit of
normality). 4. The severity of the obstructive ventilatory defect is moderately severe, based on
the post bronchodilator FEV1 % predicted of 50. 5. There is no significant response bronchodilator response. 6. The normality of the parameters is based on the Morris Polgar equation
Final Interpretation:
o Moderately severe obstructive ventilatory defect with no significant response to bronchodilator
o Please correlate results with patient’s clinical data.
Diego Tigas, MD

APPENDIX B
Institution Resource Person
Chinese General Hospital Eden D. Chua, MD, FPCCP Shirley C. Panganiban Chua, MD, FPCCP
Lung Center of the Philippines Luisito F. Idolor, MD, FPCCP Augusto S. Sablan, Jr. MD, FPCP Araceli Pascual, RT
Manila Doctors Hospital Dennis Teo, MD, FPCCP Aileen M. David-Wang, MD, FPCCP
Philippine Heart Center Rodolfo E. Tamse, MD, FPCCP Irenee Faustina J. Casiño, MD, FPCP
St. Luke’s Medical Center Myrna N. Bañares,MD, FPCCP Raphael Ryan R. Zantua, MD, FPCCP Ma. Janeth T. Samson, MD, FPCCP
UP- Philippine General Hospital Ma. Bella R. Siasoco, MD, FPCCP Jubert P. Benedicto, MD, FPCCP
University of Santo Tomas Hospital Tim S.Trinidad, MD, FPCCP Celeste Mae L. Campomanes, MD, FPCCP Apolonio G. Javier, JR., MD, FPCCP
University of Perpetual-H. D.
Medical Center
Ricardo M. Salonga, MD, FPCCP Jose Edzel V. Tamayo, MD, FPCCP Mary Leslee Tabi,RT Niño Jessielito N. Doydora, MD
Veterans Memorial Medical Center Eloisa S. De Guia, MD, FPCCP
FPCP

APPENDIX C - 1 -
PCCP Council on Diagnostics
Descriptive Survey Form for Use and Reporting of Spirometry Name of Institution: ______________________________ Equipment used (type and model): ________________________________ Please encircle your appropriate response. (NA means not at all times). DO YOU INCLUDE THE FOLLOWING DETAILS IN YOUR REPORT? I. Patient preparation
A. Patient Details
1) Name of patient YES NO NA
2) Patient Identifier (e.g. Date of birth, personal PIN) YES NO NA
3) Gender of patient YES NO NA
4) Age of patient YES NO NA
5) Measured (not stated) Height YES NO NA
6) Estimated Height of a patient with limb deformity YES NO NA
7) Measured (not stated) weight YES NO NA
8) Race of patient YES NO NA
9) Name of Referring physician YES NO NA
10) Vital signs of patient (BP, CR, RR) prior to test
YES NO NA
B. Patient Considerations
1) Symptoms of the patient YES NO NA
2) Smoking history
- Duration of smoking (# of pack years) YES NO NA
- Smoking status (Current or former) YES NO NA
- # of years stopped YES NO NA
3) Medicines taken by patient
- Short acting B agonist (SABA) salmeterol, albuterol, etc YES NO NA
- Inhaled long acting B agonist (LABA) (Salmeterol, formoterol) YES NO NA
- Oral bronchodilator (Salbutamol, formoterol, theophyllines YES NO NA
- Inhaled steroids (Flumetasone, budesonide) YES NO NA
- Oral corticosteroids (prednisone, methylprednisolone, dexamethasone) YES NO NA
- Antileukotrienes (Zafirllukast, montilukast) YES NO NA
- Acute IgE antagonist (omalizumab) YES NO NA
4) Time the above medications were last taken YES NO NA
5) History of following particular symptoms YES NO NA
- Chest or abdominal pain of any cause YES NO NA
- Oral or facial pain exacerbated by mouthpiece YES NO NA
- Stress maintenance YES NO NA
- Dementia or confusional status YES NO NA
6) Position of the patient while performing the test YES NO NA
7) Use of restrictive clothing during test YES NO NA
8) History of doing particular activities immediately prior to test YES NO NA
- Smoking within 1 hour YES NO NA
- Alcohol intake within 4 hours YES NO NA

APPENDIX C - 2 -
- Performing vigorous exercise within 30 minutes YES NO NA - Eating large meals within 2 hours YES NO NA
II. Methods
A. Procedure
Do you perform the following for recording Forced Vital Capacity: 1) Check the spirometer calibration YES NO NA 2) Explain the test YES NO NA 3) Prepare the subject YES NO NA
a. Ask about: Smoking history YES NO NA Recent illness YES NO NA
Medication use YES NO NA Reason for test YES NO NA
b. Measure weight and height without shoes YES NO NA 4) Instruct and demonstrate the test to the subject, to include YES NO NA
a. Correct posture with head slightly elevated YES NO NA b. Inhale rapidly and maximally YES NO NA c. Position of the mouthpiece YES NO NA d. Exhale with maximal force YES NO NA
5) Maneuvers proper (closed-circuit method) YES NO NA a. Have subject assume the correct posture YES NO NA b. Attack nose clip, place mouthpiece in month and close lips around the
mouthpiece YES NO NA
c. Inhale completely and rapidly with a pause of <1 sec at TLC YES NO NA d. Exhale maximally for <6 sec until no more air can be expelled while
maintaining an upright posture YES NO NA
e. Repeat instructions as necessary YES NO NA f. Coach vigorously YES NO NA g. Repeat for a minimum of 3 trials. No more than eight trials YES NO NA h. Check for acceptability YES NO NA i. Check for reproducibility YES NO NA
6) Perform maneuver (open circuit method) YES NO NA a. Have subject assume the correct posture YES NO NA b. Attack nose clip YES NO NA c. Inhale completely and rapidly with a pause of <1 sect at >LC YES NO NA d. Place mouthpiece in mouth and close lips around mouthpiece YES NO NA e. Repeat instructions as necessary YES NO NA f. Coach vigorously YES NO NA g. Repeat for a minimum of 3 trials. No more than eight trials YES NO NA h. Check for acceptability YES NO NA i. Check for reproducibility YES NO NA
Do you check for the following? YES NO NA * Acceptability Criteria YES NO NA
a. Spirograms are free from artifacts YES NO NA Cough during 1st sec of exhalation YES NO NA Glottis closure YES NO NA Early termination YES NO NA Submaximal effort YES NO NA Leaks YES NO NA Obstructed mouthpiece YES NO NA
b. Test results have good starts YES NO NA Extrapolated volume <5% of FVC or 0.15 L, whichever is greater YES NO NA
c. Test shows satisfactory exhalation YES NO NA Duration of ≥ 6s (3s for children) or a plateau in the volume-time
curve or if the subject cannot continue to exhale YES NO NA
Reproducibility Criteria YES NO NA a. After 3 acceptable spirograms have been obtained, do you apply the
following? YES NO NA
The 2 largest values of FVC must be within 0.150 L of each other YES NO NA The 2 largest values of FEV1 must be within 0.150 L of each other YES NO NA
b. If both criteria are meet, conclude test series YES NO NA c. If both criteria are not met, continue testing until ….. YES NO NA
Both criteria are met OR YES NO NA A total of eight test have been performed YES NO NA Subject can no longer continue YES NO NA
d. Save, as a minimum, 3 satisfactory maneuver YES NO NA

APPENDIX C - 3 -
Test Result Selection YES NO NA Do you select YES NO NA
The largest FVC, and largest FEV1 of the same curve YES NO NA The average of FVC and FEV1 even if the don’t come from the same
curve YES NO NA
The maneuver with the largest sum of FVC and FEV1 YES NO NA Aside from FEV1, FVC and FEV1/FVC YES NO NA Do you routinely determine the following YES NO NA
a. FEV6 YES NO NA b. FEV1 / FEV6 YES NO NA c. FEV1 / VC YES NO NA d. FEF 25-75% YES NO NA e. PEF YES NO NA f. Maximal expiratory flow-volume loop YES NO NA g. MVV YES NO NA
III. Interpretation and Reporting Are the following data included in you report? YES NO NA
1) Graphical representation of the best trial flow volume loop YES NO NA 2) Graphical representation of all trials flow volume loop YES NO NA 3) Graphical representation of best trials flow volume loop YES NO NA 4) Graphical representation of all trials flow volume loop YES NO NA 5) Super imposed (overlay) graphical representation of pre and
post bronchodilator best trial YES NO NA
6) Graphical representation of MVV maneuver of best trial YES NO NA 7) Reference equation used in predicted values (ex. Roa, Crapo,
Knudson, etc) YES NO NA
8) Predicted, actual and % predicted of FEV1/FVC YES NO NA 9) Predicted, actual and % predicted of FEV1 YES NO NA 10) Predicted, actual and % predicted of FVC YES NO NA 11) Predicted, actual and % predicted of FEV6 YES NO NA 12) Predicted, actual and % predicted of FEF25 YES NO NA 13) Predicted, actual and % predicted of FEF50 YES NO NA 14) Predicted, actual and % predicted of FEF75 YES NO NA 15) Predicted, actual and % predicted of FEF25-75 YES NO NA 16) Predicted, actual and % predicted of MIF 50 YES NO NA 17) Predicted, actual and % predicted of MEF 50 18) Predicted, actual and % predicted of MIF 50/ MEF 50
YES NO NA
19) MVV (error code) YES NO NA 20) Tabulation of serial PTT (if with previous spirometry) YES NO NA 21) Technologist comments YES NO NA 22) Name of results interpreter YES NO NA
In the interpretation of results are the comments on the following included
Quality of the test YES NO NA Ventilatory pattern of flow volume loop YES NO NA Parameters which are abnormal YES NO NA Type of ventilatory defect (objective, restrictive or mixed) YES NO NA Severity of ventilatory defect YES NO NA Response to bronchodilators YES NO NA Need for additional test (LV, DLCO, post bronchodilator test serial testing) YES NO NA Clinical correlation with patients signs and symptoms YES NO NA Need to correlate with clinical data YES NO NA
Please tick the appropriate box and fill up the blank if needed
1) Is the format of results released to patient different from what is interpreted by the physician?
YES NO NA
2) What reference equation is your laboratory test result interpreter using for classifying the normality or abnormality of the measured parameters? If using a foreign equation, kindly state the correction factor that your laboratory is using?
YES NO NA

APPENDIX C - 4 -
[ ] We are using _____________________________________________ with a correction factor of ___________________________
3) Was the decision of your laboratory interpreter in choosing your reference equation based on a local study that you had done in your institution?
YES NO NA
4) Does your laboratory results interpreter use only one reference equation for all the measured parameters? If no, kindly explain.
[ ] if no, we use the following reference equations __________________ _________________________________________________________________________________________________________________________________________________________________________________
YES NO NA
5) When does your laboratory results interpreter classify the FEV1/FVC, FEV1/FEV6 as abnormal?
[ ] < 0.7 [ ] < 80% of the predicted [ ] < percentile of the normal range
YES NO NA
6) Aside from the FEV1, FVC and FEV1/FVC, does your laboratory test results interpreter use the “other parameters” routinely (example FEF 25-75, MIF 50, MEF 50, MIF 50/MEF 50. FEV1/PEF and FEV1/FEV6
[ ] If yes. Which parameters? __________________________________ __________________________________________________________
YES NO NA
7) Are the criteria that your laboratory results interpreter uses for a positive (significant/good) response to a bronchodilator as follows: an increase in FEV1 or FVC ≥ 12% and 200 ml increase from baseline value?
[ ] If not, kindly state the criteria your laboratory uses. ____________ _________________________________________________________________________________________________________________________________________________________________________________
YES NO NA
8) Does your laboratory test result interpreter, routinely comments on the MVV?
YES NO NA
9) The criteria for the classification of ventilatory dysfunction suggested by the ATS/ERS are tabulated below. Does your laboratory test interpreter follow this classification?
YES NO NA
FEV1 % Predicted Mild > 70 Moderate 60 – 69 Moderately severe 50 – 59 Severe 35 – 49 Very severe < 39
IV. Quality Control
A. Laboratory Details 1) Name of laboratory YES NO NA 2) Address of laboratory YES NO NA 3) Phone number of laboratory YES NO NA 4) Name of technician who conducted the test YES NO NA 5) Date of procedure YES NO NA 6) Time of procedure YES NO NA 7) Room temperature at time of testing YES NO NA 8) Room atmospheric pressure at time of testing YES NO NA 9) Indication for procedure YES NO NA 10) Possible order for undertaking lung function tests YES NO NA
B. Personal Qualifications YES NO NA 1) Who interprets the result YES NO NA
a) Pulmonary fellow YES NO NA b) Pulmonary function laboratory director YES NO NA c) Pulmonary consultant on deck YES NO NA d) Patients’ attending pulmonary consultant YES NO NA
PFT techniques and Procedures
YES NO NA

APPENDIX C - 5 -
2) Do you have a manual of procedure which contain the following:
- Calibration procedure YES NO NA - Test performance procedures YES NO NA - Calculations YES NO NA - Criteria YES NO NA - Reference values source YES NO NA - Action to be taken when “panic” values are observed
YES NO NA
3) Do you have a record which documents the following?
- Schedule of instrument calibration ( daily, weekly, monthly, quarterly, others )
YES NO NA
- Problems encountered with the system YES NO NA - Correction action required YES NO NA - Systems hardware and software upgrades YES NO NA - Record of anomalous events involving either
patients / subjects or technicians and result of subsequent evaluation and responses to event
YES NO NA
- Record of continuing education of personnel YES NO NA - Record of results of evaluation and feedback
provided by medical director YES NO NA
- Schedule and procedures for routine maintenance of all equipment in the facility
YES NO NA
- Record of contact phonee numbers of appropriate maintenance personnel for each equipment used in the facility
YES NO NA
4) Is there a protocol and frequency for calibration? YES NO NA 5) Is there a protocol for testing standard subjects
monthly to supplement spirometry, LV and diffusing capacity?
YES NO NA
6) Is there a schedule for specific quality control procedures for each procedure done?
YES NO NA
7) Are tolerance limits deprived for quality control checks for each procedure?
YES NO NA
8) Is there a plan for corrective action when tolerance limits are exceeded?
YES NO NA
9) Are standard subjects tested monthly? YES NO NA 10) Is there evidence of review by medical director or
head of pulmonary laboratory? YES NO NA
11) Are manuals available for: - Equipments YES NO NA - Policies YES NO NA - Procedures YES NO NA - Safety YES NO NA
12) Are these manuals readily accessible? YES NO NA
V. Hygiene and Infection Control YES NO NA Do you perform the following precautions when performing spirometry? YES NO NA
1) Strict hand washing in between patients YES NO NA 2) Wearing gloves when handling body fluids YES NO NA 3) Require suspected potential active infection patients tested on an
isolation room or negative pressure room YES NO NA
4) Prepare testing rooms with filtration or UV decontamination device YES NO NA 5) Require patients with suspected infection airborne disease to wear
barrier protection YES NO NA
6) Require technicians to wear barrier protection YES NO NA 7) Flushing of air in a volume displacement spirometer at least 5x in
between subjects YES NO NA

APPENDIX C - 6 -
8) Require potentially infected patients with airborne disease be tested at end of day or week
YES NO NA
9) Require use of disposable mouthpiece of disinfection of tubing or any parts that come into direct contact with subjects
YES NO NA
10) Do you use an open circuit technique? (open circuit means no rebreathing through mouthpiece of through breathing tube)
If answer is YES:
YES NO NA
a) Do you change the mouthpiece between patients? YES NO NA b) Do you change the breathing tube between patients? YES NO NA
11) Do you use the closed circuit technique (closed circuit means subject rebreaths into the mouthpiece or through breathing tube and spirometer)? If answer is YES
YES NO NA
a) Do you dispose of or disinfect the mouthpiece between patients? YES NO NA b) Do you dispose of or disinfect the breathing tube between patients? YES NO NA
12) Do you use a flow sensing system in which no breathing tube is interposed between subject and device?
YES NO NA
a) Is the flow sensing element and interior tubing disinfected between patients?
YES NO NA
b) Is inspiration from the device avoided? YES NO NA 13) Do you use in-line bacterial filters? If answer is yes… YES NO NA
a) Do you calibrate machine with the filters? YES NO NA b) Do you discard the filter after use on a single subject? YES NO NA c) Do you still do regular cleaning and disinfection despite the filters? YES NO NA YES NO NA
Comments: _____________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Completed by: Noted by: ______________________________ ______________________________ Name and Position Head of the Pulmonary Laboratory

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH3 Equipment Vmax
SpectraJaeger-Master Screen
Vmax Spectra 22
Viasys Vmax Spectra
Microloop Vmax
4 Do you include the following details in your report (Are information about the following noted?)
5 Patient Preparation6 Patient Details7 1) Name of patient YES YES YES YES YES YES YES YES YES8 2) Patient identifier YES YES YES YES YES YES YES YES9 3) Gender of patient YES YES YES YES YES YES YES YES YES
10 4) Age of patient YES YES YES YES YES YES YES YES YES11 5) Measured height YES YES YES YES YES YES YES YES YES12 6) Estimated Height of a patient with limb deformity YES YES YES YES YES NO YES YES YES13 7) Measured weight YES YES YES YES YES YES YES YES YES14 8) Race of patient YES YES YES YES YES YES YES YES YES15 9) Name of referring physician YES YES YES YES YES YES YES YES YES16 10) Vitas signs of patient (BP, CR, RR) prior to test NO NO NO NO NA NO YES YES YES17 Patient Considerations18 1) Symptoms of the patient YES YES YES YES YES YES YES YES YES19 2) Smoking history 20 Duration of smoking (# of pack years) YES YES YES YES YES NO YES YES YES21 Smoking status (current or former) YES YES YES YES YES YES YES YES YES22 # of years stopped YES YES YES NO YES NO YES YES YES23 3) Medicines taken by patient24 Short acting B agonist YES YES YES YES YES NA YES YES NO25 Inhaled long acting B agonist YES YES YES YES NA YES YES NO26 Oral bronchodilator YES YES YES YES YES NA YES YES NO27 Inhaled steroids YES YES NO YES YES NA YES YES NO28 Oral corticosteroids YES NO NO YES YES NA YES YES NO29 Antileukotrienes YES NO NO YES YES NA YES YES NO30 Anti-IgE antagonist NA NO NO NO YES NA YES YES NO31 4) Time the above medications were last taken YES YES YES YES NO YES YES YES NO32 5) History of the following particular symptoms33 Chest or abdominal pain of any cause NA NO YES YES NO YES YES YES YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
34 Oral or facial pain exacerbated by mouthpiece YES NO NO NO NO NO YES YES YES35 Stress incontinence NA NO NO NO NO NO YES YES YES36 Dementia or confusional status YES NO NO NO NO NO YES YES YES37 6) Position of the patient while performing the test YES YES NO YES NO NO YES YES NO38 7) Use of restrictive clothing during the test YES NO YES NO NO NO YES YES NO39 8) History of doing particular activities immediately prior to test40 Smoking within 1 hour YES NO YES NO NO NO YES YES YES41 Alcohol intake within 4 hours YES NO YES NO NO NO YES YES YES42 Performing vigourous exercise within 30 mins YES NO YES YES NO NO YES YES YES43 Eating large meals within 2 hours YES NO YES NO NO NO YES YES YES44 Methods45 Procedure46 Do you perform the following for recording FVC47 1) Check the spirometer calibration YES YES YES YES YES YES YES YES YES48 2) Explain the test YES YES YES YES YES YES YES YES YES49 3) Prepare the subject50 Ask about: Smoking history YES YES YES YES YES YES YES YES YES51 Recent illness YES YES YES YES YES YES YES YES YES52 Medication use YES YES YES YES YES YES YES YES YES53 Reason for test YES YES YES YES YES YES YES YES YES54 Measure weight and height without shoes YES YES YES YES YES YES YES YES YES55 4) Instruct and demonstrate the test to the subject, to include56 Correct posture YES YES YES YES YES YES YES YES57 Inhale rapidly and maximally YES YES YES YES YES YES YES YES YES58 Position of the mouthpiece YES YES YES YES YES YES YES YES YES59 Exhale with maximal force YES YES YES YES YES YES YES YES YES60 5) Maneuvers proper (closed-circuit method)61 Have subject assume the correct posture YES YES YES YES YES YES YES YES YES62 Attach nose clip, place mouthpiece in mouth and close lips
around the mouthpieceYES YES YES YES YES YES YES YES YES
63 Inhale completely and rapidly with a pause of <1sec at TLC YES YES YES YES YES YES YES YES YES64 Exhale maximally for <6secs until no more air can be expelled
while maintaining an upright postureYES YES YES YES YES YES YES YES YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
65 Repeat instructions as necessary YES YES YES YES YES YES YES YES YES66 Coach vigorously YES YES YES YES YES YES YES YES YES67 Repeat for a minimum of 3 trials. No more than 8 trials YES YES YES YES YES YES YES YES YES68 Check for acceptability YES YES YES YES YES YES YES YES YES69 Check for reproducibility YES YES YES YES YES YES YES YES YES70 6) Perform maneuver (open circuit method)71 Have subject assume the correct posture YES YES YES YES NA NO YES YES YES72 Attach nose clip YES YES YES YES NA NO YES YES YES73 Inhale completely and rapidly with a pause of <1sec at TLC YES YES YES YES NA NO YES YES YES74 Place mouthpiece in mouth and close lips around mouthpiece YES YES YES YES NA NO YES YES YES75 Repeat instructions as necessary YES YES YES YES NA NO YES YES YES76 Coach vigorously YES YES YES YES NA NO YES YES YES77 Repeat for a minimum of 3 trials. No more than 8 trials YES YES YES YES NA NO YES YES YES78 Check for acceptability YES YES YES YES NA NO YES YES YES79 Check for reproducibility YES YES YES YES NA NO YES YES YES80 Do you check the following81 Acceptability Criteria82 a) Spirograms are free from artifacts83 Cough during 1st second of exhalation YES YES YES YES YES YES YES YES YES84 Glottis closure YES YES YES YES YES YES YES YES YES85 Early termination YES YES YES YES YES YES YES YES YES86 Submaximal effort YES YES YES YES YES YES YES YES YES87 Leaks YES YES YES YES YES YES YES YES YES88 Obstructive mouthpiece YES YES YES YES YES YES YES YES YES89 b) Test results have good starts90 Extrapolated volume <5% of FVC or 0.15L, whichever is greater YES YES YES YES YES NA YES YES YES
91 c) Test shows satisfactory exhalation YES YES YES YES YES YES YES YES YES92 Duration of >= 6 secs or a plateau in the volume-time curve or if
the subject cannot continue to exhaleYES YES YES YES NA YES YES YES YES
93 Reproducibility Criteria94 a) After 3 acceptable spirograms have been obtained, do you apply
the following?

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
95 The 2 largest values of FVC must be within 0.150L of each other YES YES YES YES YES YES YES YES YES
96 The 2 largest values of FEV1 must be within 0.150L of each other
YES YES YES YES YES YES YES YES YES
97 b) If both criteria are met, conclude test series YES YES YES YES YES YES YES YES YES98 c) If both criteria are not met, continue testing until99 Both criteria are met OR YES YES YES YES YES YES YES YES YES
100 A total of eight tests have been performed YES YES YES YES YES NA NO YES YES101 Subject can no longer continue YES YES YES YES * YES NO YES YES102 d) Save, as a minimum, 3 satisfactory maneuvers YES YES YES YES YES YES YES YES103 Test Result Selection104 Do you select (SELECT ONE ONLY)105 The largest FVC and the largest FEV1 of the same curve YES YES NO YES YES YES NO YES YES106 The average of FVC and FEV1 even if they don't come from the
same curveYES YES NO YES YES NO YES YES
107 The maneuver with the largest sum of FVC and FEV1 YES YES YES YES NA NO NO YES108 Aside from FEV1, FVC and FEV1/FVC, do you routinely determine
the following109 Aside from FEV1, FVC and FEV1/FVC, do you routinely determine
the following110 a) FEV6 YES NO NO NO NO YES NO YES NO111 b) FEV1/FEV6 NO NO NO NO NO NO NO YES NO112 e) PEF YES YES YES YES YES YES YES YES YES113 g) MVV YES YES YES YES YES YES YES YES YES114 Are the following data included in your report?115 Are the following data included in your report?116 Are the following data included in your report?117 1) Graphical representation of the best trial flow volume loop YES YES YES YES YES YES YES YES YES118 2) Graphical representation of all trials flow volume loop YES NO YES YES NO NO YES NO YES119 3) Graphical representation of best trials flow volume loop (SAME
AS #1)120 3) Superimposed (overlay) graphical representation of pre and post
bronchodilator best trialYES YES YES YES YES YES YES YES YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
121 4) Graphical representation of MVV maneuver of best trial YES YES YES YES YES NO YES NO YES122 5) Reference equation used in predicted values (ex. Roa, Crapo,
Knudson, etc)YES YES YES NO YES YES YES
123 6) Predicted, actual and % predicted of FEV1/FVC YES YES YES YES YES YES YES YES YES124 7) Predicted, actual and % predicted of FEV1 YES YES YES YES YES YES YES YES YES125 8) Predicted, actual and % predicted of FVC YES YES YES YES YES YES YES YES YES126 11) Predicted, actual and % predicted of FEF50 YES YES YES YES NO YES YES YES127 12) Predicted, actual and % predicted of FEF75 YES YES YES YES YES NO YES YES YES128 13) Predicted, actual and % predicted of FEF25-75 YES YES YES YES YES YES YES YES YES129 14) Predicted, actual and % predicted of MIF50 YES YES NO YES NO NO NO NA NO130 15) Predicted, actual and % predicted of MEF50 YES YES NO NO NO NO NO NA NO131 16) Predicted, actual and % predicted of MIF50/MEF50 NO NO NA132 17) MVV (error code) YES YES YES YES YES NO NO NA YES133 18) Tabulation of serial PTT (if with previous spirometry) NO NO NO NO YES NO NO NA NO134 In the interpretation of results are the comments on the following
included135 Quality of test YES YES YES YES NO YES YES YES136 Ventilatory pattern of flow volume loop YES YES YES YES YES NO YES YES YES137 Parameters which are abnormal YES YES YES YES YES YES YES YES YES138 Type of ventilatory defect (obstructive, restrictive or mixed) YES YES YES YES YES YES YES YES YES139 Severity of ventilatory defect YES YES YES YES YES YES YES YES YES140 Resonse to bronchodilators YES YES YES YES YES YES YES YES YES141 Need for additional test (LV, DLCO, postbronchodilator test
serial testing)YES YES YES YES YES YES YES YES YES
142 Clinical correlation with patients signs and symptoms YES YES NO YES NA NO YES YES YES143 Need to correlate with clinical data YES YES YES YES NA YES YES YES YES144 Please tick the appropriate box and fill up the blank if needed145 1) Is the format of results released to patient different from what is
interpreted by the physician?NO NO NO NO NO NO NO NO NO
146 2) What reference equation is your laboratory test result interpreter using for classifying the normality or abnormality of the measured parameters? If using a foreign equation, kindly state the correction factor that your laboratory is using?
Morris Polgar
Morris Polgar
Morris Polgar
ECCS Morris Polgar
ATS, GOLD
NHANES, 0.88 OF
ABS VALUE
ATS Morris Polgar

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
147 3) Was the decision of your laboratory interpreter in choosing your reference equation based on a local study that you had done in your institution?
NO NA NO YES NO NO NO NO NO
148 4) Does your laboratory results interpreter use only one reference equation for all the measured parameters? If no, kindly explain.
YES YES YES YES YES YES YES YES YES
149 5) When does your laboratory results interpreter classify the FEV1/FVC, FEV1/FEV6 as abnormal?
150 <0.7 YES YES YES (0.75) YES YES YES YES YES YES151 <80% of predicted YES YES152 < percentile of the normal range YES153 6) Aside from the FEV1, FVC and FEV1/FVC, does your laboratory
test results interpreter use the "other parameters" routinely?YES YES NO FEF25-
75, PEF, FEF25, FEF50, FEF75
FEF 25-75
FEF25-75,
FEF75-85, FEF
200-1200
FEF 25-75
NO NO
154 7) Is the criteria that your laboratory results interpreter uses for a positive response to a bronchodilator as follows: an increase in FEV1 or FVC >= 12% and 200 ml increase from baseline value
YES YES YES YES YES YES YES YES YES
155 8) Does your laboratory test result interpreter routinely comment on the MVV?
YES YES NO NO NA NO NO NA YES
156 8) Does your laboratory test result interpreter routinely comment on the MVV?
YES YES NO NO NA NO NO NA YES
157 9) Is the criteria for the classification of ventilatory dysfunction suggested by the ATS/ERS followed by your laboratory test interpreter?
YES YES YES YES YES YES YES YES YES
158 Quality Control159 Laboratory Details160 1) Name of laboratory YES YES YES YES YES YES YES YES YES161 2) Address of laboratory YES YES YES YES YES YES YES YES YES162 3) Phone number of laboratory YES YES YES YES YES NO YES YES NO163 4) Name of techinican who conducted the test YES YES YES YES YES YES YES YES YES164 5) Date of procedure YES YES YES YES YES YES YES YES YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
165 6) Time of procedure YES YES YES YES YES NO YES YES YES166 7) Room temperature at time of testing YES YES YES YES NO NO YES YES YES167 8) Room atmospheric pressure at time of testing YES YES YES YES NO NO NA NO YES168 10) Possible sequence for undertaking lung function tests YES YES YES YES NO YES YES NO169 1) Who interprets the result170 Pulmonary fellow YES YES YES YES YES YES YES YES YES171 Pulmonary function laboratory director NA NO YES NO NO YES NA YES172 Pulmonary consultant on deck YES YES YES YES YES YES YES YES YES173 Patient's attending pulmonary consultant YES YES YES YES NO YES YES NO174 PFT Techniques and Procedures175 2) Do you have a manual of procedure which contain the following
176 Calibration procedure YES YES YES YES YES YES YES YES YES177 Test performance procedures YES YES YES YES YES YES YES YES YES178 Calculations YES YES YES YES YES YES YES YES YES179 Criteria YES YES YES YES YES YES YES YES YES180 Reference values source YES YES YES YES YES YES YES YES YES181 Action to be taken when "panic" values are observed YES YES YES YES YES YES YES YES182 3) Do you have a record which documents the following183 Schedule of instrument calibration YES YES YES YES YES YES NO YES YES184 Problems encountered with the system YES YES YES YES YES YES NO YES YES185 Correction action required YES YES YES YES YES YES YES YES YES186 Systems hardware and software upgrades YES YES YES NO NO YES YES187 Record of anomalous events involving either patients/subjects or
technicians and result of subsequent evaluation and responses to event
YES YES NO YES NO YES NO YES YES
188 Record of continuing eduction of personnel NO NO NO YES YES YES YES YES YES189 Record of results of evaluation and feedback provided by
medical directorNO YES NO YES YES NO NO NA YES
190 Schedule and procedures for routine maintenance of all equipment in the facility
YES YES NO YES YES NO YES YES YES
191 Record of contact phone numbers of appropriate maintenance of all equipment in the facility
YES YES YES YES YES YES YES YES YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
192 4) Is there a protocol and frequency for calibration? YES YES YES YES YES YES YES NA YES193 5) Is there a protocol for testing standard subjects monthly to
supplement spirometry, LV and diffusing capacity?YES YES NO YES YES NA YES NA YES
194 6) Is there a schedule for specific quality control procedures for each procedure done?
YES YES NO YES YES NO YES NA YES
195 7) Are tolerance limits derived for quality control checks for each procedure?
YES YES NO YES YES YES NO NA YES
196 8) Is there a plan for corrective action when tolerance limits are exceeded?
YES YES NO YES YES YES NO NA YES
197 9) Are standard subjects tested monthly? YES NO YES YES NA NO YES NO YES198 10) Is there evidence of review by medical director or head of
pulmonary laboratory?NO YES NO YES YES NO YES NO YES
199 11) Are manuals available for200 Equipments YES YES YES YES YES YES YES YES201 Policies YES YES YES YES YES YES YES YES YES202 Procedures YES YES YES YES YES YES YES YES YES203 Safety YES YES YES YES YES YES YES YES YES204 12) Are these manuals readily accessible? YES YES YES YES YES YES YES YES YES205 Hygine and Infection Control206 Do you perform the following precautions when performing
spirometry?207 1) Strict handwashing in between patients YES YES YES YES YES YES YES YES YES208 2) Wearing gloves by the technician when handling body fluids and
equipmentYES YES YES YES YES YES YES YES YES
209 3) Require suspected potential active infection patients tested on an isolation room or negative pressure room
YES NO NO YES NA NO NA YES YES
210 4) Prepare testing rooms with filtration or UV decontamination device
NO NO NO NO NO NO NA YES
211 5) Require patients with suspected infectious airborne disease to wear barrier protection
YES NO NO YES YES YES NA NA YES
212 6) Require technicians to wear barrier protection YES NO YES YES YES YES YES YES YES213 7) Flushing of air in a volume displacement spirometer at least 5x in
between subjectsYES NO NO NO YES YES NO NA YES

Appendix D Tally of Responses to the Survey Questions
1 PCCP Council on Diagnostics: Descriptive Survey Form for Use and Reporting of Spirometry2 SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH
214 8) Require potentially infected patients with airborne disease to be tested at the end of the day or week
YES NO YES YES YES NA NA NA YES
215 9) Require use of disposable mouthpiece of disinfection of tubing or any parts that come into direct contact with subjects
YES YES YES YES YES YES YES YES YES
216 10) Do you use an open circuit technique? If yes, YES YES NO NO NO YES217 Do you change the mouthpiece between patients? YES YES YES YES YES YES YES218 Do you change the breathing tube between patients? NO NO YES NO NO NA YES219 11) Do you use the closed circuit technique? If yes, YES YES YES YES YES NA220 Do you dispose of or disinfect the mouthpiece between
patients?YES YES YES YES YES YES YES YES
221 Do you dispose of or disinfect the breathing tube between patients?
NO NO NO NO YES NO YES YES
222 12) Do you use a flow sensing system in which no breathing tube is interposed between subject and device?
YES NO YES YES NO YES YES
223 Is the flow sensing element and interior tubing disinfected between patients?
NO YES NO YES YES NO YES YES YES
224 Is inspiration from the device avoided? YES YES NO NO YES NO YES YES YES225 13) Do you use in-line bacterial filters? If yes, YES YES YES YES YES YES YES YES YES226 Do you calibrate machine with the filters? NO NO NO YES YES NO YES YES YES227 Do you discard the filter after use on a single patient? YES YES YES NO YES YES YES YES YES228 Do you still do regular cleaning and disinfection despite the
filters?YES YES YES YES YES YES NA YES YES

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH2 Do you perform the following for recording FVC3 1) Check the spirometer calibration YES YES YES YES YES YES YES YES YES4 2) Explain the test YES YES YES YES YES YES YES YES YES5 3) Prepare the subject6 Ask about: Smoking history YES YES YES YES YES YES YES YES YES7 Recent illness YES YES YES YES YES YES YES YES YES8 Medication use YES YES YES YES YES YES YES YES YES9 Reason for test YES YES YES YES YES YES YES YES YES10 Measure weight and height without shoes YES YES YES YES YES YES YES YES YES11 4) Instruct and demonstrate the test to the subject, to include12 Correct posture YES YES YES YES YES YES YES YES13 Inhale rapidly and maximally YES YES YES YES YES YES YES YES YES14 Position of the mouthpiece YES YES YES YES YES YES YES YES YES15 Exhale with maximal force YES YES YES YES YES YES YES YES YES16 5) Maneuvers proper (closed-circuit method)17 Have subject assume the correct posture YES YES YES YES YES YES YES YES YES18 Attach nose clip, place mouthpiece in mouth and close lips around
the mouthpieceYES YES YES YES YES YES YES YES YES
19 Inhale completely and rapidly with a pause of <1sec at TLC YES YES YES YES YES YES YES YES YES20 Exhale maximally for <6secs until no more air can be expelled while
maintaining an upright postureYES YES YES YES YES YES YES YES YES
21 Repeat instructions as necessary YES YES YES YES YES YES YES YES YES22 Coach vigorously YES YES YES YES YES YES YES YES YES23 Repeat for a minimum of 3 trials. No more than 8 trials YES YES YES YES YES YES YES YES YES24 Check for acceptability YES YES YES YES YES YES YES YES YES25 Check for reproducibility YES YES YES YES YES YES YES YES YES26 6) Perform maneuver (open circuit method)27 Have subject assume the correct posture YES YES YES YES NA NO YES YES YES28 Attach nose clip YES YES YES YES NA NO YES YES YES29 Inhale completely and rapidly with a pause of <1sec at TLC YES YES YES YES NA NO YES YES YES30 Place mouthpiece in mouth and close lips around mouthpiece YES YES YES YES NA NO YES YES YES31 Repeat instructions as necessary YES YES YES YES NA NO YES YES YES32 Coach vigorously YES YES YES YES NA NO YES YES YES33 Repeat for a minimum of 3 trials. No more than 8 trials YES YES YES YES NA NO YES YES YES

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH34 Check for acceptability YES YES YES YES NA NO YES YES YES35 Check for reproducibility YES YES YES YES NA NO YES YES YES36 Do you check the following37 Acceptability Criteria38 a) Spirograms are free from artifacts39 Cough during 1st second of exhalation YES YES YES YES YES YES YES YES YES40 Glottis closure YES YES YES YES YES YES YES YES YES41 Early termination YES YES YES YES YES YES YES YES YES42 Submaximal effort YES YES YES YES YES YES YES YES YES43 Leaks YES YES YES YES YES YES YES YES YES44 Obstructive mouthpiece YES YES YES YES YES YES YES YES YES45 b) Test results have good starts46 Extrapolated volume <5% of FVC or 0.15L, whichever is greater YES YES YES YES YES NA YES YES YES47 c) Test shows satisfactory exhalation YES YES YES YES YES YES YES YES YES48 Duration of >= 6 secs or a plateau in the volume-time curve or if the
subject cannot continue to exhaleYES YES YES YES NA YES YES YES YES
49 Reproducibility Criteria50 a) After 3 acceptable spirograms have been obtained, do you apply the
following?51 The 2 largest values of FVC must be within 0.150L of each other YES YES YES YES YES YES YES YES YES52 The 2 largest values of FEV1 must be within 0.150L of each other YES YES YES YES YES YES YES YES YES53 b) If both criteria are met, conclude test series YES YES YES YES YES YES YES YES YES54 c) If both criteria are not met, continue testing until55 Both criteria are met OR YES YES YES YES YES YES YES YES YES56 A total of eight tests have been performed YES YES YES YES YES NA NO YES YES57 Subject can no longer continue YES YES YES YES * YES NO YES YES58 d) Save, as a minimum, 3 satisfactory maneuvers YES YES YES YES YES YES YES YES5960 1) Who interprets the result61 Pulmonary fellow YES YES YES YES YES YES YES YES YES62 Pulmonary consultant on deck YES YES YES YES YES YES YES YES YES63 Pulmonary function laboratory director NA NO YES NO NO YES NA YES64 Do you perform the following for recording FVC

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH65 1) Check the spirometer calibration YES YES YES YES YES YES YES YES YES66 3) Do you have a record which documents the following67 Schedule of instrument calibration YES YES YES YES YES YES NO YES YES68 Problems encountered with the system YES YES YES YES YES YES NO YES YES69 Record of anomalous events involving either patients/subjects or
technicians and result of subsequent evaluation and responses to eventYES YES NO YES NO YES NO YES YES
70 Record of results of evaluation and feedback provided by medical director
NO YES NO YES YES NO NO NA YES
7172 Are the following data included in your report?73 6) Predicted, actual and % predicted of FEV1/FVC YES YES YES YES YES YES YES YES YES74 8) Predicted, actual and % predicted of FVC YES YES YES YES YES YES YES YES YES75 7) Predicted, actual and % predicted of FEV1 YES YES YES YES YES YES YES YES YES76 13) Predicted, actual and % predicted of FEF25-75 YES YES YES YES YES YES YES YES YES77 Aside from FEV1, FVC and FEV1/FVC, do you routinely determine the
following78 e) PEF YES YES YES YES YES YES YES YES YES79 g) MVV YES YES YES YES YES YES YES YES YES8081 Are the following data included in your report?82 11) Predicted, actual and % predicted of FEF50 YES YES YES YES NO YES YES YES83 12) Predicted, actual and % predicted of FEF75 YES YES YES YES YES NO YES YES YES8485 Aside from FEV1, FVC and FEV1/FVC, do you routinely determine the
following86 14) Predicted, actual and % predicted of MIF50 YES YES NO YES NO NO NO NA NO87 15) Predicted, actual and % predicted of MEF50 YES YES NO NO NO NO NO NA NO88 16) Predicted, actual and % predicted of MIF50/MEF50 NO NO NA89 a) FEV6 YES NO NO NO NO YES NO YES NO90 b) FEV1/FEV6 NO NO NO NO NO NO NO YES NO91

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH92 6) Aside from the FEV1, FVC and FEV1/FVC, does your laboratory test
results interpreter use the "other parameters" routinely?YES YES NO FEF25-
75, PEF, FEF25, FEF50, FEF75
FEF 25-75
FEF25-75, FEF75-85, FEF 200-1200
FEF 25-75
NO NO
9394 Test Result Selection95 Do you select (SELECT ONE ONLY)96 The largest FVC and the largest FEV1 of the same curve YES YES NO YES YES YES NO YES YES97 The average of FVC and FEV1 even if they don't come from the
same curveYES YES NO YES YES NO YES YES
98 The maneuver with the largest sum of FVC and FEV1 YES YES YES YES NA NO NO YES99100 6) Aside from the FEV1, FVC and FEV1/FVC, does your laboratory test
results interpreter use the "other parameters" routinely?YES YES NO FEF25-
75, PEF, FEF25, FEF50, FEF75
FEF 25-75
FEF25-75, FEF75-85, FEF 200-1200
FEF 25-75
NO NO
101102 In the interpretation of results are the comments on the following
included103 Ventilatory pattern of flow volume loop YES YES YES YES YES NO YES YES YES104105 Are the following data included in your report?106 1) Graphical representation of the best trial flow volume loop YES YES YES YES YES YES YES YES YES107 2) Graphical representation of all trials flow volume loop YES NO YES YES NO NO YES NO YES108109 In the interpretation of results are the comments on the following
included110 9) Is the criteria for the classification of ventilatory dysfunction
suggested by the ATS/ERS followed by your laboratory test interpreter?YES YES YES YES YES YES YES YES YES
111

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH112 5) When does your laboratory results interpreter classify the
FEV1/FVC, FEV1/FEV6 as abnormal?113 <0.7 YES YES YES (0.75) YES YES YES YES YES YES114 <80% of predicted YES YES115 < percentile of the normal range YES116117 7) Is the criteria that your laboratory results interpreter uses for a
positive response to a bronchodilator as follows: an increase in FEV1 or FVC >= 12% and 200 ml increase from baseline value
YES YES YES YES YES YES YES YES YES
118119 In the interpretation of results are the comments on the following
included120 Need for additional test (LV, DLCO, postbronchodilator test serial
testing)YES YES YES YES YES YES YES YES YES
121122 2) What reference equation is your laboratory test result interpreter
using for classifying the normality or abnormality of the measured parameters? If using a foreign equation, kindly state the correction factor that your laboratory is using?
Morris Polgar
Morris Polgar
Morris Polgar
ECCS Morris Polgar
ATS, GOLD
NHANES, 0.88 OF ABS VALUE
ATS Morris Polgar
123 3) Was the decision of your laboratory interpreter in choosing your reference equation based on a local study that you had done in your institution?
NO NA NO YES NO NO NO NO NO
124125 In the interpretation of results are the comments on the following
included126 Quality of test YES YES YES YES NO YES YES YES127128 Do you include the following details in your report (Are information
about the following noted?)129 Patient Details130 1) Name of patient YES YES YES YES YES YES YES YES YES131 2) Patient identifier YES YES YES YES YES YES YES YES132 3) Gender of patient YES YES YES YES YES YES YES YES YES133 4) Age of patient YES YES YES YES YES YES YES YES YES

Appendix E Tally of Responses to the Survey Questions Rearranged
1 Parameter SLMC CGH UST UP-PGH LCP PHC VMMC UPHDMC MDH134 5) Measured height YES YES YES YES YES YES YES YES YES135 6) Estimated Height of a patient with limb deformity YES YES YES YES YES NO YES YES YES136 7) Measured weight YES YES YES YES YES YES YES YES YES137 8) Race of patient YES YES YES YES YES YES YES YES YES138 9) Name of referring physician YES YES YES YES YES YES YES YES YES139 10) Vitas signs of patient (BP, CR, RR) prior to test NO NO NO NO NA NO YES YES YES140 Patient Considerations141 1) Symptoms of the patient YES YES YES YES YES YES YES YES YES142 2) Smoking history 143 Duration of smoking (# of pack years) YES YES YES YES YES NO YES YES YES144 Smoking status (current or former) YES YES YES YES YES YES YES YES YES145 # of years stopped YES YES YES NO YES NO YES YES YES146 3) Medicines taken by patient147 Short acting B agonist YES YES YES YES YES NA YES YES NO148 Inhaled long acting B agonist YES YES YES YES NA YES YES NO149 Oral bronchodilator YES YES YES YES YES NA YES YES NO150 Inhaled steroids YES YES NO YES YES NA YES YES NO151 Oral corticosteroids YES NO NO YES YES NA YES YES NO152 Antileukotrienes YES NO NO YES YES NA YES YES NO153 Anti-IgE antagonist NA NO NO NO YES NA YES YES NO154 4) Time the above medications were last taken YES YES YES YES NO YES YES YES NO155 5) History of the following particular symptoms156 Chest or abdominal pain of any cause NA NO YES YES NO YES YES YES YES157 Oral or facial pain exacerbated by mouthpiece YES NO NO NO NO NO YES YES YES158 Stress incontinence NA NO NO NO NO NO YES YES YES159 Dementia or confusional status YES NO NO NO NO NO YES YES YES160 6) Position of the patient while performing the test YES YES NO YES NO NO YES YES NO161 7) Use of restrictive clothing during the test YES NO YES NO NO NO YES YES NO162 8) History of doing particular activities immediately prior to test163 Smoking within 1 hour YES NO YES NO NO NO YES YES YES164 Alcohol intake within 4 hours YES NO YES NO NO NO YES YES YES165 Performing vigourous exercise within 30 mins YES NO YES YES NO NO YES YES YES166 Eating large meals within 2 hours YES NO YES NO NO NO YES YES YES

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

Appendix F: Sample PFT reports from PCCP PFTI

APPENDIX G
Terms Used by PCCP-PFTI in the Interpretation of Spirometry Results 1 Chinese General Hospital
Normal Comments:
– Patient performed the test maximally on standing position. – Nebulization of 5 cc distilled water was given for modified
bronchoprovocation test Interpretation
– Normal spirometry study – Bronchoprovocation showed no reduction in post FEV1 values
Probable Restrictive Ventilatory Defect Comments
– Patient performed the test maximally on standing position. – 1 neb of ventolin was given for post bronchodilator test
Interpretation – Normal FEV1/FVC and FEV1. – Decreased FVC. – There is probable restriction. Suggest lung volume studies if clinically
indicated. – There is no significant response to bronchodilator. – Please correlate clinically.
Obstructive with probable Restrictive Ventilatory Defect Comments
– Patient performed the test maximally on standing position. – 1 neb of ventolin was given for post bronchodilator test
Interpretation – There is moderate obstructive lung defect with significant response to
bronchodilator. – FVC is reduced probably due to obstructive defect and/ or restrictive lung
defect. Suggest lung volume studies if clinically indicated.
2 Lung Center of the Philippines Normal
Comments and Interpretation – Normal spirometry
Obstructive Ventilatory Defect Comments and Interpretation
– Spirometry shows a severe obstructive ventilatory pattern with significant response to bronchodilator
Probable Restrictive Ventilatory Defect Comments and Interpretation
– Spirometry shows a mild restrictive ventilatory pattern. Obstructive with probable Restrictive Ventilatory Defect
Comments and Interpretation – Spirometry shows severe obstructive ventilatory pattern with significant
bronchodilator response with moderate restrictive ventilatory pattern. Suggest post bronchodilator and lung volume studies.
3 Manila Doctors Medical Center Normal
Comments: – FVC and FV1 are normal; FEV1/ FVC ratio is normal – There is no acute bronchodilator response – Able to do 6 seconds test. MVV is normal.
Interpretation: – PFT suggest normal ventilatory pattern – There is no significant bronchodilator response

APPENDIX G
Obstructive Ventilatory Defect Comments
– FVC, FEV1 and FEV1/FVC ratio are decreased. Normal MVV – No airway resistance exam done. DLCO is decreased – There is significant bronchodilator response.
Interpretation – PFT showed severe obstructive ventilatory pattern with significant
bronchodilator response. – There is mild diffusion limitation to CO. – Suggest lung volume study if clinically indicated.
Probable Restrictive Ventilatory Defect Comments
– Spirometry shows low FEB1 and FVC while FEV1/FVC ratio, MVV and flow rates are within normal range.
– There is no significant acute bronchodilator response noted. – Lung volume shows low TLC and RV, DLCO is normal.
Interpretation – PFY is consistent with moderate restrictive ventilatory pattern with normal
DLCO. 4 St. Luke’s Medical Center Quezon City
Normal Comments & Interpretation
– Normal Spirometric Study Obstructive Ventilatory Defect
Comments & Interpretation – There is a mild obstructive lung defect – Suggest post-bronchodilator study if clinically indicated.
Probable Restrictive Ventilatory Defect Comments & Interpretation
– There is no obstructive lung defect. – Post-bronchodilator study showed a 22% improvement in the FEF25-75 – Please correlate clinically
Obstructive with probable Restrictive Ventilatory Defect Comments and Interpretation
– There is moderate obstructive lung defect with significant response to bronchodilator.
– FVC is reduced probably due to underlying obstructive lung defect and or concomitant restrictive defect. Suggest lung volume study if clinically indicated.
– Please correlate clinically. 5 University of Philippines- Philippine General Hospital
Normal Comments and Findings
– The FEV1/FVC, FEV1, FVC, FEF 25-75 values are within normal limits. – There is no scooping of the expiratory curve. – There is no acute bronchodilator response
Interpretation & Recommendation – Normal Spirometry Findings
Obstructive Ventilatory Defect Comments and Findings
– The FEV1/FVC, FEF 25-75, FEV1, FVC values are low. – There is scooping of the expiratory curve – There is an acute bronchodilator response
Interpretation & Recommendation – Spirometric findings are consistent with a severe obstructive ventilatory
defect with acute bronchodilator response. – In view of the smoking history of the patient, he maybe labeled at risk for
COPD.

APPENDIX G
Probable Restrictive Ventilatory Defect Comments and Findings
– The FEV1/FVC is normal – FEV1& FVC values are low. – There is no significant acute bronchodilator effect. – There is no scooping in the expiratory curve.
Interpretation & Recommendation – Spirometric findings are consistent with a moderate restriction in the
volume expansion of the lungs. – Suggest total lung volume studies with DLCO and or clinical correlation for
further evaluation especially if a restrictive lung disease secondary to ILD is considered.
6 Philippine Heart Center Normal
Comments & Interpretation – Normal spirometry study
Obstructive Ventilatory Defect (To be submitted) Probable Restrictive Ventilatory Defect
Comments & Interpretation – FEV1/FVC ratio is normal. FEV1 and FVC are reduced indicative of mild
restriction of the volume excursion of the lung. Obstructive with probable Restrictive Ventilatory Defect
Comments & Interpretation – FEV1/FVC ratio, FEV1 and FVC are low indicative of severe obstructive
lung defect. – Post-bronchodilator study showed no significant reversibility. – FVC is reduced probably due to underlying obstructive defect and/ or
concomitant restrictive lung defect. Suggest lung volume studies if clinical indicated.
7 University of Perpetual Health Medical Center Normal
Interpretation – Normal Spirometry
Obstructive Ventilatory Defect Interpretation
– Severe obstructive ventilatory pattern with significant post bronchodilator response.
Probable Restrictive Ventilatory Defect Interpretation
– Restrictive Ventilatory Pattern – Please Correlate Clinically – Suggest Body Phlethysmography
Obstructive with probable Restrictive Ventilatory Defect Interpretation
– Combined restrictive and obstructive ventilatory pattern due to low FVC and FEF25-75 in the background of inadequate of expiratory maneuver
– Suggest body phlethysmography. – Please correlate clinically.
8 Veterans Memorial Medical Center Normal
Comments & Interpretation – FEV1/FVC is normal. FEV1 is normal. FVC is normal. – FEV1 has no significant improvement after bronchodilator administration.
FVC has no significant improvement after bronchodilator administration. – Normal Spirometric Studies

APPENDIX G
Obstructive Ventilatory Defect Comments & Interpretation
– FEV1/FVC is low. FEV1 is low and there is an exaggerated concavity in the distal portion of the expiratory limb.
– FVC is low. FEV1 has significant improvement after bronchodilator administration. FVC has no significant improvement after post bronchodilator studies. These findings are suggestive of Moderately Obstructive Ventilatory Defect. Post bronchodilator study showed a significant degree of reversibility.
Probable Restrictive Ventilatory Defect Comments & Interpretation
– FEV/FVC is normal. FEV1 is normal. FVC is low. FEV1 has no significant improvement after bronchodilator administration. FVC has no significant improvement after bronchodilator administration.
– These findings are suggestive of a restrictive ventilatory impairment – For lung volume studies if clinically indicated
9 University of Santo Tomas Hospital Normal
Interpretation – Based on FEV1/FVC, FEV1, FVC there is no ventilatory defect – The predicted values are based on Morris and Polgar. Kindly correlate
clinically. Obstructive Ventilatory Defect
Interpretation – Based on a low FEV1/FVC and FEV1, there is a severe obstructive
ventilatory defect. – Based on a 51% change in FEV1, there is a good response to
bronchodilator – The predicted values are based on Morris and Polgar. Kindly correlate
clinically. Probable Restrictive Ventilatory Defect
Interpretations – Based on the FEV1/FVC ratio there is no obstructive ventilatory defect. – The FVC is low which maybe due to a restrictive ventilatory defect. For
verification, we suggest lung volume studies. – The predicted values are based on Morris Polgar. Kindly correlate with
clinical data. Obstructive with probable Restrictive Ventilatory Defect
– Based on the low FEV1/FVC and FEV1, there is a moderately severe obstructive ventilatory defect. Based on the 12% (120ml) change in FEV1, there is a poor response to bronchodilator. The FVC is low which maybe due to a concomitant restrictive ventilatory defect or RV hyperinflation. To verify the cause of the low FVC we suggest a lung volume study. The predicted values are based on Morris Polgar. Kindly correlate with clinical data.

APPENDIX H Definition of Terms/ Abbreviations
Definition of Terms
Closed Circuit Method Spirometry Testing: method of conducting spirometry wherein the volume is measured indirectly by a device which either measure a pressure drop across a fixed resistance or flow via means of a propeller.
Most Reliable Spirometry Parameters (MRSP): refers to the spirometry parameters used in the American Thoracic Society – European Respiratory Society Task Force on Lung Function Testing suggested algorithm for the interpretation of lung function testing. These parameters are FEV1/FVC, FEV1 and FVC.
Open Circuit Method Spirometry Testing: method of conducting spirometry wherein the volume is measured by a wedge bellows, bell, water seal or rolling seal cylinder/ piston.
Other Spirometry Parameters (OSP): refers the spirometry parameters not used in the American Thoracic Society – European Respiratory Society Task Force on Lung Function Testing suggested algorithm for the interpretation of lung function testing. These parameters are FEV1/FVC, FEV1 and FVC.
Simple spirometry: a type spirometry testing wherein only a pre-bronchodilator study is done.
Spirometry with post-bronchodilator study: a type of spirometry testing wherein a pre-bronchodilator and post bronchodilator study is done.
Abbreviations
ATS-ERS-TFLFT: American Thoracic Society Task Force on Lung Function Testing
CAO: Central airway obstruction DATS: Philippine College of Chest Physician Council on Diagnostics and
Therapeutic FEV1: Forced expiratory volume in one second FEF 25-75: Mean forced expiratory flow between 25% and 75% of FVC FEF50: Instantaneous expiratory flow when 50% of the FVC has been
expired FEF75: Instantaneous expiratory flow when 75% of the FVC has been
expired FVC: Forced vital capacity FVC6: Forced expiratory volume in 6 seconds MIF50: Maximum inspiratory flow at 50% of the FVC MEF50: Maximum expiratory flow at 50% of the FVC MRSP: Most reliable spirometry parameters MVV: Maximum voluntary ventilation OSP: Other spirometry parameters PCCP PFTI: Philippine College of Chest Physicians Pulmonary Fellowship
Training Institution PEF: Peak expiratory flow PEFR: Peak expiratory flow rate UAO: Upper airway obstruction

Appendix I
Procedural Steps for Spirometry testing (using closed circuit method)
o Calibrate the spirometer and record o Explain the test o Secure a written consent o Answer the PCCP Spirometry Testing Information Sheet (Appendix J) o Measure weight and height without shoes o Wash hands o Instruct and demonstrate the test to the subject, this includes
Proper posture Rapid and complete inhalation Proper use of mouthpiece Rapid and maximally forceful expiration
o Perform maneuver Assist the to assume the correct posture Attach the nose clip Place the mouthpiece and ask patient to close lips around the
mouthpiece Ask the patient to inhale completely and rapidly with a pause of 0.1 s at
TLC Instruct the patient to exhale maximally until no more air can be expelled
while maintaining an upright posture Repeat instructions as necessary, coaching vigorously Repeat the test until any of the following
The reproducibility criteria is met (see below) The patient cannot continue A maximum of 8 maneuvers is obtained
Save at least the best 3 spirograms o Completes the answering of the PCCP Spirometry Testing information sheet o Spirogram Reproducibility Criteria
There is at least 3 acceptable spirogram The two largest values of FVC are within 0.150 L of each other The two largest values of FEV1 are within 0.150 L of each other
o Spirogram Acceptability Criteria o It is free from artifacts
Cough during the first second of exhalation Glottis closure that influences the measurement Early termination or cut-off Effort that is not maximal throughout Leak Obstructed mouthpiece
o It shows a good start Extrapolated volume 0.5% of FVC or 0.15 L, whichever is greater
o It shows satisfactory exhalation Duration of 6 seconds A plateau in the volume–time curve

APPENDIX J
PCCP Council of Diagnostic & Therapeutic Spirometry Testing Information Sheet 1. Name: __________________________________Age: _________
2. Gender: _________ Height: ____________ Weight: ______________
3. Race of patient: ___________________
4. Date of procedure: _________________Time of procedure: ___________
5. Room temperature: __________Atmospheric pressure: _________
6. Name of referring physician: __________________________
7. Smoking History: Status (Never, Current or Previous): __________________
Pack years: __________________ Last Intake: __________________
8. Working Diagnosis/ Reason for Testing: ____________________
9. Date of Previous Spirometry Testing: _________________
10. Conditions that may influence the results (Place a check if present or x if absent)
Chest or abdominal pain of any cause
Oral or facial pain exacerbated by mouthpiece
Stress incontinence
Dementia or confusional status
Non standing position of the patient while performing the test
Use of restrictive clothing during the test
Alcohol/ Caffeinated drink intake within 4 hours prior to testing
Vigorous exercise within 30 mins prior to testing
Eating large meals within 2 hours prior to testing
11. Intake of the following respiratory drugs prior to testing
Medicine Trade Name Dosage Last Intake (Hours prior to testing)
Salbutamol
Terbutaline
Formoterol
Indacaterol
Salmeterol
Ipratropium Bromide
Tioptropium
Methylxanthines
Formoterol/
Budesonide
Salmeterol/
Fluticasone
Oral Steroid
Roflumilast
Please use the back page for additional listing of medicines if needed
12. Were the ATS/ERS reproducible criteria satisfied? _________________________
_____________________________________________________________________

Appendix K: Forms Used for Voting of the Statements/ Recommendations - 1 -
Name of Institution/ Chapter/ Key Opinion Leader: ____________________________ Name of Person Answering in behalf of Institution/ Chapter: ____________________ For each of the 51 recommendations, kindly write the letter corresponding to your answer/ vote. The choices are
A. We disagree with the recommendation. B. We agree with recommendation and are, in fact, already instituting this. C. We agree with the recommendation, and we will institute measures to implement
this. D. We agree with the recommendation but will have a hard time implementing this in the
near future. _____ 1 (R1-1) Spirometry testing using the closed circuit technique should be
performed based on the standards set by the ATS-ERS-TFLFT (1). Part of the
procedure includes the answering of the “PCCP DATS Spirometry Testing
Information Sheet”. Kindly see appendix I & J.
_____ 2 (R1-2) A referring physician can either request any of the following types of
spirometry testing: simple spirometry, spirometry with post bronchodilator study
and simple spirometry study with possible post bronchodilator study if initial
result is abnormal
_____ 3 (R1-3) In a situation wherein the referring physician requested only a simple
spirometry and it showed abnormal results, the technician in coordination with
doctor (interpreter of the results) should try to ask permission from the
referring physician to proceed in performing a post bronchodilator study while
the patient is still in the test site.
_____ 4 (R2-1) Daily instrument calibration should be done.
_____ 5 (R2-2) The interpreter (lab medical director or pulmonary consultant on deck)
should give a feedback to the technician with regards the quality of the test.
_____ 6 (R2-3) A log book should be maintained. It should contain the following: daily
calibration results, anomalous events or problems encountered with the system
and feedback of the interpreter to the technician.
_____ 7 (R3-1) The following should be measured and reported FEV1/ FVC, FVC and
FEV1.
_____ 8 (R3-2) If the spirometry machine is capable, the following should be measured
and reported (in order of decreasing importance): PEFR, FEF 25-75, FEF 75,
MIF50/ MEF50, FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50
_____ 9 (R4-1) Test result selection should be based on the recommendations set by
the ATS-ERS-TFLFT (1).
_____ 10 (R5-1) In the spirometry report, there should be 3 sections for the interpretation
of the results: technician’s comments, interpreter’s comments and final
interpretation.
_____ 11 (R5-2) There is no need to give a clinical correlation.

Appendix K: Forms Used for Voting of the Statements/ Recommendations - 2 -
For each of the 51 recommendations, kindly write the letter corresponding to your answer/ vote. The choices are
A. We disagree with the recommendation. B. We agree with recommendation and are, in fact, already instituting this. C. We agree with the recommendation, and we will institute measures to implement
this. D. We agree with the recommendation but will have a hard time implementing this in the
near future.
_____ 12 (R6-1) The spirometry report should contain a section on general data which
contains the following information: name of patient, age of patient, gender of
patient, measured height, measured weight, race of patient, date of procedure,
time of procedure, room temperature at time of testing, room atmospheric
pressure at time of testing, name of referring physician, name of the laboratory
and phone number of laboratory
_____ 13 (R7-1) The report should contain a section for technician comments.
_____ 14 (R7-2) The technician comments should state if the test done satisfies the
ATS-ERS-TFLFT (1) reproducibility criteria. If not, it should state which of the
criteria was not satisfied.
_____ 15 (R7-3) The technician comments should state if conditions that may alter the
results are present or not.
_____ 16 (R7-4) Technician comments should state if the patient is on respiratory drug
and if so when was the last intake.
_____ 17 (R7-5) Technician comments should state the patients smoking history
particular the pack years and the last time when the patient smoked cigarettes.
_____ 18 (R8-1) In the interpretation of the results, the report should use the phrase
“ventilatory defect” (not lung defect or ventilatory pattern).
_____ 19 (R9-1) Spirometry results should be interpreted based on the ATS-ERS-TFLFT
suggested algorithm.
_____ 20 (R10-1) The best trial flow volume (pre and post-bronchodilator if done) should
be part of the spirometry report.
_____ 21 (R10-2) In cases of possible upper airway obstruction interpretation, all trials
flow volume loop should be reported. If the spirometry software is not capable,
reproducibility of the flow volume loop should be mentioned in the interpreter’s
comments.
_____ 22 (R10-3) Slowing down of the terminal portion of spirogram should be described
as “exaggerated concavity in the distal portion of the expiratory limb of the flow
volume loop”. Use of the term “scooping” is discouraged.
_____ 23 (R10-4) In cases wherein the interpretation uses any of the following: flow
volume loop’s configuration, FEF25-75 and “other spirometry parameters”, it
should be stated that these parameters are suggestive but not definitive. Use
of the term “compatible” is discouraged.

Appendix K: Forms Used for Voting of the Statements/ Recommendations - 3 -
For each of the 51 recommendations, kindly write the letter corresponding to your answer/ vote. The choices are
A. We disagree with the recommendation. B. We agree with recommendation and are, in fact, already instituting this. C. We agree with the recommendation, and we will institute measures to implement
this. D. We agree with the recommendation but will have a hard time implementing this in the
near future.
_____ 24 (R11-1) Grading of severity should be based on the criteria set by ATS-ERS-
TFLFT (2).
_____ 25 (R11-2) FEV1% predicted (post bronchodilator value if available) is used both
for obstructive and restrictive ventilatory defect.
_____ 26 (R12-1) In the spirometry report, all parameters should have corresponding
actual value (in BTPS), predicted value and % predicted.
_____ 27 (R12-2) If the spirometer software is capable (optional), the value
corresponding to the 95% CI of the predicted value should be written in the
report.
_____ 28 (R12-3) If the spirometer software is capable (optional), values < 5th percentile
of the predicted should be flagged down (either a change of color or marked).
If the spirometer software is not capable, it is encouraged that the technician or
interpreter derived this value by manual computation or use an online
calculator at http://www.dynamicmt.com/dataform3.html.
_____ 29 (R12-4) The cut-off value for the FEV1/FVC ratio should be <5th percentile of
predicted value. If not available, it should stated in the interpreter’s comments
what cut off value was used for the lower limit of normality.
_____ 30 (R12-5) Cut off value for the lower limit of normality should be stated in the
interpreter’s comments.
_____ 31 (R13-1) Performance of a post-bronchodilator study should be done based on
the recommendations of ATS-ERS-TFLFT (2).
_____ 32 (R13-2) Interpretation of response to bronchodilator should be based on the
criteria set by the ATS-ERS-TFLFT (2).
_____ 33 (R13-3) FEF 25-75 should not be used in the interpretation of the post
bronchodilator response.
_____ 34 (R13-4) To standardize the semantics, response to bronchodilator will either be
labeled as “significant or no significant response to bronchodilator” {as used by
the ATS-ERS-TFLFT (2)}. Uses of other terms such as “poor or good response
to bronchodilator” are discouraged.
_____ 35 (R14-1) Interpretation should include suggestion/s on need for additional test if
warranted.
_____ 36 (R15-1) In the section on “Interpreter’s Comments” the report should state what
reference equation was used in the interpretation of the results. Statement on
the need to correlate clinically should be written in the final interpretation.

Appendix K: Forms Used for Voting of the Statements/ Recommendations - 4 -
For each of the 51 recommendations, kindly write the letter corresponding to your answer/ vote. The choices are
A. We disagree with the recommendation. B. We agree with recommendation and are, in fact, already instituting this. C. We agree with the recommendation, and we will institute measures to implement
this. D. We agree with the recommendation but will have a hard time implementing this in the
near future.
_____ 37 (R15-2) A research study will be conducted by the Council of Diagnostics &
Therapeutics to determine which reference equation is best fitted for the local
Filipino population.
_____ 38 (R16-1) In the reports section on “Interpreter’s Comments”, it should be stated
if the test satisfies the reproducibility criteria set by the ATS-ERS-TFLFT (1) or
not.
_____ 39 (R16-2) It the test does not satisfy one of the acceptability or reproducibility
criteria, it should state the consequences of this deficiency in the parameters.
_____ 40 (R17-1) The spirometry report should contain at least, the pre (and post-
bronchodilator if done) best trial flow volume loop/s
_____ 41 (R17-2) The spirometry report should contain all trials flow volume loops if an
interpretation of CAO or UAO made. If the spirometry software is not capable,
the reproducibility of the flow volume loop should be stated in the section on
“Interpreter’s Comments”.
_____ 42 (R18-1) The spirometry report should contain the measured parameters tabular
graph.
_____ 43 (R18-2) The first 3 rows of should be allotted for the MRSP in the following
order: FEV1/FVC, FVC and FEV1.
_____ 44 (R18-3) The succeeding rows maybe be allotted for the “other parameters” in
the following order of priority: PEFR, FEF 25-75, FEF 75, MIF50/ MEF50,
FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50
_____ 45 (R18-4) In the tabular graph, each parameter should have its corresponding
actual values (pre & post if done), predicted, 95% confidence interval limit (if
the spirometry software is capable), % predicted (pre & post if done) and %
change from baseline of post-bronchodilator measurement.
_____ 46 (R18-5) In the tabular graph (if the spirometry software is capable), each
parameter below the 5th percentile should be flagged down.
_____ 47 (R19-1) The report should contain a section for the interpreter’s comments (IC)
of the results.
_____ 48 (R19-2) The IC section should state if the test satisfied the ATS-ERS-TFLFT
(1) reproducibility criteria. If the test did not satisfy the criteria, the interpreter
should state the consequences of this deficiency.
_____ 49 (R19-3) The section should contain the basis for the interpretation. Specifically
it should apply, the ATS-ERS-TFLFT (2) interpretation algorithm, criteria for
severity and response to bronchodilator

Appendix K: Forms Used for Voting of the Statements/ Recommendations - 5 -
For each of the 51 recommendations, kindly write the letter corresponding to your answer/ vote. The choices are
A. We disagree with the recommendation. B. We agree with recommendation and are, in fact, already instituting this. C. We agree with the recommendation, and we will institute measures to implement
this. D. We agree with the recommendation but will have a hard time implementing this in the
near future.
_____ 50 (R20-1) The spirometry report should contain a section for the final
interpretation (FI) of the results.
_____ 51 (R20-2) The FI should contain the following information: presence or absence
of obstructive ventilatory defect and severity if present, presence or absence of
probable restrictive ventilatory defect and severity if present, positive or
negative response to bronchodilator if done, suggestion for specific additional
test if indicated, a generic sentence “Please correlate results with patient’s
clinical data.” and printed name plus signature of the interpreter/s

Appendix L
List of Voters
Philippine College of Chest Physicians Accredited Training Institutions
1. Chinese General Hospital and Medical Center (CGH) 2. Chong Hua Hospital (CHH) 3. Lung Center of the Philippines (LCP) 4. Makati Medical Center (MMC) 5. Manila Doctors Hospital (MDH) 6. Philippine Heart Center (PHC) 7. St. Luke’s Medical Center (SLMC) 8. University of Perpetual Help Dalta Medical Center (UPHM) 9. University of the Philippines - Philippine General Hospital (UP-PGH) 10. University of Santo Tomas Hospital (UST) 11. Veterans Memorial Medical Center (VMMC)
Philippine College of Chest Physicians Chapters
1. Southern Tagalog 2. Northern Mindanao 3. Negros 4. Mindanao
Key Opinion Leaders
1. Dr. Camilo Roa 2. Dr. Jennifer Wi 3. Dr. Ric Zotomayor

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R1-1) Spirometry testing using the closed circuit technique should be performed based on the standards set by the ATS-ERS-TFLFT (very good consensus)
B B B B B C B C B B B B B B B B D B
(R1-2) A referring physician can either request any of the following types of spirometry testing: simple spirometry, spirometry with post bronchodilator study and simple spirometry study with possible post bronchodilator study if initial result is abnormal. (perfect consensus)
B B B B C B B B B B B C B B B B C B

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R1-3) In a situation wherein the referring physician requested only a simple spirometry and it showed abnormal results, the technician in coordination with doctor (interpreter of the results) should try to ask permission from the referring physician to proceed in performing a post bronchodilator study while the patient is still in the test site. (very good consensus)
C B B B C C B B B C B C B B C A C B
(R2-1) Daily instrument calibration should be done. (very good consensus)
B B C B B B B B B B D B B B A B D B
(R2-2) The interpreter (lab medical director or pulmonary consultant on deck) should give a feedback to the technician with regards the quality of the test. (perfect consensus)
B B B B B B B B B C B B B B C B B C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R2-3) A log book should be maintained. It should contain the following: daily calibration results, anomalous events or problems encountered with the system and feedback of the interpreter to the technician. (very good consensus)
B B C B B B B C B C D C B B C B C B
(R3-1) The following should be measured and reported FEV1/ FVC, FVC and FEV1. (perfect consensus)
B B B B B B B B B B B B B B B B B B
(R3-2) If the spirometry machine is capable, the following should be measured and reported (in order of decreasing importance): PEFR, FEF 25-75, FEF 75, MIF50/ MEF50, FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50 (very good consensus)
B O ANSW C C B C B C B C B B B B B B B B

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R4-1) Test result selection should be based on the recommendations set by the ATS-ERS-TFLFT (1). (perfect consensus)
B B B B B B B B B C B B B B B B B B
(R5-1) In the spirometry report, there should be 3 sections for the interpretation of the results: technician’s comments, interpreter’s comments and final interpretation. (perfect consensus)
C C C B B C C C C C B C B B B B C C
(R5-2) There is no need to give a clinical correlation. (good consensus)
B B B B A O ANSW B B B A B A B B B A A A

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R6-1) The spirometry report should contain a section on general data which contains the following information: name of patient, age of patient, gender of patient, measured height, measured weight, race of patient, date of procedure, time of procedure, room temperature at time of testing, room atmospheric pressure at time of testing, name of referring physician, name of the laboratory and phone number of laboratory (very good consensus)
B B C C C C B B B B C B C C B C C
(R7-1) The report should contain a section for technician’s comments. It should state the indication for doing the test and the information about previous spirometry testing. (very good consensus)
C C D B B B C C C C B C B C B B C C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R7-2) The technician comments should state if the test done satisfies the ATS-ERS-TFLFT (1) reproducibility criteria. If not, it should state which of the criteria was not satisfied. (perfect consensus)
C B B B C C B C B C B C B C C C C C
(R7-3) The technician’s comments should state if conditions that may alter the results are present or not. (perfect consensus)
C C B B B C B C B C B C B C C C C C
(R7-4) Technician’s comments should state if the patient is on respiratory drug and if so when was the last intake. (perfect consensus)
C C C B B B B C B C B B B B B B C B
(R7-5) Technician’s comments should state the patients smoking history particularly the pack years and the last time when the patient smoked cigarettes. (perfect consensus)
C B C B C B B C B C B C B B C B C C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R8-1) In the interpretation of the results, the report should use the phrase “ventilatory defect” (not lung defect or ventilatory pattern). (very good consensus)
B C B C B B B C B C B B B C B A B C
(R9-1) Spirometry results should be interpreted based on the ATS-ERS-TFLFT suggested algorithm. (very good consensus)
B B B B B B C B C B B B D B B C B
(R10-1) The best trial flow volume (pre and post-bronchodilator if done) should be part of the spirometry report. (perfect consensus)
B B B B B B B B B B B B B B B B C B
(R10-2) In cases of possible upper airway obstruction interpretation, all of the trials flow volume loop should be reported. If the spirometry software is not capable, reproducibility of the flow volume loop should be mentioned in the interpreter’s comments. (very good consensus)
C B C C C B C C C C B B B C B B D C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R10-3) Slowing down of the terminal portion of spirogram should be described as “exaggerated concavity in the distal portion of the expiratory limb of the flow volume loop”. Use of the term “scooping” is discouraged. (perfect consensus)
C B B C C C B C C C B C B C C C C C
(R10-4) In cases wherein the interpretation uses any of the following: flow volume loop’s configuration, FEF25-75 and “other spirometry parameters”, it should be stated that these parameters are suggestive but not definitive. Use of the term “compatible” is discouraged. (very good consensus)
B B C C C C B C C C B B B D B B C B
(R11-1) Grading of severity should be based on the criteria set by ATS-ERS-TFLFT. (perfect consensus)
B B B B B B B B B B B B B B B B C B

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R11-2) FEV1% predicted (post bronchodilator value if available) is used both for obstructive and restrictive ventilatory defect. (perfect consensus)
B B B B B B B B B B B B B B B B B
(R12-1) In the spirometry report, all parameters should have corresponding actual value (in BTPS), predicted value and % predicted. (perfect consensus)
B B B B B B B B B B B B B C C B B B
(R12-2) If the spirometer software is capable (optional), the value corresponding to the 95% CI of the predicted value should be written in the report. (very good consensus)
B B B C C C C C B C B C B C C/B B D C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R12-3) If the spirometer software is capable (optional), values < 5th percentile of the predicted should be flagged down (either a change of color or marked). If the spirometer software is not capable, it is encouraged that the technician or interpreter derives this value by manual computation or uses an online calculator at http://www.dynamicmt.com/dataform3.html. (good consensus)
B B D D D A D D B C D C B C C D D C
(R12-4) The cut-off value for the FEV1/FVC ratio should be <5th percentile of predicted value. If not available, it should be stated in the interpreter’s comments what cut off value was used for the lower limit of normality. (good consensus)
B C C C D A C D C C B C B C C/B D D C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R12-5) Cut off value for the lower limit of normality should be stated in the interpreter’s comments. (very good consensus)
B C C C D A C C C C B C B C B/C D C C
(R13-1) Performance of a post-bronchodilator study should be done based on the recommendations of ATS-ERS-TFLFT (2). (perfect consensus)
B B B B B B B B B C B B B B B B C B
(R13-2) Interpretation of response to bronchodilator should be based on the criteria set by the ATS-ERS-TFLFT. (perfect consensus)
B B B B B B B ANSW B C B B B B B B C B
(R13-3) FEF 25-75 should not be used in the interpretation of the post bronchodilator response. (perfect consensus)
C B B B B C B B B C B B B C B B C C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R13-4) To standardize the semantics, response to bronchodilator will either be labeled as “significant or no significant response to bronchodilator” {as used by the ATS-ERS-TFLFT (2)}. Uses of other terms such as “poor or good response to bronchodilator” are discouraged. (perfect consensus)
B B B B B B B B C B B B B C C/B B B B
(R14-1) Interpretation should include suggestion/s on need for additional test if warranted. (very good consensus)
B B B B B B B B B B B B B D C/B B B B
(R15-1) In the section on “Interpreter’s Comments” the report should state what reference equation was used in the interpretation of the results. Statement on the need to correlate clinically should be written in the final interpretation (very good consensus).
C C C C C A B C B C B C B D A/B A C C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R15-2) A research study will be conducted by the Council of Diagnostics & Therapeutics to determine which reference equation is best fitted for the local Filipino population. (For this item, kindly just state of your agree or disagree) (very good consensus)
Y/A Y/A Y/A Y/A Y/A N/D Y/A Y/A Y/A Y/A Y/A Y/A Y/A Y/A Y/A Y/A Y/A
(R16-1) In the reports section on “Interpreter’s Comments”, it should be stated if the test satisfies the reproducibility criteria set by the ATS-ERS-TFLFT (1) or not. (very good consensus)
C C C C C C B C B C B B B B A B C C
(R16-2) It the test does not satisfy one of the acceptability or reproducibility criteria, it should state the consequences of this deficiency in the parameters. (very good consensus)
C B C C D C B C B C B B B D B B C C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R17-1) The spirometry report should contain at least, the pre (and post-bronchodilator if done) best trial flow volume loop/s. (perfect consensus)
B B B B B B B B B B B B B B B B C B
(R17-2) The spirometry report should contain the flow volume loops of all trials, if an interpretation of CAO or UAO made. If the spirometry software is not capable, the reproducibility of the flow volume loop should be stated in the section on “Interpreter’s Comments”. (very good consensus)
C B C C B C D B B C B B B C A/C C D D
(R18-1) The spirometry report should contain the measured parameters tabular graph. (very good consensus)
B B D B B C B B B B B B B B B B D B
(R18-2) The first 3 rows of the tabular graph should be allotted for the MRSP in the following order: FEV1/FVC, FVC and FEV1. (very good consensus)
B C D C B C B C C C B C B B B C B C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R18-3) The succeeding rows maybe be allotted for the “other parameters” in the following order of priority: PEFR, FEF 25-75, FEF 75, MIF50/ MEF50, FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50. (very good consensus)
B C D C B B B C C C B C B B B C B C
(R18-4) In the tabular graph, each parameter should have its corresponding actual values (pre & post if done), predicted, 95% confidence interval limit (if the spirometry software is capable), % predicted (pre & post if done) and % change from baseline of post-bronchodilator measurement. (perfect consensus)
B B B B B B B C B B B B B B B B B B
(R18-5) In the tabular graph (if the spirometry software is capable), each parameter below the 5th percentile should be flagged down. (good consensus)
B B D C D C C C B B D D B B C B C

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R19-1) The report should contain a section for the interpreter’s comments (IC) of the results. (perfect consensus)
B C B C B B B C B B B B B B B B B B
(R19-2) The IC section should state if the test satisfied the ATS-ERS-TFLFT (1) reproducibility criteria. If the test did not satisfy the criteria, the interpreter should state the consequences of this deficiency.(very good consensus)
C C C C D C C C B C B B D B C C B B
(R19-3) The IC section should also contain the basis for the interpretation. Specifically it should apply, the ATS-ERS-TFLFT (2) interpretation algorithm, criteria for severity and response to bronchodilator. (very good consensus)
C C B C B B C C C C B B D B C B B B
(R20-1) The spirometry report should contain a section for the final interpretation (FI) of the results. (perfect consensus)
B B B B B B B B B B B B B B B B B B

Appendix M: Tally of Votes
SLMC CGH VMMC LCP UP-PGH MMC CHH MDH UST PHC UPHM Dr. Roa Dr. Zotomayor Dr. Wi Mindanao S. Tagalog N. Mindanao Negros
(R20-2) The FI should contain the following information: presence or absence of obstructive ventilatory defect and severity if present, presence or absence of probable restrictive ventilatory defect and severity if present, significant or no significant response to bronchodilator if done, suggestion for specific additional test if indicated, a generic sentence “Please correlate results with patient’s clinical data.” and printed name plus signature of the interpreter/s. (very good consensus)
B B B B B B B C B C B B B B B B B

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R5-2) There is no need to give a clinical correlation. (good consensus) 6 11 64.7 0.0 G(R12-3) If the spirometer software is capable (optional), values < 5th
percentile of the predicted should be flagged down (either a change of color or marked). If the spirometer software is not capable, it is encouraged that the technician or interpreter derives this value by manual computation or uses an online calculator at http://www.dynamicmt.com/dataform3.html. (good consensus)
1 4 5 8 94.4 47.1 G
(R12-4) The cut-off value for the FEV1/FVC ratio should be <5th
percentile of predicted value. If not available, it should be stated in the interpreter’s comments what cut off value was used for the lower limit of normality. (good consensus)
1 3 10 4 94.4 23.5 G
(R18-5) In the tabular graph (if the spirometry software is capable), each parameter below the 5th percentile should be flagged down. (good consensus)
7 6 4 100.0 23.5 G
(R1-2) A referring physician can either request any of the following types of spirometry testing: simple spirometry, spirometry with post bronchodilator study and simple spirometry study with possible post bronchodilator study if initial result is abnormal. (perfect consensus)
15 3 100.0 0.0 P
(R2-2) The interpreter (lab medical director or pulmonary consultant on deck) should give a feedback to the technician with regards the quality of the test. (perfect consensus)
15 3 100.0 0.0 P
(R3-1) The following should be measured and reported FEV1/ FVC, FVC and FEV1. (perfect consensus)
18 100.0 0.0 P
(R4-1) Test result selection should be based on the recommendations set by the ATS-ERS-TFLFT (1). (perfect consensus)
17 1 100.0 0.0 P
(R5-1) In the spirometry report, there should be 3 sections for the interpretation of the results: technician’s comments, interpreter’s comments and final interpretation. (perfect consensus)
7 11 100.0 0.0 P

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R7-2) The technician comments should state if the test done satisfies the ATS-ERS-TFLFT (1) reproducibility criteria. If not, it should state which of the criteria was not satisfied. (perfect consensus)
7 11 100.0 0.0 P
(R7-3) The technician’s comments should state if conditions that may alter the results are present or not. (perfect consensus)
7 11 100.0 0.0 P
(R7-4) Technician’s comments should state if the patient is on respiratory drug and if so when was the last intake. (perfect consensus)
12 6 100.0 0.0 P
(R7-5) Technician’s comments should state the patients smoking history particularly the pack years and the last time when the patient smoked cigarettes. (perfect consensus)
9 9 100.0 0.0 P
(R10-1) The best trial flow volume (pre and post-bronchodilator if done) should be part of the spirometry report. (perfect consensus)
17 1 100.0 0.0 P
(R10-3) Slowing down of the terminal portion of spirogram should be described as “exaggerated concavity in the distal portion of the expiratory limb of the flow volume loop”. Use of the term “scooping” is discouraged. (perfect consensus)
5 13 100.0 0.0 P
(R11-1) Grading of severity should be based on the criteria set by ATS-ERS-TFLFT. (perfect consensus)
17 1 100.0 0.0 P
(R11-2) FEV1% predicted (post bronchodilator value if available) is used both for obstructive and restrictive ventilatory defect. (perfect consensus)
17 100.0 0.0 P
(R12-1) In the spirometry report, all parameters should have corresponding actual value (in BTPS), predicted value and % predicted. (perfect consensus)
16 2 100.0 0.0 P
(R13-1) Performance of a post-bronchodilator study should be done based on the recommendations of ATS-ERS-TFLFT (2). (perfect consensus)
16 2 100.0 0.0 P

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R13-2) Interpretation of response to bronchodilator should be based on the criteria set by the ATS-ERS-TFLFT. (perfect consensus)
15 2 100.0 0.0 P
(R13-3) FEF 25-75 should not be used in the interpretation of the post bronchodilator response. (perfect consensus)
12 6 100.0 0.0 P
(R13-4) To standardize the semantics, response to bronchodilator will either be labeled as “significant or no significant response to bronchodilator” {as used by the ATS-ERS-TFLFT (2)}. Uses of other terms such as “poor or good response to bronchodilator” are discouraged. (perfect consensus)
15 3 100.0 0.0 P
(R17-1) The spirometry report should contain at least, the pre (and post-bronchodilator if done) best trial flow volume loop/s. (perfect consensus)
17 1 100.0 0.0 P
(R18-4) In the tabular graph, each parameter should have its corresponding actual values (pre & post if done), predicted, 95% confidence interval limit (if the spirometry software is capable), % predicted (pre & post if done) and % change from baseline of post-bronchodilator measurement. (perfect consensus)
17 1 100.0 0.0 P
(R19-1) The report should contain a section for the interpreter’s comments (IC) of the results. (perfect consensus)
15 3 100.0 0.0 P
(R20-1) The spirometry report should contain a section for the final interpretation (FI) of the results. (perfect consensus)
18 100.0 0.0 P
(R1-1) Spirometry testing using the closed circuit technique should be performed based on the standards set by the ATS-ERS-TFLFT (very good consensus)
15 2 1 100.0 5.6 VG
(R1-3) In a situation wherein the referring physician requested only asimple spirometry and it showed abnormal results, the technician in coordination with doctor (interpreter of the results) should try to ask permission from the referring physician to proceed in performing a post bronchodilator study while the patient is still in the test site. (very good consensus)
1 10 7 94.4 0.0 VG

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R2-1) Daily instrument calibration should be done. (very good consensus)
1 14 1 2 94.4 11.8 VG
(R2-3) A log book should be maintained. It should contain the following: daily calibration results, anomalous events or problems encountered with the system and feedback of the interpreter to the technician. (very good consensus)
11 6 1 100.0 5.6 VG
(R3-2) If the spirometry machine is capable, the following should be measured and reported (in order of decreasing importance): PEFR, FEF 25-75, FEF 75, MIF50/ MEF50, FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50 (very good consensus)
12 5 94.4 0.0 VG
(R6-1) The spirometry report should contain a section on general data which contains the following information: name of patient, age of patient, gender of patient, measured height, measured weight, race of patient, date of procedure, time of procedure, room temperature at time of testing, room atmospheric pressure at time of testing, name of referring physician, name of the laboratory and phone number of laboratory (very good consensus)
8 9 94.4 0.0 VG
(R7-1) The report should contain a section for technician’s comments. It should state the indication for doing the test and the information about previous spirometry testing. (very good consensus)
7 10 1 100.0 5.6 VG
(R8-1) In the interpretation of the results, the report should use the phrase “ventilatory defect” (not lung defect or ventilatory pattern). (very good consensus)
1 11 6 94.4 0.0 VG
(R9-1) Spirometry results should be interpreted based on the ATS-ERS-TFLFT suggested algorithm. (very good consensus)
13 3 1 100.0 5.9 VG
(R10-2) In cases of possible upper airway obstruction interpretation, all of the trials flow volume loop should be reported. If the spirometry software is not capable, reproducibility of the flow volume loop should be mentioned in the interpreter’s comments. (very good consensus)
7 10 1 100.0 5.6 VG

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R10-4) In cases wherein the interpretation uses any of the following: flow volume loop’s configuration, FEF25-75 and “other spirometry parameters”, it should be stated that these parameters are suggestive but not definitive. Use of the term “compatible” is discouraged. (very good consensus)
9 8 1 100.0 5.6 VG
(R12-2) If the spirometer software is capable (optional), the value corresponding to the 95% CI of the predicted value should be written in the report. (very good consensus)
7 10 1 100.0 5.6 VG
(R12-5) Cut off value for the lower limit of normality should be stated in the interpreter’s comments. (very good consensus)
1 4 11 2 94.4 11.1 VG
(R14-1) Interpretation should include suggestion/s on need for additional test if warranted. (very good consensus)
16 1 1 100.0 5.6 VG
(R15-1) In the section on “Interpreter’s Comments” the report should state what reference equation was used in the interpretation of the results. Statement on the need to correlate clinically should be written in the final interpretation (very good consensus).
2 4 10 1 88.2 6.7 VG
(R15-2) A research study will be conducted by the Council of Diagnostics & Therapeutics to determine which reference equation is best fitted for the local Filipino population. (For this item, kindly just state of your agree or disagree) (very good consensus)
0.0 0.0 VG
(R16-1) In the reports section on “Interpreter’s Comments”, it should be stated if the test satisfies the reproducibility criteria set by the ATS-ERS-TFLFT (1) or not. (very good consensus)
1 7 10 94.4 0.0 VG
(R16-2) It the test does not satisfy one of the acceptability or reproducibility criteria, it should state the consequences of this deficiency in the parameters. (very good consensus)
8 8 2 100.0 11.1 VG

Appendix N: Computation of the Parameters Needed for the Level of Consensus Classification
A B C D % of those who Agreed % of those who answered D Level of Consensus(R17-2) The spirometry report should contain the flow volume loops of all trials, if an interpretation of CAO or UAO made. If the spirometry software is not capable, the reproducibility of the flow volume loop should be stated in the section on “Interpreter’s Comments”. (very good consensus)
7 7 3 100.0 17.6 VG
(R18-1) The spirometry report should contain the measured parameters tabular graph. (very good consensus)
15 1 2 100.0 11.1 VG
(R18-2) The first 3 rows of the tabular graph should be allotted for the MRSP in the following order: FEV1/FVC, FVC and FEV1. (very good consensus)
8 9 1 100.0 5.6 VG
(R18-3) The succeeding rows maybe be allotted for the “other parameters” in the following order of priority: PEFR, FEF 25-75, FEF 75, MIF50/ MEF50, FEV1/FV6, MVV, MIF 50, MEF 50, FEV6, FEF 25 and FEF 50. (very good consensus)
9 8 1 100.0 5.6 VG
(R19-2) The IC section should state if the test satisfied the ATS-ERS-TFLFT (1) reproducibility criteria. If the test did not satisfy the criteria, the interpreter should state the consequences of this deficiency.(very good consensus)
6 10 2 100.0 11.1 VG
(R19-3) The IC section should also contain the basis for the interpretation. Specifically it should apply, the ATS-ERS-TFLFT (2) interpretation algorithm, criteria for severity and response to bronchodilator. (very good consensus)
9 8 1 100.0 5.6 VG
(R20-2) The FI should contain the following information: presence or absence of obstructive ventilatory defect and severity if present, presence or absence of probable restrictive ventilatory defect and severity if present, significant or no significant response to bronchodilator if done, suggestion for specific additional test if indicated, a generic sentence “Please correlate results with patient’s clinical data.” and printed name plus signature of the interpreter/s. (very good consensus)
15 2 1 100.0 5.6 VG

Appendix O
PCCP-DATS Committee on Spirometry Consensus
Chair: Ma. Janeth T. Samson, MD, FPCCP Council of Diagnostics and Therapeutics Members
Caburnay, Eloise Arabelle, MD, FPCCP Campomanes, Celeste Mae L.,MD, FPCCP Chavez, Christine L., MD, FPCP Chua-Panganiban, Shirley Jane, MD, FPCCP Claveria, Angelica, MD, FPCCP Cristobal- Aquino, Ma. Flordeliza, MD, FPCCP Dalupang, Julius, MD, FPCCP Divinagracia, Charissa, MD, FPCCP Elisterio, Helarose M., MD, FPCCP Garcia, Geraldine, MD, FPCCP Germar, Arnold G., MD, FPCCP Gonzales, Andrew S.A., MD, FPCCP Lee-Chua, Rachel, MD, FPCP Llanes-Gracia, Liza, MD, FPCCP Mapanao, Daisy, MD, FPCCP Micu, Lolita Brigida, MD,FPCP Mora, Czarina J., MD, FPCCP Natividad, Ma. Piedad R., MD, FPCCP Ogbac, William George, MD,FPCP Peñafiel, Alvin, MD, FPCCP Reside, Evelyn Victoria E., MD, FPCCP Reyes, Mary Jane, MD, FPCCP Santos, Alfredo Romeo Q., MD, FPCCP Tan, Marites, MD, FPCCP Tan, Florita, MD, FPCCP Samson, Lyndon H., MD, FPCCP Trinidad, Tim S., MD, FPCCP Valenzuela, Rosauro Vicente H. Jr.,MD, FPCCP Villanueva, Anna Tessa, MD. FPCCP Villanueva, Ma. Peachy Lara, MD, FPCCP Villasanta, Edwin I.,MD,FPCCP
Zantua, Raphael Ryan R., MD, FPCCP