Embed Size (px)
Citation preview
8/8/2019 Platforms for Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memor…
http://slidepdf.com/reader/full/platforms-for-sustainable-health-systems-in-disadvantaged-communities-university 1/4
1
Platforms for Sustainable Health Systems in Disadvantaged CommunitiesVimala Ramakrishnam, New Concept Communications, Jaishankar Memorial CentreRandall Kuhn, Global Health Affairs Program, University of Denver
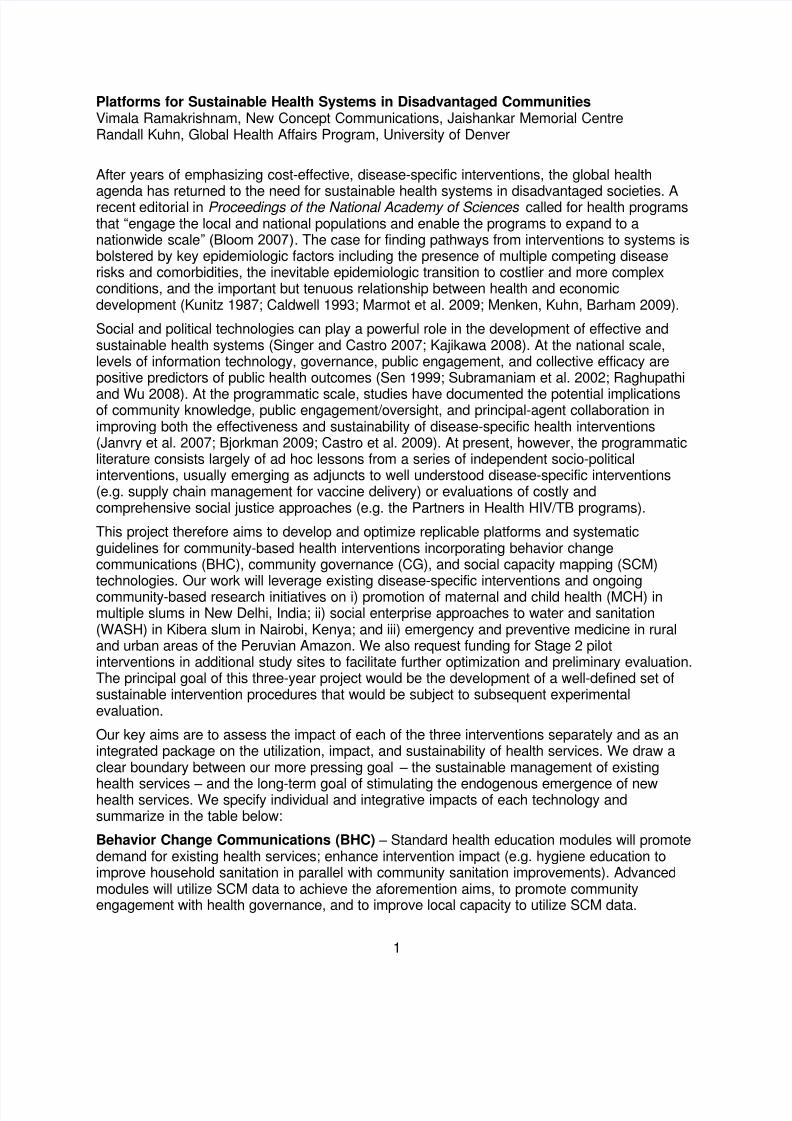
After years of emphasizing cost-effective, disease-specific interventions, the global health
agenda has returned to the need for sustainable health systems in disadvantaged societies. Arecent editorial in Proceedings of the National Academy of Sciences called for health programsthat “engage the local and national populations and enable the programs to expand to anationwide scale” (Bloom 2007). The case for finding pathways from interventions to systems isbolstered by key epidemiologic factors including the presence of multiple competing diseaserisks and comorbidities, the inevitable epidemiologic transition to costlier and more complexconditions, and the important but tenuous relationship between health and economicdevelopment (Kunitz 1987; Caldwell 1993; Marmot et al. 2009; Menken, Kuhn, Barham 2009).
Social and political technologies can play a powerful role in the development of effective andsustainable health systems (Singer and Castro 2007; Kajikawa 2008). At the national scale,levels of information technology, governance, public engagement, and collective efficacy arepositive predictors of public health outcomes (Sen 1999; Subramaniam et al. 2002; Raghupathi
and Wu 2008). At the programmatic scale, studies have documented the potential implicationsof community knowledge, public engagement/oversight, and principal-agent collaboration inimproving both the effectiveness and sustainability of disease-specific health interventions(Janvry et al. 2007; Bjorkman 2009; Castro et al. 2009). At present, however, the programmaticliterature consists largely of ad hoc lessons from a series of independent socio-politicalinterventions, usually emerging as adjuncts to well understood disease-specific interventions(e.g. supply chain management for vaccine delivery) or evaluations of costly andcomprehensive social justice approaches (e.g. the Partners in Health HIV/TB programs).
This project therefore aims to develop and optimize replicable platforms and systematicguidelines for community-based health interventions incorporating behavior changecommunications (BHC), community governance (CG), and social capacity mapping (SCM)technologies. Our work will leverage existing disease-specific interventions and ongoingcommunity-based research initiatives on i) promotion of maternal and child health (MCH) inmultiple slums in New Delhi, India; ii) social enterprise approaches to water and sanitation(WASH) in Kibera slum in Nairobi, Kenya; and iii) emergency and preventive medicine in ruraland urban areas of the Peruvian Amazon. We also request funding for Stage 2 pilotinterventions in additional study sites to facilitate further optimization and preliminary evaluation.The principal goal of this three-year project would be the development of a well-defined set ofsustainable intervention procedures that would be subject to subsequent experimentalevaluation.
Our key aims are to assess the impact of each of the three interventions separately and as anintegrated package on the utilization, impact, and sustainability of health services. We draw aclear boundary between our more pressing goal – the sustainable management of existing
health services – and the long-term goal of stimulating the endogenous emergence of newhealth services. We specify individual and integrative impacts of each technology andsummarize in the table below:
Behavior Change Communications (BHC) – Standard health education modules will promotedemand for existing health services; enhance intervention impact (e.g. hygiene education toimprove household sanitation in parallel with community sanitation improvements). Advancedmodules will utilize SCM data to achieve the aforemention aims, to promote communityengagement with health governance, and to improve local capacity to utilize SCM data.
8/8/2019 Platforms for Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memor…
http://slidepdf.com/reader/full/platforms-for-sustainable-health-systems-in-disadvantaged-communities-university 2/4
2
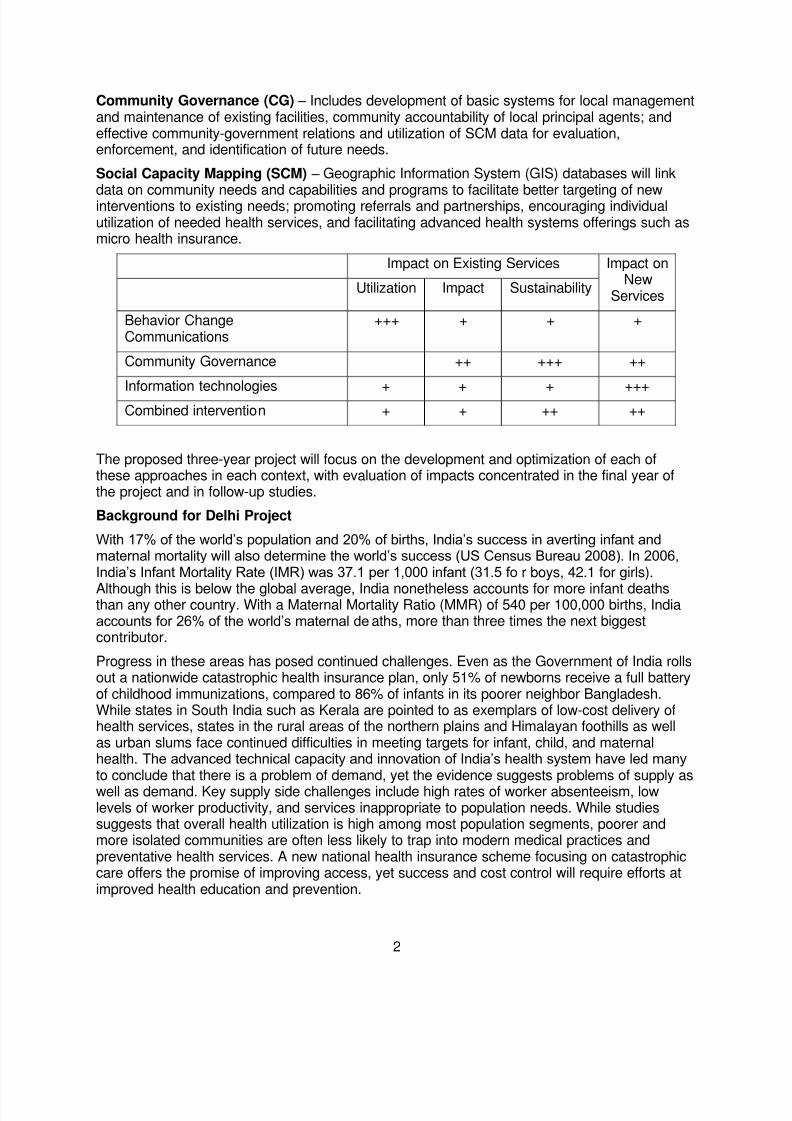
Community Governance (CG) – Includes development of basic systems for local managementand maintenance of existing facilities, community accountability of local principal agents; andeffective community-government relations and utilization of SCM data for evaluation,enforcement, and identification of future needs.
Social Capacity Mapping (SCM) – Geographic Information System (GIS) databases will link
data on community needs and capabilities and programs to facilitate better targeting of newinterventions to existing needs; promoting referrals and partnerships, encouraging individualutilization of needed health services, and facilitating advanced health systems offerings such asmicro health insurance.
Impact on Existing Services Impact onNew
ServicesUtilization Impact Sustainability
Behavior ChangeCommunications
+++ + + +
Community Governance ++ +++ ++
Information technologies + + + +++Combined intervention + + ++ ++
The proposed three-year project will focus on the development and optimization of each ofthese approaches in each context, with evaluation of impacts concentrated in the final year ofthe project and in follow-up studies.
Background for Delhi Project
With 17% of the world’s population and 20% of births, India’s success in averting infant andmaternal mortality will also determine the world’s success (US Census Bureau 2008). In 2006,India’s Infant Mortality Rate (IMR) was 37.1 per 1,000 infant (31.5 fo r boys, 42.1 for girls).
Although this is below the global average, India nonetheless accounts for more infant deathsthan any other country. With a Maternal Mortality Ratio (MMR) of 540 per 100,000 births, Indiaaccounts for 26% of the world’s maternal deaths, more than three times the next biggestcontributor.
Progress in these areas has posed continued challenges. Even as the Government of India rollsout a nationwide catastrophic health insurance plan, only 51% of newborns receive a full batteryof childhood immunizations, compared to 86% of infants in its poorer neighbor Bangladesh.While states in South India such as Kerala are pointed to as exemplars of low-cost delivery ofhealth services, states in the rural areas of the northern plains and Himalayan foothills as wellas urban slums face continued difficulties in meeting targets for infant, child, and maternalhealth. The advanced technical capacity and innovation of India’s health system have led manyto conclude that there is a problem of demand, yet the evidence suggests problems of supply aswell as demand. Key supply side challenges include high rates of worker absenteeism, lowlevels of worker productivity, and services inappropriate to population needs. While studiessuggests that overall health utilization is high among most population segments, poorer andmore isolated communities are often less likely to trap into modern medical practices andpreventative health services. A new national health insurance scheme focusing on catastrophiccare offers the promise of improving access, yet success and cost control will require efforts atimproved health education and prevention.
8/8/2019 Platforms for Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memor…
http://slidepdf.com/reader/full/platforms-for-sustainable-health-systems-in-disadvantaged-communities-university 3/4
3
Delhi Project Work in Progress
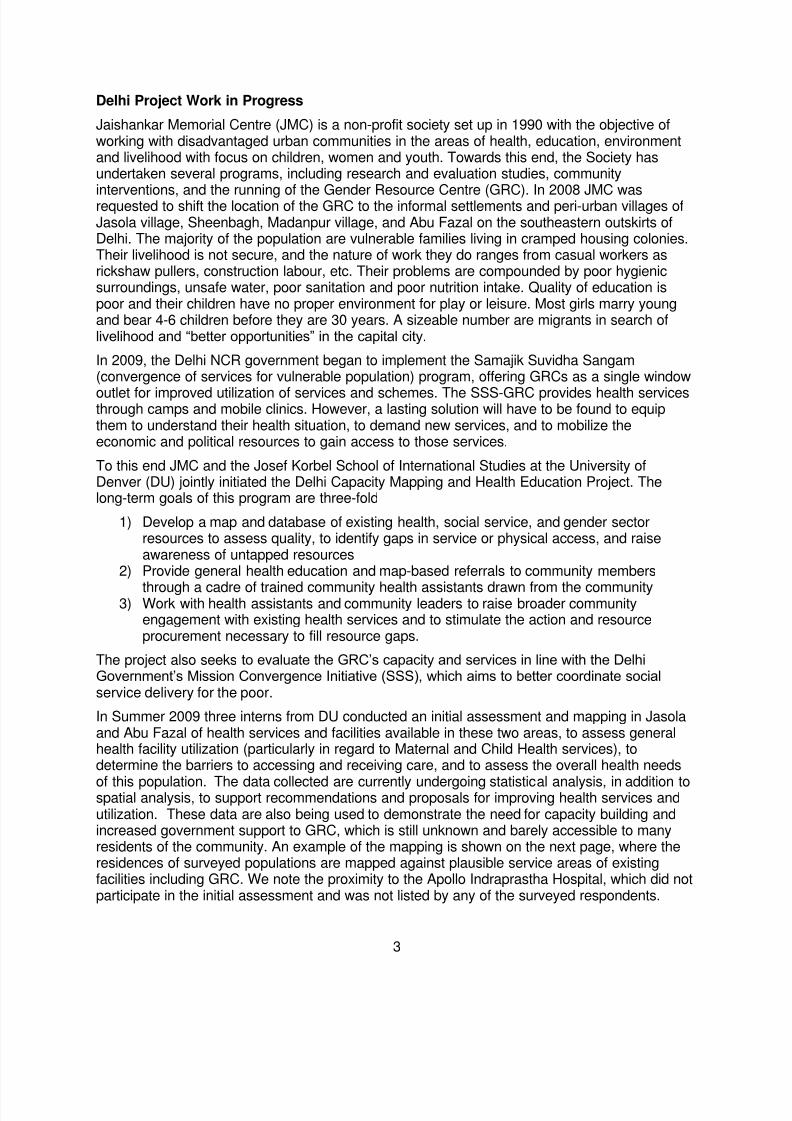
Jaishankar Memorial Centre (JMC) is a non-profit society set up in 1990 with the objective ofworking with disadvantaged urban communities in the areas of health, education, environmentand livelihood with focus on children, women and youth. Towards this end, the Society hasundertaken several programs, including research and evaluation studies, community
interventions, and the running of the Gender Resource Centre (GRC). In 2008 JMC wasrequested to shift the location of the GRC to the informal settlements and peri-urban villages ofJasola village, Sheenbagh, Madanpur village, and Abu Fazal on the southeastern outskirts ofDelhi. The majority of the population are vulnerable families living in cramped housing colonies.Their livelihood is not secure, and the nature of work they do ranges from casual workers asrickshaw pullers, construction labour, etc. Their problems are compounded by poor hygienicsurroundings, unsafe water, poor sanitation and poor nutrition intake. Quality of education ispoor and their children have no proper environment for play or leisure. Most girls marry youngand bear 4-6 children before they are 30 years. A sizeable number are migrants in search oflivelihood and “better opportunities” in the capital city.
In 2009, the Delhi NCR government began to implement the Samajik Suvidha Sangam(convergence of services for vulnerable population) program, offering GRCs as a single window
outlet for improved utilization of services and schemes. The SSS-GRC provides health servicesthrough camps and mobile clinics. However, a lasting solution will have to be found to equipthem to understand their health situation, to demand new services, and to mobilize theeconomic and political resources to gain access to those services.
To this end JMC and the Josef Korbel School of International Studies at the University ofDenver (DU) jointly initiated the Delhi Capacity Mapping and Health Education Project. Thelong-term goals of this program are three-fold
1) Develop a map and database of existing health, social service, and gender sectorresources to assess quality, to identify gaps in service or physical access, and raiseawareness of untapped resources
2) Provide general health education and map-based referrals to community members
through a cadre of trained community health assistants drawn from the community3) Work with health assistants and community leaders to raise broader community
engagement with existing health services and to stimulate the action and resourceprocurement necessary to fill resource gaps.
The project also seeks to evaluate the GRC’s capacity and services in line with the DelhiGovernment’s Mission Convergence Initiative (SSS), which aims to better coordinate socialservice delivery for the poor.
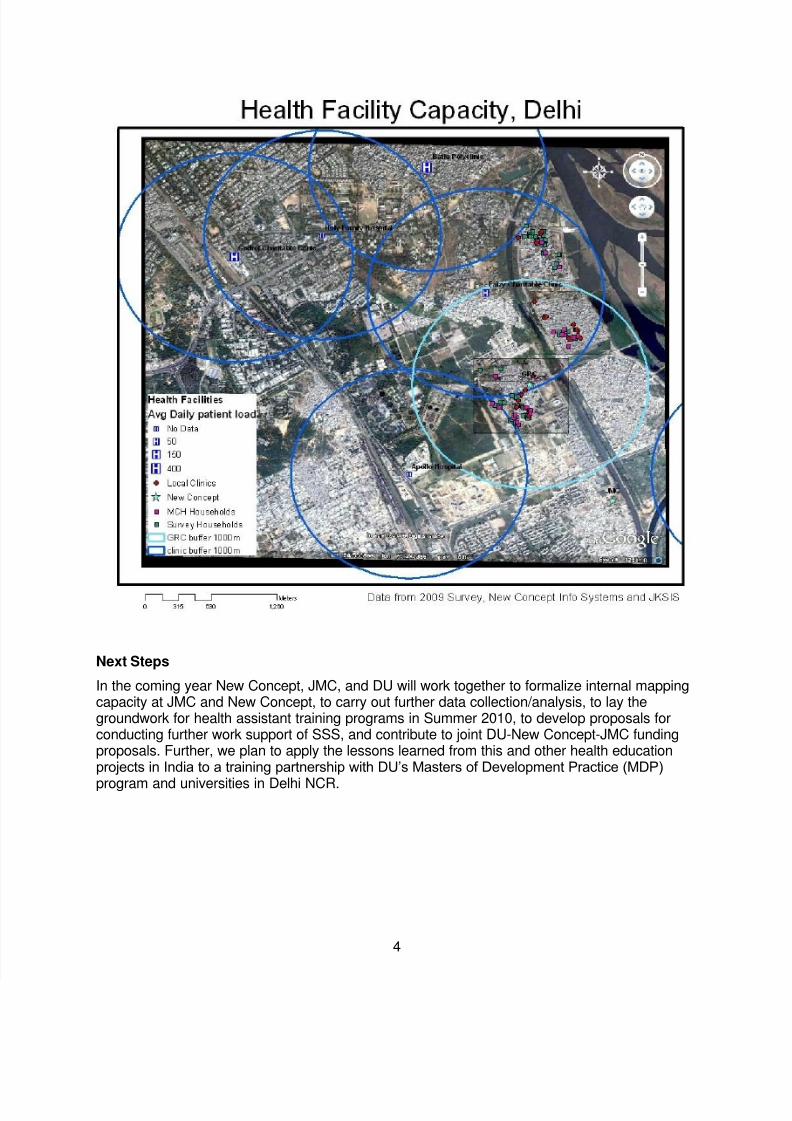
In Summer 2009 three interns from DU conducted an initial assessment and mapping in Jasolaand Abu Fazal of health services and facilities available in these two areas, to assess generalhealth facility utilization (particularly in regard to Maternal and Child Health services), todetermine the barriers to accessing and receiving care, and to assess the overall health needs
of this population. The data collected are currently undergoing statistical analysis, in addition tospatial analysis, to support recommendations and proposals for improving health services andutilization. These data are also being used to demonstrate the need for capacity building andincreased government support to GRC, which is still unknown and barely accessible to manyresidents of the community. An example of the mapping is shown on the next page, where theresidences of surveyed populations are mapped against plausible service areas of existingfacilities including GRC. We note the proximity to the Apollo Indraprastha Hospital, which did notparticipate in the initial assessment and was not listed by any of the surveyed respondents.
8/8/2019 Platforms for Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memor…
http://slidepdf.com/reader/full/platforms-for-sustainable-health-systems-in-disadvantaged-communities-university 4/4
4
Next Steps
In the coming year New Concept, JMC, and DU will work together to formalize internal mappingcapacity at JMC and New Concept, to carry out further data collection/analysis, to lay thegroundwork for health assistant training programs in Summer 2010, to develop proposals forconducting further work support of SSS, and contribute to joint DU-New Concept-JMC fundingproposals. Further, we plan to apply the lessons learned from this and other health educationprojects in India to a training partnership with DU’s Masters of Development Practice (MDP)
program and universities in Delhi NCR.