Embed Size (px)
Citation preview

Plagiocephaly and Torticollis
Mia E. Lang, MD, PhD, FRCPC
General Pediatrician, Co-Vice Dean Education
Presenter: Mia Lang
• Speakers Bureau/Honoraria: N/A
• Consulting Fees: N/A
• Grants/Research Support: N/A
• Patents: N/A
• Other: N/A
• The Alberta College of Family Physicians has provided support in the form of a speaker fee and/or expenses.
Acknowledgments
Carolyn Shinbine, RN, BScN, Pediatric Head Shape Clinic, StolleryChildren’s Hospital
Dr. Keith Aronyk, pediatric neurosurgeon
Objectives
1. Assess infants for plagiocephaly and torticollis at routine well child visits
2. Discuss infant repositioning techniques with caregivers
3. Identify indications for referral for plagiocephaly/torticollis
4. Explain rationale for various treatment modalities for plagiocephaly/torticollis
Objective # 1
Assess infants for plagiocephaly and torticollis at routine well child visits:
- Overview of plagiocephaly
- History, risk factors
- Physical examination
- Differential: torticollis and craniosynostosis
Definition of Positional Plagiocephaly
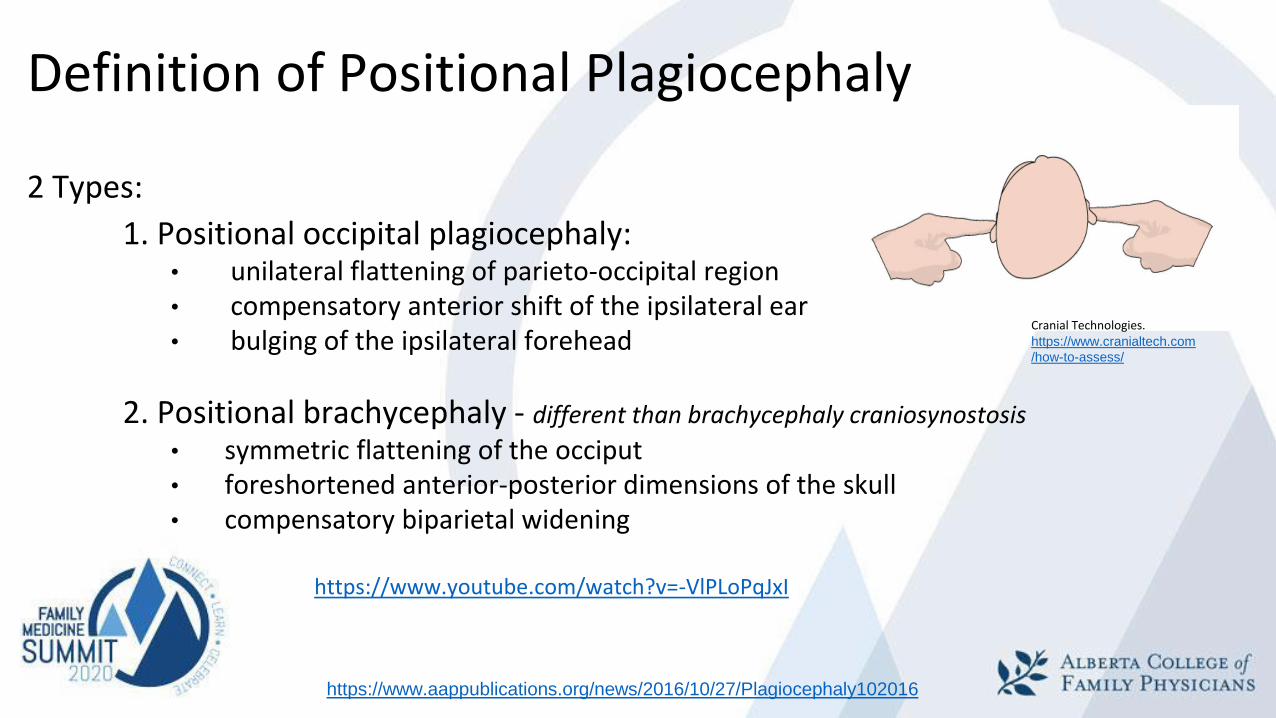
2 Types:
1. Positional occipital plagiocephaly:• unilateral flattening of parieto-occipital region• compensatory anterior shift of the ipsilateral ear• bulging of the ipsilateral forehead
2. Positional brachycephaly - different than brachycephaly craniosynostosis
• symmetric flattening of the occiput• foreshortened anterior-posterior dimensions of the skull• compensatory biparietal widening
https://www.youtube.com/watch?v=-VlPLoPqJxI
https://www.aappublications.org/news/2016/10/27/Plagiocephaly102016
Cranial Technologies. https://www.cranialtech.com
/how-to-assess/
Positional Plagiocephaly, aka Deformational, non-synostotic plagiocephaly
0.3% pre Back-To-Sleep, post = 8.2%
Prevalence:
• 6 weeks: 16 - 22 %
• 4 months: 19.7 %
• 12 months: 6.8 %
• 2 years: 3.3 %
Bialocerkowski et al., 2008
Risk Factors for Abnormal Head Shape
Prenatal:
- Male- Primip- Multiple birth
Perinatal:
- Obstetrical instrumentation- High birth weight- Prematurity- Large head circumference
Postnatal:- Supine position- Torticollis, restricted head movement- Bottle feeding without repositioning- Little “tummy time”- Development delay
Linz et al., 2017. Positional skull deformities
Physical exam
1 wk for: head shape/dysmorphism
2wk, 6wk, 4m, 6m, +/-9m, 12m for:• General: dysmorphisms
• Growth: HC
• Head: suture lines, fontanelles, mastoid process, shape, forehead
• Neck: ROM, mass
• Eyes: shape, size, symmetry
• Ears: location, symmetry
• MSK: tone, development
Differential
• Congenital muscular torticollis
• Unilateral lambdoid synostosis
• Unilateral coronal synostosis
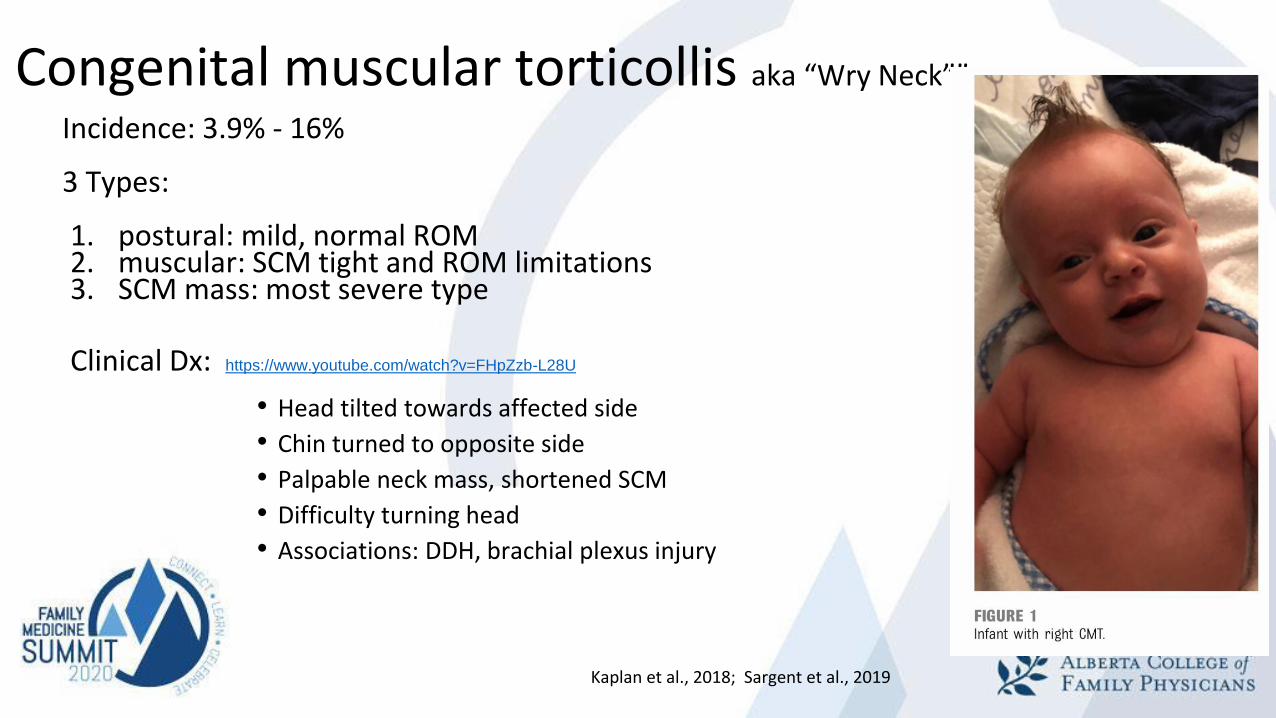
Congenital muscular torticollis aka “Wry Neck””
Incidence: 3.9% - 16%
3 Types:
1. postural: mild, normal ROM2. muscular: SCM tight and ROM limitations3. SCM mass: most severe type
Clinical Dx: https://www.youtube.com/watch?v=FHpZzb-L28U
• Head tilted towards affected side
• Chin turned to opposite side
• Palpable neck mass, shortened SCM
• Difficulty turning head
• Associations: DDH, brachial plexus injury
Kaplan et al., 2018; Sargent et al., 2019
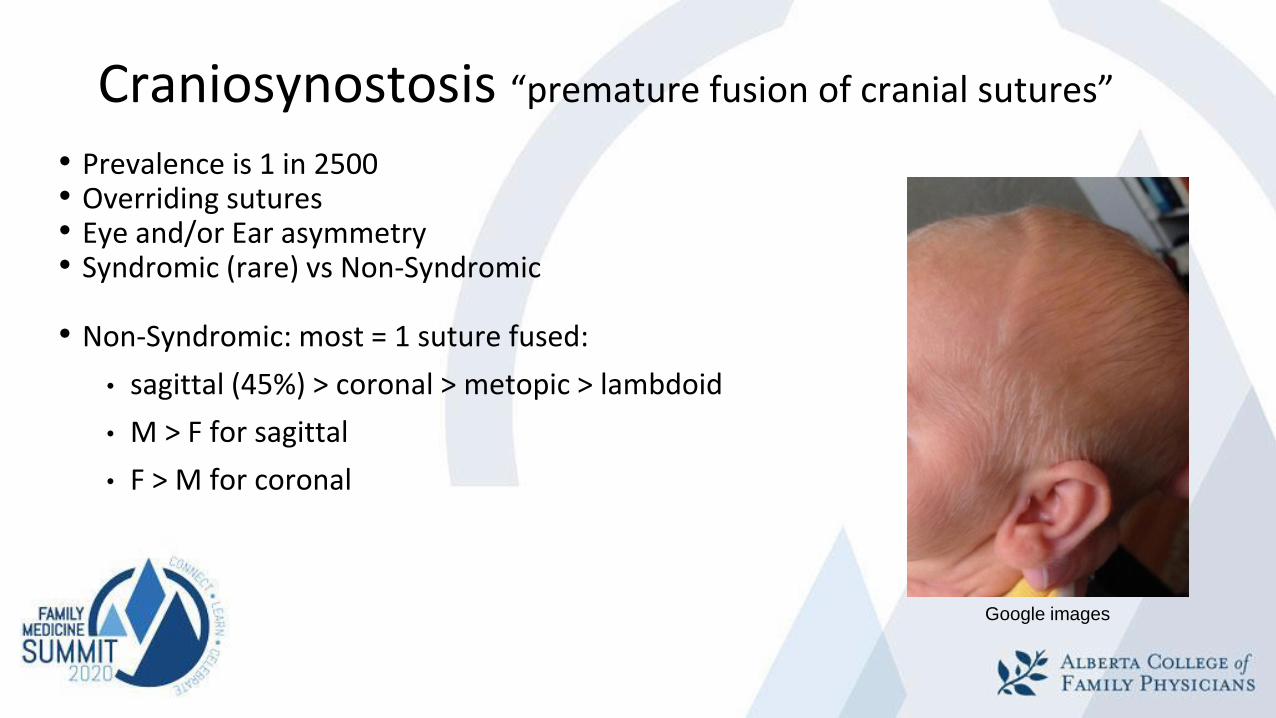
Craniosynostosis “premature fusion of cranial sutures”
• Prevalence is 1 in 2500• Overriding sutures• Eye and/or Ear asymmetry• Syndromic (rare) vs Non-Syndromic
• Non-Syndromic: most = 1 suture fused:
• sagittal (45%) > coronal > metopic > lambdoid
• M > F for sagittal
• F > M for coronal
Google images
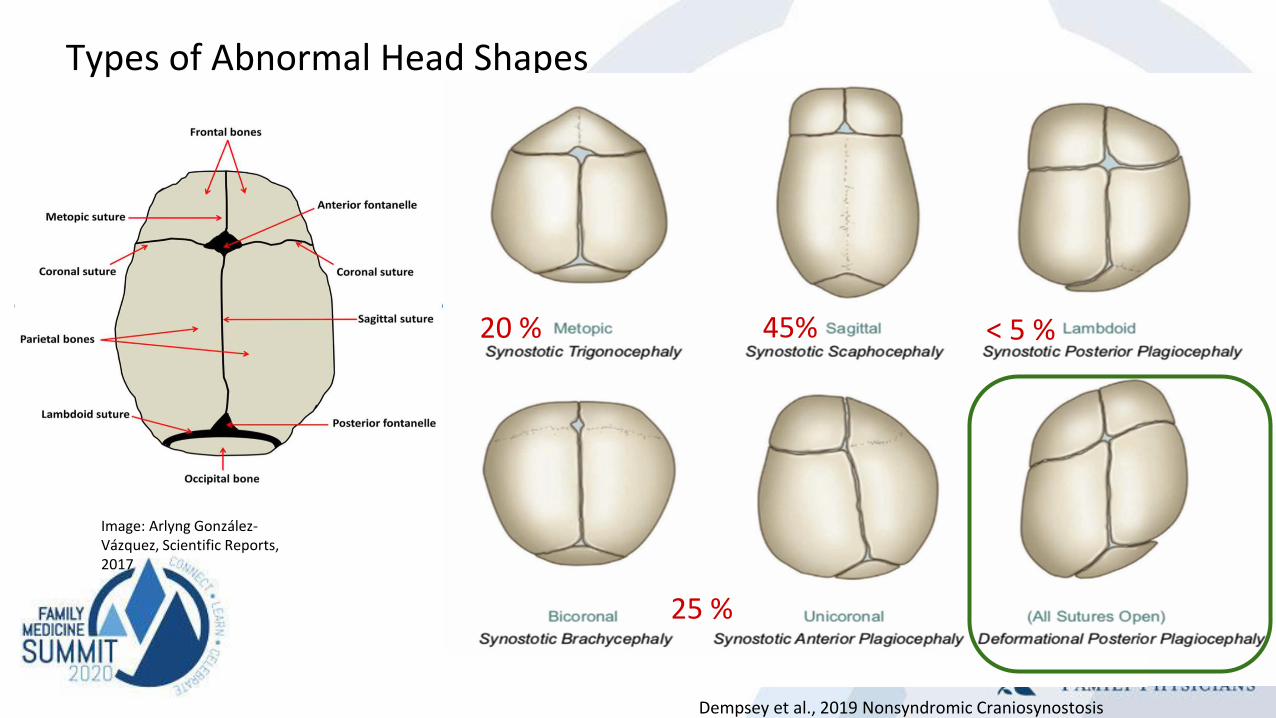
Types of Abnormal Head Shapes
Dempsey et al., 2019 Nonsyndromic Craniosynostosis
45%
25 %
20 % < 5 %
Image: Arlyng González-Vázquez, Scientific Reports, 2017
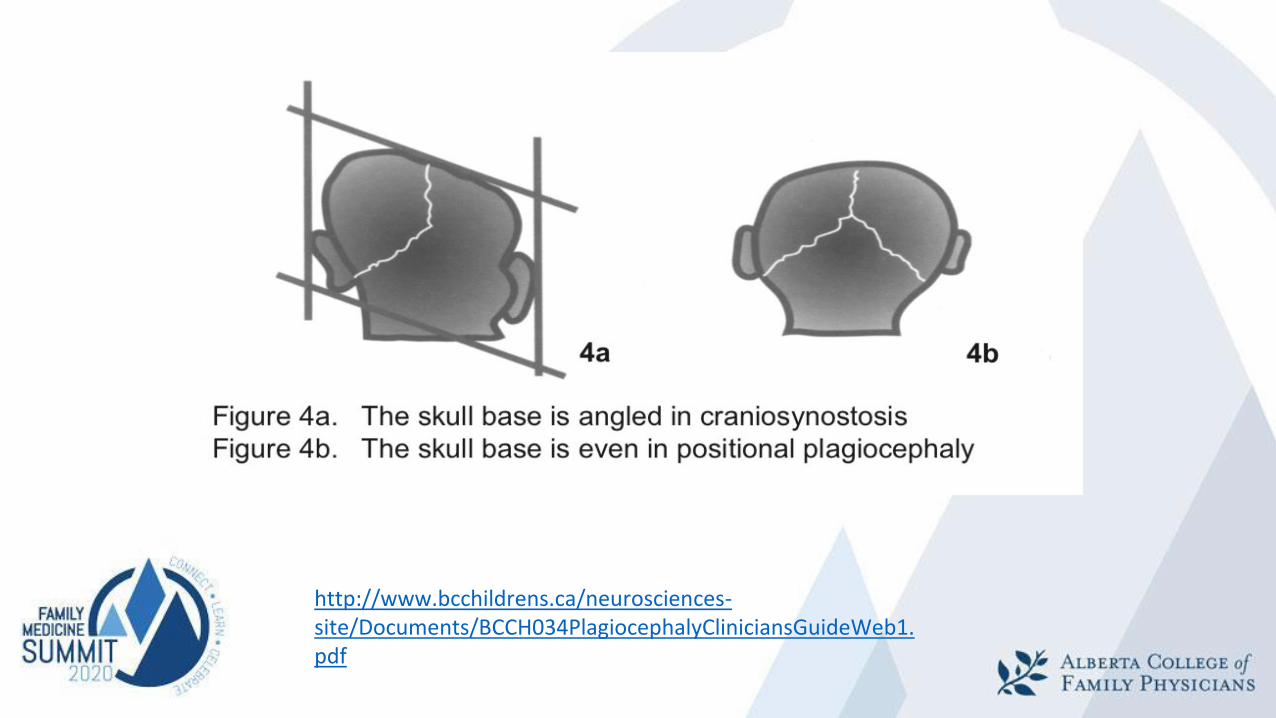
http://www.bcchildrens.ca/neurosciences-site/Documents/BCCH034PlagiocephalyCliniciansGuideWeb1.pdf
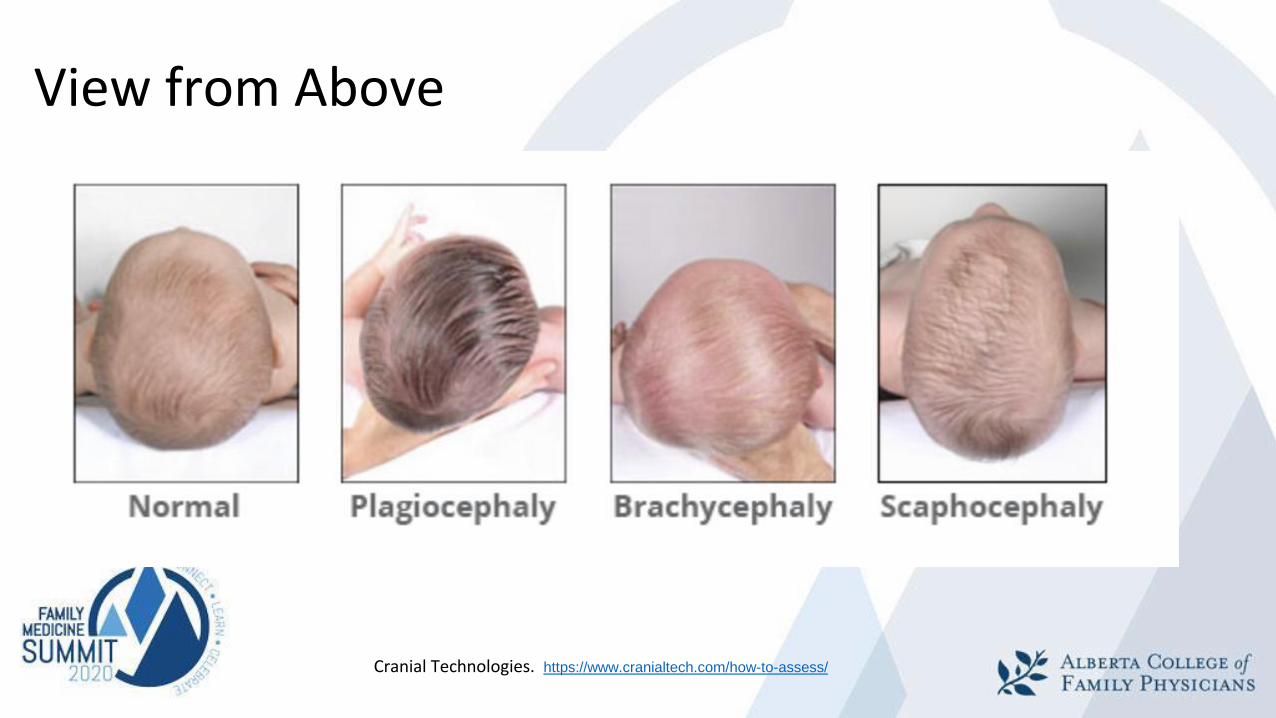
View from Above
Cranial Technologies. https://www.cranialtech.com/how-to-assess/
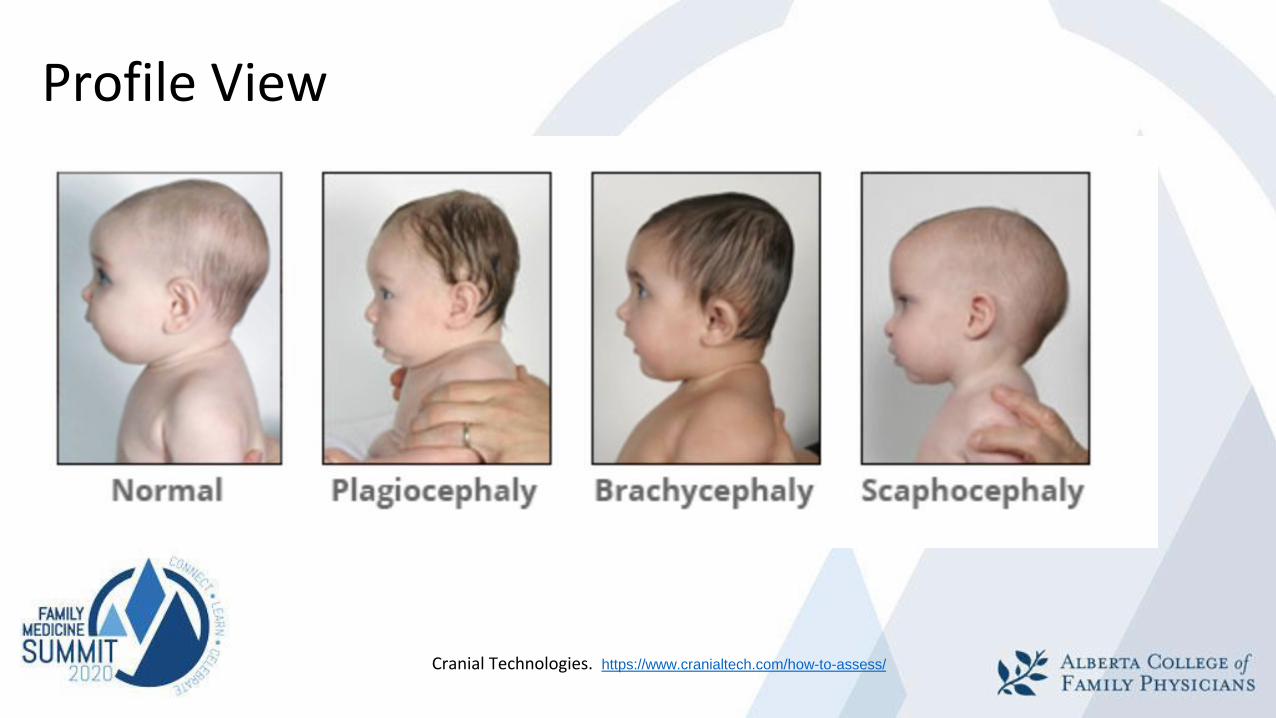
Profile View
Cranial Technologies. https://www.cranialtech.com/how-to-assess/
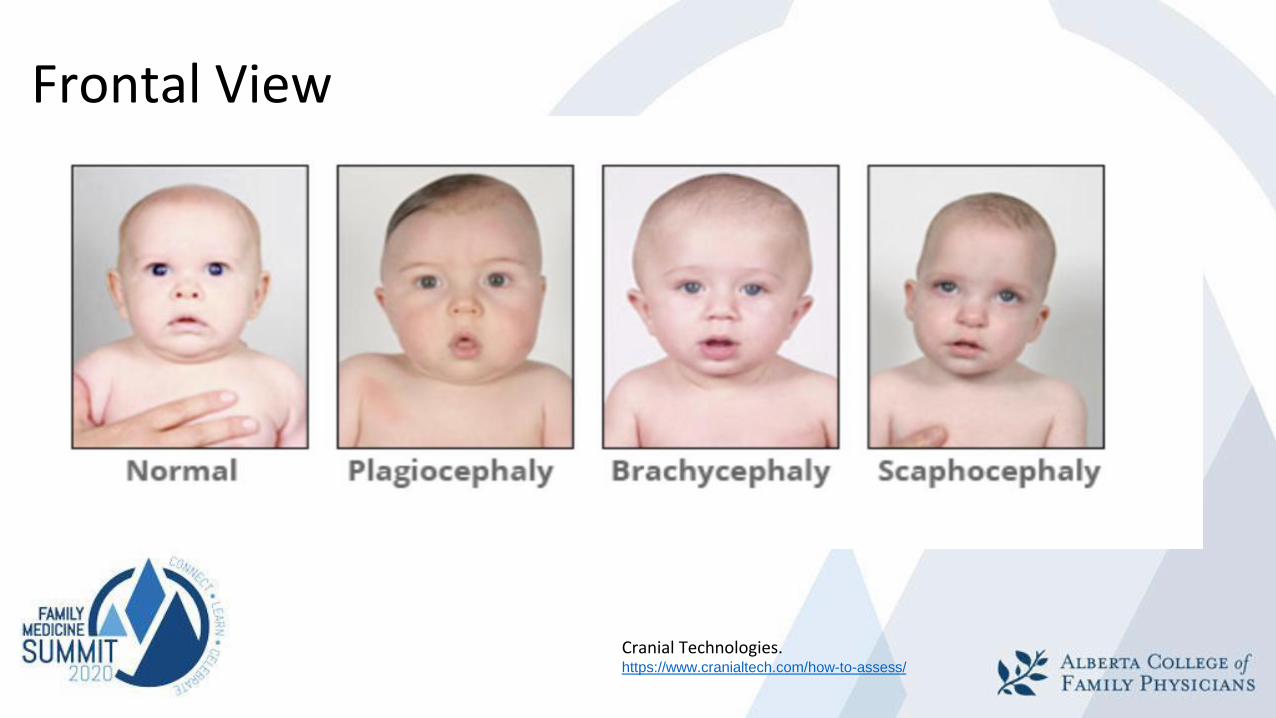
Frontal View
Cranial Technologies. https://www.cranialtech.com/how-to-assess/
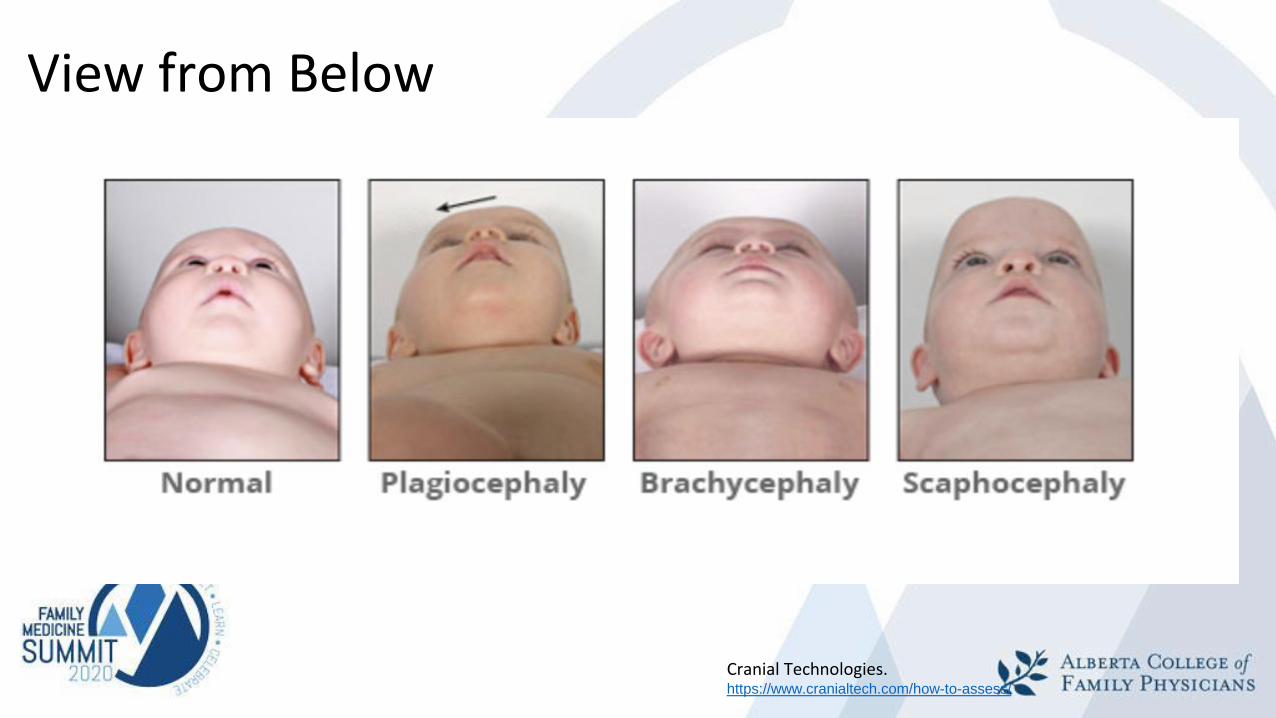
View from Below
Cranial Technologies. https://www.cranialtech.com/how-to-assess/
Objectives # 2 and # 4
Discuss infant repositioning techniques with caregivers
Explain rationale for various treatment modalities for plagiocephaly/torticollis
Prevention of Positional Plagiocephaly
• Avoidance of favourite side
• Bilateral stimuli
• Adequate tummy time: 10-15min TID
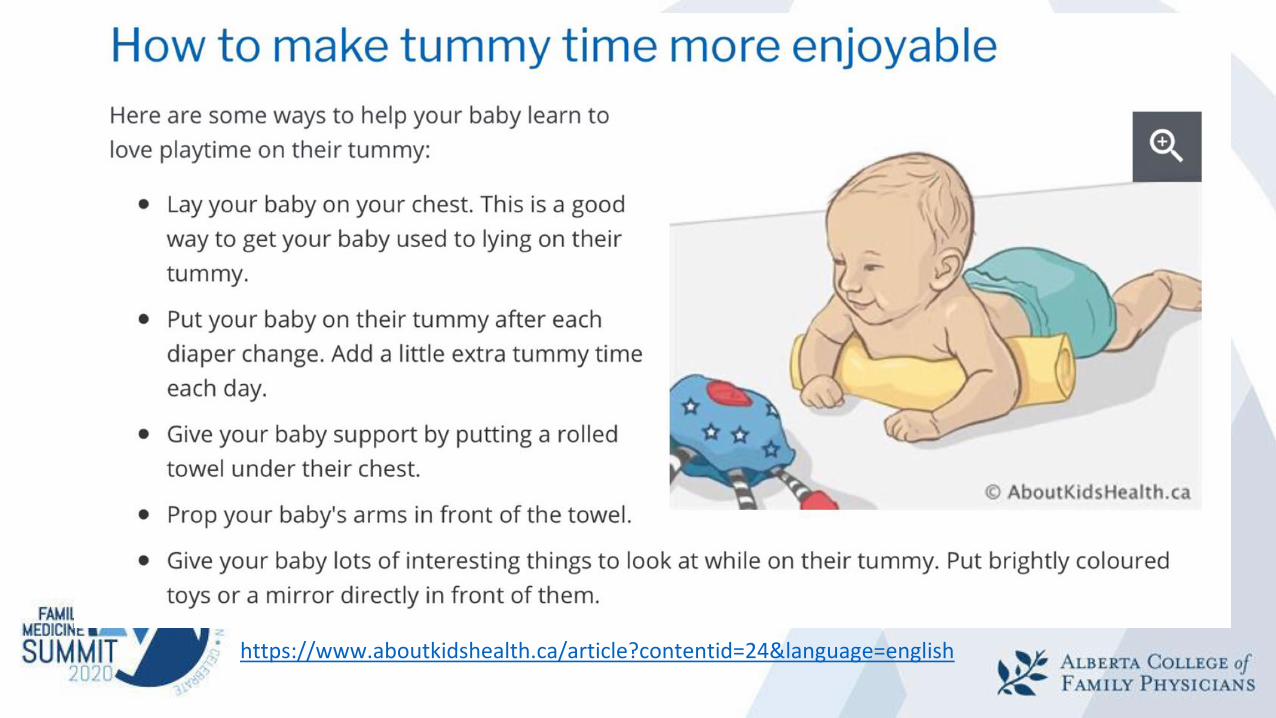
https://www.aboutkidshealth.ca/article?contentid=24&language=english
Plagiocephaly Treatment
• Surgical: for craniosynostosis
• Non-Surgical:
• Observation
• Repositioning
• Physiotherapy
• Moulding/Helmet Therapy
• Infant bed “positioning”pillows
• Chiropractic
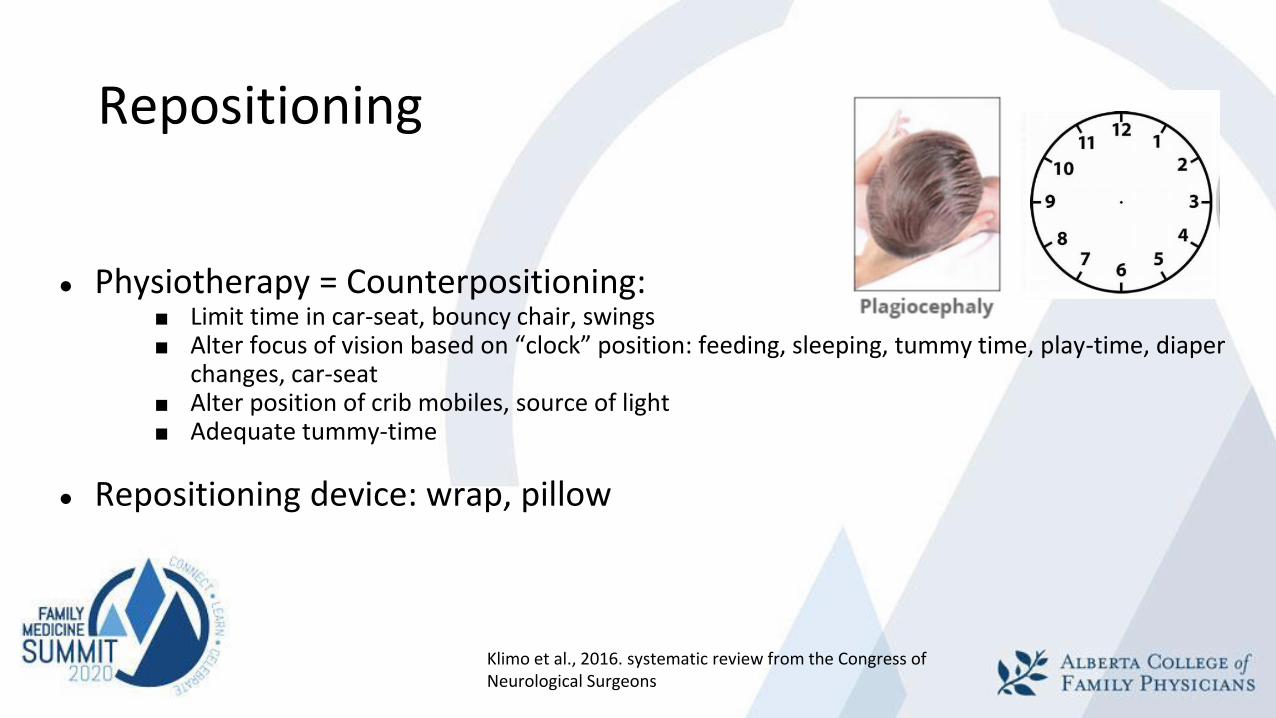
Repositioning
● Physiotherapy = Counterpositioning:■ Limit time in car-seat, bouncy chair, swings■ Alter focus of vision based on “clock” position: feeding, sleeping, tummy time, play-time, diaper
changes, car-seat■ Alter position of crib mobiles, source of light■ Adequate tummy-time
● Repositioning device: wrap, pillow
Klimo et al., 2016. systematic review from the Congress of Neurological Surgeons
Helmet/Cranial Orthosis therapy
Advantages
• Slightly faster rate of improvement in skull shape
Disadvantages
• Cost ($1800 - $2800 )• Time• Contact dermatitis, pressure sores
Best age: 6 - 9 m old (capture aggressive brain growth)Indicators:
● severe plagiocephaly (Can Ped Society, 2018)
● persistent moderate to severe plagiocephaly (Congress of Neurological Surgeons,
2016)
1. after repositioning and/or physio;
2. presenting at an advanced age

Cranial Orthotics- 23 h/day x 4 months- Orthotist visits Q2weeks
Traditional Helmet SnugKap
https://pediatricheadshape.com/snugkap/
Torticollis Treatment: Torticollis does not spontaneously resolve
Best outcomes when treatment starts before 3m old
1st Line:a. Neck passive ROM: stretch tight SCMb. Neck and trunk active ROM: strengthen opposite side SCMc. Develop symmetrical movementd. Environmental adaptations: Repositioning techniquese. Caregiver education
Physical Therapy Management of Congenital Muscular Torticollis: A 2018 Evidence-Based Clinical Practice Guideline From the APTA Academy of Pediatric Physical Therapy. Kaplan et al., 2018
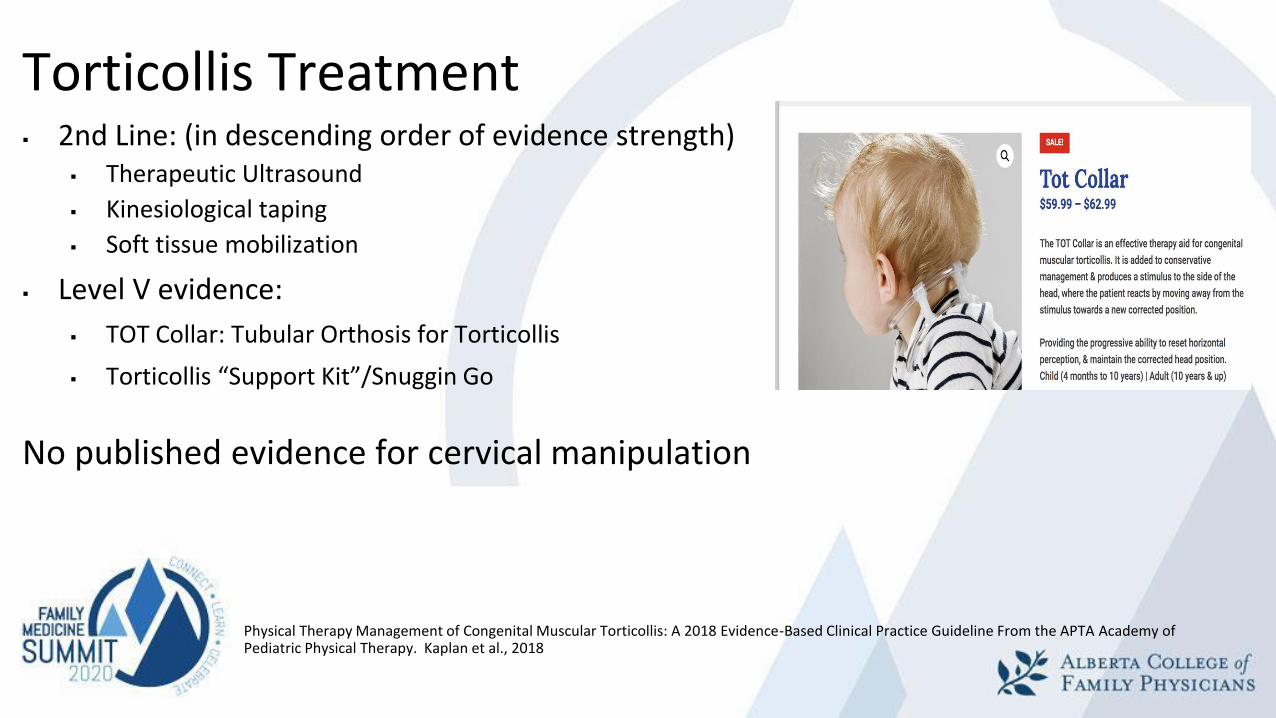
Torticollis Treatment▪ 2nd Line: (in descending order of evidence strength)
▪ Therapeutic Ultrasound
▪ Kinesiological taping
▪ Soft tissue mobilization
▪ Level V evidence:
▪ TOT Collar: Tubular Orthosis for Torticollis
▪ Torticollis “Support Kit”/Snuggin Go
No published evidence for cervical manipulation
Physical Therapy Management of Congenital Muscular Torticollis: A 2018 Evidence-Based Clinical Practice Guideline From the APTA Academy of Pediatric Physical Therapy. Kaplan et al., 2018
Objective # 3
Identify indications for referral for plagiocephaly/torticollis
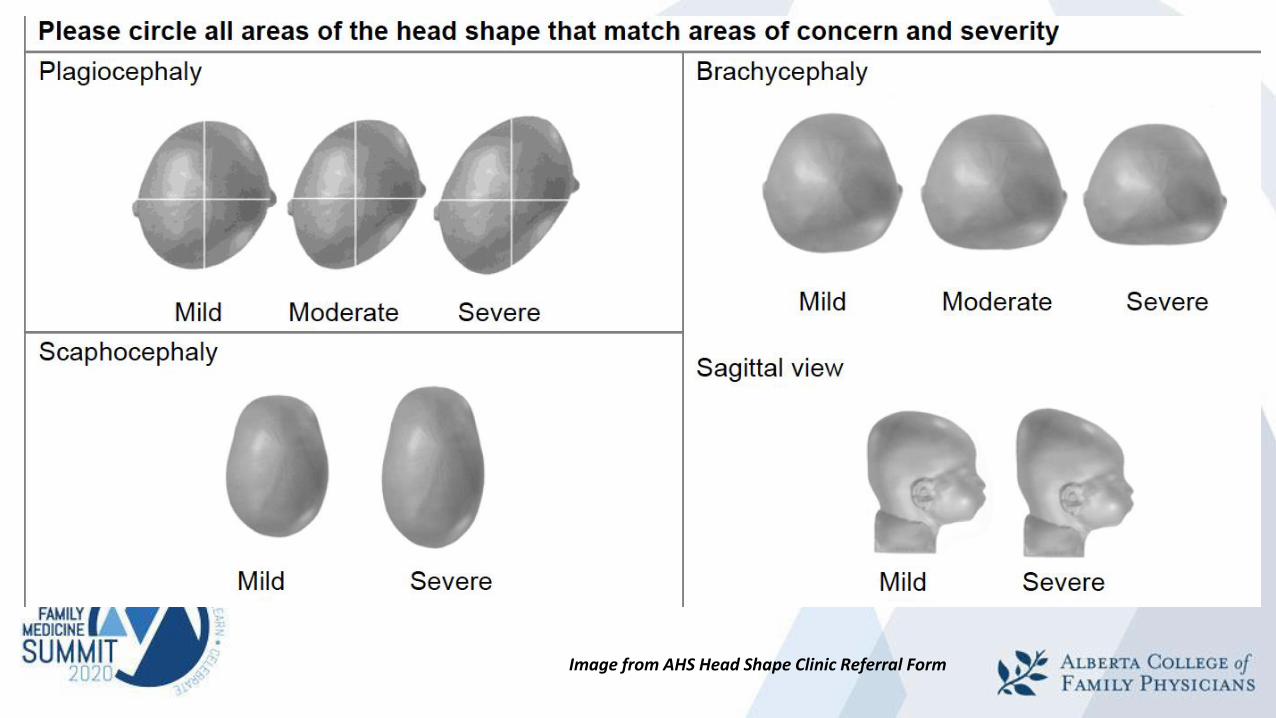
Image from AHS Head Shape Clinic Referral Form
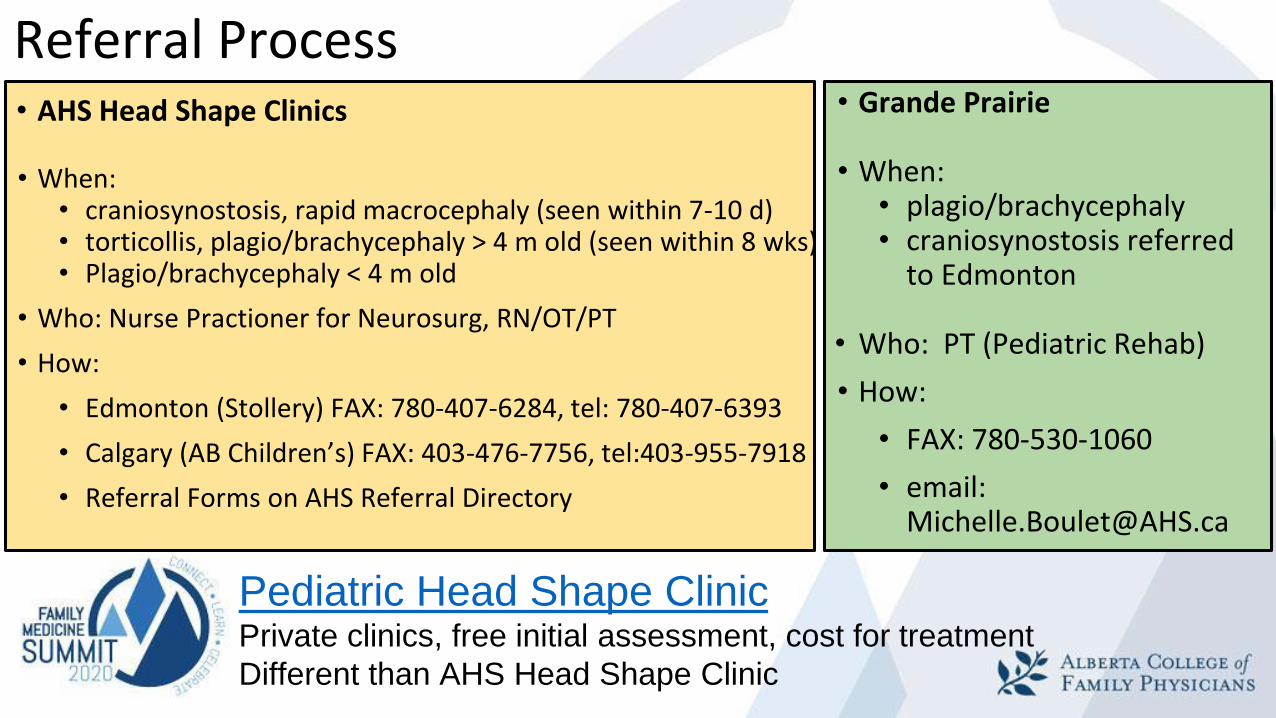
• Grande Prairie
• When:• plagio/brachycephaly• craniosynostosis referred
to Edmonton
• Who: PT (Pediatric Rehab)
• How:
• FAX: 780-530-1060
• email: [email protected]
Referral Process• AHS Head Shape Clinics
• When:• craniosynostosis, rapid macrocephaly (seen within 7-10 d)• torticollis, plagio/brachycephaly > 4 m old (seen within 8 wks)• Plagio/brachycephaly < 4 m old
• Who: Nurse Practioner for Neurosurg, RN/OT/PT
• How:
• Edmonton (Stollery) FAX: 780-407-6284, tel: 780-407-6393
• Calgary (AB Children’s) FAX: 403-476-7756, tel:403-955-7918
• Referral Forms on AHS Referral Directory
Pediatric Head Shape ClinicPrivate clinics, free initial assessment, cost for treatment
Different than AHS Head Shape Clinic
Conclusions
Positional plagiocephaly:
- common, benign, but distressing to guardians- distinguish from craniosynostosis- prevention and repositioning- referral if: dysmorphic findings, craniosynostosis, plagio > 4m- monitor development
Torticollis:
- check neck ROM at routine baby checks- refer to AHS Head Shape Clinic





























