Embed Size (px)
Citation preview

Journal of Medical Genetics 1988, 25, 104-112
A recessive form of congenital contractures andtorticollis associated with malignant hyperthermiaU G FROSTER-ISKENIUS*, J R WATERSONt, AND JUDITH G HALL*From *the Department of Medical Genetics, Clinical Genetics Unit, University of British Columbia,Vancouver, British Columbia, Canada; and tthe Department of Medical Genetics, Children's HospitalMedical Center, Akron, Ohio, USA.
SUMMARY Two families are presented, each with two affected sibs, all four of whom seem tohave a newly described and specific form of congenital contractures (arthrogryposis). Theaffected subjects have congenital torticollis, dysmorphic, asymmetrical, myopathic facialfeatures, and progressive scoliosis. Two sibs had cleft palate. Malignant hyperthermia hasoccurred in two of the patients.
The conditions which present with congenital con-tractures are a very heterogeneous group ofdisorders.They include those with a known neurological ormyopathic basis, as well as many idiopathic forms ofunknown aetiology. We report two pairs of sibsfrom two unrelated families who seem to have aspecific genetic form of congenital contractures(arthrogryposis). The affected subjects have con-genital torticollis and characteristic dysmorphiccraniofacial features, including facial asymmetry,asymmetrical, myopathic facial movements, ptosis,and cleft palate (in two sibs). They also haveprogressive scoliosis. Intelligence is high normal.Two of the patients have had episodes of malignanthyperthermia.
Case reports
FAMILY 1Patient 1 was the first child of healthy, non-consanguineous parents. Maternal age at birth was22 years and paternal age 28 years. Family historywas unremarkable. One elective termination hadoccurred before this conception. Pregnancy wascomplicated by spotting at three months and poly-hydramnios late in pregnancy. Decreased fetalmovement was noted at 34 weeks of pregnancy. Thepatient was delivered at 39 weeks by caesareansection because of failure of progression of labour.His birth weight was 3650 g (50th centile), length 50
Received for publication 12 July 1986.Revised version accepted for publication 7 January 1987.
cm (50th centile), OFC 36.6 cm (50th centile).Apgar score was 2 at one minute and 5 at fiveminutes and he required vigorous resuscitation andtherapy for respiratory distress.At birth (fig 1) he was profoundly hypotonic and
had multiple congenital contractures and facialanomalies. He had bilateral equinovarus deformitiesof the feet. The wrists were fixed in hyperextensionand the fingers were overlapping, with lack ofmovement in the IP and MP joints. No finger orpalm creases were present. Muscle tone was hypo-tonic and his muscle mass appeared decreased. Hehad a scaphocephalic skull. A Pierre-Robin anomalywith micrognathia and a V shaped cleft palate werepresent. Two natal teeth were present. He had a flatmidface and his left palpebral fissure was downwardslanted. Torticollis was present on the left. De-creased facial expression and generalised facialweakness were present. He had webbing of theneck. His chest was broad and asymmetrical, withthe right side more prominent than the left, and thesternum was mildly depressed. Chest x ray showedvery thin ribs. At the age of two years, three monthshe was on the 10th centile for height (85.4 cm),below the 5th centile for weight (8-9 kg), with anOFC on the 50th centile (47-5 cm). Physical findingsat that age included a persistent torticollis on the leftand plagiocephaly with a prominent metopic suturewhich had fused prematurely. He had rather fullcheeks, a downturned, small mouth, and a tendencyto hold it open with some drooling. The facialmuscles appeared hypotonic and there was littlemovement of the face. His face was asymmetrical
104
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

A recessiveform ofcongenital contractures and torticollis associated with malignant hyperthermia
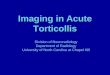
FIG 1 Patient 1 shortly after birth. Note asymmetrical face,torticollis, excessive skin, and webbing of neck.
with flattening of the left side and a more prominentright side. He had a small nose. There weredownward slanting palpebral fissures and ptosis ofthe eyelids, both being more obvious in the right eyethan in the left. Facial movements showed asym-metry in that the right side of the face moved lessthan the left. Both hands showed ulnar deviationand camptodactyly in the IP joints of the second,third, fourth, and fifth fingers. Partial proximalcutaneous syndactyly of the second and third fingerswas also noted. The thumbs were dislocated andfixed in the IP joints. There was a limited range ofmovement in his legs with the knees lacking 100 ofextension and the ankles lacking full dorsiflexionand full plantar flexion. A mild conductive hearingloss was found bilaterally. Motor milestones werewithin normal limits. His speech development wasdelayed because of his cleft palate. He had learnedto sit at the age of five and a half months and startedto speak a few words at the age of two years, threemonths. His vocabulary at this age was about twomonths behind.At the age of four years, 10 months (fig 2) he was
FIG 2 Patients 2 and 1 showing similar features, with facialasymmetry, myopathic facies, mild ptosis, persistenttorticollis, scoliosis, and webbing across joints.
below the 5th centile for height and weight (89 cm,13-5 kg). His OFC was on the 50th centile for his age(51 cm). Craniofacial features showed the sameanomalies as described at the age of two years, threemonths. Palpebral fissure length (2.5 cm) and innercanthal distance (2-7 cm) were appropriate (50thcentile) to his head circumference. He had a longphiltrum (2-0 cm) (.2 SD), micrognathia, and arepaired cleft palate. His voice was very nasal. Theteeth were carious. The ears were mildly posteriorlyrotated, but of normal size (5-4 cm) (50th centile)and normal shape. His chest circumference mea-sured 54 cm (50th centile) with an internippledistance of 16 cm (.97th centile). The chest wasclear. No abnormal heart murmurs were heard. Amarked thoracolumbar scoliosis with a 550 curve waspresent with 170 of kyphosis. The kyphoscoliosis wasapparently due to a muscular imblance, since novertebral defects were found on x ray. Webbing ofhis neck and in the axillary region was present.There were dimples at both elbows. The upperlimbs showed a good passive range of movement.His hands were 11 cm long (10th centile), with slight
105
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

U G Froster-Iskenius, J R Waterson, and Judith G Hall
camptodactylyandulnar deviation stillpresent. Therewere no flexion creases on his fingers or his palms,but he had a relatively full range of movement in thehands. The fingernails appeared hyperconvex andmild tapering of the fingers was present. The musclemass in his arms was decreased. A discrepancy in leglength was seen with the left leg being 1 cm shorterthan the right. He did not have pterygia in thepopliteal or inguinal region, but had some extra skinbehind his knees. Some muscle mass in the legs wasdecreased. There were no obvious flexion contrac-tures in his hips. The abdomen was normal. Hisgenitalia were male with a normal size penis and histestes were descended. His skin was soft.
Dermatoglyphics showed no distal triradii oneither hand. The distribution of pattern on thefingertips was: right hand Lu, W, Lu, Lu, A; lefthand W, W, Lu, Lu, Lu. Intellectual developmentwas normal with an IQ in the high normal range.
Scarring of the sclera developed because he didnot completely close his eyes during sleep. Heunderwent operations for bilateral inguinal hernia atthe age of 13 months and foot surgery at ninemonths of age. His cleft palate was repaired when hewas 22 months old. He had experienced an episodeof malignant hyperthermia during anaesthesia forhis club foot repair at nine months. Serious raisingof body temperature had also occurred duringsurgical repair of his inguinal herniae. Between theage of three and four years a progressive scoliosisdeveloped which was treated with a brace and withphysiotherapy. Laboratory investigations showed anormal to low CK of 24 units. A muscle biopsy ofthe left abductor hallucis longus showed mildneuropathic changes. Electron microscopy studieswere performed but did not show specific changesfor a congenital myopathy.
Patient 2 is the younger sister of patient 1. Shewas born after an uneventful pregnancy, monitoredwith realtime ultrasound for contractures and fetalmovements at 16, 20, and 24 weeks of gestation.Abnormal fetal movements were not recognisedduring the prenatal ultrasound investigations. Shewas born by repeat caesarean section one week afterterm. Her birth weight was 3300 g (50th centile). Atbirth she was noted to have torticollis on the rightside and contractures of the limbs similar to thoseseen in her brother, including a metatarsus adductuson the left side and slight ulnar deviation of thefingers with camptodactyly of the third, fourth, andfifth fingers bilaterally. She had long, taperingfingers and overlapping toes (third over second).At the age of six months her height was on the
10th centile (62.5 cm), her weight on the 25thcentile, and her OFC on the 50th centile (42 cm).Her skull was plagiocephalic and her face asymmet-
rical, with the left cheek showing more fullness thanthe right. She had a prominent metopic suture whichhad fused prematurely. The torticollis was persis-tent. Her craniofacial features were further remark-able for a ptosis of her eyelids which was moreobvious on the right than on the left. Her nose wasslightly deviated. Her mouth was downturned andsmall, with a tendency to be held open and withintermittent drooling. A V shaped cleft palate wasalso present.She could not open her mouth fully. At 11 months
she was still on the 10th centile for length (69.5 cm)and on the 5th centile for weight with an OFC on the25th centile. By the age of two years she was belowthe 5th centile for length (80.4 cm) and on the 5thcentile for weight (9-9 kg). OFC was 48 cm (50thcentile). At that age she still had the right sidedpersistent torticollis. Helmet therapy for pla-giocephaly had not been successful. Her cleft palatehad been repaired at 20 months of age and she had apossible episode of malignant hyperthermia aftersurgery. She suffered from recurrent otitis media.At the age of 19 months a mild conductive hearingloss was noted.On examination at two years of age (fig 2) slight
webbing of her axillary regions was observed, butthere was no webbing in the popliteal and inguinalregion. Increased asymmetry of her facial featureshad developed. Her palpebral fissures measured 2-3cm, and her inner canthal distance 2-4 cm (25thcentile). She had a long philtrum (1-6 cm) (.2 SD).Her primary teeth appeared mottled. Her chest wasclear without abnormal heart sounds. Chest cir-cumference was 51 cm, on the 75th centile for herchronological age, and her internipple distance was12*5 cm (95th centile). A mildly depressedsternum was present. A mild scoliosis haddeveloped. Her hands showed both index fingerscurved ulnarly with stiffness in the IP joints. Heraffected left leg showed a full range of movement inthe knee. Her motor and intellectual developmentwas unremarkable. She had appropriate speechdevelopment for her age. Her voice had a high nasalquality. Her IQ, however, appeared high normal.
FAMILY 2Patient 3 was the second child born to a healthy 28year old mother and an unrelated, healthy 30 yearold father. The family already had a healthydaughter. The pregnancy itself was basically uncom-plicated. The mother took vitamins throughout anda cough medicine containing caramiphen edisylate,chlorpheniramine maleate, phenylpropanolaminehydrochloride, isopropamide iodide, and alcoholduring the first trimester. There was spotting for a
106
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

A recessiveform ofcongenital contractures and torticollis associated with malignant hyperthermia
few days during the fifth month. Fetal movementwas considered normal.The patient was born at 36 weeks of gestation.
Membranes ruptured and labour was subsequentlyinduced. Delivery was spontaneous vertex. Apgarscores were 6 at one minute and 7 at five minutes.His birth weight was 2310 g (25th centile) (fig 3). Atbirth, multiple joint contractures and facial abnor-malities were noted. His hips were held in partialflexion and abducted. His knees were extended. Hehad bilateral equinovarus feet with both forefeet inthe varus position. In the upper limbs there werefixed flexion contractures of 900 at the elbow and thewrists were completely flexed. He had long taperingfingers with long nails and palmar creases wereabnormal but not further specified at birth.Craniofacial features included an OFC on the 50thcentile (32-4 cm) and a brachycephalic skull with adownward sloping forehead. The nose was deviatedto the right with a prominent nasal bridge and flatnasal tip. The eyes appeared widely set; the innercanthal distance measured 2-0 cm (1 SD) and theouter canthal distance was 6-25 cm (.2 SD).Palpebral fissure length was 2*0 for the right and 1-9for the left eye (.2 SD). The eyes showed mildproptosis. The mouth had a prominent cupid bow.The philtrum was rather long (1-1 cm, 2 SD). Hismandible was small. He had anteverted, roundedshoulders and his neck showed a palpable masswhich was diagnosed as a cystic hygroma. His chestwas symmetrical with a circumference of 30-25 cm(mean) with widely spaced nipples. Internipple
distance was 9 cm (2 SD). His genitalia were malewith a small, normal appearing penis, but unde-scended testes and a poorly developed scrotal sac.The skin showed a pigmented intradermal naevus onthe left posterolateral side of the thorax. The boydied four days after birth from respiratory insuffi-ciency. Additional findings at necropsy were onlytwo vessels in the umbilical cord and pleuricysticrenal disease with a moderate number of ectatictubules and ectatic Bowman's capsule. The muscula-ture, especially of the lower extremities, was palewhitish in colour. Scanty muscle tissue was replacedby fibrous and adipose tissue. Sections of the muscleshowed atrophy of individual scattered fibres and ofentire fascicles with marked endomysial and perimy-sial fibrosis. Neuropathological investigations showeddiffuse and focal bilateral but asymmetrical absenceof motor neurones at all levels of the spinal cord,most severe in the cervical region. Torticollis,asymmetrical face, and ptosis of the eyelids were notdescribed at birth, but appear to have been present,as seen in the patient's photographs (fig 3).Two first trimester spontaneous abortions occur-
red between patient 3 and patient 4. Both of thosepregnancies were also complicated by vaginalinfections treated with metronidazole (Flagyl).
Patient 4 is the younger brother of patient 3.Maternal age was 32 years and paternal age 33 yearswhen he was born. Pregnancy history was unevent-ful. There was use of metronidazole in the fourthmonth of pregnancy. Fetal movements were felt tobe normal. Ultrasound monitoring was performed at
f _ _ FIG 3 Patient 3.Post mortemphotographs. Note
_fxed contracturesand prominentbridge of nose.
107
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

U G Froster-Iskenius, J R Waterson, and Judith G Hall
two months, five months, and just before delivery.No comment on fetal movement was made. He wasdelivered at term by caesarean section because ofbreech presentation. His birth weight was 2810 g(25th centile). He was found to have flexioncontractures of his joints at birth, including atorticollis to the left side. Physical examination atthe age of 13 months (fig 4) showed that he was onthe 25th centile for length (25 cm) and on the 50thcentile for weight (8-2 kg). His head circumferencemeasured 43-5 cm (50th centile) while his headshape was brachycephalic and plagiocephalic. Theanterior fontanelle was closed. He had a long facewith torticollis on the left side. Other craniofacialfeatures included an inner canthal distance of 2-0 cm(3rd centile) and an outer canthal distance of 5-7 cm(3rd centile). His ears were asymmetrical and theright ear had a poorly formed helix. Ear length was4-8 cm (25th centile). The ears appeared low set andslightly posteriorly rotated. His nose had a flat tipand a prominent nasal bridge. He had micrognathiaand a broad alveolar ridge which gave the impress-ion of a high arched palate. His teeth appearedsmall. Decreased and asymmetrical facial move-ments were noted.
FIG 4 Patient 4. Note torticollis, prominent bridge anddepressed tip of nose, facial asymmetry, and abnormal ear.
The neck was short with mild webbing mainly onthe left side. The range of motion of his head waslimited. His chest was symmetrical with a mildpectus excavatum and increased AP diameter. Noabnormal heart murmurs were noted. His shoulderswere anteriorly rotated. Decreased range of move-ment was observed in all joints. The upper limbsshowed dimples over the elbows and wrists. Campto-dactyly of the fingers was present with webbingbetween the metacarpophalangeal and proximalphalangeal joints. Palmar creases showed bilateralsimian creases with a decreased number of plantarand palmar creases. His feet were still in bilateraltalipes equinovarus position. His genitalia weremale with undescended testes and a poorly de-veloped scrotum with a prominent median raphe.He learned to sit independently at nine months
and started to talk at 18 months. At the age of18 months he had an episode of unconsciousnesswhich seemed to be related to an apnoeic spell. Herecovered from this episode with no apparentsequellae. When examined at the age of 19 monthshe was below the 5th centile for length (75 cm) andweight (8.4 kg). His head circumference measured45-5 cm (.5th centile). He had downward slanting
A
FIG 5 Patient 4. Note ptosis, facial asymmetry, andpersistent contractures.
108
1. W.1-
PPV
.s.V.A t".t
"p
il. "..ik&-
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

A recessiveform ofcongenital contractures and torticollis associated with malignant hyperthermia
palpebral fissures and some ptosis of the eyelids. Hisfine motor and intellectual development werenormal to high normal. He still requires assistance inwalking at two and a half years. He has developedmild scoliosis. The torticollis has responded rela-tively well to bracing therapy. A muscle biopsy atthe age of two years showed atrophic muscle cells,only type I muscle fibres, and an overall impressionof degenerated skeletal muscle with enlargementand remodelling of motor units consistent with aneuropathy. Laboratory investigations revealed alow serum CK level of 29 units (normal for age 35 to232 units).
Summary of clinical findings (table 1)
These four patients had several features in common.The most striking were torticollis, asymmetry of theface, and decreased facial movements. On the sideof the torticollis, the side of the face was flattenedwith a prominent cheek on the opposite side. Thefacial features were also remarkable because ofptosis of the eyelids and downturned corners of themouth. They had myopathic facial expressions. Thephiltrum, when measured, was long (.2 SD). Twosibs had cleft palate and one had prominent alveolarridges which gave him a high appearing palate.
Micrognathia and low set, posteriorly rotated ears
were also noted in all patients. In one patient, theadditional finding of two natal teeth was observed.Congenital flexion contractures were found in all ofthem and included ulnar deviation of the fingers inthe IP and MP joints, fixed wrists and elbows withoverlying dimples, equinovarus position of the feet,and contractures (both flexion and extension) of theknee joints. Webbing of the neck and progressiveaxillary webbing were also present in all livingpatients. Scoliosis developed between the ages oftwo and three years in the living patients and hasbeen progressive in nature. No vertebral defectswere found. Episodes of malignant hyperthermiaoccurred in both patients from family 1 undergeneral anaesthesia. The other two patients eitherdid not have surgery or exposure to anaesthesia orpreventive precautions have been taken. Intellectualand motor development appeared to be normal inthe living patients. Two patients had developedconductive hearing loss, possibly related to chronicofitis, and one patient had an episode of apnoea.Muscle biopsies were performed in two patients andrevealed no specific myopathic changes, but mildneuropathic changes. Neuropathological examina-tion at necropsy in one patient showed atrophy ofmuscle fibres consistent with anterior horn cell loss.
TABLE 1 Summary of clinical findings.
Patient I Patient 2 Patient 3 Patient 4
Sex M F M MAge at last examination 4 y 2 y 36 wk gest 19 mthPlagiocephaly + + + +Ptosis + + (+)Facial asymmetry + + +Torticollis + + + +Long philtrum + + + +Scoliosis + + +Birth (wk) 41 41 36 TermBirth weight (g) 365(0 (50%) 33(J) (50%) 2310 (25%) 28()0 (25%)<5% length + + - +Pectus excavatum + - +IQ n n nDecreased muscle mass + + + +Anterior horn cell loss ? ? + ?Malignant hyperthermia + +Long, tapering fingers + + + +Flexion contractures (elbows) - - + +
(wrists) + +(knees) + + Extended +(ankles) + + +(hips) + + + +
Camptodactyly + + + +Pes equinovarus + + + +Neck webbing + + + +Axillary webbing + + +Cleft palate + +Deviated nose - + +Small mandible + + + +Hearing loss + +Low set ears, posteriorly rotated + + +
109
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

U G Froster-Iskenius, J R Waterson, and Judith G Hall
Discussion
In the two sibships reported here congenital contrac-tures are associated with a unique pattern ofanomalies, the most striking of which are torticollisand malignant hyperthermia.
Torticollis is a fixed contraction of the neckmuscles, usually occurring at or around the time ofbirth. It primarily involves the sternocleidomastoidmuscle or those muscles supplied by the spinalaccessory nerve. The persistent muscle contractionin the neck leads to rotation of the head to one sidesuch that the chin points to the opposite side fromthe contracted muscle. The frequency of congenitaltorticollis is estimated at between 4/1000 to1/150 000.1 Different aetiological factors have beenconsidered, including birth injuries, abnormal in-trauterine position, infectious vascular disturbances,and neurogenic causes.2 It is not entirely clearwhether torticollis usually begins before birth oroccurs because of the birth process. Familial occurr-ence of congenital torticollis has been reported, butappears to be rare.3 Associated anomalies arecommon with torticollis. The most frequent is hipdysplasia, occurring in 14-8 to 20% of cases oftorticollis. Other problems frequently mentionedinclude club foot, pyloric stenosis, seizures, andmental retardation. Cleft palate and natal teethhave been reported in one patient with congenitaltorticollis without further detailed description of thephysical findings.5 Among the associated anomaliesfrequently observed and thought to be secondary tothe torticollis are asymmetry of the face and skull,including flattening of the frontal prominence of theaffected side of the head, epicanthic folds, and shorteyebrows. Plagiocephaly and facial asymmetry areseen in 15 to 100% of patients with torticollis andmay be caused by late intrauterine moulding of thehead' or as a consequence of pressure after birth. Inthe four patients described here, the plagiocephaly,flattening, and asymmetry of the face may well bethe consequence of what can be called the 'torticollissequence', that is, they are secondary to thepersistent contracture of the neck muscles that arepart of the torticollis condition itself.
In the two sibships reported here congenitaltorticollis was associated with other facial anoma-lies, congenital contractures of the limbs, webbingof the neck and axillary region, and, in two patients,with episodes of malignant hyperthermia. The facialanomalies in these patients include ptosis of theeyelids, downward slanting palpebral fissures,downturned corners of the mouth, long philtrum,micrognathia, cleft palate, prominent alveolarridges, natal teeth, and an overall myopathic facialexpression. All of these facial anomalies cannot
satisfactorily be explained as a consequence of thetorticollis but rather appear to be part of the specificcondition we are reporting. Muscle weakness ofprenatal onset could explain many of the facialfindings in these children and could possibly havepredisposed to torticollis developing before or atbirth.The congenital contractures in our patients in-
clude ulnar deviation of the fingers at the IP and MPjoints, contractures of the wrists and elbows withoverlying dimples, contractures of the feet andankles (primarily equinovarus position of the feet),and contractures of the hips and knees. Later in lifewebbing of the neck, but also in the axillary and theinguinal regions, as well as progressive scoliosis,have developed in the three living patients. Whilescoliosis with webbing of cervical vertebrae has beendescribed in patients with torticollis,7 x rays of thespine in our patients did not reveal vertebralanomalies.Among conditions with congenital contractures
and pterygia, at least five separate groups have beendescribed.8 Progressive scoliosis together with con-genital contractures and pterygia across joints in theneck region are found in some patients with theautosomal recessive multiple pterygium syndrome.Patients with the multiple pterygium syndrome showprogressive axillary and neck webbing and progres-sion of the contractures, as well as myopathic facialexpression, ptosis of the eyelids, and overall muscu-lar wasting. Normal intelligence and lack of specificmyopathic changes in muscle biopsy are additionalsimilarities of the condition described here with themultiple pterygium syndrome. However, in patientswith the multiple pterygium syndrome, webbinginvolves most major joints, including the elbows andpopliteal and inguinal region, while in our twosibships webbing has been limited to the neck,axillary, and inguinal regions. Furthermore, thecontractures in our patients appear to be less severeand more responsive to physical therapy and bracingtherapy than usually seen in multiple pterygiumsyndrome. However, all our patients are young, lessthan five years old, and pterygia formation mayincrease with age and progression of muscle wasting.Nevertheless the presence of torticollis and malig-nant hyperthermia without vertebral anomalies sug-gests that our patients represent a distinct entity.
Malignant hyperthermia was mentioned in apatient with congenital contractures,9 but has notbeen a reported feature of the multiple pterygiumsyndrome. Episodes of malignant hyperthermiaoccurred with anaesthesia in the two sibs of family 1.The other living patient had not been exposed toanaesthesia, as preventive precautions were takenbeforehand. Malignant hyperthermia, which is
110
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

A recessive form ofcongenital contractures and torticollis associated with malignant hyperthermia
characterised by a marked rise in body temperature,rigidity of muscle, cardiac arrhythmia, and furthermetabolic abnormalities, is often triggered by in-halational and muscle relaxing drugs but also bysome anaesthetics. Occasionally it can also be aresponse to physical or emotional stress. Perhapsbirth represented such a stress to patient 3, althoughno rise in body temperature was reported before orat birth.
Incidence figures for malignant hyperthermiarange between 1 in 10 000 to 1 in 100 000 inresponse to general anaesthesia. "' Malignant hyper-thermia can occur as an isolated autosomal domi-nant trait but it has also been observed in severaldifferent muscle diseases such as muscular dystro-phy and central core disease." 12 Non-specificmyopathic abnormalities in muscle biopsies frompatients with malignant hyperthermia or at risk for itare commonly found.' (CK is otten raised inasymptomatic subjects, so it is of interest that two ofour patients actually have low CK levels.A well documented condition of malignant hyper-
thermia and a progressive myopathy has beenreported as King's syndrome.'4 This disorder pre-sents with short stature, kyphoscoliosis, pectuscarinatum, hypoplastic mandible, ptosis, epicanthicfolds, undescended testes in the male, and a slowlyprogressive myopathy. Both male and female pa-tients have been described. 15 16 Raised CK levels inother family members and a mild myopathy in twoprevious generations in one family suggest a domi-nant mode of inheritance with possible reducedpenetrance in King's syndrome.'6 Several featuresdistinguish the condition described here from King'ssyndrome; the most prominent are the congenitalcontractures, congenital torticollis, and progressivedevelopment of webbing.The findings in our patients are different from
features seen in King's syndrome and the multiplepterygium syndrome (table 2). We suspect that weare observing a new and distinct condition; thepathogenesis, however, is not yet clear. Sincepersons of both sexes are affected in family 1, andthe parents do not show features of the disorder, anautosomal recessive mode of transmission is cer-tainly possible, even though there is no consanguinityin either family. In both families no unaffected childhas been born after the affected children and both ofthe first affected children followed either a termina-tion of pregnancy or a spontaneous abortion. Thismakes an environmental factor aetiologically possi-ble; however, no common drug, infection, orprenatal exposure to any common agent could beidentified.The clinical findings of prenatal onset of contrac-
tures, progressive muscular wasting, myopathic
TABLE 2 Comparison of features with King's syndromeand multiple pterygium syndrome
King's Miultiple Patients 1-4svndrome ptervgium
syndronte
Ptosis + + +Lordosis + + +Nasal speech + + + (3/4)Otitis media + ? + (2/4)Downward slanting (+) + + (1/4)
palpebral fissuresMicrognathia + + +Kyphoscoliosis + + with vertebral +
abnormalitiesShort stature + + +Asymmetrical face + from - +
pictureMidface hypoplasia + - +Raised CK + (+)Malignant hyperthermia + (+) + (2/4)Motor development
slightly retarded + (+) + (3/4)Webbing across joints - + +Contractures - + +Torticollis ? - +Low set ears + - +Pectus carinatus + + + (2/4)Cryptorchidism + + + (2/3)Muscular weakness + + +Renal anomalies - - + (1/4)Multipie cutaneous naeviVaricose veinsEarly dental caries '? ? +Normal 10 + + +
facies, episodes of malignant hyperthermia, andanterior horn cell loss in one patient are compatiblewith either an underlying neuropathic process or amyopathic disorder of prenatal onset, even thoughmuscle biopsies did not show specific changes of aknown myopathy.A maternal factor which would lead to the
destruction of fetal muscle tissue in utero withretrograde loss of anterior horn cells is anotheraetiological consideration. Such a factor could bedue to either a circulating antibody or a humoralfactor. Alternatively, maternal stress such as fevercould, in a fetus who had inherited a gene formalignant hyperthermia from the father, lead to anepisode of intrauterine malignant hyperthermia withdestruction of muscle tissue in utero. However, noevidence for malignant hyperthermia is present ineither father, and no episode of fever duringpregnancy was reported in the mothers.With regard to the management of patients with
this type of congenital contractures, it is importantto point out that real time ultrasound investigationsperformed in mid-trimester in patient 2 of family 1failed to diagnose an affected child before birth.This suggests that decreased intrauterine movementcould not be distinguished early enough in preg-nancy to make a diagnosis prenatally, even though the
ill
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from

U G Froster-Iskenius, J R Waterson, and Judith G Hall
pattern of anomalies present at birth clearly speaksfor a prenatal onset of the disorder. Nevertheless,we would strongly recommend prenatal real timeultrasound evaluations in any such family in thefuture, since ultrasound technology is continuing toimprove all the time. Specific precautions beforeanaesthesia in patients with torticollis and congeni-tal contractures in a pattern similar to these patientsappears to be an appropriate recommendation toavoid precipitating unexpected episodes of malig-nant hyperthermia in patients who require surgery.
. In summary, the families presented here appearto represent a new form of arthrogryposis probablyoccurring as an autosomal recessive trait. Thepresence of torticollis in patients with congenitalcontractures should raise suspicion of this diagnosis.Because of the possibility of malignant hyperther-mia, care should be taken during surgery or fever forany patients who have a similar phenotype.
U G Froster-Iskenius was supported by a grantfrom the Deutsche Forschungsgemeinschaft Fr 653/1-2. The March of Dimes has supported this work inpart. The authors acknowledge the help of DrsDiane Lindner, Ute Ochs, Steve Chentow, JoelHaas, Susan Reed, David Shurtleff, and PatriciaHayden, and Ms Melanie Pepin.
References
McDaniel A, Hirsch BE, Kornglut AD, Armbustuaches VM.Torticollis in infancy and adolescence. Ear Nose Throat J1984;63:478-87.
2 Lidge RT, Bechtol RC, Lambert CN. Congenital musculartorticollis. J Bone Joint Surg (Ain) 1957;39:1165-82.
3Barenfeld PA, Weseley MS. Congenital muscular torticollis:case reports in siblings. Bull Hosp Joint Dis 1963;24:130-4.Hummer CD, MacEwen GD. The coexistcncc of torticollis andcongenital dysplasia of the hip. J Bonie Joinit Surg (Amn)1972;54:1255-6.
5 Isigbert E. Uuteosuchungen uber die Hereditat orthopadischevLeiden. III. De aujeborene Scichis. Arch Orthop Unfallchir1931;30:459-94.
6 Clarren SK, Smith DW, Hanson JW. Helmet treatmcnt forplagiocephaly and congenital muscular torticollis. J Pediatr1979;94:43-6.
7Oh 1, Nowacek CJ. Surgical release of congenital torticollis inadults. Clin Orthop 1978;131:141-5.Hall JG, Reed SD, Rosenbaum KN, Gershanik J, Chen H,Wilson KM. Limb pterygium syndromes: a review and report ofeleven patients. Am J Med Genet 1982;12:377-409.Relton YES. Malignant hypothermia - anaesthetic tcchniquesand agents. In: Britt BA, ed. International Symposium onMalignant Hyperthermia. New York; Grune & Stratton, 1973.Denborough MA, Galloway GJ, Hopkinson KC. Malignanthyperpyrexia and sudden infant death. Lancet 1982;ii:1068-9.Willner J. Malignant hyperthermia. Pediatr Ann 1984;13:128-34.
2 Kelfer HM, Singer WD, Reynolds RN. Malignant hyperthermiain a child with Duchenne muscular dystrophy. Pediatrics1983;71:118-9.
13 Brownell AKW, Paasukc RT, Elash A, et al. Malignanthyperthermia in Duchenne muscular dystrophy. Anesthesiology1983;58:180-2.
4 King JO, Denborough MA. Anesthetic-induced malignanthyperpyrexia in children. J Pediatr 1973;83:37-40.
5 McPherson EW, Taylor CA. The King syndrome: malignanthyperthermia, myopathy and multiple anomalies. Am J MedGenet 1981;8:159-65.
6 Saul RA, Stevenson RE, Roberts TL. A female with the Kingsyndrome in a family with elevated CPK levels. Proc Green-wood Genet Center 1984;3:7-10.
Correspondence and requests for reprints toProfessor Judith G Hall, Department of MedicalGenetics, Clinical Genetics Unit, University ofBritish Columbia, 4490 Oak Street, Vancouver,British Columbia, Canada V6H 3V5.
112
copyright. on A
ugust 31, 2021 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.2.104 on 1 F
ebruary 1988. Dow
nloaded from