Embed Size (px)
Citation preview
Plantar Fasciitis:Plantar Fasciitis: Nonsurgical & Surgical Options for Nonsurgical & Surgical Options for Chronic Heel PainChronic Heel Pain
Mathew M. John, DPM, FACFASMathew M. John, DPM, FACFASAtlanta, GAAtlanta, GA
Heel Pain:Plantar fasciitisHeel Pain:Plantar fasciitis
Over 2 million Over 2 million Americans suffer Americans suffer from heel painfrom heel painMost common Most common cause of plantar cause of plantar heel painheel pain
AnatomyAnatomy
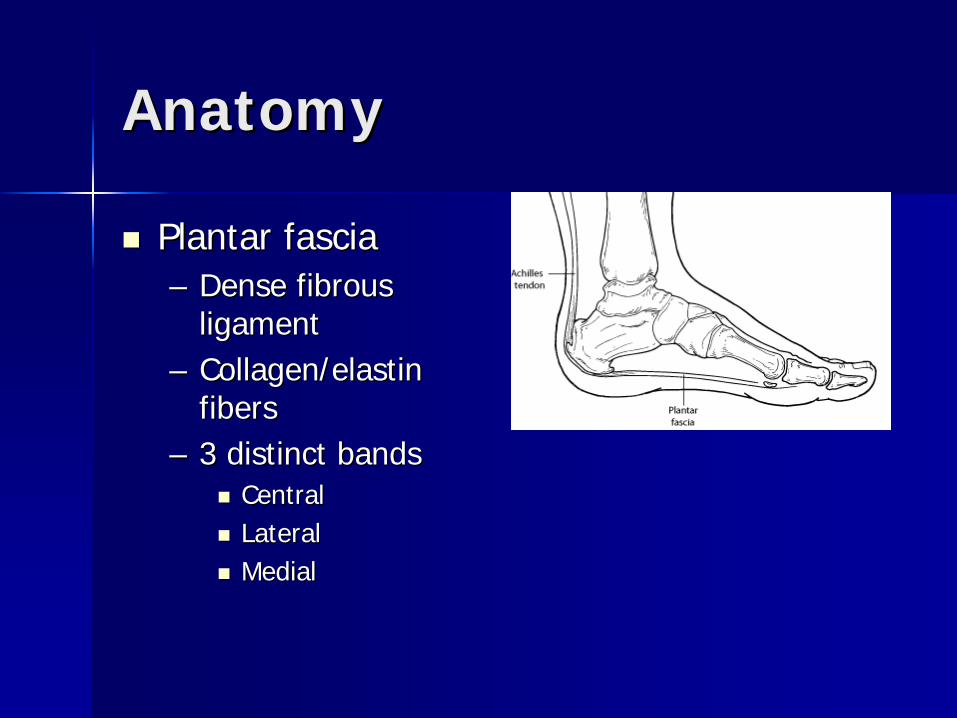
Plantar fasciaPlantar fascia–– Dense fibrous Dense fibrous
ligamentligament–– Collagen/elastin Collagen/elastin
fibersfibers–– 3 distinct bands3 distinct bands
CentralCentralLateralLateralMedialMedial

AnatomyAnatomy
Plantar fasciaPlantar fascia–– OriginOrigin
Medial calcaneal Medial calcaneal tuberositytuberosity
–– InsertionInsertionFlexor tendons / Flexor tendons / base proximal base proximal phalanxphalanx
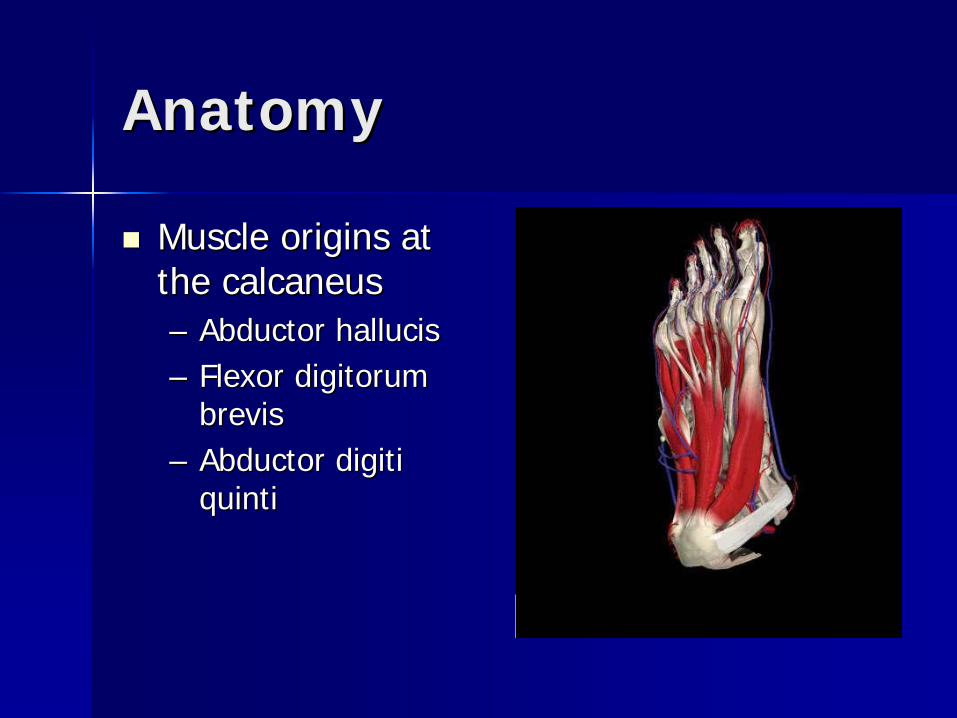
AnatomyAnatomy
Muscle origins at Muscle origins at the calcaneusthe calcaneus–– Abductor hallucisAbductor hallucis–– Flexor digitorum Flexor digitorum
brevisbrevis–– Abductor digiti Abductor digiti
quintiquinti

AnatomyAnatomy
Origins near Origins near calcaneal tuberositycalcaneal tuberosity–– Quadratus plantaeQuadratus plantae–– Long plantar Long plantar
calcaneocuboid calcaneocuboid ligamentligament

AnatomyAnatomy
Subcalcaneal bursaSubcalcaneal bursa–– Between the Between the
calcaneal tuberosity calcaneal tuberosity and fat padand fat pad

AnatomyAnatomy
Tibial nerveTibial nerve–– Medial Calcaneal Medial Calcaneal
nervenerve–– Lateral plantar Lateral plantar
nervenerve11stst branchbranch
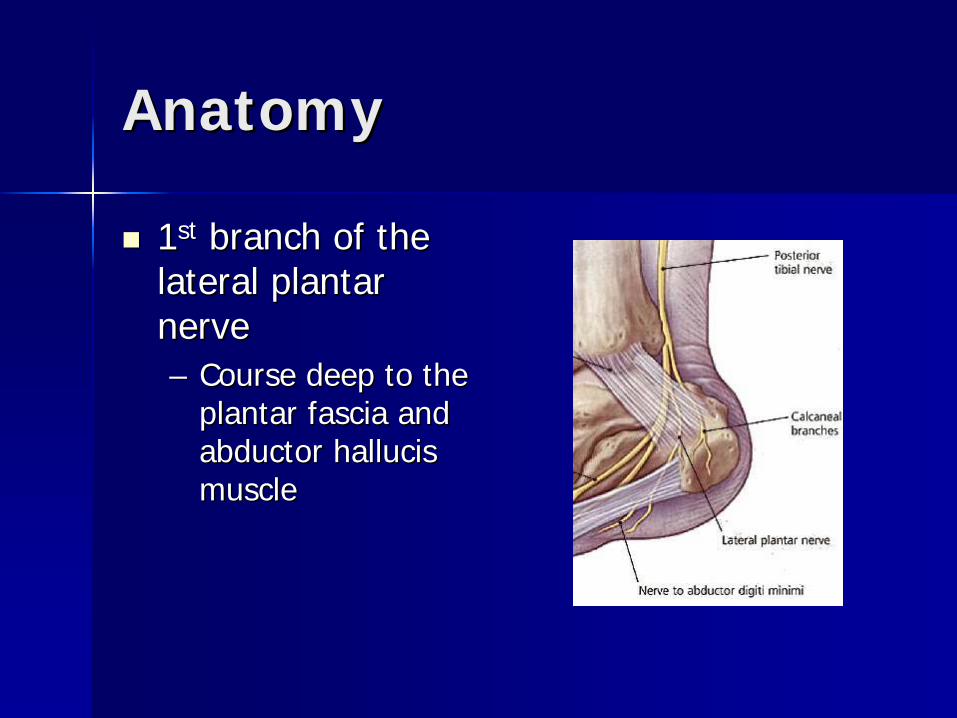
AnatomyAnatomy
11stst branch of the branch of the lateral plantar lateral plantar nervenerve–– Course deep to the Course deep to the
plantar fascia and plantar fascia and abductor hallucis abductor hallucis musclemuscle

Basic BiomechanicsBasic Biomechanics
100100--200% of body 200% of body weight with each weight with each heel strikeheel strikeWindlass Windlass mechanismmechanism

Basic BiomechanicsBasic Biomechanics
Windlass Windlass MechanismMechanism–– Dorsiflexion of the Dorsiflexion of the
halluxhallux–– Elevation of the Elevation of the
longitudinal archlongitudinal arch–– Midfoot lockedMidfoot locked
SymptomsSymptoms
Pain with prolonged Pain with prolonged standing or walking standing or walking or exerciseor exerciseNo specific traumaNo specific traumaDeep acheDeep acheOccasional Occasional burning/throbbingburning/throbbingRelief with restRelief with rest

SymptomsSymptoms
Post static dyskinesiaPost static dyskinesia–– Pain with initial Pain with initial
weightbearing after weightbearing after restrest
–– Initially improves but Initially improves but returns later in the dayreturns later in the day
SymptomsSymptoms
Chronic painChronic pain–– Typically >6 moTypically >6 mo
Plantar fasciosisPlantar fasciosis–– Pain constant with Pain constant with
weightbearingweightbearing–– Antalgic gaitAntalgic gait
Chronic vs. Acute PainChronic vs. Acute Pain
Plantar FasciosisPlantar Fasciosis–– Decreased edemaDecreased edema–– NoninflammatoryNoninflammatory–– Localized fibrosisLocalized fibrosis–– Collagen necrosisCollagen necrosis–– Fibroblastic Fibroblastic
hyperplasiahyperplasia
Plantar fasciitisPlantar fasciitis–– Localized edemaLocalized edema–– InflammationInflammation–– Microtearing of Microtearing of
fasciafascia–– Insertional Insertional
thickening of fasciathickening of fascia
Associated symptomsAssociated symptoms
Achilles tendonitisAchilles tendonitisPosterior tibial tendonitisPosterior tibial tendonitisLateral column painLateral column painLower leg muscle painLower leg muscle painKnee / back painKnee / back pain
Associated ConditionsAssociated Conditions
Pes planusPes planusPes cavusPes cavusEquinusEquinusLimb length differenceLimb length difference

Aggravating FactorsAggravating Factors
ObesityObesityRunning / aerobic Running / aerobic exerciseexerciseProlonged standing Prolonged standing on hard surfaceson hard surfacesPoor shoewearPoor shoewear
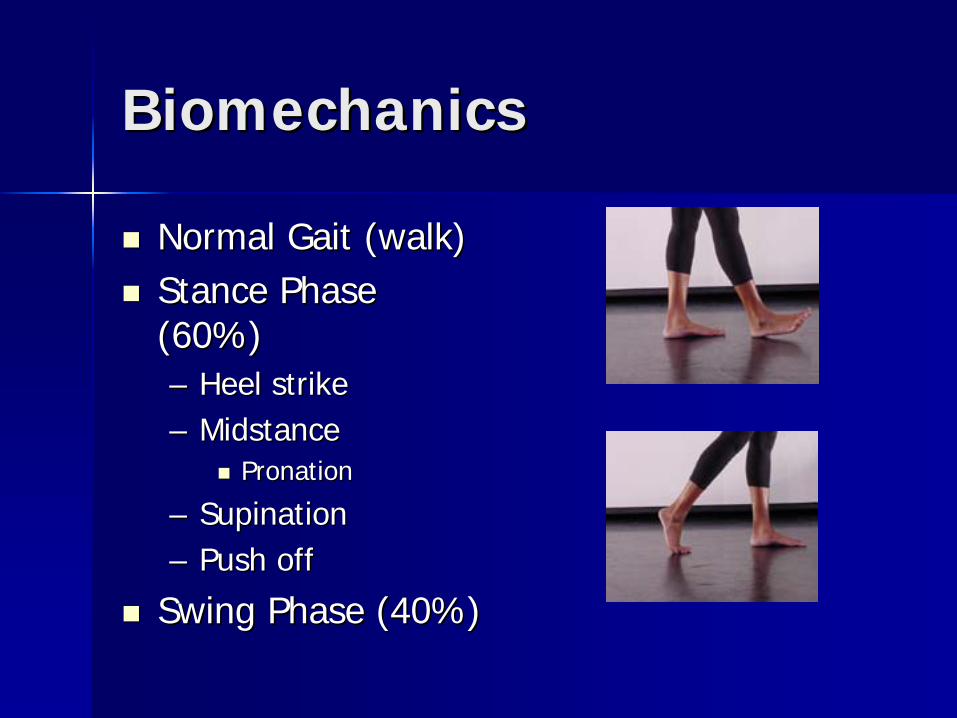
BiomechanicsBiomechanics
Normal Gait (walk)Normal Gait (walk)Stance Phase Stance Phase (60%)(60%)–– Heel strikeHeel strike–– MidstanceMidstance
PronationPronation
–– SupinationSupination–– Push offPush off
Swing Phase (40%)Swing Phase (40%)

BiomechanicsBiomechanics
EquinusEquinus–– Decreased ankle Decreased ankle
joint dorsiflexionjoint dorsiflexion<10 degrees<10 degrees
–– Compensatory Compensatory pronationpronation
Increased strain on Increased strain on plantar fascia plantar fascia ligamentligament

BiomechanicsBiomechanics
OverOver--PronationPronation–– Not Not ‘‘flat feetflat feet’’–– eversion / eversion /
dorsiflexiondorsiflexion–– Weak posterior tibial Weak posterior tibial
tendontendon–– Increased subtalar Increased subtalar
joint motionjoint motion
BiomechanicsBiomechanics
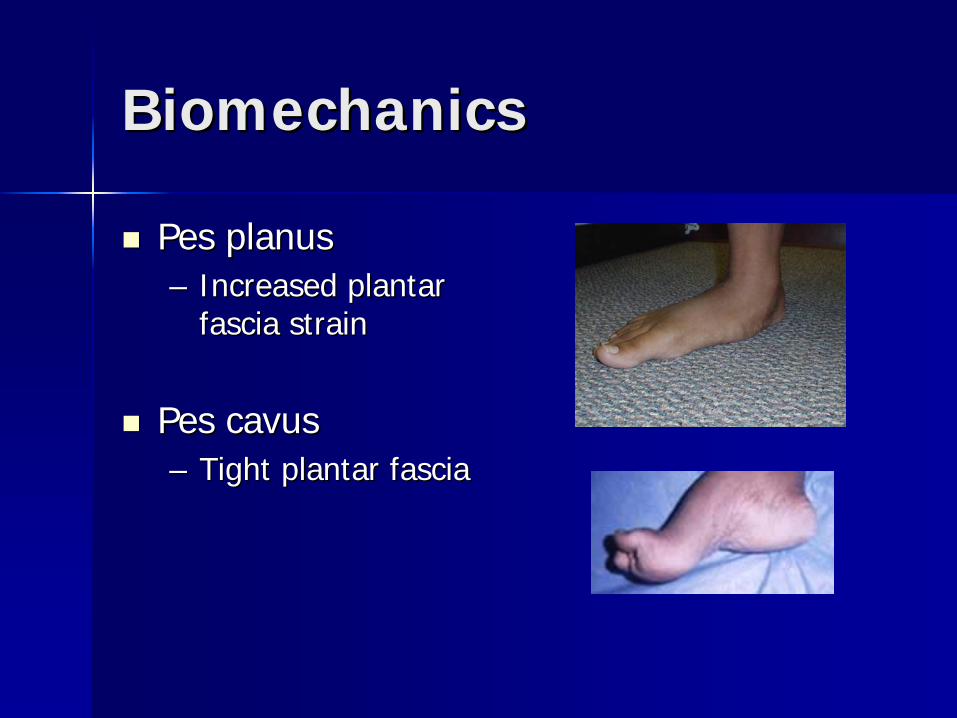
Pes planusPes planus–– Increased plantar Increased plantar
fascia strainfascia strain
Pes cavusPes cavus–– Tight plantar fasciaTight plantar fascia
Physical ExamPhysical Exam
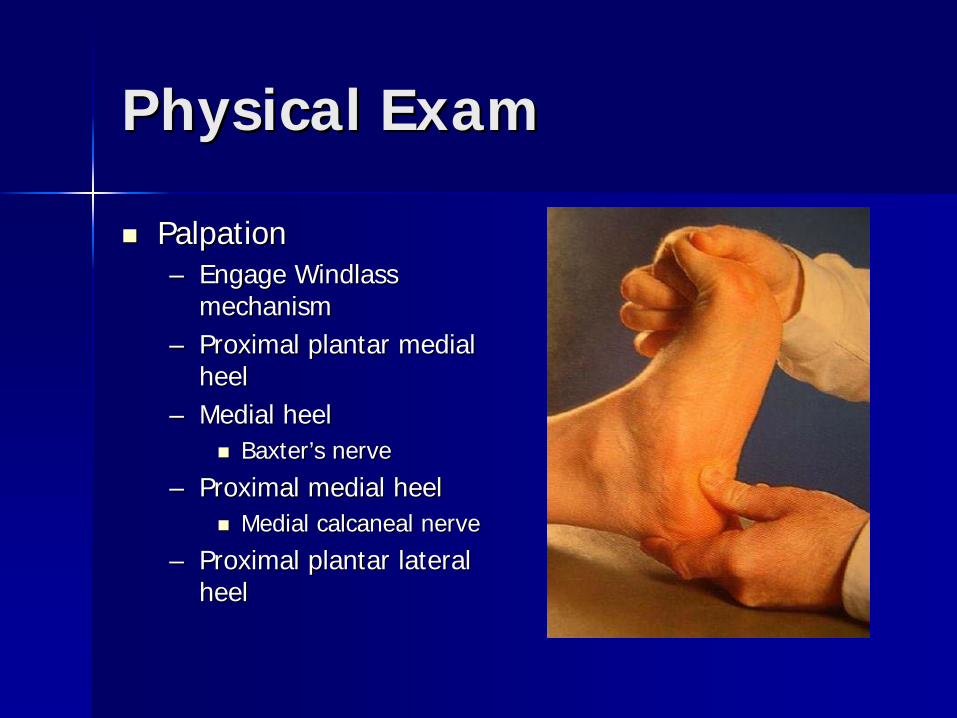
PalpationPalpation–– Engage Windlass Engage Windlass
mechanismmechanism–– Proximal plantar medial Proximal plantar medial
heelheel–– Medial heelMedial heel
BaxterBaxter’’s nerves nerve
–– Proximal medial heelProximal medial heelMedial calcaneal nerveMedial calcaneal nerve
–– Proximal plantar lateral Proximal plantar lateral heelheel

Physical ExamPhysical Exam
PalpationPalpation–– Central plantar fasciaCentral plantar fascia–– Side to side Side to side
compression calcaneuscompression calcaneus–– Central calcaneusCentral calcaneus
BursaBursa
–– Posterior tibial tendon Posterior tibial tendon insertioninsertion
NavicularNavicular
Palpate/percussionPalpate/percussion–– Tarsal tunnelTarsal tunnel

Physical ExamPhysical Exam
Range of MotionRange of Motion–– SubtalarSubtalar
inversion / inversion / plantarflexionplantarflexioneversion / eversion / dorsiflexiondorsiflexion
–– MidtarsalMidtarsal–– AnkleAnkle
dorsiflexiondorsiflexion
Physical ExamPhysical Exam
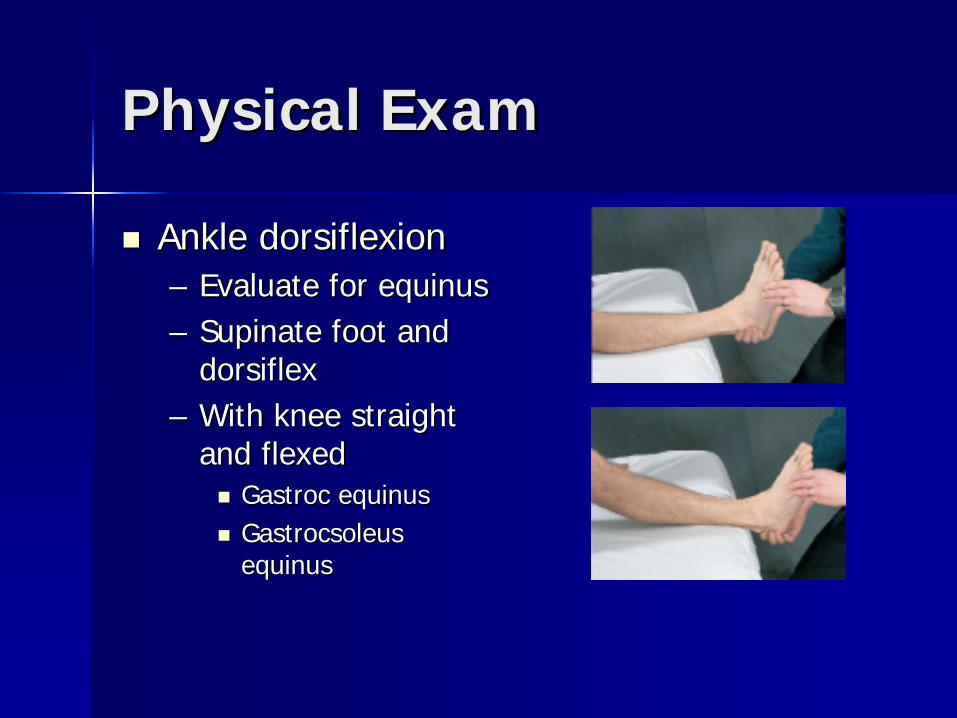
Ankle dorsiflexionAnkle dorsiflexion–– Evaluate for equinusEvaluate for equinus–– Supinate foot and Supinate foot and
dorsiflexdorsiflex–– With knee straight With knee straight
and flexedand flexedGastroc equinusGastroc equinusGastrocsoleus Gastrocsoleus equinusequinus
Physical ExamPhysical Exam
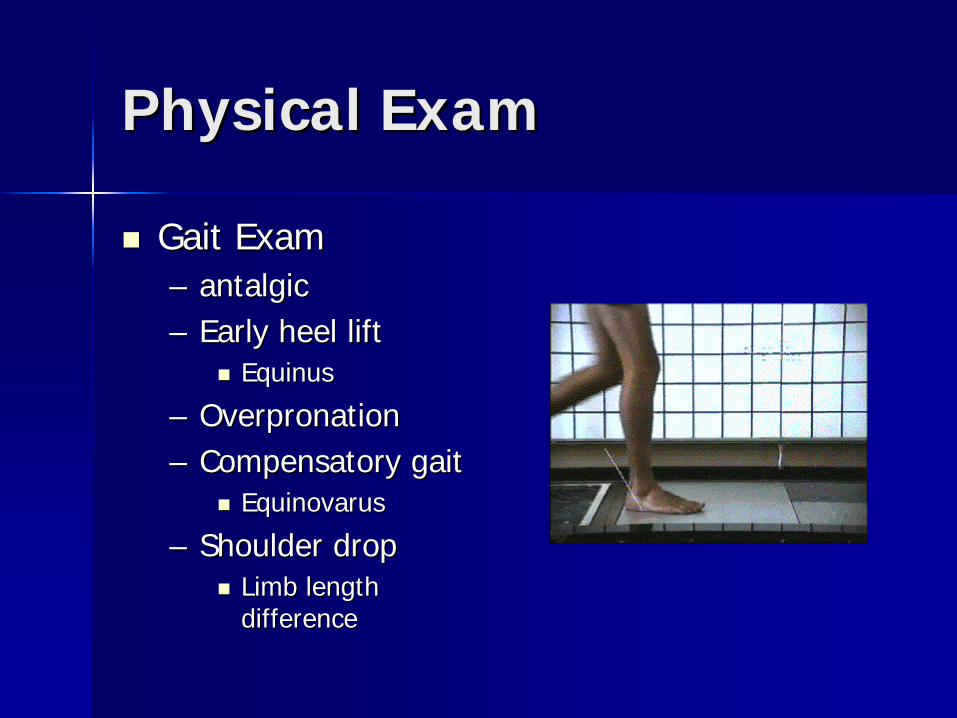
Gait ExamGait Exam–– antalgicantalgic–– Early heel liftEarly heel lift
EquinusEquinus
–– OverpronationOverpronation–– Compensatory gaitCompensatory gait
EquinovarusEquinovarus
–– Shoulder dropShoulder dropLimb length Limb length differencedifference
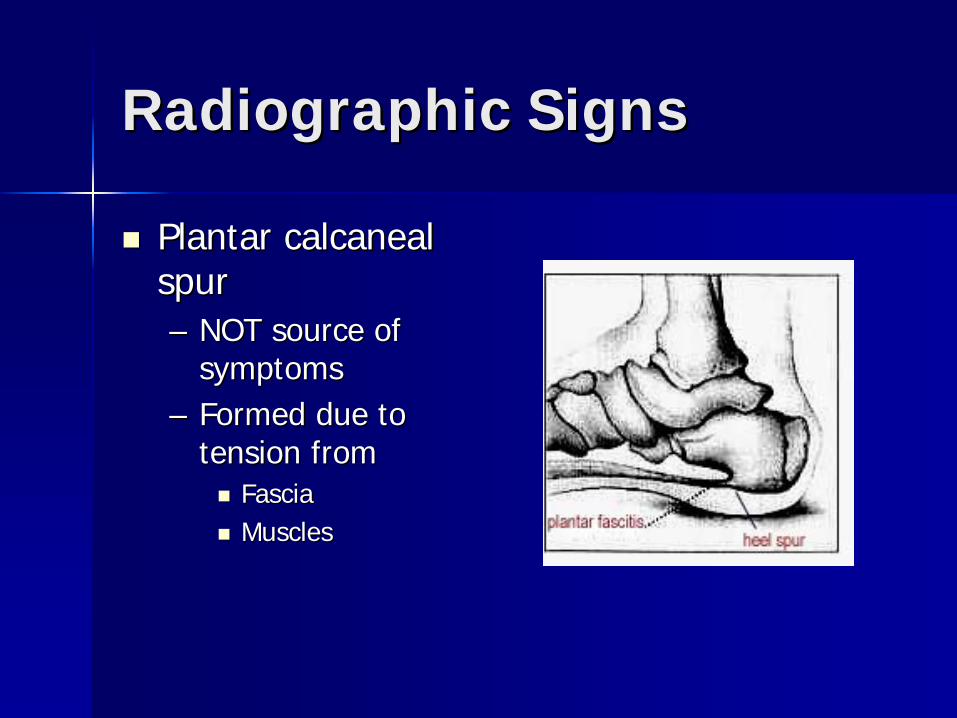
Radiographic SignsRadiographic Signs
Plantar calcaneal Plantar calcaneal spurspur–– NOT source of NOT source of
symptomssymptoms–– Formed due to Formed due to
tension fromtension fromFasciaFasciaMusclesMuscles

Radiographic SignsRadiographic Signs
Plantar calcaneal Plantar calcaneal spurspur–– Present in over 50% Present in over 50%
of patients who of patients who suffer from PFsuffer from PF
–– Also present in Also present in asymptomatic asymptomatic patientspatients
Other Diagnostic TestsOther Diagnostic Tests
Bone scanBone scanMRIMRIUltrasoundUltrasound

Bone ScanBone Scan
4 phase 4 phase TechnetiumTechnetium–– Increased uptake:Increased uptake:
Calcaneal fracturesCalcaneal fracturesInfectionInfectionBone tumorsBone tumors
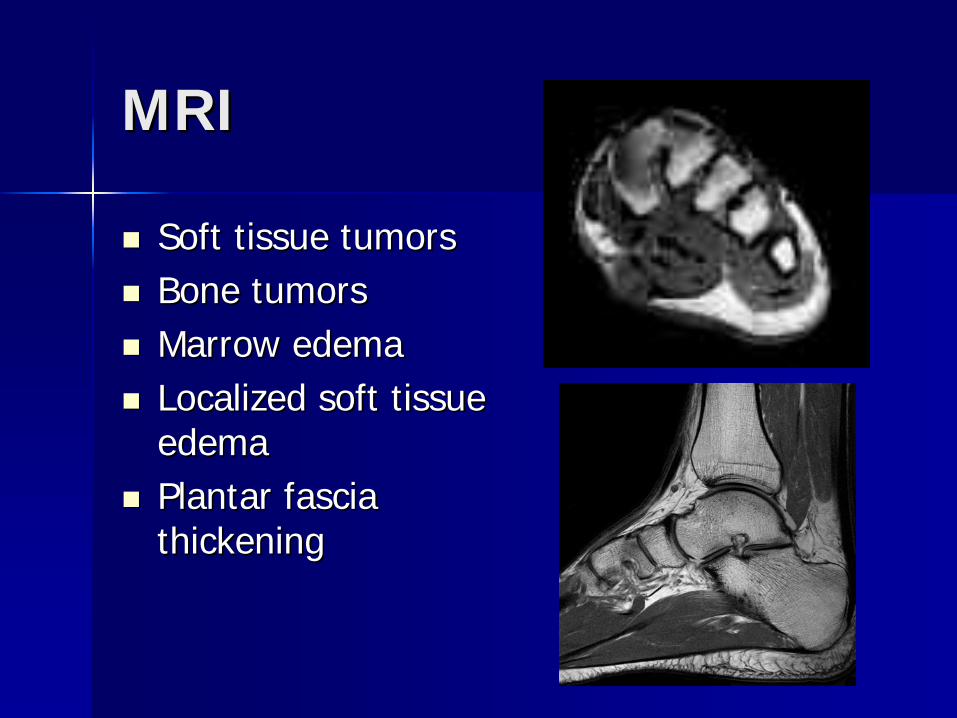
MRIMRI
Soft tissue tumorsSoft tissue tumorsBone tumorsBone tumorsMarrow edemaMarrow edemaLocalized soft tissue Localized soft tissue edemaedemaPlantar fascia Plantar fascia thickeningthickening

Magnetic Resonance Magnetic Resonance Imaging Imaging --MRIMRI
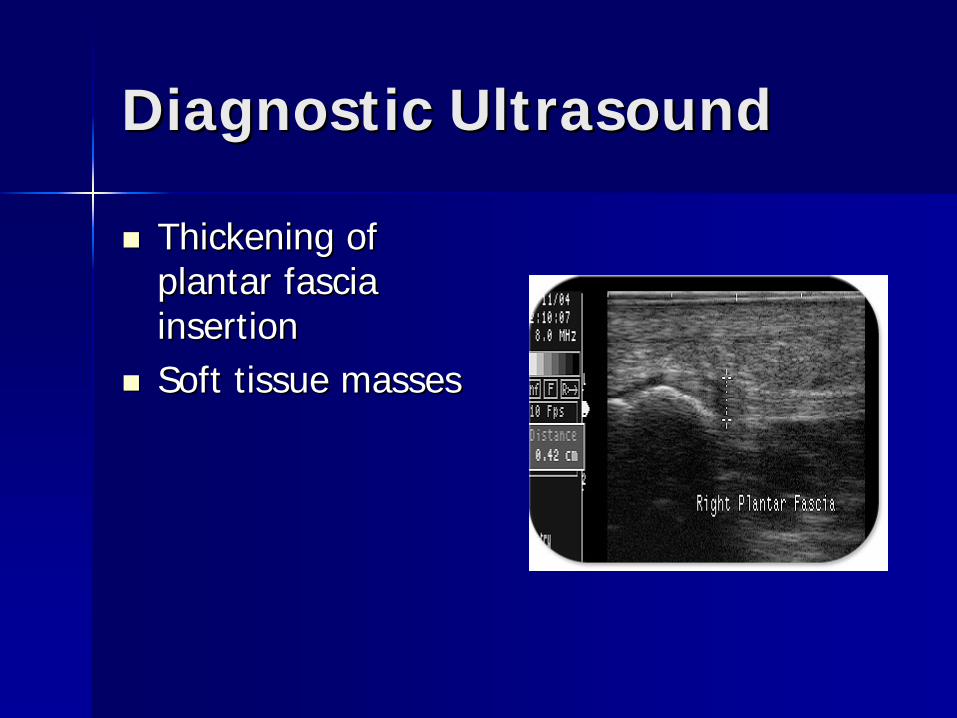
Diagnostic UltrasoundDiagnostic Ultrasound
Thickening of Thickening of plantar fascia plantar fascia insertioninsertionSoft tissue massesSoft tissue masses

Diagnostic UltrasoundDiagnostic Ultrasound

Diagnostic UltrasoundDiagnostic Ultrasound

Diagnostic TestsDiagnostic Tests
Help to identify differential diagnosesHelp to identify differential diagnosesDiagnosis of plantar fasciitis mainly Diagnosis of plantar fasciitis mainly clinicalclinicalDoes not dictate treatment Does not dictate treatment management of plantar fasciitismanagement of plantar fasciitis
Differential DiagnosesDifferential Diagnoses
Calcaneal apophysitisCalcaneal apophysitisCalcaneal bursitisCalcaneal bursitisTarsal tunnel syndromeTarsal tunnel syndromeCalcaneal stress fractureCalcaneal stress fractureInflammatory arthritisInflammatory arthritisSoft tissue or bone neoplasmSoft tissue or bone neoplasmInfectionInfectionLower lumbar radiculopathyLower lumbar radiculopathyNeuritisNeuritis
Calcaneal ApophysitisCalcaneal Apophysitis
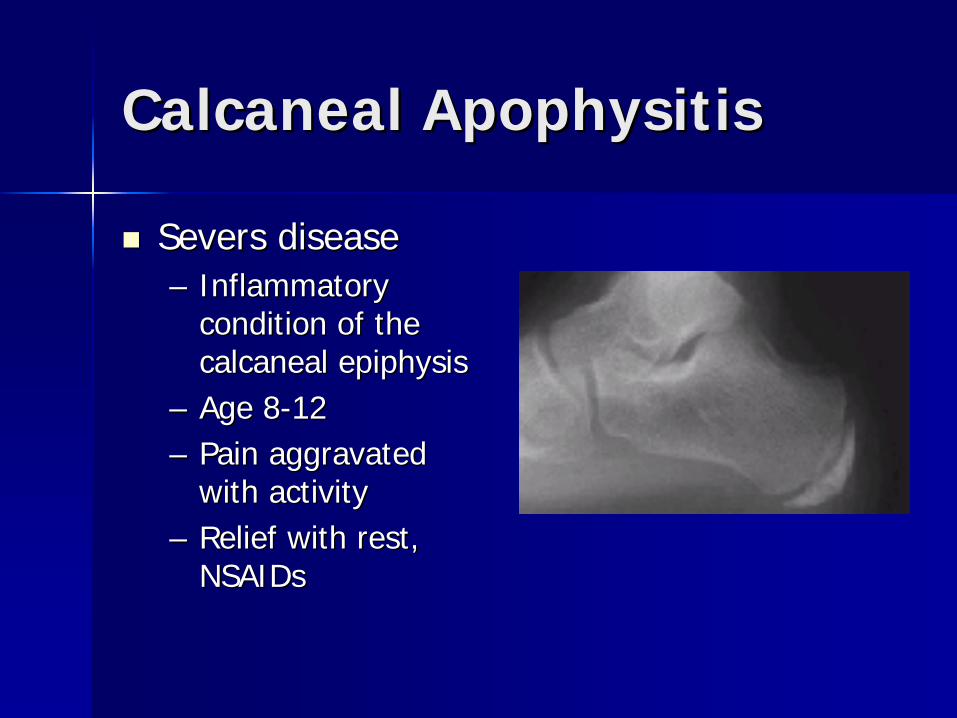
Severs diseaseSevers disease–– Inflammatory Inflammatory
condition of the condition of the calcaneal epiphysiscalcaneal epiphysis
–– Age 8Age 8--1212–– Pain aggravated Pain aggravated
with activitywith activity–– Relief with rest, Relief with rest,
NSAIDsNSAIDs
Calcaneal BursitisCalcaneal Bursitis
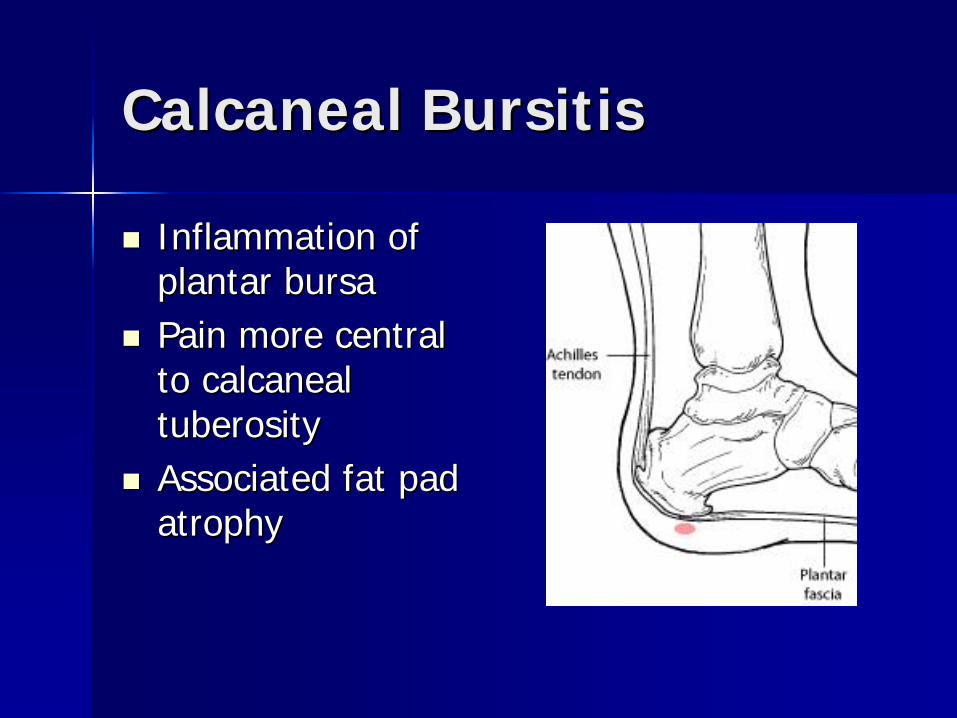
Inflammation of Inflammation of plantar bursaplantar bursaPain more central Pain more central to calcaneal to calcaneal tuberositytuberosityAssociated fat pad Associated fat pad atrophyatrophy

Tarsal Tunnel SyndromeTarsal Tunnel Syndrome
Compression of Compression of neurovascular neurovascular structures in tarsal structures in tarsal tunneltunnelPain at the tarsal Pain at the tarsal tunneltunnelRadiating to medial Radiating to medial heel and archheel and archPain constantPain constant

Calcaneal Stress FractureCalcaneal Stress Fracture
Pain with side to Pain with side to side compression of side compression of the calcaneusthe calcaneusAxial calcaneal Axial calcaneal radiographradiographBone scanBone scan
Inflammatory ArthritisInflammatory Arthritis
Rheumatoid arthritisRheumatoid arthritisPsoriatic arthritisPsoriatic arthritisGoutGout–– Acute pain/swellingAcute pain/swelling
Reiter's syndromeReiter's syndrome–– Conjunctivitis/urethritis/arthritisConjunctivitis/urethritis/arthritis
Ankylosing spondylitisAnkylosing spondylitisSystemic lupus erythematosus(SLE)Systemic lupus erythematosus(SLE)

Bone NeoplasmsBone Neoplasms
Aneurysmal bone Aneurysmal bone cystcystUnicameral bone Unicameral bone cystcystOsteoid osteomaOsteoid osteoma–– Night painNight pain
ChondroblastomaChondroblastoma

Soft tissue neoplasmSoft tissue neoplasm
Plantar fibromaPlantar fibromaNeurilemomaNeurilemomaAngiolipomaAngiolipomaFibrolipoma Fibrolipoma FibrosarcomaFibrosarcoma

InfectionInfection
AbscessAbscessOsteomyelitisOsteomyelitis
SymptomsSymptoms–– Constant painConstant pain
Mild to severeMild to severe
–– ErythemaErythema–– Localized edemaLocalized edema

Lower Lumbar Lower Lumbar RadiculopathyRadiculopathy
Compression of Compression of lower lumbar lower lumbar nervesnerves–– L4L4--5, S15, S1--22
Sciatica painSciatica painNCV/EMG requiredNCV/EMG required
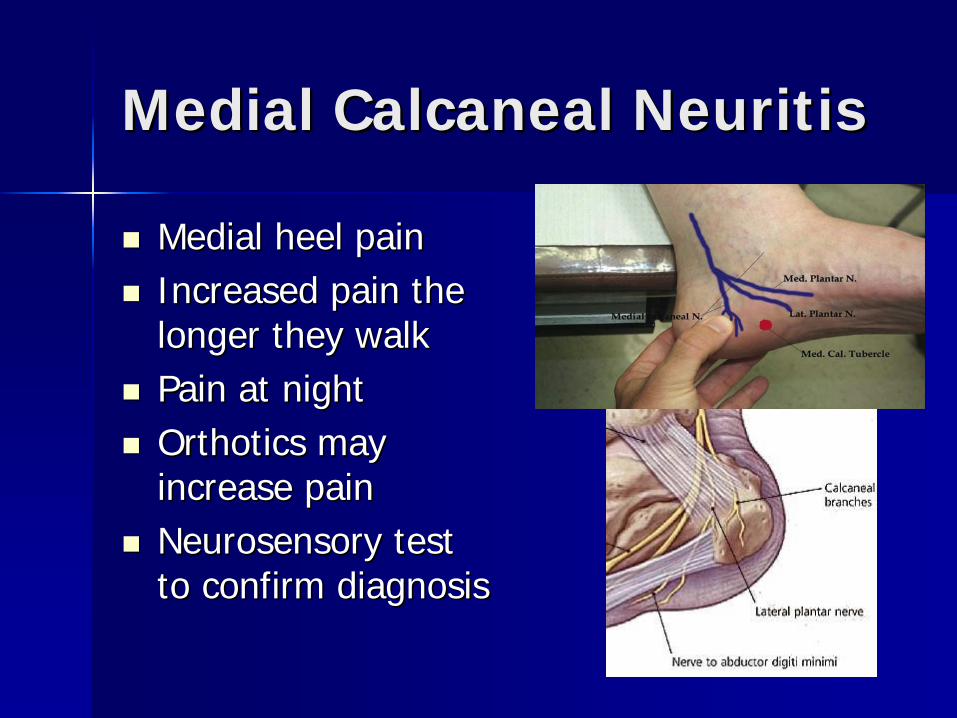
Medial Calcaneal NeuritisMedial Calcaneal Neuritis
Medial heel painMedial heel painIncreased pain the Increased pain the longer they walklonger they walkPain at nightPain at nightOrthotics may Orthotics may increase painincrease painNeurosensory test Neurosensory test to confirm diagnosisto confirm diagnosis
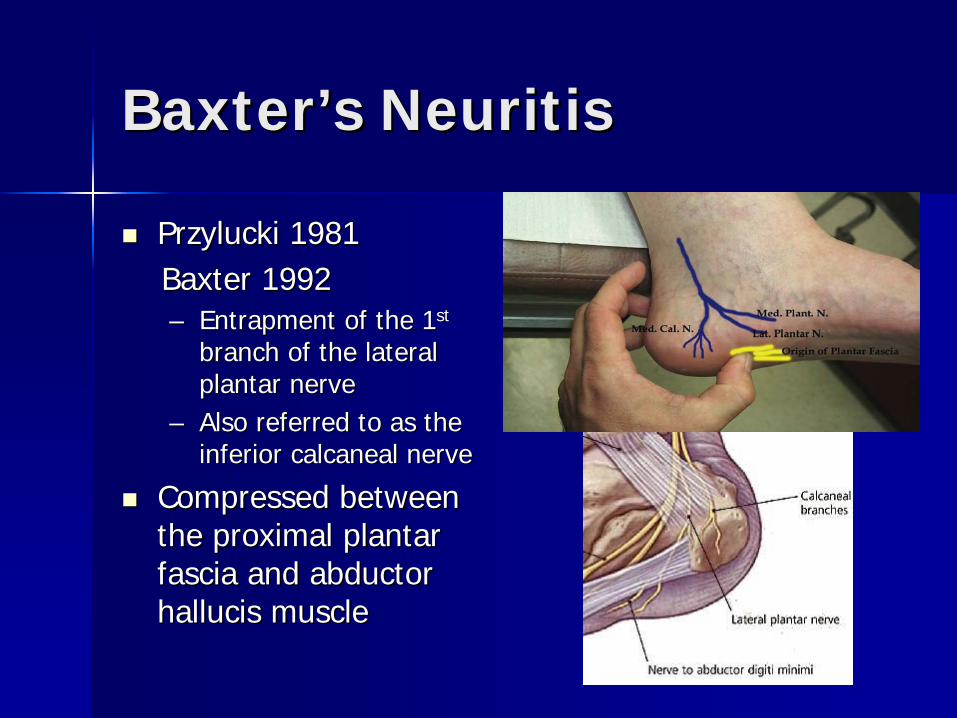
BaxterBaxter’’s Neuritiss Neuritis
Przylucki 1981Przylucki 1981Baxter 1992Baxter 1992–– Entrapment of the 1Entrapment of the 1stst
branch of the lateral branch of the lateral plantar nerveplantar nerve
–– Also referred to as the Also referred to as the inferior calcaneal nerveinferior calcaneal nerve
Compressed between Compressed between the proximal plantar the proximal plantar fascia and abductor fascia and abductor hallucis musclehallucis muscle
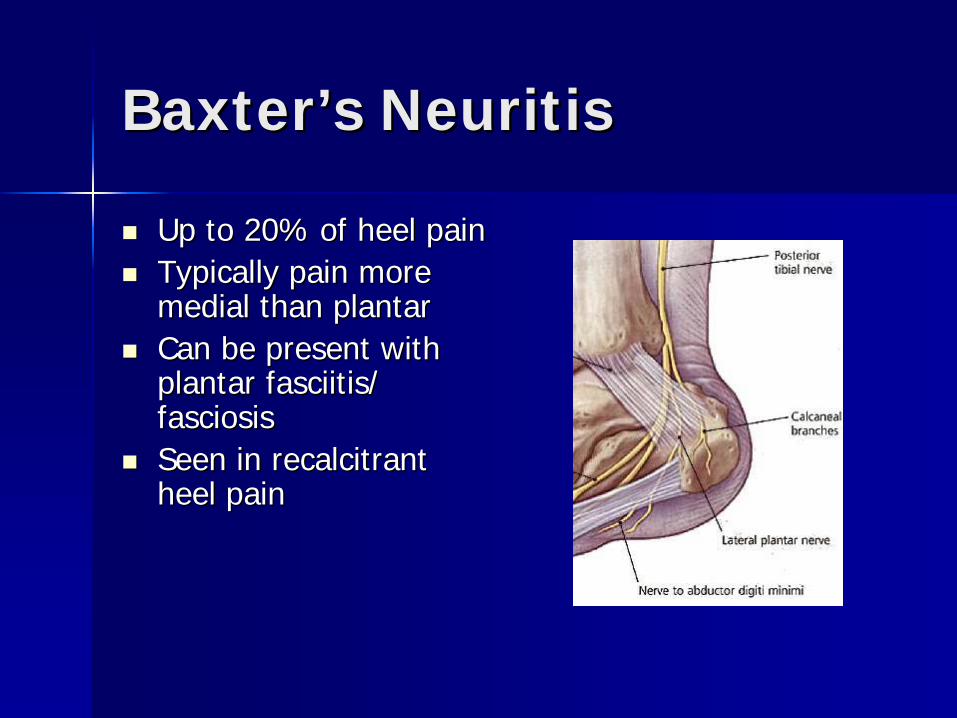
BaxterBaxter’’s Neuritiss Neuritis
Up to 20% of heel painUp to 20% of heel painTypically pain more Typically pain more medial than plantarmedial than plantarCan be present with Can be present with plantar fasciitis/ plantar fasciitis/ fasciosisfasciosisSeen in recalcitrant Seen in recalcitrant heel painheel pain

TreatmentTreatment
8585--90% success with conservative 90% success with conservative treatmenttreatment–– ACFAS Heel Pain Guide 2001ACFAS Heel Pain Guide 2001
3 phase treatment protocol3 phase treatment protocol
No one universal treatment successfulNo one universal treatment successful–– Combination of treatment optionsCombination of treatment optionsConservative treatment for at least 6 Conservative treatment for at least 6 months prior to surgical optionsmonths prior to surgical options

Treatment Treatment ––Phase 1Phase 1
NSAIDsNSAIDsStretchingStretchingcryotherapycryotherapyAppropriate shoewearAppropriate shoewear–– Athletic running shoeAthletic running shoe–– OTC arch supportOTC arch support
Padding/strappingPadding/strappingCorticosteroid injection Corticosteroid injection Activity limitationActivity limitation

Treatment Treatment –– Phase 1Phase 1
Nonsteroidal AntiNonsteroidal Anti--inflammatory Drugsinflammatory Drugs–– CelebrexCelebrex–– ibuprofenibuprofen–– diclofenacdiclofenac
Provides reduction Provides reduction of symptoms onlyof symptoms only
NSAIDsNSAIDs
Donley et al. (2007)Donley et al. (2007)–– 29 patients29 patients–– Mild improvement in Mild improvement in
overall treatment overall treatment vs. no use of NSAIDvs. no use of NSAID
Treatment Treatment –– Phase 1Phase 1
StretchingStretching–– Focused on Focused on
gastrocsoleus / gastrocsoleus / Achilles tendonAchilles tendon
–– Plantar fascia Plantar fascia ligamentligament
–– HamstringsHamstringsReduce forefoot Reduce forefoot loadingloading

Plantar Fascia StretchPlantar Fascia Stretch
DiGiovanni et al. (2003)DiGiovanni et al. (2003)–– Prospective study showed plantar fascia Prospective study showed plantar fascia
stretching to be more be more beneficial stretching to be more be more beneficial than weightbearing Achilles stretchthan weightbearing Achilles stretch
Treatment Treatment –– Phase 1Phase 1
CryotherapyCryotherapy–– Various methodsVarious methods–– TherapistTherapist’’s s
‘‘wonder drugwonder drug’’–– IntermittentIntermittent
10 min on/off/on10 min on/off/on

Treatment Treatment –– Phase 1Phase 1
Appropriate Appropriate shoewearshoewearReplace old Replace old shoewearshoewearAvoid going Avoid going barefootbarefoot
Treatment Treatment –– Phase 1Phase 1
OTC arch supportOTC arch support–– SoftSoft–– SemiSemi--flexibleflexible
Low dye strappingLow dye strapping–– With or without With or without
metatarsal padmetatarsal pad–– Plantar fascia Plantar fascia
supportsupport
Low Dye StrappingLow Dye Strapping
Landorf et al. (2005)Landorf et al. (2005)–– 65 low dye strapping65 low dye strapping–– 40 patients with no strapping40 patients with no strapping–– 33--5 days5 days–– ResultsResults
Significant improvement in pain levelsSignificant improvement in pain levels

Low Dye StrappingLow Dye Strapping
Treatment Treatment –– Phase 1Phase 1
Corticosteroid Corticosteroid injectioninjection–– Mixture of Mixture of
anesthetic/short anesthetic/short acting steroid/ long acting steroid/ long acting steroidacting steroid
–– Limited to no more Limited to no more than 3 injections to than 3 injections to one area/6 moone area/6 mo--1yr1yr
Tissue atrophyTissue atrophyPlantar fascia rupturePlantar fascia rupture
Corticosteroid InjectionCorticosteroid Injection
Reduces inflammatory response to Reduces inflammatory response to injuryinjuryInhibits leukocyte & macrophage Inhibits leukocyte & macrophage proliferationproliferationInhibits vasoactive kinin releaseInhibits vasoactive kinin releaseInhibits destructive enzyme releaseInhibits destructive enzyme releaseDecreases prostaglandin formationDecreases prostaglandin formation

Corticosteroid InjectionCorticosteroid Injection
Crawford et al. (1999)Crawford et al. (1999)–– 160 patients160 patients
Steroid + lidocaineSteroid + lidocaineTibial nerve block, steroid + lidocaineTibial nerve block, steroid + lidocaineLidocaine onlyLidocaine onlyTibial nerve block, lidocaine onlyTibial nerve block, lidocaine only
–– Significant pain relief at 1 mo f/uSignificant pain relief at 1 mo f/u–– But no difference at 3, 6 month f/uBut no difference at 3, 6 month f/u
Corticosteroid InjectionsCorticosteroid Injections
Varied Varied combinations and combinations and approachesapproaches–– MedialMedial–– Plantar Plantar
Post injection flarePost injection flareElevated glucose in Elevated glucose in DM patientsDM patients

Treatment Treatment –– Phase 1Phase 1
Activity limitationActivity limitation–– Cut workouts in halfCut workouts in half–– Stop all high impact Stop all high impact
workoutsworkoutsNo runningNo runningNo aerobicsNo aerobics
Activity LimitationActivity Limitation
Riddle et al. (2003)Riddle et al. (2003)–– Working in a standing position all day Working in a standing position all day
increases risk for plantar fasciitis to increases risk for plantar fasciitis to developdevelop
–– Increase in BMI = increase incidence of Increase in BMI = increase incidence of plantar fasciitis plantar fasciitis

Treatment Treatment –– Phase 1Phase 1
Physical TherapyPhysical Therapy–– UltrasoundUltrasound–– IontophoresisIontophoresis–– PhonophoresisPhonophoresis–– Interferential Interferential
currentcurrent–– AnodyneAnodyne–– StretchingStretching–– Deep massageDeep massage

IontophoresisIontophoresis
Gudeman et al. (1997)Gudeman et al. (1997)–– 36 patients36 patients
0.4% dexamethasone vs. placebo0.4% dexamethasone vs. placebo6 treatments over 2 weeks6 treatments over 2 weeksSignificant decrease in symptoms for treated Significant decrease in symptoms for treated groupgroupNo difference 1 mo after end of treatmentNo difference 1 mo after end of treatment
Treatment Treatment –– Phase 1Phase 1
Symptoms should resolve within 6 Symptoms should resolve within 6 weeksweeksIf improvement is noted treatment If improvement is noted treatment should be continued until symptoms should be continued until symptoms are resolvedare resolvedIf symptoms plateau Phase 2 If symptoms plateau Phase 2 treatment should be initiatedtreatment should be initiated
Treatment Treatment –– Phase 2Phase 2
Continuation of Phase 1 treatmentContinuation of Phase 1 treatmentCustom molded orthoticsCustom molded orthoticsNightsplintNightsplintCast boot walkerCast boot walker
Treatment Treatment –– Phase 2Phase 2
Custom molded Custom molded orthotics(orthoses)orthotics(orthoses)–– Neutral castNeutral cast–– Proper rearfoot / Proper rearfoot /
forefoot postingforefoot posting–– Type of orthotic Type of orthotic
patient/activity patient/activity dependantdependant
OrthosesOrthoses
Pfeffer et al (1999)Pfeffer et al (1999)–– 200 patients200 patients
Silicone heel padSilicone heel padFelt arch padFelt arch padTullis rubber heel cupTullis rubber heel cupCustom molded polypropylene orthoticCustom molded polypropylene orthotic
–– Prefabricated inserts provided better pain Prefabricated inserts provided better pain relief than custom orthosesrelief than custom orthoses

OrthosesOrthoses
Rome et al. (2004)Rome et al. (2004)–– Compared functional orthoses vs. Compared functional orthoses vs.
accommodative insertsaccommodative inserts–– Prefabricated orthosesPrefabricated orthoses
Functional orthoses provided significant Functional orthoses provided significant improvement in pain relief compared with improvement in pain relief compared with accommodative insertsaccommodative inserts
OrthosesOrthoses
Collins et al. (2007)Collins et al. (2007)–– “…“… insufficient evidence to support or insufficient evidence to support or
refute the use of foot orthoses, custom or refute the use of foot orthoses, custom or prefabricated, in the treatment of lower prefabricated, in the treatment of lower limb overuse injuries.limb overuse injuries.””

Treatment Treatment –– Phase 2Phase 2
Night splintNight splint–– Static dorsiflexionStatic dorsiflexion–– DynamicDynamic
Prolonged low load Prolonged low load stretch of tendo stretch of tendo AchillesAchilles
Orthoses / Night splintOrthoses / Night splint
Roos et al. showed significant Roos et al. showed significant improvement in symptoms:improvement in symptoms:–– Custom orthoticCustom orthotic–– Custom orthotic + night splintCustom orthotic + night splint–– Night splint aloneNight splint alone
Long term pain relief noted with Long term pain relief noted with continued use of orthoticscontinued use of orthotics

Night SplintNight Splint
Batt et al. (1996)Batt et al. (1996)–– 34 patients34 patients–– All 17 patients wearing dorsiflexion night All 17 patients wearing dorsiflexion night
splint showed improvement in symptomssplint showed improvement in symptoms
Powell et al. (1998)Powell et al. (1998)–– 37 patients37 patients–– After 1 mo treatment group showed After 1 mo treatment group showed
significant improvementsignificant improvement
Night SplintNight Splint
Probe et al. (1999)Probe et al. (1999)–– 116 patients116 patients–– NSAIDs, Achilles stretch, shoe wearNSAIDs, Achilles stretch, shoe wear–– Above treatment + night splint x 3 moAbove treatment + night splint x 3 mo
–– Did not find any significant difference Did not find any significant difference with use of night splintwith use of night splint
Treatment Treatment –– Phase 2Phase 2
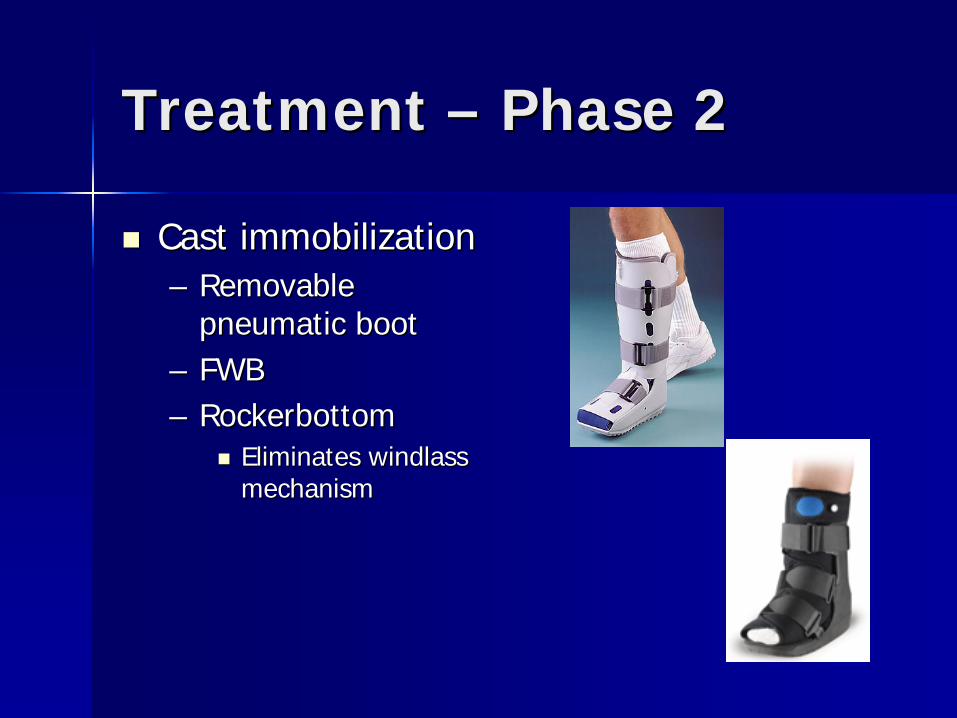
Cast immobilizationCast immobilization–– Removable Removable
pneumatic bootpneumatic boot–– FWBFWB–– RockerbottomRockerbottom
Eliminates windlass Eliminates windlass mechanismmechanism

Treatment Treatment –– Phase 2Phase 2
Symptoms typically resolve in 2Symptoms typically resolve in 2--3 3 months (4months (4--6 mo from initial treatment)6 mo from initial treatment)If improvement noted continue If improvement noted continue treatment from both Phase 1 and treatment from both Phase 1 and Phase 2 until symptoms resolvePhase 2 until symptoms resolveIf symptoms plateau or do not If symptoms plateau or do not improve then proceed to Phase 3improve then proceed to Phase 3
Treatment Treatment –– Phase 3Phase 3
Nonweightbearing cast immobilizationNonweightbearing cast immobilizationSurgical plantar fasciotomySurgical plantar fasciotomyEndoscopic plantar fasciotomy (EPF)Endoscopic plantar fasciotomy (EPF)Extracorporeal shockwave therapy Extracorporeal shockwave therapy (ESWT)(ESWT)CoblationCoblation--based fasciotomybased fasciotomy
Treatment Treatment –– Phase 3Phase 3
Nonweightbearing Nonweightbearing cast immobilizationcast immobilization–– RemovableRemovable–– FiberglassFiberglass
Limitation on Limitation on stretchingstretching
Treatment Treatment –– Phase 3Phase 3
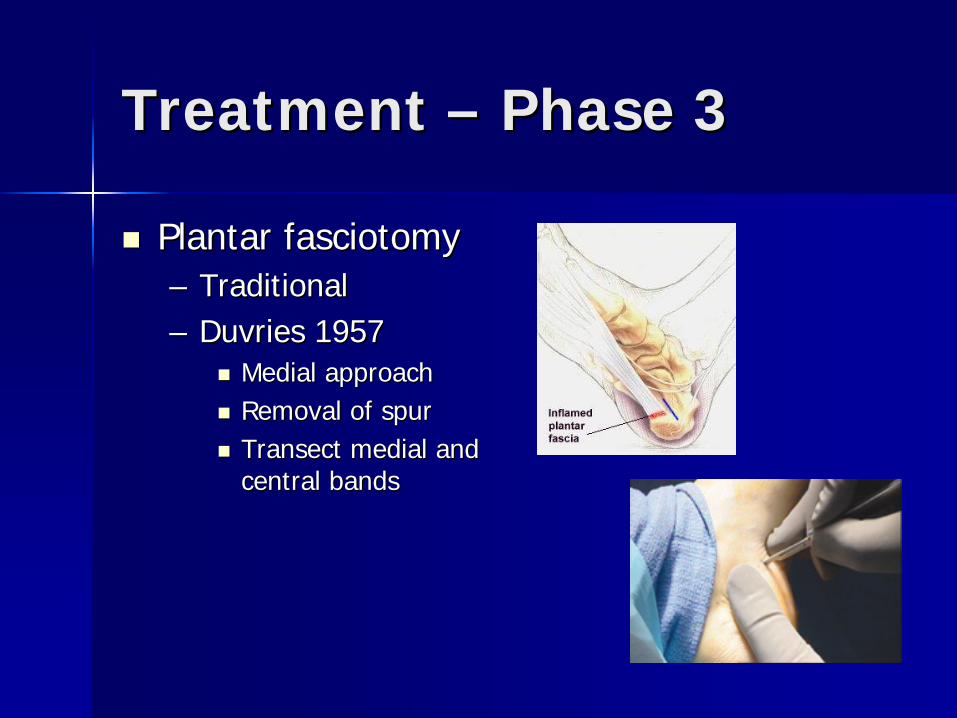
Plantar fasciotomyPlantar fasciotomy–– TraditionalTraditional–– Duvries 1957Duvries 1957
Medial approachMedial approachRemoval of spurRemoval of spurTransect medial and Transect medial and central bandscentral bands

Treatment Treatment –– Phase 3Phase 3
Instep fasciotomyInstep fasciotomy–– Direct visualizationDirect visualization–– Reduced risk of Reduced risk of
nerve entrapmentnerve entrapment–– Allows immediate Allows immediate
PWB to FWBPWB to FWB–– Incision parallel to Incision parallel to
relaxed skin tension relaxed skin tension lineslines

Instep Plantar Instep Plantar FasciotomyFasciotomy

Instep Plantar Instep Plantar FasciotomyFasciotomy
Postoperative CoursePostoperative Course–– 22--3 weeks in sterile bandages3 weeks in sterile bandages–– PWB to FWB in CAM walkerPWB to FWB in CAM walker–– Physical Therapy initiated once incision Physical Therapy initiated once incision
healedhealed–– No high impact activity x 6 weeksNo high impact activity x 6 weeks–– Full recovery may take 12 weeksFull recovery may take 12 weeks

Instep Plantar Instep Plantar FasciotomyFasciotomy
Complications / risksComplications / risks–– Lateral column painLateral column pain
Alteration of biomechanicsAlteration of biomechanics
–– Nerve entrapmentNerve entrapment–– Painful hypertrophic scarPainful hypertrophic scar

Plantar FasciotomyPlantar Fasciotomy
Lane & London (2004)Lane & London (2004)–– Retrospective studyRetrospective study–– 29 patients29 patients–– 96% success rate96% success rate
Ave 21 months postopAve 21 months postopVAS reduced from 8.4 to 1.2VAS reduced from 8.4 to 1.2

Plantar FasciotomyPlantar Fasciotomy
Fishco et al. (2000)Fishco et al. (2000)–– Retrospective studyRetrospective study–– 83 patients83 patients
Heel pain ave 14 months prior to surgeryHeel pain ave 14 months prior to surgery
–– 21 months postop21 months postop–– 93.6% success93.6% success

Treatment Treatment –– Phase 3Phase 3
Endoscopic Plantar Endoscopic Plantar Fasciotomy (EPF)Fasciotomy (EPF)–– Release of fascia Release of fascia
ligament through ligament through uniuni or two portal or two portal endoscopeendoscope

Endoscopic Plantar FasciotomyEndoscopic Plantar Fasciotomy
Postoperative CoursePostoperative Course–– 1010--14 days incision healing14 days incision healing–– FWB in CAM walkerFWB in CAM walker–– Physical Therapy initiated 1Physical Therapy initiated 1--2 weeks2 weeks–– No exercise activity x 6 weeksNo exercise activity x 6 weeks–– Full recovery up to 12 weeksFull recovery up to 12 weeks
Endoscopic Plantar FasciotomyEndoscopic Plantar Fasciotomy
AdvantagesAdvantages–– Minimally invasiveMinimally invasive–– Quicker recoveryQuicker recovery
DisadvantagesDisadvantages–– Risk of nerve Risk of nerve
entrapmententrapment–– Learning curveLearning curve–– Risk of reoccurrence Risk of reoccurrence
of heel painof heel pain
Treatment Treatment –– Phase 3Phase 3
Extracorporeal Extracorporeal Shockwave Therapy Shockwave Therapy (ESWT)(ESWT)–– Propagation of Propagation of
shockwave shockwave transmitted through transmitted through to injured tissueto injured tissue
Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
NeovascularizationNeovascularizationLocal hyperemiaLocal hyperemia
tissue growth tissue growth factorsfactorsInhibition of pain Inhibition of pain receptorsreceptors

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
Developed from Developed from lithotripsylithotripsyEarly 1990s Early 1990s –– Orthopedic use Orthopedic use
(orthotripsy)(orthotripsy)–– FDA approved for FDA approved for
chronic plantar chronic plantar fasciitis (fasciosis)fasciitis (fasciosis)

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
3 types3 types–– ElectrohydraulicElectrohydraulic
OssaTronOssaTron
–– ElectromagneticElectromagneticDornier EposDornier Epos
–– PiezoelectricPiezoelectricPiezosonPiezoson
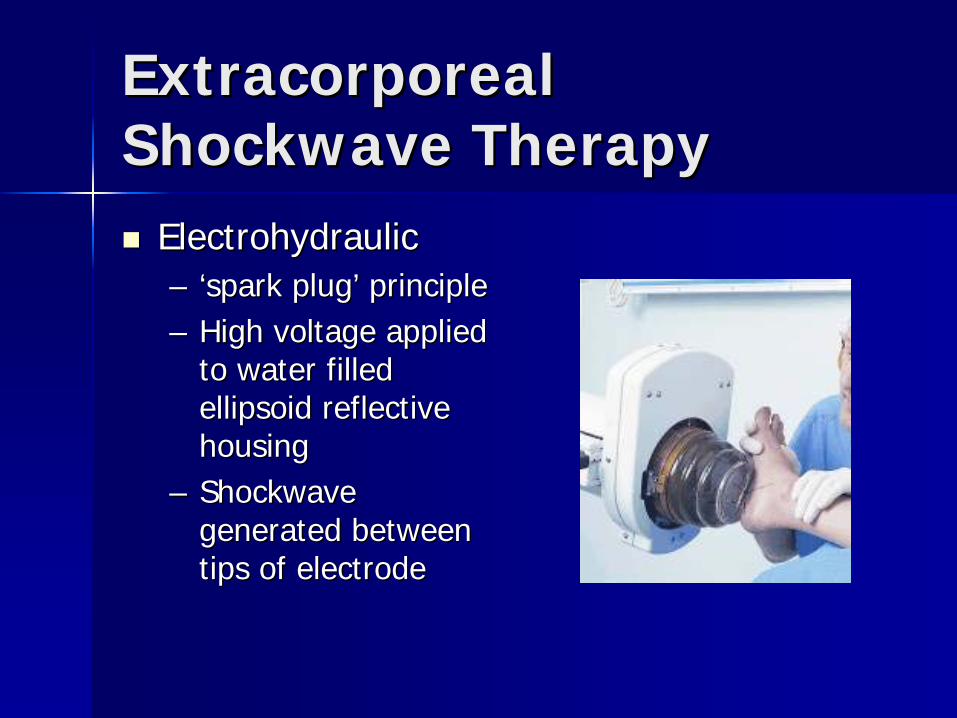
Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
ElectrohydraulicElectrohydraulic–– ‘‘spark plugspark plug’’ principleprinciple–– High voltage applied High voltage applied
to water filled to water filled ellipsoid reflective ellipsoid reflective housinghousing
–– Shockwave Shockwave generated between generated between tips of electrodetips of electrode

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
ElectromagneticElectromagnetic–– Electric current Electric current
passed through coil passed through coil generating a generating a magnetic fieldmagnetic field
–– Shockwave Shockwave generated from generated from water immersed water immersed conductive conductive membranemembrane
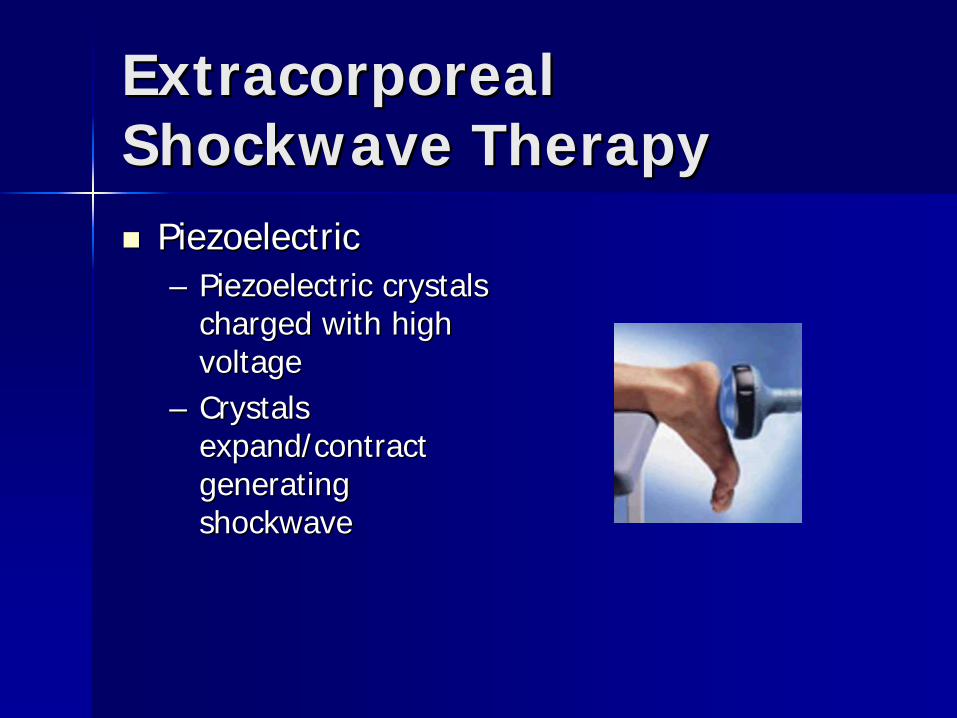
Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
PiezoelectricPiezoelectric–– Piezoelectric crystals Piezoelectric crystals
charged with high charged with high voltagevoltage
–– Crystals Crystals expand/contract expand/contract generating generating shockwaveshockwave
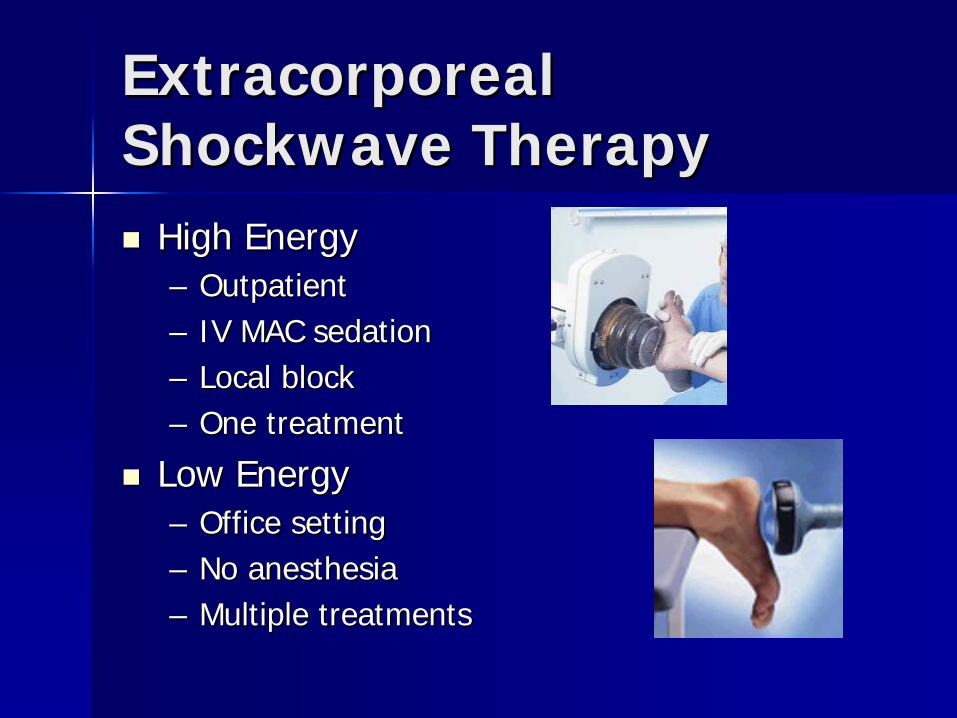
Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
High EnergyHigh Energy–– OutpatientOutpatient–– IV MAC sedationIV MAC sedation–– Local blockLocal block–– One treatmentOne treatment
Low EnergyLow Energy–– Office settingOffice setting–– No anesthesiaNo anesthesia–– Multiple treatmentsMultiple treatments
ESWT Postop CourseESWT Postop Course
Immediate weightbearing in athletic Immediate weightbearing in athletic shoe w/ orthosesshoe w/ orthosesNo NSAIDsNo NSAIDsContinue nightsplint, stretchingContinue nightsplint, stretching11--2 weeks of continued heel pain2 weeks of continued heel painFull recovery up to 12 weeksFull recovery up to 12 weeks

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
ComplicationsComplications–– Localized swellingLocalized swelling–– Localized bruisingLocalized bruising–– Reoccurrence of Reoccurrence of
heel painheel pain

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
AdvantagesAdvantages–– NoninvasiveNoninvasive–– Quick recoveryQuick recovery–– Minimal to no Minimal to no
complicationscomplications
DisadvantagesDisadvantages–– High costHigh cost–– Insurance coverageInsurance coverage–– No universally No universally
accepted protocolaccepted protocol

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
Buchbinder et al. (2002)Buchbinder et al. (2002)–– DoubleDouble--blind prospective studyblind prospective study–– 160 patients diagnosed with plantar 160 patients diagnosed with plantar
fasciitis for at least 6 weeksfasciitis for at least 6 weeks–– Low energy deviceLow energy device
Weekly treatment x 3 weeksWeekly treatment x 3 weeks
–– No significant difference in symptomsNo significant difference in symptoms

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
Ogden et al. (2004)Ogden et al. (2004)–– Prospective studyProspective study–– 293 patients293 patients–– High energy ESWTHigh energy ESWT–– 47% success at 3 months47% success at 3 months

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
Malay et al. (2006)Malay et al. (2006)–– Prospective doubleProspective double--blind studyblind study–– 172 patients (115:57)172 patients (115:57)–– Electrohydraulic device (high energy)Electrohydraulic device (high energy)–– No anesthesiaNo anesthesia–– Overall reduction of pain on VASOverall reduction of pain on VAS–– 43% ESWT group vs. 19.6% placebo43% ESWT group vs. 19.6% placebo

Extracorporeal Extracorporeal Shockwave TherapyShockwave Therapy
Efficacy still controversialEfficacy still controversialNo standardized treatment protocolNo standardized treatment protocolHigh energy vs. low energyHigh energy vs. low energyRetrospective studies reveal 60% Retrospective studies reveal 60% success ratesuccess rateProspective studies vary in success Prospective studies vary in success rates dependant on type of ESWTrates dependant on type of ESWT

Treatment Treatment –– Phase 3Phase 3
CoblationCoblation--based based fasciotomy / fasciotomy / microtenotomymicrotenotomy–– Use of bipolar Use of bipolar
radiofrequencyradiofrequency–– Evolved from Evolved from
cardiology researchcardiology research
Coblation fasciotomyCoblation fasciotomy
Stimulates Stimulates inflammatory inflammatory responseresponseAngiogenesisAngiogenesisAntinociceptive Antinociceptive effecteffect–– Rapid pain Rapid pain
reductionreduction

Coblation fasciotomyCoblation fasciotomy
IndicationsIndications–– Plantar fasciosisPlantar fasciosis
>6 months heel pain>6 months heel pain
TechniquesTechniques–– OpenOpen–– PercutaneousPercutaneous
Postop coursePostop course–– PWBPWB--FWB in CAM FWB in CAM
walker 2walker 2--3 weeks3 weeks

Coblation fasciotomyCoblation fasciotomy
AdvantagesAdvantages–– Rapid recoveryRapid recovery–– Less invasiveLess invasive
percutaneouspercutaneous
RisksRisks–– Plantar fascia Plantar fascia
rupturerupture–– Nerve entrapmentNerve entrapment
Coblation fasciotomyCoblation fasciotomy
Tendon coblation has shown over 90% Tendon coblation has shown over 90% improvement in VAS pain scaleimprovement in VAS pain scaleInitial studies show significant improvement Initial studies show significant improvement in pain levels as early as 2 weeksin pain levels as early as 2 weeksPain continued to improve up to 6 monthsPain continued to improve up to 6 monthsLarger, prospective studies needed to Larger, prospective studies needed to assess effect on plantar fascia ligamentassess effect on plantar fascia ligament
SummarySummary
Diagnosis of heel pain etiology Diagnosis of heel pain etiology essential for proper treatmentessential for proper treatmentA combination of conservative A combination of conservative treatment requiredtreatment requiredTreatment can extend for months, no Treatment can extend for months, no quick fixesquick fixesSurgery: last option Surgery: last option

Thank youThank you