Embed Size (px)
Citation preview
Talc Pleurodesis for the Treatment of Pneumothoraxand Pleural Effusion*
Lisa Kennedy, M.D.; and Steven A. Sahn, M.D., F.C.C.P.
(Chest 1994; 106:1215-22)Key Words: pleurodesis; poudrage; slurry; talc
Early interest in the development of pleural sym-physis resulted from the desire of surgeons to
produce adhesions to facilitate lobectomy.1 Variousagents were tried but were found to be of limitedvalue. The indications for pleurodesis have expandedover the years to include the treatment of benign andmalignant effusions, the prevention of recurrence ofpneumothoraces, and, more recently, to assist in theclosure of persistent bronchopleural fistulas.
Over the past 20 years, the favorable safety profile,low cost, availability, and ease of administration ledto widespread use of tetracycline as the first-linepleurodesis agent. However, parenteral tetracyclineis no longer available in the United States. As an ef-fective, inexpensive, and safe pleurodesis agent foruse at the bedside is needed, there has been renewedinterest in bleomycin and talc as well as new inves-tigation of tetracycline-like agents, such as minocy-cline2-4 and doxycycline.5'6
Because of its excellent record of successful pleu-rodesis7-9 and low cost, talc has received substantialattention recently. The purpose of this article is toreview the chemical properties, efficacy, and safetyof talc as a pleurodesis agent.
MINEROLOGY
Talc is a tri-layered magnesium sheet silicate thathas significant lubricative properties that make ituseful in cosmetic as well as industrial applications.The basic talc structure was determined in 193410 butthe geometry and spacial relationships of the octa-hedrally coordinated Mg(OH)2 and the two tetrahe-drally linked SiO4 groups were not described until thelate 1960s.11,12 The empirical chemical compound,*From the Division of Pulmonary and Critical Care Medicine,Department of Medicine, Medical University of South Carolina,Charleston.
Manuscript received January 4, 1994; revision accepted March 14.Reprint requests: Dr. Sahn, Div. of Pulmonary and Critical CareMedicine, Medical University of South Carolina, 171 AshleyAve., Charleston 29425
Mg3Si4Oo(OH)2>, is rarely found as a pure entity innature because of frequent cation substitutionswherein magnesium is replaced by iron, nickel,chromium, or manganese.13 Furthermore, complexgeologic processes reacting on diverse preexistingrock types commonly result in the formation of no-table impurities such as tremolite, chrysotile, andanthophyllite.13"14 There are many sources of talc oreand the composition varies widely. Large NorthAmerican deposits are found in New York, Califor-nia, Texas, and Vermont.14
TALC AS A PLEURODESIS AGENT
The use of talc for the production of pleural sym-physis was first described by Bethune'5 in 1935. Thisearly work involved the creation of pneumothoracesin cats and dogs followed by the insufflation of iodi-nated talc. He also described two patients whoreceived a dusting of talc as a preliminary to lobec-tomy, thus, documenting the first use of intrapleuraltalc in humans. His observations were confirmed bySinger et al16 and Hanrahan et al17 who simulta-neously published studies using talc poudrage andtalc slurry in animals.
Several animal models have been used in the studyof talc pleurodesis, including cats, dogs, rabbits, pigs,and guinea pigs. Descriptions of gross specimens 3 to6 weeks after pleurodesis note the presence of mac-roscopic talc on the parietal surface and occasionalfilmy adhesions.15-17 Frankel et all8 described denseadhesions in dogs who had undergone talc pleuro-desis 3 to 4 months prior to death. In a recent reportby Mathlouthi et al,19 dogs given talc by insufflationwere examined at 1, 2, 7, 15, and 30 days. Parietal andvisceral pleural inflammation at 1 and 2 days wasnoted. Granulomatous pleural reaction, which wasnot dose dependent, was also observed.
Early experimental models of talc pleurodesislacked detailed description of the microscopic pro-cess that occurs following the intrapleural applicationof talc. At 2, 3, 6, 12, and 16 weeks following intra-pleural talc (slurry and poudrage), visceral pleural
CHEST / 106/4/ OCTOBER, 1994 1215
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

thickening with fibroblast proliferation, macrophageinfiltration, and foreign body reaction has been con-sistently reported in all animal models. Schepers andDurkan20 studied the tissue reaction to intravenouslyadministered and inhaled talc particles; intrapleuraladministration was not performed. They noted thatparticle size was more important than particle com-position and that tissue reaction was almost negligi-ble when the talc particles were less than 3 Am in size.To our knowledge, the pleural reaction to talc relatedto the particle size has not been reported.
Iodine is occasionally included when talc pleur-odesis is performed. Singer et al16 noted no differencein the microscopic or macroscopic reaction to talcwith or without iodine in rabbits. To our knowledge,there are no clinical or animal studies that comparethe pleurodesis potential of talc to talc plus iodine.The efficacy of pleurodesis in those series in whichiodine was used is 95 percent (222 of 234), which issimilar to the efficacy reported in all other series (90percent, 1,052 of 1,168). There is one report of anallergic reaction following the use of iodinated talc.2'
PREPARATION OF TALC FOR PLEURODESIS
Talc used for pleurodesis is United States Phar-macopea (USP) asbestos free and must meet minimalcriteria with regard to loss on ignition, acid-solublesubstances, water-soluble substances, arsenic, lead,and heavy metals.22 Additional product specifica-tions vary among manufacturers. Talc particle sizedepends on the nature and quantity of impurities aswell as the manufacturing process. Particles aregenerally less than 50,m in size; fine grades havingparticles no greater than 10 Am size may be pur-chased. Talc is available from most suppliers of sci-entific products and chemicals. Some of the largersuppliers are as follows: (1) Amend Drug and Chem-ical Company, Irvington, NY; (2) J.T. Baker, Phill-ipsburg, NJ; (3) City Chemical Corporation, NewYork; (4) Humco Laboratory, Texarkana, Tex; (5)Integra Chemical Company, Renton, Wash; (6) Spec-trum Chemical Manufacturing Corporation, Garde-nia, Calif; and (7) American Drug Industries, Chi-cago. The price of talc ranges from $5 to $25 perpound.
While talc is not packaged sterilely by the manu-facturer, limitation on the number of micro-organ-isms is a part of USP specifications and total bacteriacount cannot exceed 500/g. Despite the long-termuse of talc for pleurodesis, there is no standardmethod of sterilization. Dry heat sterilization is themost frequently noted method of sterilization.23-28Three different temperatures and durations of ster-ilization have been reported: 160°C for 2 h,27 1250Cfor 12 h23 and 132°C for 6 hs.28 Ethylene oxide gassterilization has also been described,7'9'29 but details
have not been published. Most recently, Bubik30recommended gamma irradiation. Protocols ofteninvolve either culture of the talc for bacterial patho-gens or inclusion of biologic indicators during thesterilization process.
Talc poudrage may be accomplished by severaldifferent techniques; the most frequently describedmethod is the use of an atomizer or bulb syringe atthe time of thoracotomy or thoracostomy. A talcslurry results when talc is mixed in saline solution andthen gently agitated. The volume of slurry is variable;10 to 250 ml of normal saline solution has been used.
TALC IN PNEUMOTHORAX
The experimental studies of the 1940s initiatedwidespread interest in the treatment of spontaneouspneumothorax of tuberculous3' and nontubercu-IOus32 origin. Both slurry and poudrage were used,and talc quickly became the accepted pleurodesisagent. Anecdotal reports of greater efficacy withpoudrage, as well as the frequent need for the surgi-cal removal of blebs, led to less enthusiasm for talcslurry. In 1956, Gaensler33 advocated partial pleu-rectomy as the preferred treatment for spontaneouspneumothorax stating that "pleurodesis has also lostfavor because of pain which is often worse than af-ter major thoracotomy, febrile reactions, shock, thenecessity for repeated treatments, and prolongedhospitalization which exceeds by far the period ofrecovery after surgery. Further, use of powder hasresulted in talcum embolism with hemiplegia both inman and experimental animals." The popularity oftalc in the United States waned during the 1960s butremained the primary pleurodesis agent in Europe.The 1980s marked the return of talc poudrage for thetreatment of pneumothorax.
Recent clinical applications have included thetreatment of pneumothorax secondary to Pneumo-cystis carinii pneumonia,34 metastatic osteosarco-ma,35 pleural endometriosis,3637 lymphangioleiomy-omatosis,38 and cystic fibrosis.39'40
Table 1 summarizes the English literature publi-cations reporting the use of talc in the treatment ofpneumothorax. While talc slurry31'40'4' has been usedwith success in the treatment of pneumothorax,poudrage at the time of thoracotomy, thoracostomy,and pleuroscopy is by far the most common methodof administration. Various doses of talc have beenused with 2 to 10 g being most common. Criteria forsuccess varies. The effect of dose on success cannot bedetermined from the published data. Steele,31 whosesuccess rate was only 57 percent (17 of 30), definedsuccess as the inability to induce pneumothorax fol-lowing pleurodesis. Most other authors, who use re-currence of pneumothorax as the marker of a failedprocedure, report much higher success rates. The
Talc Pleurodesis for Pneumothorax and Pleural Effusion Treatment (Kennedy, Sahn)1216
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

Table 1-Talc Pleurodesis in the Treatment of Pneumothorax*
Dose, Pneumothorax Success/TotalSource, yr Method g Classification (%) Comments
Steele,3' 1947 Slurry 2 PSP, SSP 5/16 (31) Secondary to tuberculosis; fever,
Steele,3' 1947Meade and Blades,32 1949Shefts et al,73 1954Marrangoni et al,74 1955Smith and Rothwell,25 1962Jackson and Bennett,72 1969
Crosby,36 1973
3-10N/AN/AN/A2-510
Poudrage N/A
PSP, SSPPSP, SSPPSP, SSPPSPPSP, SSPPSP
SSP
Poudrage "Large" SSP
Dieter and Leisen,37 1981
Tribble et al,39 1986Bourke et al,35 1987
Verschoof et al,75 1988Almind et al,4' 1989Spector and Stern,40 1989Pouwels and Wouters,556 1989
Daniel et al,23 1990t
Tunon-de-Lara et al,34 1992
Ohri et al,47 1992
Warren et al,38 1993
Van de Brekel et al,76 1993Kennedy et al,28 1994
Poudrage N/A
Poudrage 2Poudrage N/A
Poudrage 3Slurry 5Slurry 10Poudrage 3
Poudrage 2-10.5
N/A
SSP
SSPSSP
PSP, SSPPSP, SSPSSPSP
PSP, SSP, IP
SSP
2-5 SSP
Poudrage N/A
Poudrage N/ASlurry 10
SSP
SPIP
12/14 (86)6/6 (100)
33/33 (100)25/25 (100)58/61 (95)
1/1 (100)
pain reportedSecondary to tuberculosisTalc with sulfanilamide used
Iodine usedCase report chest wall tumor
following pleurodesis; iodineused
1/1 (100) Secondary to thoracicendometriosis
22/22 (100) Secondary to systemic lupuserythematosus, chronicobstructive pulmonary disease,asthma and tuberculosis; 2respiratory failure deaths
1/1 (100) Secondary to thoracicendometriosis
5/5 (100) Secondary to cystic fibrosis2/2 (100) Secondary to metastatic
osteosarcoma37/38 (97) Iodine used27/29 (93) Fever, pain reported
5/5 (100) Secondary to cystic fibrosis29/30 (97) Fever, pain, and pneumonia
reported19/20 (95) Secondary to cystic fibrosis,
chronic obstructive pulmonarydisease, and postoperativebronchopulmonary fistula
1/1 (100) Secondary to Pneumocystis carinuipneumonia
15/15 (100) Secondary to tuberculosis andchronic obstructive pulmonarydisease
2/2 (100) Secondary tolymphangioleiomyomatosis
313/356 (88)3/3 (100) Secondary to postoperative
bronchopleural fistulas617/681 (91)
*N/A=not available; PSP=primary spontaneous pneumothorax; SSP=secondary spontaneous pneumothorax; SP=spontaneous pneumothorax,unspecified etiology; IP=iatrogenic pneumothorax.
tIncludes five patients previously described in article by Tribble et al.39 Results were not duplicated in total.
overall success rate is 91 percent (620 of 684).
TALC IN PLEURAL EFFUSION
In the first report of talc in the treatment of pleu-ral effusion in 1958, Chambers25 noted clinical suc-
cess in 17 of 20 patients who received talc slurry fortreatment of malignant pleural effusions. The litera-ture that followed this initial report, until recently,dealt almost exclusively with the application of drytalc at the time of thoracotomy (dusting), thoracos-copy (insufflation), or through a series of chest tubes(Venturi propulsion).42 Recent reports9'28 note theresurgence of interest in the use of talc slurry, which
may be especially applicable to those patients inwhom thoracoscopy poses a risk.
Talc has been used to produce pleural symphysisin patients with all types of effusions. While malig-nant effusions are most commonly treated, there are
numerous reports of its use in the treatment of effu-sions secondary to radiation,23'43 chylothorax,23'44-46yellow nail syndrome,23'47 systemic lupus erythema-tosus,48 empyema,4749 Waldenstrom's macroglobu-linemia,23 Dressler's syndrome,47 constrictive peri-carditis,28 and congestive heart failure.9The efficacy of talc in the control of malignant
pleural effusions has been compared with several
CHEST / 106 / 4 / OCTOBER, 1994 1217
PoudrageDustingPoudragePoudragePoudragePoudrage
Nandi,42 1980
N/A
Poudrage
Total
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017
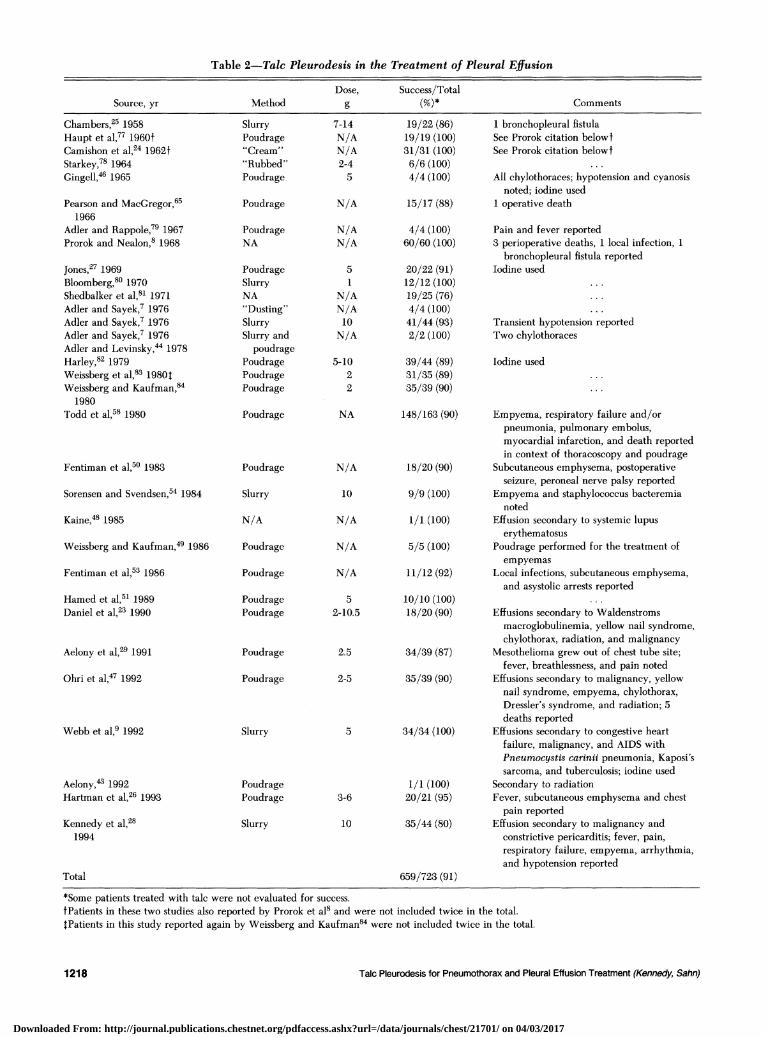
Table 2-Talc Pleurodesis in the Treatment of Pleural Effusion
Dose, Success/TotalSource, yr Method g (%)* Comments
Chambers,25 1958Haupt et al,77 1960tCamishon et al,24 1962tStarkey,71 1964Gingell,46 1965
Pearson and MacGregor,651966
Adler and Rappole,79 1967Prorok and Nealon,8 1968
Jones,27 1969Bloomberg,80 1970Shedbalker et al,8' 1971Adler and Sayek,7 1976Adler and Sayek,7 1976Adler and Sayek,7 1976Adler and Levinsky,44 1978Harley,82 1979Weissberg et al,83 1980$Weissberg and Kaufman,84
1980Todd et al,58 1980
Fentiman et al,50 1983
Sorensen and Svendsen,54 1984
Kaine,48 1985
Weissberg and Kaufman,49 1986
Fentiman et al,53 1986
Hamed et al,5' 1989Daniel et al,23 1990
Aelony et al,29 1991
Ohri et al,47 1992
Webb et al,9 1992
Aelony,43 1992Hartman et al,26 1993
Kennedy et al,281994
SlurryPoudrage"Cream""Rubbed"Poudrage
Poudrage
PoudrageNA
PoudrageSlurryNA"Dusting"SlurrySlurry and
poudragePoudragePoudragePoudrage
Poudrage
Poudrage
Slurry
N/A
Poudrage
Poudrage
PoudragePoudrage
Poudrage
Poudrage
Slurry
PoudragePoudrage
Slurry
Total
7-14N/AN/A2-45
N/A
N/AN/A
51
N/AN/A10N/A
5-1022
19/22 (86)19/19 (100)31/31 (100)6/6 (100)4/4 (100)
15/17 (88)
4/4 (100)60/60 (100)
20/22 (91)12/12 (100)19/25 (76)4/4 (100)41/44 (93)2/2 (100)
39/44 (89)31/35 (89)35/39 (90)
1 bronchopleural fistulaSee Prorok citation belowfSee Prorok citation belowf
All chylothoraces; hypotension and cyanosisnoted; iodine used
1 operative death
Pain and fever reported3 perioperative deaths, 1 local infection, 1
bronchopleural fistula reportedIodine used
Transient hypotension reportedTwo chylothoraces
Iodine used
NA 148/163(90) Empyema, respiratory failure and/orpneumonia, pulmonary embolus,myocardial infarction, and death reportedin context of thoracoscopy and poudrage
N/A 18/20 (90) Subcutaneous emphysema, postoperativeseizure, peroneal nerve palsy reported
10 9/9 (100) Empyema and staphylococcus bacteremianoted
N/A
N/A
N/A
2-
2
2
3
1/1 (100)
5/5 (100)
11/12 (92)
Effusion secondary to systemic lupuserythematosus
Poudrage performed for the treatment ofempyemas
Local infections, subcutaneous emphysema,and asystolic arrests reported
5 10/10 (100) ...10.5 18/20 (90) Effusions secondary to Waldenstroms
macroglobulinemia, yellow nail syndrome,chylothorax, radiation, and malignancy
t.5 34/39 (87) Mesothelioma grew out of chest tube site;fever, breathlessness, and pain noted
'-5 35/39 (90) Effusions secondary to malignancy, yellownail syndrome, empyema, chylothorax,Dressler's syndrome, and radiation; 5deaths reported
5 34/34 (100) Effusions secondary to congestive heartfailure, malignancy, and AIDS withPneumocystis carinii pneumonia, Kaposi'ssarcoma, and tuberculosis; iodine used
1/1 (100) Secondary to radiation1-6 20/21 (95) Fever, subcutaneous emphysema and chest
10 35/44 (80)pain reported
Effusion secondary to malignancy andconstrictive pericarditis; fever, pain,respiratory failure, empyema, arrhythmia,and hypotension reported
659/723(91)
Talc Pleurodesis for Pneumothorax and Pleural Effusion Treatment (Kennedy, Sahn)
*Some patients treated with talc were not evaluated for success.tPatients in these two studies also reported by Prorok et a18 and were not included twice in the total.$Patients in this study reported again by Weissberg and Kaufman84 were not included twice in the total.
1218
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

different agents, including mustine,50 bleomy-cin,65152 tetracycline,2653 quinacrine,40 and tubethoracostomy alone.54 In all comparisons, talc wasfound to be superior.
Reports from the English literature that describethe use of talc for the treatment of pleural effusion aresummarized in Table 2. Success was defined differ-ently, primarily on the basis of clinical criteria orradiographic findings. In several studies, the com-plete and persistent absence of pleural fluid was thedeterminant of successful pleurodesis, while in othersthe lack of need for further pleural drainage was thesole criterion. Follow-up times were variable; somepatients were followed up long term while otherswere evaluated for success only at 1 month afterpleurodesis. Doses from 1 to 14 g have been used. Itis problematic to determine the effect of dose onsuccess since no head-to-head comparisons of similarpatient populations have been made. Similar rates ofsuccess are noted with .5 g (221 of 241, 91 percent)or >5 g (85 of 97, 88 percent). Using success criteriareported by each author, an overall success rate of 91percent (657 of 721) was noted. When analyzed bythe method of administration, a success rate of 91percent (151 of 166) was observed after talc slurryand 91 percent (418 of 461) after poudrage.
SAFETY AND LONG-TERM SURVIVAL
Several safety aspects should be considered withintrapleural talc: (1) short-term, procedure-relatedissues such as pain, fever, infection, systemic embo-lization, hemodynamic compromise, and respiratoryfailure; and (2) long-term effects on pulmonaryfunction, survival, and risk of malignancy.
Most pleurodesis agents are associated with pain atthe time of instillation into the pleural space. In areview of pleurodesis agents by Walker-Renard andcolleagues,55 pain was associated with doxycycline,minocycline, tetracycline, bleomycin, cisplatin, cyt-arabine, doxorubicin, Corynebacterium parvum,mitomycin C, and talc. The degree of pain associatedwith talc has been variously reported from nonexist-ent to severe. Walker-Renard and colleagues55 re-ported pain with talc in 9 of 131 (7 percent) patients.To our knowledge, there are no controlled studiesthat compare talc-induced pain with that caused byother agents.
Fever following pleurodesis is common and hasbeen noted following the administration of mostagents.55 Fever following talc poudrage26'29'55'56 andslurry28,41 is common, occurring from 16 to 69 per-cent of the time. Fever characteristically occurs 4 to12 h following talc instillation and may last for 72 h.Empyema and local site infections are recognized,
although infrequent, complications of thoracentesisand tube thoracostomy.57 Empyema has been re-
ported with talc slurry from 0 to 11 percent of pro-cedures,28'41'54'56 while poudrage is associated with a0 to 3 percent incidence.8 29'58 Local site infection isuncommon.8'53
Cardiovascular complications, such as arrhyth-mias,28'47 cardiac arrest,53 chest pain,26 myocardialinfarction,58 and hypotension7'28'46 have been noted.In many instances, it is difficult to ascertain whetherthe complications are a result of the surgical proce-dure or related to talc per se.
Both inhalation59'60 and injection60O62 of talc areassociated with the development of pulmonary dis-ease. Respiratory insufficiency has been reportedwith both talc poudrage and talc slurry. Rinaldo andcolleaguesc3 reported the development of adult res-piratory distress syndrome in three patients who re-ceived a 10-g talc slurry via a chest tube; two patientsrecovered. The mechanism of respiratory failure isunclear; however, the authors speculated that a sys-temic inflammatory response or talc impurity mayhave been responsible. Bouchama and associates64reported a case of acute pneumonitis that followedclosed pleural biopsy and 2-g talc slurry pleurodesis;they postulated that respiratory failure occurredfrom talc emboli to the lungs. Todd and colleagues58reported respiratory failure/pneumonia in sevenpatients and Nandi42 reported two deaths secondaryto respiratory failure at 3 days and 6 weeks, all inpatients who had talc poudrage. In a recent report byKennedy and colleagues,28 three cases of respiratoryfailure were attributed to talc slurry pleurodesis. Onepatient who underwent bilateral, simultaneous talcpleurodesis procedures required mechanical ventila-tion while two other patients were treated with oxy-gen and corticosteroids alone. It is doubtful that themethod of administration plays a major role in thedevelopment of respiratory failure, although the doseof talc may be important.Death has been reported in several series in which
patients underwent talc pleurodesis.27'40'42'58,63,65 Thecause of death in each of these series was not defin-itively determined.Lange et a166 noted lung function 22 to 35 years
after treatment for pneumothorax with tube thora-costomy and talc poudrage. Those who received talchad a lower total lung capacity than those whoreceived tube drainage alone, 89 vs 96 percent ofpredicted, respectively. There was no difference be-tween the VC or FEVI when comparing the twogroups. Short-term follow-up after talc poudrage67'68revealed no difference in lung function when com-pared with other patients who have undergone tho-racotomy. The use of talc in the treatment of patientswith cystic fibrosis prompted a study that showedminimal impairment in pulmonary compliance ingrowing pigs who underwent poudrage.69
CHEST / 106 / 4 / OCTOBER, 1994 1219
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

Survival data on most patients who receive talcpleurodesis for the treatment of pleural effusion arelimited because of the nature of their disease. Mor-tality has been primarily related to the progression ofthe underlying disease or in operative proceduresinvolving debilitated patients. Case reports describ-ing the use of talc in nonmalignant effusions supportlong-term survival without significant sequelae.Long-term follow-up of 240 patients who receivedtalc or kaolin for the treatment of spontaneouspneumothorax70 revealed a higher death rate whencompared with a control population. However, thehigher death rate was attributed to a selection bias forpatients with underlying pulmonary disease and wasnot attributed to the use of talc. The only otherlong-term follow-up available66 did not address mor-tality.An association between talc and cancer has been
described in those who mine and process talc;7' thisassociation is attributed to asbestos, which is com-monly found in association with talc. While there isa single report72 of a patient who developed an ad-enocarcinoma of the pleura 2 years following iodizedtalc insufflation for spontaneous pneumothorax, talcwas not thought to be causative. Lange and col-leagues66 noted the absence of mesothelioma 20 to 35years after talc poudrage. Chappell and associates70found no increase in lung cancer in another group ofpatients who were followed up long term. Althoughno animal studies have been conducted with regardto the carcinogenic potential of intrapleural asbestos-free talc, to our knowledge, there is currently no ev-idence to suggest that an increase risk of cancer ex-ists in those who undergo talc pleurodesis.
CONCLUSIONSTalc is a highly effective pleurodesis agent when
administered either via poudrage or slurry in patientswith pleural effusion or pneumothorax. Success ratesare similar for the two primary modes of adminis-tration: 87 percent (189 of 217) for talc slurry and 93percent (988 of 1,062) for talc poudrage. The over-all success rate is 91 percent in the treatment ofpneumothorax (570 of 621) and in pleural effusion(659 of 723). The short-term adverse effects includefever, pain, infection (local and empyema), and res-piratory failure, the latter probably being doserelated. Long-term safety does not appear to be anissue if the asbestos-free product is used. Since thesuccess rate does not appear to be dose related andthere is some evidence to suggest that adverse effectsmay be associated with larger doses, we recommendpleurodesis, via poudrage or slurry, with a 5-g doseof talc.
REFERENCES1 Robinson S. Resection of lobesf lb fthe lung. JAMA 1917; 69:355
2 Dryzer SR, Joseph J, Baumann M, Birmingham K, Sahn SA,Strange C. Early inflammatory response of minocycline andtetracycline on the rabbit pleura. Chest 1993; 104:1585-88
3 Hatta T, Tsubota N, Yoshimura M, Yanagawa M. Intrapleuralminocycline for postoperative air leakage and control ofmalignant pleural effusions. Kyobu Geka 1990; 43:283-86
4 Light RW, Sassoon CSH, Vargas FS, Gruer SE, Despars JA,Wang NS. Comparison of the effectiveness of tetracycline andminocycline as pleural sclerosing agents in rabbits [abstract].Am Rev Respir Dis 1992; 145:A868
5 Kitamura S, Sugiyama Y, Izumi T, Hayashi R, Kosaka K.Intrapleural doxycycline for control of malignant pleural effu-sion. Curr Ther Res 1981; 30:515-21
6 Mansson T. Treatment of malignant pleural effusion with dox-ycycline. Scand J Infect Dis 1988; 53:29-34
7 Adler RH, Sayek I. Treatment of malignant pleural effusion: amethod using tube thoracostomy and talc. Ann Thorac Surg1976; 22:8-15
8 Prorok J, Nealon TF. Pleural symphysis by talc poudrage in thetreatment of malignant pleural effusion. Bull Soc Int Chir 1968;6:630-35
9 Webb WR, Ozmen V, Moulder PV, Shabahang B, Breaux J.Iodized talc pleurodesis for the treatment of pleural effusions.J Thorac Cardiovasc Surg 1992; 103:881-86
10 Gruner JW. The crystal structure of talc and pyrophillite. ZeitKrist 1934; 88:412-19
11 Rayner JH, Brown G. Triclinic form of talc. Nature 1966;212:1352-53
12 Ross M, Smith WL, Ashton WH. Triclinic talc and associatedamphiboles from gouverner mining district, New York. AmMinerol 1968; 53:751-69
13 Rohl AN, Langer AM, Selikoff IJ, Todini A, Klimentidis R,Bowes DR, et al. Consumer talcums and powders: mineral andchemical characterization. J Toxicol Environ Health 1976;2:255-84
14 Weiss B, Boettner EA. Commercial talc and talcosis. Arch En-viron Health 1967; 14:304-08
15 Bethune N. A new technic for the deliberate production ofpleural adhesions as a preliminary to lobectomy. J Thorac Surg1935; 4:251-61
16 Singer JJ, Jones JC, Tragerman LJ, Sherman L. Aseptic pleuri-tis experimentally produced. J Thorac Surg 1941; 10:251-83
17 Hanrahan EM, Adams R, Klopstock R. The role of experimen-tally produced intrapleural adhesions in extrapleural pneu-monolysis and the prevention of surgical atelectasis in animals.J Thorac Surg 1941; 10:284-99
18 Frankel A, Krasna I, Baronofsky ID. An experimental study ofpleural symphysis. J Thorac Cardiovasc Surg 1961; 42:43-51
19 Mathlouthi A, Chabchoub A, Labbene N, Amara A, Ghorbel A,Kacem S, et al. Etude anatomopathologique experimentale dutalcage pleural. Rev Mal Respir 1992; 9:617-21
20 Schepers GWH, Durkan TM. An experimental study of theeffects of talc dust on animal tissue. Arch Indust Health 1955;12:317-28
21 Smith WG, Rothwell PPG. Treatment of spontaneous pneu-mothorax. Thorax 1962; 17:342-49
22 United States Pharmacopea XXII. 22nd ed. Rockville, MD:Mack Printing, 1990; 1309-10
23 Daniel TM, Tribble CG, Rodgers BM. Thoracoscopy and talcpoudrage for pneumathoraces and effusions. Ann Thorac Surg1990; 50:186-89
24 Camishon RC, Gibbon JH, Nealon TF. Talc poudrage in thetreatment of pleural effusion due to cancer. Surg Clin NorthAm1962; 42:1521-26
25 Chambers JS. Palliative treatment of neoplastic pleural effusionwith intercostal intubation and talc instillation. West J SurgObstet Gynecol 1958; 66:26-8
Talc Pleurodesis for Pneumothorax and Pleural Effusion Treatment (Kennedy, Sahn)1220
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

26 Hartman DL, Gaither JM, Kesler KA, Mylet DM BJ, MathurPN. Comparison of insufflated talc under thoracoscopic guid-ance with standard tetracycline and bleomycin pleurodesis forthe control of malignant pleural effusions. J Thorac CardiovascSurg 1993; 105:743-48
27 Jones GR. Treatment of recurrent malignant pleural effusion byiodized talc pleurodesis. Thorax 1969; 24:69-73
28 Kennedy L, Rusch VW, Strange C, Ginsberg RJ, Sahn SA.Pleurodesis using talc slurry. Chest (in press)
29 Aelony Y, King R, Boutin C. Thoracoscopic talc poudragepleurodesis for chronic recurrent pleural effusions. Ann InternMed 1991; 115:778-82
30 Bubik JS. Preparation of sterile talc for the treatment of pleu-ral effusion. Am J Hosp Pharm 1992; 49:562-63
31 Steele JD. Production of pleural adhesions for therapeuticpurposes. Am Rev Tuberc 1947; 56:299-302
32 Meade RH, Blades BB. The surgical treatment of recurrent andchronic spontaneous pneumothorax of nontuberculous origin.Am Rev Tuberc 1949; 60:683-98
33 Gaensler EA. Parietal pleurectomy for recurrent spontaneouspneumothorax. Surg Gynecol Obstet 1956; 102:293-308
34 Tunon-de-Lara JM, Constans J, Vincent MP, Receveur MC,Conri C, Taytard A. Spontaneous pneumothorax associatedwith Pneumocystis carinil pneumonia: successful treatmentwith talc pleurodesis. Chest 1992; 101:1177-78
35 Bourke S, Kelly C, Bundi RS, Boyd G. Bilateral talc pleurode-sis in metastatic pneumothorax [letter]. Chest 1987; 92:576
36 Crosby DJ. Catamenial pneumothorax. Ariz Med 1973;30:260-61
37 Dieter RA, Leisen GJ. Vicarious menstruation and recurrentcatamenial pneumothorax. Ill Med J 1981; 159:234-36
38 Warren SE, Lee D, Martin V, Messink W. Pulmonary lym-phangiomyomatosis causing bilateral pneumothorax duringpregnancy. Ann Thorac Surg 1993; 55:998-1000
39 Tribble CG, Selden RF, Rodgers BM. Talc poudrage in thetreatment of spontaneous pneumathoraces in patients withcystic fibrosis. Ann Surg 1986; 204:677-79
40 Spector ML, Stern RC. Pneumothorax in cystic fibrosis: a26-year experience. Ann Thorac Surg 1989; 47:204-07
41 Almind M, Lange P, Viskum K. Spontaneous pneumothorax:comparison of simple drainage, talc pleurodesis, and tetracy-cline pleurodesis. Thorax 1989; 44:627-30
42 Nandi P. Recurrent spontaneous pneumothorax: an effectivemethod of talc poudrage. Chest 1980; 77:493-95
43 Aelony Y. Thoracoscopic talc poudrage: comparison with tet-racycline and use in Hodgkin's disease [letter]. Chest 1992;102:1922-23
44 Adler RH, Levinsky L. Persistent chylothorax: treatment by talcpleurodesis. J Thorac Cardiovasc Surg 1978; 76:859-64
45 Frey JG, Tschopp JM. Chylothorax: traitement par pleurodeseau talc. Schweiz Med Wochenschr 1987; 117:1624-27
46 Gingell JC. Treatment of chylothorax by producing pleurode-sis using iodized talc. Thorax 1965; 20:261-69
47 Ohri SK, Oswal SK, Townsend ER, Fountain SW. Early and lateoutcome after diagnostic thoracoscopy and talc pleurodesis.Ann Thorac Surg 1992; 53:1038-41
48 Kaine JL. Refractory massive pleural effusion in systemic lupuserythematosus treated with talc poudrage. Ann Rheum Dis1985; 44:61-4
49 Weissberg D, Kaufman M. The use of talc for pleurodesis in thetreatment of resistant empyema. Ann Thorac Surg 1986;41:143-45
50 Fentiman IS, Rubens RD, Hayward JL. Control of pleural ef-fusions in patients with breast cancer. Cancer 1983; 52:737-39
51 Hamed H, Fentiman IS, Chaudary MA, Rubens RD. Compar-ison of intracavitary bleomycin and talc for the control ofpleural effusions secondary to carcinoma of the breast. Br J Surg
1989; 76:1266-6752 Weissberg D. Bleomycin and talc for the control of pleural ef-
fusions. Br J Surg 1990; 77:99553 Fentiman IS, Rubens RD, Hayward JL. A comparison of in-
racavitary talc and tetracycline for the control of pleural effu-sions secondary to breast cancer. Eur J Cancer Clin Oncol 1986;22:1079-81
54 Sorensen PG, Svendsen TL. Treatment of malignant pleuraleffusion with drainage, with and without instillation of talc. EurJ Respir Dis 1984; 65:131-35
55 Walker-Renard P, Vaughn L, Sahn SA. Chemical pleurodesisfor the treatment of malignant pleural effusions. Ann InternMed 1994; 120:56-64
56 Pouwels HMM, Wouters EFM. Spontaneous pneumothorax.Lancet 1989; 335:607
57 Miller KS, Sahn SA. Chest tubes: indications, technique, man-agement and complications. Chest 1987; 91:258-64
58 Todd TRJ, Delarue NC, Ilves R, Pearson FG, Cooper JD. Talcpoudrage for malignant pleural effusion [abstract]. Chest 1980;78:542-43
59 Gamble LF, Fellner W, Dimeo MJ. An epidemiologic study ofa group of talc workers. Am Rev Respir Dis 1979; 119:741-53
60 Tomashefski JF, Hirsch CS. The pulmonary and vascularlesions of intravenous drug abuse. Hum Pathol 1980; 11:133-45
61 Hopkins GB, Taylor DG. Pulmonary talc granulomatosis: acomplication of drug abuse. Am Rev RespirDis 1970; 101:101-04
62 Crouch E, Churg A. Progressive massive fibrosis of the lungsecondary to intravenous drug abuse. Am J Clin Pathol 1983;80:520-26
63 Rinaldo JE, Owens GR, Rogers RM. Adult respiratory distresssyndrome following intrapleural instillation of talc. J ThoracCardiovasc Surg 1983; 85:523-26
64 Bouchama A, Chastre J, Gaudichet A, Soler P, Gibert C. Acutepneumonitis with bilateral pleural effusion after talc pleuro-desis. Chest 1984; 86:795-97
65 Pearson FG, MacGregor DC. Talc poudrage for malignantpleural effusion. J Thorac Cardiovasc Surg 1966; 51:732-38
66 Lange P, Mortensen J, Groth S. Lung function 23-35 years af-ter treatment of idiopathic spontaneous pneumothorax withtalc poudrage or simple drainage. Thorax 1988; 43:559-61
67 Knowles JH, Storey CF. Effects of pleural talc poudrage onpulmonary function. J Thorac Surg 1957; 34:250-56
68 Paul JS, Beattie EJ, Blades B. Lung function studies in poudragetreatment of recurrent spontaneous pneumothorax. J ThoracSurg 1951; 22:52-61 A
69 McGahren ED, Teague WG, Flanagan T, White B, RodgersBM. The effects of talc pleurodesis on growing swine. J Pedi-atr Surg 1990; 25:1147-51
70 Chappell AG, Johnson A, Charles JWJ, Seal RME, Berry G,Nicholson D. A survey of the long-term effects of talc and ka-olin pleurodesis. Br J Dis Chest 1979; 73:285-88
71 Kleinfeld M, Messite J, Kooyman 0, Zaki MH. Mortality amongtalc miners and millers in new york state. Arch Environ Health1967; 14:663-67
72 Jackson JW, Bennett MH. Chest wall tumour following iodizedtalc pleurodesis. Thorax 1969; 28:788-93
73 Shefts LM, Gilpatrick C, Swindell H, Gabbard JG. Manage-ment of spontaneous pneumothorax. Dis Chest 1954; 26:273-85
74 Marrangoni AG, Storey CF, Geib PO. The management ofspontaneous pneumothorax. Am Rev Tuberc Pulm Dis 1955;72:257-67
75 Verschoof AC, Ten Velde GPM, Greve LH, Wouters EFM.Thoracoscopic pleurodesis in the management of spontaneouspneumothorax. Respiration 1988; 53:197-200
76 Van de Brekel JA, Duurkens VAM, Vanderschueren RGJRA.Pneumothorax: results of thoracoscopy and pleurodesis withtalc poudrage and thoracotomy. Chest 1993; 103:345-47
CHEST / 106 / 4 / OCTOBER, 1994 1221
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017

77 Haupt GJ, Camishon RC, Templeton JY. Treatment of malig-nant pleural effusions by talc poudrage. JAMA 1960; 172:918-21
78 Starkey GWB. Recurrent malignant pleural effusions. N EnglJ Med 1964; 270:436-38
79 Adler RH, Rappole BW. Recurrent malignant pleural effusionsand talc powder aerosol treatment. Surgery 1967; 62:1000-06
80 Bloomberg AE. Thoracoscopy in diagnosis of pleural effusions.N Y State J Med 1970; 70:1974-77
81 Shedbalker AR, Head JM, Head LR, Murphy DJ, Mason JH.
Evaluation of talc pleural symphysis in management of malig-nant pleural effusion. J Thorac Cardiovasc Surg 1971; 61:492-97
82 Harley HRS. Malignant pleural effusions and their treatmentby intercostal talc pleurodesis. Br J Surg 1979; 73:173-77
83 Weissberg D, Kaufman M, Zurkowski Z. Pleuroscopy inpatients with pleural effusion and pleural masses. Ann ThoracSurg 1980; 29:205-08
84 Weissberg D, Kaufman M. Diagnostic and therapeutic pleuro-scopy: experience with 127 patients. Chest 1980; 78:732-35
Talc Pleurodesis for Pneumothorax and Pleural Effusion Treatment (Kennedy, Sahn)1 222
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21701/ on 04/03/2017





























